Submitted:
31 July 2024
Posted:
02 August 2024
Read the latest preprint version here
Abstract
The medical research field has been tremendously galvanized to improve the prediction of therapy efficacy by the revolution in artificial intelligence (AI). An earnest desire to find better ways to predict the effectiveness of therapy with the use of AI has propelled the evolution of new models in which it can become more applicable in clinical settings such as breast cancer detection. However, in some instances, the U.S. Food and Drug Administration was obliged to back some previously approved inaccurate models for AI-based prognostic models because they eventually produce inaccurate prognoses for specific patients who might be at risk of heart failure. In light of instances in which the medical research community has often evolved some unrealistic expectations regarding the advances in AI and its potential use for medical purposes, implementing standard procedures for AI-based cancer models is critical. Specifically, models would have to meet some general parameters for standardization, transparency of their logistic modules, and avoidance of algorithm biases. In this review, we summarize the current knowledge about AI-based prognostic methods and describe how they may be used in the future for predicting antibody-drug conjugate efficacy in cancer patients. We also summarize findings of recent late-phase clinical trials using these conjugates for cancer therapy.
Keywords:
artificial intelligence
; antibody drug conjugates
; prognostic
; clinical trials
Introduction
Many aspects of society have been influenced by the recent advancements in artificial intelligence (AI). Medicine is one field with the potential for a gradual revolution through the use of AI in the development of drugs and their implementation in clinical trials, stratification of patients for treatment, and prediction of response to cancer therapy. Overall, the purpose of AI in medicine is to reduce humans’ workload while achieving objectives more effectively. It fits in all aspects of medicine, ranging from communication and managerial organization to aiding the more complex issue of selecting therapies for patients.
AI functions through machine learning (ML) algorithms, which can find common patterns within a series of data sets that require classification. Deep learning (DL) is a subset of ML that employs artificial neural networks. DL involves more sophisticated and interconnected elements than ML, which resemble electrical impulses in the human brain [1]. When artificial neural networks receive an input, they are trained based on it and use single or multiple linked algorithms to solve problems [2]. The three types of artificial neural networks are multilayer perceptron networks, recurrent neural networks, and convolutional neural networks. They use either supervised or unsupervised training procedures [2,3].
Pharmaceutical companies have used these new AI technologies recently for faster testing of new drugs [4]. Worth noting is that newly discovered drugs have been ranked based on efficacy values (IC50 and binding affinity) through molecular simulations and ultimately via in vitro validation experiments. This could be used to discover new drugs more efficiently. Therefore, feeding such AI databases could derive more powerful and targeted pharmaceutical products. [5,6]
Historically, the process of drug development has been very slow and expensive. The steps from initiation of a drug discovery program to approval by a national drug regulatory agency take 12-15 years [1]. Also, the average cost to bring a drug to the market is $2.5 billion [7]. Demonstration of the effectiveness of AI-based methods in shortening these times and reducing these costs in future clinical trials will prove their validity. Recently, a Boston Consulting Group investigation evinced that AI could cut drug discovery costs and time by 25-50% up to the clinical testing stage and that in a 2022 analysis, 20 AI-intensive companies had developed 158 drug candidates compared with 333 candidates developed by other 20 big pharmaceutical companies, which are the world’s largest pharmaceutical companies [4]. This provides a glimpse at how fast this field is evolving.
In contrast with conventional chemotherapy, which can damage healthy cells, antibody-drug conjugates (ADCs) deliver chemotherapeutic agents to cancer cells in a more specific manner, targeting cancer cells only [8]. ADCs rely on a monoclonal antibody’s recognition of a specific target expressed on the surface of cancer cells. After the antibody recognizes a receptor on a cell, the ADC is internalized by the cell. The ADC then releases the cytotoxic drug via a linker attached to the antibody inside the cancer cell, permitting the specific release of the drug to the cancer cells having that specific cell membrane receptor. Fully human monoclonal antibodies are highly targeted, have long circulating half-lives, and have low immunogenicity. The role of the linker in this process is paramount because they should firmly keep the payload bound to the antibody. These drug conjugates should be constructed to be stable enough to prevent cleavage of the linker before they become internalized in cancer cells [8,9]. If the payload is accidentally released before reaching its target, it could cause toxicity. Among the benefits of this type of therapy related to the specificity of antibody-receptor recognition is a reduction in toxicity because much fewer normal cells are targeted than in conventional chemotherapy. Therefore, dose escalation could be performed using ADCs, enhancing the efficacy of treatment [10]. Currently, 13 ADCs are approved by the U.S. Food and Drug Administration (FDA), and 100 are going through clinical trials [10].
In this review, we summarize the current knowledge about AI-based prognostic methods and describe how they may be used in the future for predicting antibody-drug conjugate efficacy in cancer patients. We also summarize findings of recent late-phase clinical trials using these conjugates for cancer therapy.
Prediction of Cancer Responsiveness and Resistance to ADCs
Various AI methods have been developed to develop new cancer drugs, cancer prognoses, and responses to cancer therapies. These technologies are discussed below to show how they can be employed in the construction of new AI algorithms for the use of ADCs, specifically, in identifying potential challenges in the field of oncology and cancer therapy selection and determining how they could be solved based on the knowledge generated in related fields where AI has produced promising results.
Researchers have developed many AI methods to discover potential anticancer drugs. Because drug discovery is beyond the scope of this review, we mention only a few to explain how they are being employed in medical research around the world. The mainstream AI methods employed for drug discovery use a wide variety of data resources, such as ChEMBL and DrugBank. AI converts such data into computer-readable formats. After the drugs’ potential efficacy is ranked, their toxicity, bioactivity, and physicochemical properties are ranked. [11] The Response Algorithm for Drug Positioning and Rescue (Lantern Pharma) is an AI platform capable of rapidly developing novel ADC, including cryptomycin-derived ADCs. This technology integrates data from preclinical and clinical tests, such as data in CellMinerCDB [12] with The Cancer Genome Atlas [13], the Catalogue of Somatic Mutations in Cancer [14], the Gene Expression Omnibus [15,16], and identifying published articles, to generate new insights into the drug structures and targeting of proteins of interest. Another developing algorithm is AtomNet, which is very effective in predicting the binding activity of novel chemicals to their intended therapeutical targets. [17] Various AI-based tools are capable of identifying the physicochemical properties of drugs. Each pharmaceutical company may have a patent-protected AI drug discovery method, which complicates the comparison of the methods. A more comprehensive review of AI drug discovery methods was performed by Paul et al. [1]
Conceivably, these algorithms and databases could be adapted to test ADC responsiveness during clinical trials. Of note is that the potential of an AI system depends on the quality of the data used to feed the ML process. Table 1 summarizes the current databases that can be used to create AI models for cancer therapy response prediction, drug design. With the accrual of information from clinical studies on molecular biomarkers in tumor tissue, circulating tumor DNA [18,19], or circulating cell-free DNA [20,21] more data is generated that could help to predict the responsiveness of cancer to therapy, having AI systems to help process such data more efficiently would be beneficial. This could result in the provision of real-time information to physicians regarding the potential responsiveness of cancer to ADCs and what courses of action could be planned in case a drug is statistically likely to fail in a specific case.
Currently, AI-aided methods of cancer prognosis have demonstrated notable advances when compared with image-based prognosis. For example, the combination of radiomics and AI has successfully extracted and processed multidimensional data from cancer images, such as magnetic resonance imaging, computed tomography, ultrasound (US), digital subtraction angiography, and X-ray images [22]. For hepatocellular carcinoma (HCC) patients, AI coupled with radiomics has shown the potential to improve tumor characterization and offer a better prognosis than conventional radiological methods. This coupling yields insights into the complex relationship between radiomic variables and clinical outcomes [23]. The process of automatic segmentation in programming ML, which delineates the volume of interest, could help predict treatment response [24,25]. Also, DL can bypass the conventional steps of ML radiomic analysis. The output is calculated via DL through filtering and calculations of unprocessed images of HCC lesions serving as inputs. The outputs can include prediction of response or nonresponse to treatment. Furthermore, convolutional neural networks are capable of learning, thereby increasing the accuracy of their overall prediction of ML [26]. Notably, DL can incorporate time as a variable during the evaluation of lesion enhancement patterns in images [27,28]. DL requires more computational power than ML and is more dependent on training with large data sets and a variety of data. DL has greater potential than ML to predict the response of cancers to therapy. In the future, this could be used for ADC-based therapy response prediction, as well.
Zhang et al. [27] used a DL system to make an automatic tumor segmentation model capable of integrating clinical variables and preprocedural digital subtraction angiography videos to predict the response of ADC to transarterial chemoembolization. The authors observed a marked difference in the 3-year progression-free survival rate between responders and nonresponders with their fully automated framework (DSA-Net). Their DSA-Net entails a U-net model employed to automate tumor segmentation (Model 1) and a ResNet model that is used to predict response to therapy to the first TACE (Model 2). Both models were tested in 360 patients. For validation 124 internal patients and 121 external patients’ data were used. Also, Peng et al. [29] developed a pyradiomics method to predict the response of TACE treatment based on a conventional ML model that was capable of predicting the initial response of cancer to transarterial chemoembolization by exploiting pretreatment computed tomography images. They showed that patients predicted to be treatment responders had longer progression-free and overall survival than predicted nonresponders. Additionally, Peng and colleagues applied this model to 46 HCC patients with data in The Cancer Genome Atlas to analyze the differential gene expression across their cohort and the TCGA-HCC cohort to explore the potential mechanisms of action of transarterial chemoembolization. They further used ML to incorporate TCGA genetic data into their data, again showing how versatile this ML method can be in processing large data sets.
Researchers have also examined post-ablation prognosis for cancer therapy using AI. For example, Ma et al. [28] compared the performance of a DL model trained using contrast-enhanced US (CEUS) with that of a conventional ML model trained using static US to predict HCC recurrence after ablation. As expected, the DL model outperformed the ML model, possibly because CEUS, besides providing morphological images, can provide real-time dynamic blood perfusion information that correlates well with the success of ablation.
In addition, Liu et al. [10] used clinical data as well as features extracted from CEUS images to predict the 2-year progression-free survival rate in early-stage HCC patients who underwent radiofrequency ablation and surgical resection as well as to determine the optimal treatment for these patients. They found that 17.3% and 27.3% of the patients receiving radiofrequency ablation and surgical resection, respectively, would have had better outcomes if they had received the other treatment instead. A multicenter study with more patients is needed to determine the statistical power of this study. However, this study still demonstrates the potential of AI methods in selecting optimal ADC-based treatments for cancer patients.
Despite the encouraging findings, these image-based AI methods require further testing and standardization before they can be effectively integrated into clinical practice. They are operator-dependent and involve different machines, variables, and contrast doses as well as timing [30].
These and similar AI models used for cancer prognostication must be improved to ensure safe and effective patient care. They also must be submitted for and receive FDA approval before implementation in clinical settings. Recently, the FDA proposed a pathway that could lead to the use of ML software applications as medical devices [31]. The AI model should include the following: 1) good ML practice, which means it should be evidence-based for reproducibility purposes, have standardized steps (e.g., the extraction algorithms), use different time points to permit generalizability [32], and have the consistency of AI analysis and increase the operability across clinical institutions around the world [22,33]; 2) avoidance of algorithm biases, which should be ensured by validating the testing process with external data to confirm the generalizability of the model; and 3) transparency of the AI models’ logic, which could be achieved by clearly explaining the mechanisms of the AI decision-making process and familiarizing oncologists with these new models [34,35,36].
Standardization of the protocols can be achieved by specifically following commonly approved steps and protocols. One such step is having open databases where previous ADC data could be stored and made available for training purposes.
For decades, prediction tools have been used to support clinical decisions regarding therapy selection, including the ABCD [37] score [38], Framingham Risk Score [39], Model for End-Stage Liver Disease [40], and Nottingham Prognostic Index [41]. In recent years, hundreds of more prediction model studies have appeared [42]. To prevent the scientific community from becoming mesmerized by the AI revolution and enable ML prediction models to be appropriately developed, tested, and, if needed, tailored to different contexts before they can be employed in daily medical practice, steps have been taken. In response, new methods have been deemed necessary to resolve the issue of incomplete reporting of models in prediction model studies [43,44]. Specifically, The Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) method was designed to guide the key items to report in new studies or update clinical prediction models [45,46,47]. In AI-based discovery of medical diagnosis, one must also consider that some FDA-approved clinician-free, AI-based imaging diagnostic tools used for the identification of wrist fractures and strokes in adults have given false diagnoses [48]. This shows the importance of having methods to facilitate the organic, healthy development of new AI-based prognostic methods. It also shows how today AI is not unfailing.
Previously, the TRIPOD method was based on the use of regression models. However, a new TRIPOD initiative specific to ML has been developed. This initiative aims to use ML prediction algorithms to establish long-term standardized methodologies for the prediction of prognostic and diagnostic prediction models. New guidelines for the efficient use of prognostic models should be made available with the TRIPOD-Artificial Intelligence (TRIPOD-AI) tool and the Prediction model Risk of Bias Assessment Tool-Artificial Intelligence (PROBAST-AI) [49]. These guidelines are valuable for many AI-based prognostic models, including future methods to predict ADC efficacy. TRIPOD-AI and PROBAST-AI are being developed following guidance from the EQUATOR Network, which consists of five stages: 1) two systematic reviews to examine the quality of the published ML prediction model studies, 2) consultation with key stakeholders using the Delphi method to identify items that should be included in the method, 3) virtual consensus meetings to consolidate and prioritize the key items to be included, 4) development of a TRIPOD-AI checklist and the PROBAST-AI tool, and 5) dissemination of information about the new written algorithms the TRIPOD-AI and PROBAST-AI in journals, conferences, and social media [49].
Another field in which AI has recently shown great promise is cancer immunotherapy. Immunotherapy consists of controlling and eliminating tumors in the human body by eliciting the body’s immune system against cancer, leading to an antitumor immune response. The two main cancer immunotherapy types are immune checkpoint blockade and adoptive cell therapy [50]. AI technology can be used for neoantigen recognition, antibody design, and immunotherapy response prediction [51]. Also, AI can be used to predict new tumor antigens in patients’ cancer rapidly and accurately, reducing experimental screening and validation costs. AI-enhanced antibodies can be developed that have the potential for further success than conventional therapies in cancer treatment. Finally, AI can be used to identify patients whose disease may respond to immunotherapy using multimodal, multiscale biomarkers and immune microenvironments feeding the algorithms for prediction [51].
Anticancer ADCs that Have Entered Clinical Trials
After years of research and refinement, significant technological advancements, and a deeper understanding by the scientific community of ADC mechanisms have culminated in the FDA's approval of 11 ADCs, each offering tangible benefits to cancer patients. Among them, fam-trastuzumab deruxtecan-nxki (Enhertu) stands out, as it is poised to capture a substantial market share within the ADC landscape. Its versatility in treating various breast cancer subsets (HER2+, HR+/HER2-, and triple-negative) and extended treatment duration underscore its potential positive impact on breast cancer therapy.
Despite the inherent risks associated with drug development, the trajectory of novel anticancer therapies suggests an imminent surge in ADC approvals. Whether through the introduction of novel ADCs or chemical modification of previous drugs, the outlook for ADC-based cancer therapy is promising. Since the inception of the first ADC clinical trial in 1997, the field has witnessed remarkable proliferation, with 266 additional ADCs undergoing evaluation in more than 1,200 clinical trials. This surge indicates a paradigm shift toward targeted cancer therapy.
Presently, 275 clinical ADC trials are active (Table 2), in which investigators are testing different ADCs for accurate delivery of cytotoxic agents (Figure 1), which in the future could be done with the help of AI (Figure 2). Notably, discontinued ADCs also underwent rigorous clinical testing, reflecting the commitment to scientific rigor and patient safety regarding treatment with these agents.
Moreover, the therapeutic potential of ADCs transcends oncology, extending into realms such as autoimmune and cardiovascular diseases, diabetes, and antimicrobial infections. For instance, Seagen has initiated a phase 2 clinical trial (NCT03222492) exploring the utility of the ADC brentuximab vedotin (Adcetris) in treating systemic sclerosis, addressing a significant unmet medical need. Leveraging the established safety profile of and accumulated clinical data on Adcetris, Seagen anticipates promising outcomes in this trial. Additionally, repurposing of ADCs offers expedited development timelines and enhanced cost efficiency, thereby enhancing their attractiveness to pharmaceutical companies. Furthermore, brentuximab vedotin was approved by the FDA for the treatment of Hodgkin lymphoma in combination with chemotherapy in 2018.
Although cancer has served as the proving ground for ADC-based therapies, their applicability across diverse medical domains is increasingly being recognized. With growing interest from major pharmaceutical companies, the ADC market is poised for sustained expansion, fueling optimism for the emergence of blockbuster ADCs in the near future.
Figure 2.
Clinically tested ADCs. This bar graph shows the 277 ADCs that have undergone clinical trials along with their trial status (completed, active/recruiting, not yet recruiting, suspended, and unknown). Additionally, to the right of the main Total bar, the active/recruiting ADCs are broken down into additional columns to highlight their highest developmental stage (phases 1-4 [P1-P4]).
Figure 2.
Clinically tested ADCs. This bar graph shows the 277 ADCs that have undergone clinical trials along with their trial status (completed, active/recruiting, not yet recruiting, suspended, and unknown). Additionally, to the right of the main Total bar, the active/recruiting ADCs are broken down into additional columns to highlight their highest developmental stage (phases 1-4 [P1-P4]).
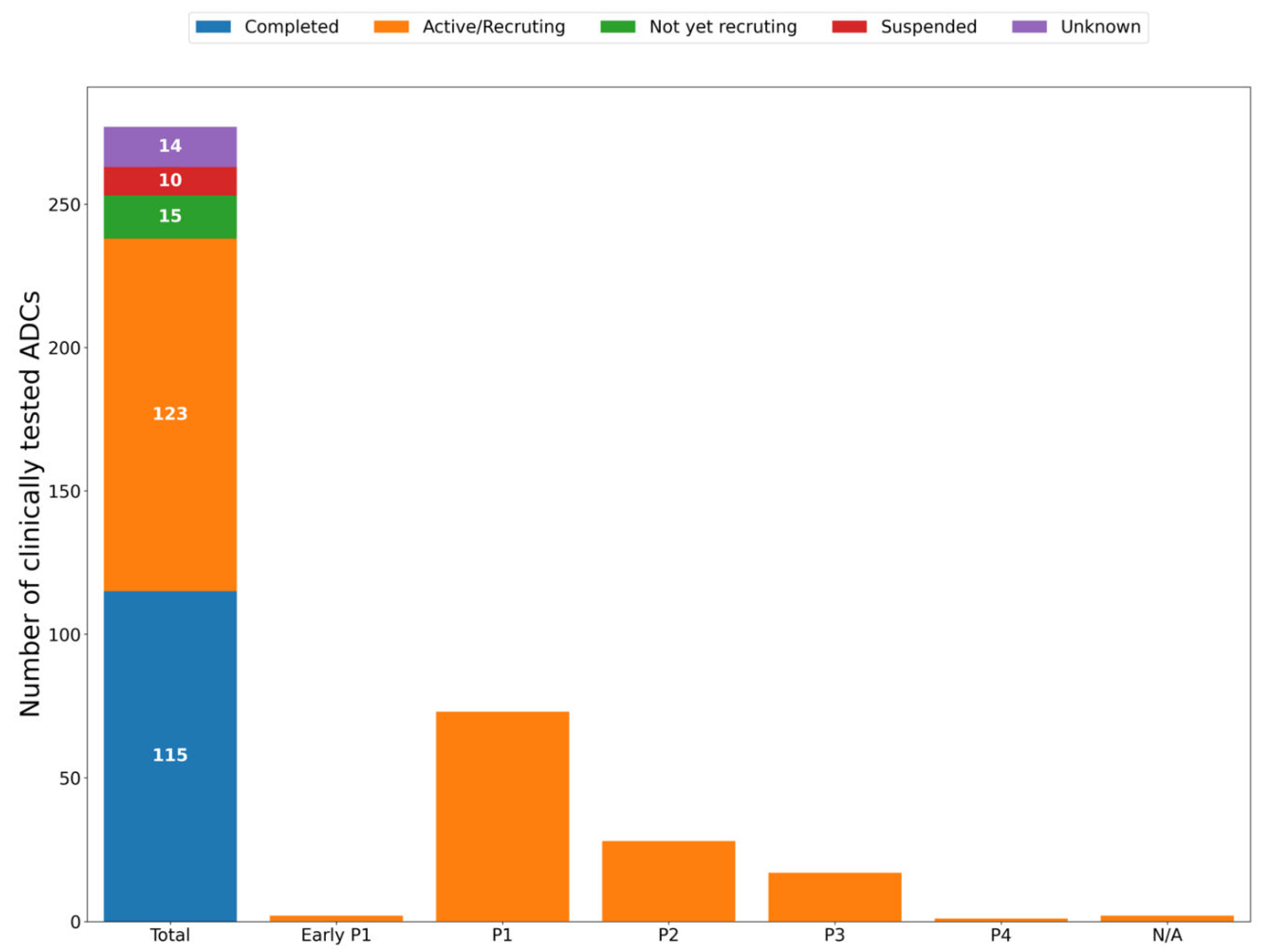
Figure 2.
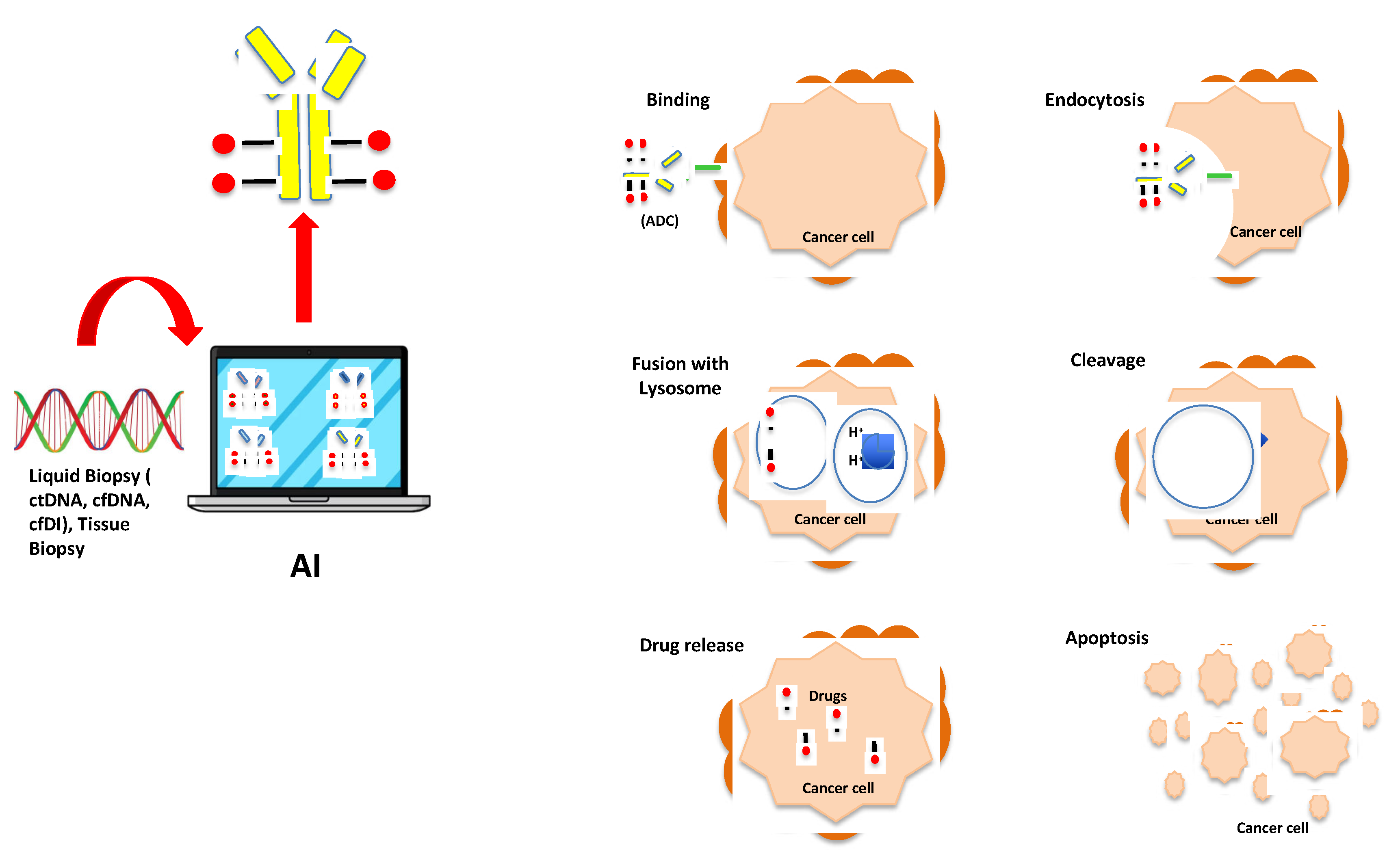
Artificial intelligence assisted antibody-drug conjugate selection for the treatment of cancer.
Figure 2.
Artificial intelligence assisted antibody-drug conjugate selection for the treatment of cancer.
Discussion
Over the past decade, advances in AI have pushed the boundaries of the medical field. Despite the successful development and use of AI-based diagnostic tools for prediction of cancer treatment response, response to certain targeted therapies remains unpredictable. However, in the field of ADCs, in which cancer patients are stratified for treatment based on the expression of a receptor on the cancer cell membrane that can be specifically bound by an antibody carrying the cytotoxic payload, more accurate prognostic methods that can predict whether patients’ disease would respond to ADCs are needed. ML has shown great potential in many fields, including mammography for early breast cancer detection, it could play an important role in this prediction of ADC response in cancer therapy based on data coming from biomarkers that can be found in liquid biopsy or tissue samples or even the tumor microenvironment.
Ethics approval and consent to participate
Not applicable to this review article.
Availability of data and material
Not applicable to this review article.
Competing interests
The authors declare that they have no conflict of interest.
Author Contributions
N.S. wrote the first draft, researched the literature, and revised the manuscript; A.D.A. contributed with his medical expertise to the clinical trials section; G.M. wrote her medical overview and opinion in the introduction and discussed the manuscript; M.P. helped summarize the field and composed the Figure 2; D.G. gave the original idea, revised the paper and figures.
Funding
No funding to report.
References
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2020, 26, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Luc Steels, RB. The Artificial Life Route to Artificial Intelligence (1995).
- Bielecki, A. Models of Neurons and Perceptrons: Selected Problems and Challenges; Springer Nature: Dordrecht, GX, Netherlands, 2019. [Google Scholar]
- AI's potential to accelerate drug discovery needs a reality check. Nature, 622(7982), 217 (2023).
- Schneider, G. Automating drug discovery. Nature Reviews Drug Discovery, 17, 97–113 (2018).
- Sobhani, N.; Tardiel-Cyril, D.R.; Chai, D.; Generali, D.; Li, J.-R.; Vazquez-Perez, J.; Lim, J.M.; Morris, R.; Bullock, Z.N.; Davtyan, A.; et al. Artificial intelligence-powered discovery of small molecules inhibiting CTLA-4 in cancer. BJC Rep. 2024, 2, 1–15. [Google Scholar] [CrossRef] [PubMed]
- DiMasi, J.A.; Grabowski, H.G.; Hansen, R.W. Innovation in the pharmaceutical industry: New estimates of R&D costs. J. Health Econ. 2016, 47, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.; Brown, S. Antibody–drug conjugates as novel anti-cancer chemotherapeutics. Biosci. Rep. 2015, 35, e00225. [Google Scholar] [CrossRef]
- Sobhani, N. NEW AND MOST POWERFUL MOLECULES FOR THE TREATMENT AND DIAGNOSIS OF NEUROENDOCRINE CANCERS (NETs) AND THE STEM CELLS OF NETs. In:. Google Patents . (Ed.^(Eds) (Navid Sobhani, Italy, 2018. [Google Scholar]
- Liu, K.; Li, M.; Li, Y.; Li, Y.; Chen, Z.; Tang, Y.; Yang, M.; Deng, G.; Liu, H. A review of the clinical efficacy of FDA-approved antibody‒drug conjugates in human cancers. Mol. Cancer 2024, 23, 1–16. [Google Scholar] [CrossRef]
- Chen, W.; Liu, X.; Zhang, S.; Chen, S. Artificial intelligence for drug discovery: Resources, methods, and applications. Mol. Ther. - Nucleic Acids 2023, 31, 691–702. [Google Scholar] [CrossRef]
- Rajapakse, V.N.; Luna, A.; Yamade, M.; Loman, L.; Varma, S.; Sunshine, M.; Iorio, F.; Sousa, F.G.; Elloumi, F.; Aladjem, M.I.; et al. CellMinerCDB for Integrative Cross-Database Genomics and Pharmacogenomics Analyses of Cancer Cell Lines. iScience 2018, 10, 247–264. [Google Scholar] [CrossRef]
- Tomczak, K.; Czerwińska, P.; Wiznerowicz, M. Review The Cancer Genome Atlas (TCGA): an immeasurable source of knowledge. Contemp. Oncol. 2015, 2015, 68–77. [Google Scholar] [CrossRef]
- Tate, J.G.; Bamford, S.; Jubb, H.C.; Sondka, Z.; Beare, D.M.; Bindal, N.; Boutselakis, H.; Cole, C.G.; Creatore, C.; Dawson, E.; et al. COSMIC: The Catalogue of Somatic Mutations in Cancer. Nucleic Acids Res. 2019, 47, D941–D947. [Google Scholar] [CrossRef]
- Edgar, R.; Domrachev, M.; Lash, A.E. Gene Expression Omnibus: NCBI gene expression and hybridization array data repository. Nucleic Acids Res. 2002, 30, 207–210. [Google Scholar] [CrossRef]
- Barrett, T.; Wilhite, S.E.; Ledoux, P.; Evangelista, C.; Kim, I.F.; Tomashevsky, M.; Marshall, K.A.; Phillippy, K.H.; Sherman, P.M.; Holko, M.; et al. NCBI GEO: archive for functional genomics data sets—update. Nucleic Acids Res. 2012, 41, D991–D995. [Google Scholar] [CrossRef] [PubMed]
- Izhar Wallach MD, Abraham Heifets. AtomNet: A Deep Convolutional Neural Network for Bioactivity Prediction in Structure-based Drug Discovery. arXiv, (2015).
- Sobhani N, Generali D, Zanconati F, Bortul M, Scaggiante B. Cell-free DNA integrity for the monitoring of breast cancer: Future perspectives? World J Clin Oncol, 9(2), 26-32 (2018).
- Conca, V.; Ciracì, P.; Boccaccio, C.; Minelli, A.; Antoniotti, C.; Cremolini, C. Waiting for the “liquid revolution” in the adjuvant treatment of colon cancer patients: A review of ongoing trials. Cancer Treat. Rev. 2024, 126, 102735. [Google Scholar] [CrossRef] [PubMed]
- Sobhani, N.; Sirico, M.; Generali, D.; Zanconati, F.; Scaggiante, B. Circulating cell-free nucleic acids as prognostic and therapy predictive tools for metastatic castrate-resistant prostate cancer. World J. Clin. Oncol. 2020, 11, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Zeng, Q.; Wang, Z.; Li, C.; Xu, Y.; Cui, P.; Zhu, X.; Lu, H.; Wang, G.; Cai, S.; et al. Circulating cell-free DNA for cancer early detection. Innov. 2022, 3, 100259. [Google Scholar] [CrossRef]
- Hsieh, C.; Laguna, A.; Ikeda, I.; Maxwell, A.W.P.; Chapiro, J.; Nadolski, G.; Jiao, Z.; Bai, H.X. Using Machine Learning to Predict Response to Image-guided Therapies for Hepatocellular Carcinoma. Radiology 2023, 309, e222891. [Google Scholar] [CrossRef] [PubMed]
- Danilo Bzdok NA, Martin Krzywinski Statistics versus machine learning. Nature Methods, 15, 233–234 (2018).
- Morshid, A.; Elsayes, K.M.; Khalaf, A.M.; Elmohr, M.M.; Yu, J.; Kaseb, A.O.; Hassan, M.; Mahvash, A.; Wang, Z.; Hazle, J.D.; et al. A Machine Learning Model to Predict Hepatocellular Carcinoma Response to Transcatheter Arterial Chemoembolization. Radiol. Artif. Intell. 2019, 1, e180021. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, Z.; An, C.; Chen, H.; Li, X. Multi-Task Deep Learning Approach for Simultaneous Objective Response Prediction and Tumor Segmentation in HCC Patients with Transarterial Chemoembolization. J. Pers. Med. 2022, 12, 248. [Google Scholar] [CrossRef] [PubMed]
- Mazaheri, Y.; Thakur, S.B.; Bitencourt, A.G.; Gullo, R.L.; Hötker, A.M.; Bates, D.D.B.; Akin, O. Evaluation of cancer outcome assessment using MRI: A review of deep-learning methods. BJR|Open 2022, 4, 20210072. [Google Scholar] [CrossRef]
- Zhang, L.; Jiang, Y.; Jin, Z.; Jiang, W.; Zhang, B.; Wang, C.; Wu, L.; Chen, L.; Chen, Q.; Liu, S.; et al. Real-time automatic prediction of treatment response to transcatheter arterial chemoembolization in patients with hepatocellular carcinoma using deep learning based on digital subtraction angiography videos. Cancer Imaging 2022, 22, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ma QP, He XL, Li K et al. Dynamic Contrast-Enhanced Ultrasound Radiomics for Hepatocellular Carcinoma Recurrence Prediction After Thermal Ablation. Mol Imaging Biol, 23(4), 572-585 (2021).
- Peng, J.; Lu, F.; Huang, J.; Zhang, J.; Gong, W.; Hu, Y.; Wang, J. Development and validation of a pyradiomics signature to predict initial treatment response and prognosis during transarterial chemoembolization in hepatocellular carcinoma. Front. Oncol. 2022, 12, 853254. [Google Scholar] [CrossRef]
- Lyshchik, A.; Kono, Y.; Dietrich, C.F.; Jang, H.-J.; Kim, T.K.; Piscaglia, F.; Vezeridis, A.; Willmann, J.K.; Wilson, S.R. Contrast-enhanced ultrasound of the liver: technical and lexicon recommendations from the ACR CEUS LI-RADS working group. Abdom. Imaging 2017, 43, 861–879. [Google Scholar] [CrossRef] [PubMed]
- Artificial Intelligence and Machine Learning in Software as a Medical Device. 2024.
- Iseke, S.; Zeevi, T.; Kucukkaya, A.S.; Raju, R.; Gross, M.; Haider, S.P.; Petukhova-Greenstein, A.; Kuhn, T.N.; Lin, M.; Nowak, M.; et al. Machine Learning Models for Prediction of Posttreatment Recurrence in Early-Stage Hepatocellular Carcinoma Using Pretreatment Clinical and MRI Features: A Proof-of-Concept Study. Am. J. Roentgenol. 2023, 220, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Puijk, R.S.; Ahmed, M.; Adam, A.; Arai, Y.; Arellano, R.; de Baère, T.; Bale, R.; Bellera, C.; Binkert, C.A.; Brace, C.L.; et al. Consensus Guidelines for the Definition of Time-to-Event End Points in Image-guided Tumor Ablation: Results of the SIO and DATECAN Initiative. Radiology 2021, 301, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Li, Y. Artificial Intelligence Decision-Making Transparency and Employees’ Trust: The Parallel Multiple Mediating Effect of Effectiveness and Discomfort. Behav. Sci. 2022, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- Wang F, Casalino LP, Khullar D. Deep Learning in Medicine-Promise, Progress, and Challenges. JAMA Intern Med, 179(3), 293-294 (2019).
- Calderaro, J.; Seraphin, T.P.; Luedde, T.; Simon, T.G. Artificial intelligence for the prevention and clinical management of hepatocellular carcinoma. J. Hepatol. 2022, 76, 1348–1361. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ 2017, 357, j2099. [Google Scholar] [CrossRef]
- Johnston, S.C.; Rothwell, P.M.; Nguyen-Huynh, M.N.; Giles, M.F.; Elkins, J.S.; Bernstein, A.L.; Sidney, S. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet 2007, 369, 283–292. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef]
- Malinchoc, M.; Kamath, P.S.; Gordon, F.D.; Peine, C.J.; Rank, J.; ter Borg, P.C. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 2000, 31, 864–871. [Google Scholar] [CrossRef]
- van Gorp MJ, Steyerberg EW, Van der Graaf Y. Decision guidelines for prophylactic replacement of Björk-Shiley convexo-concave heart valves: impact on clinical practice. Circulation, 109(17), 2092-2096 (2004).
- Damen, J.A.A.G.; Hooft, L.; Schuit, E.; A Debray, T.P.; Collins, G.S.; Tzoulaki, I.; Lassale, C.M.; Siontis, G.C.M.; Chiocchia, V.; Roberts, C.; et al. Prediction models for cardiovascular disease risk in the general population: systematic review. BMJ 2016, 353, i2416. [Google Scholar] [CrossRef] [PubMed]
- Bouwmeester, W.; Zuithoff, N.P.A.; Mallett, S.; Geerlings, M.I.; Vergouwe, Y.; Steyerberg, E.W.; Altman, D.G.; Moons, K.G.M. Reporting and Methods in Clinical Prediction Research: A Systematic Review. PLOS Med. 2012, 9, e1001221–12. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; A de Groot, J.; Dutton, S.; Omar, O.; Shanyinde, M.; Tajar, A.; Voysey, M.; Wharton, R.; Yu, L.-M.; Moons, K.G.; et al. External validation of multivariable prediction models: a systematic review of methodological conduct and reporting. BMC Med Res. Methodol. 2014, 14, 40–40. [Google Scholar] [CrossRef] [PubMed]
- Gary S Collins KGMM. Reporting of artificial intelligence prediction models. Lancet, 393(10181), 1577-1579 (2019).
- Gary S Collins JBR, Douglas G Altman & Karel GM Moons Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD Statement. BMC Medicine, 13 (2015).
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [PubMed]
- Ratner, M. FDA backs clinician-free AI imaging diagnostic tools. Nat. Biotechnol. 2018, 36, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Dhiman, P.; Navarro, C.L.A.; Ma, J.; Hooft, L.; Reitsma, J.B.; Logullo, P.; Beam, A.L.; Peng, L.; Van Calster, B.; et al. Protocol for development of a reporting guideline (TRIPOD-AI) and risk of bias tool (PROBAST-AI) for diagnostic and prognostic prediction model studies based on artificial intelligence. BMJ Open 2021, 11, e048008. [Google Scholar] [CrossRef] [PubMed]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Li, T.; Li, Y.; Zhu, X.; He, Y.; Wu, Y.; Ying, T.; Xie, Z. Artificial intelligence in cancer immunotherapy: Applications in neoantigen recognition, antibody design and immunotherapy response prediction. Semin. Cancer Biol. 2023, 91, 50–69. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



