
Submitted:
27 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Background: Cancer therapies predispose survivors to a high symptom burden. This study utilized mobile health (mHealth) technology to assess the feasibility of collecting daily symptoms from adult survivors of childhood cancer and evaluate symptom fluctuation and associations with future health-related quality-of-life (HRQOL).
Methods: A prospective study using an mHealth platform to distribute a 20-item cancer-related symptom survey (5 consecutive days each month) and an HRQOL survey (the day after symptom survey) over 3 consecutive months to participants from the Childhood Cancer Survivor Study. PROMIS-29 Profile and Neuro-QOL assessed HRQOL. Daily symptom burden was calculated by summing the severity (mild, moderate, or severe) of 20 symptoms. Univariate linear mixed-effects models analyzed total, person-to-person, day-to-day, and month-to-month variability for the burden of 20 individual symptoms. Multivariable linear regression analyzed the association between daily symptom burden in the first month and HRQOL in the third month, adjusting covariates.
Results: Out of the 60 survivors invited, 41 participated in this study (68% enrollment rate); 83% reported their symptoms ≥3 times and 95% reported HRQOL, both in each week across 3 months. Variability of daily symptom burden differed from person-to-person (74%), day-to-day (18%), and month-to-month (8%). Higher first-month symptom burden was associated with poorer HRQOL related to anxiety (regression coefficient: 6.56; 95%CI: 4.10-9.02), depression (6.32; 95%CI: 3.18-9.47), fatigue (7.93; 95%CI: 5.11-10.80), sleep (6.07; 95%CI: 3.43-8.70), pain (5.16; 95%CI: 2.11-8.22), and cognitive function (-6.89; 95%CI: -10.00 to -3.79) in the third month.
Conclusion: Daily assessment reveals fluctuations in symptomology, and higher symptom burden was associated with poorer HRQOL in the future. Utilizing mHealth technology for daily symptom assessment improves our understanding of symptom dynamics and sources of variability.
Keywords:
Childhood Cancer Survivors
; Health-Related Quality of Life
; mHealth
; Momentary Assessment
; Symptoms
Introduction
In the modern era, >85% of children diagnosed with cancer will become five-year survivors. However, the very therapies that cure pediatric cancers also predispose survivors to a range of late effects, such as physical and psychological sequelae, chronic health conditions, subsequent neoplasms, and premature death [1,2,3,4]. In addition to these late effects, a significant proportion of survivors experience poor patient-reported outcomes (PROs), including various symptoms [5] (e.g., pain, abnormal sensation, memory problems, somatization, pulmonary symptoms, and cardiac symptoms) and impaired health-related quality-of-life (HRQOL) [6]. Over 75% of childhood cancer survivors reported experiencing multiple symptoms [5], and 50% of the survivors had moderate or high severity of symptom burden [7]. More severe symptom burden among childhood cancer survivors has been significantly associated with clinically ascertained physical and cognitive performance deficits and poorer HRQOL [7]. Importantly, previous research has reported the association between experiencing a greater symptom burden and an increased risk of mortality [8].
Symptom reporting is clinically relevant for individuals with cancer because the assessment can identify early signs of adverse events and improve patient-clinician communication for decision-making [9,10,11,12]. Conventional symptom assessments require participants to recall their symptom experiences over an extended period [i.e., seven days using the Patient Reported Outcomes Measurement Information System (PROMIS) or four weeks using the Short-Form 36 Health Survey Questionnaire (SF-36)], which yields averaged symptom information and introduces a recall bias. Moreover, symptom burden may vary over time, especially among individuals with a high disease burden. However, there is limited research exploring both within- and between-person variability in symptom experiences over time among cancer individuals. Assessing the rhythm of symptom change by considering within-person variability may indicate a signal for a change in health conditions and suggest further clinical assessment and interventions.
The application of ecological momentary assessment (EMA) allows for the real-time reporting of symptoms, HRQOL, and other PROs [13]. EMA is less subject to recall bias than retrospective surveys and recognizes the fluctuation in symptom severity [14,15,16]. With the increasing accessibility of mobile health (mHealth) technology, EMA can be rapidly conducted through handheld devices such as tablets and smartphones [17,18] For cancer survivors, leveraging mHealth technology to monitor symptoms and other PROs in real-time provides promising opportunities to detect adverse health events between clinic visits (or before the annual appointment) and to offer timely interventions [13,19,20]. Previous studies have identified barriers to using mHealth for PRO assessments or clinical interventions, such as protecting personal health information and technology challenges (i.e., unreliable Wi-Fi connection or application malfunction) [21,22,23]. Barriers to mHealth implementation may lead to poor compliance with data collection and healthcare engagement [21,24,25].
This present study evaluated the feasibility and adherence status of using an mHealth platform to collect daily symptom data and assessed the association between the fluctuation of different daily symptoms and future HRQOL over a 3-month window among adult survivors of childhood cancer. To improve adherence to daily symptom reporting, we applied technology-driven methods to communicate with participants throughout the study. Additionally, we estimated the within- and between-person variability for the severity of 20 individual symptoms relevant to the late effects of cancer therapies and tested the association of daily symptom burden with future HRQOL. Furthermore, we evaluated participants’ satisfaction with using the mHealth platform for daily symptom assessment and the potential of using mHealth-based daily symptom reports to communicate with healthcare providers for late-effect management.
Methods
Study Design
This prospective study used an internet-based, mobile-enabled platform to examine 20 symptoms relevant to the late effects of cancer therapies and HRQOL among adult survivors of childhood cancer who were enrollees of the Childhood Cancer Survivor Study (CCSS). Participants self-reported their symptoms for 5 consecutive days per week on Weeks 1, 5, and 9 over 3 consecutive months (Figure 1). At the end of each week, participants completed an HRQOL assessment. To prompt the PRO report, automatic text and e-mail reminders were sent for the daily symptom report (daily for 5 days) and weekly HRQOL assessment (once per week) during Weeks 1, 5, and 9, using a participant interface platform. The automatic communications included the links to the online surveys that participants were required to complete that day.
Data Collection
Eligible survivors included diagnosis of cancer before 18 years of age, survival >5 years after cancer diagnosis, and attained age of ≥18 years at the time of enrollment. Data collection occurred from May 2019 to October 2019. A random sample of 60 survivors meeting the criteria were invited to participate, with 20 from each of the three symptom burden groups (low, moderate, and high). Per the methods of our previous publication [26], data from 10 symptom domains, derived from 37 symptom items present in CCSS, were used to categorize eligible participants into low, moderate, and high symptom burden associated with physical and mental summary of HRQOL. Specifically, we categorized survivors as low burden if they reported symptoms in 0-1 domains [indicating normal HRQOL; 0.5 standard deviation (SD) above the norm], moderate burden if they reported symptoms in 2-5 domains (indicating moderate HRQOL impairment; 0.5-0.99 SD below the norm), and high burden if they reported symptoms in 6 or more domains (indicating high HRQOL impairment; 1 SD below the norm).
PRO Assessment
This study evaluated 20 symptoms commonly experienced by childhood cancer survivors. These symptoms were selected based on data from previous symptom epidemiology research [5,7] and an opinion survey of 15 clinicians from St. Jude Comprehensive Cancer Center who provide clinical and survivorship care for childhood cancer patients and survivors. In the daily symptom survey, if study participants reported a symptom as present in the past 24 hours, they were asked to indicate the severity (mild, moderate, or severe) of that symptom during the same time frame. The 20 individual symptoms were irritability, anxiety, depression, fatigue or feeling weak, difficulty falling or staying asleep at night, sleepy during the day, poor memory, lack of concentration, shortness of breath, chest pain during physical exercise, numbness or tingling, problem with balance, headache, bodily pain, swelling, cramps, constipation, diarrhea, lack of appetite, and poor coordination.
The outcome variables of interest were participation rate, adherence rate, variability of symptom burden over time (15 days over a three-month period), and the longitudinal association of symptom burden in the first month with HRQOL in the third month. The participation rate was defined as the number of participants who enrolled in this study compared to those who were invited to participate. The weekly adherence rate of a given week was defined as completing at least 3 daily symptom surveys and an HRQOL report in the same week. Overall adherence rate was defined as completing at least 12 of the 18 surveys (≥3 symptoms surveys and an HRQOL report in each of the 3 months) distributed throughout the entire study. To assess the longitudinal association of symptom burden with subsequent HRQOL, participants completed 6 domains from the PROMIS-29 Profile [27] and the Neuro-QOL Cognitive Function-Short Form [28]. We used the PROMIS-29 to assess PROs in anxiety, depression, fatigue, sleep disturbance, and pain interference domains, with higher scores indicating poorer HRQOL. The Neuro-QoL Cognitive Function contains a single domain of perceived cognitive functioning, with higher scores indicating higher function status. The domain scores were calculated using a T-metric with a mean of 50 and a standard deviation of 10.
Satisfaction Survey
At the end of the 3-month study, participants completed an 8-item satisfaction survey designed by this study to provide feedback on their experience of study participation. Participants reported the degree (strongly agree, agree, neither agree nor disagree, disagree, strongly disagree) to which they agreed with the following statements: (1) “It was easy for me to complete brief daily symptom evaluations (e.g., a few days in a week) over the past 3 months”; (2) “I would be willing to take part in symptom evaluations on a regular basis to help doctors understand more”; (3) “I would be willing to take part in symptom evaluations 2-3 times per day to help doctors learn the symptom changes on a daily basis”; (4) “I am interested in taking part in a clinical trial to help doctors use my symptom data for advancing treatment strategies”; (5) “In the future studies, I would be interested in receiving a report after my symptom evaluations are done”; (6) “I am interested in discussing problematic symptoms with my oncologists or primary care physicians”; (7) “I am interested in learning skills for self-managing my problematic symptoms”; and (8) “I believe that effective symptom controls may improve my quality of life.”
Covariates
Participants’ basic sociodemographic and treatment information was obtained from the CCSS database. Sociodemographic variables included attained age at time of the first survey, time since cancer diagnosis, sex, race/ethnicity, and educational attainment. Clinical variables included chemotherapy with anthracyclines, methotrexate, plant alkaloids, cyclophosphamide, bleomycin, cytarabine, and steroids; radiation to the brain, chest, or pelvis; and invasive surgery.
Statistical Analysis
Statistical analysis was limited to those meeting the overall adherence criteria, at least 12 of the 18 surveys (i.e., ≥3 daily symptoms reports and 1 HRQOL report in each of the 3 weeks). For each participant, the burden of up to 15 daily symptom reports (5 days x 3 months) was calculated using the available symptom surveys. The daily burden across 20 symptoms was defined as the sum of the severity scores (none=0, mild=1, moderate=2, severe=3) for each of the 20 symptoms reported in the same week, yielding a range from 0 to 60. The monthly burden across 20 individual symptoms was defined as the average daily burden of these symptoms over 5 days for each of the three months, yielding a range from 0 to 60. Both daily and monthly burdens were standardized with division by the standard deviation of all monthly burdens, which was 7.20.
A total variation, consisting of between-person and within-person variations, was estimated for each of the 20 symptoms using the standardized values. Within-person variability was further decomposed into month-to-month and day-to-day variation. For each symptom variable, a univariate linear mixed model was conducted by incorporating symptom surveys collected over all three months. Nested random intercepts at both the person and month levels estimated person-to-person variance and month-to-month variance components. The residual variance was interpreted as day-to-day variation. These three variances, expressed as a fraction of the total variance, provided the variability in symptom burden attributable to the person-to-person, month-to-month, and day-to-day components.
The longitudinal association of symptom burden with future HRQOL was assessed with multivariable linear regression. The exposure variable (i.e., standardized monthly symptom burden across 20 individual symptoms) was calculated from the first month’s symptom survey, and the dependent variable (i.e., each of the six HRQOL domains) was calculated from the third month’s HRQOL survey. A separate model was performed for each of the HRQOL outcomes. Covariates adjusted in the analysis included attained age at first symptom survey, sex, radiation, chemotherapy, and invasive surgery.
Results
Out of 60 survivors invited to participate, 41 (68%) enrolled in the study (Table 1). Of the 41 survivors, 34 (83%) reported their symptoms at least 3 times each week over 3 months and 39 (95%) reported their HRQOL each week over 3 months (Supplemental Table 1). Of the enrolled survivors, 66% were female; 73% were white, 59% were aged 30-39.9 years at the time of enrollment; 68% had been diagnosed 20-29 years ago prior to the study (Table 1). Cancer diagnoses included central nervous system tumor (37%), solid tumor (26%), leukemia (20%), and lymphoma (17%). Participants underwent cancer therapies including chemotherapy (61%), radiation (27%), and invasive surgery (78%).
Symptoms most reported as the highest prevalence in each month were difficulty falling/staying asleep, bodily pain, headache, and anxiety (Supplemental Figure 1). The total burden across 20 symptoms over 3 months (i.e., the mean of symptom burdens over 3 months) among participants was 6.93 (Supplemental Figure 1). The variance of total burden across 20 symptoms over 3 months was attributed to person-to-person (74%), day-to-day (18%), and month-to-month (8%) (Figure 2). Four symptoms (poor memory, bodily pain, lack of concentration, irritability, anxiety, and difficulty sleeping) were more likely to vary from person-to-person (≥50% of the total variance). The other 16 symptoms (70%) exhibited within-person variability that accounted for >50% of the total variability. Cramps, diarrhea, poor coordination, shortness of breath, constipation, and chest pain during exercise were more likely to vary day-to-day (≥50% of the total variance). Bodily pain, irritability, anxiety, difficulty sleeping, headache, and fatigue had a high total variance of symptom burden (≥0.80).
A higher burden of 20 symptoms in the first month was significantly associated with poorer HRQOL in the third month, adjusting for age at Week 1’s symptom survey, sex, and the history of chemotherapy, radiation, and invasive surgery (Figure 3). Specifically, a one standard deviation increase in the burden of 20 symptoms in the first month was associated with poorer HRQOL scores for all domains in the third month, including 7.93 (95% CI: 5.11, 10.80) in fatigue interference, 6.56 (95% CI: 4.10, 9.02) in anxiety interference, 6.32 (95% CI: 3.18, 9.47) in depression interference, 6.07 (95% CI: 3.43, 8.70) in sleep interference, 5.16 (95% CI: 2.11, 8.22) in pain interference, and -6.89 (95% CI: -10.00, -3.79) in cognitive function.
Most participants (89.7%) reported that the daily activities were easy to complete and that they would be willing to participate in symptom evaluations on a daily basis (Table 2). Additionally, participants related that they would be interested in receiving a report of their symptom evaluations (82.1%), learning skills for self-managing problematic symptoms (87.2%), and discussing problematic symptoms with their providers (76.9%).
Discussion
This study found that the burden of individual symptoms among adult survivors of childhood cancer can vary from person-to-person and from day-to-day. The use of momentary symptom data collection typically facilitates capturing the frequent fluctuation in PROs and within-person and between-person variabilities of PROs, emphasizing the importance of conducting momentary symptom assessments to collect dynamic symptom data from this population who are at risk of high disease burden and premature mortality [3,4]. This study further demonstrates the feasibility of utilizing an mHealth platform to gather complex daily symptom data and reveals a significant association between daily symptom fluctuations and future HRQOL in adult survivors of childhood cancer. Participants also demonstrated high adherence to daily study activities, and most reported that these activities were easy to complete and expressed willingness to participate in a similar study in the future. Altogether, leveraging technology-based communication and data collection enhances the ability to capture momentary PRO data in large-scale research and clinical practice.
The dynamic data collected via momentary assessments revealed that the burden of each symptom fluctuated both day-to-day and month-to-month within individual survivors, as well as between survivors. While 74% of the total variability in daily symptom burden was due to differences between individual survivors, the majority of the individual symptoms (14 out of 20) exhibited within-person variability that accounted for >50% of the total variability. This finding suggests the clinical importance of assessing specific symptoms more frequently (i.e., at least monthly), as these symptoms may change from day-to-day or from month-to-month. The conventional use of a one-time symptom assessment in clinical practice (i.e., one symptom assessment from an annual survivorship follow-up visit) would not fully capture the natural progression of these symptoms.
An important goal of survivorship care for childhood cancer survivors, many of whom face multiple chronic health conditions, is to improve or maintain optimal HRQOL. The discovery of a significant association between higher daily symptom burden in an early month and poorer HRQOL in a later month underscores the importance of collecting momentary symptom data. This approach enables precise tracking of long-term symptom fluctuations, providing deeper insights into survivors’ well-being and functional status [32]. Providers could conduct a symptom burden assessment to monitor the progression of late effects and integrate this information into the design of clinical interventions targeting late-effect management. Future studies can utilize the mHealth approach for momentary data collection to examine the determinants of symptom burden and variability [7]. Recent findings suggest that regular symptom assessments can facilitate earlier diagnosis of cancer in adults [33]. Leveraging mHealth technology for this purpose provides promising opportunities to improve risk prediction of impaired health status and deliver timely, target interventions.
Study participants reported high satisfaction with completing the daily symptom reporting and expressed a desire to learn more from their providers about managing problematic symptoms. The mHealth approach to collecting symptoms proves to be useful technology, enabling day-by-day data collection, which is more efficient and reliable than the traditional, time-consuming paper-and-pencil-based method. However, it is important to acknowledge that the use of mHealth technology has its limitations due to issues of data security, inaccessibility to technology, and completeness of the data [34,35,36]. Though this study addressed data security concerns by using a secure server and messaging system, the reliance on technology (e.g., smartphones or tablets) may inherently be biased toward individuals with access to smartphones and network services (e.g., Wi-Fi or data plans).
This feasibility study was limited to a small sample size. Therefore, we were unable to stratify the results by cancer diagnosis or treatment. Cancer diagnosis and/or treatment factors may affect compliance with study activities due to the impact of cognitive functions (i.e., brain tumors or radiation) [37,38]. Additionally, this study did not consider seasonal variability or other environmental factors that may fluctuate the symptom burden throughout the year.
This study found that adult survivors of childhood cancer were adherent to completing frequent symptom assessments. Frequent symptom assessments further acknowledged the within-person and between-person variability in the burden of individual symptoms over a 3-month period. Future studies are warranted to implement frequent symptom monitoring and apply ecological momentary assessment through the mHealth platform to assess complex, dynamic symptom burdens for childhood cancer survivors.
Author Contributions
Conceptualization: ICH; Data curation: AM, GTA, ICH; Funding acquisition: KKN, MMH, GTA, YY, ICH; Methodology: KEH, YY, ICH; Project administration: AM, ICH; Resources: KKN, MMH, GTA; Supervision: ICH; Drafting: KEH, ICH; Review and editing: all co-authors; All authors have read and agreed to the submitted version of the manuscript.
Funding
The research reported in this manuscript was supported by the U.S. National Cancer Institute under award numbers U01CA195547 (Hudson/Ness), U24CA055727 (Armstrong), R01CA258193 (Huang/Yasui), R01CA238368 (Huang/Baker), and P30CA021765 (St. Jude Comprehensive Cancer Center). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Informed Consent Statement
The study involves human participants and was reviewed and approved by the Institutional Review Board at St. Jude Children’s Research Hospital. The participants provided their written informed consent to participate in this study.
Data Availability Statement
The Childhood Cancer Survivor Study is a U.S. National Cancer Institute-funded resource (U24CA55727) to promote and facilitate research among long-term survivors of cancer diagnosed during childhood and adolescence. CCSS data are publicly available on dbGaP at https://www.ncbi.nlm.nih.gov/gap/ through its accession number phs001327.v2.p1. and on the St. Jude Survivorship Portal within the St. Jude Cloud at https://survivorship.stjude.cloud/. In addition, utilization of the CCSS data that leverages the expertise of CCSS Statistical and Survivorship research and resources will be considered on a case-by-case basis. For this utilization, a research Application of Intent followed by an Analysis Concept Proposal must be submitted for evaluation by the CCSS Publications Committee. Users interested in utilizing this resource are encouraged to visit http://ccss.stjude.org. Full analytical data sets associated with CCSS publications since January of 2023 are also available on the St. Jude Survivorship Portal at https://viz.stjude.cloud/community/cancer-survivorship-community~4/publications.
Conflicts of Interest
No conflicts of interest.
References
- Oeffinger KC, Mertens AC, Sklar CA, et al.: Chronic health conditions in adult survivors of childhood cancer. N Engl J Med 355:1572-82, 2006.
- Hudson MM, Ness KK, Gurney JG, et al.: Clinical ascertainment of health outcomes among adults treated for childhood cancer. JAMA 309:2371-2381, 2013.
- Bhakta N, Liu Q, Ness KK, et al.: The cumulative burden of surviving childhood cancer: an initial report from the St Jude Lifetime Cohort Study (SJLIFE). Lancet 390:2569-2582, 2017.
- Friedman DL, Whitton J, Leisenring W, et al.: Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst 102:1083-95, 2010.
- Huang IC, Brinkman TM, Kenzik K, et al.: Association between the prevalence of symptoms and health-related quality of life in adult survivors of childhood cancer: a report from the St Jude Lifetime Cohort study. J Clin Oncol 31:4242-51, 2013.
- Huang IC, Brinkman TM, Armstrong GT, et al.: Emotional distress impacts quality of life evaluation: a report from the Childhood Cancer Survivor Study. J Cancer Surviv 11:309-319, 2017.
- Shin H, Dudley WN, Bhakta N, et al.: Associations of Symptom Clusters and Health Outcomes in Adult Survivors of Childhood Cancer: A Report From the St Jude Lifetime Cohort Study. J Clin Oncol 41:497-507, 2023.
- Yeh JM, Nekhlyudov L, Goldie SJ, et al.: A model-based estimate of cumulative excess mortality in survivors of childhood cancer. Ann Intern Med 152:409-17, 2010.
- Xiao C, Polomano R, Bruner DW: Comparison between patient-reported and clinician-observed symptoms in oncology. Cancer Nurs 36:E1-e16, 2013.
- Basch E, Deal AM, Kris MG, et al.: Symptom Monitoring With Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. J Clin Oncol 34:557-65, 2016.
- Snyder CF, Aaronson NK, Choucair AK, et al.: Implementing patient-reported outcomes assessment in clinical practice: a review of the options and considerations. Qual Life Res 21:1305-14, 2012.
- Basch E, Deal AM, Dueck AC, et al.: Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 318:197-198, 2017.
- Shiffman S, Stone AA, Hufford MR: Ecological momentary assessment. Annu Rev Clin Psychol 4:1-32, 2008.
- Petersen C: Patient-generated health data: a pathway to enhanced long-term cancer survivorship. J Am Med Inform Assoc 23:456-61, 2016.
- Jim HSL, Hoogland AI, Brownstein NC, et al.: Innovations in research and clinical care using patient-generated health data. CA Cancer J Clin 70:182-199, 2020.
- Phillips KM, Faul LA, Small BJ, et al.: Comparing the retrospective reports of fatigue using the Fatigue Symptom Index with daily diary ratings in women receiving chemotherapy for gynecologic cancer. J Pain Symptom Manage 46:282-8, 2013.
- Mobile Fact Sheet, Pew Research Center, 2019.
- Krebs P, Duncan DT: Health App Use Among US Mobile Phone Owners: A National Survey. JMIR Mhealth Uhealth 3:e101, 2015.
- Carlson EB, Field NP, Ruzek JI, et al.: Advantages and psychometric validation of proximal intensive assessments of patient-reported outcomes collected in daily life. Qual Life Res 25:507-16, 2016.
- Schneider S, Stone AA: Ambulatory and diary methods can facilitate the measurement of patient-reported outcomes. Qual Life Res 25:497-506, 2016.
- Abelson JS, Kaufman E, Symer M, et al.: Barriers and benefits to using mobile health technology after operation: A qualitative study. Surgery 162:605-611, 2017.
- Atienza AA, Zarcadoolas C, Vaughon W, et al.: Consumer Attitudes and Perceptions on mHealth Privacy and Security: Findings From a Mixed-Methods Study. J Health Commun 20:673-679, 2015.
- Ancker J, Silver M, Miller M, et al.: Consumer experience with and attitudes toward health information technology: A nationwide survey. J Am Med Inform Assoc 20:152-6, 2013.
- Williams MT, Lewthwaite H, Fraysse F, et al.: Compliance With Mobile Ecological Momentary Assessment of Self-Reported Health-Related Behaviors and Psychological Constructs in Adults: Systematic Review and Meta-analysis. J Med Internet Res 23:e17023, 2021.
- Jones A, Remmerswaal D, Verveer I, et al.: Compliance with ecological momentary assessment protocols in substance users: a meta-analysis. Addiction 114:609-619, 2019.
- Shin H, Dudley WN, Bhakta N, et al.: Associations of Symptom Clusters and Health Outcomes in Adult Survivors of Childhood Cancer: A Report From the St Jude Lifetime Cohort Study. J Clin Oncol 41:497-507, 2023.
- Cook KF, Jensen SE, Schalet BD, et al.: PROMIS measures of pain, fatigue, negative affect, physical function, and social function demonstrated clinical validity across a range of chronic conditions. J Clin Epidemiol 73:89-102, 2016.
- Gershon RC, Lai JS, Bode R, et al.: Neuro-QOL: quality of life item banks for adults with neurological disorders: item development and calibrations based upon clinical and general population testing. Qual Life Res 21:475-86, 2012.
- StataCorp: Stata Statistical Software: Release 14.2. College Station, TX, StataCorp LLC, 2016.
- Team RC: R: A Language and Environment for Statistical Computing. Vienna, Austria, R Foundation for Statitical Computing, 2023.
- Team P: RStudio: Integrated Development Environment for R. Boston, MA, Posit Software PBC, 2023.
- Burkett VS, Cleeland CS: Symptom burden in cancer survivorship. J Cancer Survi 1:167-175, 2007.
- Koo MM, Swann R, McPhail S, et al.: Presenting symptoms of cancer and stage at diagnosis: evidence from a cross-sectional, population-based study. Lancet Oncol 21:73-79, 2020.
- Collaborative Ne: Patient-generated health data technical expert panel: Final report, 2013.
- Chung AE, Basch EM: Potential and challenges of patient-generated health data for high-quality cancer care. J Oncol Pract 11:195-7, 2015.
- Weissmann J, Mueller A, Messinger D, et al.: Improving the Quality of Outpatient Diabetes Care Using an Information Management System: Results From the Observational VISION Study. J Diabetes Sci Technol 10:76-84, 2015.
- Hutchinson AD, Pfeiffer SM, Wilson C: Cancer-related cognitive impairment in children. Curr Opin Support Palliat Care 11:70-75, 2017.
- Docking KM, Knijnik SR: Prospective longitudinal decline in cognitive-communication skills following treatment for childhood brain tumor. Brain Inj 35:1472-1479, 2021.
Figure 1.
Study Design and Timeline. S = Symptom Assessment; Q = Health-Related Quality-of-Life Assessment.
Figure 1.
Study Design and Timeline. S = Symptom Assessment; Q = Health-Related Quality-of-Life Assessment.

Figure 2.
Variability of Daily Symptom Burden Across 3 Months Among 41 Survivors.
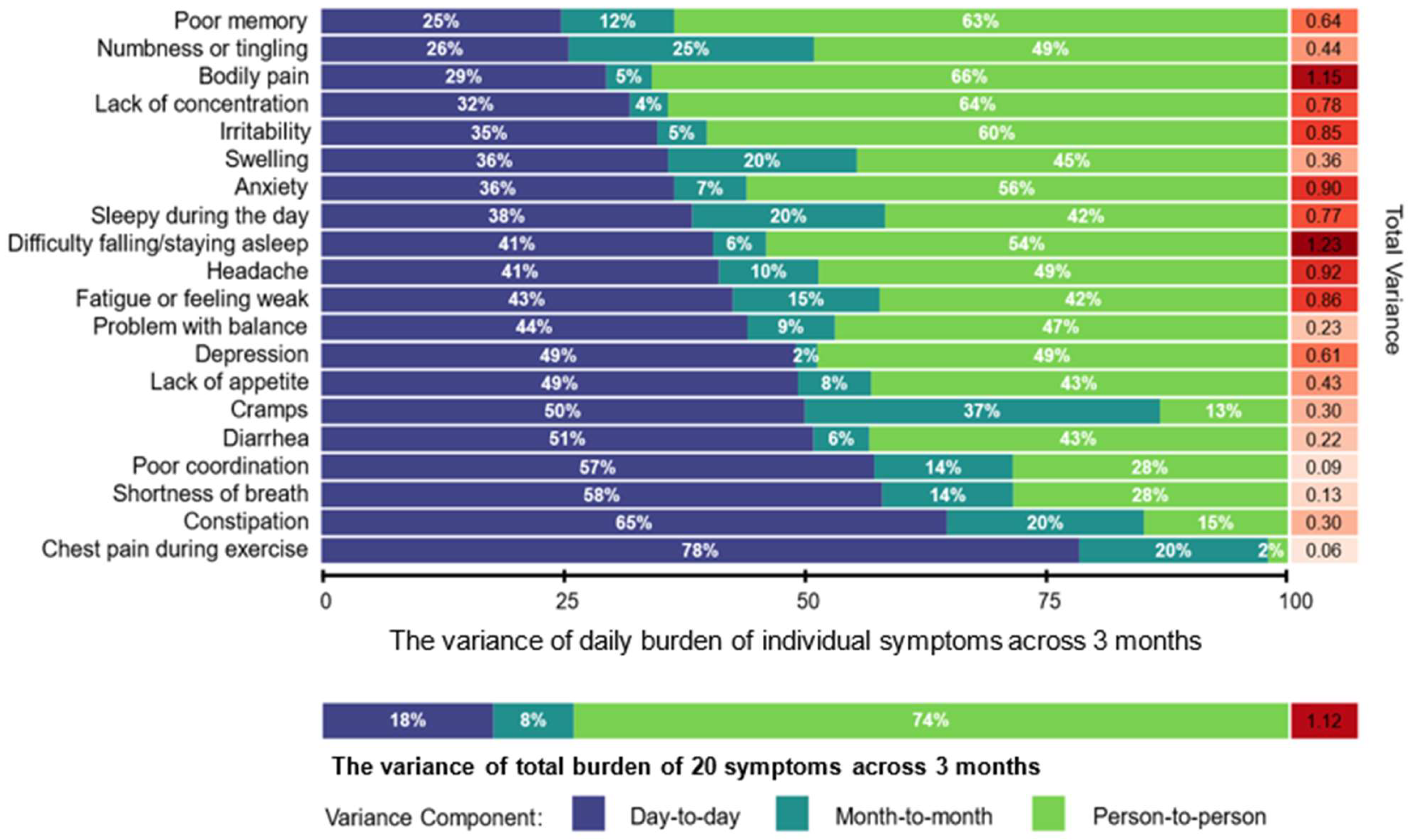
Figure 3.
Multivariable regression coefficient for the burden of 20 symptoms in the first month Associated with HRQOL in the third month. 1) The coefficients depict the degree to which the HRQOL T-score changed by one standard deviation increase in monthly symptom burden; 2) HRQOL was measured using the PROMIS-29 Profile and the Neuro-QOL; 3) Higher scores indicate worse HRQOL for all domains in the PROMIS-29 Profile, and better cognitive function in the Neuro-QOL; 4) Models are adjusted for attained age at symptom survey in Week 1 of Month 1, sex, chemotherapy, radiation, and invasive surgery.
Figure 3.
Multivariable regression coefficient for the burden of 20 symptoms in the first month Associated with HRQOL in the third month. 1) The coefficients depict the degree to which the HRQOL T-score changed by one standard deviation increase in monthly symptom burden; 2) HRQOL was measured using the PROMIS-29 Profile and the Neuro-QOL; 3) Higher scores indicate worse HRQOL for all domains in the PROMIS-29 Profile, and better cognitive function in the Neuro-QOL; 4) Models are adjusted for attained age at symptom survey in Week 1 of Month 1, sex, chemotherapy, radiation, and invasive surgery.
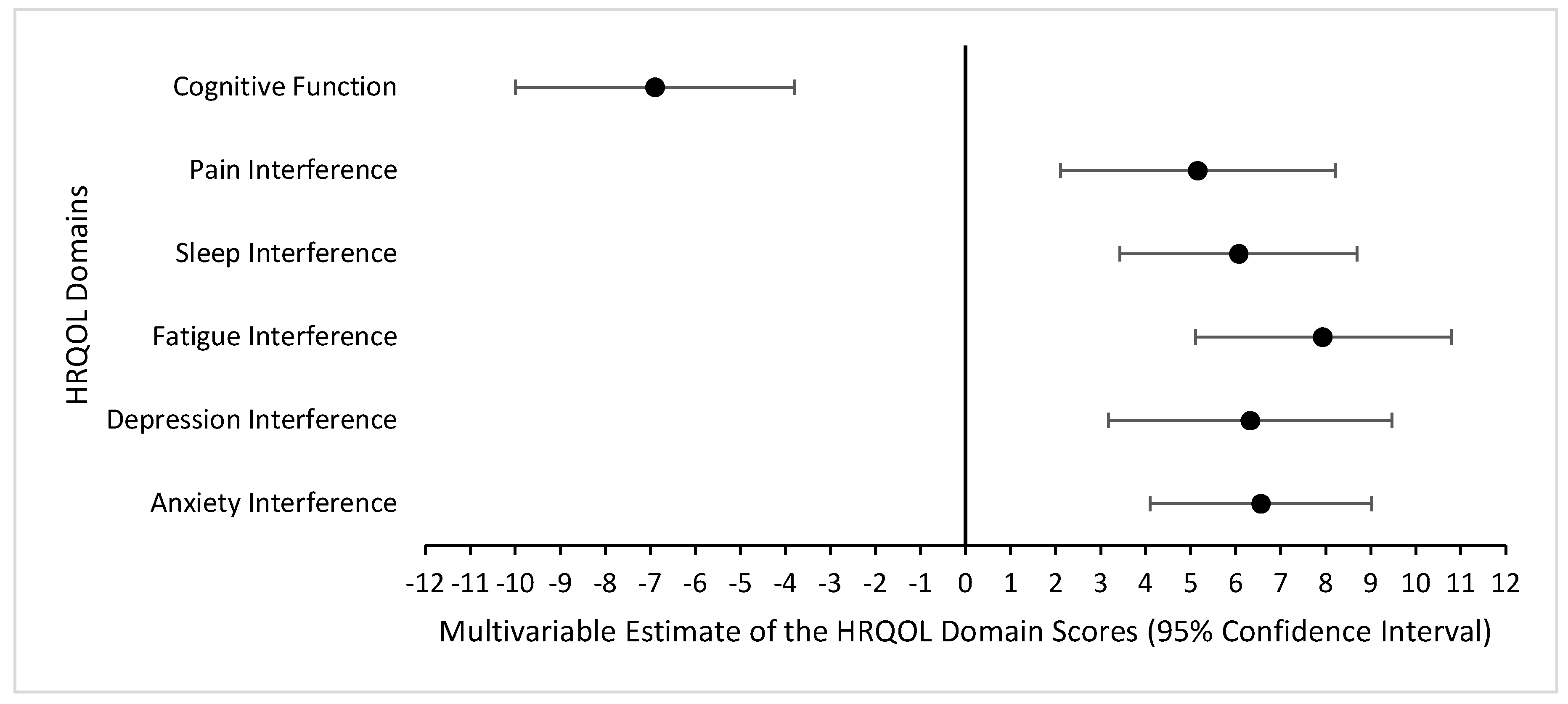

Table 1.
Demographic and Treatment Characteristics of Study Participants (N=41).
| Characteristics | N (%) or Mean (SD; min, max) |
|---|---|
| Age at study enrollment (in years) | 34.0 (5.3; 25.7, 47.1) |
| Age at study enrollment (%) | |
| 18–29.9 years | 10 (24) |
| 30–39.9 years | 24 (59) |
| ≥ 40 years | 7 (17) |
| Time since cancer diagnosis (in years) | 26.1 (3.7; 19.5, 32.4) |
| Time since cancer diagnosis (%) | |
| 10–19 years | 3 (7) |
| 20–29 years | 28 (68) |
| ≥ 30 years | 10 (24) |
| Sex (%) | |
| Male | 14 (34) |
| Female | 27 (66) |
| Race/Ethnicity (%) | |
| White non-Hispanic | 30 (73) |
| Black non-Hispanic | 11 (27) |
| Educational Attainment | |
| High school/GED or less | 6 (15) |
| Some college or post-high school training | 21 (51) |
| College graduate or post-graduate level | 14 (34) |
| Cancer diagnosis (%) | |
| Central nervous system tumor | 15 (37) |
| Acute lymphoblastic leukemia | 8 (20) |
| Wilms tumor | 5 (12) |
| Non-Hodgkin lymphoma | 5 (12) |
| Hodgkin lymphoma | 2 (5) |
| Neuroblastoma | 2 (5) |
| Rhabdomyosarcoma | 2 (5) |
| Osteosarcoma | 1 (2) |
| Ewing sarcoma | 1 (2) |
| Cancer Treatment | |
| Chemotherapy (%) | 25 (61) |
| Radiation (%) | 11 (27) |
| Invasive surgery (%) | 32 (78) |
| PROMIS-29 Profile reported in Month 3 | |
| Anxiety Interference | 56.3 (9.6; 40.3, 73.4) |
| Depression Interference | 55.7 (10.4; 41.0, 79.3) |
| Fatigue Interference | 54.5 (11.8; 33.7, 75.8) |
| Sleep Interference | 56.0 (9.5; 36.9, 73.3) |
| Pain Interference | 54.0 (10.9; 41.6, 75.6) |
| Neuro-QOL reported in Month 3 | |
| Cognitive Function | 47.1 (11.2; 22.8, 64.2) |
Table 2.
Satisfaction with Daily Symptom Assessment and Future Use for Survivorship Care (N=39).
| Questions | Strongly Agree/Agree | Neutral | Strongly Disagree/Disagree |
|---|---|---|---|
| It was easy for me to complete brief daily symptom evaluations (e.g., a few days in a week) over the past 3 months | 35 (89.7%) | 2 (5.1%) | 2 (5.1%) |
| I would be willing to take part in symptom evaluations on a regular basis to help doctors understand more | 35 (89.7%) | 3 (7.7%) | 1 (2.6%) |
| I would be willing to take part in symptom evaluations 2-3 times per day to help doctors learn the symptom changes on a daily basis | 26 (66.7%) | 9 (23.1%) | 4 (10.3%) |
| I am interested in taking part in a clinical trial to help doctors use my symptom data for advancing treatment strategies | 31 (79.5%) | 8 (20.5%) | 0 (0%) |
| In future studies, I would be interested in receiving a report after my symptom evaluations are done | 32 (82.1%) | 5 (12.8%) | 2 (5.1%) |
| I am interested in discussing problematic symptoms with my oncologists or primary care physicians | 30 (76.9%) | 9 (23.1%) | 0 (0%) |
| I am interested in learning skills for self-managing my problematic symptoms | 34 (87.2%) | 5 (12.8%) | 0 (0%) |
| I believe that effective symptom control may improve my quality of life | 31 (79.5%) | 7 (17.9%) | 1 (2.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



