Submitted:
10 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
Abstract: Ovarian cancer (OC) ranks as the fifth most common cancer among women in the United States and globally, posing a significant health threat. Reactive oxygen species (ROS) have emerged as critical factors in the pathophysiology of this malignancy. ROS, characterized by their instability due to an unpaired electron, are involved in essential cellular functions and play a crucial role in the immune response under normal physiological conditions. However, an imbalance in ROS homeostasis, leading to excessive ROS production, results in oxidative stress (OS), which can cause indiscriminate damage to cellular structures and contribute to the pathogenesis of specific diseases, including OC. OC is primarily classified based on the originating cell type into epithelial, stromal, and germinal tumors, with epithelial tumors being the most prevalent. Despite advancements in medical technology, early detection of OC remains challenging, often leading to delayed treatment initiation. Current therapeutic approaches include surgical excision of tumor tissue, radiotherapy and chemotherapy. While these treatments are effective in early-stage OC, high mortality rates and frequent relapse underscore the urgent need for novel diagnostic and therapeutic strategies. This review aims to elucidate the role of ROS in OC, emphasizing the potential for developing innovative diagnostic tools and treatments that target ROS-mediated pathways. Given the critical impact of early detection and effective treatment, advancing our understanding of ROS in the context of OC could significantly enhance patient outcomes.
Keywords:
Reactive Oxygen Species
; Ovarian Cancer
; Oxidative Stress
; Ovarian Cancer Treatment.
1. Introduction
OC is a group of neoplasms that develop in the ovaries, classified by the type of cell differentiation [1]. OC ranks as the eighth most common cancer type [2] and is the fifth leading cause of cancer-related deaths among women, with a survival rate of only 30% [3]. Currently, detection methods often identify OC at a late stage [4], resulting in poor treatment outcomes due to drug resistance, metastasis, angiogenesis, and a high recurrence rate [5,6]. The standard treatment involves surgical removal of the tumor, chemotherapy, and targeted therapies such as anti-VEGF (Vascular endothelial growth factor) and PARP (Poly ADP-ribose polymerase) inhibitors [7]. Early detection significantly improves survival rates, with a 92% survival rate when OC is caught early compared to just 29% for advanced stages. However, early-stage OC typically presents no visible symptoms or signs [8], leading to 70% of cases being diagnosed at stage III or IV [9].
Detection of OC primarily involves ultrasound and the measurement of biomarkers such as cancer antigen-125 (CA-125), human epididymis protein 4 (HE4), and carbohydrate antigen 19-9 (CA19-9) [10]. However, these methods are not effective for early-stage OC detection, contributing to high cancer mortality rates. To address this, improvements may include investigating early-stage symptoms [11], surgical removal of compromised tissues, better understanding of molecular pathogenesis, and studying new biomarkers for earlier detection [12]. Additionally, the recurrence rate of OC in late-stage patients exceeds 50% within two years, highlighting the urgent need for new early-detection approaches [13]. Current diagnostic standards involve collecting samples for histopathology, transvaginal ultrasonography, and measuring CA-125 and HE4 antigens in serum to stage malignancy risk [14,15]. For more accurate diagnosis, biopsy samples are also important. Treatment primarily includes surgical intervention, radiotherapy, chemotherapy, and targeted therapy [16].
Reactive oxygen species (ROS) play a crucial role in regulating ovarian cycles and are involved in numerous signaling pathways, such as WNT/β-catenin, Keap1/Nrf2/ARE (Kelch-like ECH-Associating protein 1/Nuclear factor erythroid 2 related factor 2/Antioxidant response element), Notch, and PI3K/AKT/mTOR (Phosphoinositide 3-kinase/Protein kinase B/Mammalian target of rapamycin). These pathways are vital for the physiological functions of the ovary. However, an imbalance between ROS and antioxidants can lead to the development of OC. Excessive ROS accumulation creates OS, causing multiple disruptions in cell division. Additionally, ROS buildup in the tumor microenvironment (TME) fosters an immunosuppressive environment, contributing to OC development and progression by affecting immune cells [17]. This raises important questions about the role of ROS in OC and underscores the need for further investigation into its significance.
2. OC: Etiology, Epidemiology, Risk factors, Characteristics, and Prognosis
Globally, OC affects approximately 225,000 women each year, leading to an average of 152,000 deaths. In the United States, around 22,500 women are diagnosed with OC annually, resulting in a mortality rate of about 62%. In Great Britain, approximately 7,000 women are diagnosed with OC each year, with a mortality rate close to 60%. The average age of diagnosis for OC patients is 58 years, with an incidence rate ranging from 1 to 10 per 100,000 women [18]. Despite advancements in medical science, OC mortality rates have not significantly declined over the past decades, with an overall survival rate of 45.6% [19]. OC is typically diagnosed at advanced stages, contributing to its high mortality rate due to the absence of specific OC-related symptoms. Common symptoms include abdominal pain, bloating or distension, back pain, irregular periods, frequent urination, weight loss, fatigue, early satiety, and pain during intercourse [20].
OC can be classified into three major types: epithelial, germ cell, and sex-cord-stromal. Within these, there are nine subtypes, including mixed epithelial and mesenchymal, miscellaneous, soft tissue, monodermal teratoma and somatic-type tumors arising in dermoid cysts, mesothelial, tumor-like lesions, secondary tumors, and lymphoid/myeloid tumors ([1231, A) [21]. The epithelial type is the most common and, based on tumorigenic pathways, the World Health Organization has divided it into two categories: type I and type II. Type I epithelial OC is typically diagnosed at an early stage and includes low-grade, well-differentiated tumors such as low-grade serous carcinoma, low-grade epithelial carcinoma, mucinous carcinoma, and clear-cell carcinoma. In contrast, type II epithelial OC is usually diagnosed at a late stage and is characterized by rapid and aggressive progression. This type includes high-grade serous tumors, carcinosarcoma, and undifferentiated carcinoma [22]. Ovarian epithelial tumors can also be classified based on tumor cell morphology (Figure1, B), into serous, endometrioid, clear cell, Brenner, mucinous, and seromucinous tumors. Serous tumors, which account for approximately 70% of epithelial tumors, share similarities with the neoplastic epithelial cells of the fallopian tube. Endometrioid tumors, making up 10-20%, resemble endometrial cells, while mucinous tumors, constituting up to 3%, resemble endocervical cells. Clear-cell tumors account for about 10% of epithelial tumors [22]. Serous carcinomas are further divided into high-grade and low-grade subtypes. Specific genetic mutations, including those in the PIK3CA (Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha), PTEN (Phosphatase and tensin homolog), and BRCA1/BRCA2 (Breast cancer gene 1/2) genes, have been found to lead to the formation of different types of serous tumors [23].
In high-grade serous carcinomas, the predominant mutations occur in the TP53 (tumor protein 53) gene (Figure 1, D). Conversely, low-grade carcinomas show a higher frequency of mutations in KRAS (Kirsten ras oncogene) and BRAF (B-Raf proto-oncogene, serine/threonine kinase), which activate MAPK (Mitogen activated kinase-like protein) pathway, resulting in cyclin D1 overexpression. Low-grade carcinomas also exhibit elevated levels of p21/WAF1 (Wild-type p53-activated fragment 1) and express cell growth suppressors such as B cell translocation gene 2 and GADD34 (Growth arrest and deoxyribonucleic acid (DNA) damage-inducible protein) [24]. Interestingly, KRAS and BRAF mutations have also been detected in high-grade serous carcinomas. Both types of OC evade immune responses through increased expression of human leukocyte antigen-G [25]. Mutations in genes responsible for DNA repair also elevate OC risk; mutations in BRIP1 (BRCA1 interacting helicase 1) increase risk by 5.8%, RAD51C (RAD51 homolog C) by 5.2%, and RAD51D (RAD51 paralog D) by 12% [26].
One of the most significant risk factors for OC is a family history of the disease, particularly among first-degree relatives. Having a relative diagnosed with OC increases the chance of developing the disease by 36%, especially if the diagnosis occurred at age 50 or older [27]. The presence of a BRCA1 mutation elevates the risk of OC to as high as 50%, while a BRCA2 mutation increases it to 10-20% [28]. Additionally, specific loci such as CHEK2 (Checkpoint kinase 2), WNT4 (Wnt family member 4), TERT (Telomerase reverse transcriptase), ABO (Alpha 1-3-N-acetylgalactosaminyltransferase and alpha 1-3-galactosyltransferase), and regions like 3q25, 17q12, 17q21, and 19p13.11 are associated with increased cancer risk, as are mutations in the BRIP1 and RAD51 genes [29]. Dysfunction of the p53 gene, a tumor suppressor, also heightens cancer risk [30]. Interestingly, pregnancies reduce OC risk, even among BRCA1 mutation carriers, with each childbirth lowering the risk by 10-20%. Age and menopausal onset are crucial risk factors [31]. Being overweight increases OC risk by 5 to 30% due to lower globulin levels and higher estradiol levels. Conversely, breastfeeding, which inhibits ovulation, reduces OC risk by 20-25%. The use of oral contraceptives lowers OC risk by 30% in both women with BRCA1/BRCA2 mutations and the general population, with protection persisting for up to 5 years after cessation, potentially preventing about 30,000 new cases [32]. Menopausal hormone therapy can reduce OC risk by 40%, but discontinuation increases risk by 20% after 5 years. Tubal ligation decreases risk by 20-30% [33]. Other conditions such as endometriosis have been shown to increase the risk of OC by 2.5 times. Pelvic inflammatory diseases elevate OC risk by 30-50%, and women with diabetes face a 17% increased risk of developing OC. Certain medications like insulin and sulfonylureas are associated with higher OC risk, whereas metformin has been linked to reduced risk. Additionally, the use of acetylsalicylic acid, an anti-inflammatory and analgesic drug, lowers OC risk by 20%. Lifestyle factors such as smoking and alcohol consumption are subtype-specific risk factors, while diet, including consumption of eggs and lactose, may also impact OC risk [34]. The prognosis for women diagnosed with OC heavily depends on the disease stage at diagnosis. Survival rates are significantly higher when OC is detected early, before metastasis occurs. Therefore, it is crucial to raise awareness about OC symptoms and encourage timely medical consultation.
3. ROS: General Definition, Balance and Levels of ROS, and Positive Role of ROS
Introduction to ROS
The history of free radicals traces back over a century, but significant advancements began after World War II, when scientists delved into the effects of radiation on the human body. It was in 1954, following Barry Commoner's groundbreaking work, that the presence of free radicals in living organisms was first conclusively demonstrated. Since then, our understanding of free radicals has evolved far beyond basic concepts. These highly reactive molecules or atoms typically possess at least one unpaired electron in their outer electron layer, leading to their remarkable reactivity and unstable nature. Today, we recognize their crucial roles in various physiological processes, influencing both health and disease states [35].
Free radicals typically arise from cellular metabolic processes when electrons with unpaired spins in the outer energy shell engage in reactions, forming partially reduced and highly reactive particles [36]. These radicals are categorized based on which atom carries the unpaired electron in the outer electron layer, such as oxygen, nitrogen, chlorine, and others. ROS are derivatives known for their ability to oxidize organic substrates [37]. The composition of ROS remains debated, but four species are most commonly recognized: superoxide (O2•–), singlet oxygen (1O2), hydroxyl radical (HO•) and hydrogen peroxide (H2O2), of which hydrogen peroxide is the least reactive [38]. ROS can exist in radical and non-radical forms; non-radical forms include hydrogen peroxide and singlet oxygen, while radical forms include hydroxyl radical and superoxide [38], [39]. Singlet oxygen can be produced during free radical reactions and can contribute to the generation of new free radicals, while hydrogen peroxide can be converted to hydroxyl radicals through interactions with specific metals [39,40].
The Balance of ROS and Antioxidants
Intracellular metabolic processes inevitably generate a significant amount of ROS, which play a crucial role in mediating intracellular and intercellular signaling within the human body [41]. Despite their essential functions, excessive ROS production can lead to OS, where ROS accumulate within cells, potentially damaging various cellular structures and increasing the risk of mutations [42]. Currently, OS is classified in at least two ways based on its intensity and level, although consensus on a unified classification remains elusive [43]. To counteract OS, the body relies on an antioxidant defense system [44]. This system involves the production of antioxidants that help reduce ROS levels and restore balance between antioxidants and ROS. Antioxidants can be synthesized by the body itself or obtained externally through consumption of foods rich in these compounds [45].
Antioxidants are classified into enzymatic and non-enzymatic groups based on their nature and mode of action, with enzymatic antioxidants playing a critical role in maintaining ROS homeostasis within cells [45]. Non-enzymatic antioxidants include zinc, taurine, vitamin C, glutathione, selenium, β-carotene, and vitamin E, which react with ROS and convert them into less harmful compounds for the body [46]. Among these, glutathione is particularly significant; its reduced form (GSH), and oxidized form, glutathione disulfide (GSSG), can serve as markers of OS based on their ratio within cells [46]. Glutathione not only directly neutralizes ROS and supports antioxidant enzymes but also regenerates vitamins C and E to their active forms [47]. Enzymatic antioxidants encompass superoxide dismutase (SOD), glutathione peroxidase, glutathione reductase (GR), and catalase (CAT) (Figure 2) [48]. CAT, primarily located in peroxisomes in mammals, is crucial for converting hydrogen peroxide into water and oxygen, thus regulating ROS balance effectively [49]. SOD exists in various forms throughout the body; copper-zinc SOD (Cu/ZnSOD) is found in the cytoplasm, manganese SOD (MnSOD) in both the cytoplasm and mitochondria, while an extracellular form also exists [49,50].
Representation of ROS and Enzymatic and Non-Enzymatic Antioxidants Balance in Healthy Cells
SOD functions primarily by catalyzing the dismutation of superoxide anions, converting them into less reactive hydrogen peroxide, which is subsequently broken down into water and oxygen with the assistance of other enzymes [50]. Glutathione peroxidase exists in two forms: selenium-dependent (GPx) and selenium-independent (GST), located within the cell in both the cytosol and mitochondrial matrix. This enzyme primarily reduces ROS by converting peroxides into water, utilizing glutathione in the process, which is converted from its reduced form GSH to its oxidized form GSSG [51]. GR is a key enzyme in the ascorbate-glutathione cycle, crucial for maintaining ROS balance. It facilitates the conversion of oxidized GSSG back to reduced glutathione using NADPH (nicotinamide adenine dinucleotide phosphate) as an electron donor [52].
Beneficial Role of ROS in Physiological Processes of the Healthy Ovary
Initially, ROS were thought to be exclusively harmful agents, associated with cellular damage due to their high levels. However, it has since been discovered that their role is more nuanced, and under certain conditions, they can benefit the organism [53]. ROS serve as crucial effector and signaling molecules in essential biological processes at the cellular level. They regulate cell growth, apoptosis, proliferation, and various signaling pathways, including those involved in inflammatory responses and responses to growth factors. At the organismal level, ROS play a key role in immune function [53,54]. Their immune function includes limiting specific immune responses, regulating inflammation, and directly targeting bacteria and fungi for destruction [54].
In the ovary, ROS play a crucial role in regulating the ovarian cycle, which includes processes such as meiosis and ovulation, as well as influencing the corpus luteum and related hormone production. During meiosis, the interplay between ROS and antioxidants directly impacts the entire process: during meiosis I, the balance shifts towards ROS, while during meiosis II, antioxidants become predominant [55]. Ovulation, akin to an inflammatory process, involves the production of ROS similar to inflammatory cells like neutrophils and macrophages [56]. Prior to ovulation, luteinizing hormone induces an environment with heightened ROS levels, triggering processes that facilitate ovulation (Figure 3) [56]. Following ovulation, the corpus luteum forms in the ovary, producing progesterone. In the event of fertilization, progesterone supports pregnancy; without fertilization, the corpus luteum regresses, reducing progesterone levels in preparation for the next ovulation cycle. Maintaining a balance between ROS and SOD is critical in regulating progesterone levels. SOD aids in neutralizing ROS, thereby sustaining the corpus luteum and ensuring adequate progesterone levels (Figure 3) [57]. Conversely, when regression of the corpus luteum and reduction in progesterone levels are required, SOD activity decreases and ROS levels increase, leading to corpus luteum regression (Figure 3) [58]. This regression involves a gradual decline in function followed by complete disappearance from the ovary [59].
4. Generation of ROS and the Role of OS in OC Pathogenesis, and the Clinical Impact of ROS
OS is a condition where the balance between reactive metabolites, the antioxidant defense system, and free radicals is disrupted. This imbalance leads to damage of molecules, thereby impairing tissue or organismal functions [60]. An imbalance in the levels of ROS and reactive nitrogen species (RNS) can disrupt normal bodily functions. Excessive amounts of these components can overwhelm antioxidant defenses, resulting in oxidative damage to lipids, proteins, nucleic acids, and other cellular structures [61,62]. ROS are primarily generated in mitochondria during cellular respiration (endogenous sources) or through the damage of cellular macromolecules (exogenous sources) (Figure4). Environmental factors such as heavy metals, pollutants, ionizing radiation, UV light, and chemotherapeutics can also lead to the formation of ROS, thereby altering cellular functions [63,64].
ROS are involved in regulating the ovarian cycle and participate in key signaling pathways in the ovary. The ROS/antioxidant balance significantly influences the development of OC. When ROS production exceeds the capacity of the antioxidant defense system, it can lead to the development of OC and other serious diseases by affecting cell proliferation signaling pathways and apoptotic genes. Moreover, ROS act as signaling molecules, directly affecting the activation of pro-oncogenic pathways and metastasis development. Cancer cells tend to produce increased amounts of ROS through NADPH oxidase (NOX) proteins and mitochondria [65]. Chronic inflammation in cells leads to the production of ROS and RNS, activating immune cells and causing dysregulation, which can result in the formation of preneoplastic cells. When ROS and RNS levels surpass the antioxidant response, irreversible reactions occur, leading to protein carbonylation, lipid peroxidation (malondialdehyde), and nucleic acid damage (8-hydroxy-2'-deoxyguanosine or 8-OHdG). These changes can cause genetic and epigenetic alterations, contributing to carcinogenesis by dysregulating oncogenes and tumor suppressor genes [66,67]. Epigenetic changes encompass modifications in histones, DNA methylation, chromatin remodeling, and the expression of miRNA (micro ribonucleic acid) [67]. miRNA represents a small class of endogenous non-coding RNA molecules, typically 18-25 nucleotides in length. It regulates gene expression at the post-transcriptional level by recognizing target sequences based on complementary 3' UTR (untranslated) regions, leading to the inhibition of the translation process and miRNA degradation [68]. miRNAs are located within cancer-related genomic regions and can function as tumor promoters or suppressors at different stages of cancer initiation. Altered miRNA expression is considered a hallmark of cancer and is associated with cancer development, progression, and metastasis [69].
OS contributes to the development of OC by causing dysregulation of genes, signaling pathways, and the TME. When ROS levels exceed the body's antioxidant defense, OS occurs, resulting in damage and altered function of biomolecules along with abnormal cellular events [63]. The high rate of aerobic glycolysis (Warburg effect) in cancer cells is proportional to OS and ROS generation [70]. Alterations in genetic and metabolic processes, along with changes in the TME, cause persistent generation of high levels of ROS in cancer cells [71]. The TME is often characterized by hypoxia, OS, and excess ROS molecules [72]. Altered signaling pathways, such as integrin activation during metastasis, can also lead to higher ROS generation [73]. These mechanisms contribute to significant increases in ROS levels in cancer cells, thereby implicating them in cancer initiation, progression, and metastasis [74]. ROS-mediated metastasis is driven by anoikis resistance, which uncouples attachment and programmed cell death in cancer cells [75].
Research indicates that ROS trigger the activation of ERK1/2 (extracellular signal-regulated kinase 1/2), MAPK, PI3K, and AKT signaling pathways, all of which play significant roles in cell division. They also increase the level of gene mutations, such as TP53, PTEN/PIK3CA, and BRCA1/BRCA2, which can trigger the development of cancer [76]. The increase in ROS is associated with NADPH-oxidase activity, mitochondrial activity, and NADPH-oxidase NOX4. Additionally, NOX, TGF-β1 (transforming growth factor-beta), and NF-κB (Nuclear factor kappa-light-chain-enhancer of activated B cells) activation have also been linked to increased ROS levels [77]. ROS and RNS alter genetic and molecular mechanisms to promote rapid and aggressive tumor division and growth, reducing the chance of cure [78,79]; however, a crucial aim for tumors is to find a way to regulate ROS to both promote accelerated proliferation and avoid inducing apoptosis or ferroptosis [80,81]. ROS leads to DNA damage, contributing to carcinogenesis, while the regulation of gene expression influences redox balance and activates transcription factors in cancer cells [82]. Overall, OS promotes the production of ROS by inducing genetic changes, such as damage to mitochondrial and nuclear DNA, altering miRNA expression, activating transcription factors, influencing signaling pathways, and affecting the TME. Additionally, OS leads to modifications in signaling pathways, including Notch, Wnt/β-catenin, Keap1-Nrf2-ARE, and PI3K/AKT/mTOR [82].
When the balance between the production and utilization of ROS is disturbed in cancer cells, large amounts of ROS accumulate, negatively affecting cellular metabolism and potentially disrupting cellular structures. Despite this, cancer cells do not die on their own, as they have developed the ability to affect antioxidant functions and counteract OS over time. Moreover, increased OS is associated with chemoresistance. It has been proposed that chemotherapy induces point mutations in redox enzymes, leading to a pro-oxidant state in cancer cells [83] .
5. OS and Signaling Pathways
OS is characterized by the excessive generation of ROS and/or a reduction in antioxidant defenses during cellular metabolism. OS has been found to play a role in the pathophysiology of many human malignancies. ROS-mediated cellular pathways promote cell survival, oncogenesis, metastasis, and render cancer cells resistant to treatment (Figure 5) [84].
5.1. Keap1-Nrf2-ARE Signaling Pathway
The Keap1-Nrf2-ARE pathway plays a crucial role in regulating cellular metabolism and redox balance [85]. This pathway consists of three components: Keap1, Nrf2, and ARE. Nrf2 activation is associated with various human malignancies, including breast, prostate, and OC. Abnormalities in the Keap1-Nrf2-ARE pathway can result in genomic instability, drug resistance, metastasis, resistance to apoptosis, and alterations in metabolic functions [86,87]. Under normal conditions, Keap1 inhibits Nrf2 by binding to it and promoting cullin3-mediated ubiquitination and proteasomal degradation. However, during OS, ROS oxidizes Keap1 cysteine residues, preventing Nrf2 degradation and leading to its activation. The activated Nrf2 then forms a heterodimer with Maf proteins in the nucleus and binds to AREs located within the promoter regions of target genes [88]. Keap1 and Nrf2 act as sensors for ROS-induced damage through the constant shuttling of Keap1 between the nucleus and the cytoplasm under physiological conditions [89]. Any alterations in this pathway can lead to OS, mitochondrial dysfunction, and inflammation [90]. Moreover, hyperactivation of the Keap1-Nrf2-ARE pathway supports the growth and survival of both normal and cancer cells by shielding them from OS, radiation, and chemotherapeutics, thereby contributing to oncogenesis and making it an attractive target for cancer therapy [91,92,93]. In epithelial OC cells, ROS-activated miRNAs, such as miR-200a and miR-141, lead to OS and Nrf2 signaling activation, ultimately promoting ovarian tumorigenesis [94].
5.2. PI3K/AKT/mTOR Signaling Pathway
The PI3K/AKT/mTOR signaling pathway is the most frequently altered pathway in human malignancies, playing a central role in regulating cellular activities and cancer development processes. These include cell survival, cell cycle progression, drug resistance, apoptosis regulation, protein synthesis, hormone and growth factor response, angiogenesis, and genomic instability [95,96,97,98,99]. Ovarian tumors often carry abnormalities in the PIK3CA gene, which encodes the catalytic subunit of class I PI3K, and the PIK3R1 gene, which encodes the regulatory subunit of class I PI3K [100,101]. ROS activates this pathway by inhibiting protein tyrosine phosphatases (PTPs) and PTEN activity in OC [102,103,104] mediated activation of the PI3K/AKT/mTOR signaling pathway results in the upregulation of VEGF and promotes de novo fatty acid and cholesterol biosynthesis, thereby facilitating OC growth and metastasis . In a transgenic mouse model, the combination of the PIK3CA H1047R mutation and PTEN deletion resulted in the development of granulosa cell tumors and ovarian serous adenocarcinoma [105].
5.3. Wnt/β-Catenin Signaling Pathway
There are three well-defined Wnt signaling pathways, the canonical Wnt/β-catenin pathway, the non-canonical planar cell polarity pathway, and the non-canonical Wnt–Ca2+ pathway. The canonical Wnt/β-catenin pathway is β-catenin dependent and the non-canonical pathway is β-catenin independent [106]. Accumulating evidence shows that hyperactivation of the Wnt/β-catenin pathway is associated with key aspects of cancer development in various cancer types like proliferation, chemoresistance, metastasis, immune suppression, and angiogenesis [107,108,109,110]. Though recent studies show that genetic alterations in this pathway are uncommon, mainly in serous type, the signaling components still play a major role in molecular events that lead to ovarian oncogenesis [111]. Epithelial OC harbor gene aberrations in β-catenin gene, CTNNB1 accounting for 54% cases [112,113,114]. Previous study shows that NOX1-derived ROS by inactivating nucleoredoxin (redox-sensitive protein that negatively controls the Wnt/β-catenin pathway) stimulates this pathway thereby promoting cancer progression [115]. Tankyrase, a tumorigenic regulator, activates the Wnt/β-catenin/Snail pathway and favors aerobic glycolysis in OC [116].
5.4. Notch Signaling Pathway
Notch receptors are transmembrane proteins comprising an extracellular portion rich in epidermal growth factor like repeats, a transmembrane domain, and a large intracellular domain containing a regulation of amino acid metabolism 23 site [117]. Notch signaling is involved in the activation of nitric oxide-soluble guanylate cyclase pathway resulting in the OC cell growth and survival. A study conducted by Jung et al. reported high miRNA levels of Notch3, Jag1 and Jag2 and high Notch3 and Jag2 protein levels in serous OC samples when compared to benign controls [118]. According to previous findings, there were high Notch1 intracellular domain (NICD1) levels in OVCAR3, SKOV3 and CaOV3 cell lines. Western blot confirmed NICD1 expression in 76% of primary human serous OC samples [119]. Retrovirus-mediated overexpression of the Notch3 intracellular domain (NICD3) in ovarian surface epithelium and low-grade serous OC cells with low endogenous Notch3 levels resulted in upregulation of the Nanog and Oct4 genes, implying main role of the Notch pathway in cancer stemness [120]. NICD3 was also overexpressed in OVCA429 serous OC cells inducing epithelial-to-mesenchymal transition (EMT) process and was confirmed by high levels of mesenchymal markers and low levels of epithelial markers. Compared to OVCA429 control cells, NICD3 overexpressed cells showed resistance to carboplatin-induced apoptosis [121]. An investigation revealed upregulation of 23 genes in ovarian tumor endothelial cells compared to benign ovarian endothelial cells, among which Jag1 was responsible for tube formation and migration of endothelial cells [122]. Altogether, these studies evidence the role of Notch pathway in EMT, invasion, metastasis, stemness, endothelial cell function and angiogenesis in serous ovarian tumors.
6. Diagnostic Methods
Detecting OC early is crucial for reducing mortality rates associated with the disease, as it is often diagnosed at advanced stages. Improving the specificity and sensitivity of detection methods could introduce novel approaches for diagnosing OC at stages where treatment outcomes are more favorable. Detecting OC early is crucial for reducing mortality rates associated with the disease, as it is often diagnosed at advanced stages. Improving the specificity and sensitivity of detection methods could introduce novel approaches for diagnosing OC at stages where treatment outcomes are more favorable [123]. The National Comprehensive Cancer Network in the USA and the National Institute for Health and Care Excellence in the UK recommend testing for individuals experiencing symptoms such as abdominal pain, bloating, unexplained weight loss, loss of appetite or early satiety after eating small meals, changes in bowel habits, or increased urinary frequency. These symptoms warrant prompt evaluation to facilitate early detection and intervention [124].
While ultrasonography is a recommended method for detecting OC, testing serum levels of CA125 and other biomarkers (Figure 6) is considered more reliable. This approach aims to facilitate early surgical removal of tumors [125]. CA125, a heavily glycosylated membrane-spanning mucin (MUC16) glycoprotein of approximately 5 MDa, is released into the pericellular space and blood when the extracellular domain of MUC16 is cleaved near the surface of OC cells. Elevated CA125 levels are typically found in patients with OC stages III-IV [126]; however, CA125 can also be elevated in cases of menstruation, ovarian cysts, or endometriosis, indicating its presence in benign conditions and as a physiological precursor to ovulation [127].
Moreover, only half of women with stage I OC exhibit elevated CA125 levels, making it unreliable for evaluating benign diseases. In contrast, ultrasonography can detect both malignant and benign lesions using the "malignant" (m) and "benign" (b) rule, achieving sensitivities of 95% and specificities of 91%, respectively [128]. The risk of OC algorithm (ROCA) utilizes CA125 marker levels for OC screening, categorizing patients into three risk groups. Depending on ROCA results, women may be recommended for annual screening using ultrasonography, repeat CA125 testing in three months, or repeat CA125 testing combined with transvaginal ultrasonography in six weeks. While ROCA-screening has demonstrated higher rates of early-stage OC detection, it has not significantly reduced mortality rates [129]. Transvaginal sonography can perform image analysis, but it may not adequately detect small pre- or invasive lesions. Additionally, this method primarily images the adnexa, and it cannot visualize the fallopian tubes [130].
Another imaging method involves the use of microbubble contrast, which has demonstrated promising results in distinguishing malignant from benign lesions. In contrast, hyperpolarized 13C MRI (Hyperpolarized carbon-13 magnetic resonance imaging), magnetic relaxometry, and superconducting quantum interference detection have shown distinctive characteristics in various other cancer types and may potentially be employed for detecting OC [130,131,132].
Human epididymal protein 4 (HE4) is another biomarker utilized for detecting OC, characterized as a 124-amino-acid glycosylated whey protein. Elevated levels of HE4 in serum are observed in 65-75% of OC patients [133]. In contrast, cancer antigen 15.3 (CA15.3) and cancer antigen 72.4 (CA72.4) represent distinct epitopes on the MUC1 mucin. However, only 18% of patients who are negative for CA125 detection can be diagnosed using HE4, CA15.3, and CA72.4 [134]. Other biomarkers include OVA1 (Ovarian malignancy algorithm) and mesothelin. OVA1 assesses the levels of Beta2-microglobulin, CA125, transthyretin (pre-albumin), ApoA1 (Apolipoprotein A1), and transferrin in serum to evaluate the risk of OC. This algorithm considers biomarker levels along with the menopausal status of patients. Mesothelin is a protein associated with OC cells' adherence, survival, and disease progression. Increased levels of mesothelin indicate the presence of OC, and it has been observed in 40%-67% of patients [135].
Another potential option is the detection of TP53 alterations, as TP53 mutations are prevalent in OC, particularly in 96% of high-grade serous carcinomas. Testing for TP53 autoantibody levels has demonstrated significant advantages over CA125 testing, with clinical implications suggesting reduced detection times [136]. Additionally, autoantibodies targeting interleukin-8 (IL-8), EpCAM (Epithelial cell adhesion molecule), PLAT (Tissue type plasminogen activator), c-Myc (Cellular myelocytomatosis oncogene), MDM2 (Mouse double minute 2 homolog) , and HOXA7 (Homeobox A7) have shown sensitivities ranging from 9% to 67% at specificities between 98% and 100% for detecting OC across all stages [123].
Proximal tumor fluids can serve as screening tools, as somatic mutations in TP53 have been isolated from uterine lavage and even menstrual blood in women with OC. The PapSEEK test, an experimental liquid biopsy test, is utilized for early detection of endometrial and OC based on DNA alterations caused by these diseases. The PapSEEK test exhibits a sensitivity of 33% and a specificity of 99% for detecting OC [137].
miRNAs play strong regulatory roles in various cellular processes and any alteration in their expression results in various cancer types, especially chemotherapy resistant OC. So, there is a need to identify novel targets like OC-associated miRNAs for early diagnosis and treatment [138]. Often the miRNA levels differ in healthy persons and patients with OC, and as such their levels are not increased in benign OC patients [139]. Likewise, the expression profile of miR-200A, miR-200B, and miR-200C are significantly greater in healthy tissues and expression profiles of miR-199A, miR-140, miR-145, and miR-125B1 are lower in OC [140]. miR-10a and miR-10b considerably suppressed the proliferation of ovarian granulosa cells [141]. Various types of RNA including miR-182 and miR-200 family members (mainly miR-200a, miR-200b, and miR-200c) are overexpressed in high-grade serous epithelial OC [142,143]. miR-183 is highly expressed in OC and its downregulation induced apoptosis thereby inhibiting growth and progression of OVCAR-3 and SKOV-3 cell lines [144]. miR-151 activates AKT/mTOR pathway and results in tumorigenesis and progression of OC [145]. Overexpressed miR-10b in OC activates Ras homolog family member C and matrix metallopeptidase 14 that are responsible for metastasis [146]. It was shown that miRNA can be detected in body fluids of OC patients, highlighting the significance of miRNA as a biomarker [147].
To conclude, all currently used detection methods are not reliable due to risk of false-negative results and there are no markers that can be used as stand-alone screening tests. Even two-stage methods that are used do not have a reliable sensitivity, despite an adequate specificity. OC early detection is a key factor for reduction in mortality and provides a field of future studies and investigations. Early detection still remains an elusive goal, and the significance of both cost-effective and efficient methods to diagnose OC is a key.
7. Treatment Options for OC and the Role of Oxidative Stress in Chemotherapy Resistance
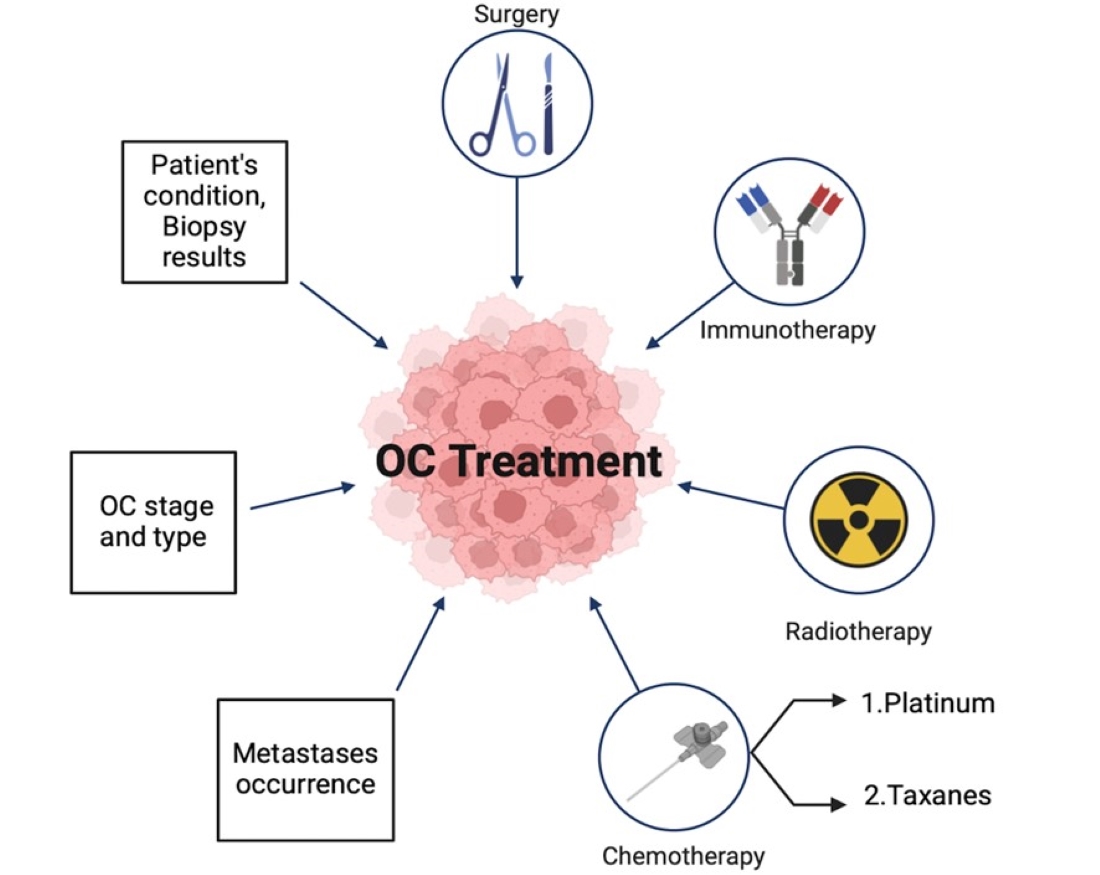
Currently, the standard treatment for OC includes chemotherapy, radiotherapy, and surgical intervention (Figure7). Combination therapy involving these approaches may be tailored based on factors such as the patient's condition, treatment sensitivity, disease stage, and other variables [148]. Before initiating treatment, several considerations must be taken into account, including the type of cancer, location and presence of metastases, and biopsy results. Primary surgical cytoreduction is the primary treatment for newly diagnosed OC. The main objective of surgery is complete resection of disseminated carcinomatosis and en bloc removal of any affected organs such as the bowel, uterus, or adnexal masses, ensuring that tumors are surgically removed intact without breaching their capsules [149]. Furthermore, pelvic and para-aortic lymph node dissection is essential for patients at both early and late stages of OC, as lymph node metastases can complicate treatment and increase risks. In some instances, additional procedures such as colonoscopy and/or upper endoscopy may be necessary to rule out the possibility of primary gastrointestinal cancer [150].
Surgical intervention for OC primarily aims at debulking, which involves removing the ovaries, fallopian tubes, and, in some cases, a partial or complete hysterectomy, along with the omentum and other affected tissues. If the disease has spread to other organs, additional resections may be necessary, including the spleen, bowel, peritoneum, and diaphragm [151]. Whole-abdomen radiotherapy, developed in the 1960s, uses high doses of radiation to induce antitumor effects by causing DNA lysis in tumor cells. Radiotherapy can be applied after surgery at lower doses in combination with other treatments to minimize the toxic effects of each method while enhancing the overall therapeutic effect [152].
Adjuvant chemotherapy is another treatment approach used for OC. Whether to use adjuvant chemotherapy or not depends on a biopsy confirming pathological changes in ovarian, tubal, or peritoneal cancer, as well as on the grade and stage of the cancer. For stage I OC, surgical removal often leads to a cure. However, patients receiving chemotherapy are typically treated with carboplatin in combination with paclitaxel, or carboplatin alone, or with neoadjuvant chemotherapy alone [28]. There are two main types of chemotherapeutic drugs used for OC treatment: platinum-based drugs, including carboplatin and cisplatin, and taxanes, such as paclitaxel and docetaxel. Carboplatin, a platinum-based drug, is less toxic and has fewer adverse effects. Patients with OC often show significant sensitivity to carboplatin, which can increase survival rates. The drug can be administered intravenously or through heated intraperitoneal chemotherapy [153].
Nevertheless, chemotherapy has significant limitations due to the development of chemotherapy resistance. Research has shown that the inactivation of tumor-suppressor genes such as PTEN, RB1 (retinoblastoma transcriptional corepressor 1), RAD51B, and NF1 (neurofibromin 1) contributes to this resistance [154]. Additionally, changes at the molecular level within cells, often induced by OS, further complicate treatment. High-dose chemotherapeutic agents also cause significant side effects, presenting another major challenge in the effective management of OC [155].
Recurrence of OC is a significant issue, as it is incurable in most cases. Approximately 80% of patients with advanced-stage OC experience recurrence, and only a small percentage can achieve a cure upon recurrence. Therefore, monitoring CA125 levels, evaluating symptoms, and performing radiographic imaging every 2 to 4 months after treatment completion are essential [156]. OC cells possess certain genes that inhibit apoptosis, allowing cancer cells to survive and proliferate. Apoptosis inhibition occurs through two main pathways: the intrinsic pathway (regulated by Bcl-2 family proteins) and the extrinsic pathway (regulated by tyrosine-protein kinases). Both intrinsic and extrinsic apoptotic inhibitors contribute to chemotherapy resistance [157].
The Bcl-2 protein family, which includes Bcl-X and Mcl-1, is not only overexpressed in OC but also contributes to decreased survival due to chemotherapy resistance. Clinical trials for Bcl-2 inhibitors have shown improved survival rates and a high response to cisplatin treatment [158]. Another well-studied inhibitor is survivin, which targets apoptotic proteins. The use of drugs that suppress survivin results in tumor regression and enhanced sensitivity to chemotherapy [159]. Tyrosine-protein kinase Met (c-Met) levels are elevated in patients with OC, promoting angiogenesis, anti-apoptotic activity, and cancer cell proliferation. Studies have shown that radiotherapy can induce c-Met expression, leading to better treatment responses and higher survival rates by reducing apoptosis and cancer cell proliferation [160].
OC cells commonly develop resistance to chemotherapeutic treatments like paclitaxel, cisplatin, vincristine, and doxorubicin due to P-glycoprotein (Pgp), which is often overexpressed in OC patients [161]. Pgp functions by actively transporting drugs out of the cell against their concentration gradient, thereby reducing their cytotoxic effects. Additionally, OC cells can express MRP1 (encoded by ABCC1 or ATP binding cassette subfamily C member 1) and MRP2 (encoded by ABCC2 or ATP binding cassette subfamily C member 2) through the formation of transport proteins. The MDR-1 (multidrug resistance mutation 1) gene, which encodes the 170-kD adenosine triphosphate (ATP)-dependent glycoprotein, also known as MDR-associated proteins, which also contribute to drug resistance. These mechanisms collectively hinder the efficacy of chemotherapy in treating OC [162].
In OC, chromatin alterations and the activation of insulin-like growth factor (IGF-1) pathways contribute to increased drug resistance. Inhibiting IGF-1 and targeting cytotoxic genes represent potential strategies to enhance therapeutic efficacy and improve patient survival [163]. During OC progression, EMT occurs alongside angiogenesis. Overexpression of endothelin-1 and endothelin-A promotes this transition, transforming epithelial cells into mesenchymal cells with anti-apoptotic properties. This transition contributes to drug resistance and higher mortality rates in OC [164].
Molecularly targeted therapy and immunotherapy represent innovative approaches for treating OC. Immunotherapy aims to activate the adaptive or innate immune systems by enhancing T-cell or Natural killer (NK) cell activation, or by modulating immune responses through the inhibition of immune checkpoints, targeting regulatory T cells, or overcoming immunosuppression in the TME [165]. Targeted therapy can be classified into passive and active approaches. Passive targeted therapy involves delivering generic antibodies, lymphocytes, or other immune system components to target OC cells. Active immunotherapy stimulates the patient's immune response to produce antibodies or lymphocytes specifically targeting OC cells [166].
Immunotherapy is using multiple strategies, including viruses (T-VEC/Talimogene laherparepvec), bacterias, therapeutic vaccines (Intravenous oncolytic vaccinia virus GL-ONC1), NK, dendritic cells (DC), TIL (tumor-infiltrating lymphocytes), or T-cell transfer, monoclonal antibodies (mAbs), immunostimulatory cytokines, and antigen specific chimeric antigen receptors or CARs (CTL019/tisagenlecleucel; Axicabtagene ciloleucel). Checkpoint inhibitors that are currently in clinical trials are Ipilimumab (CTLA-4 inhibitor), Nivolumab and Pembrolizumab (programmed cell death or PD-1 inhibitors), Durvalumab, Atezolizumab, and Avelumab (Programmed death-ligand 1 or PD-L1 inhibitors), Relatlimab (Lymphocyte activation gene-1 or LAG-1 inhibitor), that target angiogenesis [167].
The success rate for therapy for OC treatment remains low and there are only certain drugs approved by the Food and Drug Administration (FDA) [168], including melphalan (Alkeran) [169], carboplatin (Paraplatin) [170,171], cyclophosphamide [172], topotecan hydrochloride (Hycamtin) [173], and cisplatin [174] which are chemotherapeutic drugs that cause tumor cell growth arrest by DNA damage [171]. Other chemotherapeutic agents include doxorubicin hydrochloride (Anthracycline) and doxorubicin hydrochloride liposomes, which cause DNA damage by targeting topoisomerase II activity [175], gemcitabine hydrochloride (Gemzar, Infugem) that targets cancer cell’s DNA and RNA formation by mimicking their block building [176]. Paclitaxel taxane chemotherapy is also approved by FDA, that inhibits tumor cells dividing by chromosomal changes [177].
Other FDA-approved drugs include bevacizumab (Avastin, Alymsys, Mvasi, Zirabev) which is VEGF-inhibitor [178,179] mirvetuximab soravtansine-gynx (Elahere) that is maytansinoid microtubule inhibitor and a folate receptor alpha (FRα)-directed antibody conjugate [180,181], niraparib tosylate monohydrate (Zejula) and olaparib (Lynparza) are PARP inhibitor by which DNA breaks are not getting repaired and tumor cells death occurs [182], and rucaparib camsylate (Rubraca) which is PARP-1, PARP-2, and PARP-3 inhibitor [183].
8. Future Perspectives for OC Treatment
Despite advancements in treating OC, the disease's mortality remains high in late stages, with limited variability in effective treatments. As a result, ongoing research is focusing on experimental methods that promise to be more targeted and efficacious compared to current therapies patients with stage III and IV OC [184]. One promising approach under investigation is Vigil, a tumor vaccine designed to target TGFβ1 and TGFβ2, which play roles in cell motility, angiogenesis, and immunity [185]. By affecting the proprotein convertase furin, Vigil aims to enhance its therapeutic effects without significant side effects, as observed in a study involving 92 patients with stage III and IV OC [186]. CAR-T immunotherapy, another innovative method, involves genetically modifying T cells with chimeric antigen receptors (CARs) to target cancer cells more effectively. Despite the potential for severe cytokine release syndrome, CAR-T therapy has shown promise in attacking OC cells [187]. DCVAC (Dendritic cell-based immunotherapy) utilizes a patient's own dendritic cells exposed to tumor-associated antigens to stimulate an immune response against cancer cells. This approach has demonstrated effectiveness in clinical trials with minimal side effects, warranting further investigation [188].
Peptide-based chemotherapy, leveraging proteins to specifically bind to cancer cell receptors and deliver chemotherapy drugs, offers advantages such as low toxicity and high specificity. However, its efficacy remains to be fully validated through ongoing research [189]. Viral treatments, utilizing oncolytic viruses like adenoviruses to induce cancer cell lysis and stimulate tumor-specific immunity, have shown potential when combined with chemotherapy. Challenges include delivery limitations due to existing immunity against adenoviruses and their inability to replicate effectively in studied models [190]. Cell metabolism targeting focuses on disrupting cancer cells' vital metabolic pathways, such as lipid and glucose metabolism. While promising, this approach carries risks of affecting immune cell function and potentially accelerating tumor growth, necessitating careful exploration in future studies [191]. Immune checkpoint inhibitors, which block immune cell checkpoints to enhance the immune system's ability to recognize and attack cancer cells, have shown effectiveness in treating some cancers [192] but remain less effective in OC compared to other malignancies like uterine endometrial cancer [193]. In conclusion, these innovative therapies represent promising avenues for improving OC treatment outcomes, addressing current limitations, and advancing towards more personalized and effective treatment strategies.
9. Conclusion
OC is a prevalent and highly lethal disease, primarily due to challenges in early diagnosis. Despite being one of the most common cancers affecting women, effective methods for early detection remain elusive, leading to limited treatment options in advanced stages. Risk factors such as genetic mutations, family history, obesity, age, and comorbidities contribute to its onset. ROS play a pivotal role in OC development by influencing cellular pathways, OS, and signaling. Maintaining a balance between ROS and antioxidants is critical, as ROS can function as vital molecules in immune response, signaling, and ovarian cycle regulation. Early diagnosis is paramount, as survival rates drastically improve when OC is detected early, contrasting starkly with late-stage diagnoses where survival rates are significantly lower. Current diagnostic methods like CA125 are limited by the disease's asymptomatic early stages. Treatment typically involves surgery, chemotherapy and radiotherapy. Despite ongoing challenges in diagnosis and treatment, research in OC remains critical due to its high mortality rate and nonspecific early symptoms.
References
- Arora, T., S. Mullangi, and M.R. Lekkala, Ovarian cancer. 2021.
- Siegel, R.L. , et al., Cancer statistics, 2023. CA: A Cancer Journal for Clinicians, 2023. 73(1): p. 17-48.
- Morand, S. , et al., Ovarian Cancer Immunotherapy and Personalized Medicine. International Journal of Molecular Sciences, 2021. 22(12): p. 6532.
- Stewart, C., C. Ralyea, and S. Lockwood. Ovarian cancer: an integrated review. in Seminars in oncology nursing. 2019. Elsevier.
- Lheureux, S. , et al., Epithelial ovarian cancer. The Lancet, 2019. 393(10177): p. 1240-1253.
- Akter, S. , et al., Recent Advances in Ovarian Cancer: Therapeutic Strategies, Potential Biomarkers, and Technological Improvements. Cells, 2022. 11(4): p. 650.
- Garg, V. and A.M. Oza, Treatment of Ovarian Cancer Beyond PARP Inhibition: Current and Future Options. Drugs, 2023. 83(15): p. 1365-1385.
- Zapardiel, I., M. Diestro, and G. Aletti, Conservative treatment of early stage ovarian cancer: oncological and fertility outcomes. European Journal of Surgical Oncology (EJSO), 2014. 40(4): p. 387-393.
- Roett, M.A. and P. Evans, Ovarian cancer: an overview. Am Fam Physician, 2009. 80(6): p. 609-16.
- Cirillo, P.D.R. , et al., Multi-analytical test based on serum miRNAs and proteins quantification for ovarian cancer early detection. PLoS One, 2021. 16(8): p. e0255804.
- Zhang, R. , et al., Molecular Biomarkers for the Early Detection of Ovarian Cancer. International Journal of Molecular Sciences, 2022. 23(19): p. 12041.
- Clarke, A., Y. M. Chang, and K. McPherson, Removing organs “just in case”—is prophylactic removal of the ovaries a good thing? 2006, BMJ Publishing Group Ltd. p. 186-187.
- Garzon, S. , et al., Secondary and tertiary ovarian cancer recurrence: what is the best management? Gland Surgery, 2020. 9(4): p. 1118-1129.
- Oranratanaphan, S. , et al., Assessment of Diagnostic Values among CA-125, RMI, HE4, and ROMA for Cancer Prediction in Women with Nonfunctional Ovarian Cysts. Obstetrics and Gynecology International, 2018. 2018: p. 7821574.
- Renjen, P.N. , et al., Paraneoplastic Cerebellar Degeneration Associated With Ovarian Adenocarcinoma: A Case Report and Review of Literature. Annals of Indian Academy of Neurology, 2018. 21(4): p. 311-314.
- National Academies of Sciences, E. , et al., Ovarian Cancers: Evolving Paradigms in Research and Care. 2016: National Academies Press.
- Zheng, M. , et al., Oxidative Stress Response Biomarkers of Ovarian Cancer Based on Single-Cell and Bulk RNA Sequencing. Oxidative Medicine and Cellular Longevity, 2023. 2023: p. 1261039.
- Jayson, G.C. , et al., Ovarian cancer. The Lancet, 2014. 384(9951): p. 1376-1388.
- Siegel, R.L. , et al., Cancer statistics, 2022. CA: A Cancer Journal for Clinicians, 2022. 72(1): p. 7-33.
- Rooth, C. , Ovarian cancer: risk factors, treatment and management. Br J Nurs, 2013. 22(17): p. S23-30.
- Zamwar, U.M. and A.P. Anjankar, Aetiology, Epidemiology, Histopathology, Classification, Detailed Evaluation, and Treatment of Ovarian Cancer. Cureus, 2022. 14(10): p. e30561.
- Kossaï, M. , et al., Ovarian Cancer: A Heterogeneous Disease. Pathobiology, 2017. 85(1-2): p. 41-49.
- Murali, R. , et al., Deregulated Metabolic Pathways in Ovarian Cancer: Cause and Consequence. Metabolites, 2023. 13(4): p. 560.
- Meinhold-Heerlein, I. , et al., Molecular and prognostic distinction between serous ovarian carcinomas of varying grade and malignant potential. Oncogene, 2005. 24(6): p. 1053-1065.
- Singer, G. , et al., Mutations in BRAF and KRAS Characterize the Development of Low-Grade Ovarian Serous Carcinoma. JNCI: Journal of the National Cancer Institute, 2003. 95(6): p. 484-486.
- Suszynska, M., M. Ratajska, and P. Kozlowski, BRIP1, RAD51C, and RAD51D mutations are associated with high susceptibility to ovarian cancer: mutation prevalence and precise risk estimates based on a pooled analysis of ~30,000 cases. J Ovarian Res, 2020. 13(1): p. 50.
- Reid, B.M., J. B. Permuth, and T.A. Sellers, Epidemiology of ovarian cancer: a review. Cancer Biology and Medicine, 2017. 14(1): p. 9-32.
- Matulonis, U.A. , et al., Ovarian cancer. Nature reviews Disease primers, 2016. 2(1): p. 1-22.
- Webb, P.M. and S.J. Jordan, Epidemiology of epithelial ovarian cancer. Best practice & research Clinical obstetrics & gynaecology, 2017. 41: p. 3-14.
- Torre, L.A. , et al., Ovarian cancer statistics, 2018. CA: A Cancer Journal for Clinicians, 2018. 68(4): p. 284-296.
- Huber, D. , et al., Use of oral contraceptives in BRCA mutation carriers and risk for ovarian and breast cancer: a systematic review. Archives of Gynecology and Obstetrics, 2020. 301(4): p. 875-884.
- Goldzieher, J.W. and F.Z. Stanczyk, Oral contraceptives and individual variability of circulating levels of ethinyl estradiol and progestins. Contraception, 2008. 78(1): p. 4-9.
- Lacey, J. , James V., et al., Menopausal Hormone Replacement Therapy and Risk of Ovarian Cancer. JAMA, 2002. 288(3): p. 334-341.
- Orchard, S.G. , et al., Association of metformin, aspirin, and cancer incidence with mortality risk in adults with diabetes. JNCI Cancer Spectr, 2023. 7(2).
- Hensley, K. and R.A. Floyd, Reactive oxygen species and protein oxidation in aging: a look back, a look ahead. Archives of biochemistry and biophysics, 2002. 397(2): p. 377-383.
- Fruehauf, J.P. and F.L. Meyskens, Jr., Reactive Oxygen Species: A Breath of Life or Death? Clinical Cancer Research, 2007. 13(3): p. 789-794.
- Ciani, F. , et al., Influence of ROS on ovarian functions. New discoveries in embryology, 2015: p. 41-73.
- Collin, F. , Chemical Basis of Reactive Oxygen Species Reactivity and Involvement in Neurodegenerative Diseases. International Journal of Molecular Sciences, 2019. 20(10): p. 2407.
- Aldred, E.M. , Pharmacology: a handbook for complementary healthcare professionals. 2008: Elsevier Health Sciences.
- Baker, M.A., J. Netherton, and R.J. Aitken, From past to present: an historical overview of the concept of spermatozoa, reactive oxygen species, and male-factor infertility, in Oxidants, antioxidants and impact of the oxidative status in male reproduction. 2019, Elsevier. p. 17-26.
- Fujii, J., Y. Iuchi, and F. Okada, Fundamental roles of reactive oxygen species and protective mechanisms in the female reproductive system. Reproductive Biology and Endocrinology, 2005. 3(1): p. 43.
- Singh, R. and P.P. Manna, Reactive oxygen species in cancer progression and its role in therapeutics. Exploration of Medicine, 2022. 3(1): p. 43-57.
- Lushchak, V.I. , Free radicals, reactive oxygen species, oxidative stress and its classification. Chemico-biological interactions, 2014. 224: p. 164-175.
- Al-Dalaen, S.M. and A.I. Al-Qtaitat, Oxidative stress versus antioxidants. American journal of Bioscience and Bioengineering, 2014. 7(1): p. 60-71.
- Patekar, D. , et al., Antioxidant defence system. Oral & Maxillofacial Pathology Journal, 2013. 4(1).
- Moussa, Z., Z. Judeh, and S.A. Ahmed, Nonenzymatic exogenous and endogenous antioxidants. Free radical medicine and biology, 2019. 1: p. 11-22.
- Owoade, A.O. and A. Olorunnisola, The supportive role of dietary antioxidants in antioxidant defence system. Advanced in Life Science and Technology, 2019. 73: p. 53-9.
- Irato, P. and G. Santovito, Enzymatic and Non-Enzymatic Molecules with Antioxidant Function. Antioxidants, 2021. 10(4): p. 579.
- Jeeva, J.S. , et al., Enzymatic antioxidants and its role in oral diseases. Journal of Pharmacy and Bioallied Sciences, 2015. 7(Suppl 2): p. S331-S333.
- Asakura, H. and T. Kitahora, Antioxidants in Inflammatory Bowel Disease, Ulcerative Colitis, and Crohn. Bioactive Food as Dietary Interventions for Liver and Gastrointestinal Disease: Bioactive Foods in Chronic Disease States, 2013: p. 37.
- Katiyar, S.K., F. Afaq, and H. Mukhtar, Effects of solar radiation on detoxification mechanisms in the skin, in Comprehensive Series in Photosciences. 2001, Elsevier. p. 419-436.
- Mir, R.A. and M.A. Khah, Recent progress in enzymatic antioxidant defense system in plants against different environmental stresses. Improving Stress Resilience in Plants, 2024: p. 203-224.
- Janků, M., L. Luhová, and M. Petřivalský, On the Origin and Fate of Reactive Oxygen Species in Plant Cell Compartments. Antioxidants, 2019. 8(4): p. 105.
- Yang, Y. , et al., Reactive oxygen species in the immune system. International reviews of immunology, 2013. 32(3): p. 249-270.
- Liang, J. , et al., Reactive oxygen species and ovarian diseases: Antioxidant strategies. Redox Biology, 2023. 62: p. 102659.
- Shkolnik, K. , et al., Reactive oxygen species are indispensable in ovulation. Proceedings of the National Academy of Sciences, 2011. 108(4): p. 1462-1467.
- SUGINO, N. , Roles of reactive oxygen species in the corpus luteum. Animal Science Journal, 2006. 77(6): p. 556-565.
- Sugino, N. , et al., Superoxide dismutase expression in the human corpus luteum during the menstrual cycle and in early pregnancy. Molecular Human Reproduction, 2000. 6(1): p. 19-25.
- Stocco, C., C. Telleria, and G. Gibori, The Molecular Control of Corpus Luteum Formation, Function, and Regression. Endocrine Reviews, 2007. 28(1): p. 117-149.
- Pizzino, G. , et al., Oxidative Stress: Harms and Benefits for Human Health. Oxidative Medicine and Cellular Longevity, 2017. 2017: p. 8416763.
- Wang, Q. , et al., Mechanistic study of TRPM2-Ca2+-CAMK2-BECN1 signaling in oxidative stress-induced autophagy inhibition. Autophagy, 2016. 12(8): p. 1340-1354.
- Berlett, B.S. and E.R. Stadtman, Protein oxidation in aging, disease, and oxidative stress. Journal of Biological Chemistry, 1997. 272(33): p. 20313-20316.
- Brieger, K. , et al., Reactive oxygen species: from health to disease. Swiss Medical Weekly, 2012. 142(3334): p. w13659.
- Sullivan, L.B. and N.S. Chandel, Mitochondrial reactive oxygen species and cancer. Cancer & metabolism, 2014. 2: p. 1-12.
- Moloney, J.N. and T.G. Cotter, ROS signalling in the biology of cancer. Semin Cell Dev Biol, 2018. 80: p. 50-64.
- Jelic, M.D. , et al., Oxidative stress and its role in cancer. J Cancer Res Ther, 2021. 17(1): p. 22-28.
- Marí-Alexandre, J. , et al., Interplay Between MicroRNAs and Oxidative Stress in Ovarian Conditions with a Focus on Ovarian Cancer and Endometriosis. International Journal of Molecular Sciences, 2019. 20(21): p. 5322.
- Bartel, D.P. , MicroRNAs: target recognition and regulatory functions. Cell, 2009. 136(2): p. 215-33.
- Hanahan, D. and R.A. Weinberg, The hallmarks of cancer. Cell, 2000. 100(1): p. 57-70.
- Hart, P.C. , et al., MnSOD upregulation sustains the Warburg effect via mitochondrial ROS and AMPK-dependent signalling in cancer. Nature communications, 2015. 6(1): p. 6053.
- Kim, J., J. Kim, and J.-S. Bae, ROS homeostasis and metabolism: a critical liaison for cancer therapy. Experimental & molecular medicine, 2016. 48(11): p. e269-e269.
- Wang, Y. , et al., The double-edged roles of ROS in cancer prevention and therapy. Theranostics, 2021. 11(10): p. 4839.
- Chiarugi, P. , et al., Reactive oxygen species as essential mediators of cell adhesion: the oxidative inhibition of a FAK tyrosine phosphatase is required for cell adhesion. The Journal of cell biology, 2003. 161(5): p. 933-944.
- Takeuchi, T., M. Nakajima, and K. Morimoto, Relationship between the intracellular reactive oxygen species and the induction of oxidative DNA damage in human neutrophil-like cells (vol 17, pg 1543, 1996). 1997, OXFORD UNIV PRESS GREAT CLARENDON ST, OXFORD, ENGLAND OX2 6DP. p. 1683-1683.
- Douma, S. , et al., Suppression of anoikis and induction of metastasis by the neurotrophic receptor TrkB. Nature, 2004. 430(7003): p. 1034-9.
- Stieg, D.C. , et al., ROS and miRNA Dysregulation in Ovarian Cancer Development, Angiogenesis and Therapeutic Resistance. International Journal of Molecular Sciences, 2022. 23(12): p. 6702.
- Xia, C. , et al., Reactive Oxygen Species Regulate Angiogenesis and Tumor Growth through Vascular Endothelial Growth Factor. Cancer Research, 2007. 67(22): p. 10823-10830.
- Caneba, C.A. , et al., Nitric oxide is a positive regulator of the Warburg effect in ovarian cancer cells. Cell Death Dis, 2014. 5(6): p. e1302.
- Galadari, S. , et al., Reactive oxygen species and cancer paradox: To promote or to suppress? Free Radic Biol Med, 2017. 104: p. 144-164.
- Dodson, M., R. Castro-Portuguez, and D.D. Zhang, NRF2 plays a critical role in mitigating lipid peroxidation and ferroptosis. Redox Biol, 2019. 23: p. 101107.
- Redza-Dutordoir, M. and D.A. Averill-Bates, Activation of apoptosis signalling pathways by reactive oxygen species. Biochim Biophys Acta, 2016. 1863(12): p. 2977-2992.
- Ding, D.N. , et al., Insights into the Role of Oxidative Stress in Ovarian Cancer. Oxid Med Cell Longev, 2021. 2021: p. 8388258.
- Sharifi-Rad, M. , et al., Lifestyle, Oxidative Stress, and Antioxidants: Back and Forth in the Pathophysiology of Chronic Diseases. Front Physiol, 2020. 11: p. 694.
- Franco, R. , et al., Oxidative stress, DNA methylation and carcinogenesis. Cancer Lett, 2008. 266(1): p. 6-11.
- Xu, M. , et al., Taurine alleviates oxidative stress in porcine mammary epithelial cells by stimulating the Nrf2-MAPK signaling pathway. Food Sci Nutr, 2023. 11(4): p. 1736-1746.
- Rojo de la Vega, M., E. Chapman, and D.D. Zhang, NRF2 and the Hallmarks of Cancer. Cancer Cell, 2018. 34(1): p. 21-43.
- Kerins, M.J. and A. Ooi, A catalogue of somatic NRF2 gain-of-function mutations in cancer. Sci Rep, 2018. 8(1): p. 12846.
- Nguyen, T., P. Nioi, and C.B. Pickett, The Nrf2-antioxidant response element signaling pathway and its activation by oxidative stress. J Biol Chem, 2009. 284(20): p. 13291-5.
- Dinkova-Kostova, A.T., W. D. Holtzclaw, and N. Wakabayashi, Keap1, the sensor for electrophiles and oxidants that regulates the phase 2 response, is a zinc metalloprotein. Biochemistry, 2005. 44(18): p. 6889-99.
- Sun, Z. , et al., KPNA6 (Importin {alpha}7)-mediated nuclear import of Keap1 represses the Nrf2-dependent antioxidant response. Mol Cell Biol, 2011. 31(9): p. 1800-11.
- Ma, Q. , Role of nrf2 in oxidative stress and toxicity. Annu Rev Pharmacol Toxicol, 2013. 53: p. 401-26.
- Klaunig, J.E., L. M. Kamendulis, and B.A. Hocevar, Oxidative stress and oxidative damage in carcinogenesis. Toxicol Pathol, 2010. 38(1): p. 96-109.
- Kumar, B. , et al., Oxidative stress is inherent in prostate cancer cells and is required for aggressive phenotype. Cancer Res, 2008. 68(6): p. 1777-85.
- Mateescu, B. , et al., miR-141 and miR-200a act on ovarian tumorigenesis by controlling oxidative stress response. Nat Med, 2011. 17(12): p. 1627-35.
- Chen, Z. , et al., MAP kinases. Chem Rev, 2001. 101(8): p. 2449-76.
- Innocenti, M. , et al., Phosphoinositide 3-kinase activates Rac by entering in a complex with Eps8, Abi1, and Sos-1. J Cell Biol, 2003. 160(1): p. 17-23.
- Pimienta, G. and J. Pascual, Canonical and alternative MAPK signaling. Cell Cycle, 2007. 6(21): p. 2628-32.
- Qiu, X. , et al., COX2 and PGE2 mediate EGF-induced E-cadherin-independent human ovarian cancer cell invasion. Endocr Relat Cancer, 2014. 21(4): p. 533-43.
- Fruman, D.A. and C. Rommel, PI3K and cancer: lessons, challenges and opportunities. Nat Rev Drug Discov, 2014. 13(2): p. 140-56.
- Levine, D.A. , et al., Frequent mutation of the PIK3CA gene in ovarian and breast cancers. Clin Cancer Res, 2005. 11(8): p. 2875-8. [CrossRef]
- Philp, A.J. , et al., The phosphatidylinositol 3'-kinase p85alpha gene is an oncogene in human ovarian and colon tumors. Cancer Res, 2001. 61(20): p. 7426-9.
- Sakamoto, K. , et al., Role of the tumor suppressor PTEN in antioxidant responsive element-mediated transcription and associated histone modifications. Mol Biol Cell, 2009. 20(6): p. 1606-17.
- van der Reest, J. , et al., Proteome-wide analysis of cysteine oxidation reveals metabolic sensitivity to redox stress. Nat Commun, 2018. 9(1): p. 1581.
- Wu, W.S. , The signaling mechanism of ROS in tumor progression. Cancer Metastasis Rev, 2006. 25(4): p. 695-705.
- Kinross, K.M. , et al., An activating Pik3ca mutation coupled with Pten loss is sufficient to initiate ovarian tumorigenesis in mice. J Clin Invest, 2012. 122(2): p. 553-7.
- Arend, R.C. , et al., The Wnt/β-catenin pathway in ovarian cancer: a review. Gynecol Oncol, 2013. 131(3): p. 772-9.
- Jung, Y.S. and J.I. Park, Wnt signaling in cancer: therapeutic targeting of Wnt signaling beyond β-catenin and the destruction complex. Exp Mol Med, 2020. 52(2): p. 183-191.
- Wiese, K.E., R. Nusse, and R. van Amerongen, Wnt signalling: conquering complexity. Development, 2018. 145(12).
- Groden, J. , et al., Identification and characterization of the familial adenomatous polyposis coli gene. Cell, 1991. 66(3): p. 589-600.
- van Schie, E.H. and R. van Amerongen, Aberrant WNT/CTNNB1 Signaling as a Therapeutic Target in Human Breast Cancer: Weighing the Evidence. Front Cell Dev Biol, 2020. 8: p. 25.
- Gatcliffe, T.A. , et al., Wnt signaling in ovarian tumorigenesis. Int J Gynecol Cancer, 2008. 18(5): p. 954-62. [CrossRef]
- Wu, R. , et al., Diverse mechanisms of beta-catenin deregulation in ovarian endometrioid adenocarcinomas. Cancer Res, 2001. 61(22): p. 8247-55.
- Nusse, R. and H. Clevers, Wnt/β-Catenin Signaling, Disease, and Emerging Therapeutic Modalities. Cell, 2017. 169(6): p. 985-999.
- Nguyen, V.H.L. , et al., Wnt/β-catenin signalling in ovarian cancer: Insights into its hyperactivation and function in tumorigenesis. J Ovarian Res, 2019. 12(1): p. 122.
- Wu, Y. , et al., Molecular mechanisms underlying chronic inflammation-associated cancers. Cancer Lett, 2014. 345(2): p. 164-73.
- Yang, H.Y. , et al., Tankyrase Promotes Aerobic Glycolysis and Proliferation of Ovarian Cancer through Activation of Wnt/β-Catenin Signaling. Biomed Res Int, 2019. 2019: p. 2686340.
- Radtke, F. and K. Raj, The role of Notch in tumorigenesis: oncogene or tumour suppressor? Nature Reviews Cancer, 2003. 3(10): p. 756-767.
- El-Sehemy, A. , et al., Notch activation augments nitric oxide/soluble guanylyl cyclase signaling in immortalized ovarian surface epithelial cells and ovarian cancer cells. Cell Signal, 2013. 25(12): p. 2780-7.
- Rose, S.L. , et al., Notch 1 signaling is active in ovarian cancer. Gynecol Oncol, 2010. 117(1): p. 130-3.
- Park, J.T. , et al., Notch3 overexpression is related to the recurrence of ovarian cancer and confers resistance to carboplatin. Am J Pathol, 2010. 177(3): p. 1087-94.
- Gupta, N. , et al., Notch3 induces epithelial-mesenchymal transition and attenuates carboplatin-induced apoptosis in ovarian cancer cells. Gynecol Oncol, 2013. 130(1): p. 200-6.
- Lu, C. , et al., Gene alterations identified by expression profiling in tumor-associated endothelial cells from invasive ovarian carcinoma. Cancer Res, 2007. 67(4): p. 1757-68.
- Elias, K.M., J. Guo, and R.C. Bast, Jr., Early Detection of Ovarian Cancer. Hematol Oncol Clin North Am, 2018. 32(6): p. 903-914.
- Sundar, S., R. D. Neal, and S. Kehoe, Diagnosis of ovarian cancer. Bmj, 2015. 351: p. h4443.
- Charkhchi, P. , et al., CA125 and Ovarian Cancer: A Comprehensive Review. Cancers (Basel), 2020. 12(12).
- Matte, I. , et al., Ascites from ovarian cancer patients stimulates MUC16 mucin expression and secretion in human peritoneal mesothelial cells through an Akt-dependent pathway. BMC Cancer, 2019. 19(1): p. 406.
- Zhang, M. , et al., Roles of CA125 in diagnosis, prediction, and oncogenesis of ovarian cancer. Biochim Biophys Acta Rev Cancer, 2021. 1875(2): p. 188503.
- Timmerman, D. , et al., Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. Bmj, 2010. 341: p. c6839.
- Skates, S.J. , Ovarian cancer screening: development of the risk of ovarian cancer algorithm (ROCA) and ROCA screening trials. Int J Gynecol Cancer, 2012. 22 Suppl 1(Suppl 1): p. S24-6.
- Folkins, A.K. , et al., A candidate precursor to pelvic serous cancer (p53 signature) and its prevalence in ovaries and fallopian tubes from women with BRCA mutations. Gynecol Oncol, 2008. 109(2): p. 168-73.
- Nelson, S.J. , et al., Metabolic imaging of patients with prostate cancer using hyperpolarized [1-13C] pyruvate. Science translational medicine, 2013. 5(198): p. 198ra108-198ra108.
- Adolphi, N.L. , et al., Imaging of Her2-targeted magnetic nanoparticles for breast cancer detection: comparison of SQUID-detected magnetic relaxometry and MRI. Contrast Media Mol Imaging, 2012. 7(3): p. 308-19.
- James, N.E., C. Chichester, and J.R. Ribeiro, Beyond the Biomarker: Understanding the Diverse Roles of Human Epididymis Protein 4 in the Pathogenesis of Epithelial Ovarian Cancer. Front Oncol, 2018. 8: p. 124.
- Yang, W.L., Z. Lu, and R.C. Bast, Jr., The role of biomarkers in the management of epithelial ovarian cancer. Expert Rev Mol Diagn, 2017. 17(6): p. 577-591.
- Chandra, A. , et al., Ovarian cancer: Current status and strategies for improving therapeutic outcomes. Cancer Med, 2019. 8(16): p. 7018-7031.
- Vang, R. , et al., Molecular Alterations of TP53 are a Defining Feature of Ovarian High-Grade Serous Carcinoma: A Rereview of Cases Lacking TP53 Mutations in The Cancer Genome Atlas Ovarian Study. Int J Gynecol Pathol, 2016. 35(1): p. 48-55.
- Cohen, J.D. , et al., Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science, 2018. 359(6378): p. 926-930.
- Xu, S. , et al., MiR-497 decreases cisplatin resistance in ovarian cancer cells by targeting mTOR/P70S6K1. Oncotarget, 2015. 6(28): p. 26457-71.
- Kan, C.W. , et al., Elevated levels of circulating microRNA-200 family members correlate with serous epithelial ovarian cancer. BMC Cancer, 2012. 12: p. 627.
- Iorio, M.V. , et al., MicroRNA signatures in human ovarian cancer. Cancer Res, 2007. 67(18): p. 8699-707.
- Jiajie, T. , et al., Conserved miR-10 family represses proliferation and induces apoptosis in ovarian granulosa cells. Sci Rep, 2017. 7: p. 41304.
- Vescarelli, E. , et al., MiR-200c sensitizes Olaparib-resistant ovarian cancer cells by targeting Neuropilin 1. J Exp Clin Cancer Res, 2020. 39(1): p. 3.
- Choi, P.W. and S.W. Ng, The Functions of MicroRNA-200 Family in Ovarian Cancer: Beyond Epithelial-Mesenchymal Transition. Int J Mol Sci, 2017. 18(6).
- Zhou, J. , et al., miR-183 modulated cell proliferation and apoptosis in ovarian cancer through the TGF-β/Smad4 signaling pathway. Int J Mol Med, 2019. 43(4): p. 1734-1746.
- Lv, Y., F. -L. Li, and P.-S. Liu, MiR-151 promotes ovarian cancer through activation of akt/mTOR signaling pathway by decreasing RhoGDIA. Int. J. Clin. Exp. Pathol, 2016. 9: p. 11222-11229.
- Nakayama, I. , et al., Loss of HOXD10 expression induced by upregulation of miR-10b accelerates the migration and invasion activities of ovarian cancer cells. Int J Oncol, 2013. 43(1): p. 63-71.
- Staicu, C.E. , et al., Role of microRNAs as Clinical Cancer Biomarkers for Ovarian Cancer: A Short Overview. Cells, 2020. 9(1).
- Orr, B. and R.P. Edwards, Diagnosis and treatment of ovarian cancer. Hematology/Oncology Clinics, 2018. 32(6): p. 943-964.
- Cummings, M., O. Nicolais, and M. Shahin, Surgery in Advanced Ovary Cancer: Primary versus Interval Cytoreduction. Diagnostics (Basel), 2022. 12(4).
- Bacalbasa, N. , et al., The Risk of Para-Aortic Lymph Node Metastases in Apparent Early Stage Ovarian Cancer. Medicina (Kaunas), 2020. 56(3).
- Kurnit, K.C., G. F. Fleming, and E. Lengyel, Updates and New Options in Advanced Epithelial Ovarian Cancer Treatment. Obstet Gynecol, 2021. 137(1): p. 108-121.
- Herrera, F.G. , et al., Rational combinations of immunotherapy with radiotherapy in ovarian cancer. Lancet Oncol, 2019. 20(8): p. e417-e433.
- Zhang, C. , et al., Platinum-based drugs for cancer therapy and anti-tumor strategies. Theranostics, 2022. 12(5): p. 2115-2132.
- Erol, A., M. Niemira, and A.J. Krętowski, Novel Approaches in Ovarian Cancer Research against Heterogeneity, Late Diagnosis, Drug Resistance, and Transcoelomic Metastases. Int J Mol Sci, 2019. 20(11).
- Chehelgerdi, M. , et al., Progressing nanotechnology to improve targeted cancer treatment: overcoming hurdles in its clinical implementation. Mol Cancer, 2023. 22(1): p. 169.
- Wang, Q. , et al., The prognostic factor for recurrence in advanced-stage high-grade serous ovarian cancer after complete clinical remission: a nested case-control study. J Ovarian Res, 2021. 14(1): p. 179.
- Qian, S. , et al., The role of BCL-2 family proteins in regulating apoptosis and cancer therapy. Front Oncol, 2022. 12: p. 985363.
- Kaloni, D. , et al., BCL-2 protein family: attractive targets for cancer therapy. Apoptosis, 2023. 28(1-2): p. 20-38.
- Mobahat, M., A. Narendran, and K. Riabowol, Survivin as a preferential target for cancer therapy. Int J Mol Sci, 2014. 15(2): p. 2494-516.
- Zhang, Y. , et al., Function of the c-Met receptor tyrosine kinase in carcinogenesis and associated therapeutic opportunities. Mol Cancer, 2018. 17(1): p. 45.
- Surowiak, P. , et al., Significance of cyclooxygenase 2 and MDR1/P-glycoprotein coexpression in ovarian cancers. Cancer Lett, 2006. 235(2): p. 272-80.
- Januchowski, R. , et al., Analysis of MDR genes expression and cross-resistance in eight drug resistant ovarian cancer cell lines. J Ovarian Res, 2016. 9(1): p. 65.
- Vella, V. , et al., Insulin/IGF Axis and the Receptor for Advanced Glycation End Products: Role in Meta-inflammation and Potential in Cancer Therapy. Endocr Rev, 2023. 44(4): p. 693-723.
- Bilyk, O. , et al., Epithelial-to-Mesenchymal Transition in the Female Reproductive Tract: From Normal Functioning to Disease Pathology. Front Oncol, 2017. 7: p. 145.
- Singh, S. , et al., Small Molecule Targeting Immune Cells: A Novel Approach for Cancer Treatment. Biomedicines, 2023. 11(10).
- Galluzzi, L. , et al., Classification of current anticancer immunotherapies. Oncotarget, 2014. 5(24): p. 12472-508.
- Macpherson, A.M. , et al., Epithelial ovarian cancer and the immune system: biology, interactions, challenges and potential advances for immunotherapy. Journal of clinical medicine, 2020. 9(9): p. 2967.
- Drugs Approved for Ovarian, Fallopian Tube, or Primary Peritoneal Cancer. 2022; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/ovarian.
- Davis-Perry, S. , et al., Melphalan for the treatment of patients with recurrent epithelial ovarian cancer. Am J Clin Oncol, 2003. 26(4): p. 429-33.
- Carboplatin. 2023; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/carboplatin.
- Collins, I.M. , et al., Carboplatin dosing in ovarian cancer: problems and pitfalls. Int J Gynecol Cancer, 2011. 21(7): p. 1213-8.
- Handolias, D. , et al., Oral cyclophosphamide in recurrent ovarian cancer. Asia Pac J Clin Oncol, 2016. 12(1): p. e154-60.
- Lihua, P., X. Y. Chen, and T.X. Wu, Topotecan for ovarian cancer. Cochrane Database Syst Rev, 2008. 2008(2): p. Cd005589.
- Song, M., M. Cui, and K. Liu, Therapeutic strategies to overcome cisplatin resistance in ovarian cancer. Eur J Med Chem, 2022. 232: p. 114205.
- Doxorubicin Hydrochloride. 2023; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/doxorubicinhydrochloride.
- Gemcitabine Hydrochloride. 2023; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/gemcitabinehydrochloride.
- Weaver, B.A. , How Taxol/paclitaxel kills cancer cells. Mol Biol Cell, 2014. 25(18): p. 2677-81.
- Nakai, H. and N. Matsumura, The roles and limitations of bevacizumab in the treatment of ovarian cancer. Int J Clin Oncol, 2022. 27(7): p. 1120-1126.
- Bevacizumab. 2023; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/bevacizumab.
- Mirvetuximab Soravtansine-gynx. 2024; Available from: https://www.cancer.gov/about-cancer/treatment/drugs/mirvetuximab-soravtansine-gynx.
- Dilawari, A. , et al., FDA Approval Summary: Mirvetuximab Soravtansine-Gynx for FRα-Positive, Platinum-Resistant Ovarian Cancer. Clin Cancer Res, 2023. 29(19): p. 3835-3840.
- Moore, K. , et al., Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N Engl J Med, 2018. 379(26): p. 2495-2505.
- Dockery, L.E., C. C. Gunderson, and K.N. Moore, Rucaparib: the past, present, and future of a newly approved PARP inhibitor for ovarian cancer. Onco Targets Ther, 2017. 10: p. 3029-3037.
- Schmid, B.C. and M.K. Oehler, New perspectives in ovarian cancer treatment. Maturitas, 2014. 77(2): p. 128-36.
- Gogineni, V. , et al., Current Ovarian Cancer Maintenance Strategies and Promising New Developments. J Cancer, 2021. 12(1): p. 38-53.
- Rocconi, R.P. , et al., Maintenance vigil immunotherapy in newly diagnosed advanced ovarian cancer: Efficacy assessment of homologous recombination proficient (HRP) patients in the phase IIb VITAL trial. Journal of Clinical Oncology, 2021. 39(15_suppl): p. 5502-5502.
- Wang, X. , et al., A transgene-encoded cell surface polypeptide for selection, in vivo tracking, and ablation of engineered cells. Blood, 2011. 118(5): p. 1255-63.
- Rob, L. , et al., Safety and efficacy of dendritic cell-based immunotherapy DCVAC/OvCa added to first-line chemotherapy (carboplatin plus paclitaxel) for epithelial ovarian cancer: a phase 2, open-label, multicenter, randomized trial. J Immunother Cancer, 2022. 10(1).
- Xiao, Y.F. , et al., Peptide-Based Treatment: A Promising Cancer Therapy. J Immunol Res, 2015. 2015: p. 761820.
- Hoare, J., N. Campbell, and E. Carapuça, Oncolytic virus immunotherapies in ovarian cancer: moving beyond adenoviruses. Porto Biomed J, 2018. 3(1): p. e7.
- Pal, S. , et al., Targeting cancer-specific metabolic pathways for developing novel cancer therapeutics. Front Immunol, 2022. 13: p. 955476.
- Basudan, A.M. , The Role of Immune Checkpoint Inhibitors in Cancer Therapy. Clin Pract, 2022. 13(1): p. 22-40.
- Pirš, B. , et al., Overview of Immune Checkpoint Inhibitors in Gynecological Cancer Treatment. Cancers (Basel), 2022. 14(3).
Figure 1.
The major types of OC. The figure represents (A) 12 types of OC, (B) 6 main types of epithelial tumors based on the cell morphology of the tumor, which are the most common types of OC, and 2 types of the serous type of epithelial tumors, which are (C) high-grade, and (D) low-grade.
Figure 1.
The major types of OC. The figure represents (A) 12 types of OC, (B) 6 main types of epithelial tumors based on the cell morphology of the tumor, which are the most common types of OC, and 2 types of the serous type of epithelial tumors, which are (C) high-grade, and (D) low-grade.
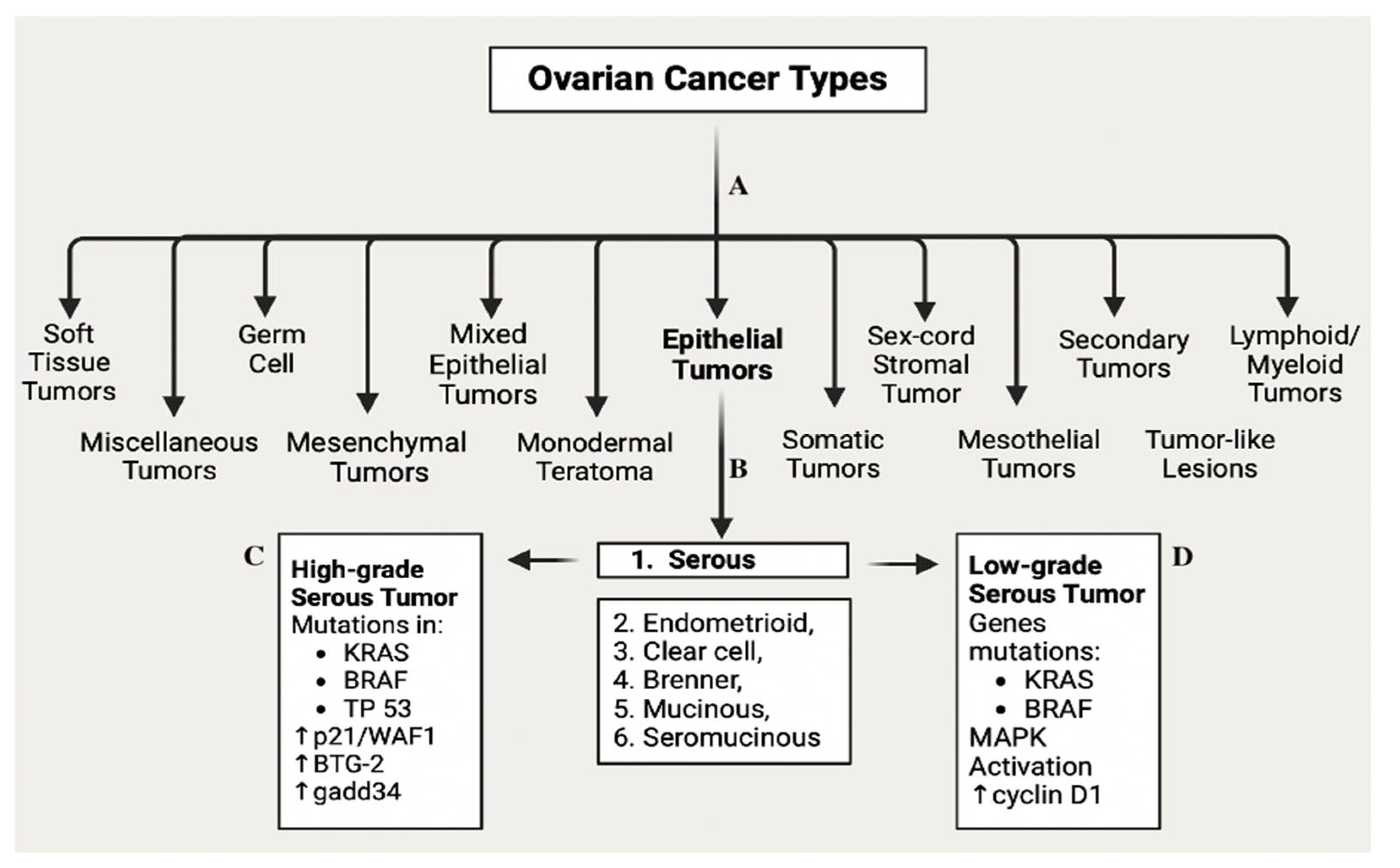
Figure 2.
Representation of enzymatic and non-enzymatic antioxidants and balance between ROS and antioxidants.
Figure 2.
Representation of enzymatic and non-enzymatic antioxidants and balance between ROS and antioxidants.
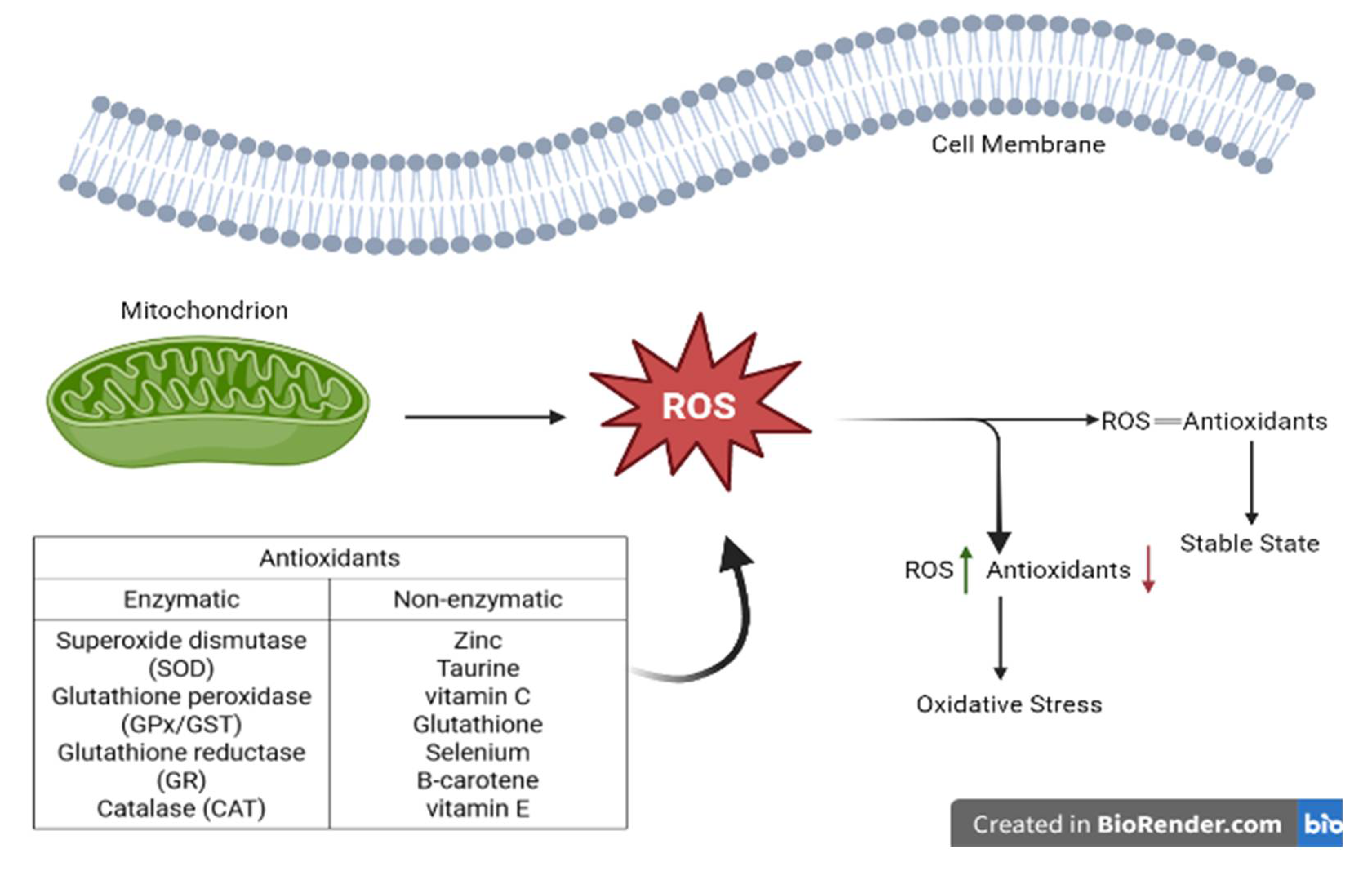
Figure 3.
Ovulation cycle (a) ovary without a corpus luteum, (b) ovary with a corpus luteum.
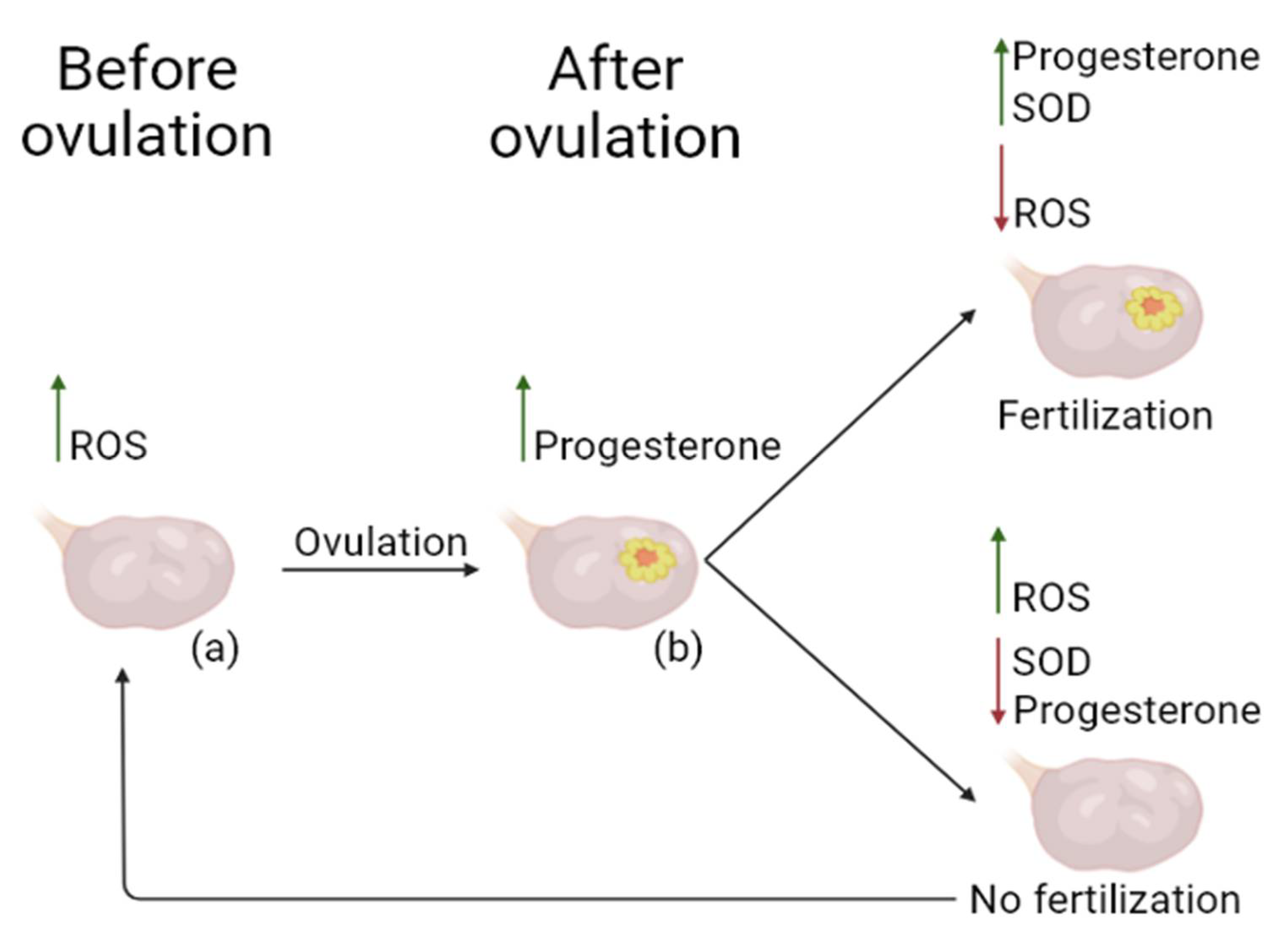
Figure 4.
Sources of ROS generation leading to OS that ultimately contributes to several pathological conditions in OC.
Figure 4.
Sources of ROS generation leading to OS that ultimately contributes to several pathological conditions in OC.
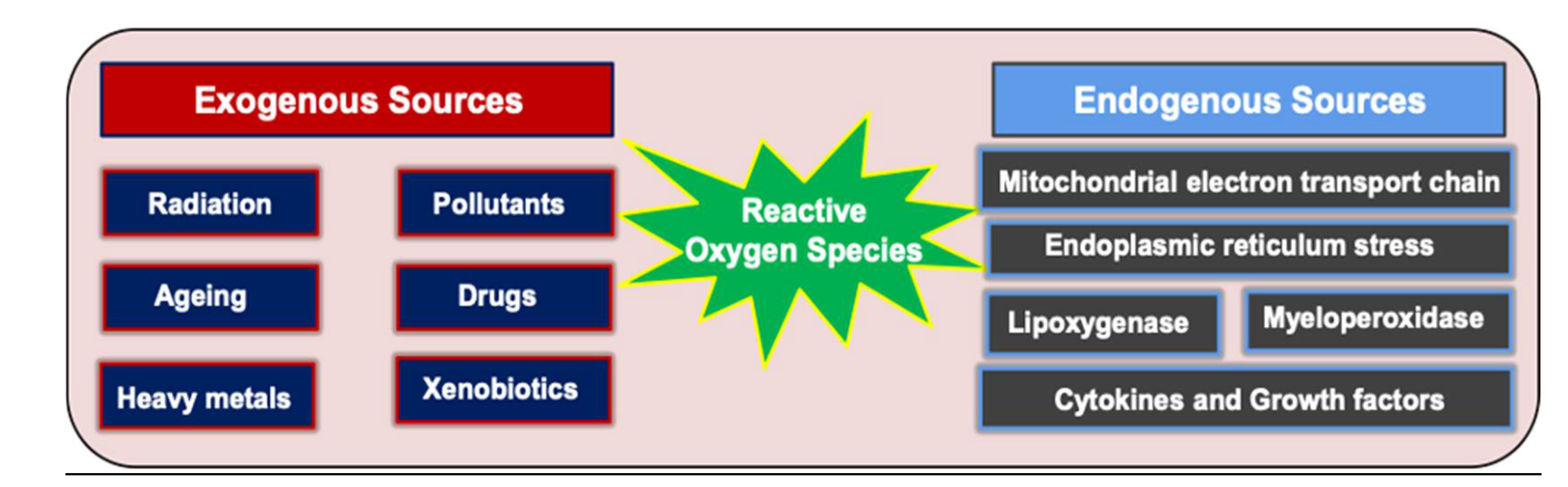
Figure 5.
Schematic illustration of ROS mediated various cell signaling pathways and their role in OC.
Figure 5.
Schematic illustration of ROS mediated various cell signaling pathways and their role in OC.
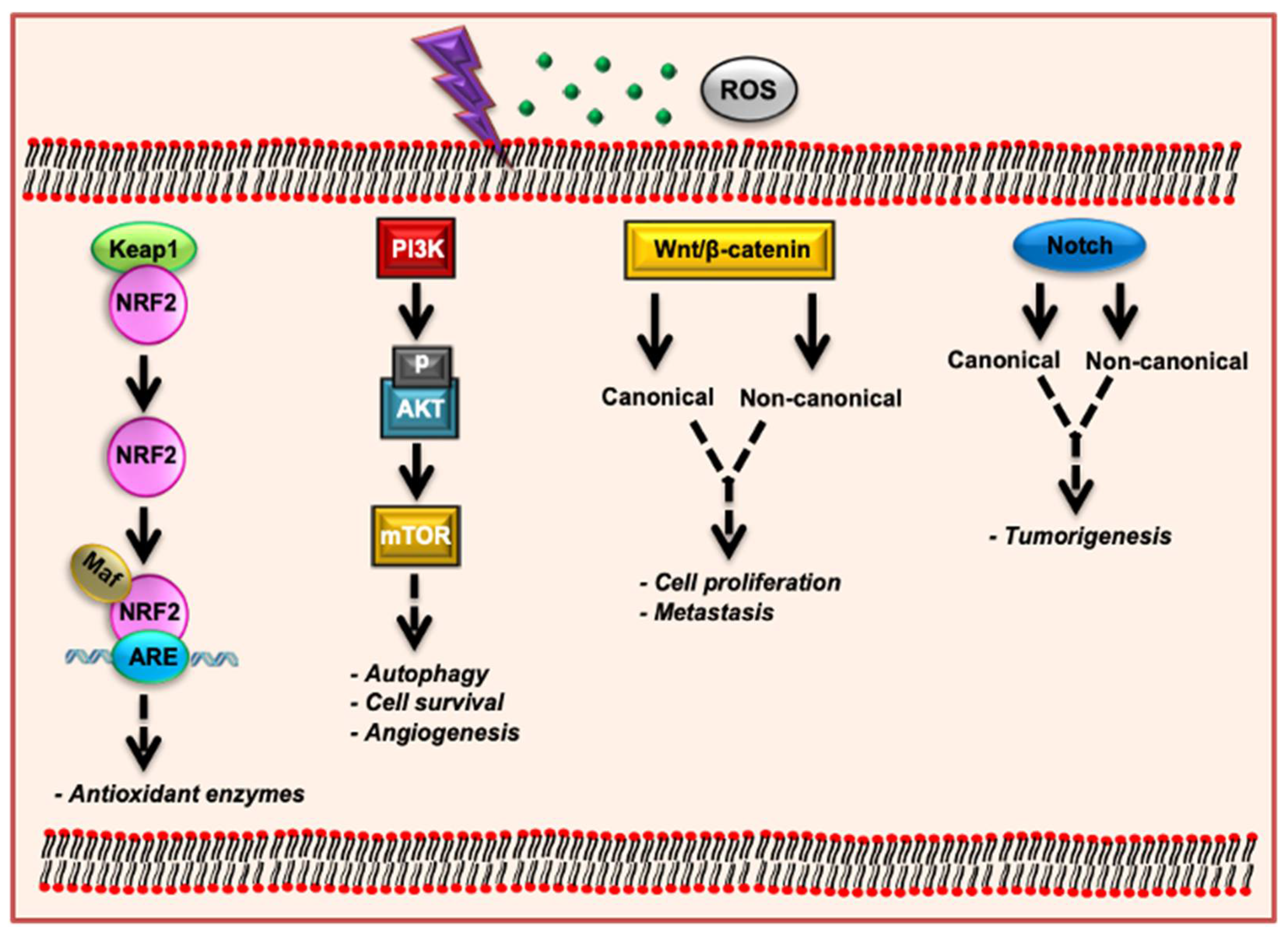
Figure 6.
Representation of biomarkers that were found to increase blood serum in patients with OC. CA125 is the most used and common biomarker nowadays; however, there are novel biomarkers that are used in combination with CA125, or alone for the detection and evaluation of OC, such as HE4, CA15.3, CA72.4, mesothelin, miRNAs, as well as autoantibodies against IL-8, EpCAM, PLAT, c-Myc, MDM2, and HOXA7.
Figure 6.
Representation of biomarkers that were found to increase blood serum in patients with OC. CA125 is the most used and common biomarker nowadays; however, there are novel biomarkers that are used in combination with CA125, or alone for the detection and evaluation of OC, such as HE4, CA15.3, CA72.4, mesothelin, miRNAs, as well as autoantibodies against IL-8, EpCAM, PLAT, c-Myc, MDM2, and HOXA7.

Figure 7.
Representing factors that should be considered before the treatment, including condition of the patient and the disease stage; and the main treatment types that are used nowadays, such as surgery, chemotherapy, radiotherapy, and immunotherapy.
Figure 7.
Representing factors that should be considered before the treatment, including condition of the patient and the disease stage; and the main treatment types that are used nowadays, such as surgery, chemotherapy, radiotherapy, and immunotherapy.
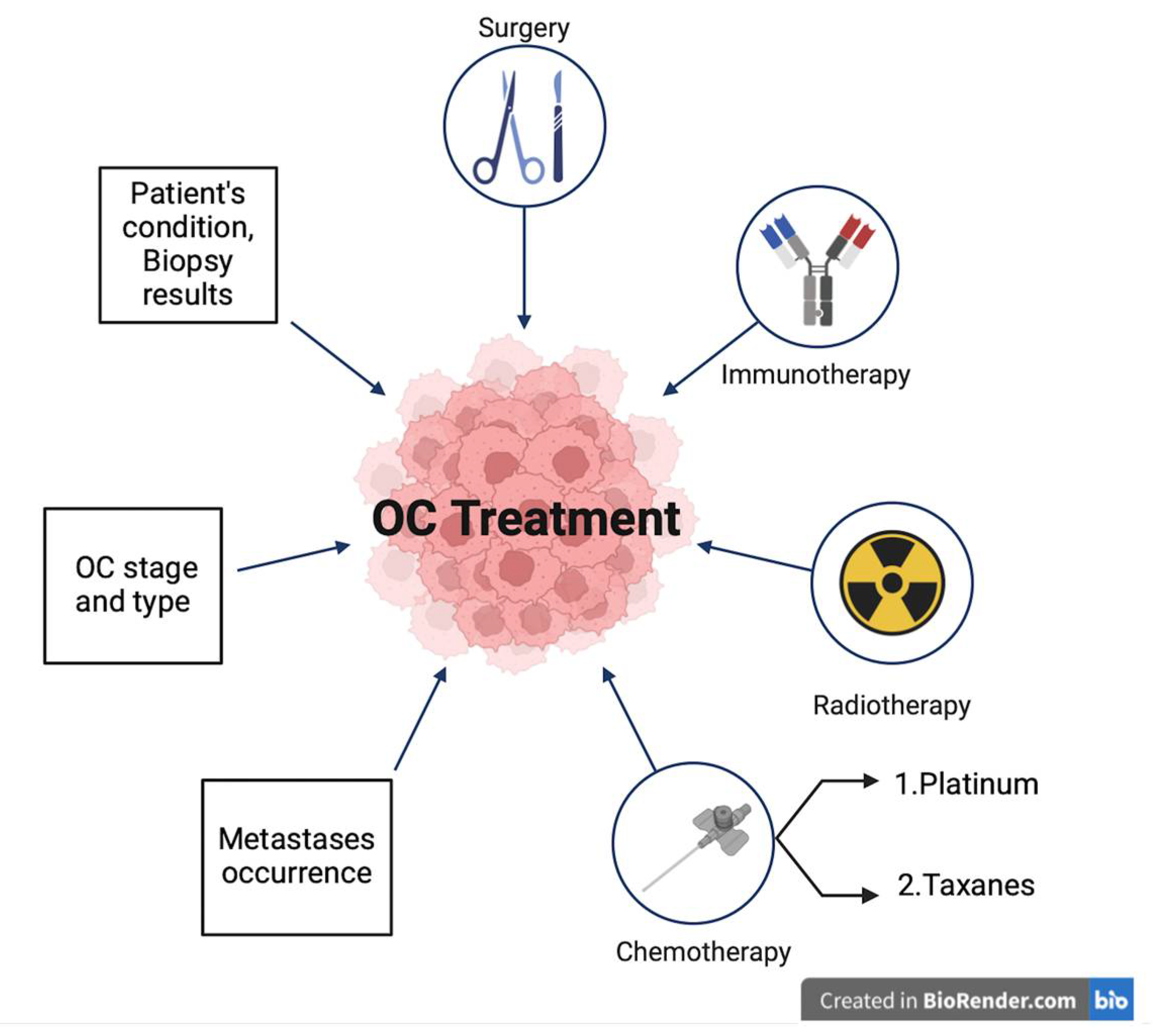
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



