Submitted:
09 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
Rates of involuntary childness are on the uprise which can bring high medical costs and emotional afflictions. This review explores the emerging roles of CoQ10 - including the ubiquinol form in fertility. PubMed, Science Direct and Google Scholar were searched for RCTs, retrospective or prospective controlled studies published between January 1, 2009, and April 31, 2024. The keywords CoQ10, ubiquinol, fer/sub/infertility, ovarian reserve, oocyte quality, ovulation, amenorrhea, polycystic ovary syndrome, sperm quality, seminal fluid, and IVF were used. A total of 15 publications were identified. From a mechanistic stance CoQ10 appears to improve mitochondrial energetics, attenuate oxidative stress and modifications to DNA, proteins, and lipids. Such mechanisms appear to underpin improvements in oocyte quality/fertilization, markers of sperm quality and more broadly PCOS symptoms and hormone levels which can impact on fertility. The role of the ubiquinol form looks particularly promising, which may be attributed to its bioavailability. Ongoing research is needed but there is scope to raise CoQ10 awareness amongst reproductive health experts.
Keywords:
Coenzyme Q10
; Conception
; Infertility
; Mitochondria
; Oocyte
; Reproduction
; Sperm quality
; Ubiquinol.
1. Introduction
Large and indeed increasing proportions of people are being affected by infertility with approximately 17.5% (around 1 in 6) experiencing infertility [1]. From a statistical stance infertility has been estimated to affect around 48 million couples and 186 million individuals worldwide [2]. In turn, infertility can contribute to stigma, financial hardship, significant distress, depression, anxiety and reduced life quality [1].
A range of terms can be used to describe childlessness. The term involuntary childlessness encompasses the inability to conceive alongside those who are unable to access fertility treatments [3]. Subfertility can be used interchangeably with the term infertility and generally refers to any form of reduced fertility [4,5]. The World Health Organisation (2023) defines infertility a disease of the reproductive system (female or male) defined by the failure to achieve a pregnancy after 12 months or more of regular unprotected sexual intercourse [1].
Causes of infertility can be multifaceted including genetic, environmental (such as xenobiotics; synthetic chemical compounds), immunological, and metabolic reasons, among others [6,7,8]. Amongst male lifestyle factors ageing, testicular dysfunction, endocrinopathies, congenital anatomical factors and gonadotoxic exposures are some potential explanations [9]. For females endocrine disruptors have been found to be associated with diseases linked to infertility such as irregular menstrual cycles, endometriosis, and polycystic ovary syndrome (PCOS) [2]. Globally, PCOS is one of the most frequent endocrine diseases, affecting up to 6.2-19.5% women in European countries and the USA [10,11].
Given present rates of infertility coupled with the fact that medical costs for a round of in vitro fertilization (IVF) are often higher than the average annual income [12] the role of nutrition and lifestyle has become increasingly important. A range of nutritional factors including energy intake, vitamins B12, D and B6, biotin, methionine, choline, selenium, zinc, folic acid, resveratrol, and quercetin have been identified as having epigenetic mechanisms capable of influencing genes influencing fertility [13]. Increasingly, the role of coenzyme Q10 (CoQ10) in health and disease has been advancing over the last decade, with fertility being a major field of interest and this being referred to as a ‘miracle nutrient’ [14,15]. Given this, the present narrative review focuses on latest evidence related to this specific nutrient, with particular interest in the ubiquinol form.
2. CoQ10 Ubiquinol
Coenzyme Q10 (CoQ10) is a lipid-soluble vitamin-like coenzyme that occurs naturally in the body and has a ‘ubiquitous’ presence in living organisms, hence is often referred to as ‘ubiquinone’[16,17]. It has vital roles in cell function, mitochondrial bioenergetics, scavenging of free radicals and reactive oxygen species, serving as an antioxidant [8]. CoQ10 can be produced in vivo and obtained from the diet [18].
CoQ10 can be derived from the diet with oily fish such as sardines and salmon, organ meats (such as liver), poultry, whole grains, and green vegetables such as broccoli and spinach being predominant sources [18,19,20]. As CoQ10 is lipid-soluble it is absorbed more effectively when ingested with a meal or food providing some lipids [20]. In instances where diets are balanced most individuals obtain sufficient amount of CoQ10 [20]. However, it should be recognised that endogenous synthesis of CoQ10 requires tyrosine participation and eight vitamins, thus is a complex process affected by status of other micronutrients [21]. Subsequently, shortfalls in micronutrient intakes, as evidenced from dietary surveys [22,23,24] could impact on CoQ10 status.
CoQ10 exists and alternates between two forms – ubiquinone which is the inactive oxidised form and ubiquinol which is the active reduced form [15]. When ubiquinone is taken orally, during absorption it is converted to ubiquinol and stays in its reduced form in the blood and lymph (Figure 1) [15,25,26]. Ubiquinol makes up approximately 95% of all CoQ10 circulating in the body [16]. Bioavailability research comparing 200mg/day supplementation with ubiquinone and ubiquinol over 4 weeks found that ubiquinol had superior bioavailability and raised plasma CoQ10 levels from 0.9 to 4.3µg/mL [27]. In a double-blind trial with older men ubiquinol (200 mg/d) compared with ubiquinone after 2 weeks was more effective at improving CoQ10 status [28]. Other research has shown that after 4 weeks of consuming 300mg ubiquinol daily [29] blood ubiquinol levels were more than twice as high as CoQ10 levels after 4 weeks of 900mg/d ubiquinone [30].
Adapted from: Mantle & Dybring [25]
3. Potential Mechanisms
CoQ10 is a recognised lipid antioxidant, preventing free radical generation and modifications to DNA, proteins and lipids [20]. The human body contains around 500-1500mg CoQ10, an amount that can decline with maternal and paternal age [20].
In females mature oocytes (egg cells) house around 100,000 mitochondria [31] compared with about 1000-2500 mitochondria in other human cells [32]. Mitochondria are the energy factories of cells, and reduced amounts can diminish fertilisation rates and embryonic development [33]. As women age oocytes are susceptible to oxidative stress, mitochondrial dysfunction and a corresponding decline in CoQ10 levels [8]. CoQ10 administration is thought to be one means to offsetting this [34].
In around 50% of cases, infertility can arise from the male [35]. In the case of human sperm, mitochondria are wrapped helically around the centre of the tail, providing the energy that drives the force of motility[36]. Oxidative stress is one factor that can underpin idiopathic male infertility and CoQ10 is thought to reduce this [37]. Meta-analytical evidence implies that sperm motility, morphology and sperm counts could potentially be favourably modulated by CoQ10 supplementation [38].
4. Materials and Methods
This narrative review article investigated latest data regarding CoQ10 (ubiquinol focus) from supplements and associations with female and male fertility. PubMed, Science Direct, Google Scholar and ClinicalTrials.gov were used to search the literature for articles published between January 1. 2009 and April 30, 2024. The search conducted used the following keywords: “Coenzyme Q10” or “ubiquinol” and “infertility”, or “subfertility”, or “fertility”, or “ovarian reserve” or “oocyte quality” or “ovulation”, or “amenorrhea” or “polycystic ovary syndrome”, or “IVF” or “sperm” or “seminal fluid”. The search was restricted to mainly Randomised Controlled Trials (RCTs) regarded as the gold standard for effectiveness research [39]. Some retrospective or prospective controlled studies were also included. Reference lists were searched for relevant articles. Articles were excluded if they did not include any biomarkers related to reproduction or fertility or were duplicate articles. Any retracted articles were also excluded. Fifteen articles were identified for this narrative review, indicating that there is a growing evidence-base in this field.
5. Results
5.1. Females
Eight key studies have been conducted with females [40,41,42,43,44,45,46,47] (Table 1). Amongst females, four studies recruited women with PCOS at baseline [41,42,44,46], with two observing beneficial reductions in testosterone levels with 100-200mg/d CoQ10 administration for 8-12 weeks [41,42]. Jamal et al. (2023) provided 50mg CoQ10 thrice daily over 45-days to women with PCOS finding that chances of ovulation induction increased which was successful in 23.5% patients when CoQ10 was combined with Clomiphene citrate [40]. Ammar et al. (2021) found in Clomiphene Citrate resistant patients that 100mg/d CoQ10 (ubiquinol) from the 2nd day of the cycle until the day of hCG triggering augmented ovarian responsiveness, endometrial thickness, number of stimulated cycles, luteal function and the pregnancy rate with results comparable to the conventional hCG stimulation protocol [44]. Similarly, in Clomiphene Citrate resistant patients with PCOS 60mg CoQ10 thrice daily improved markers of ovarian health (follicle size, endometrial thickness, pregnancy rate) in women trying to conceive compared with the control group [46].
In a study of 169 females with poor ovarian reserve CoQ10 administration (200mg thrice a day) for 60 days preceding IVF significantly increased the number of oocytes retrieved [43]. Those receiving CoQ10 also had more high-quality embryos and a higher fertilization rate compared to those with no treatment before IVF [43]. In research with 299 women undergoing in vitro fertilisation and intracytoplasmic sperm injection (IVF-ICSI), the subgroup (n=139) using a supplement providing 100mg CoQ10 (+600mg omega-3, 300mg eicosapentaenoic acid, 230mg docosahexaenoic acid) had a pregnancy rate that was statistically significantly higher (p<0.05; 49.6%) than those who did not use the supplement which was 32.9% [45]. Caballero et al. (2016) did not report any significant differences between CoQ10 use (600mg twice daily) and the number of oocytes retrieved, implantation or pregnancy rate, possibly due to the small sample size [47].
5.2. Males
Seven key studies have been undertaken with males [48,49,50,51,52,53,54] (Table 2). Five studies recruited males with idiopathic oligoasthenoteratozoospermia (OAT; 3 sperm parameters affected - number, movement, and shape) [48,49,50,52,54]. CoQ10 as a dose of 200mg/d was administered in four of these studies and 300 mg/d in research by Safarinejad et al. (2009) [54]. Four out of five of these studies found improvements in semen parameters, antioxidant measures and reduced DNA fragmentation [48], sperm progressive and total motility and concentration [49], sperm morphology and antioxidant activity [50] and sperm density and motility [54].
In earlier research by Nadjarzadeh et al. (2011) whilst total antioxidant capacity in seminal fluid increased after 6-months of CoQ10 supplementation (200mg/d) no significant changes in semen parameters were observed [52]. This may have been attributed to the smaller sample size (n=47) in this study. A later study by the same research team with n=60 infertile men found that normal sperm morphology, catalase, and superoxide dismutase (SOD) levels were significantly and positively correlated with CoQ10 levels [50]. 300mg/d CoQ10 administered to infertile males over 26-weeks has also been found to be effective at improving sperm density, motility and morphology [54].
Safarinejad et al. (2012) recruited 228 men with unexplained fertility and after administering 200mg/d ubiquinol over 26-weeks identified positive associations (using correlation coefficients) between ubiquinol treatment duration and sperm motility, density and morphology [51]. Balercia et al. (2009) recruited males with idiopathic low sperm motility at baseline and administered 200mg/d CoQ10 over 6-months [53]. It was found that those with lower sperm motility levels were more likely to respond to CoQ10 administration which could help to improve sperm kinetic features [53].
6. Discussion and Future Directions
Infertility can be specific to one gender, or affect both partners, with a range of factors being involved [5]. Oocyte failure and/or poor semen quality in modern-day are driving up the need for assisted reproduction [55]. Underpinning factors can be multi-faceted but lifestyle factors such as poor air quality and nutritional factors such as dietary energy, nutrients and non-nutrients can impact on fertility [13]. In past publications a range of nutrients such as zinc, selenium, omega-3 fatty acids and carnitine have been linked to increased sperm quality and pregnancy rates, but few have focused on the role(s) of ubiquinol CoQ10.
The science on CoQ10 and the ubiquinol form is surfacing in relation to its potential protective effects on reproductive health and fertility [8,14]. Several studies have been published studying the effects of CoQ10/ubiquinol on aspects of female fertility [40,41,42,43,44,45]. For females several RCTs recruiting women with PCOS have shown that 200mg/d CoQ10 can improve hormone profiles (namely reductions in testosterone) and the chances of ovulation induction [40,41,42] or ovarian responsiveness in Clomiphene Citrate resistant PCOS patients [44].
Regarding the efficacy of CoQ10/ubiquinol in women undergoing in vitro fertilization and/or intracytoplasmic injection there is promising evidence that CoQ10 has potential to improve embryo quality, the number of oocytes retrieved and fertilization and pregnancy rates [43,45]. For example, Ozdemir et al. (2019) reported that the total gonadotropin dose needed for stimulation was significantly lower (p<0.01) in patients using antioxidants which included CoQ10 as ubiquinol [45]. The median gonadotropin dose was 2550 IU in the patients supplementing with antioxidants versus 3600 IU in those not taking these [45]. Other research with infertile women undergoing IVF found that those taking ubiquinol CoQ10 capsules (30mg) for eight-weeks before undergoing in vitro fertilization had a significantly higher number of oocytes retrieved, number of metaphase II oocytes, number of fertilized oocytes, number of Day 3 embryos, and top- quality D3 embryos compared with the control group (no supplements) [56,57]. Other research with 50 amenorrhic infertile patients found 150mg/d ubiquinol over 4 months increased follicle stimulating and luteinizing hormones with reduced oxidative stress in the neuroendocrine system thought to be one plausible explanation [58].
A growing number of RCTs have also studied men with idiopathic OAT as baseline [48,49,50,52,54]. Amongst these the administration of 200mg/d CoQ10/ubiquinol over the course of 3-6 months appears to benefit semen parameters which included sperm concentration, motility, and morphology [48,49,50]. Higher dosages of 300mg/d CoQ10 administered to infertile males over 26-weeks have also been found to be effective as improving sperm density, motility and morphology [54]. It would be beneficial for future studies to clearly specify the form of CoQ10 used alongside the dosage.
Regarding sources, a well-balanced diet may supply sufficient amounts of CoQ10, but supplementation may be beneficial in particular situations [18]. Interestingly, in a study of 211 males with subfertility mean daily CoQ10 intake from food was 19.2mg/d which was not associated with any semen parameters [59]. This indicates that CoQ10 from food alone may not be sufficient in terms of optimising semen parameters – intakes were 10-fold lower than supplemental doses used in clinical trials[59]. As mentioned, tyrosine and micronutrients appear to play a role in CoQ10 metabolic pathways [21]. Further studies assessing habitual intakes of CoQ10 would be beneficial, particularly amongst those of reproductive age. It is plausible that CoQ10 intakes could be lower than anticipated due to transitional (plant-based) dietary movements excluding some CoQ10 food sources [60]. It is also important to consider that certain mutations in genes involved the multi-step biochemical pathway of CoQ10 synthesis can alter status and result in primary deficiency [61]. In humans at least 10 genes are required for CoQ10 biosynthesis and mutations in any of these may impact on CoQ10 status and result in deficits [62]. Individuals with such mutations may subsequently be most responsive to supplementation programmes [62]. Future fertility clinics may consider screening for these.
The European Food Safety Authority in 2010 [63] authorised several health claims, some of which relate to adults of reproductive age. After reviewing evidence for CoQ10 the panel considered that ‘contribution to normal energy-yielding metabolism is a beneficial physiological effect’ and that ‘protection of DNA, proteins and lipids from oxidative damage may be a beneficial physiological effect’ [63]. In terms of dosages, most RCTs administered 200 mg/d CoQ10 daily with the longest interventions being conducted over 6-months [42,48,49,50,51,52,53]. Previous research has also found that plasma CoQ10 levels increase in a dose-dependent manner in a daily dose of up to 200mg [64]. Data from preclinical and clinical studies generally shows that CoQ10 supplementation is safe and well tolerated, although gastrointestinal side-effects may be observed when doses exceed beyond 1,200 mg/d/person [17,65].
CoQ10/ubiquinol supplementation appears to be a low-cost and low-risk strategy that could attenuate the impact of aging, mitochondrial damage and reproductive toxicity induced by environmental xenobiotics on fertility [8,18,66]. Health care practitioners, including those working in reproductive medicine or with couples seeking to conceive may wish to consider the potential roles of CoQ10, particularly ubiquinol which appears to be more bioavailable [27,28]. Targeted educational programmes in this field may pave the way for CoQ10 to be used as an adjunct alongside IVF treatments, or as a lifestyle measure for those planning to conceive. This could be of particular benefit to those experiencing sub or infertility or who are of advanced maternal/paternal age.
7. Conclusions
The underpinning causes of involuntary childness/sub and infertility are complex and multi-faceted. Increasingly, rising costs of IVF coupled with advanced maternal and paternal age means that nutritional adjunctives could have a role to play in the field of reproductive health. A growing body of evidence from RCTs, retrospective or prospective controlled studies indicates that CoQ10/ubiquinol could have a role to play by improving mitochondrial energetics, reducing oxidative stress and modifications to DNA, proteins, and lipids. This appears to benefit oocyte quality/fertilization, markers of sperm quality and could have a role in attenuating symptoms of PCOS which in turn impact on fertility. There is scope to raise awareness about CoQ10, particularly the bioavailable ubiquinol form amongst reproductive and medical healthcare practitioners.
Author Contributions
ED wrote the first draft and edited the publication.
Funding
E.D. received funding provided by Kaneka to research and write the article.
Conflicts of Interest
E.D. received funding provided by Kaneka to research and write the article. Kaneka played no role in the writing or production of the article.
References
- WHO. World Health Organisation. Infertility Prevalence Estimates, 1990–2021. Available online: (accessed on.
- Silva, A.B.P.; Carreiro, F.; Ramos, F.; Sanches-Silva, A. The role of endocrine disruptors in female infertility. Mol Biol Rep 2023, 50, 7069–7088. [Google Scholar] [CrossRef]
- Cavaliere, G. Involuntary Childlessness, Suffering, and Equality of Resources: An Argument for Expanding State-funded Fertility Treatment Provision. J Med Philos 2023, 48, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Gnoth, C.; Godehardt, E.; Frank-Herrmann, P.; Friol, K.; Tigges, J.; Freundl, G. Definition and prevalence of subfertility and infertility. Hum Reprod 2005, 20, 1144–1147. [Google Scholar] [CrossRef] [PubMed]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin Biochem 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Sang, Q.; Ray, P.F.; Wang, L. Understanding the genetics of human infertility. Science 2023, 380, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Kicinska, A.M.; Maksym, R.B.; Zabielska-Kaczorowska, M.A.; Stachowska, A.; Babinska, A. Immunological and Metabolic Causes of Infertility in Polycystic Ovary Syndrome. Biomedicines 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Hornos Carneiro, M.F.; Colaiacovo, M.P. Beneficial antioxidant effects of Coenzyme Q10 on reproduction. Vitam Horm 2023, 121, 143–167. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, M.L.; Esteves, S.C.; Lamb, D.J.; Hotaling, J.M.; Giwercman, A.; Hwang, K.; Cheng, Y.S. Male infertility. Nat Rev Dis Primers 2023, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Belenkaia, L.V.; Lazareva, L.M.; Walker, W.; Lizneva, D.V.; Suturina, L.V. Criteria, phenotypes and prevalence of polycystic ovary syndrome. Minerva Ginecol 2019, 71, 211–223. [Google Scholar] [CrossRef]
- Chiaffarino, F.; Cipriani, S.; Dalmartello, M.; Ricci, E.; Esposito, G.; Fedele, F.; La Vecchia, C.; Negri, E.; Parazzini, F. Prevalence of polycystic ovary syndrome in European countries and USA: A systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol 2022, 279, 159–170. [Google Scholar] [CrossRef]
- Njagi, P.; Groot, W.; Arsenijevic, J.; Dyer, S.; Mburu, G.; Kiarie, J. Financial costs of assisted reproductive technology for patients in low- and middle-income countries: A systematic review. Hum Reprod Open 2023, 2023, hoad007. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, K.; Sanlier, N.T.; Sanlier, N. Are epigenetic mechanisms and nutrition effective in male and female infertility? J Nutr Sci 2023, 12, e103. [Google Scholar] [CrossRef] [PubMed]
- Cirilli, I.; Damiani, E.; Dludla, P.V.; Hargreaves, I.; Marcheggiani, F.; Millichap, L.E.; Orlando, P.; Silvestri, S.; Tiano, L. Role of Coenzyme Q(10) in Health and Disease: An Update on the Last 10 Years (2010-2020). Antioxidants (Basel) 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Pelton, R. Coenzyme Q(10): A Miracle Nutrient Advances in Understanding. Integr Med (Encinitas) 2020, 19, 16–20. [Google Scholar] [PubMed]
- Acosta, M.J.; Vazquez Fonseca, L.; Desbats, M.A.; Cerqua, C.; Zordan, R.; Trevisson, E.; Salviati, L. Coenzyme Q biosynthesis in health and disease. Biochim Biophys Acta 2016, 1857, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Arenas-Jal, M.; Sune-Negre, J.M.; Garcia-Montoya, E. Coenzyme Q10 supplementation: Efficacy, safety, and formulation challenges. Compr Rev Food Sci Food Saf 2020, 19, 574–594. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, M.; Colaiacovo, M. Chapter Six - Beneficial antioxidant effects of Coenzyme Q10 on reproduction. Vitamins and Hormones 2023, 121, 143–167. [Google Scholar]
- Weber, C.; Bysted, A.; Holmer, G. Coenzyme Q10 in the diet--daily intake and relative bioavailability. Mol Aspects Med 1997, 18 Suppl, S251–254. [Google Scholar] [CrossRef]
- Saini, R. Coenzyme Q10: The essential nutrient. J Pharm Bioallied Sci 2011, 3, 466–467. [Google Scholar] [CrossRef]
- Alcazar-Fabra, M.; Navas, P.; Brea-Calvo, G. Coenzyme Q biosynthesis and its role in the respiratory chain structure. Biochim Biophys Acta 2016, 1857, 1073–1078. [Google Scholar] [CrossRef]
- Derbyshire, E. Micronutrient Intakes of British Adults Across Mid-Life: A Secondary Analysis of the UK National Diet and Nutrition Survey. Front Nutr 2018, 5, 55. [Google Scholar] [CrossRef] [PubMed]
- Mitsopoulou, A.V.; Magriplis, E.; Michas, G.; Micha, R.; Chourdakis, M.; Chrousos, G.P.; Roma, E.; Panagiotakos, D.B.; Zampelas, A.; Karageorgou, D.; et al. Micronutrient dietary intakes and their food sources in adults: The Hellenic National Nutrition and Health Survey (HNNHS). J Hum Nutr Diet 2021, 34, 616–628. [Google Scholar] [CrossRef]
- Liu, J.; Zhu, X.; Fulda, K.G.; Chen, S.; Tao, M.H. Comparison of Dietary Micronutrient Intakes by Body Weight Status among Mexican-American and Non-Hispanic Black Women Aged 19-39 Years: An Analysis of NHANES 2003-2014. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Mantle, D.; Dybring, A. Bioavailability of Coenzyme Q(10): An Overview of the Absorption Process and Subsequent Metabolism. Antioxidants (Basel) 2020, 9. [Google Scholar] [CrossRef]
- Bhagavan, H.N.; Chopra, R.K.; Craft, N.E.; Chitchumroonchokchai, C.; Failla, M.L. Assessment of coenzyme Q10 absorption using an in vitro digestion-Caco-2 cell model. Int J Pharm 2007, 333, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Langsjoen, P.H.; Langsjoen, A.M. Comparison study of plasma coenzyme Q10 levels in healthy subjects supplemented with ubiquinol versus ubiquinone. Clin Pharmacol Drug Dev 2014, 3, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, J.; Chen, X.Q.; Oliver Chen, C.Y. Ubiquinol is superior to ubiquinone to enhance Coenzyme Q10 status in older men. Food Funct 2018, 9, 5653–5659. [Google Scholar] [CrossRef] [PubMed]
- Hosoe, K.; Kitano, M.; Kishida, H.; Kubo, H.; Fujii, K.; Kitahara, M. Study on safety and bioavailability of ubiquinol (Kaneka QH) after single and 4-week multiple oral administration to healthy volunteers. Regul Toxicol Pharmacol 2007, 47, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Ikematsu, H.; Nakamura, K.; Harashima, S.; Fujii, K.; Fukutomi, N. Safety assessment of coenzyme Q10 (Kaneka Q10) in healthy subjects: A double-blind, randomized, placebo-controlled trial. Regul Toxicol Pharmacol 2006, 44, 212–218. [Google Scholar] [CrossRef]
- Babayev, E.; Seli, E. Oocyte mitochondrial function and reproduction. Curr Opin Obstet Gynecol 2015, 27, 175–181. [Google Scholar] [CrossRef]
- Pizzorno, J. Mitochondria-Fundamental to Life and Health. Integr Med (Encinitas) 2014, 13, 8–15. [Google Scholar] [PubMed]
- Labarta, E.; de Los Santos, M.J.; Escriba, M.J.; Pellicer, A.; Herraiz, S. Mitochondria as a tool for oocyte rejuvenation. Fertil Steril 2019, 111, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ben-Meir, A.; Burstein, E.; Borrego-Alvarez, A.; Chong, J.; Wong, E.; Yavorska, T.; Naranian, T.; Chi, M.; Wang, Y.; Bentov, Y.; et al. Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell 2015, 14, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Skoracka, K.; Eder, P.; Lykowska-Szuber, L.; Dobrowolska, A.; Krela-Kazmierczak, I. Diet and Nutritional Factors in Male (In)fertility-Underestimated Factors. J Clin Med 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Hirata, S.; Hoshi, K.; Shoda, T.; Mabuchi, T. Spermatozoon and mitochondrial DNA. Reprod Med Biol 2002, 1, 41–47. [Google Scholar] [CrossRef]
- Alahmar, A.T.; Calogero, A.E.; Singh, R.; Cannarella, R.; Sengupta, P.; Dutta, S. Coenzyme Q10, oxidative stress, and male infertility: A review. Clin Exp Reprod Med 2021, 48, 97–104. [Google Scholar] [CrossRef]
- Salas-Huetos, A.; Rosique-Esteban, N.; Becerra-Tomas, N.; Vizmanos, B.; Bullo, M.; Salas-Salvado, J. The Effect of Nutrients and Dietary Supplements on Sperm Quality Parameters: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Adv Nutr 2018, 9, 833–848. [Google Scholar] [CrossRef]
- Hariton, E.; Locascio, J.J. Randomised controlled trials - the gold standard for effectiveness research: Study design: Randomised controlled trials. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef]
- Jamal, H.; Waheed, K.; Mazhar, R.; Sarwar, M.Z. Comparative Study Of Combined Co-Enzyme Q10 And Clomiphene Citrate Vs Clomiphene Citrate Alone For Ovulation Induction In Patients With Polycystic Ovarian Syndrome. J Pak Med Assoc 2023, 73, 1502–1505. [Google Scholar] [CrossRef]
- Karamali, M.; Gholizadeh, M. The effects of coenzyme Q10 supplementation on metabolic profiles and parameters of mental health in women with polycystic ovary syndrome. Gynecol Endocrinol 2022, 38, 45–49. [Google Scholar] [CrossRef]
- Izadi, A.; Ebrahimi, S.; Shirazi, S.; Taghizadeh, S.; Parizad, M.; Farzadi, L.; Gargari, B.P. Hormonal and Metabolic Effects of Coenzyme Q10 and/or Vitamin E in Patients With Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2019, 104, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Nisenblat, V.; Lu, C.; Li, R.; Qiao, J.; Zhen, X.; Wang, S. Pretreatment with coenzyme Q10 improves ovarian response and embryo quality in low-prognosis young women with decreased ovarian reserve: A randomized controlled trial. Reprod Biol Endocrinol 2018, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Ammar, I.; Abdou, A. Effect of Ubiquinol supplementation on ovulation induction in Clomiphene Citrate resistance. Middle East Fertility Society Journal 2021, 26, 22. [Google Scholar] [CrossRef]
- Ozdemir, A.; Ayas, B.; Guven, D.; Bakay, A.; Karlh, P. Antioxidant Supplement Improves the Pregnancy Rate in Patients Undergoing in Vitro Fertilization for Unexplained Infertility. Open Journal of Obstetrics and Gynecology 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Sen Sharma, D. Co-enzyme Q10-A mitochondrial antioxidant – a new hope for success in infertility in clomiphene-citrate-resistant polycystic ovary syndrome. Int. J. Obstet. Gynaecol. Oral Commun. [CrossRef]
- Caballero, T.; Fiameni, F.; Valcarcel, A.; Buzzi, J. Dietary supplementation with coenzyme Q10 in poor responder patients undergoing IVF-ICSI Treatment. Fertility and Sterility 2016, 106, E58. [Google Scholar] [CrossRef]
- Alahmar, A.T.; Naemi, R. Predictors of pregnancy and time to pregnancy in infertile men with idiopathic oligoasthenospermia pre- and post-coenzyme Q10 therapy. Andrologia 2022, 54, e14385. [Google Scholar] [CrossRef] [PubMed]
- Alahmar, A.T.; Sengupta, P. Impact of Coenzyme Q10 and Selenium on Seminal Fluid Parameters and Antioxidant Status in Men with Idiopathic Infertility. Biol Trace Elem Res 2021, 199, 1246–1252. [Google Scholar] [CrossRef] [PubMed]
- Nadjarzadeh, A.; Shidfar, F.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Nazeri Kakhki, S.A.; Akhondi, M.M.; Sadeghi, M.R. Effect of Coenzyme Q10 supplementation on antioxidant enzymes activity and oxidative stress of seminal plasma: A double-blind randomised clinical trial. Andrologia 2014, 46, 177–183. [Google Scholar] [CrossRef]
- Safarinejad, M.R.; Safarinejad, S.; Shafiei, N.; Safarinejad, S. Effects of the reduced form of coenzyme Q10 (ubiquinol) on semen parameters in men with idiopathic infertility: A double-blind, placebo controlled, randomized study. J Urol 2012, 188, 526–531. [Google Scholar] [CrossRef]
- Nadjarzadeh, A.; Sadeghi, M.R.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Akhondi, M.A.; Yavari, P.; Shidfar, F. Coenzyme Q10 improves seminal oxidative defense but does not affect on semen parameters in idiopathic oligoasthenoteratozoospermia: A randomized double-blind, placebo controlled trial. J Endocrinol Invest 2011, 34, e224–228. [Google Scholar] [CrossRef]
- Balercia, G.; Buldreghini, E.; Vignini, A.; Tiano, L.; Paggi, F.; Amoroso, S.; Ricciardo-Lamonica, G.; Boscaro, M.; Lenzi, A.; Littarru, G. Coenzyme Q10 treatment in infertile men with idiopathic asthenozoospermia: A placebo-controlled, double-blind randomized trial. Fertil Steril 2009, 91, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Safarinejad, M.R. Efficacy of coenzyme Q10 on semen parameters, sperm function and reproductive hormones in infertile men. J Urol 2009, 182, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Skakkebaek, N.E.; Lindahl-Jacobsen, R.; Levine, H.; Andersson, A.M.; Jorgensen, N.; Main, K.M.; Lidegaard, O.; Priskorn, L.; Holmboe, S.A.; Brauner, E.V.; et al. Environmental factors in declining human fertility. Nat Rev Endocrinol 2022, 18, 139–157. [Google Scholar] [CrossRef]
- Wu, C.C.; Li, C.J.; Lin, L.T.; Wen, Z.H.; Cheng, J.T.; Tsui, K.H. Examining the Effects of Nutrient Supplementation on Metabolic Pathways via Mitochondrial Ferredoxin in Aging Ovaries. Nutrients 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.H.; Su, W.P.; Li, C.J.; Lin, L.T.; Sheu, J.J.; Wen, Z.H.; Cheng, J.T.; Tsui, K.H. Investigating the Role of Ferroptosis-Related Genes in Ovarian Aging and the Potential for Nutritional Intervention. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Thakur, A.S.; Littaru, G.P.; Funahashi, I.; Painkara, U.S.; Dange, N.S.; Chauhan, P. Effect of Ubiquinol on Serum Reproductive Hormones of Amenorrhic Patients. Indian J Clin Biochem 2016, 31, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Tiseo, B.C.; Gaskins, A.J.; Hauser, R.; Chavarro, J.E.; Tanrikut, C.; Team, E.S. Coenzyme Q10 Intake From Food and Semen Parameters in a Subfertile Population. Urology 2017, 102, 100–105. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Hosoe, K.; Funahashi, I. Lower plasma coenzyme Q10 concentrations in healthy vegetarians and vegans compared with omnivores. Nutrafoods 2022, 1, 379–386. [Google Scholar]
- Hargreaves, I.; Heaton, R.A.; Mantle, D. Disorders of Human Coenzyme Q10 Metabolism: An Overview. Int J Mol Sci 2020, 21. [Google Scholar] [CrossRef]
- Mantle, D.; Millichap, L.; Castro-Marrero, J.; Hargreaves, I.P. Primary Coenzyme Q10 Deficiency: An Update. Antioxidants (Basel) 2023, 12. [Google Scholar] [CrossRef]
- EFSA. European Food Safety Authority. Scientific Opinion on the substantiation of health claims related to coenzyme Q10 and contribution to normal energy-yielding metabolism (ID 1508, 1512, 1720, 1912, 4668), maintenance of normal blood pressure (ID 1509, 1721, 1911), protection of DNA, proteins and lipids from oxidative damage (ID 1510), contribution to normal cognitive function (ID 1511), maintenance of normal blood cholesterol concentrations (ID 1721) and increase in endurance capacity and/or endurance performance (ID 1913) pursuant to Article 13(1) of Regulation (EC) No 1924/20061. EFSA Journal 2010, 8, 1793. [Google Scholar]
- Kaikkonen, J.; Tuomainen, T.P.; Nyyssonen, K.; Salonen, J.T. Coenzyme Q10: Absorption, antioxidative properties, determinants, and plasma levels. Free Radic Res 2002, 36, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Villalba, J.M.; Parrado, C.; Santos-Gonzalez, M.; Alcain, F.J. Therapeutic use of coenzyme Q10 and coenzyme Q10-related compounds and formulations. Expert Opin Investig Drugs 2010, 19, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.F.; Soares, M.; Almeida-Santos, T.; Ramalho-Santos, J.; Sousa, A.P. Aging and oocyte competence: A molecular cell perspective. WIREs Mech Dis 2023, 15, e1613. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CoQ10 pathway and ubiquinol production: Stomach to blood circulation.
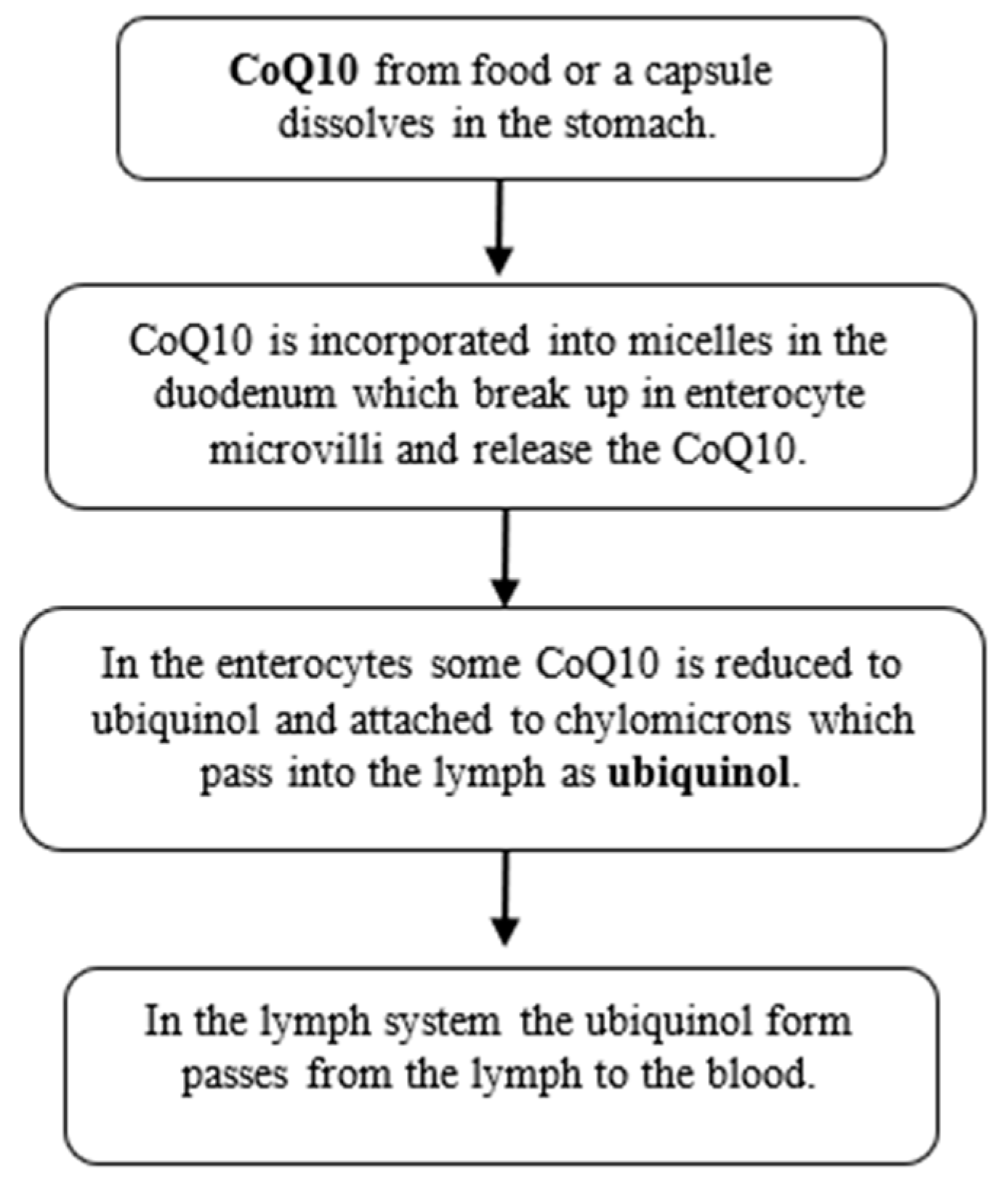

Table 1.
Key RCTs, retrospective or prospective controlled studies investigating Coenzyme Q10/ubiquinol administration and aspects of female fertility.
Table 1.
Key RCTs, retrospective or prospective controlled studies investigating Coenzyme Q10/ubiquinol administration and aspects of female fertility.
| Author | Sample population | Type and duration of study | Outcome of focus | Supplement dosage | Main Findings |
|---|---|---|---|---|---|
| Females | |||||
| [40] | n=136 females with PCOS | 45-day randomized controlled trial | Ovulation induction | 50mg CoQ10 in soft gel capsules thrice per day | In the CoQ10 plus Clomiphene citrate group ovulation induction was observed in 23.5% patients, indicating that with the addition of CoQ10 improved the chances of ovulation induction. |
| [41] | n=55 PCOS women (aged 18-40 yrs) | 12-week double-blinded, placebo-controlled randomized clinical trial | Hormonal indices, oxidative stress | 100mg/day of CoQ10 | The CoQ10 group had a significant drop in total testosterone (p = .004), DHEAS (p < .001), hirsutism (p = .002) and MDA (p = .001) levels & a significant rise in SHBG (p < .001) & TAC (p < .001) levels in serum than the placebo group. |
| [44] | n=148 PCOS patients with Clomiphene Citrate resistance (75 treated with ubiquinol and Clomiphene Citrate, and 73 with human menopausal gonadotropins) | Randomized controlled trial | Ovarian responsiveness | 100mg/d of CoQ10 as ubiquinol added to Clomiphene Citrate | No statistically significant differences (P > 0.05) between studied groups regarding ovarian responsiveness. |
| [42] | n=86 females with PCOS | 8-week randomized, double-blind, placebo-controlled clinical trial | Hormonal markers | 200mg/d CoQ10 | CoQ10 with or without vitamin E supplementation among women with PCOS had beneficial effects on total testosterone levels (p<0.001). |
| [45] | n=299 females undergoing IVF-ICSI (135 treated with OMEPA Q10 and 164 controls) | 2-months #break#retrospective case-controlled study | Pregnancy rate,#break#total amount of gonadotropins dose | 100mg/day of CoQ10 as ubiquinol together with omega-3 | Ubiquinol with omega-3 supplementation increased pregnancy rate (p<0.002) and reduced the total gonadotropin dose (p<0.001).#break# |
| [43] | n=169 females with POR (76 treated with CoQ10 and 93 controls) preceding IVF | 60-day randomized controlled trial | Ovarian response, embryo quality | 200mg CoQ10 thrice per day | The CoQ10 group had increased number of retrieved oocytes, higher fertilization rate (67.49%) and more high-quality embryos; p < 0.05. |
| [46] | n=62 infertile females with PCOS | Randomized controlled trial during cycle. | Size of matured follicle, endometrial thickness, clinical pregnancy, miscarriage rate | 60mg CoQ10 thrice per day | Follicle size, endometrial thickness and clinical pregnancy rate were improved in the group receiving CoQ10 and miscarriage rate was lower compared with the control group. |
| [47] | n=78 poor responders in a prior IVF cycle. | 12-week prospective randomized controlled study. | Oocytes retrieved, implantation rate, clinical pregnancy rate | 600 mg Co Q10 twice per day | No significant differences were detected between the CoQ10 and control group. |
Key: CoQ10, Coenzyme Q10; DHEAS, Dehydroepiandrosterone Sulfate; FSH, Follicle Stimulating Hormone; IVF, In Vitro Fertilization; LH, Luteinizing Hormone; MDA, Malondialdehyde; PCOS, Polycystic Ovary Syndrome; POR, Poor Ovarian Response; SHBG, Sex Hormone-Binding Globulin; TAC, Total Antioxidant Capacity.
Table 2.
Key RCTs, retrospective or prospective controlled studies investigating Coenzyme Q10/ubiquinol administration and aspects of male fertility.
Table 2.
Key RCTs, retrospective or prospective controlled studies investigating Coenzyme Q10/ubiquinol administration and aspects of male fertility.
| Author | Sample population | Type and duration of study | Outcome of focus | Supplement dosage | Main Findings |
|---|---|---|---|---|---|
| Males | |||||
| [48] | n=178 male patients with idiopathic OAT and 84 fertile men (controls) | 6-month prospective controlled clinical study | Time to pregnancy | 200mg/d CoQ10 as ubiquinol | CoQ10 significantly improved semen parameters, antioxidant measures and reduced sperm DNA fragmentation. |
| [49] | n=70 men with idiopathic OAT | 3-month randomized controlled trial | Semen parameters | 200mg/d ubiquinol or selenium | Sperm concentration, progressive and total motility significantly increased with CoQ10 treatment (p<0.01) with this being most effective. |
| [50] | n=60 infertile men with idiopathic OAT | 3-month randomized placebo-controlled trial | Oxidative stress and antioxidant enzymes in seminal plasma | 200mg/d CoQ10 | CoQ10 levels significantly increased from 44.74 ± 36.47 to 68.17 ± 42.41 ng ml(-1) following supplementation (p < 0.001). CoQ10 group had higher catalase and SOD activity than the placebo. CoQ10 concentration and normal sperm morphology (p= 0.037), catalase (p= 0.041) and SOD (p < 0.001) were significantly & positively correlated. |
| [51] | n=228 men with unexplained infertility | 26-week double-blind, placebo controlled, randomized trial | Semen parameters | 200mg/d CoQ10 as ubiquinol | Correlation coefficients identified a positive association between ubiquinol treatment & sperm density (r = 0.74, p = 0.017), sperm motility (r = 0.66, p = 0.024) and sperm morphology (r = 0.57, p = 0.027). |
| [52] | n=47 infertile men with idiopathic OAT | 12-week double-blind placebo controlled clinical trial | Semen parameters | 200mg CoQ10 daily | There were non-significant changes in semen parameters in CoQ10 group, but total antioxidant capacity of seminal fluid increased significantly (p<0.05) |
| [53] | n=60 infertile patients (27-39 years of age) with specific baseline sperm selection criteria (idiopathic asthenozoospermia) | 6-month double-blind, placebo controlled, randomized trial | Semen parameters | 200mg/d CoQ10 | CoQ10 and ubiquinol increased significantly in sperm cells and seminal plasma, with males with reduced sperm motility at baseline responding and sperm kinetic features improving. |
| [54] | n=212 infertile men with idiopathic OAT | 26-week randomised controlled trial | Semen parameters, sperm function and reproductive hormones | 300mg/d CoQ10 | Sperm density and motility significantly improved with CoQ10 (p=0.01). Sperm morphology and count also improved. |
Key: DNA, deoxyribonucleic acid; CoQ10, Coenzyme Q10; OAT, Oligoasthenoteratozoospermia; SOD, Superoxide Dismutase.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



