Submitted:
08 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
Food fortification with micronutrients was initially justified in developed countries by lack of availability of micronutrients in staple crops, mainly due to soil exhaustion. However, in Sub-Saharan arable lands soil fatigue is not predominant and communities consume mostly home-grown organic non-processed crops. African food systems are nevertheless deeply entwined with food insecurity, driver of illnesses. Family production can promote subsistence, food stability and self-sufficiency, the main African setback being the vicious cycle of poverty and the lack of dietary variety, contributing to malnutrition. Poverty reduction, and women's education, are significant strategies for reducing child and adolescent undernourishment. Fortification of foods consumed daily by individuals makes sense and can minimize if not entirely eliminate deficiencies. Mass fortification in Sub-Saharan Africa with single micronutrients is however controversial working in synergy among each other and the food matrix, for optimal absorption and metabolism. Since the causes of malnutrition are many, caused by diverse, unequal and unjust food distribution, interrelated with political, social, cultural or economic factors, education status of the population, season and climatic changes, and effectiveness of nutrition programmes, just food fortification cannot solve the composite of these elements. Further, compulsory fortification is excessive, unproductive and likely harmful to human health, while many challenges remain in accessing quality of premixes. However, aiming at dietary diversification is the best approach of increasing trace elements intake from commonly accessible and easily available food sources.
Keywords:
poverty
; food supplements
; undernourishment
; childcare
; premix
1. Introduction
Food production has changed over the decades and is still under permanent improvement namely in productivity rates in most food crops and cash crops value chains. The current structure of the African food systems lies at the centre of a network of global problems, stretching from poverty to environmental degradation.
The necessary increase in food production and productivity, required to meet future demands, cannot be attained by continuing with the existing present directions of growth and intensification, since it will undermine the particular support on which the food systems revolve [1]. There is meanwhile no possible sustainable population growth or development without social justice and end of under nutrition, famine, and poverty [2].
Over the last half century, in general, agricultural intensification of staple crops, mainly maize and wheat, has escalated, required to feed the growing and increasingly demanding human population, taking place in different forms, principles and concepts, norms and values, to be effective forms of sustainable and ecological intensification [3]. The most salient feature of sustainable intensified agro food systems is the greater yield per unit land and time, but may originate hidden environmental, health and social overheads and benefits to the food production chains [4].
Food, not nutrients, is the unit in nutrition, and food diversity and food synergies are determinants for overall health and wellness [5]. Moreover, over 75% of the world’s food production depends on family farmers, representing the vast majority of farming worldwide, both in developed and developing countries. In low income Sub-Saharan African (SSA) countries people indeed consume monotonous diets, a less resilient food system, being prone to nutrient deficiencies [6].
In SSA, food systems have not been suitably accompanied by adequate interventions on access to water, sanitation and hygiene. Globally, some 2.5 billion people (32%) do not have access to clean and safe drinking water, and approximately 3.6 billion people (46% of the world’s population) lack adequate sanitation services [7].
Food and drinkable water affects almost every SSA citizen. Consequently, food and water access, and their quality, are key issues in African human development. A society cannot be considered as developed if these issues are not primarily resolved, since they affect public health, the welfare of people and human capital, hence affecting people’s capacity for development [8].
Indeed, the triangle food - water - hygiene insecurities, are complex, multi-dimensional phenomena that entail more than availability and access [9], and the present disruptions of supply chains, food, and energy markets did impact the long-term effects and the future remains uncertain [10]. Indeed, within the context of the current and consecutive world disasters, sharing common economic, social, climatic, and poly crisis, it is indispensably to consider and react in relation to global food systems, namely cereals.
Globally, no country can produce all the foods that it needs. Food production has been enough for humankind, but distribution is inadequate, while it does not exist a food system that can feed every person, every day, everywhere. At least 90% of rural population in SSA, where food insecurity has steadily risen, depends on agriculture as its primary source of food, income and survival [11].
The World Bank, International Monetary Fund (IMF), OPEC Fund for International Development (OFID), and United Nations have established global targets as part of the Sustainable Development Goals to reduce poverty and “end hunger by 2030”, “the not-so-impossible dream”. While globally there has been some progress in past decades, this target is far from being reached, mainly in SSA, where standards of living are still very low, and chronic poverty is widespread with negative impacts on family dynamics [12].
Food insecurity in SSA must be tackled from a multidimensional perspective, beginning with Governments’ spending on education and health, presently growing very slowly in most SSA countries [13]. Another core problem in SSA has been corruption, abuse of power, and inefficiency of competent authorities, leading to ineffective resource management. Most of the revenues from the exploitation of natural resources (e.g. oil & gas, coal, gold, precious stones) and agricultural staples (e.g. sugar, coffee, cocoa, vegetable oil) fall into political party elites, and national income is not properly distributed to the lower classes, raising the paradox “poverty in the midst of plenty”.
The global assessment of the state of food security and nutrition presently reveals that over 900 million people of the 8 billion people in the world, almost one in eight, were suffering from hunger or, more formally, chronic undernourishment, with the highest rates in SSA [14].
Population needs access to quality and safe nutritious food ingredients, along with access to health services and safe environment [15].
Sub-Saharan Africa as a whole, chiefly Nigeria, South Africa and Kenya, imports wheat for bread production, and rice, from mainly Pakistan, Vietnam, Thailand, France, Russia, Argentine, Brazil, and India, while maize is the main grain staple for more than 50% of the population, family harvested [16].
2. A Brief History of Food Fortification
The industrial fortification of widely-consumed foods was developed as a strategy to prevent and reduce the prevalence of specific nutritional deficiencies as a consequence of the limited availability and affordability of an adequate diversified diet, that includes plant- and animal-source foodstuffs [17].
WHO defines food fortification as the practice of a deliberate increase in the content of one or more micronutrients (i.e., vitamins and minerals) in a food or condiment, to improve their nutritional quality, thereby providing a public health benefit with minimal risks [18].
The earliest food fortification was suggested by a French chemist in 1820, with a proposal of fortifying salt with iodine, and in Switzerland in 1923 and the United States in 1924, when iodine was primarily combined to table salt on an optional basis, in an effort to manage the widespread health problem of goitre [19].
The sourcing of foods from many diverse locations has essentially eliminated the problems of goitre caused by a deficiency of iodine in foods from certain geographical areas, and attention is given presently to pregnant women and women of childbearing age, who may be at risk for mild to moderate iodine deficiency [20].
Fortification is usually carried out by public or private stakeholders aiming public health protection from deficiencies, with micronutrient premixes supplied by several mega-corporations, which are added mainly to flour in the industrial milling process. They should not affect the taste, smell, texture, or baking qualities of the end product.
In SSA communities people eat considerable amounts of leafy greens, manioc tubers and sweet potatoes, local beans of all kinds, nuts (e.g. cashew, coconut), seeds (e.g. sesame), and peanuts, fish and seafood, herbs and spices (Figure 1) [21,22]. Only on special occasions they eat meat and sweets. This scenario is probably superior when compared to developed countries where ultra-processed fast foods and frizzy drinks prevail and overweight/obesity is very high [23,24]. African native diets hold potential nutrients and foods that may be beneficial in protecting them from having chronic diseases including cancer, as opposed to the ‘Western diet’ that increased the risk for multiple types of cancers. There is however, a need for large cohort studies with comprehensive datasets for effective research [25].
In the poor rural regions of SSA, despite the minor levels of ultra-processed foods, micronutrient malnutrition (or hidden hunger) exists namely when there is undernutrition caused by crop shortages. This is becoming common in cases of lack of diet diversification [14].
While SSA governments have taken several steps to address these issues, food fortification has emerged as a widely-discussed solution to tackle malnutrition. However, it is not only malnutrition but also non-communicable diseases (NCD) being an equivalent burden [26].
Food enrichment is the practice of adding micronutrients back to a foodstuff that lost them during picking or processing, while fortification adds additional micronutrients absent (or present in minor amounts) prior to processing [27]. Increasing the levels of essential vitamins and minerals in growing staple crops that are widely consumed by people in affected communities such as in SSA is another sustainable strategy named biofortification, which addresses micronutrient deficiencies [28]; [29].
Large scale public health programmes with single nutrients were perceived to have a poor impact on the target health desired outcomes, both in Asia and in Africa, as for example seen on the dormant reaction of the frequency of anaemia to ongoing iron supplementation programmes [30].
Indeed, to be really successful, and presently absent in SSA, local settings, sociocultural influences, and environmental conditions should be considered as key determinants for enhancement of the micronutrient status of populations [31]. Moreover, the dietary characteristics of the population should be taken into account in order to select the adequate fortification condition with the highest effectiveness potential [32].
This is not performed or managed adequately and routinely, and recurrently it is considered as a freestanding diagnosis. Furthermore, deficiencies in blood are in fact clinical signs which show an underlying aetiology. However, elucidation of its cause is required. Clinical discordance in both the formal definition of deficiencies and in screening protocols is clearly shown [33].
3. Global Large-Scale Food Fortification
Although being mandatory in most SSA countries, food fortification in the United States of America has evolved tremendously over the years and is not generally compulsory, and the FDA made a decision in the 1940s that it would not require mandatory fortification for any food product. This policy is still in place and, with exception to wheat flour, enrichment is not a requirement generally speaking, but if enrichment/fortification is claimed then there are standards that must be met [35].
In Canada some sectors of the food industry and consumers see the current regulatory controls on the addition of vitamins and minerals to foods as overly restrictive [36,37].
Food consumption varies widely among countries and is influenced by many factors, including social, economic, cultural, environmental, educational, health- related and physiological elements [38]. The European Union has published, by commissioning many interested parties, connected with cereal milling and micronutrient suppliers, legislation on fortification of foods and condiments, without mentioning the way how to measure the outcomes and evaluate its contribution to improving public health objectives [39].
Food fortification is not prohibited by laws or regulations of the European Union, as long as certain requirements are fulfilled, such as minimum and maximum amounts of nutrients added. Fortification is not allowed for alcoholic beverages and unprocessed foods and adding vitamins and minerals to food is permitted but not compulsory in the European Union through regulation 1925/2006. Many EU member states have mandatory fortification legislation, but it is possible that the extent of food fortification changes over time, also in the absence of clear fortification policies, which makes up-to-date summaries difficult.
Food intended for specialised nutrition, namely foods for infants and young children, foods for calorie-restricted diets, and dietary foods, is not considered voluntarily fortified since they are covered by specific legislation [40].
The United Kingdom has a distinct large-scale mandatory programme of fortification of wheat flour with iron and other key nutrients since the 1940s. In the UK, the Bread and Flour Regulations (1998) lay down labelling and compositional standards for bread and flour; they also specify that calcium, iron, thiamine (Vitamin B1) and niacin (Vitamin B3) must be added to all white and brown flour. Large-scale mandatory fortification of wheat flour and vegetable oil exists in Burkina Faso, Cameroon, Côte d’Ivoire, Mali, Nigeria and Senegal [41].
In India, fortification of foods is not compulsory, except for iodised salt, with plans to make fortification mandatory for packaged edible oil and milk, pushed by corporate classes which stand to benefit economically from for fortification in India, and after alleged flagrant conflicts of interest in official regulation bodies. However, with many criticisms against mandatory food fortification, with the decision-making body remaining opaque, pushes for iron fortification of rice, is still a topic of debate [42].
In China and Mongolia, where the prevalence of multiple micronutrient deficiencies has decreased substantially in recent decades, despite pressure from the global micronutrient industries, food and beverage fortification has been mandatory only for iodized salt and, on a voluntary basis, for some 50 types of products [43]. A policy of large-scale industrial fortification of wheat flour and wheat flour products, edible oil, and milk has been in place in Mongolia since 2018 [44].
The picture is somewhat different in the SSA region, where the livelihoods of small-scale producers and processors have been swiftly threatened by stringent mandatory regulations, varying with the food vehicle, difficult to implement even by local regulatory authorities.
A sharp fortification programme can only be responsible, effective and sustainable if there is an adequate knowledge of target foodstuffs and diet composition, and an accurate control of micronutrient deficiencies, both yet impractical in most SSA countries.
In developed countries regulation exists for the marketing and labelling of both fortified foods and supplements namely for the individual use of athletes in sports use [45]. A totally different objective of large-scale food fortification in SSA is met, where legislation on compulsory fortification has been unaccountably established.
In SSA many hundreds of national, regional and global organizations with assorted designations and agendas are well established, created towards supporting private or public stakeholders, to improve the supply of missing nutrients (e.g. vitamin A, thiamine, riboflavin, niacin, pyridoxine, folic acid, iodine, iron and zinc) in developing countries [46].
However, and despite the implementation of national regulations to fortification of foods in some 29 African countries and in other continents, foisted by corporate-led premix suppliers, and not backed by adequate dietary indigenous studies, the procedure has been conducted without the necessary pre-evaluation on the composition of local native foodstuffs, plants, and type of diets, gut microbiota profile, specific for each regional location.
This development aid/assistance obviously covers the economic interests of these “non-profit” organizations, which reap direct or indirectly colossal benefits, with no follow-ups on the outcomes of such programmes or the design of guidelines for effective intervention public health strategies [47].
Nevertheless, despite the lack of adequate epidemiological studies for each region or population, it is commonly generalized that there are deficiencies in micronutrients such as iodine, iron, zinc, and vitamin A. These are usually diagnosed by specific symptoms in ambulatory clinic and are common in developing countries, compromising the physical health and cognitive abilities of millions of people [48].
However, in SSA countries dietary assessment, necessary to ensure adequate complementary nutrition and hydration intake has been absent, therefore food fortification has been conducted on a bemused manner, with good intention. After more than three decades of implementation, the science underpinning the policy for micronutrients addition to foods continues to evolve, but in SSA in our view, there is the need for a more flexible framework.
We have enhanced that nutrient requirement values are just guidelines and not fixed figures [49], and it must be noted that the micronutrient balance is determined by complex mechanisms, including in the past not taken into account, gut microbiota modulation specific for different populations [50], and micronutrient deficiency measured by just serum/plasma levels, is not adequate when utterly associated with dietary inadequacy, varying according to individual and community characteristics [51,52].
In Africa, the justification of soil overuse for fortifying staple foods is not acceptable neither evident, and degradation and restoration is not the main cause, although deforestation may be a cause in some occasions. Forests, or better, large trees, are continuously destroyed on the search for energy as firewood, and namely timber sales to developed countries, causing increased environmental damage and soil erosion [53].
Despite the poor definition of agricultural sustainable intensification [54], at all situations, novel approaches and practices to sustainable agriculture in different regional models, are required in order to apply innovative technologies and principles, namely in heterogeneous and marginal lands [55].
Sustainable food systems for food security in SSA needs combining local and global approaches, considering the links between food security, access to land and natural resources at the local level, handling of losses and wastes, flexible food value chains, while observing the unpredictability and risk in markets and in the supply chain [56].
4. Micronutrient Deficiencies
The reality is that most African countries lack adequate evidence of the populations’ nutritional status, knowledge of the population consumption patterns, adequate laboratory facilities and trained staff for micronutrient evaluation, permanently facing the challenge of determination of the levels of nutrients’ deficiency and the need for supplementation.
The “big 4” principal micronutrient deficiencies of public health concern in SSA include: vitamin A, iron, iodine, and zinc. But many questions can be raised. The question is if this is true and applies for these micronutrients? Another posed question refers to the place of evaluation and the laboratories involved, local or not. Just by deficiency symptoms or clinical observation? Another challenge rises by the nutrient interactions and the hidden commercial interests behind these statements. Is the claim correct regarding support of FAO or WHO? Another question is related to the pressures exerted from multinational mega enterprises and “non-profit” NGOs on national governments.
Multiple vitamins and minerals status is rarely measured in rural and semi urban areas of SSA, even in group risks such as pregnant women. In a semi-urban area of Ghana, the relatively low prevalence of individual micronutrient deficiencies and the micronutrient status were not related to common blood-based health biomarkers, leading to co-occurring and overlapping of multiple deficiencies [57].
Since diet-related micronutrient deficiencies are concurrent with multiple micronutrients, food and beverages fortified with single micronutrients have been considered frail since only coordinated multi-micronutrient programmes may combat the co-existing deficiencies [58]. However, since the status of the general and high-risk populations are not monitored on a regular basis, eventual deficiency diagnosis is not normally diagnosed in the SSA communities, but it is compelled by the hundreds of organizations supplying nutritional indications or means of fortification, the most prominent “non-profit” having strong links to premix megacorporation producers [59].
Fortification of staple foods such as rice, maize and wheat flour in SSA has been reported as a strategy for combating micronutrient malnutrition [60,61]. Moreover, commercial compulsory food fortification has been small-scale in SSA and other developing regions [62,63] due to socioeconomic factors hindering the practice and the cost of commercial fortified food products and official control of the programme. In addition, the choice of delivery vehicle may affect the bioavailability of the micronutrients in fortified foods [64].
Since the causes of malnutrition are many, the silent hunger of micronutrient deficiencies continues, based on diverse and interrelated political, social, cultural or economic factors, education status of the population, season and climatic changes, urbanization, family disunity, alcohol intake, prevalence of infectious diseases and the effectiveness of nutrition programmes [65], the evident question being how a food fortification system may solve the set of these problems [66].
Obese individuals show a higher prevalence of micronutrient deficiencies compared to normal-weight people [67], despite them eating more to satisfy their nutritional requirements. In countries where overweight and obese prevail as a malnutrition manifestation, there is no enforcement of food fortification, but it is globally an ongoing debate [68].
In most of SSA, the age of the child strongly correlates with increased levels of malnutrition. New-borns in many African households live in an unhealthy environment and, in many cases, receive suboptimal feeding, that is, lack of exclusive breastfeeding and inappropriate or untimely complementary feeding leading to the decline in nutritional status from birth [69]. The first year of life shows a growth retardation and is considered very difficult to overcome in the later years of childhood. But there is no substantial long-term evidence if this is true [70].
Fortification is considered one of the most cost-effective interventions that subsist to address micronutrient malnutrition (Table 1). While in South Africa’s food and beverage vitamin fortified and mineral enriched market is pulverized, dynamic and fierce in nature, having a large number of national and megacorporation stakeholders striving to capture a significant share and competing for market quota, this however may not be replicated in most other SSA countries in the same manner [71].
African communities consume diets with low content of animal products and a high consumption of vegetables and cereal crops rich in phytates, which may induce zinc deficiency [72].
Therefore, compulsory food fortification is debatable and should not be uniform in SSA, where indigenous foods’ composition and gut microbiota studies were never or rarely conducted, absolutely necessary for adequate assessment of micronutrient requirements. This has raised the question if food and beverage fortification in Africa is based on science or business, or both [73].
Available data concerning malnutrition in Africa derives mainly from international organizations that calculate data, rather than being determined by national observations or statistics. Locally conducted nutritional trials are practically inexistent, so malnutrition levels are inferred indirectly from agriculture production, foodstuff imports and from consumption based on population numbers [74].
Other “sophisticated” complex assessment includes the computation of customary dietary crude energy intake levels (Kcal/person/day) for the average individual, the probability distribution and modelling of a parametric probability. The precision of the estimates is considered generally low due to the probabilistic nature of the inference and the margins of uncertainty associated with the variables in the model [14].
Even FAO bases their data by comparing estimated dietary energy intake with average energy requirement standards, to measure food deprivation and undernutrition. However, this factorial methodology estimates the population means or totals on energy requirements, but does not take into account micronutrients, and the actual individual requirements, at different physiological stages, which is unknown [75].
Furthermore, this may not reflect the African picture adequately, and awareness must be evidence-based and built on data that accurately and completely captures the occurrence, causes, prevention, and treatment of malnutrition in all African sub-populations [76]. These data are critical for researchers, clinicians, non-governmental organizations, ministries of health and other policy makers to prioritize efforts that address SSA’s malnutrition burden. Furthermore, it is important that all stakeholders, are represented in data collection and application, taking into account the effect of ecological area into the dietary patterns of the African community, and the specificities and food habits of each region [77].
Sustainability in health can be achieved with maximization of the connections between ecological systems and food systems, hygiene-sanitation, food security, and safekeeping. None of these is sufficient by itself, and all are necessary for high quality human development [78].
5. The “Big Four” Micronutrients
Daily Reference Intakes (DRIs) for most micronutrients (vitamins and trace elements), have been established in the USA by the federal government’s 2020–2025 Dietary Guidelines for Americans [79], but not in SSA, where WHO guidelines are followed [59,80].
It must be emphasized that some of these micronutrients may interact with bioactive food components capable of forming insoluble complexes (e.g. phytates) and medications [81].
5.1. Iodine
Globally some 2 billion individuals have insufficient intake of iodine, and around 50% of the adult population in Western developed countries are iodine-deficient. Iodine in the thyroid gland participates in a complex series of reactions to produce thyroid hormones. The average adult only needs some 150-250 μg/day, which can be supplied by less than half of a teaspoon of iodized salt. Nevertheless, about half of the manufacturers of salt no longer add iodine to their product, because foods from other regions (e.g. of marine origin) have high natural iodine levels and sourcing them has essentially eliminated the problems [82].
5.2. Vitamin A
A review suggests that fortifying staple foods with vitamin A may make little or no difference to the serum retinol levels, a biomarker of vitamin A status. Another case to examine would be serum/plasma retinol of 70 μmol/L or less defined as subclinical vitamin A deficiency. No difference would be made there too. It is not very clear whether reduction of clinical vitamin-A deficiency can be achieved with this fortification [83].
Animal livers encloses large amounts of vitamin A, followed by alternative origins such as meats, eggs and some fish [84]. Consumption of 100 g of orange flesh sweet potatoes will provide 50 µg of Vitamin A [85]. Recommended Dietary Allowances (RDAs) for Vitamin A have been well established for different physiological stages and ages [86]. It must be enhanced that a high consumption of vitamin A, leading to hypervitaminosis, has been considered to cause a number of adverse effects and even appears to be teratogen [87].
Utilization of orange flesh sweet potatoes (Ipomoea batatas) appears as a source of vitamin A along with β-carotenes being labelled in African products as beneficial [88]. Nevertheless, most SSA populations have access to vitamin A, via organ meats that contain a higher percentage of vitamin A than orange pulp sweet potatoes [89], and rich plant sources (e.g. chili and red peppers, papaya, loquat, mango) of β-cryptoxanthin or its esters [90].
Therefore, the poor vitamin A status varies a lot across SSA countries in children 2-5 years old, averaging 42%, and supplementation needs to take this into account with adequate diagnosis, since large doses of vitamin A can cause liver damage [91]. However, addition of vitamin A alone to the staple foods might show little or no effect on vitamin A status or deficiency. Comparison of staple foods fortified with vitamin A versus no intervention has been evident in very few or no studies [83].
It must also be noted, before fortification, that low levels of plasma concentration of vitamin A may be also related with onchocerciasis (“river blindness”), a parasitic worm infection transmitted by flies, affecting millions of people in the endemic regions of SSA, and often control programmes integrates vitamin A supplementation with ivermectin treatment [92].
Provision of staple foods fortified with vitamin A plus other micronutrients, does not necessarily increase serum retinol concentration but apparently lowers the risk of subclinical vitamin A deficiency compared to unfortified foods [83].
A comparison of RAE (retinol activity equivalent) among different food sources is shown in Table 2.
5.3. Zinc
It is easy to get enough zinc from a healthy diet. Zinc, an important cofactor in the body and naturally present in some foods (e.g. oysters, red meat and poultry, fish, seafood, beans, peanuts, cashew nuts, and whole grains), is involved in cellular metabolism, namely for the catalytic activity of hundreds of enzymes, playing a role in enhancing immune function, protein and DNA synthesis, wound healing, and cell signaling and division.
Therefore, it is difficult to assess accurately zinc insufficiency or excess [81,93], and successful zinc fortification strategies should consider the impact on zinc bioavailability on the whole diet due to the impact of phytate and protein on zinc absorption. The recommended dietary allowance is 11 mg for men and 8 mg for women. Taking daily high amounts for long periods have been connected with aggressive prostate cancer, warranting precaution of excessive usage of zinc among adult men [94].
Zinc can decrease the effectiveness of antibiotics (e.g., ciprofloxacin, tetracycline), antirheumatic drug penicillamine, and blood pressure drugs, so mass fortification usually does not take this into account [95]. Considering the possible toxicity of high dietary intake of zinc, its load and source should be taken into consideration prior to fortification.
5.4. Iron
Haem iron is found in meat, poultry, and fish, while non-haem iron is identified in plants, eggs, and nuts. Chronic iron deficiency is the world’s most prevailing mineral deficiency and is the most common cause of anaemia among an estimated 2 billion people worldwide [96]. Adults should not take any more than 45 mg of iron a day as it can be harmful, since an iron overdose can be toxic causing organ damage [97]. The generally recommended dose of ferrous sulfate for children is 3 mg/kg of iron once or twice daily (maximum total daily dose, 150 mg of elemental iron) [98].
Biofortification is based on plant breeding to improve the nutritional quality of food by increasing the nutrient content and availability [99]. This approach has proven to have better iron accessibility and bioavailability than fortification, being inexpensive, sustainable and efficient in providing micronutrients for poor populations, complementing conventional interventions [100]. Biofortification also involves the use of biotechnological techniques (e.g. genetic modifications) with transgenic and breeding techniques being employed for the biofortification of cassava, banana and cauliflower, and banana [101,102].
Food-to-food fortification (FtFF) is another strategy being involved for promotion of the bioavailability of essential micronutrients. This is done by increasing the content of micronutrients and enhancers of their absorption and decreasing the levels of inhibitors of micronutrient bioavailability [103]. Improvement of iron and zinc bioaccessibility in pearl millet has been carried out with FtFF with moringa leaves and baobab fruit pulp [104]. Same for maize [105]. Similarly, for sorghum-based foods where extrusion cooking helped alleviate iron deficiency by reducing the content of anti-nutrients [106]. Iron levels in African foods are described in Table 3.
6. The Link Poverty, Food Insecurity, and Malnutrition
A reciprocal connection exists between poor nutrition and poverty, creating a vicious cycle with each fueling the other, both serving as the cause and consequence of each other. Undernutrition produces conditions of poverty by reducing the economic potential of the population and likewise, poverty reinforces malnutrition by increasing the risk of food insecurity [107].
Despite the general claims of the United Nations that an increase in extreme rural poverty in developing countries, is totally linked to the global food insecurity crisis [108], in SSA countries action plans have been approved for family subsistence farming, which have strengthened their resilience and provided effective solutions to deal with the emerging needs of agro food systems, leveraging local and regional cooperation to accelerate inclusive development and reduce poverty [109].
Ending world absolute poverty is an illogical goal, and the chances of ending poverty entirely are zero. But a sustained poverty reduction is a key concern of all those interested in the development of poor countries. Poverty, no matter how defined (there is no universal definition), is a relative concept, with its multidimensionality, requiring different policies for poverty reduction, since it is not confined to material aspects of life, and include social, cultural and political aspects [110].
Solving poverty grounded solely on economic strategies is not realistic, as it involves a holistic attention on a set of harmonized initiatives and all-round economic recovery, necessary to increase wages and consumption. Indeed, despite the good economic development in several SSA countries, poverty and hunger continue to persist (Figure 2).
6.1. Mother-Child Malnutrition in SSA
The initiation of breastfeeding within 1 hour of birth, exclusive breastfeeding for the first 6 months, is the best way to give infants the nutrition they need [111], and in order to try and overcome micronutrient deficiencies and coexisting complications in < 2 years of age children, food and beverage fortification schemes have been implemented in several SSA countries, together with a continuation of breastfeeding for up to 2 years of age or beyond [112].
Fortification feeding practices revealed a noticeable beneficial effect on the continuous growth of a child within the first 2 years of life, however, with no evident direct demonstration cause-effect relationship between fortification and growth [113].
Child malnutrition is affected by several determinants, such as intrauterine growth restriction, lack of exclusive breastfeeding, inappropriate complementary feeding, and the recurrence of infectious illnesses, food scarcity, and micronutrient deficiencies [114,115].
The most commonly employed indicators of child malnutrition in Africa have been the anthropometric measures of child nutritional status (stunting, underweight and wasting). However, the most used indicator, the body mass index (BMI), dating back nearly 2 centuries, is considered unsound, basic, obsolete, overrated, and inaccurate measure of body fat content and does not take into account muscle mass, bone density, overall body composition, and racial and sex differences, and can result in missed diagnoses [116].
Fortification of maize meal and wheat flour involved in bread production, is mandatory, and commercial infant products are widely available in several SSA countries [61,117], This practice of complementary feeding practices of young children has its risks since excessive intakes may remain unacceptable. This child survival strategy for developmental outcomes shows unclear benefits [118,119].
The poor health and nutrition of the mother leads to low birth weight reflecting foetal growth retardation, and also serves as an indicator of the risk of infant mortality and future poor health [120]. The burden of undernutrition through life cycle and across generations and the persistent transmission of poverty trauma within African communities, remains unacceptably high and is a critical measure [107,121].
7. Alternatives to Food Fortification
While fortification is considered a successful short to medium-term strategy to tackle nutritional risk in endangered communities in some frameworks, dietary diversification, on the other hand, rather challenging to implement, is a sharper and sustainable way to overcome micronutrient deficiencies, with long-term benefits, besides nutritional, with provision of ecosystem resilience [29].
Being originated in the region, indigenous foods are by far superior than introduced exotic foods, are culturally acceptable, adapted to local climatic conditions, having been consumed traditionally for generations [122]. Reintroducing and scaling up neglected crops can be a sustainable food and climate-smart solution for SSA, by building local and regional markets with public incentives and investments, including in infrastructure development, regulations, and subsidies [123].
As another alternative to individual food fortification, the latest evidence shows that small-quantity (ca. 20 g/sachet) lipid-based nutrient supplements (SQ-LNS) for young children (6–23 months of age) significantly reduce child mortality, stunting, wasting, anaemia and adverse developmental outcomes, and it is considered more cost-effective than other options such as micronutrient supplementation or the provision of complementary food [124,125,126].
SQ-LNS usually include ω-3 fatty acid-rich vegetable oil (e.g., canola/rapeseed or soybean oil), legumes (e.g., peanut, chickpea, lentil, and/or soy), milk powder and a small amount of sugar (for palatability). In addition, the formulation is fortified with 23 vitamins and minerals, including micronutrients (e.g., vitamin A, B vitamins, iron) and macrominerals (e.g., calcium, potassium, phosphorus, and magnesium) [127].
Therefore, the question remains if present programmes, donations, charity aid foundations, alliances on food and beverage fortification, frequently supported by well-known international premix producers, NGOs and national regulations, towards supposedly tackling the malnutrition burden in SSA countries, will contribute towards reduction of malnutrition or affect child malnutrition, reflected in general public health.
One Health is a collaborative, multi-sectorial, and trans-disciplinary approach towards achieving optimal public health outcomes, demanding surveillance, prevention, and mitigation, including water and food security/safety, socioeconomic and cultural factors, which is influenced by food fortification. (Figure 3) [128].
8. Some Challenges in Sub-Saharan Africa
SSA food systems supply most of the food for its growing population (1.2 billion), and reveal some regions with high levels of resilience, others with significant vulnerabilities to specific shocks, depending on global markets and export-oriented cash crops (e.g. cotton, cacao, tea, and palm oil).
Bringing back neglected crops (e.g. sorghum and millet; kale, eggplant; algae), displaced by crops better suited to commercial farming, is important to increase the number of food options and diversifying markets, while building resilience to climate changes. For example, finger millet (Eleusine coracana), fonio (Digitaria exilis), and teff (Eragrostis teff), have higher iron contents than maize, rice, and wheat [129].
Despite many attempts by multiple NGOs striving to sustain positive outcomes, by building local resources and capacity, assisting attitude changes, and strengthening the enabling environment to save lives, improve health, build resilience, increase economic productivity, and advance development [130], the fact is SSA family-based agriculture small-scale food chains’ actors, and small millers, do not have the regular access to funding and production inputs, to attend the present mandatory legislation and prohibitive costs of premixes, technological demands, and staff training [131].
The Gates Foundation has been supporting large-scale food and certain vehicles of fortification programmes in some 29 countries in Africa since 2008, through grants to the GAIN-Global Alliance for Improved Nutrition, and UNICEF [132]. Although the African Union declared 2022 as its “Year of Nutrition”, many questions remains as to whether national statistics are reliable enough to enable proper decision-making on food and beverage fortification, and how to implement the compliance to standards among the millers and suppliers of premixes in SSA [132].
Most SSA countries, unseen in developed countries, have produced harsh legislation for food processors and millers, on compulsory fortification of maize, wheat, cooking oil, sugar, and salt, initiatives propelled by foreign pressures and national lawyers’ offices, for business purposes, but with no scientific support on assessments of African foods [133].
Another significant and ignored question is the potential socioeconomic effects concerning the risk of competition between large-scale, small-scale processors, and possible adverse effects on the sustainability of poor smallholder family farmers and communities [134].
There is still the question whether and how the mechanisms of mixing foods and delivery of premix supplementation and vehicles can benefit/jeopardize domestic food chains family producers and generate overall socioeconomic development locally [135].
Food-based strategies to combat micronutrient deficiencies have been absent which does not sustainably solve the micronutrient deficiencies but enriches few actors. Enforcement for fortification should focus on the origin of bulk items by large-scale producers and never the small miller [136]. Present foreign aid and other support does not reach directly the small producer and is used to cover the premix costs and the unnecessary national committees coordinating and monitoring the fortification activity, under high fines by national authorities to the non-compliant.
Fortification could be an effective medium-term strategy to tackle nutritional risk in vulnerable populations in some contexts, but after more several decades experience, it can be seen to have carried negative environmental, economic, and social impacts [137]. Dietary diversification, on the contrary, is known to be a sustainable way to overcome micronutrient deficiencies, bringing long-term benefits, including nutritional, and provision of ecosystem services [138].
Nutrition performance needs to be linked with sustainable agricultural systems, thus strengthening the agro-biodiversity of resilient cropping systems. This would enable the strengthening of the link between agro-biodiversity, aquaculture systems, and food diversity [139].
In the framework of the SDGs, the EU–Africa RI Strategic Partnership on FNSSA proposals describe how projects can contribute to sustainable, healthy African diets.
The research, innovation and action EU project InnoFoodAfrica (2023) focuses on nutrition, with the aim to improve the nutrition and well-being of African people via the analysis of diets. A survey was conducted on Sub-Saharan diets with the example of aquaculture and fishery industries managed in Africa hence guaranteeing food security and economic growth [140,141,142,143].
8.1. The Global Supply and Use od Premix
The social injustice behind our food systems, from growing and harvesting to procurement is serious and lasting. Basically, the United Nations FAO, the hundreds of nutritional aid/assistance organizations, and even SSA governments, have been subject of a “corporate capture” of the global and national food and nutrition policy spaces, where under nutrition has been separated from its social, public health, economic, political and cultural causes, not addressing the basic questions [42].
This may be exemplified by the failure of the “Green Revolution”, sought to halve hunger in 20 African nations and double the income and yields of over 30 million small-scale farmers by 2020. However, instead of delivering on its promises, it appears that hunger has actually escalated by 30% in these countries [144].
The pharmaceutical industry, because of possible hazard to a patient’s life, is the industry more highly regulated in the world, however, vitamins and trace element premixes to include in diets are not included in this scrutiny [145]. The role of a premix producer may be simple mixing, pelleting, microencapsulation, delivery, or some other form of activity before delivering the final form of the product to the manufacturer or brand owner.
An example of wheat flour fortified with folic acid shows the interpretation of the “minimum” content as the average of addition by the industry. The problem arises from the premix formulation because the instructions of addition are being followed by the millers from what they receive from the manufacturers. Hence, misinterpreting the minimum content as the average content, the program delivers half the amount of folic acid that it is planned to be provided [146].
In Chile there is variation of fortification and more than 50% of samples were either below or above the regulatory range. In the US an average of 100 μg/day of folic acid was provided with a minimum content of 1.4 mg/kg for cereal flours [146]. Hence, this content was selected as a basis for attaining benefits for those in need without potentially risking the excess intakes that may go beyond the UL [147].
Most SSA governments have produced food fortification mandatory laws, without pilot studies, in partnership with external “non-profit” groups, clearly associated with the premix industry, with no precautionary principles such as caution against consuming iron-fortified food by patients with thalassemia and sickle cell anaemia [148].
There is a clear global need for a new intervention framework, very difficult to achieve due to market cartels, presently governed by huge corporations some even in the past guilty to participation in a worldwide conspiracy to raise and fix prices for vitamins [149].
The Dutch DSM Nutritional Products, the world’s largest supplier of vitamins, carotenoids and other biochemical products, having acquired Swiss Roche Vitamins, is the main world manufacturer of nutritional and pharma ingredients. For enzymes and trace minerals, Cargill, Incorporated (U.S.), ADM (U.S.), BASF SE (Germany), Bluestar Adisseo Co., Ltd (China), Unilever, and many others, are in control of markets. Several “non-profit” organizations in SSA have present or past commercial links with some [150,151].
Umbrella-groups or coalition of NGOs, significant international consortium partners since 2002, GAIN-Global Alliance for Improved Nutrition, and FFI-Food Fortification Initiative, public-, private-, and civic-sector partnerships, are referred to as lobby groups for vitamins, minerals, and nutraceuticals, operating its own premix facilities to produce and supply fortified foods to SSA markets [152].
It must be noted that the WHO-World Health Organisation’s standing committee on Nongovernmental organisations (NGOs) deferred the accreditation of Swiss based GAIN as an NGO raising the issue of conflict of interest in NGOs’ ties with businesses. GAIN’s vision is tied to fortifying food with “missing nutrients” with the help of global food companies and selling it to people ‘at low cost’.
Based on publicly available information, national regulatory bodies include private advantages from corporate actors, many domestic and international NGOs functioning as pressure groups, some with predatory tactics to advocate for fortification-friendly policies in SSA, and other parts of the world, with national authorities not preventing this conflict of interest [153].
Although there is no recommended daily intake figure, FDA and EFSA suggests guidelines of tolerable upper intake levels for vitamins and minerals considered to be both safe and sufficient [154].
The global food premix market is a massive business valued at $ 6.31 billion US$ in 2023, and estimated at 10.7 billion US$ by 2029, and projected to consistently increase. The global animal feed premix market, segmented into amino acids, vitamins, minerals, antibiotics, antioxidants, blends, and others, is even higher and expected to reach 33 billion US$ in 2025, to maintain global sustainability of livestock, poultry, and fish production [155].
While in intensive animal production systems the need for premixes is easier to calculate through feed conversion efficiency data, in humans there is no single best test to evaluate nutritional status and nutritional requirements of healthy individuals depend on various factors, such as type of diets, age, sex, and activity [156]. Furthermore, to date, there is no precise data on requirements of most micronutrient for individuals or communities, and recommended values of dietary intakes strongly vary for each group of individuals [49].
Large-scale food fortification programmes face one of the most significant recurring input costs and that is vitamin and mineral premix. Despite some noteworthy innovative approaches for improving access to quality vitamin and mineral premix in fortification initiatives [157], a number of barriers persist in SSA to search for adequate quality premix, accessing suppliers, due to volatile premix prices, lack of national quality assurance and monitoring of delivered products, and absence of funds to purchase them.
Instead of pushing mandatory food fortification of doubtful benefit and potential harm, and insisting on unsustainable, uncertain, and expensive procedure of large scale mass food fortification, there is the need to launch a major awareness campaign to improve the SSA food and nutrition security, by replacing of refined, mostly imported, wheat for pleasant bread products, shifting to a more realistic nutritionally balanced diets, increasing economic revenues and equitable benefits, and improving sustainability and resilience of the SSA food system [158].
The difference in food preferences and their content in micronutrients are often not taken into account to measure undernourishment of SSA populations. Presently, only limited food availability data (estimates for few commodities) exist, from production and trade, using consumption levels across the populations. This is the basis to unfairly estimate what proportion of the SSA communities is unable to meet their daily nutrient requirements [159].
Although these assessments are in essence inaccurate and vague, with many valid criticisms against them, in the absence of better indicators they are used extensively to monitor food security status [160]. Only local studies based either on real food analyses and traditional behaviour may provide genuine data. Lack of knowledge of foreign experts on the use of traditional foods, herbs, condiments, and medicinal plants, and estimation methods leads to overestimation of malnutrition percentage levels in SSA [161]. For instance, estimates of the undernutrition prevalence, namely in pregnant women, could vary a lot and range between 5–18% and 14–48% for the same populations, as reported in different studies [162].
These developments helped the further ‘medicalization’ of nutrition, which presented donor agencies with simplistic, ‘magic bullet’ product-based solutions, such as food fortification, to malnutrition [163].
Another claim is that growth retardation experienced in the first year of life is very difficult to overcome in the later years of childhood. The fact that an individual child has a short stature, falls below the 5th percentile on a growth reference curve may reflect normal variation in growth within a population. An individual child may be short simply because both parents carried genes for tininess and not by virtue of deficient nutrition [164,165].
The SSA countries with the largest frequency of impaired growth and development is found in south eastern regions, reflecting a complex set of challenges that include civil conflict, economic downturns, commodity price shocks, and droughts and floods, or the legacies of such events [159].
It is important to observe that food production is not the limiting element in many of these hunger hotspots of malnutrition, and a multiplicity of factors, including socio-cultural perspectives, are deeply involved, and there has been an unfair access to food. [166].
Unsuitably, SSA governments are often presented by the United Nations and premix manufacturers with an imaginary consensus on the way to solve malnutrition that emphasizes the role of the private sector and the need to include fortification of food in policy formulation.
9. Fortification Strategies
Food fortification is not philanthropic or charitable and involves overall heavy costs, and can assume various shapes, and three different forms may be accepted: a) Mass fortification consists of the incorporation of micronutrients to edible products routinely ingested by consumers, such as cereals, oils and vegetable fats, milk, sugar, and condiments [167]; b) Targeted fortification is the process of adding a large amount of micronutrients to foodstuffs for abundance of the daily requirements designed for specific population subgroups, e.g. complementary foods for infants, for school feeding programmes, and those for crisis circumstances [168]; and c) Market-driven fortification is the process by which a food manufacturer intentionally decides to add one or more micronutrients to processed foods, with the purpose of attracting consumers and increasing sales [169].
Fortification practices and rules, now embedded in public food schemes, are different for each type of food fortification. Food fortification can be a useful tool in combatting micronutrient deficiencies. Its effectiveness depends on the skill and experience with which it is applied. Countries often face the challenge of determining which levels of nutrients are both efficacious and safe for the population at large. WHO’s updated guidelines for maize flour and corn meal fortification include some 10 micronutrients, but for iron, zinc and vitamin B12, less than 50% of the standards were met by the countries [170].
The lack of an overall programme design, the prohibitive cost of the fortified foods’ system, technological demands, monitoring and evaluation difficulties, need to ensure that fortified foods are consumed in adequate amounts, and ethical concerns, impede the widespread adoption and effectiveness of this strategy in SSA. It is not a properly designed tool in all situations and needs to be combined with other techniques in order to obtain the optimal result, therefore its use in SSA is debatable [171].
It is critical to identify all factors involved in any given nutritional problem: food insecurity, inadequate dietary diversity, lack of nutrition education and the state of local food processing, are among the most significant factors adopted for determination of the most appropriate strategy [172].
There are different considerations involved in the establishment of food fortification programmes in developing countries as opposed to developed ones. The standards for fortified foods were published for example in India [173] but such guidelines for Africa are difficult to implement such as for example the provisions for the reference of the purity criteria of micronutrients. The identified vehicle must be consumed in roughly constant quantities throughout the year by the majority of the population, which is hard to achieve in SSA. Again, the facilitation of a rigidly controlled fortification process, requires that the fortified food passes through a central point. Finally, acceptable ranges of fortification must be defined, but facilities are not readily available in SSA.
Furthermore, the provision of the micronutrients to those people who need the intervention, must be determined while avoiding imbalanced or excessive intakes for other groups. The distribution of nutritional requirements and susceptibility to toxicity determine this risk/benefit calculation and it seems that neither has been determined for most of the micronutrients [174].
Indeed, consumers in developed countries seek foods that promise health benefits, and industry is providing just that and more [175]. But this scenario is not yet valid for most SSA countries, where subsistence rural farmers prevail, and food purchases are not yet influenced by a health concern, such as managing fat and cholesterol, salt and sugar, reducing risk of a disease, defying the aging process, or following doctor’s orders. In reality, some 80% of the SSA population attend traditional doctors and access to imported pharmaceuticals in Africa faces numerous challenges [176,177].
A notable disparity persists between rural and urban areas and indeed, food with a future will require that everyone should have access to a healthy and ecologically sustainable diet, issues still not a reality for all in SSA [178,179].
The marketing of fortified food products can be quite complex. The actual quantity of fortificants added to foods is another issue. Folic acid is a good case in point, since wheat flour contains folate but not folic acid, and it must be provided in effective amounts to women of childbearing age, without providing too much to the rest of the population. Hence there is a need to have the same food product fortified with different amounts of a fortificant for different categories of consumers [146].
Similarly, while general fortification of baby food is widely accepted as being an excellent way of adding micronutrients to their diet, it often cannot meet the growth and development needs of young children who ingest smaller amounts of foods and have higher micronutrient requirements. Hence there is a need to determine how to provide the necessary micronutrients to those people who need them, while avoiding imbalanced or excessive intakes for other groups [180].
The majority of infant weaning foods available do not provide the nutrient density and diversity of taste and texture needed in this formative stage. Furthermore children weaned on these products can develop unhealthy sweet tooth habits in the future, since 65% or more of these foods are sweetened [181].
Multinational firms have sometimes been responsible for health problems due to their fortified foods, for example, some consumers filed in 2017 a lawsuit against Nestlé USA, for their bottled common groundwater and illegally mislabelled “spring”, “purified”, “mineral”, “sparkling”, water fortified with fluoride [182]. Similarly there was a lawsuit against Gerber Products Company for their baby food and infant formula products fortified with fluoride [183].
In Nigeria, Nestlé introduced water enriched with zinc to overcome national deficiency of this mineral aiming at strengthening immunity [184,185], and Coca Cola released “vitaminwater®” with vitamins, electrolytes and new flavour variants [186]. The need and suitability of such fortified beverage products are questionable, since they are not based on accurate and reliable information regarding the dietary habits, nutrition requirements, and nutrition status of target populations in the concerned SSA countries.
The current levels of micronutrients added to maize meal and bread flour are considered unsatisfactory in South Africa. This is likely to be due to inadequate incorporation of premix at the mills. This affects the intake of the fortified product, and likely prevents the wanted reduction in micronutrient deficiencies anticipated from such a flour fortification programme [187,188].
Such a case study clearly indicates that there is a need to conduct large-scale studies on crop composition, and nutrient availability in the food matrix before creating dependence on imported micronutrient fortification, and to identify the right nutrients to be added to the right foods for populations most at risk for micronutrient deficiencies.
The FDA in the USA and EFSA in Europe, have always been against the practice of adding nutrients to “junk foods” just to make them seem healthy. But this does not stop food manufacturers, especially soft drink and juice manufacturers, from trying.
Some authors go as far as even suggesting a role of soft drink industry in improving child health in SSA, advocating fortification of soft drinks with micronutrients. In fact, instead of suggesting public health measures to counter the well-documented effects of soft drinks on rising rates of obesity or on tooth decay rates among children in developing countries, the authors propose that soft drink companies add vitamins and minerals to their drinks [189].
The Bill Gates Foundation partnered with Coca-Cola in Uganda and Kenya to increase production and distribution of mango and passion fruit juices as a way to stimulate production of these fruits and use in Coca-Cola’s locally produced and sold fruit juices. Such a win-win partnership would also involve micronutrient fortification, empowering small farmers to increase productivity, improve crop quality and access reliable markets critical to addressing global hunger and poverty [190].
The reality is that 3 out of 4 Americans do not consume the U.S. recommended daily allowance (RDA) for vitamins and nutrients [191]. So the question is how one can expect Africans to be much better, despite having SADC Minimum Standards for Food Fortification been developed to provide member states with guidance on micronutrient additions to staple foods and condiments within the region [192]. Indeed, for RDA to accurately assist heterogeneous populations, they must be more inclusive of cultural differences and honour social practices to improve diet and reduce disparities [193].
In South Africa, there is a process of mandatory fortification (e.g. wheat, maize) which has been efficiently and effectively managed, supported by adequate monitoring and evaluation, food regulations, labelling and quality assurance. However, these procedures are not easy to implement in most of the other SSA countries [188]. Regarding cooking oil, some oil producers fortify on a voluntary basis, namely in Kenya since 2012 [194,195].
While whole Africa has 30 countries with mandatory wheat flour legislation, the Americas (North and South) have 35 countries with mandatory legislation for wheat. For salt, Africa as a whole has 45, Asia 35, while Americas 21 countries with mandatory legislation [196].
It is evident that nutritional fortification of foods has been very effective in the past, at least immediately, in eliminating widespread nutritional deficiencies in developed countries. As consumer health awareness and scientific knowledge increase, there is a great need for the fortification policies to be re-evaluated.
Furthermore, the amount of ingredients and nutraceuticals, such as ω-3 fatty acids, are not regulated, meaning that not only do consumers misperceive how much they should ingest, but manufacturers are not required to disclose how much or how little they are adding in their foods. Fortification has been portrayed as a silver bullet solution without considering critical perspectives and evidence, while private interests have been housed within national and international regulatory bodies.
Just because a food product is fortified does not mean it is healthy, and there are some limitations to this strategy. Fortified foods are usually heavily processed, and some micronutrients are sensitive to temperature, light or oxygen, and get degraded when exposed or processed. The protection by micro encapsulation methods may not work for all micronutrients namely ω-3 oils, quite easily degraded by oxidation [197].
Fortified foods interventions to reduce low birth weight and to improve infant and child malnutrition were ranked only as “fair” [198]. Poor rural SSA populations have restricted access to fortified foods in the open markets due to low purchasing power and an immature distribution channel.
In fact, SSA populations eat regularly more native maize-based foods, vegetables, cassava leaves, yams, herbs, spices, condiments, and tropical fruits, than the 70% of Americans, at the root of the obesity epidemic and many of its associated diseases, who consume processed cereals, drink soda daily, with meat rich diets, too low in vegetables, fruit, and dairy, falling short of meeting the dietary guidelines recommendations, and where fortification started [199].
All trace elements are toxic if consumed at sufficiently high levels for long enough periods. The art of premix consists in mixing all these ingredients homogeneously and to limit the interactions, selecting carefully the raw materials. As the current literature on the stability of vitamins in vitamin premixes and vitamin/trace mineral premixes is limited [200], millers and premix suppliers tend to often add vitamins at dangerous levels, up to 100% of the recommended daily allowance in a single serving, possibly causing to exceed the limit. In fact, fortification and enrichment of food products are not as innocent as they seem, since long term health consequences of vitamins consumption are unknown [201].
Although fortification may increase the intake of vitamins and minerals, there is little evidence to suggest that adding nutrients (other than folic acid) may improve health [202]. Several experimental plans are available to reduce micronutrient deficiencies, but uncoordinated implementation of multiple interventions may result in excessive intakes [203].
In fact, there are growing concerns that fortifying and enriching foods may be harmful [204], and vitamin A was even suggested to be excluded from multivitamin supplements and food fortificants [205,206].
Supplements added to foods, even if consumed consistently, reveal less bioavailability, although these studies are complex since present methods do not allow to distinguish nutrients in the experimental diet from endogenous nutrients present in the body [207]. The immune system incorporates many organs and biological functions, and the so called “boost your immune system” with micronutrients makes very little scientific sense [208].
Fortified foods are more likely to spoil than are unfortified foods, and the addition of micronutrients creates an osmotic environment suitable for a wide range of microbiota, shaping the structure, composition, and function of the gut microbiome [209,210].
A major shift in our perception of food, agriculture and nutrition is taking place in this era of globalisation. Therefore, the high prevalence of malnutrition has become a good market for industrially produced food, which is technically designed for the corporate sector rather than farming communities [211].
The critics of mandatory food fortification call it out as ineffective, wasteful and coercive. There is no evidence, that it reduces the structural causes of micronutrients deficiencies and food insecurity. A mandatory policy, and scaling it up without adequate infrastructure and quality control, has concerning implications for the health and safety of vulnerable populations [212].
High level of commitment is required from government agencies and food producers, and extensive data necessary for effective programme design and monitoring, and financial and infrastructure requirements for implementation of food fortification in SSA.
10. Other Strategies or Vehicles for Fortification
Bouillon cubes constitute a vehicle for fortification to overcome micronutrient deficiencies in Sub-Saharan Africa providing flavor enhancement to savory foods. However, they possess a high sodium content, being a risk factor for hypertension and cardiovascular disease (CVD) [213]. Several multinational food companies are involved in the African bouillon market including Maggi (Nestle), Knorr/Royco (Unilever), and Jumbo (GB Foods) [214].
Unilever favours salt reduction having set benchmarks for sodium levels for different product groups. Formulation/modelling of benchmarks has been based on a total diet approach considering the contribution of the product group to overall daily salt intake [215,216].
Nestle’s Nutrition Profiling System (NNPS) has been developed for reformulation of their products [217,218].
Micronutrient fortified whole-grain maize meal (WGMM), in tropical Africa, employed in nutrition schemes and in packaged products [219], needs to have a long storage life due to challenges in distribution to rural areas. Hence, a thermal treatment is required to retard rancidity development in micronutrient fortified WGMM. Hot-air drying of maize grain to 11.6% moisture substantially retards rancidity development in fortified WGMM development as reported by Taylor et al. [220].
11. Policy Implications
It is largely unknown the nutritional composition of Sub-Saharan foods and dietary patterns based on intake of healthier foods and nutrients, where food cultures’ dynamics have not received much attention [221].
The notion of “healthy food” has become omnipresent in medical, political, and media debate as well as among lay population. Indeed, most foods are in fact neither healthy, nor unhealthy, but are just foods. Under the definition by WHO of a healthy diet [222], depending on individual characteristics, cultural context, local availability of food, climatic and ecological conditions, dietary customs and preferences, most Africans definitely enjoy better, less processed or unhealthy foods, exercise more and have poorer but healthier lifestyles than the average North American who eat unhealthy diets [223].
Nevertheless, the implementation of compulsory food fortification has been conducted almost exclusively to Africa, where mega entrepreneurs under several “initiatives” and “alliances” did not encounter a variety of scientific, technological, regulatory, and political barriers. In contrast, in Asian giants’ India and China, as in many developed countries, there has been general strong resistance to fortification.
Through advocacy and framing activities, out-of-Africa influential mega corporations producers of micronutrients, mostly leading to conflict of interests, exerted well documented policy interferences, even seeking to shape WHO policies, through non-profit organizations or public-private partnerships, by planning, implementing, but very few times evaluating the outcomes of fortification.
Fortification programmes encountered barriers associated to price, shops and bazaars, and compulsory large-scale fortification programmes normally has not been effective in delivering to the poorest due to imperfect food vehicle choices, the market partition characterized by the predominance of informal traditional trade as well as noncompliance by food and beverage manufacturing operations.
Lack of micronutrients can only be solved by dietary diversity and food fortification with single micronutrients is just a band aid solution. However, food fortification has been for decades largely a political public health intervention. Force balance between certain business interest- and public interest- non-government organisations, under the umbrella of interested global food regulatory system, have been exerting substantial influence over food fortification.
This article aimed at enhancing the fact that Sub-Saharan Africa national authorities were inveigled in many ways and unwarranted mandatory food fortification laws, rarely evaluated or considered on eventual occurring adverse impacts on health and livelihoods.
12. Prediction of Excessive Intake of Micronutrients
Some studies have shown opposite results regarding non-impact of food fortification programmes and guaranteeing safe upper limits [224].
Success in food fortification is ensured by establishing the micronutrients’ Tolerable Upper Intake Level (UL) [225]. The WHO proposed a methodology for calculation and definition of the safe upper limit in the Guidelines on Food Fortification with Micronutrients. However, large consumption of the fortified food among the same population and utilization of multiple food vehicles is a challenge [226]. In Cameroon, excess of UL among children was reported following consumption of multiple Vitamin A fortified vehicles such as sugar or wheat flour with edible oil [227,228].
A model has been based on the estimation of a Feasible Fortification Level (FFL), which then is used as a basis for determination of the average, minimum, and maximum contents of the nutrients during production, taking into account the acceptable variation of the fortification process [229].
The usefulness of the application of mathematical modelling for the determination of nutritional requirement levels and providing the basis for the rational formulation of complex mixtures of nutrients (diets) have been tested and developed to optimize accurate estimates for dietary nutrient levels, skipping human trials [230].
13. Concluding Remarks
Uncertainty encircling plausible fortuitous outcomes has led to apprehension, underlining the need to constantly monitor fortification programmes for well-aimed measures of their effect and the capacity to manage concerns as they arise.
SSA people ingest plant foods unknown by western caregiver’s supporters, and micronutrient interactions within different food matrix can impact absorption and bioavailability, and this should be a basic priority for an adequate fortification policy. The ongoing corporate capture of global nutrition business by hundreds of actors threatens the achievement of food sovereignty and the full emancipation of women in the SSA region, bringing industrialized food fortification that do not serve SSA public health goals. Most aid organizations often have multiple purposes, and alongside their public health objectives, they assist commercial companies in the creation of markets for their products.
Statutory food safety regulators in SSA countries have made fortification mandatory but failed to avoid conflict of interest and of blurring information. This opened up a new market for multinational premix companies and the large food industry, while doing little to address the crisis of chronic under-nourishment and nothing to support family farmers.
Presently in SSA, while trying to cover multiple nutrient interventions by different stakeholders, there is no effective surveillance or regular dietary surveys to help ensure these interventions achieve their objectives. Since the intervention of fortification is not being monitored for decades, no evidence is generated on its benefit or safety, while such a policy has been blindly accepted and law enforced. Perhaps, the investment could be more rewarding on alternative sustainable solutions based on indigenous foods while improving food diversity and the access to basic public health care.
In SSA countries, without the lack of evidence and scientific consensus, compulsory food fortification has been adopted, ignoring the role of native foods and of a balanced and diversified diet for addressing the variety of nutritional problems. To date, it is not possible to estimate this intervention on follow-ups such as mortality, morbidity, adverse effects, congenital anomalies, as no trials included these long-term outcomes.
Food industry first ultra-process staple foods, depriving them of essential micronutrients, and subsequently fortify them, on a claimed cost-effective public health intervention to reduce micronutrient deficiencies. This market-driven fortification does not however specify how to ensure its compatibility with indigenous foods and public health.
Corporate-led fortification is becoming the main policy thrust, while holistic, balanced natural diets, produced and processed by communities themselves, are not receiving the same attention. It is therefore uncertain whether food and beverage fortification reduces the risk of subclinical deficiencies the corroboration has been assessed as very low.
Food fortification should support dietary improvement strategies as a complementary master plan and not as an alternative strategy despite the fact that fortification has proven effective in treating nutritional single deficiencies in the past. From relative past success with fortification in other world regions, the key ingredients should be a formal cooperation among government bodies and food industry, public education, based on epidemiological evaluations to assess the initiative, and with no direct conflict of interests.
Author Contributions
Conceptualization; supervision: TF; writing: original draft preparation, TF, VB; investigation: ARR, JF, VB; writing: review and editing, TF, TV, ARR, VB; validation: TF, TV. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Giller, K.E.; Delaune, T.; Silva, J.V.; Descheemaeker, K.; van de Ven, G.; Schut, A.G.T.; van Wijk, M.; Hammond, J.; Hochman, Z.; Taulya, G.; et al. The Future of Farming: Who Will Produce Our Food? Food Secur. 2021, 13, 1073–1099. [Google Scholar] [CrossRef]
- International Labour Office The End to Poverty Initiative The ILO and the 2030 Agenda The End to Poverty Initiative: The ILO and the 2030 Agenda; Geneva, 2016.
- Struik, P.C.; Kuyper, T.W. Sustainable Intensification in Agriculture: The Richer Shade of Green. A Review. Agron. Sustain. Dev. 2017, 37, 1–15. [Google Scholar]
- Wijerathna-Yapa, A.; Pathirana, R. Sustainable Agro-Food Systems for Addressing Climate Change and Food Security. Agriculture 2022, 12, 1554. [Google Scholar] [CrossRef]
- Jacobs, D.R.; Tapsell, L.C. Food, Not Nutrients, Is the Fundamental Unit in Nutrition. Nutr. Rev. 2007, 65, 439–450. [Google Scholar] [PubMed]
- Olabisi, M.; Obekpa, H.O.; Liverpool-Tasie, S. Is Growing Your Own Food Necessary for Dietary Diversity? Evidence from Nigeria. Food Policy 2021, 104, 102144. [Google Scholar] [CrossRef]
- Ritchie, H.; Spooner, F.; Roser, M. Clean Water. Available online: https://ourworldindata.org/clean-water (accessed on 21 January 2024).
- Emenike, C.P.; Tenebe, I.T.; Omole, D.O.; Ngene, B.U.; Oniemayin, B.I.; Maxwell, O.; Onoka, B.I. Accessing Safe Drinking Water in Sub-Saharan Africa: Issues and Challenges in South–West Nigeria. Sustain. Cities Soc. 2017, 30, 263–272. [Google Scholar] [CrossRef]
- Workman, C.L.; Stoler, J.; Harris, A.; Ercumen, A.; Kearns, J.; Mapunda, K.M. Food, Water, and Sanitation Insecurities: Complex Linkages and Implications for Achieving WASH Security. Glob. Public Health 2022, 17, 3060–3075. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, B.; Paulavets, K.; Barreto-Gomez, L.; Echeverri, L.G.; Pachauri, S.; Boza-Kiss, B.; Zimm, C.; Rogelj, J.; Creutzig, F.; Ürge-Vorsatz, D.; et al. Pandemic, War, and Global Energy Transitions. Energies 2022, 15, 6114. [Google Scholar] [CrossRef]
- Wudil, A.H.; Usman, M.; Rosak-Szyrocka, J.; Pilař, L.; Boye, M. Reversing Years for Global Food Security: A Review of the Food Security Situation in Sub-Saharan Africa (SSA). Int. J. Environ. Res. Public Health 2022, 19, 14836. [Google Scholar] [CrossRef] [PubMed]
- OFID Zero Hunger by 2030: The Not-so-Impossible Dream; Viena, Austria, 2016.
- Rother, B.; Sosa, S.; Kim, D.; Kohler, L.; Pierre, G.; Kato, N.; Debbich, M.; Castrovillari, C.; Sharifzoda, K.; Heuvelen, E. Van; et al. Tackling the Global Food Crisis: Impact, Policy Response, and the Role of the IMF; Washington, DC, 2022. 2022. [Google Scholar]
- FAO, IFAD, UNICEF, W. and W. The State of Food Security and Nutrition in the World 2023; FAO: Rome, 2023.
- Kesari, A.; Noel, J.Y. Nutritional Assessment. StatPearls 2023, 1–14. [Google Scholar] [CrossRef]
- Odjo, S.; Traoré, F.; Zaki, C. Africa Agriculture Trade Monitor 2023; Kigali and Washington, DC, 2023.
- IFC Food Fortification. Global Agribusiness; Washington, DC, 2023.
- WHO Food Fortification. Available online: https://www.who.int/health-topics/food-fortification#tab=tab_1 (accessed on 21 January 2024).
- Leung, A.M.; Braverman, L.E.; Pearce, E.N. History of U. S. Iodine Fortification and Supplementation. Nutrients 2012, 4, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Lisco, G.; De Tullio, A.; Triggiani, D.; Zupo, R.; Giagulli, V.A.; De Pergola, G.; Piazzolla, G.; Guastamacchia, E.; Sabbà, C.; Triggiani, V. Iodine Deficiency and Iodine Prophylaxis: An Overview and Update. Nutrients 2023, 15, 1004. [Google Scholar] [CrossRef] [PubMed]
- Katsidzira, L.; Gangaidzo, I.; Thomson, S.; Rusakaniko, S.; Matenga, J.; Ramesar, R. The Shifting Epidemiology of Colorectal Cancer in Sub-Saharan Africa. Lancet Gastroenterol. Hepatol. 2017, 2, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Maiyoh, G.K.; Tuei, V.C. Rising Cancer Incidence and Role of the Evolving Diet in Kenya. Nutr. Cancer 2019, 71, 531–546. [Google Scholar] [CrossRef] [PubMed]
- Bigman, G.; Otieno, L.; Adebamowo, S.N.; Adebamowo, C. Dietary Intake and Cancer in Sub-Saharan Africa: A Critical Review of Epidemiological Studies. Nutr. Cancer 2022, 74, 2803–2814. [Google Scholar] [CrossRef] [PubMed]
- Valicente, V.M.; Peng, C.H.; Pacheco, K.N.; Lin, L.; Kielb, E.I.; Dawoodani, E.; Abdollahi, A.; Mattes, R.D. Ultraprocessed Foods and Obesity Risk: A Critical Review of Reported Mechanisms. Adv. Nutr. 2023, 14, 718–738. [Google Scholar] [CrossRef] [PubMed]
- Farvid, M.S.; Spence, N.D.; Holmes, M.D.; Barnett, J.B. Fiber Consumption and Breast Cancer Incidence: A Systematic Review and Meta-Analysis of Prospective Studies. Cancer 2020, 126, 3061–3075. [Google Scholar] [CrossRef]
- Zahangir, M.S.; Hasan, M.M.; Richardson, A.; Tabassum, S. Malnutrition and Non-Communicable Diseases among Bangladeshi Women: An Urban–Rural Comparison. Nutr. Diabetes 2017, 7, e250–e250. [Google Scholar] [CrossRef] [PubMed]
- Ofori, K.F.; Antoniello, S.; English, M.M.; Aryee, A.N.A. Improving Nutrition through Biofortification–A Systematic Review. Front. Nutr. 2022, 9, 1043655. [Google Scholar] [CrossRef] [PubMed]
- Avnee; Sood, S. ; Chaudhary, D.R.; Jhorar, P.; Rana, R.S. Biofortification: An Approach to Eradicate Micronutrient Deficiency. Front. Nutr. 2023, 10, 1233070.
- Chaudhary, V.; Saraswathy, K.; Sarwal, R. Dietary Diversity as a Sustainable Approach towards Micronutrient Deficiencies in India. Indian J. Med. Res. 2022, 156, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, A. V.; Ghosh, S.; Thomas, T.; Bandyopadhyay, S.; Goswami, R.; Gupta, A.; Gupta, P.; John, A.T.; Kapil, U.; Kulkarni, B.; et al. Perspective: When the Cure Might Become the Malady: The Layering of Multiple Interventions with Mandatory Micronutrient Fortification of Foods in India. Am. J. Clin. Nutr. 2021, 114, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Bechoff, A.; de Bruyn, J.; Alpha, A.; Wieringa, F.; Greffeuille, V. Exploring the Complementarity of Fortification and Dietary Diversification to Combat Micronutrient Deficiencies: A Scoping Review. Curr. Dev. Nutr. 2023, 7. [Google Scholar] [CrossRef]
- Das, J.K.; Salam, R.A.; Mahmood, S. Bin; Moin, A.; Kumar, R.; Mukhtar, K.; Lassi, Z.S.; Bhutta, Z.A. Food Fortification with Multiple Micronutrients: Impact on Health Outcomes in General Population. Cochrane Database Syst. Rev. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.M.; Rai, M.; Morando, D.W. Anemia Screening. StatPearls 2023.
- Duggal, M.; Sesikeran, B.; Arlappa, N.; Nair, S.; Shekhar, V.; Sabharwal, V. Large-Scale Staple Food Fortification as a Complementary Strategy to Address Vitamin and Mineral Vulnerabilities in India: A Critical Review. Indian J. Public Health 2022, 66, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Pike, A. A Brief History of Food Fortification in the U.S. Available online: https://foodinsight.org/is-food-fortification-necessary-a-historical-perspective/ (accessed on 19 June 2024).
- Health Canada Addition of Vitamins and Minerals to Foods. Proposed Policy Recommendations; Ottawa, Canada.
- Institute of Medicine Dietary Reference Intakes: Guiding Principles for Nutrition Labeling and, Fortification; National Academies Press: Washington, D.C. Institute of Medicine Dietary Reference Intakes: Guiding Principles for Nutrition Labeling and Fortification; National Academies Press: Washington, D.C., 2003; ISBN 978-0-309-09143-5.
- Chen, P.J.; Antonelli, M. Conceptual Models of Food Choice: Influential Factors Related to Foods, Individual Differences, and Society. Foods 2020, 9, 1898. [Google Scholar] [CrossRef] [PubMed]
- Hoogendoorn, A.; Luthringer, C.; Parvanta, I.; Garrett, G.S. Food Fortification Global Mapping Study 2016; Technical assistance for strengthening capacities in food fortification, Publications Office, 2016.
- European Union Regulation (EU) No 609/2013 of the European Parliament and of the Council. Available online: https://eur-lex.europa.eu/eli/reg/2013/609/oj (accessed on 19 June 2024).
- UNICEF Landscape Analysis of Large-Scale Fortification of Oil and Wheat Flour in Some West and Central African Countries: Status, Challenges and Opportunities for the Future; 2022.
- ASHA Do India’s Food Safety Regulator (FSSAI) and Indian Citizens Need Saving From (Foreign & Indian) Private Players Behind Food Fortification Initiatives? – A Report on the Objectionable Conflict of Interest That Pervades India’s Food Fortification Public Po; New Delhi, India, 2023.
- Bromage, S.; Gonchigsumlaa, E.; Traeger, M.; Magsar, B.; Wang, Q.; Bater, J.; Li, H.; Ganmaa, D. Awareness and Attitudes Regarding Industrial Food Fortification in Mongolia and Harbin. Nutrients 2019, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Bater, J.; Bromage, S.; Jambal, T.; Tsendjav, E.; Lkhagvasuren, E.; Jutmann, Y.; Martineau, A.R.; Ganmaa, D. Prevalence and Determinants of Vitamin D Deficiency in 9595 Mongolian Schoolchildren: A Cross-Sectional Study. Nutrients 2021, 13, 4175. [Google Scholar] [CrossRef] [PubMed]
- Menal-Puey, S.; Marques-Lopes, I. Regulatory Framework of Fortified Foods and Dietary Supplements for Athletes: An Interpretive Approach. Nutrients 2021, 13, 3858. [Google Scholar] [CrossRef] [PubMed]
- Global Fortification Data Exchange Country Fortification Dashboard. Available online: https://fortificationdata.org/list-of-countries-for-the-food-fortification-dashboard/ (accessed on 21 January 2024).
- OECD/EU Development Assistance and Conditionality: Challenges in Design and Options for More Effective Assistance; Washington, DC, 2017.
- Han, X.; Ding, S.; Lu, J.; Li, Y. Global, Regional, and National Burdens of Common Micronutrient Deficiencies from 1990 to 2019: A Secondary Trend Analysis Based on the Global Burden of Disease 2019 Study. eClinicalMedicine 2022, 44. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.H.; Bell, V. The Imprecision of Micronutrient Requirement Values: The Example of Vitamin D. J. Food Sci. 2024, 89, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Liang, Q.; Balakrishnan, B.; Belobrajdic, D.P.; Feng, Q.J.; Zhang, W. Role of Dietary Nutrients in the Modulation of Gut Microbiota: A Narrative Review. Nutrients 2020, 12, 381. [Google Scholar] [CrossRef] [PubMed]
- Shortt, C.; Hasselwander, O.; Meynier, A.; Nauta, A.; Fernández, E.N.; Putz, P.; Rowland, I.; Swann, J.; Türk, J.; Vermeiren, J.; et al. Systematic Review of the Effects of the Intestinal Microbiota on Selected Nutrients and Non-Nutrients. Eur. J. Nutr. 2017, 57, 25–49. [Google Scholar] [CrossRef] [PubMed]
- Hermes Sales, C.; de Mello Fontanelli, M.; Macedo Rogero, M.; Mori Sarti, F.; Fisberg, R.M. Dietary Inadequacies Overestimate the Blood Deficiencies of Magnesium, Zinc, and Vitamins A, C, E, and D among Residents of Sao Paulo. Clin. Nutr. ESPEN 2023, 53, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Wynants, M.; Kelly, C.; Mtei, K.; Munishi, L.; Patrick, A.; Rabinovich, A.; Nasseri, M.; Gilvear, D.; Roberts, N.; Boeckx, P.; et al. Drivers of Increased Soil Erosion in East Africa’s Agro-Pastoral Systems: Changing Interactions between the Social, Economic and Natural Domains. Reg. Environ. Chang. 2019, 19, 1909–1921. [Google Scholar] [CrossRef]
- Xie, H.; Huang, Y.; Chen, Q.; Zhang, Y.; Wu, Q. Prospects for Agricultural Sustainable Intensification: A Review of Research. Land 2019, 8, 157. [Google Scholar] [CrossRef]
- Oberč, B.P.; Arroyo Schnell, A. Approaches to Sustainable Agriculture: Exploring the Pathways towards the Future of Farming; IUCN, International Union for Conservation of Nature: Brussels, Belgium, 2020. ISBN 978-2-8317-2057-9.
- Sustainable Food Systems for Food Security. Need for Combination of Local and Global Approaches; Thomas, A., Alpha, A., Barczak, A., Zakhia-Rozis, N., Eds.; éditions Quae: Versailles, 2022. ISBN 978-2-7592-3576-6.
- Gernand, A.D.; Aguree, S.; Pobee, R.; Colecraft, E.K.; Murray-Kolb, L.E. Concurrent Micronutrient Deficiencies Are Low and Micronutrient Status Is Not Related to Common Health Indicators in Ghanaian Women Expecting to Become Pregnant. Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef] [PubMed]
- Houghton, L.A.; Trilok-Kumar, G.; McIntosh, D.; Haszard, J.J.; Harper, M.J.; Reid, M.; Erhardt, J.; Bailey, K.; Gibson, R.S. Multiple Micronutrient Status and Predictors of Anemia in Young Children Aged 12-23 Months Living in New Delhi, India. PLoS One 2019, 14, e0209564. [Google Scholar] [CrossRef]
- WHO and FAO Guidelines on Food Fortification with Micronutrients; Allen, L., Benoist, B. de, Dary, O., Hurrell, R., Eds.; World Health Organization: Geneva, Switzerland, 2006; ISBN 92 4 159401 2.
- Saha, S.; Roy, A. Whole Grain Rice Fortification as a Solution to Micronutrient Deficiency: Technologies and Need for More Viable Alternatives. Food Chem. 2020, 326, 127049. [Google Scholar] [CrossRef]
- Swanepoel, E.; Havemann-Nel, L.; Rothman, M.; Laubscher, R.; Matsungo, T.M.; Smuts, C.M.; Faber, M. Contribution of Commercial Infant Products and Fortified Staple Foods to Nutrient Intake at Ages 6, 12, and 18 Months in a Cohort of Children from a Low Socio-Economic Community in South Africa. Matern. Child Nutr. 2019, 15. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidelines on Food Fortification with Micronutrients; Geneva, Switzerland, 2006.
- Liyanage, C.; Hettiarachchi, M. Food Fortification. Ceylon Med. J. 2011, 56, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Shubham, K.; Anukiruthika, T.; Dutta, S.; Kashyap, A. V.; Moses, J.A.; Anandharamakrishnan, C. Iron Deficiency Anemia: A Comprehensive Review on Iron Absorption, Bioavailability and Emerging Food Fortification Approaches. Trends Food Sci. Technol. 2020, 99, 58–75. [Google Scholar] [CrossRef]
- Wells, J.C.K.; Marphatia, A.A.; Amable, G.; Siervo, M.; Friis, H.; Miranda, J.J.; Haisma, H.H.; Raubenheimer, D. The Future of Human Malnutrition: Rebalancing Agency for Better Nutritional Health. Global. Health 2021, 17, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Chadare, F.J.; Idohou, R.; Nago, E.; Affonfere, M.; Agossadou, J.; Fassinou, T.K.; Kénou, C.; Honfo, S.; Azokpota, P.; Linnemann, A.R.; et al. Conventional and Food-to-Food Fortification: An Appraisal of Past Practices and Lessons Learned. Food Sci. Nutr. 2019, 7, 2781–2795. [Google Scholar] [CrossRef] [PubMed]
- Damms-Machado, A.; Weser, G.; Bischoff, S.C. Micronutrient Deficiency in Obese Subjects Undergoing Low Calorie Diet. Nutr. J. 2012, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- OECD Regulatory Governance of Large-Scale Food Fortification: Literature Review Theoretical and Empirical Foundations for Developing a Measurement Framework; 2024.
- Akombi, B.J.; Agho, K.E.; Merom, D.; Renzaho, A.M.; Hall, J.J. Child Malnutrition in Sub-Saharan Africa: A Meta-Analysis of Demographic and Health Surveys (2006-2016). PLoS One 2017, 12, e0177338. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.; De Sanctis, V.; Alaaraj, N.; Ahmed, S.; Alyafei, F.; Hamed, N.; Soliman, N. Early and Long-Term Consequences of Nutritional Stunting: From Childhood to Adulthood. Acta Biomed. Atenei Parm. 2021, 92, 11346–11346. [Google Scholar] [CrossRef]
- Mordor Intelligence Africa Vitamin Fortified and Mineral Enriched Food & Beverage Market Size & Share Analysis - Growth Trends & Forecasts (2024 - 2029). Available online: https://www.mordorintelligence.com/industry-reports/africa-vitamin-fortified-and-mineral-enriched-food-beverage-market (accessed on 15 January 2024).
- Liria-Domínguez, R.; Penny, M.; Kroon, P.A.; Burgos, G.; Dainty, J.; Zeder, C.; Zimmermann, M.B.; King, J.; Mithen, R.; Boy, E.; et al. Biofortified Yellow-Fleshed Potatoes Provide More Absorbable Zinc than a Commonly Consumed Variety: A Randomized Trial Using Stable Isotopes in Women in the Peruvian Highlands. J. Nutr. 2023, 153, 2893–2900. [Google Scholar] [CrossRef] [PubMed]
- Bell, V.; Barros, A.B.; Fernandes, T.H. Food Fortification in Sub Saharan Africa: Science or Business? In Food and Nutrition Security in Africa; Fernandes, T.H., Ferrão, J., Facknath, S., Eds.; Mozambique: Alcance Ed., 2020 ISBN 978-989-8934-05-5.
- Reardon, T.; Tschirley, D.; Liverpool-Tasie, L.S.O.; Awokuse, T.; Fanzo, J.; Minten, B.; Vos, R.; Dolislager, M.; Sauer, C.; Dhar, R.; et al. The Processed Food Revolution in African Food Systems and the Double Burden of Malnutrition. Glob. Food Sec. 2021, 28, 100466. [Google Scholar] [CrossRef] [PubMed]
- Naiken, L. FAO Methodology for Estimating the Prevalence of Undernourishment. Available online: https://www.fao.org/3/Y4249E/y4249e06.htm (accessed on 10 January 2024).
- Fanzo, J. The Nutrition Challenge in Sub-Saharan Africa; Rome, 2012.
- Mukanu, M.M.; Mchiza, Z.J.R.; Delobelle, P.; Thow, A.M. Nutrition Policy Reforms to Address the Double Burden of Malnutrition in Zambia: A Prospective Policy Analysis. Health Policy Plan. 2023, 38, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Clapp, J.; Moseley, W.G.; Burlingame, B.; Termine, P. Viewpoint: The Case for a Six-Dimensional Food Security Framework. Food Policy 2022, 106, 102164. [Google Scholar] [CrossRef]
- DGA Dietary Guidelines for Americans, 2020-2025. Available online: https://www.dietaryguidelines.gov/resources/2020-2025-dietary-guidelines-online-materials (accessed on 3 January 2024).
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN Micronutrient Guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)—Zinc Review. J. Nutr. 2016, 146, 858S–885S. [Google Scholar] [CrossRef]
- Fischer, P.W.F.; L’Abbé, M. Iodine in Iodized Table Salt and in Sea Salt. Can. Inst. Food Sci. Technol. J. 1980, 13, 103–104. [Google Scholar] [CrossRef]
- Hombali, A.S.; Solon, J.A.; Venkatesh, B.T.; Nair, N.S.; Peña-Rosas, J.P. Fortification of Staple Foods with Vitamin a for Vitamin a Deficiency. Cochrane Database Syst. Rev. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Majchrzak, D.; Fabian, E.; Elmadfa, I. Vitamin A Content (Retinol and Retinyl Esters) in Livers of Different Animals. Food Chem. 2006, 98, 704–710. [Google Scholar] [CrossRef]
- Blaner, W.S. Vitamin A and Provitamin A Carotenoids. In Present Knowledge in Nutrition; Academic Press, 2020; pp. 73–91.
- National Institutes of Health Vitamin A and Carotenoids. Available online: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/ (accessed on 19 January 2024).
- Scientific Committee for Animal Nutrition Report of the Scientific Committee for Animal Nutrition on the Risk Of Hypervitaminosis A; 1992.
- Neela, S.; Fanta, S.W. Review on Nutritional Composition of Orange-Fleshed Sweet Potato and Its Role in Management of Vitamin A Deficiency. Food Sci. Nutr. 2019, 7, 1920–1945. [Google Scholar] [CrossRef] [PubMed]
- Carazo, A.; Macáková, K.; Matoušová, K.; Krčmová, L.K.; Protti, M.; Mladěnka, P. Vitamin A Update: Forms, Sources, Kinetics, Detection, Function, Deficiency, Therapeutic Use and Toxicity. Nutrients 2021, 13, 1703. [Google Scholar] [CrossRef] [PubMed]
- Szabó, É.; Csölle, I.; Felső, R.; Kuellenberg de Gaudry, D.; Nyakundi, P.N.; Ibrahim, K.; Metzendorf, M.I.; Ferenci, T.; Lohner, S. Benefits and Harms of Edible Vegetable Oils and Fats Fortified with Vitamins A and D as a Public Health Intervention in the General Population: A Systematic Review of Interventions. Nutrients 2023, 15, 5135. [Google Scholar] [CrossRef] [PubMed]
- Gebregziabher, B.S.; Gebremeskel, H.; Debesa, B.; Ayalneh, D.; Mitiku, T.; Wendwessen, T.; Habtemariam, E.; Nur, S.; Getachew, T. Carotenoids: Dietary Sources, Health Functions, Biofortification, Marketing Trend and Affecting Factors – A Review. J. Agric. Food Res. 2023, 14, 100834. [Google Scholar] [CrossRef]
- Zambou, N.F.; Mbiapo, T.F.; Lando, G.; Tchana, K.A.; Gouado, I. [Effect of Onchocerca Volvulus Infestation on Plasma Vitamin A Concentration in School Children in a Rural Region of Cameroon]. Sante 1999, 9, 151–155. [Google Scholar] [PubMed]
- Gupta, S.; Brazier, A.K.M.; Lowe, N.M. Zinc Deficiency in Low- and Middle-Income Countries: Prevalence and Approaches for Mitigation. J. Hum. Nutr. Diet. 2020, 33, 624–643. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Song, M.; Mucci, L.A.; Giovannucci, E.L. Zinc Supplement Use and Risk of Aggressive Prostate Cancer: A 30-Year Follow-up Study. Eur. J. Epidemiol. 2022, 37, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Grüngreiff, K.; Gottstein, T.; Reinhold, D. Zinc Deficiency—An Independent Risk Factor in the Pathogenesis of Haemorrhagic Stroke? Nutrients 2020, 12, 3548. [Google Scholar] [CrossRef] [PubMed]
- Hanif, N.; Anwer, F. Chronic Iron Deficiency. StatPearls 2023.
- Yuen, H.-W.; Gossman, W.G. Iron Toxicity. StatPearls 2023.
- Miniero, R.; Talarico, V.; Galati, M.C.; Laura; Giancotti; Saracco, P.; Raiola, G.; Miniero, R.; Talarico, V.; Galati, M.C.; et al. Iron Deficiency and Iron Deficiency Anemia in Children. In Public Health and Nutrition in Developing Countries Part-I; IntechOpen, 2018; pp. 638–662 ISBN 978-1-78985-444-2.
- Singh, U.; Praharaj, C.S.; Singh, S.S.; Singh, N.P. Biofortification: Introduction, Approaches, Limitations, and Challenges. In Biofortification of Food Crops; Springer India, 2016; pp. 3–18 ISBN 9788132227168.
- Coelho, R.C.; Barsotti, R.C.F.; Maltez, H.F.; Lopes Júnior, C.A.; Barbosa, H. de S. Expanding Information on the Bioaccessibility and Bioavailability of Iron and Zinc in Biofortified Cowpea Seeds. Food Chem. 2021, 347, 129027. [CrossRef]
- Garg, M.; Sharma, N.; Sharma, S.; Kapoor, P.; Kumar, A.; Chunduri, V.; Arora, P. Biofortified Crops Generated by Breeding, Agronomy, and Transgenic Approaches Are Improving Lives of Millions of People around the World. Front. Nutr. 2018, 5, 301899. [Google Scholar] [CrossRef] [PubMed]
- Ohanenye, I.C.; Emenike, C.U.; Mensi, A.; Medina-Godoy, S.; Jin, J.; Ahmed, T.; Sun, X.; Udenigwe, C.C. Food Fortification Technologies: Influence on Iron, Zinc and Vitamin A Bioavailability and Potential Implications on Micronutrient Deficiency in Sub-Saharan Africa. Sci. African 2021, 11, e00667. [Google Scholar] [CrossRef]
- Kruger, J. Potential of Food-to-Food Fortification with Cowpea Leaves and Orange-Fleshed Sweet Potato, in Combination with Conventional Fortification, to Improve the Cellular Uptake of Iron and Zinc from Ready-to-Eat Maize Porridges. Food Sci. Nutr. 2020, 8, 3190–3199. [Google Scholar] [CrossRef] [PubMed]
- Adetola, O.Y.; Kruger, J.; White, Z.; Taylor, J.R.N. Comparison between Food-to-Food Fortification of Pearl Millet Porridge with Moringa Leaves and Baobab Fruit and with Adding Ascorbic and Citric Acid on Iron, Zinc and Other Mineral Bioaccessibility. LWT 2019, 106, 92–97. [Google Scholar] [CrossRef]
- Adetola, O.Y.; Kruger, J.; Ferruzzi, M.G.; Hamaker, B.R.; Taylor, J.R.N. Potential of Moringa Leaf and Baobab Fruit Food-to-Food Fortification of Wholegrain Maize Porridge to Improve Iron and Zinc Bioaccessibility. Int. J. Food Sci. Nutr. 2022, 73, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Lubaale, J.; Taylor, J.R.N.; Emmambux, M.N.; Duodu, K.G. Extrusion Cooking of Food-to-Food Fortified Wholegrain Sorghum-Based Porridges Enhances Caco-2 Ferritin Formation. Cereal Chem. 2023, 100, 371–383. [Google Scholar] [CrossRef]
- Siddiqui, F.; Salam, R.A.; Lassi, Z.S.; Das, J.K. The Intertwined Relationship Between Malnutrition and Poverty. Front. Public Heal. 2020, 8, 525026. [Google Scholar] [CrossRef] [PubMed]
- United Nations (UN) Extreme Poverty in Developing Countries Inextricably Linked to Global Food Insecurity Crisis, Senior Officials Tell Second Committee.
- FAO Food Systems Resilience-Building for East and Southern Africa Enters New Phase. Available online: https://www.fao.org/support-to-investment/news/detail/en/c/1655420/ (accessed on 3 January 2024).
- Ruggeri Laderchi, C.; Saith, R.; Stewart, F. Does It Matter That We Do Not Agree on the Definition of Poverty? A Comparison of Four Approaches. Oxford Dev. Stud. 2003, 31, 243–274. [Google Scholar] [CrossRef]
- Dieterich, C.M.; Felice, J.P.; O’Sullivan, E.; Rasmussen, K.M. Breastfeeding and Health Outcomes for the Mother-Infant Dyad. Pediatr. Clin. North Am. 2013, 60, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Dewi, N.U.; Mahmudiono, T. Effectiveness of Food Fortification in Improving Nutritional Status of Mothers and Children in Indonesia. Int. J. Environ. Res. Public Health 2021, 18, 2133. [Google Scholar] [CrossRef] [PubMed]
- Okeyo, D.O. Impact of Food Fortification on Child Growth and Development during Complementary Feeding. Ann. Nutr. Metab. 2018, 73, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Mphasha, M.H.; Makwela, M.S.; Muleka, N.; Maanaso, B.; Phoku, M.M. Breastfeeding and Complementary Feeding Practices among Caregivers at Seshego Zone 4 Clinic in Limpopo Province, South Africa. Children 2023, 10, 986. [Google Scholar] [CrossRef] [PubMed]
- UNICEF-WHO-WB Joint Child Malnutrition Estimates 2023. Available online: https://datatopics.worldbank.org/child-malnutrition/ (accessed on 4 January 2024).
- Colecraf, E.K.; Otoo, G.E. Methods and Metrics for Food Security and Nutrition Outcome Indicators; African Economic Research Consortium, 2022.
- Abebe, Z.; Haki, G.D.; Baye, K. Simulated Effects of Home Fortification of Complementary Foods with Micronutrient Powders on Risk of Inadequate and Excessive Intakes in West Gojjam, Ethiopia. Matern. Child Nutr. 2018, 14. [Google Scholar] [CrossRef]
- Suchdev, P.S.; Jefferds, M.E.D.; Ota, E.; da Silva Lopes, K.; De-Regil, L.M. Home Fortification of Foods with Multiple Micronutrient Powders for Health and Nutrition in Children under Two Years of Age. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Masuke, R.; Msuya, S.E.; Mahande, J.M.; Diarz, E.J.; Stray-Pedersen, B.; Jahanpour, O.; Mgongo, M. Effect of Inappropriate Complementary Feeding Practices on the Nutritional Status of Children Aged 6-24 Months in Urban Moshi, Northern Tanzania: Cohort Study. PLoS One 2021, 16, e0250562. [Google Scholar] [CrossRef] [PubMed]
- Jamshed, S.; Khan, F.-.; Begum, A.; Ali, B.B.; Akram, Z.; Ariff, M.; Jamshed, S.; Khan, F.; Begum, A.; Ali, B.B.; et al. Frequency of Low Birth Weight and Its Relationship With Maternal Nutritional and Dietary Factors: A Cross-Sectional Study. Cureus 2020, 12. [CrossRef]
- Khatun, W.; Rasheed, S.; Alam, A.; Huda, T.M.; Dibley, M.J. Assessing the Intergenerational Linkage between Short Maternal Stature and Under-Five Stunting and Wasting in Bangladesh. Nutrients 2019, 11, 1818. [Google Scholar] [CrossRef] [PubMed]
- Akinola, R.; Pereira, L.M.; Mabhaudhi, T.; de Bruin, F.M.; Rusch, L. A Review of Indigenous Food Crops in Africa and the Implications for More Sustainable and Healthy Food Systems. Sustainability 2020, 12, 3493. [Google Scholar] [CrossRef] [PubMed]
- Kamgain, T.; Kwazi Zuma, A.D.; Mbhenyane, M.; Knowledge, X.; Kesa, H.; Kamgain, A.D.T.; Kwazi Zuma, M.; Mbhenyane, X. Knowledge, Perception and Consumption of Indigenous Foods in Gauteng Region, South Africa. Int. J. Environ. Res. Public Health 2023, 20, 6961. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.L.; Arnold, C.D.; Wessells, K.R.; Stewart, C.P.; Abbeddou, S.; Adu-Afarwuah, S.; Arnold, B.F.; Ashorn, U.; Ashorn, P.; Becquey, E.; et al. Small-Quantity Lipid-Based Nutrient Supplements for Children Age 6–24 Months: A Systematic Review and Individual Participant Data Meta-Analysis of Effects on Developmental Outcomes and Effect Modifiers. Am. J. Clin. Nutr. 2021, 114, 43S–67S. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.P.; Vosti, S.A.; Arnold, C.D.; Engle-Stone, R.; Prado, E.L.; Stewart, C.P.; Wessells, K.R.; Dewey, K.G. The Cost-Effectiveness of Small-Quantity Lipid-Based Nutrient Supplements for Prevention of Child Death and Malnutrition and Promotion of Healthy Development: Modelling Results for Uganda. Public Health Nutr. 2023, 26, 2083–2095. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Arnold, C.D.; Wessells, K.R.; Stewart, C.P. Lipid-Based Nutrient Supplements for Prevention of Child Undernutrition: When Less May Be More. Am. J. Clin. Nutr. 2023, 118, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Small Supplements for the Prevention of Malnutrition in Early Childhood (Small Quantity Lipid-Based Nutrient Supplements). Brief Guidance Note 2023.
- Bell, V.; Ferrão, J.; Pimentel, L.; Pintado, M.; Fernandes, T. One Health, Fermented Foods, and Gut Microbiota. Foods 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- FAO Unleashing the Potential of Millets; FAO: Rome, Italy. 2023; ISBN 978-92-5-138105-2.
- Mahajan, S.; Hausladen, C.I.; Argota Sánchez-Vaquerizo, J.; Korecki, M.; Helbing, D. Participatory Resilience: Surviving, Recovering and Improving Together. Sustain. Cities Soc. 2022, 83, 103942. [Google Scholar] [CrossRef]
- Children’s Work in African Agriculture. The Harmful and the Harmless.; Sumber, J., Wheeler, R.S.-, Eds.; Bristol University Press.: Bristol, 2023; ISBN 978-1-5292-2607-2. [Google Scholar]
- Un-Nutrition Transforming Nutrition. UN-Nutrition J. 2022, 1. Un-Nutrition Transforming Nutrition. UN-Nutrition J. 2022, 1. [CrossRef]
- Method, A.; Tulchinsky, T.H. Commentary: Food Fortification: African Countries Can Make More Progress. Adv. Food Technol. Nutr. Sci. - Open J. 2015, SE, S22–S28. [CrossRef]
- Mokoena, O.P.; Ntuli, T.S.; Ramarumo, T.; Seeletse, S.M. Sustainability of Rural Small-Scale Farmers Using a Thematic Content-Fed Analytic Hierarchy Process. Sustainability 2023, 15, 11983. [Google Scholar] [CrossRef]
- Sirdey, N.; Alpha, A. Food Fortification and Domestic Small-Scale Food Chains’ Actors - The Case of Burkina Faso; CIRAD-ES-UMR MOISA, 2020.
- Ebata, A.; Thorpe, J.; Islam, A.; Sultana, S.; Mbuya, M.N.N. Understanding Drivers of Private-Sector Compliance to Large-Scale Food Fortification: A Case Study on Edible Oil Value Chains in Bangladesh. Food Policy 2021, 104, 102127. [Google Scholar] [CrossRef] [PubMed]
- Luthringer, C.L.; Rowe, L.A.; Vossenaar, M.; Garrett, G.S. Regulatory Monitoring of Fortified Foods: Identifying Barriers and Good Practices. Glob. Heal. Sci. Pract. 2015, 3, 446–461. [Google Scholar] [CrossRef] [PubMed]
- Malézieux, E.; Verger, E.O.; Avallone, S.; Alpha, A.; Ngigi, P.B.; Lourme-Ruiz, A.; Bazile, D.; Bricas, N.; Ehret, I.; Martin-Prevel, Y.; et al. Biofortification versus Diversification to Fight Micronutrient Deficiencies: An Interdisciplinary Review. Food Secur. 2023, 1–15. [Google Scholar] [CrossRef]
- Varzakas, T.; Smaoui, S. Global Food Security and Sustainability Issues: The Road to 2030 from Nutrition and Sustainable Healthy Diets to Food Systems Change. Foods 2024, 13, 306. [Google Scholar] [CrossRef] [PubMed]
- Haysom, G. Integrating Food Sensitive Planning and Urban Design into Urban Governance Actions. Urban Forum 2021, 32, 289–310. [Google Scholar] [CrossRef]
- Ju, P.; Anser, M.K.; Osabohien, R.; Ochuba, O.; Ahuru, R.R.; Ashraf, J. Trade Openness, Foreign Direct Investment and Sustainable Agriculture in Africa. Probl. Ekorozwoju 2022, 17, 246–255. [Google Scholar] [CrossRef]
- Ahwireng, A.K. Small Pelagic Fish for Food: Governance and Performance of Small Pelagic Fish Value Chains for Food Security and Nutrition in Ghana, Amsterdam Institute for Social Science Research (AISSR), 2022.
- Iitembu, J.A.; Mafwila, S.K.; Ndara, S.; Erasmus, V.N. Observed Fishery Regulatory Violations in Namibia and Their Possible Implications for the Sustainable Management of Fishery Resources. Reg. Stud. Mar. Sci. 2023, 63, 103004. [Google Scholar] [CrossRef]
- Voortman, R.L. Why the Green Revolution Failed in Sub-Saharan Africa. Rural 21 2013.
- Niazi, S.K. Handbook of Pharmaceutical Manufacturing Formulations; CRC Press, 2004.
- Dary, O. Establishing Safe and Potentially Efficacious Fortification Contents for Folic Acid and Vitamin B12. Food Nutr. Bull. 2008, 29. [Google Scholar] [CrossRef] [PubMed]
- Yetley, E.A.; Rader, J.I. Modeling the Level of Fortification and Post-Fortification Assessments: U. S. Experience. Nutr. Rev. 2004, 62, S50–S59. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.B.; Arnipalli, S.R.; Mehta, P.; Carrau, S.; Ziouzenkova, O. Iron Deficiency Anemia: Efficacy and Limitations of Nutritional and Comprehensive Mitigation Strategies. Nutrients 2022, 14, 2976. [Google Scholar] [CrossRef] [PubMed]
- Marshall, R.C.; Marx, L.M.; Raiff, M.E. Cartel Price Announcements: The Vitamins Industry ☆. Int. J. Ind. Organ. 2008, 26, 762–802. [Google Scholar] [CrossRef]
- Sight and Life Mauricio Müller Adade. Available online: https://sightandlife.org/about-us/our-team/mauricio-muller-adade (accessed on 21 January 2024).
- DSM Nutritional Products: Structural Adjustments in the Region of Basel as a Consequence of Acquisitions and a Strategic Re-Direction. Available online: https://www.dsm.com/anh/news/press-releases/2014/2014-01-21-dsm-nutritional-products-structural-adjustments-in-the-region-of-basel-as-a-consequence-of-acquisitions-and-a-strategic-re-direction.html# (accessed on 15 March 2024).
- Food Fortification Initiative Flour Millers Toolkit for Fortification. Available online: https://www.ffinetwork.org/implement_sub (accessed on 20 January 2024).
- The Lancet Unveiling the Predatory Tactics of the Formula Milk Industry. Lancet 2023, 401, 409. [CrossRef] [PubMed]
- EFSA Tolerable Upper Intake Levels for Vitamins and Minerals; 2006.
- Fortune Business Insights The Food Premix Market Is Projected to Grow from $6.69 Billion in 2022 to $10.70 Billion by 2029, at a CAGR of 6.93% during the Forecast Period, 2022-2029. Available online: https://www.fortunebusinessinsights.com/food-premix-market-102456 (accessed on 15 January 2024).
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 8, 1065. [Google Scholar] [CrossRef] [PubMed]
- Guinot, P.; Jallier, V.; Blasi, A.; Guyondet, C.; Van Ameringen, M. GAIN Premix Facility: An Innovative Approach for Improving Access to Quality Vitamin and Mineral Premix in Fortification Initiatives. Food Nutr. Bull. 2012, 33. [Google Scholar] [CrossRef] [PubMed]
- Noort, M.W.J.; Renzetti, S.; Linderhof, V.; du Rand, G.E.; Marx-Pienaar, N.J.M.M.; de Kock, H.L.; Magano, N.; Taylor, J.R.N. Towards Sustainable Shifts to Healthy Diets and Food Security in Sub-Saharan Africa with Climate-Resilient Crops in Bread-Type Products: A Food System Analysis. Foods 2022, 11, 135. [Google Scholar] [CrossRef] [PubMed]
- FAO, IFAD, UNICEF, W. and W. The State of Food Security and Nutrition in the World 2022; FAO, 2022.
- Manikas, I.; Ali, B.M.; Sundarakani, B. A Systematic Literature Review of Indicators Measuring Food Security. Agric. Food Secur. 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Mitra, P.; Unsal, F.; Farid, M.; Kemoe, L.; Fayad, D.; Spray, J.; Okou, C.; Salgado Baptista, D.M.; Lanci, L.; Muehlschlegel, T.; et al. Climate Change and Chronic Food Insecurity in Sub-Saharan Africa. Dep. Pap. 2022, 2022, 1. [Google Scholar] [CrossRef]
- Chea, N.; Tegene, Y.; Astatkie, A.; Spigt, M. Prevalence of Undernutrition among Pregnant Women and Its Differences across Relevant Subgroups in Rural Ethiopia: A Community-Based Cross-Sectional Study. J. Heal. Popul. Nutr. 2023, 42, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Valente, F.L.S. The Corporate Capture of Food and Nutrition Governance: A Threat to Human Rights and Peoples’ Sovereignty. Right to Food Nutr. Watch 2015, 1, 15–22. [Google Scholar]
- Scheffler, C.; Hermanussen, M.; Soegianto, S.D.P.; Homalessy, A.V.; Touw, S.Y.; Angi, S.I.; Ariyani, Q.S.; Suryanto, T.; Matulessy, G.K.I.; Fransiskus, T.; et al. Stunting as a Synonym of Social Disadvantage and Poor Parental Education. Int. J. Environ. Res. Public Health 2021, 18, 1350. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.E.; Shah, M.; Badireddy, M. Failure to Thrive. StatPearls 2023, 183–199. [Google Scholar] [CrossRef]
- Frumence, G.; Jin, Y.; Kasangala, A.A.; Mang’enya, M.A.; Bakar, S.; Ochieng, B. A Qualitative Exploration on Perceived Socio-Cultural Factors Contributing to Undernutrition Among Under-Fives in the Southern Highlands of Tanzania. Int. J. Public Health 2023, 68, 1605294. [Google Scholar] [CrossRef] [PubMed]
- Dary, O.; Hainsworth, M. The Food Fortification Formulator: Technical Determination of Fortification Levels and Standards for Mass Fortification; 2008.
- Tam, E.; Keats, E.C.; Rind, F.; Das, J.K.; Bhutta, Z.A. Micronutrient Supplementation and Fortification Interventions on Health and Development Outcomes among Children Under-Five in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 289. [Google Scholar] [CrossRef] [PubMed]
- WHO and FAO Implementing Effective and Sustainable Food Fortification Programmes. In Guidelines on food fortification with micronutrients; Allen, L., Benoist, B. de, Dary, O., Hurrell, R., Eds.; WHO: Geneva, Switzerland, 2006.
- WHO WHO Guideline: Fortification of Maize Flour and Corn Meal with Vitamins and Minerals; WHO: Geneva, Switzerland, 2016. ISBN 9789241549936.
- Ohanenye, I.C.; Emenike, C.U.; Mensi, A.; Medina-Godoy, S.; Jin, J.; Ahmed, T.; Sun, X.; Udenigwe, C.C. Food Fortification Technologies: Influence on Iron, Zinc and Vitamin A Bioavailability and Potential Implications on Micronutrient Deficiency in Sub-Saharan Africa. Sci. African 2021, 11. [Google Scholar] [CrossRef]
- Lopes, S.O.; Abrantes, L.C.S.; Azevedo, F.M.; Morais, N. de S. de; Morais, D. de C.; Gonçalves, V.S.S.; Fontes, E.A.F.; Franceschini, S. do C.C.; Priore, S.E. Food Insecurity and Micronutrient Deficiency in Adults: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 1074. [Google Scholar]
- Ministry of Health and Family Welfare Food Safety and Standards (Fortification of Foods) Regulations, 2018. Gaz. India 2018, Part III-S.
- Renwick, A.G. Toxicology of Micronutrients: Adverse Effects and Uncertainty. J. Nutr. 2006, 136, 493S–501S. [Google Scholar] [CrossRef] [PubMed]
- Pinto, V.R.A.; Campos, R.F. de A.; Rocha, F.; Emmendoerfer, M.L.; Vidigal, M.C.T.R.; da Rocha, S.J.S.S.; Lucia, S.M. Della; Cabral, L.F.M.; de Carvalho, A.F.; Perrone, Í.T. Perceived Healthiness of Foods: A Systematic Review of Qualitative Studies. 2021, 4, 100056. [CrossRef]
- Regional Committee for Africa Progress Report on the Implementation of the Regional Strategy on Enhancing the Role of Traditional Medicine in Health Systems 2013–2023: Information Document; 2020.
- Adebisi, Y.A.; Nwogu, I.B.; Alaran, A.J.; Badmos, A.O.; Bamgboye, A.O.; Rufai, B.O.; Okonji, O.C.; Malik, M.O.; Teibo, J.O.; Abdalla, S.F.; et al. Revisiting the Issue of Access to Medicines in Africa: Challenges and Recommendations. Public Heal. Challenges 2022, 1, e9. [Google Scholar] [CrossRef]
- Giller, K.E.; Delaune, T.; Silva, J.V.; Descheemaeker, K.; van de Ven, G.; Schut, A.G.T.; van Wijk, M.; Hammond, J.; Hochman, Z.; Taulya, G.; et al. The Future of Farming: Who Will Produce Our Food? Food Secur. 2021, 13, 1073–1099. [Google Scholar] [CrossRef]
- Vilar-Compte, M.; Burrola-Méndez, S.; Lozano-Marrufo, A.; Ferré-Eguiluz, I.; Flores, D.; Gaitán-Rossi, P.; Teruel, G.; Pérez-Escamilla, R. Urban Poverty and Nutrition Challenges Associated with Accessibility to a Healthy Diet: A Global Systematic Literature Review. Int. J. Equity Health 2021, 20, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Salas, S.; Gonzalez-Arias, M. Nutrition: Micronutrient Intake, Imbalances, and Interventions. StatPearls 2023.
- Grammatikaki, E.; Wollgast, J.; Caldeira, S. High Levels of Nutrients of Concern in Baby Foods Available in Europe That Contain Sugar-Contributing Ingredients or Are Ultra-Processed. Nutrients 2021, 13, 3105. [Google Scholar] [CrossRef] [PubMed]
- Lieber, C. A Lawsuit Is Accusing Poland Spring of Selling “Ordinary Groundwater”. The Suit Highlights the Opaque, Controversial Business of Bottled Water. Available online: https://www.vox.com/the-goods/2019/4/3/18292549/poland-spring-water-nestle-lawsuit-spring-water (accessed on 15 January 2024).
- Australian Food News Nestle and Gerber Sued over Fluoride-Fortified Food Products. Available online: https://www.ausfoodnews.com.au/2011/10/12/nestle-and-gerber-sued-over-fluoride-fortified-food-products.html (accessed on 15 January 2024).
- Kujinga, P.; Galetti, V.; Onyango, E.; Jakab, V.; Buerkli, S.; Andang’O, P.; Brouwer, I.D.; Zimmermann, M.B.; Moretti, D. Effectiveness of Zinc-Fortified Water on Zinc Intake, Status and Morbidity in Kenyan Pre-School Children: A Randomised Controlled Trial. Public Health Nutr. 2018, 21, 2855–2865. [Google Scholar] [CrossRef] [PubMed]
- Nestlé Nigeria Corporate Communications and Public Affairs Nestlé Nigeria. Creating Shared Value Report 2013; Ilupeju, 2013.
- Coca-Cola Adds Two New Flavor Variants to Its Vitamin Water Range. Available online: https://www.foodbusinessafrica.com/coca-cola-adds-two-new-flavor-variants-to-its-vitamin-water-range/ (accessed on 15 January 2024).
- Yusufali, R.; Sunley, N.; de Hoop, M.; Panagides, D. Flour Fortification in South Africa: Post-Implementation Survey of Micronutrient Levels at Point of Retail. Food Nutr. Bull. 2012, 33. [Google Scholar] [CrossRef] [PubMed]
- Van Jaarsveld, P.J.; Faber, M.; Van Stuijvenberg, M.E. Vitamin A, Iron, and Zinc Content of Fortified Maize Meal and Bread at the Household Level in 4 Areas of South Africa. Food Nutr. Bull. 2015, 36, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Wojcicki, J.M.; Heyman, M.B. Malnutrition and the Role of the Soft Drink Industry in Improving Child Health in Sub-Saharan Africa. Pediatrics 2010, 126, e1617–e1621. [Google Scholar] [CrossRef] [PubMed]
- TechnoServe The Coca-Cola Company, TechnoServe and The Gates Foundation Partner to Boost Incomes of 50,000 Small-Scale Farmers in East Africa. Available online: https://www.technoserve.org/news/the-coca-cola-company-technoserve-and-the-gates-foundation-partner-to-boost/ (accessed on 15 January 2024).
- Council for Responsible Nutrition (CRN) Americans Do Not Get All the Nutrients They Need From Food. Available online: https://www.crnusa.org/resources/americans-do-not-get-all-nutrients-they-need-food (accessed on 16 January 2024).
- SADC SADC Minimum Standard for Food Fortification; Gaborone, Botswana, 2022.
- Wang, V.H.C.; Foster, V.; Yi, S.S. Are Recommended Dietary Patterns Equitable? Public Health Nutr. 2022, 25, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Aaron, G.J.; Friesen, V.M.; Jungjohann, S.; Garrett, G.S.; Neufeld, L.M.; Myatt, M. Coverage of Large-Scale Food Fortification of Edible Oil, Wheat Flour, and Maize Flour Varies Greatly by Vehicle and Country but Is Consistently Lower among the Most Vulnerable: Results from Coverage Surveys in 8 Countries. J. Nutr. 2017, 147, 984S–994S. [Google Scholar] [CrossRef] [PubMed]
- Theriault, V.; Kirimi, L.; Wineman, A.; Kinyumu, E.; Tschirley, D. Assessment of the Policy Enabling Environment for Large-Scale Food Fortification: A Novel Framework with an Application to Kenya. PLOS Glob. Public Heal. 2024, 4, e0003211. [Google Scholar] [CrossRef] [PubMed]
- Global Fortification Data Exchange Interactive Map. Available online: https://fortificationdata.org/interactive-map-fortification-legislation/ (accessed on 27 June 2024).
- Kroker-Lobos, M.F.; Mazariegos, M.; Guamuch, M.; Ramirez-Zea, M. Ultraprocessed Products as Food Fortification Alternatives: A Critical Appraisal from Latin America. Nutrients 2022, 14, 1413. [Google Scholar] [CrossRef] [PubMed]
- Horton, S. The Economics of Food Fortification. J. Nutr. 2006, 136, 1068–1071. [Google Scholar] [CrossRef] [PubMed]
- Ekpa, O.; Palacios-Rojas, N.; Kruseman, G.; Fogliano, V.; Linnemann, A.R. Sub-Saharan African Maize-Based Foods - Processing Practices, Challenges and Opportunities. Food Rev. Int. 2019, 35, 609–639. [Google Scholar] [CrossRef]
- Yang, P.; Wang, H.; Zhu, M.; Ma, Y. Effects of Choline Chloride, Copper Sulfate and Zinc Oxide on Long-Term Stabilization of Microencapsulated Vitamins in Premixes for Weanling Piglets. Animals 2019, 9, 1154. [Google Scholar] [CrossRef] [PubMed]
- Datta, M.; Vitolins, M.Z. Food Fortification and Supplement Use—Are There Health Implications? Crit. Rev. Food Sci. Nutr. 2016, 56, 2149–2159. [Google Scholar] [CrossRef] [PubMed]
- Guallar, E.; Stranges, S.; Mulrow, C.; Appel, L.J.; Miller, E.R. Enough Is Enough: Stop Wasting Money on Vitamin and Mineral Supplements. Ann. Intern. Med. 2013, 159, 850–851. [Google Scholar] [CrossRef] [PubMed]
- Engle-Stone, R.; Vosti, S.A.; Luo, H.; Kagin, J.; Tarini, A.; Adams, K.P.; French, C.; Brown, K.H. Weighing the Risks of High Intakes of Selected Micronutrients Compared with the Risks of Deficiencies. Ann. N. Y. Acad. Sci. 2019, 1446, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Hamishehkar, H.; Ranjdoost, F.; Asgharian, P.; Mahmoodpoor, A.; Sanaie, S. Vitamins, Are They Safe? Adv. Pharm. Bull. 2016, 6, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Rogovik, A.L.; Vohra, S.; Goldman, R.D. Safety Considerations and Potential Interactions of Vitamins: Should Vitamins Be Considered Drugs? Ann. Pharmacother. 2010, 44, 311–324. [Google Scholar] [CrossRef] [PubMed]
- McEldrew, E.P.; Lopez, M.J.; Milstein, H. Vitamin A. In StatPearls; StatPearls Publishing, 2023.
- Degerud, E.M.; Manger, M.S.; Strand, T.A.; Dierkes, J. Bioavailability of Iron, Vitamin A, Zinc, and Folic Acid When Added to Condiments and Seasonings. Ann. N. Y. Acad. Sci. 2015, 1357, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Bangham, C.R.M. HTLV-1 Persistence and the Oncogenesis of Adult T-Cell Leukemia/Lymphoma. Blood 2023, 141, 2299–2306. [Google Scholar] [CrossRef] [PubMed]
- Elechi, J.O.G.; Sirianni, R.; Conforti, F.L.; Cione, E.; Pellegrino, M. Food System Transformation and Gut Microbiota Transition: Evidence on Advancing Obesity, Cardiovascular Diseases, and Cancers—A Narrative Review. Foods 2023, 12, 2286. [Google Scholar] [CrossRef] [PubMed]
- SHI, J.; XIE, Y.; LI, Y.; REN, D.; ZHANG, Y.; SHAO, H.; LIU, Y.; WANG, X.; LI, Y. Effects of Food-Grade Iron(III) Oxide Nanoparticles on Cecal Digesta- and Mucosa-Associated Microbiota and Short-Chain Fatty Acids in Rats. Biosci. microbiota, food Heal. 2024, 43. [CrossRef]
- Bobrek, K.S.; Broersen, B.; Aburto, N.J.; Garg, A.; Serdula, M.; Beltrán Velázquez, F.; Wong, E.C.; Pachón, H. Most National, Mandatory Flour Fortification Standards Do Not Align with International Recommendations for Iron, Zinc, and Vitamin B12 Levels. Food Policy 2021, 99. [Google Scholar] [CrossRef]
- Schutter, O. de Report of the Special Rapporteur on the Right to Food, Olivier de Schutter. Final Report : The Transformative Potential of the Right to Food; United Nations, 2014.
- Archer, N.S.; Cochet-Broch, M.; Mihnea, M.; Garrido-Bañuelos, G.; Lopez-Sanchez, P.; Lundin, L.; Frank, D. Sodium Reduction in Bouillon: Targeting a Food Staple to Reduce Hypertension in Sub-Saharan Africa. Front. Nutr. 2022, 9, 746018. [Google Scholar] [CrossRef] [PubMed]
- Moretti, D.; Hurrell, R.F.; Cercamondi, C.I. Bouillon Cubes. In Food Fortification in a Globalized World; Mannar, M.G.V., Hurrell, R.F., Eds.; Academic Press, 2018; pp. 159–165.
- Nijman, C.A.J.; Zijp, I.M.; Sierksma, A.; Roodenburg, A.J.C.; Leenen, R.; van den Kerkhoff, C.; Weststrate, J.A.; Meijer, G.W. A Method to Improve the Nutritional Quality of Foods and Beverages Based on Dietary Recommendations. Eur. J. Clin. Nutr. 2007, 61, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Dötsch-Klerk, M.; Pmm Goossens, W.; Meijer, G.W.; Van Het Hof, K.H. Reducing Salt in Food; Setting Product-Specific Criteria Aiming at a Salt Intake of 5 g per Day. Eur. J. Clin. Nutr. 2015, 69, 799–804. [Google Scholar] [CrossRef]
- Vlassopoulos, A.; Masset, G.; Charles, V.R.; Hoover, C.; Chesneau-Guillemont, C.; Leroy, F.; Lehmann, U.; Spieldenner, J.; Tee, E.S.; Gibney, M.; et al. A Nutrient Profiling System for the (Re)Formulation of a Global Food and Beverage Portfolio. Eur. J. Nutr. 2017, 56, 1105–1122. [Google Scholar] [CrossRef] [PubMed]
- Vieux, F.; Privet, L.; Masset, G. Food- and Diet-Based Validations of a Nestlé Nutrient Profiling System for Reformulation in Two Nationally Representative Surveys. Br. J. Nutr. 2018, 120, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Fortified Whole Grain Alliance Rwanda. Available online: https://fwg-alliance.org/our-initiatives/rwanda/ (accessed on 30 June 2024).
- Taylor, J.R.N.; de Kock, H.L.; Makule, E.; Hamaker, B.R.; Milani, P. Reduction in Rancidity Development in Fortified Whole-Grain Maize Meal by Hot-Air Drying of the Grain. Cereal Chem. 2024, 101, 323–333. [Google Scholar] [CrossRef]
- Holmes, M.D.; Dalal, S.; Sewram, V.; Diamond, M.B.; Adebamowo, S.N.; Ajayi, I.O.; Adebamowo, C.; Chiwanga, F.S.; Njelekela, M.; Laurence, C.; et al. Consumption of Processed Food Dietary Patterns in Four African Populations. Public Health Nutr. 2018, 21, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- WHO Healthy Diet. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 7 February 2024).
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary Quality among Men and Women in 187 Countries in 1990 and 2010: A Systematic Assessment. Lancet Glob. Heal. 2015, 3, e132–e142. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.; Gavin-Smith, B.; Ferraboschi, C.; Kraemer, K. Food Fortification: The Advantages, Disadvantages and Lessons from Sight and Life Programs. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press (US): Washington, D.C. 2001.
- Assuncąõ, M.C.; Santos, I.S.; Barros, A.J.; Gigante, D.P.; Victora, C.G. Flour Fortification with Iron Has No Impact on Anaemia in Urban Brazilian Children – Corrigendum. Public Health Nutr. 2013, 16, 188–188. [Google Scholar] [CrossRef]
- Engle-Stone, R.; Vosti, S.A.; Luo, H.; Kagin, J.; Tarini, A.; Adams, K.P.; French, C.; Brown, K.H. Weighing the Risks of High Intakes of Selected Micronutrients Compared with the Risks of Deficiencies. Ann. N. Y. Acad. Sci. 2019, 1446, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Noh, M.F.M.; Mustar, R.D.N.G.; Suraiami, A.; Noh, M.F.M.; Mustar, R.D.N.G.; Suraiami, A. Vitamin A in Health and Disease. In Vitamin A; IntechOpen, 2019 ISBN 978-1-78923-946-1.
- Dary, O. Establishing Safe and Potentially Efficacious Fortification Contents for Folic Acid and Vitamin B12. Food Nutr. Bull. 2016, 29. [Google Scholar] [CrossRef] [PubMed]
- Pavlova, K.; Trichkova-Kashamova, E.; Dimitrov, S. Applying a Mathematical Model for Calculating the Ideal Nutrition for Sheep. Mathematics 2024, 12, 1270. [Google Scholar] [CrossRef]
Figure 1.
A sprawling perennial herb (Sesuvium portulacastrum), from the family Aizoaceae, grows in coastal and mangrove areas throughout the world, is a staple food and typical dish (“sirisiri matapa”) in the north of Mozambique. Tropical fruits are abundant.
Figure 1.
A sprawling perennial herb (Sesuvium portulacastrum), from the family Aizoaceae, grows in coastal and mangrove areas throughout the world, is a staple food and typical dish (“sirisiri matapa”) in the north of Mozambique. Tropical fruits are abundant.

Figure 2.
Interdependence among poverty, social exclusion, diseases, human capital, food security, and micronutrient deficiencies.
Figure 2.
Interdependence among poverty, social exclusion, diseases, human capital, food security, and micronutrient deficiencies.
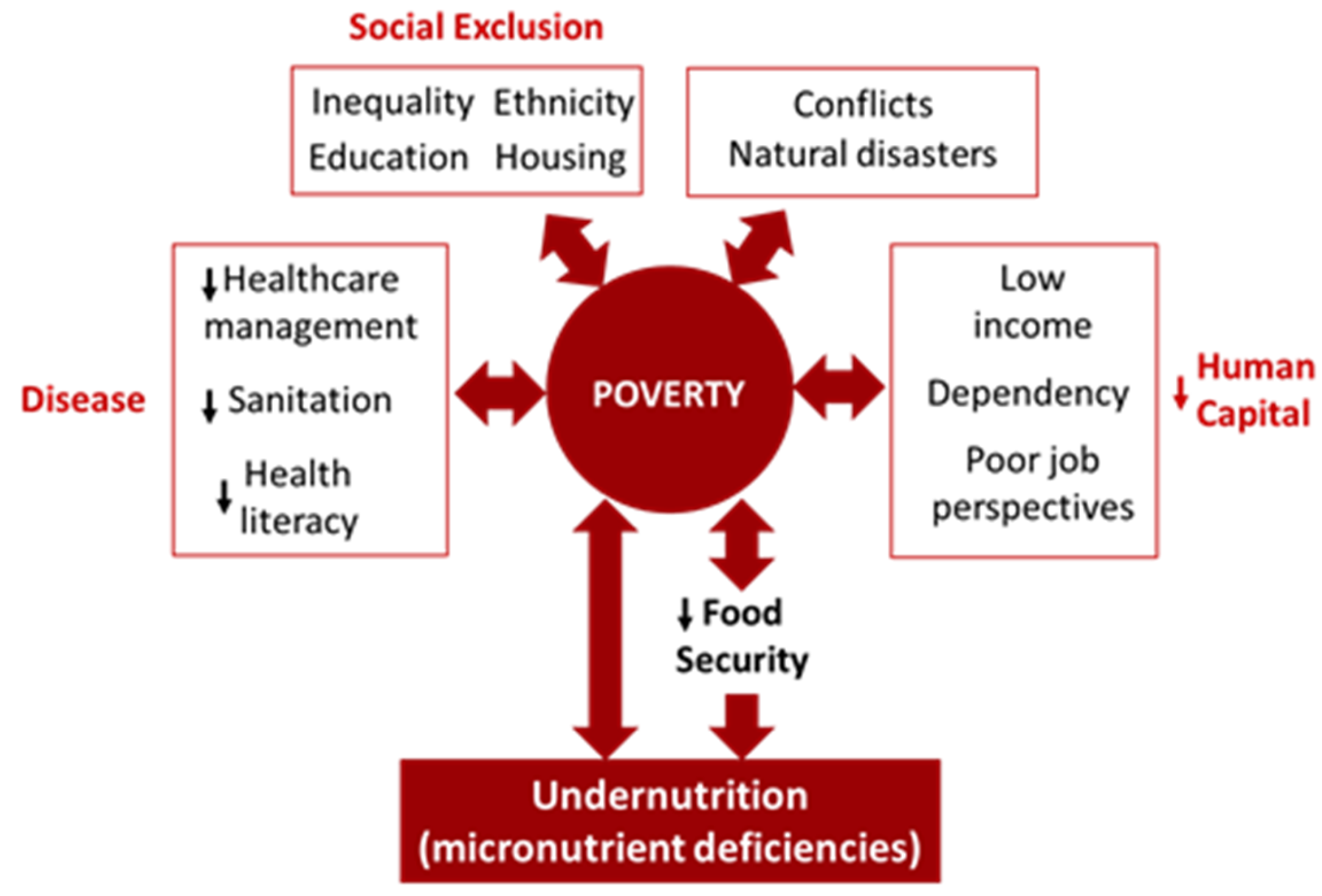
Figure 3.
Fortification versus diversification, reducing micronutrient deficiencies within the holistic concept of One Health.
Figure 3.
Fortification versus diversification, reducing micronutrient deficiencies within the holistic concept of One Health.


Table 1.
Some four main micronutrients are involved in different types of food fortification.
| Iodine | Iron | Vitamin A | Zinc | |
|---|---|---|---|---|
| Condiments | Salt | Sauces (soy, fish) | Sugar | |
| Cereals | Wheat flour, corn flour, pasta, rice | Cereal flours | Cereals | |
| Dairy products | Milk (powder&liquid) | Milk | ||
| Fat & Oils | Oil, margarine | |||
| Vegetables | Potatoes, beans |
Table 2.
A comparison of RAE (retinol activity equivalent) among different food sources.
| Food | RAE per serving (mcg) | Daily Value (%) |
|---|---|---|
| Animal liver 85g | 6600 | 731 |
| Orange flesh sweet potato 100g | 1600 | 156 |
| Spinach 60g | 570 | 64 |
| Pumpkin 130g | 490 | 54 |
| Papaya 100g | 756 | 32 |
Table 3.
Iron levels in common African Foods.
| African Food | Iron (mg/100g FW) |
|---|---|
| Cowpea (Vigna unguiculata) | 4,7 |
| African spinach (Amaranthus caudatus) | 5,9 - 12,7 |
| Algae sirisiri (Sesuvium portulacastrum) | 33,5 |
| Alligator pepper (Aframomum melegueta) | 37,8 |
| Beef liver | 6,7 |
| Locust bean (Leucaena leucocephala) | 33,6 |
| Moringa (Moringa oleifera) leaves | 28 |
| Squash (Pumpkin cucurbita) leaves | 3,2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



