
Submitted:
28 June 2024
Posted:
01 July 2024
You are already at the latest version
Abstract
Background/Objectives: Head and neck free flap reconstructions are often required to treat tumors or extensive post-traumatic jaw defects. The facial artery is the standard receiving vessel for intraoral microvascular anastomoses. However, its use is associated with several disadvantages, such as lesions of buccal nerve branches or the parotid duct and variability in course and diameter. This study aims to investigate whether sublingual artery branches can be considered an alternative intraoral supply vessel to the facial artery to avoid these drawbacks. Methods: 12 formalin-fixed cadaveric heads with 24 sides were dissected. The sublingual artery's origin, course, branching pattern, and distribution were examined. In addition, the diameters of the branches of the sublingual artery were assessed to identify potential supply vessels for anastomoses. Results: In ten of the 24 cases (41.7 %), the sublingual artery originated from the lingual artery and nine cases (37.5 %) from the facial artery. The main trunk of the sublingual artery was present in the floor of the mouth in all cases (100 %) with a diameter of ≥ 0.9 mm in vitro (1 mm in vivo). In 15 of the 24 half heads (62.5 %), branches of the sublingual artery with ≥ 0.9 mm were identified in this space. Conclusions: The large diameter of the sublingual artery on the floor of the mandible suggests that this vessel or its branches could be considered alternative pedicles for intraoral anastomoses in mandibular microvascular free flap grafts.
Keywords:
Sublingual artery
; Pedicle
; Microvascular free flap reconstruction
; Intraoral anastomosis
; Head and neck cancer
; Tumor surgery
1. Introduction
Microvascular free flap grafting is a suitable reconstructive treatment option to ensure tension-free wound coverage of significant defects and fulfill aesthetic and functional aspects. Therefore, appropriate pedicle vessels are crucial for the success of graft vascularization. Conventional extraoral microvascular anastomoses, typically supplied by ventral branches of the external carotid artery, necessitate invasive neck exposure. Alternatively, intraoral microvascular anastomoses can be applied in the treatment where it is not necessary to surgically expose the neck (e.g., benign tumors, post-traumatic defects, etc.) [1,2,3,4]. The procedure is less invasive in these cases, where the neck is not exposed. It avoids morbidities such as impairments of the external appearance due to scarring or damage to the marginal mandibular branch of the facial nerve [5,6]. In addition, less invasive intraoral anastomoses enable short pedicle flaps without interposition grafts. The literature indicates similar success rates when comparing intraoral and extraoral techniques [1,5,6]. However, as the facial artery is the standard receiving vessel for the intraoral procedure, intraoral anastomoses are technically challenging and have several disadvantages limiting the procedure. The approach can injure the buccal branches of the facial nerve or the parotid duct, and the course and diameter of the facial vessels are often unpredictable and variable [6]. To overcome these limitations, using the lingual artery, especially the sublingual artery, may be an alternative source for intraoral anastomosis that may not be associated with such drawbacks. Anatomically, the lingual artery generally arises from the external carotid artery in the carotid triangle; a trunk may occur with the facial artery (linguofacial trunk, 18 %), the superior thyroid artery (thyrolingual trunk, 2 %) or even both (< 1 %) [7]. Under the hypoglossal nerve, the lingual artery takes its course on the middle pharyngeal constrictor muscle medial to the hyoglossus muscle, giving rise to the hyoid branch and the dorsal lingual branches (supply to the root of the tongue and the palatine tonsil). In the sublingual region at the oral border of the hyoglossus muscle, the lingual artery releases the sublingual artery (supply to the sublingual gland and the muscles and mucosa of the floor of the mouth). The lingual artery ends as a ‘deep lingual artery’ running to the tip of the tongue (supply to the tongue muscles). [8] Various studies have examined the course of the lingual artery and its branches in the last decades. Authors proclaimed several classifications [9,10,11,12] and descriptions [9,13] differing from standard anatomical textbooks. However, so far, there is no complete consensus in the literature regarding the origin and appearance of the sublingual artery and the vascular supply of the floor of the mouth. Nakajima et al. observed that the sublingual artery sets off from the lingual artery in only about half of the specimens (in 49 %, the facial artery was the origin) [9]. Shangkuan et al. divided the course of the lingual artery into four segments. They precisely depicted the appearance and diameter of these segments but without applying this to the sublingual artery and its arterial supply to the floor of the mouth [10]. This study performs a comprehensive anatomical investigation of the course, appearance, diameter, and branching pattern of the lingual and sublingual artery and its branches to evaluate its reliability as a potential alternative pedicle for intraoral anastomoses in head and neck free flap reconstruction.
2. Materials and Methods
12 formalin embalmed human cadaver heads (nine females, three males) with 24 sides (n = 24; 12 right and 12 left) were acquired for this study [14]. The bodies were donated by people who had given their informed consent for their use for scientific and educational purposes before death. The specimens had a mean age at death of 83.2 years (62-93 years) and a mean height of 164 cm (range: 151-175 cm). None of the corpses showed any evidence of trauma, previous surgery, or gross pathology to the head and neck region.
The following anatomical dissection protocol was applied: The skin, platysma, subcutaneous tissue, and two superficial layers of the cervical fascia were removed to expose the external carotid artery in the anterior cervical region. The lingual artery was identified and followed distal. The digastric muscle, stylohyoid muscle, connective tissue, and fat were resected to get a closer overview. The mylohyoid muscle was split longitudinally, and the hyoglossus muscle transversally to the muscle fibers and unfolded. All branches of the lingual artery and accompanying veins were carefully traced up to the horizontal section of the tongue. The sublingual artery was precisely revealed on the floor of the mouth with all branches up to the insertion in the mandible.
The course, branching pattern, and distribution of the lingual and the sublingual artery were examined using the segment classification of Shangkuan and surveyed with a tape measure (XD P113.432, XD Collection, China) [10]. Documentation was made photographically using a high-resolution camera (iPhone XR ®, Apple Inc., USA). All branches of the arterial vessels mentioned above were assessed for their inner luminal diameter with a 0.9 mm stylet (Vasocan ®, 22 G / 0.9 x 25 mm, B. Braun, Germany). Figure 1 illustrates the technical procedure.
A luminal diameter of 1 mm was defined as the lowest limit since in vivo microvascular anastomoses can be performed surgically from this caliber. However, as this is an in vitro study, the specimens’ shrinkage of the arteries due to contraction caused by the loss of pressure and embalming must be considered. According to Danesh-Meyer et al., this shrinkage amounts to about 8 % [15]. Therefore, the stylet was chosen in size described previously.
The measurement parameters’ mean, range, and standard deviation (SD) were determined. Descriptive statistics were calculated using Excel (Microsoft Office, Microsoft Corp., USA).
3. Results
- Anatomical findings:
The lingual artery was found and exposed in all specimens (100%). In 17 of the 24 hemiheads (70.8 %), the lingual artery originated from the external carotid artery. A linguofacial trunk was found in six (25 %) and a thyrolingual trunk in one (4.2 %) case. In the original segment (classification of Shangkuan et al.), an average of 1.4 branches (range: 0-3 branches) arose from the lingual artery. These branches most frequently coursed downwards to supply the hyoid bone. 57.6 % of these branches had less, while 42.4 % had at least 0.9 mm inner diameter. Within the hyoglossus segment, 3.2 branches ( 1-6 branches) averagely originated from the lingual artery. Up to four dorsal lingual branches most frequently lead upwards to supply the root of the tongue and the palatine tonsil. 38.5 % of these branches had less, while 61.5 % had at least 0.9 mm luminal diameter. Also, up to four branches coursed downwards to the hyoid bone or the surrounding muscles. 54.5 % of these branches had less, while 45.5 % had at least 0.9 mm luminal diameter. On five sides, the sublingual artery arose in this segment, most frequently leading downwards. All these sublingual arteries had at least 0.9 mm luminal diameter. In the ascending segment, an average of 3.5 branches ( 1-7 branches) arose from the lingual artery. These branches most frequently coursed upwards to supply the tongue muscles. 79.5 % of these branches had less, while 20.5 % had at least 0.9 mm inner diameter. The sublingual artery arose in this segment on ten sides, always leading downwards. 80% of these sublingual arteries had a luminal diameter of at least 0.9 mm, while 20% had a smaller diameter. Length measurements of the lingual artery are shown in Table 1.
The sublingual artery was found and exposed in all specimens (100%). In ten of the 24 cases (41.7 %), the sublingual artery originated from the lingual artery (Figure 2 and Figure 3).
The facial artery gave rise to the sublingual artery in nine cases (37.5 %) (Figure 4).
The sublingual artery was present twice on four sides (16.7 %). One sublingual artery originated from the facial artery, and the other from the lingual artery. In one case (4.2 %), an anastomosis was found between the facial artery and the lingual artery in addition to a sublingual artery arising from the lingual artery. From the point of origin to the insertion in the mandible, the straight length averaged 36.1 mm (range: 12-59 mm; SD: ± 9.3 mm), and the stretched length averaged 47.1 mm (range: 15-70 mm; SD: ± 13.2 mm). The main trunk of the sublingual artery was present on the floor of the mouth in all cases (100 %) and had a diameter of ≥ 0.9 mm. On average, the sublingual artery set off four branches (range: 1-11 branches). Most frequently, these branches coursed upwards to supply the sublingual gland and the muscles and mucosa of the floor of the mouth. In 15 of the 24 hemiheads (62.5 %), at least one branch was found with not less than 0.9 mm luminal diameter. In four of these 15 sites, two branches and in one of the 15 sites, four branches with a luminal diameter of at least 0.9 mm were found. Figure 2 shows this vividly. In nine of the 24 cases (37.5 %), no branch with an inner diameter of at least 0.9 mm lumen was identified. In four of these nine sites, the sublingual artery was marginally present.
A fascia layer between the mylohyoid and the hyoglossus muscle was found in each specimen (Figure 2 and Figure 3). Branches of the mandibular nerve ran through this layer.
Clinical Application:
The main trunk of the sublingual artery or its large caliber branches seem suitable for intraoral anastomoses. To approach these vessels from enoral, a sagittal incision through the anterior oral mucosa is required. Care must be taken to ensure that the incision and subsequent dissection are not made in the lateral area of the floor of the mouth to preserve the lingual nerve, the Warton duct, and the sublingual glandular tissue. The genioglossus muscle serves as a guide structure for identifying the sublingual artery. The vessel can be mobilized from the depths cranially to the mylohyoid muscle. Figure 5 illustrates this access procedure.
4. Discussion
Surgical treatment in the head and neck area can result in extensive defects compromising soft and hard tissue structures. Such interventions require sufficient reconstruction to enable patients’ aesthetic and functional rehabilitation. Microvascular grafts such as the radial forehand flap or the osteocutaneous fibula graft can be used for this purpose. Decisive for success is tension-free wound coverage and sufficient anastomoses of the pedicle vessels to ensure flap survival. These supply anastomoses are conventionally conducted via extraoral approaches using external carotid branches. However, this implies an invasive dissection of the neck, which leads to comorbidities and scarring. Several studies describe an alternative intraoral approach for cases in which neck dissection is not necessitated. The range of indications includes benign neoplasms or jaw defects following traumatic injuries, as well as fibrous dysplasia and cleft palates [1,2,3,4,16,17]. This intraoral technique eliminates morbidities such as impairment of the external appearance or lesions of the facial nerve’s marginal mandibular branch [5,6]. Furthermore, short pedicle flaps can be utilized without interposition grafts [1,6]. Previous studies have shown similar success rates compared to extraoral techniques [1,5,6]. Kämmerer et al. reported total flap loss in two of 130 cases (1.5%) and Brandtner et al. in one of 70 cases (1.4%) [1,6]. In this study, with a high probability of occurrence, in the floor of the mouth, the main trunk and branches of the sublingual artery were identified that could be used for intraoral anastomoses (diameter ≥ 0.9 mm in vitro and 1 mm in vivo). The decisive advantage of this recipient vessel over the facial artery is that, due to its different topographical course, injury to the parotid duct or the buccal nerve branches can be ruled out [6]. In addition, these sublingual vessels are easier to localize, as they do not run deep in the cheek like the facial artery and are not protected by fatty tissue and muscles. Due to the topographical course beneath the oral mucosa, it would be predestined for reconstructive surgery in the mandibular region. Compared to the facial artery, this surgical access route is technically less difficult and not as restricted in terms of diameter size [6]. Most of the previous anatomical studies concerning the sublingual artery in detail were conducted on the Asian population [9,10,11,12,18]. In contrast, this study was conducted on a sample of the Central European population to provide results from a different ethnic group. More precisely, the specimens donated to the Division of Clinical and Functional Anatomy of the Medical University of Innsbruck constituted a representative sample of the Austrian population [19]. In this investigation, the definition of Shangkuan was applied to classify the course of the lingual artery (the original segment, the segment within the hyoglossus, and the ascending segment). The fourth segment (the horizontal segments of the deep lingual artery) was not implemented because the intralingual section of the lingual artery was not part of the study objectives. Shangkuan et al. provided decent anatomical bases for tongue flaps, while we focused on the floor of the mouth to investigate a potential application for mandibular microvascular reconstruction [10]. Instead of ascertaining absolute measurements, we chose the technique with the stylet to determine the inner luminal diameters of the branches, as the specimens surveyed had no vascular pressure. According to Danesh-Meyer et al., the arteries’ shrinkage of 8 % to 10 % arose mainly due to contraction caused by the loss of pressure rather than the embalming process with formalin [15]. Therefore, this method seemed to be the best way to acquire data that was closest to the artery condition in vivo. Former publications showed different origins of the sublingual artery [9,12,20]. Loukas et al. found the sublingual artery originating from the lingual artery in 73 % and the submental artery in 23 % of their 100 examined cadaveric heads [20]. In the study of Masui et al., the sublingual artery set off from the lingual artery in 60 %, from the facial artery near the origin of the submental artery in 12 %, from the proximal portion of the submental artery in 5 %, and from a distal portion of the submental artery in 19 % of their 101 cases [12]. Nakajima et al. concluded that the probability of the sublingual artery arising from the facial or lingual artery is about the same after dissecting their 75 cadaveric heads [9]. Our samples confirmed this, where the sublingual artery arose from the lingual artery in less than half of the cases. The different courses of the sublingual artery may be of considerable anatomical significance. Still, clinically and functionally, they are decisive, as peripheral large-caliber branches are present to supply the mucosa of the floor of the mouth. These branches do not necessarily originate from the sublingual artery. Supply patterns have been reported suggesting that the submental artery (facial artery) may also extend into the sublingual space (by piercing the mylohyoid muscle) to release supply branches to the floor of the mouth when the sublingual artery is less prominent present [13,18]. Loukas et al. found the mucosal branches with a mean diameter of 0.9 mm in the lateral incisor region in 72 %, the canine region in 62 %, and the first premolar region in 81 % of their 100 cadaveric heads examined [20]. Our already sufficiently described findings of the large caliber branches of the sublingual artery combined with the findings of Loukas et al. [20] are highly relevant from the clinical point of view, as they indicate that reliable pedicle branches of the sublingual artery occur with a remarkable percentage. The diameter cut-off was set at 0.9 mm in vitro (1 mm in vivo) in this investigation because, in our experience, microvascular anastomoses of this caliber can be safely performed surgically, especially if the pedicle feeds more component flaps or large-size flaps needing high-volume perfusion. Calibers smaller than 1 mm were not calculated in this study. However, numerous studies in the literature describe techniques for using smaller luminal diameters down to 0.3 mm [21,22,23,24]. When this is considered, our data must be interpreted differently, as the number of usable branches of the sublingual artery would increase significantly.
The following limitations regarding this study should be mentioned: Measurements were performed manually and evaluated macroscopically with a tape measure, which unintentionally may lead to slight deviations in the measurement process. However, this seems negligible, as the data collected only diverge in the low micrometer range. As already described comprehensively, we used the stylet to determine the calibers of the arteries and did not additionally survey the absolute measurements to avoid additional bias. Even though we have considered the specimens’ shrinkage of the arteries (according to the literature [15]), there is most likely a slight difference between the in vitro study situation and an in vivo clinical setting. Future research should also focus on the venous recipient vessels since this paper did not address the venous system. Although a higher case number would probably provide more validation to the findings of this study, anatomical cadaver studies with similar case numbers can be found in the literature. This study provides preliminary results of the sublingual artery.
5. Conclusions
The sublingual artery is equally likely to originate from the facial or lingual arteries. The main trunk and large caliber branches of the sublingual artery (diameter ≥ 0.9 mm in vitro or 1 mm in vivo) were identified on the floor of the mouth. The high probability of occurrence suggests that these vessels could be considered alternative pedicles for anastomoses in microvascular free flap grafts. Due to the location of these branches directly under the mucosa in the mandibular region, they appear surgically accessible without significant limitations. This study provides the anatomical basis that the sublingual artery branches constitute a potential alternative for intraoral anastomosis. An upcoming project in a clinical setting is planned to prove this study’s results.
Author Contributions
Conceptualization, VS, RS, JW, EB; methodology, VS, RS, JW, SM, JM, EB; software, VS, EB; validation, VS, RS, JW, SM, JM, EB; formal analysis, VS, EB; investigation, VS, RS, JW, SM, JM, EB; resources, EB; data curation, VS; writing—original draft preparation, VS, JW, EB, SM, JM; writing—review and editing, VS, RS, JW, SM, JM, EB; visualization, VS, SM, EB, JW; supervision, VS, RS, JW, SM, JM, EB; project administration, EB; funding acquisition, EB All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable (This article does not contain any studies with living human participants or animals performed by the authors.)
Informed Consent Statement
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Findings derived from such research endeavors have the potential to augment humanity’s collective understanding, subsequently enhancing the quality of patient care. Therefore, these donors and their families deserve our highest gratitude.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brandtner, C.; Bürger, H.; Hachleitner, J.; Gaggl, A. The intraoral anastomosing technique in reconstructive surgery of the face–A consecutive case series of 70 patients. Journal of Cranio-Maxillofacial Surgery 2015, 43, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Gaggl, A.; Bürger, H.; Virnik, S.; Chiari, F. An intraoral anastomosing technique for microvascular bone flaps in alveolar ridge reconstruction: first clinical results. International journal of oral and maxillofacial surgery 2009, 38, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Agaimy, A.; von Wilmowsky, C.; Eitner, S. Mandibular reconstruction using intraoral microvascular anastomosis following removal of an ameloblastoma. Journal of Oral and Maxillofacial Surgery 2013, 71, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, J.; Lv, M.M.; Wang, L.; Gupta, A.; Shen, Y. Expanded Transoral Microvascular Mandibular Reconstruction: A Scar-Free Approach. J Oral Maxillofac Surg 2022, 80, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-Y.; Shao, Z.; Jia, J.; Liu, B.; Bu, L.-L. Analysis of intraoral microvascular anastomosis in maxillofacial defects reconstruction. Journal of Cranio-maxillo-facial Surgery: Official Publication of the European Association for Cranio-maxillo-facial Surgery, 2023, S1010-5182 (1023) 00008. [Google Scholar]
- Kämmerer, P.W.; Tavakoli, M.; Gaggl, A.; Maranzano, M. Intraoral Microvascular Anastomosis in Immediate Free Flap Reconstruction for Midfacial Tumor Defects: A Retrospective Multicenter Study. Journal of Clinical Medicine 2023, 12, 7064. [Google Scholar] [CrossRef] [PubMed]
- Lippert, H.; Pabst, R. Arterial variations in man: classification and frequency; Springer Verlag: 1985.
- von Lanz, T.; Wachsmuth, W. Praktische Anatomie: ein Lehr-und Hilfsbuch der anatomischen Grundlagen ärztlichen Handelns; Springer-Verlag: 2013.
- Nakajima, K.; Tagaya, A.; Otonari-Yamamoto, M.; Seki, K.; Araki, K.; Sano, T.; Okano, T.; Nakamura, M. Composition of the blood supply in the sublingual and submandibular spaces and its relationship to the lateral lingual foramen of the mandible. Oral Surg Oral Med Oral Pathol Oral Radiol 2014, 117, e32–38. [Google Scholar] [CrossRef] [PubMed]
- Shangkuan, H.; Xinghai, W.; Zengxing, W.; Shizhen, Z.; Shiying, J.; Yishi, C. Anatomic bases of tongue flaps. Surg Radiol Anat 1998, 20, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Seki, S.; Sumida, K.; Yamashita, K.; Baba, O.; Kitamura, S. Gross anatomical classification of the courses of the human lingual artery. Surg Radiol Anat 2017, 39, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Masui, T.; Seki, S.; Sumida, K.; Yamashita, K.; Kitamura, S. Gross anatomical classification of the courses of the human sublingual artery. Anat Sci Int 2016, 91, 97–105. [Google Scholar] [CrossRef]
- Bavitz, J.B.; Harn, S.D.; Homze, E.J. Arterial supply to the floor of the mouth and lingual gingiva. Oral Surg Oral Med Oral Pathol 1994, 77, 232–235. [Google Scholar] [CrossRef]
- Platzer, W.; Putz, R.; Poisel, S. Ein neues Konservierungs-und Aufbewahrungssystem für anatomisches Material. Cells Tissues Organs 1978, 102, 60–67. [Google Scholar] [CrossRef]
- Danesh-Meyer, H.V.; Savino, P.J.; Bilyk, J.R.; Eagle, R.C.; Sergott, R.C. Shrinkage: fact or fiction? Archives of Ophthalmology 2001, 119, 1217–1217. [Google Scholar] [PubMed]
- Sosin, M.; Sinada, G.G.; Rodriguez, E.D.; Dorafshar, A.H. Intraoral microvascular anastomosis of an iliac free flap for maxillary fibrous dysplasia. Journal of Oral and Maxillofacial Surgery 2015, 73, 2068–e2061. [Google Scholar] [CrossRef] [PubMed]
- Landes, C.; Cornea, P.; Teiler, A.; Ballon, A.; Sader, R. Intraoral anastomosis of a prelaminated radial forearm flap in reconstruction of a large persistent cleft palate. Microsurgery 2014, 34, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Katsumi, Y.; Tanaka, R.; Hayashi, T.; Koga, T.; Takagi, R.; Ohshima, H. Variation in arterial supply to the floor of the mouth and assessment of relative hemorrhage risk in implant surgery. Clinical Oral Implants Research 2013, 24, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Konschake, M.; Brenner, E. “Mors auxilium vitae”—Causes of death of body donors in an Austrian anatomical department. Annals of Anatomy-Anatomischer Anzeiger 2014, 196, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Loukas, M.; Kinsella Jr, C.R.; Kapos, T.; Tubbs, R.S.; Ramachandra, S. Anatomical variation in arterial supply of the mandible with special regard to implant placement. International journal of oral and maxillofacial surgery 2008, 37, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Harii, K. Microvascular surgery in plastic surgery: Free-tissue transfer. Microsurgery 1979, 1, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W. Lymphaticovenular bypass for lymphedema management in breast cancer patients: a prospective study. Plastic and reconstructive surgery 2010, 126, 752–758. [Google Scholar] [CrossRef]
- Kim, J.S.; Choi, T.H.; Kim, N.G.; Lee, K.S.; Han, K.H.; Son, D.G.; Kim, J.H.; Lee, S.-I.; Kang, D. The replantation of an amputated tongue by supermicrosurgery. Journal of plastic, reconstructive & aesthetic surgery 2007, 60, 1152–1155. [Google Scholar]
- Liu, H.-L. Microvascular anastomosis of submillimeter vessels—a training model in rats. Journal of hand and microsurgery 2013, 5, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Riederer, B.M.; Bolt, S.; Brenner, E.; Bueno-López, J.L.; Circulescu, A.R.; Davies, D.; Caro, R.d.; Gerrits, P.; McHanwell, S.; Pais, D. The legal and ethical framework governing body donation in Europe–1st update on current practice. 2012.
- McHanwell, S.; Brenner, E.; Chirculescu, A.R.; Drukker, J.; van Mameren, H.; Mazzotti, G.; Pais, D.; Paulsen, F.; Plaisant, O.; Caillaud, M.M. The legal and ethical framework governing Body Donation in Europe-A review of current practice and recommendations for good practice. European Journal of Anatomy 2020, 12, 1–24. [Google Scholar]
Figure 1.
Technical method to assess the branch diameter with a 0.9 mm stylet. m: mandible; view from caudal.
Figure 1.
Technical method to assess the branch diameter with a 0.9 mm stylet. m: mandible; view from caudal.
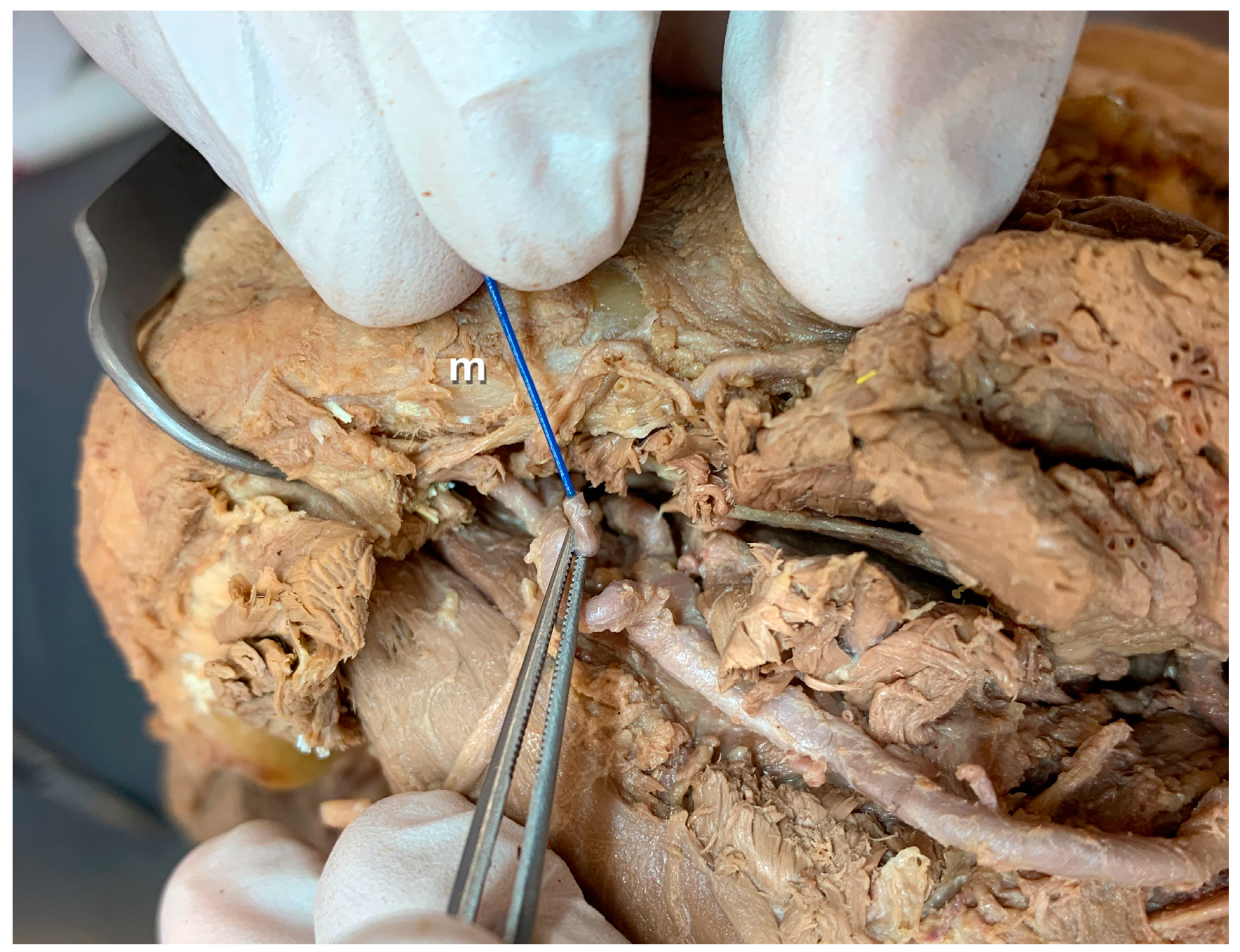
Figure 2.
The sublingual artery branching off the lingual artery—Overview. fl: facial layer, gm: geniohyoid muscle, l: lingual artery, l2: hyoglossus segment, l3: ascending segment, m: mandible(angle), mm: mylohyoid muscle, s: sublingual artery;
Figure 2.
The sublingual artery branching off the lingual artery—Overview. fl: facial layer, gm: geniohyoid muscle, l: lingual artery, l2: hyoglossus segment, l3: ascending segment, m: mandible(angle), mm: mylohyoid muscle, s: sublingual artery;
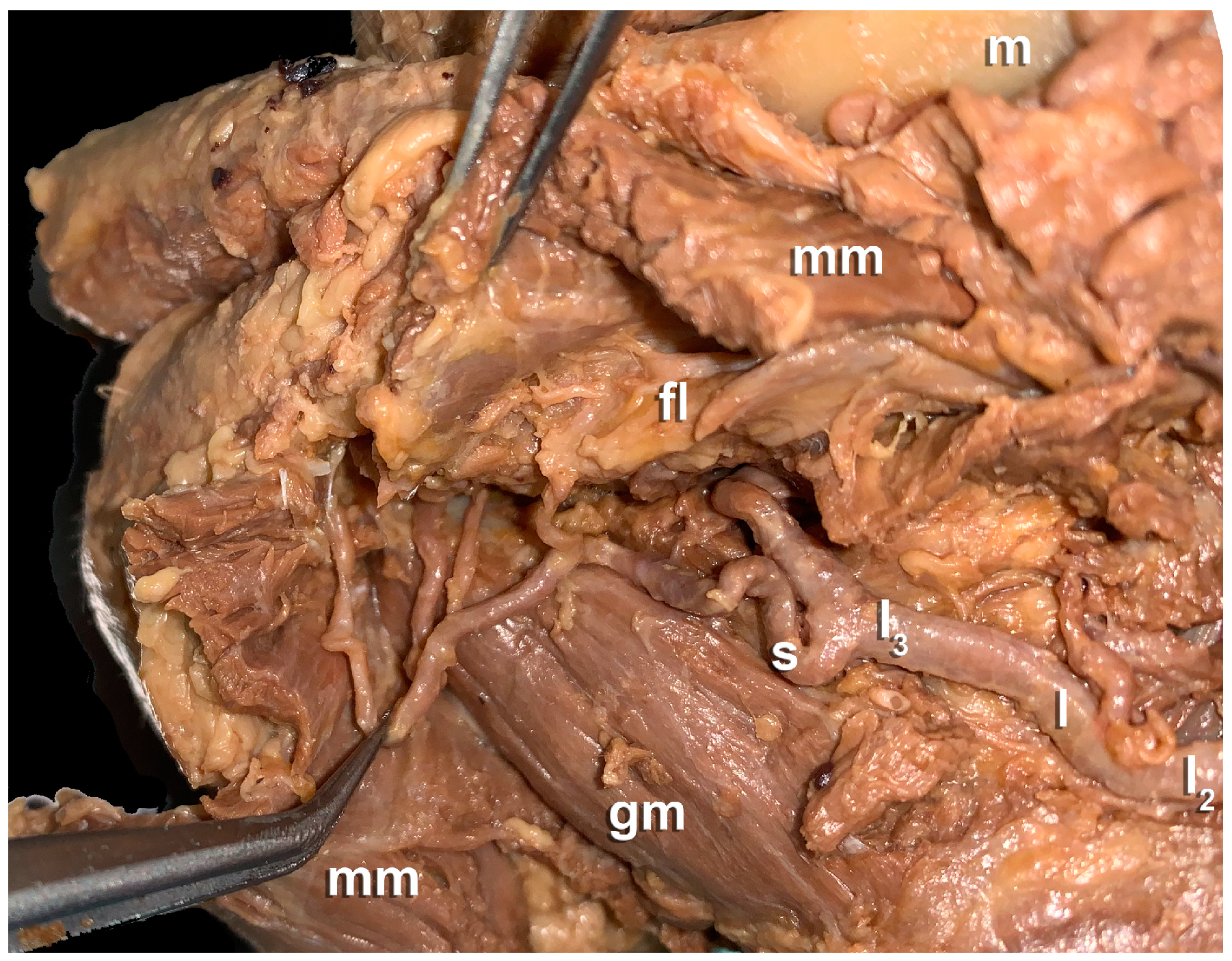
Figure 3.
The sublingual artery branching off the lingual artery—Detailed illustration. dm: digastric muscle, fl: facial layer, gm: geniohyoid muscle, hm: hyoglossus muscle, l: lingual artery, l1: original segment, l2: hyoglossus segment, l3: ascending segment, m: mandible, mm: mylohyoid muscle, s: sublingual artery;
Figure 3.
The sublingual artery branching off the lingual artery—Detailed illustration. dm: digastric muscle, fl: facial layer, gm: geniohyoid muscle, hm: hyoglossus muscle, l: lingual artery, l1: original segment, l2: hyoglossus segment, l3: ascending segment, m: mandible, mm: mylohyoid muscle, s: sublingual artery;
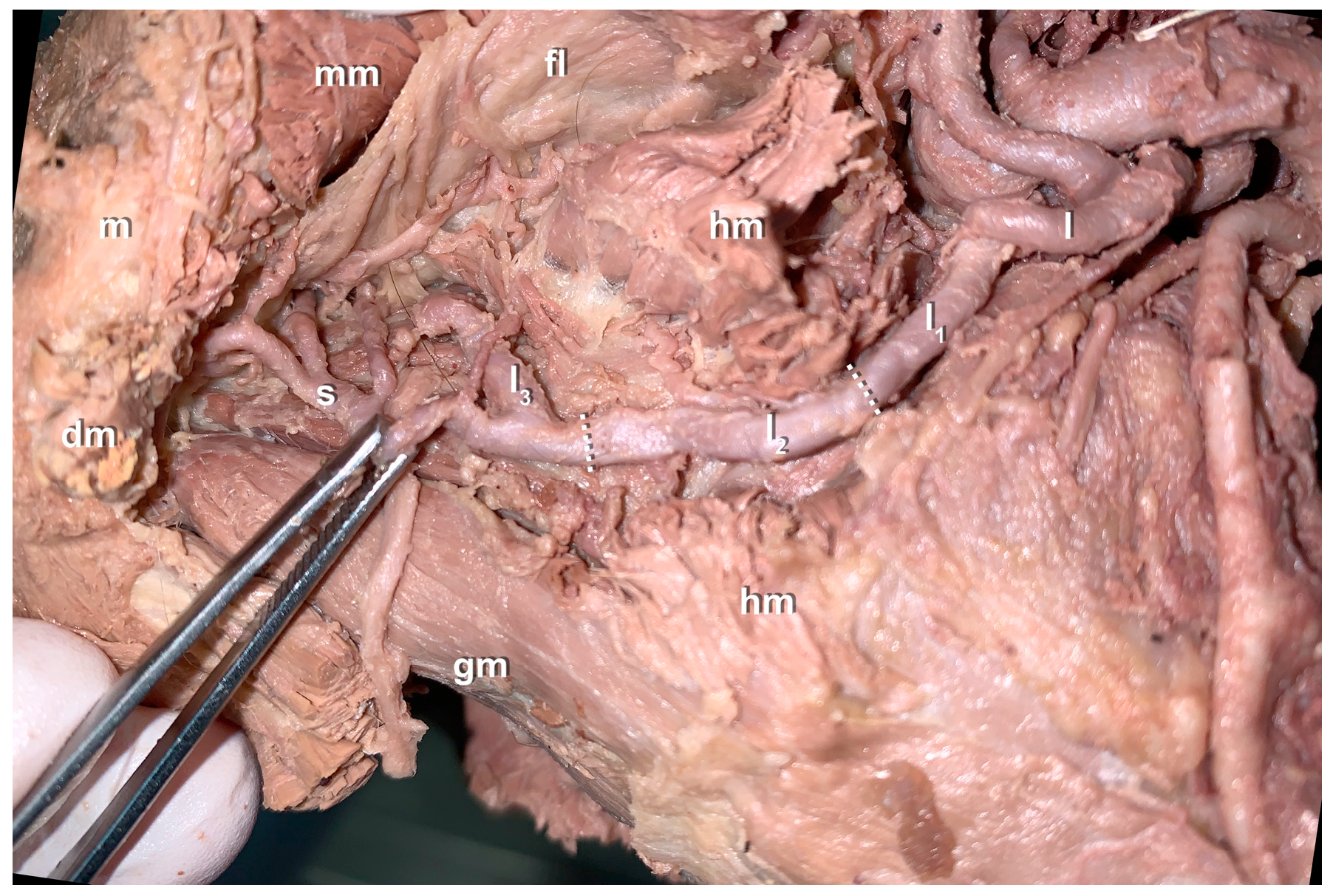
Figure 4.
The sublingual artery branching off the facial artery. dm: digastric muscle, f: facial artery, gm: geniohyoid muscle, m: mandible(angle), mm: mylohyoid muscle, s: sublingual artery;
Figure 4.
The sublingual artery branching off the facial artery. dm: digastric muscle, f: facial artery, gm: geniohyoid muscle, m: mandible(angle), mm: mylohyoid muscle, s: sublingual artery;
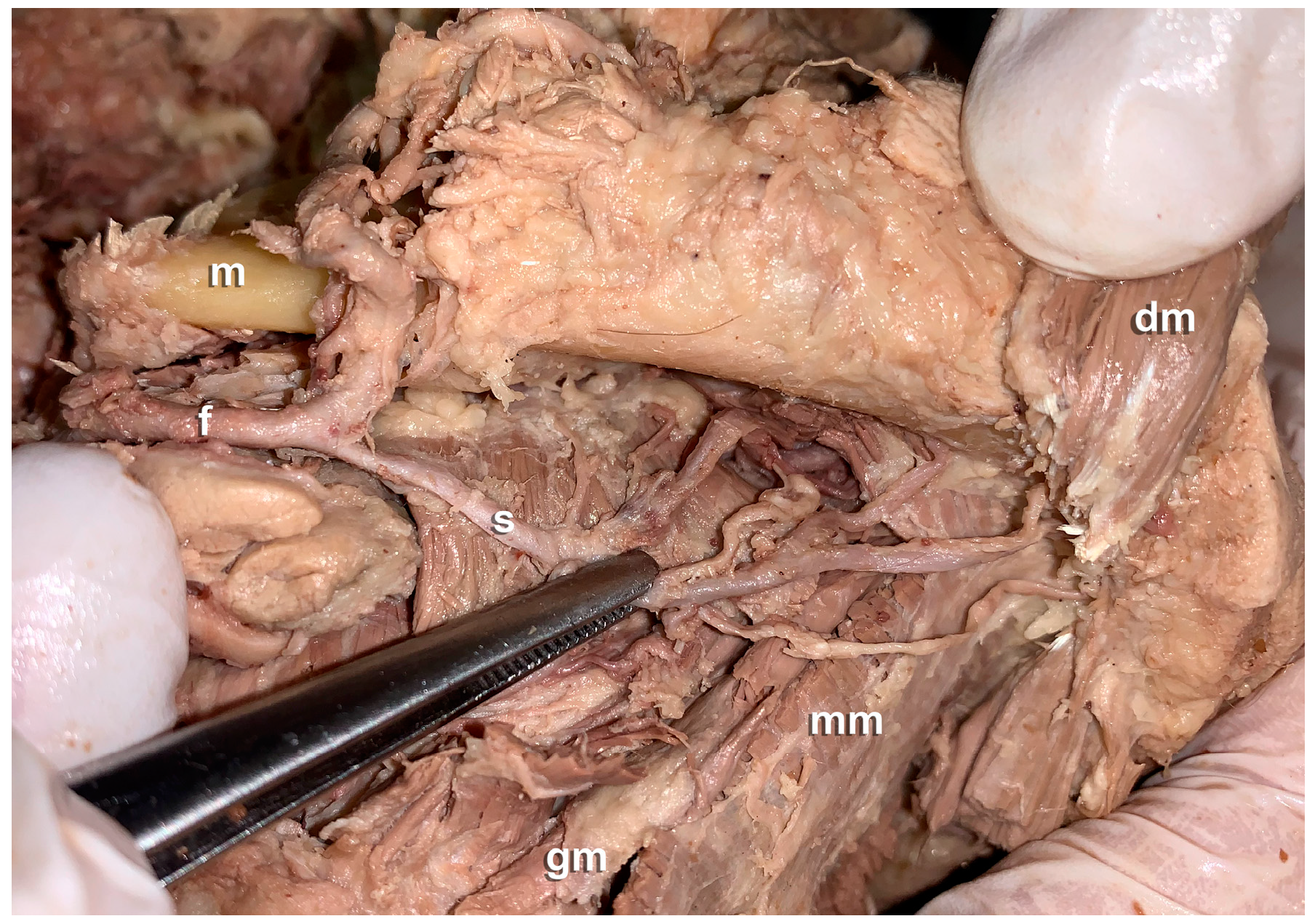
Figure 5.
Access procedure A shows the incision of the oral mucosa to access the anterior floor of the mouth (red line); particular care must be taken to ensure that the incision is not made further laterally to avoid injury to the lingual nerve the Warton duct and the sublingual glandular tissue; the tongue (post-mortem black tongue discoloration) was retained; B and C show the mobilized main trunk of the sublingual artery in the sublingual space with the accompanying vein; the tongue was hemidissected to provide a better overview. Hence, the dorsal root artery was also cut; D shows the sectioned lumen of the main trunk of the sublingual artery (caliper gauge: vessel diameter 2.2 mm);c d: dorsal root artery (lingual artery), genioglossus muscle, m: mandible, s: sublingual artery, v: accompanying sublingual vein;.
Figure 5.
Access procedure A shows the incision of the oral mucosa to access the anterior floor of the mouth (red line); particular care must be taken to ensure that the incision is not made further laterally to avoid injury to the lingual nerve the Warton duct and the sublingual glandular tissue; the tongue (post-mortem black tongue discoloration) was retained; B and C show the mobilized main trunk of the sublingual artery in the sublingual space with the accompanying vein; the tongue was hemidissected to provide a better overview. Hence, the dorsal root artery was also cut; D shows the sectioned lumen of the main trunk of the sublingual artery (caliper gauge: vessel diameter 2.2 mm);c d: dorsal root artery (lingual artery), genioglossus muscle, m: mandible, s: sublingual artery, v: accompanying sublingual vein;.
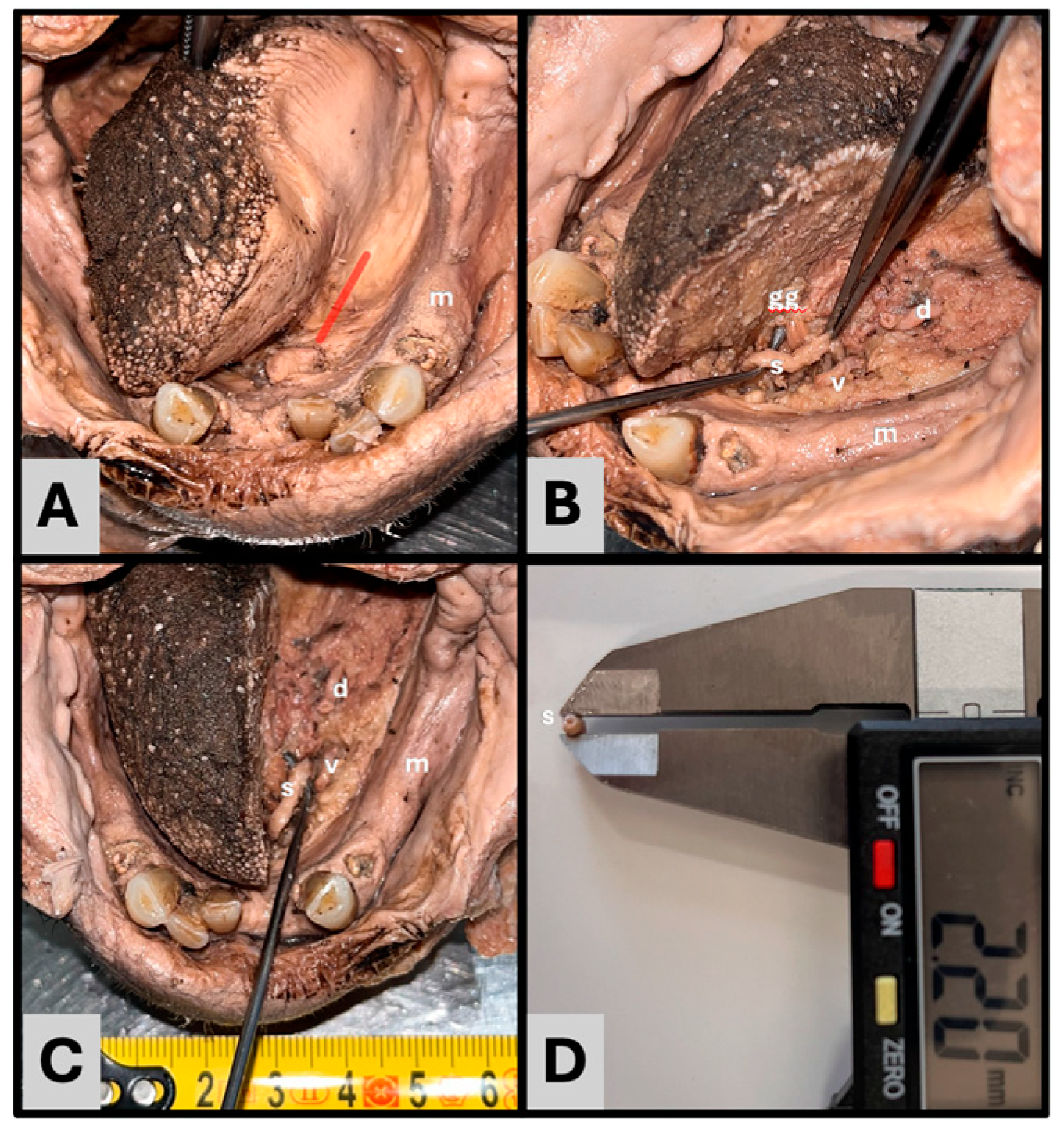

Table 1.
Length measurements of the lingual artery.
| Straight length | Stretched length | |
| Original segment | 21.9 ± 6.6 (7-30) | 39 ± 13.3 (20-70) |
| Segment within the hyoglossal muscle | 20.4 ± 5.0 (11-30) | 25.2 ± 7.8 (11-42) |
| Ascending segment of the deep lingual artery | 18.9 ± 5.2 (13-34) | 23.1 ± 5.5 (13-39) |
The distances in mm are reported as mean ± standard deviation and (range) measured in 12 hemiheads (n = 24). n: number;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



