
Submitted:
06 June 2024
Posted:
07 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The persistence of symptoms following COVID-19 infection represents a significant challenge in healthcare management. During the outbreak, tele-rehabilitation emerged as a new tool to support healthcare structures in providing rehabilitation services. This study assessed the effectiveness and the feasibility of a 3-week home-based motor and respiratory rehabilitation program for long COVID-19 individuals after traditional rehabilitation. Twenty-three patients completed the program and underwent functional tests at different time points (i.e. baseline, after hospital discharge, and after tele-rehabilitation). Motor function was evaluated using the instrumented Six-Minutes Walking Test (i6MWT), with monitored heart rate and oxygen saturation. Conversely, respiratory function was measured via forced vital capacity (FVC) and maximal voluntary ventilation (MVV) tests. Significant improvements (p < 0.05) in motor and respiratory function were observed throughout the intervention, including an 18.3% increase in walked distance from the baseline. The findings suggest that a home-based tele-rehabilitation can enhance motor and respiratory function in post-COVID patients. Despite limitations such as sample size and lack of control group, the positive outcomes seem to support the feasibility of the proposed tele-rehabilitation program in managing long COVID symptoms and promoting functional recovery. Further research is needed to validate these findings and explore tele-rehabilitation’s potential in broader patient populations.
Keywords:
COVID-19
; long COVID
; rehabilitation
; tele-rehabilitation
; motor rehabilitation
; respiratory rehabilitation
1. Introduction
“Long COVID”, also known as “post-COVID syndrome”, is a term used to describe presence of various symptoms persisting even weeks or months after acquiring SARS-CoV-2 infection, and it can affect anyone exposed to the virus, regardless of age or severity of original symptoms [Sugiyama 2024, Raveendran 2021; Bures 2021]. The World Health Organization (WHO) defines it as the condition occurring in individuals with a history of probable or confirmed SARS-CoV-2 infection, typically commencing three months post-onset of COVID-19 and which symptoms last for at least two months and cannot be attributed to an alternate diagnosis [1,2,3].
The prevalence of long COVID symptoms recorded varies depending on the study subjects and methods, but it has been reported that 10–20% of individuals experience a variety of mid and long-term effects after they recover from their initial illness [4]. COVID-19 pandemic has brought significant challenges to the global healthcare system, both in managing patients in the disease’s acute phase, but also in treating those COVID-19 patients who have experienced symptoms lasting over time (Raveendran 2021; Bures 2021). Long COVID can present with several symptoms: the most common include fatigue, breathing difficulties, dyspnoea, muscle weakness and headache [1,5,6], but also mental disorders (i.e. attention deficit, sleep disturbance, depression), olfactory and gustatory dysfunction, and some more severe symptoms affecting respiratory, cardiovascular and gastrointestinal systems have been reported [1,5,7]. There is evidence that these long-term symptoms can also occur in people who have mild or no symptoms during acute infection [8,9], resulting in a lower quality of life and in greater difficulties to perform daily living activities (i.e., walking, climbing stairs or lifting) [6].
Long COVID-19 syndrome has significantly impacted global health, affecting an estimated 65 million people [10,11], and it has been recognized as a public health problem requiring appropriate rehabilitation interventions from the acute to the post-acute phase [2,12,13]. Rehabilitation plays a key role in the functional recovery of long-COVID-19 patients and should be targeting mainly the respiratory and motor symptoms [2]. Since COVID-19 infections have been linked to respiratory problems [14,15], respiratory rehabilitation is a desirable treatment approach for these patients, as pulmonary rehabilitation has been shown to be effective in improving respiratory function in several respiratory diseases, such as chronic obstructive pulmonary disease (COPD) or asthma [16,17,18,19,20]. Moreover, patients who have been infected with COVID-19 often complain of fatigue, and muscle weakness, making it necessary for them to participate in targeted and interactive programs focused on improving their physical activity levels [21].
During the COVID-19 outbreak, the access to traditional rehabilitation had to be rethought. Many components of rehabilitation do indeed require patient contact, but the physical distancing for protection of both healthcare workers and patients could result in increased disability and morbidity due to the lack of necessary rehabilitation services [22]. To cope with this new situation, the use of telerehabilitation was introduced as a strategy to provide rehabilitation services remotely, with the aim of improving and facilitating access to rehabilitation [22]. Previous research has demonstrated the beneficial effects of tele-rehabilitation and tele-coaching on patients with idiopathic pulmonary fibrosis and chronic obstructive pulmonary disease (COPD) in terms of symptom severity reduction, increased physical activity and exercise capacity, and health-related quality of life [21,23,24,25]. Furthermore, according to a recent systematic review telerehabilitation could be an effective tool for the treatment of persistent symptoms in patients who suffered from COVID-19 infection, improving their physical performance and quality of life [26]. Even though the COVID-19 pandemic lockdowns are currently over, health systems are encouraged to adopt telemedicine practices for strengthening healthcare delivery, and telerehabilitation may still be regarded as a practical way to care for patients since it is a practical and easily accessible tool that enables long-distance communication and follow-up via Information and Communication Technology (i.e. telephone, internet-based applications and mobile applications) [6,22,27]. Moreover, according to a recent Cochrane Review [28] many patients see telerehabilitation as affordable and cost-saving if the equipment and infrastructure have been provided.
Taking all these aspects into account, the aim of this study was to evaluate the effectiveness of a home-based motor and respiratory tele-rehabilitation program on the recovery of functional exercise capacity in post-COVID hospitalized patients.
2. Materials and Methods
2.1. Participants
This study addressed a group of individuals suffering disabling motor and/or respiratory symptoms after SARS-CoV-2 infection. The eligibility criteria included adult participants of both sexes, ranging in age from 37 to 75 years, who were admitted to the functional recovery units of San Giuseppe Hospital (IRCCS Istituto Auxologico Italiano, Piancavallo, IT) and Clinica Hildebrand – Centro di Riabilitazione Brissago (Brissago, CH) due to SARS-CoV2 outcomes. Conversely, individuals presenting severe comorbidities (e.g. uncontrolled cardiovascular and/or musculoskeletal diseases), cognitive impairments or psychiatric pathologies preventing a correct use of technology for tele-rehabilitation were excluded. Approval for the study was obtained from Ethics Research Committees of both Institutes (trial registration: NCT05739552), and all procedures were conducted in accordance with their ethical guidelines as well as with the principles outlined in the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all participants prior to their involvement in the study.
2.2. Therapeutic Intervention
Patients admitted to the functional recovery units followed a four-week multidisciplinary rehabilitation program including physiotherapy, physical activity and conditioning sessions, breathing exercises, medical support, and nutritional intervention. Upon discharge, patients were provided with a personalized three-week motor and respiratory tele-rehabilitation program based on individual assessments and hospital rehabilitation course, along with proper, easy-to-use technological equipment for remote rehabilitation. During their hospital stay, patients were instructed on how to use the technologies and become accustomed to them.
In particular, the technology provided to each patient consisted of a respiratory muscle training device (SpiroTiger, MVM Italya, Lainate, IT) and a motor rehabilitation device (Euleria home, Euleria Health, Rovereto, IT).
The SpiroTiger is a device specifically designed to train respiratory muscles allowing for the execution of deep and fast breathing acts without incurring the consequences of hyperventilation, such as hypocapnia. The device Figure 1 consists of a portable grip housing monitoring electronics and a small display. It is fitted with a silicone breathing bag for air recycling, a mouthpiece oriented at 90 degrees, and a lateral port enabling fresh air inspiration and expiration. Additionally, the port incorporates a valve regulating the maintenance of the isocapnic state. The tuning of the specific parameters of the device allows for a personalized respiratory training by enabling maximal inspirations and expirations without the risk of hyperventilation, eliciting activation of all respiratory muscle groups, thereby enhancing thoracic flexibility and breathing coordination [29].
Concerning motor training, euleria home is a CE class 1/m medical device designed for home-based rehabilitation. It consists of an IMU (Xsens DOT, Movella Technologies-NL, size: 36.3 x 30.4 x 10.8 mm, weight: 11.2 g) wirelessly connected to a tablet running a dedicated application that guides the user through the execution of a set of motor tasks selected by clinicians from a wide integrated library. The sensor can be easily worn on different body segments with adjustable elastic bands. Once it is in place, the user simply needs to start the application on the tablet and follow the audio-video cues on the screen to perform the exercises. Biofeedback technology and integration with the sensor simplify the execution of the tasks and the completion of the session, while also motivating the patient with an effective gamification mechanism. Through a cloud-based management system, clinicians can remotely monitor patients’ compliance with rehabilitation and adjust personalized exercise-therapy programs according to patients’ health status. Additionally, the system facilitates communication with patients through its integrated chat and video call functions.
The exercise protocol for tele-rehabilitation was sorted by clinicians based on individual assessment of the patients prior to hospital discharge. For respiratory rehabilitation, patients engaged in personalized breathing exercises up to five times per week. Conversely, motor rehabilitation mainly included simple free body exercises targeting trunk, upper and lower limbs, to be performed three to five times per week. On a weekly basis, clinicians reviewed the exercise reports to monitor and adjust the program as needed. Since the SpiroTiger does not allow for remote monitoring of the performed session, weekly phone calls were made to evaluate user tracking. In addition, daily monitoring of the program was performed via WhatsApp, and any deviations from adherence was noted, specifically recording any adverse incidents. At the end of the program, participants completed a satisfaction questionnaire (System Usability Scale, SUS) [30] regarding the use of both devices. A flow diagram of the study is shown in Figure 2
2.3. Functional and Clinical Assessment
Post-COVID patients often experience a downward spiral, leading to reduced functional abilities to perform functional tasks due to breathing difficulties, early fatigue and muscle weakness [8,31].
To track and highlight changes in their health status throughout the rehabilitation process, patients underwent functional tests for motor and respiratory function at different time points. Specifically, patients were evaluated at the beginning of their hospital-based rehabilitation program (T0), at discharge time (T1), and at the end of their home-based tele-rehabilitation program (T2).
Regarding motor function, patients performed the instrumented Six-Minutes Walking Test (i6MWT) [32,33,34], a common sub-maximal test used to assess aerobic capacity and endurance in patients with various diagnoses, including those with cardiopulmonary issues [35]. The i6MWT was recorded using a single miniaturized inertial sensor (70 mm x 40 mm x 18 mm) (G-Sensor®, BTSBioengineering, Milan, Italy) placed at the L4-L5 vertebrae level with an ergonomic belt. The device, previously validated for gait investigations in both unaffected individuals and those with various pathological conditions [33,36,37,38], integrates a triaxial accelerometer 16 bit/axes with multiple sensitivity ( ± 2, ± 4, ± 8, ± 12g), a triaxial gyroscope 16 bit/axes with multiple sensitivity ( ±250, ±500, ±1000, ±2000 °/s) and a triaxial magnetometer 13 bit (± 1200 mT).
The i6MT was conducted indoors along a flat 30-meters hospital corridor. Regular 3-meter intervals along the corridor were marked with coloured tape, while two cones defined the turnaround points. Patients were instructed to walk as fast as possible at their self-pace. Rest was permitted as needed, and verbal cues to cues to motivate the patients were provided in accordance with the guidelines from the European Respiratory Society and the American Thoracic Society [39,40]. All assessed patients completed the test without reporting adverse events such as chest pain, severe dyspnoea or other signs of severe distress. Heart rate and oxygen saturation (SpO2) were measured using pulse oximetry both before and after the test.
At the end of the i6MWT, acceleration data (sample frequency: 100 Hz) were wirelessly transmitted to a laptop and processed using a dedicated software (BTS® G-Studio, BTS Bioengineering S.p.A.; ver. 3.2.20) for data collection, elaboration, and reporting. The distance covered over 6 minutes (i.e. walked distance), which typically serves as the primary outcome measure for assessing changes in patient’s performance, was retrieved and considered for further analysis. Additionally, other relevant gait spatio-temporal parameters, including gait speed, cadence and stride length, were also recorded. Furthermore, upper limb strength and function were evaluated by measuring the maximum isometric force exerted during handgrip for both the dominant (D) and non-dominant (ND) upper limb using a dynamometer.
With regard to respiratory function, two 1-minute maximal voluntary ventilation (MVV) tests were conducted using the SpiroTiger device, along with the assessment of the forced vital capacity (FVC). In particular, the first test utilized a ventilation frequency of 25 acts/min (MVV @25) to specifically load inspiratory muscles, whilst the second test targeted expiratory muscles with ventilation frequency of 34 acts/min (MVV @34) [41]. The recorded FVC, FVV @25, and FVV @34 were taken into account for further analysis.
2.4. Statistical Analysis
Descriptive statistics were employed to characterize the sample in terms of age, sex, and individual variables such as height and weight. Data from motor and respiratory assessment were checked for normal distribution and homogeneity of variance using the Shapiro-Wilk and Levene’s test, respectively.
To evaluate and quantify the effect of rehabilitation and tele-rehabilitation, a comparison across the three recorded testing sessions (i.e. T0, T1, and T2) was conducted via ANOVA analysis, followed by post-hoc analyses including paired t-tests between the observed time points (i.e. T1-T0, T2-T1, T2-T0).
3. Results
Rehabilitation centres evaluated 40 patients from May 16, 2022, to August, 15 2023. Out of the assessed patients, 12 did not meet the inclusion criteria or refused the program. As a result, a total of 28 post-COVID patients started the program, but only 23 completed the intervention and were included in the analysis. Five participants withdrew from the study due to personal reasons unrelated to the rehabilitation program. Participants’ characteristics are summarized in Table 1 . It should be noted that the most common comorbidity was obesity: at the beginning of the rehabilitation program, only two patients could be categorized as normal weight and overweight, respectively, according to their BMI, while the other 21 patients showed different degrees of obesity.
Shapiro-Wilk test confirmed the normality of the distribution, while the homogeneity of variances was confirmed by Lavene’s test for all parameters, allowing their representation in terms of mean and standard deviation. Inter-session variations for gait spatio-temporal parameters were all found to be significant (p < 0.05), except for stride length, while cadence appeared to be significant only between T0 and T2. Conversely, no significant variation was found for the maximum isometric force values, both for the dominant and non-dominant upper limb. Regarding respiratory parameters, significance (p < 0.05) was found in all inter-session variations. Motor and respiratory parameters are summarized in Table 2 and in Figure 3 .
At the end of the program, patients completed the satisfaction questionnaire. The mean SUS scores were 85.5/100 for the respiratory training device and 84.1/100 for the motor training device, respectively.
Table 3 reports the intra-session changes in heart rate and oxygen saturation before and after the execution of the i6MWT at each time point. A significant (p < 0.05) variation was found in the pre-post test heart rate in all sessions, whilst a significant variation for SpO2 was observed only at the baseline session. No significant (p > 0.05) inter-session variations were found. However, it is noteworthy that the intra-session variation decreases for SpO2, indicating changes in patients’ oxygen desaturation after the test.
4. Discussion
COVID-19 patients often experience a heterogenous sequelae of long-term health issues that can persist for months after the infection, hindering their return to normal life and negatively impacting both their mental and physical well-being. Managing post-COVID symptoms and effects is crucial across all stages of the disease, from the acute to post-acute period. However, access to rehabilitation facilities was often limited during the pandemic outbreak. In this context, tele-rehabilitation emerged as a novel solution to support healthcare facilities in coping with the demand for rehabilitation, not only for chronic patients, but also for COVID-19 survivors. Therefore, this study aimed to assess the effectiveness of a home-based tele-rehabilitation program tailored for post-COVID patients, with a specific focus on motor and respiratory training.
The results demonstrate an overall improvement in both motor and respiratory function, observed between the baseline assessment at T0 and the completion of hospital-based rehabilitation at T1, as well as between T0 and after tele-rehabilitation at T2. Regarding motor evaluation, the spatio-temporal parameters of gait derived from the i6MWT exhibit a significant (p < 0.05) upward inter-session trend, with the exception of stride length. In the traditional 6MWT assessment, walked distance serves as the benchmark for comparing changes in patients’ exercise tolerance, with increased distance indicating improved basic mobility[42,43]. Literature suggests that a minimum inter-session difference of 30 m should be observed to indicate a clinically relevant change in patients with respiratory diseases [44]. In this study, the walked distance increased by approximately 73 m between the baseline and final assessment, with a more pronounced variation observed between baseline and hospital-based rehabilitation ( > 50 m) compared to tele-rehabilitation (< 25 m). Alongside this variation, there is an increase in the mean pre-post test heart rate, consistent with the variation in walked distance [45]. Furthermore, for T0 and T1 session, it is noticeable that SpO2 decreases less after the execution of the i6MW, as an effect of the training. Conversely, a slight increase in the pre-post SpO2 variation can be observed at T2. However, it should be acknowledged that for the final assessment, most patients returned to a clinical center which is situated approximately 1300 m above sea level, potentially influencing the saturation value due to altitude changes [46]. Beyond walked distance, it should be noticed that the i6MWT performed with a body-worn device allowed for the acquisition of other relevant gait parameters, contributing to a more comprehensive understanding of patients’ functional exercise capacity and gait [47]. Previous studies have highlighted the influence of the interplay between cadence and stride length on gait speed, impacting critical spatio-temporal aspects of walking and motor control [48,49,50]. Gait speed can be adjusted by modifying either cadence, stride length or both simultaneously [51]. In this study, although the variation in stride length did not reach statistical significance (p > 0.05), the observable upward trend, in line with the rise in cadence, suggests enhanced motor control aimed at augmenting gait speed to increase walked distance during the test.
Regarding maximum isometric force, an increase between sessions is observable for both dominant and non-dominant upper limbs, although no significant difference (p > 0.05) was found. Typically, improvements in muscle strength become noticeable within a few weeks of a structured training program. However, significant changes usually become more evident after several weeks to a few months of consistent training. In this study, the rehabilitation regimen did not specifically target strength training, and the time between sessions may not have been sufficient to observe visible changes in strength [52]. However, the observed differences may reflect general improvements in overall physical condition rather than specific gains in muscle strength. Future studies with longer intervention periods or targeted strength training protocols may provide further insights into the effects of rehabilitation on muscle strength in post-COVID patients.
Significant improvements were reported for all the considered respiratory parameters. FVC is a proxy of lung functional capacity because it quantifies the ability to inhale and exhale. In healthy adults, it typically ranges between 3.0 and 5.0 L, with diminished values often associated with diseases impacting lung function, such as COVID-19. In this study, patients initially exhibited borderline FVC values, which significantly and progressively improved after the hospital- and home-based rehabilitation. Simultaneously, a statistically significant (p < 0.05) and coordinated improvement in inspiratory and expiratory muscle strength was observed, as indicated by the results of the maximal 1-minute ventilation tests. The respiratory system relies on the interplay of several muscles to facilitate breathing. Therefore, a simultaneous increase in both inspiratory and expiratory muscle strength can lead to improved respiratory function, increased lung capacity and overall breathing performance, as well as reduced fatigue [53,54].
With respect to tele-rehabilitation, the aggregated findings of this study appear promising in supporting both the feasibility and the safety of the approach, as well as its role in enhancing functional exercise capacity and managing long-lasting symptoms in post-COVID individuals. Out of the total population, only five patients initially enrolled did not complete the program, resulting in a dropout rate of approximately 18%, consistent with existing literature for post-COVID individuals, which ranges from 10% to 32% [12]. Among these, three dropped due to a lack of cooperation, while the others withdrew from the program due to personal reasons. Throughout tele-rehabilitation, participants received regular monitoring from healthcare professionals via video calls and messages as needed. This continuous monitoring likely aided patients in maintaining consistency with the training regimen, since dropout in tele-rehabilitation has been reported to stem from patients’ misperceptions of their actual needs and loss of human contact with clinicians [12]. Furthermore, rehabilitation plans were tailored to address the individual needs of each patient and scheduled to accommodate their daily lives and routines, as programs demanding high commitment in terms of both physical effort and time are more prone to dropout.
Regarding technological aspects, patient feedback on the use of the devices for tele-rehabilitation supports the sustainability of the proposed approach. Patients generally expressed satisfaction and motivation with using the devices at home and being followed up weekly (albeit remotely) by healthcare professionals. This positive feedback was also confirmed by the completion of satisfaction questionnaires, whose SUS scores would suggest exceptional usability for both the devices [55]. Although the introduction of specific technological platforms and devices may pose some challenges and slow down the implementation of tele-rehabilitation [56], particularly for patients unfamiliar with technology, no issues were reported by the participants. The devices were selected for their ease of use and accessibility, and patients had the opportunity to familiarize themselves with the devices during their hospital stays. During tele-rehabilitation, only sporadic technical issues such as disconnections and device failures were reported, although they were promptly addressed by technical support.
While the study highlights positive aspects of the rehabilitation program, several limitations should be taken into account. Firstly, the study population was not consistent due to changes in the pandemic situation in Italy during the study period. The reduced number of participants thus limits the robustness of the statistical findings, which may not be representative of a broader population. Furthermore, the majority of participants had comorbid obesity, potentially impacting the generalizability of the findings. Chronic inflammation of adipose tissue alongside with reduced lung capacity and impaired ventilation are reported to increase the vulnerability of obese individuals to severe illness from COVID-19 so it is not unusual to have a high number of patients with comorbid obesity dealing with post-COVID symptoms [57]. However, it is worth mentioning it should that the clinical center that treated the majority of patients is specialized in the treatment of patients with metabolic disorders, so recruitment was done according to the availability of eligible patients regardless of their BMI. However, recovery mechanisms and timings from COVID-19 may differ for healthy weight individuals [58,59].
Another limitation is the absence of a control group, as reported in previous studies [2,60,61]. Without a control group, caution is needed in interpreting the data, as distinguishing whether improvements are due to the rehabilitation course or the natural evolution of the disease over time may be challenging [60,61]. Moreover, since patients underwent hospital-based before tele-rehabilitation, quantifying their respective impacts on patients’ recovery is difficult. Also, the absence of a gold-standard method for assessing respiratory capacity, such as the spirometry test, limits generalizability of results.
This study employed a hybrid approach combining traditional face-to-face rehabilitation and tele-rehabilitation, ultimately leading to positively synergic effects on the outcomes. Throughout the pandemic period, the demand for rehabilitation services has increased significantly. Tele-rehabilitation is not meant to fully replace traditional rehabilitation, rather, its implementation offers a viable new approach balancing patient quality of life and healthcare system sustainability [62,63,64]. Besides the observed benefits in motor and respiratory function among program participants, tele-rehabilitation can also yield socio-economic advantages for both patients and healthcare facilities. Utilizing digital technology to deliver rehabilitation has the potential to reduce hospital stay, decrease the demand for human resources and lowering hospitalization costs [65,66,67].
5. Conclusion
The aim of this study was to evaluate the effectiveness of a therapeutic intervention delivered via tele-rehabilitation in facilitating motor and respiratory recovery among post-COVID individuals. Despite the discussed limitations, the findings seem to support not only the clinical advantages of this approach in promoting recovery in post-COVID patients but also its adherence and safety aspects. Given the current COVID-19 diffusion and its evolving landscape, enlarging the patient population or incorporating a control group looks very challenging. Nevertheless, there might be the potential to extend the tele-rehabilitation protocol to individuals presenting other conditions affecting respiratory and/or motor functions. Given the outcomes and their implications from both patient and healthcare center perspectives, the tele-rehabilitation approach proposed in this study emerges as a viable, safe, and effective strategy in addressing rehabilitation needs, thus opening new perspectives in tele-health applications supporting healthcare centres in the provision of rehabilitation services.
Author Contributions
Conceptualization, S.C. and V.Ci.; methodology, S.C. and V.Ci, formal analysis, V.Ci., P.C. and P.R.; data curation, S.C., F.V. and V.Ci.; writing—original draft preparation, S.C., F.V.; writing— review and editing, P.C., P.R., V.Cv., and G.B.; supervision, P.C., P.R., M.G. and V.Ci. All authors have read and agreed to the published version of the manuscript.
Funding
The research was conducted in the field of TRIALS Project “La teleriabilitazionene nel lpaziente post-covid: l’esperienza Italia-Svizzera”, project co-funded by the European Union (FESR), Italy, Swiss Confederation and Swiss Cantons—Interreg V-A Italy-Switzerland” and partially supported by the Italian Ministry of Health.
Institutional Review Board Statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the IRCCS Istituto Auxologico Italiano (Protocol number 2022_05_17_02) and of Comitato etico cantonale 6501 Bellinzona (2022-01071, Rif CETI 4120).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available on request in Zenodo repository (https://doi.org/10.5281/zenodo.11353640) due to restrictions, e.g., privacy or ethical.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jangnin, R.; Ritruangroj, W.; Kittisupkajorn, S.; Sukeiam, P.; Inchai, J.; Maneeton, B.; Maneetorn, N.; Chaiard, J.; Theerakittikul, T. Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era. J. Clin. Med. 2024, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Estebanez-Pérez, M.J.; Pastora-Bernal, J.M.; Martín-Valero, R. The Effectiveness of a Four-Week Digital Physiotherapy Intervention to Improve Functional Capacity and Adherence to Intervention in Patients with Long COVID-19. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. Organization, W.H. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: interim guidance, 13 March 2020; World Health Organization: Geneva PP - Geneva.
- Sugiyama, A.; Takafuta, T.; Sato, T.; Kitahara, Y.; Yoshinaga, Y.; Abe, K.; Chanroth, C.; Ataa, A.G.; Phyo, Z.; Kurisu, A.; et al. Natural course of post-COVID symptoms in adults and children. Sci. Rep. 2024, 14, 3884. [Google Scholar] [CrossRef] [PubMed]
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Paniagua, J.; Díaz-Arribas, M.J.; Valera-Calero, J.A.; Gallardo-Vidal, M.I.; Fernández-De-las-Peñas, C.; López-De-Uralde-Villanueva, I.; del Corral, T.; Plaza-Manzano, G. A tele-health primary care rehabilitation program improves self-perceived exertion in COVID-19 survivors experiencing Post-COVID fatigue and dyspnea: A quasi-experimental study. PLoS One 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Agergaard, J.; Leth, S.; Pedersen, T.H.; Harbo, T.; Blicher, J.U.; Karlsson, P.; Østergaard, L.; Andersen, H.; Tankisi, H. Myopathic changes in patients with long-term fatigue after COVID-19. Clin. Neurophysiol. 2021, 132, 1974–1981. [Google Scholar] [CrossRef] [PubMed]
- Tirelli, U.; Taibi, R.; Chirumbolo, S. Post COVID syndrome: a new challenge for medicine. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4422–4425. [Google Scholar] [CrossRef]
- Quaranta, V.N.; Portacci, A.; Dragonieri, S.; Locorotondo, C.; Buonamico, E.; Diaferia, F.; Iorillo, I.; Quaranta, S.; Carpagnano, G.E. The Predictors of Long COVID in Southeastern Italy. J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Cerfoglio, S.; Capodaglio, P.; Rossi, P.; Verme, F.; Boldini, G.; Cvetkova, V.; Ruggeri, G.; Galli, M.; Cimolin, V. Tele-Rehabilitation Interventions for Motor Symptoms in COVID-19 Patients: A Narrative Review. Bioeng. (Basel, Switzerland) 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.J.; Lin, C.W.; Hsiao, M.Y.; Wang, T.G.; Liang, H.W. Long COVID and rehabilitation. J. Formos. Med. Assoc. 2024, 123, S61–S69. [Google Scholar] [CrossRef] [PubMed]
- Meng, M.; Wei, R.; Wu, Y.; Zeng, R.; Luo, D.; Ma, Y.; Zhang, L.; Huang, W.; Zeng, H.; Leung, F.W.; et al. Long-term risks of respiratory diseases in patients infected with SARS-CoV-2: a longitudinal, population-based cohort study. EClinicalMedicine 2024, 69, 102500. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.J.; Baldwin, M.M.; Daynes, E.; Evans, R.A.; Greening, N.J.; Jenkins, R.G.; Lone, N.I.; McAuley, H.; Mehta, P.; Newman, J.; et al. Respiratory sequelae of COVID-19: pulmonary and extrapulmonary origins, and approaches to clinical care and rehabilitation. Lancet. Respir. Med. 2023, 11, 709–725. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.T.; Dolezal, B.A.; Cooper, C.B. Pulmonary Rehabilitation for Chronic Obstructive Pulmonary Disease: Highly Effective but Often Overlooked. Tuberc. Respir. Dis. (Seoul). 2020, 83, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Zampogna, E.; Paneroni, M.; Cherubino, F.; Pignatti, P.; Rudi, M.; Casu, G.; Vitacca, M.; Spanevello, A.; Visca, D. Effectiveness of a Pulmonary Rehabilitation Program on Persistent Asthma Stratified for Severity. Respir. Care 2019, 64, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Cameron-Tucker, H.L.; Wood-Baker, R.; Owen, C.; Joseph, L.; Walters, E.H. Chronic disease self-management and exercise in COPD as pulmonary rehabilitation: a randomized controlled trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 513–523. [Google Scholar] [CrossRef]
- Kerti, M.; Balogh, Z.; Kelemen, K.; Varga, J.T. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 717–724. [Google Scholar] [CrossRef]
- Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; Anarte-Lazo, E.; Bernal-Utrera, C.; Perez-Ale, M.; Rodriguez-Blanco, C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef]
- Bures, M.; Neumannova, K.; Blazek, P.; Klima, M.; Schvach, H.; Nema, J.; Kopecky, M.; Dygryn, J.; Koblizek, V. A Sensor Network Utilizing Consumer Wearables for Telerehabilitation of Post-acute COVID-19 Patients. IEEE Internet Things J. 2022, PP, 1. [Google Scholar] [CrossRef]
- Bezuidenhout, L.; Joseph, C.; Thurston, C.; Rhoda, A.; English, C.; Conradsson, D.M. Telerehabilitation during the COVID-19 pandemic in Sweden: a survey of use and perceptions among physiotherapists treating people with neurological diseases or older adults. BMC Health Serv. Res. 2022, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Demeyer, H.; Louvaris, Z.; Frei, A.; Rabinovich, R.A.; de Jong, C.; Gimeno-Santos, E.; Loeckx, M.; Buttery, S.C.; Rubio, N.; Van der Molen, T.; et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: a multicentre randomised controlled trial. Thorax 2017, 72, 415–423. [Google Scholar] [CrossRef]
- Holland, A.E.; Hill, C.J.; Rochford, P.; Fiore, J.; Berlowitz, D.J.; McDonald, C.F. Telerehabilitation for people with chronic obstructive pulmonary disease: feasibility of a simple, real time model of supervised exercise training. J. Telemed. Telecare 2013, 19, 222–226. [Google Scholar] [CrossRef] [PubMed]
- M. K., S.; T., J.; E.Y.L., W.; W.M., R.; N.G., J.; G.F., M. Using Telehealth technology to deliver pulmonary rehabilitation to patients with chronic obstructive pulmonary disease. Can. Respir. J. 2011, 18, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Valverde-Martínez, M.Á.; López-Liria, R.; Martínez-Cal, J.; Benzo-Iglesias, M.J.; Torres-Álamo, L.; Rocamora-Pérez, P. Telerehabilitation, A Viable Option in Patients with Persistent Post-COVID Syndrome: A Systematic Review. Healthc. (Basel, Switzerland) 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Zampolini, M.; Hermens, H.J.; Ilsbroukx, S. Tele-rehabilitation : present and future. 2008.
- Velez, M.; Lugo-Agudelo, L.H.; Patiño Lugo, D.F.; Glenton, C.; Posada, A.M.; Mesa Franco, L.F.; Negrini, S.; Kiekens, C.; Spir Brunal, M.A.; Roberg, A.S.B.; et al. Factors that influence the provision of home-based rehabilitation services for people needing rehabilitation: a qualitative evidence synthesis. Cochrane Database Syst. Rev. 2023, 2023. [Google Scholar] [CrossRef]
- Włodarczyk, O.M.; Barinow-Wojewódzki, A. The impact of resistance respiratory muscle training with a SpiroTiger(®) device on lung function, exercise performance, and health-related quality of life in respiratory diseases. Kardiochirurgia i torakochirurgia Pol. = Polish J. cardio-thoracic Surg. 2015, 12, 386–390. [Google Scholar] [CrossRef]
- Hyzy, M.; Bond, R.; Mulvenna, M.; Bai, L.; Dix, A.; Leigh, S.; Hunt, S. System Usability Scale Benchmarking for Digital Health Apps: Meta-analysis. JMIR Mhealth Uhealth 2022, 10, e37290. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Rasekaba, T.; Lee, A.L.; Naughton, M.T.; Williams, T.J.; Holland, A.E. The six-minute walk test: a useful metric for the cardiopulmonary patient. Intern. Med. J. 2009, 39, 495–501. [Google Scholar] [CrossRef]
- Cimolin, V.; Gobbi, M.; Buratto, C.; Ferraro, S.; Fumagalli, A.; Galli, M.; Capodaglio, P. A Comparative Analysis of Shoes Designed for Subjects with Obesity Using a Single Inertial Sensor: Preliminary Results. Sensors 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Gonçalves, N.; Matthews, H.; Isaacs, T.; Duffen, J.; et al. A systematic review of the characteristics and validity of monitoring technologies to assess Parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13, 24. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Cesareo, A.; Reni, G.; Biffi, E. Wearable inertial sensors to assess gait during the 6-minute walk test: A systematic review. Sensors (Switzerland) 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Mandaresu, S.; Pilloni, G.; Porta, M.; Coghe, G.; Marrosu, M.G.; Cocco, E. Smoothness of gait detects early alterations of walking in persons with multiple sclerosis without disability. Gait Posture 2017, 58, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Schifino, G.; Cimolin, V.; Pau, M.; da Cunha, M.J.; Leban, B.; Porta, M.; Galli, M.; Souza Pagnussat, A. Functional Electrical Stimulation for Foot Drop in Post-Stroke People: Quantitative Effects on Step-to-Step Symmetry of Gait Using a Wearable Inertial Sensor. Sensors (Basel). 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Cau, N.; Malchiodi Albedi, G.; Aspesi, V.; Merenda, V.; Galli, M.; Capodaglio, P. Do wearable sensors add meaningful information to the Timed Up and Go test? A study on obese women. J. Electromyogr. Kinesiol. 2019, 44, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- ATS statement: guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef]
- Sartori, R.; Barbi, E.; Poli, F.; Ronfani, L.; Marchetti, F.; Amaddeo, A.; Ventura, A. Respiratory training with a specific device in cystic fibrosis: A prospective study. J. Cyst. Fibros. 2008, 7, 313–319. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M. Reliability of outcome measures for people with lower-limb amputations: distinguishing true change from statistical error. Phys. Ther. 2011, 91, 555–565. [Google Scholar] [CrossRef]
- Rostagno, C.; Gensini, G.F. Six minute walk test: A simple and useful test to evaluate functional capacity in patients with heart failure. Intern. Emerg. Med. 2008, 3, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European respiratory society/American thoracic society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Lachant, D.J.; Light, A.; Offen, M.; Adams, J.; White, R.J. Heart rate monitoring improves clinical assessment during 6-min walk. Pulm. Circ. 2020, 10. [Google Scholar] [CrossRef]
- Dünnwald, T.; Kienast, R.; Niederseer, D.; Burtscher, M. The use of pulse oximetry in the assessment of acclimatization to high altitude. Sensors (Switzerland) 2021, 21, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Pires, I.M.; Villasana, M.V.; Sá, J.; Denysyuk, H.V.; Marques, D.L.; Morgado, J.F.; Albuquerque, C.; Zdravevski, E. Development Technologies for the Monitoring of Six-Minute Walk Test: A Systematic Review. Sensors 2022, 22, 1–29. [Google Scholar] [CrossRef]
- Ardestani, M.M.; Ferrigno, C.; Moazen, M.; Wimmer, M.A. From normal to fast walking: Impact of cadence and stride length on lower extremity joint moments. Gait Posture 2016, 46, 118–125. [Google Scholar] [CrossRef]
- Egerton, T.; Danoudis, M.; Huxham, F.; Iansek, R. Central gait control mechanisms and the stride length - cadence relationship. Gait Posture 2011, 34, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.P.; Kory, R.C.; Clarkson, B.H.; Sepic, S.B. Comparison of free and fast speed walking patterns of normal men. Am. J. Phys. Med. 1966, 45, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Howard, C.; Wallace, C.; Stokic, D.S. Stride length-cadence relationship is disrupted in below-knee prosthesis users. Gait Posture 2013, 38, 883–887. [Google Scholar] [CrossRef]
- Abe, T.; DeHoyos, D.V.; Pollock, M.L.; Garzarella, L. Time course for strength and muscle thickness changes following upper and lower body resistance training in men and women. Eur. J. Appl. Physiol. 2000, 81, 174–180. [Google Scholar] [CrossRef]
- Morgan, S.P.; Visovsky, C.; Thomas, B.; Klein, A.B. Respiratory Muscle Strength Training in Patients Post-COVID-19: A Systematic Review. Clin. Nurs. Res. 2024, 33, 60–69. [Google Scholar] [CrossRef] [PubMed]
- McNarry, M.A.; Berg, R.M.G.; Shelley, J.; Hudson, J.; Saynor, Z.L.; Duckers, J.; Lewis, K.; Davies, G.A.; Mackintosh, K.A. Inspiratory muscle training enhances recovery post-COVID-19: a randomised controlled trial. Eur. Respir. J. 2022, 60. [Google Scholar] [CrossRef]
- Grier, R.A.; Bangor, A.; Kortum, P.; Peres, S.C. The system usability scale: Beyond standard usability testing. Proc. Hum. Factors Ergon. Soc. 2013, 187–191. [Google Scholar] [CrossRef]
- Tiruneh, S.A.; Tesema, Z.T.; Azanaw, M.M.; Angaw, D.A. The effect of age on the incidence of COVID-19 complications: a systematic review and meta-analysis. Syst. Rev. 2021, 10, 80. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. an Off. J. Int. Assoc. Study Obes. 2020, 21, e13128. [Google Scholar] [CrossRef] [PubMed]
- Steenblock, C.; Hassanein, M.; Khan, E.G.; Yaman, M.; Kamel, M.; Barbir, M.; Lorke, D.E.; Everett, D.; Bejtullah, S.; Lohmann, T.; et al. Obesity and COVID-19: What are the Consequences? Horm. Metab. Res. 2022, 54, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Nour, T.Y.; Altintaş, K.H. Effect of the COVID-19 pandemic on obesity and it is risk factors: a systematic review. BMC Public Health 2023, 23, 1–24. [Google Scholar] [CrossRef]
- Dalbosco-Salas, M.; Torres-Castro, R.; Leyton, A.R.; Zapata, F.M.; Salazar, E.H.; Bastías, G.E.; Díaz, M.E.B.; Allers, K.T.; Fonseca, D.M.; Vilaró, J. Effectiveness of a primary care telerehabilitation program for post-covid-19 patients: A feasibility study. J. Clin. Med. 2021, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kortianou, E.A.; Tsimouris, D.; Mavronasou, A.; Lekkas, S.; Kazatzis, N.; Apostolara, Z.E.; Isakoglou, M.; Dimakou, G.; Barmparessou, Z.; Tsikrika, S.; et al. Application of a home-based exercise program combined with tele-rehabilitation in previously hospitalized patients with COVID-19: A feasibility, single-cohort interventional study. Pneumon 2022, 35, 1–10. [Google Scholar] [CrossRef]
- Theodoros, D.; Russell, T. Telerehabilitation: current perspectives. Stud. Health Technol. Inform. 2008, 131, 191–209. [Google Scholar]
- Baroni, M.P.; Jacob, M.F.A.; Rios, W.R.; Fandim, J.V.; Fernandes, L.G.; Chaves, P.I.; Fioratti, I.; Saragiotto, B.T. The state of the art in telerehabilitation for musculoskeletal conditions. Arch. Physiother. 2023, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zampolini, M.; Oral, A.; Barotsis, N.; Aguiar Branco, C.; Burger, H.; Capodaglio, P.; Dincer, F.; Giustini, A.; Hu, X.; Irgens, I.; et al. Evidence-based position paper on Physical and Rehabilitation Medicine (PRM) professional practice on telerehabilitation. The European PRM position (UEMS PRM Section). Eur. J. Phys. Rehabil. Med. 2024, 60, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Rogante, M.; Grigioni, M.; Cordella, D.; Giacomozzi, C. Ten years of telerehabilitation: A literature overview of technologies and clinical applications. NeuroRehabilitation 2010, 27, 287–304. [Google Scholar] [CrossRef] [PubMed]
- Rogante, M.; Kairy, D.; Giacomozzi, C.; Grigioni, M. A quality assessment of systematic reviews on telerehabilitation: what does the evidence tell us? Ann. Ist. Super. Sanita 2015, 51, 11–18. [Google Scholar] [CrossRef]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef]
Figure 1.
Visual representation of the SpiroTiger device (left). A patient training with the device (right).
Figure 1.
Visual representation of the SpiroTiger device (left). A patient training with the device (right).

Figure 2.
Study workflow.
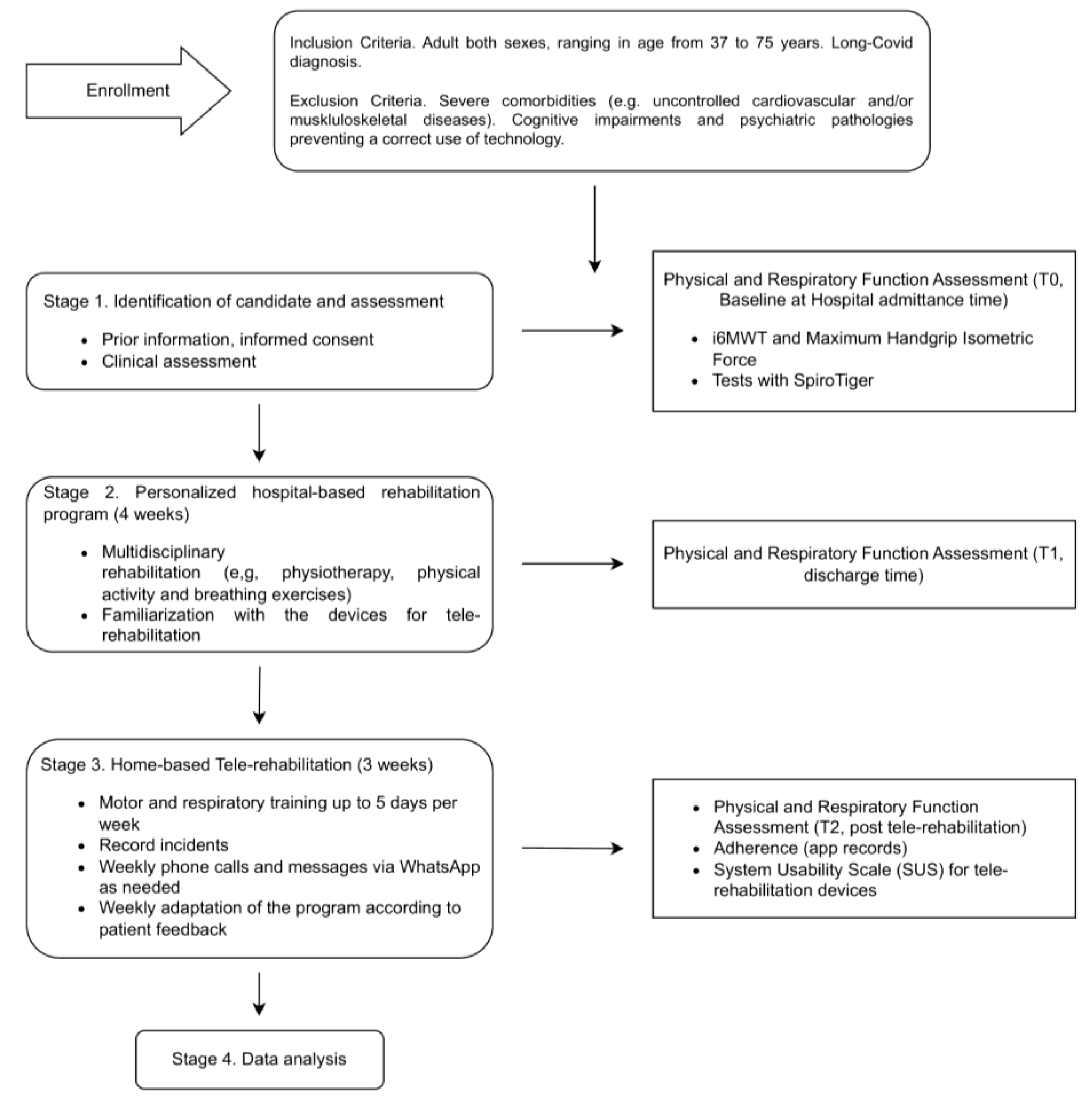
Figure 3.
Visual representation of the average values and standard errors of physical and respiratory parameters for each session (T0, T1 and T2).
Figure 3.
Visual representation of the average values and standard errors of physical and respiratory parameters for each session (T0, T1 and T2).
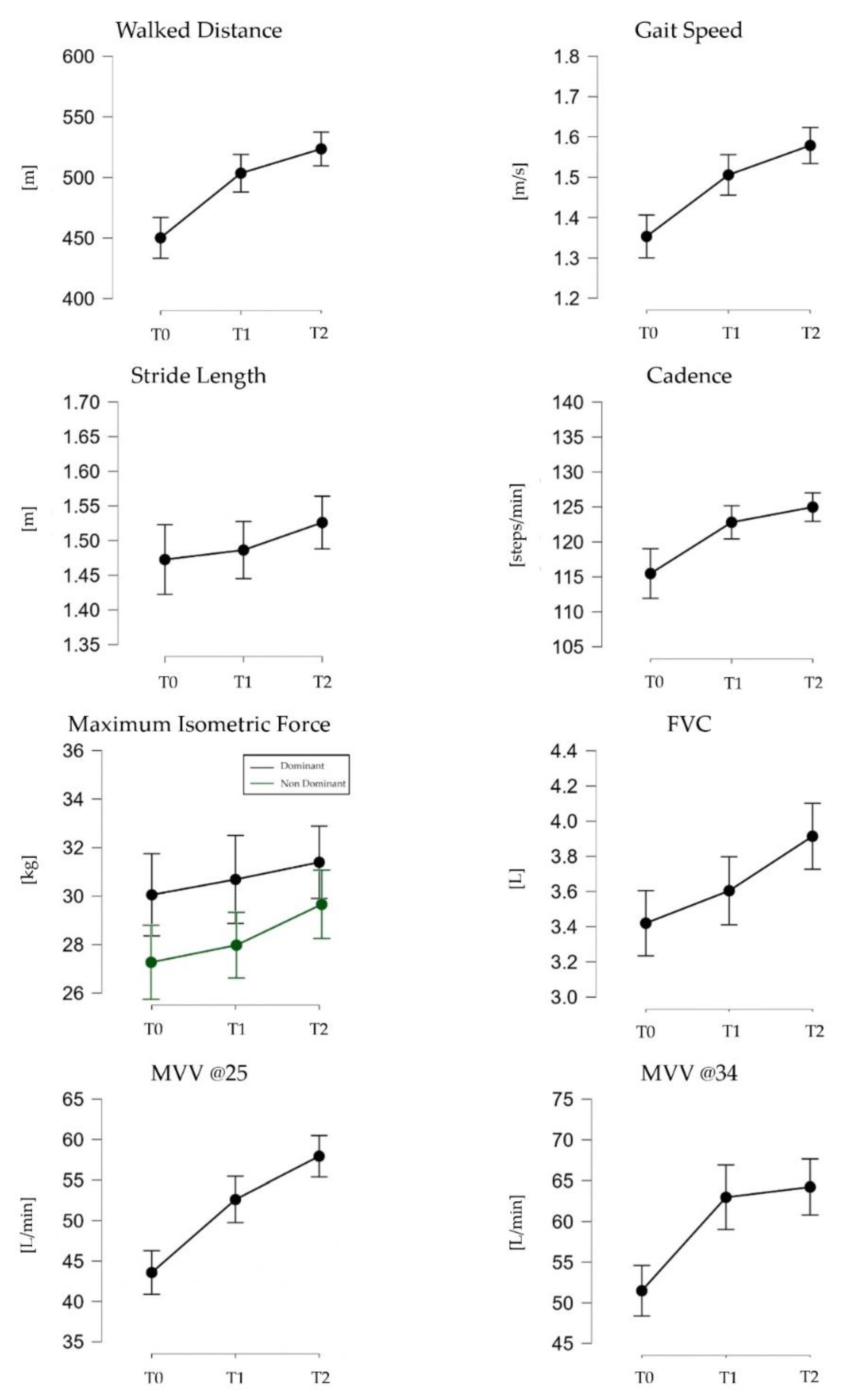

Table 1.
Demographic characteristics of the post-COVID patients who completed the program. Values are expressed as mean (SD).
Table 1.
Demographic characteristics of the post-COVID patients who completed the program. Values are expressed as mean (SD).
| Participants (n= 23) | |
|---|---|
| M/F | 6/17 |
| Age (years) | 55.91 ± 7.57 |
| Height (cm) | 164.58 ± 6.20 |
| Weight (kg) | 98.11 ± 17.82 |
| BMI (kg/m2) | 36.38 ± 7.06 |
Table 2.
Mean and standard deviation of the parameters related to motor and respiratory assessment. *= p < 0.05, if T0 vs. T1 and/or T2; += p < 0.0, if T1 vs. T2.
Table 2.
Mean and standard deviation of the parameters related to motor and respiratory assessment. *= p < 0.05, if T0 vs. T1 and/or T2; += p < 0.0, if T1 vs. T2.
| Sessions | |||
|---|---|---|---|
| T0 | T1 | T2 | |
| Walked Distance (m) | 450.16 (69.24) | 503.52 (63.85) * | 523.59 (57.59) * |
| Gait speed (m/s) | 1.35 (0.22) | 1.51 (0.20) * | 1.58 (0.18) * |
| Stride Length (m) | 1.47 (0.21) | 1.49 (0.16) | 1.53 (0.16) |
| Cadence (steps/min) | 115.48 (14.59) | 122.81 (9.44) | 124.99 (8.43) * |
| Maximum Isometric Force (kg) (D) | 30.05 (7.56) | 30.69 (8.53) | 31.40 (6.81) |
| Maximum Isometric Force (kg) (ND) | 27.39 (8.05) | 28.22 (7.48) | 30.20 (7.62) |
| FVC (L) | 3.42 (0.81) | 3.60 (0.91) | 3.91 (0.88) *,+ |
| MVV @25 (L/min) | 43.57 (12.09) | 52.61 (12.38)* | 57.93 (12.02) *,+ |
| MVV @34 (L/min) | 51.49 (12.89) | 62.97 (18.54)* | 64.23 (16.09)* |
Table 3.
Mean and standard deviation of heart rate and SpO2 before and after the i6MWT. *= p < 0.05, pre-test vs. post-test in each session (i.e. T0, T1 and T2).
Table 3.
Mean and standard deviation of heart rate and SpO2 before and after the i6MWT. *= p < 0.05, pre-test vs. post-test in each session (i.e. T0, T1 and T2).
| Hear Rate (bpm) | SpO2(%) | |||
|---|---|---|---|---|
| Session | Pre-test | Post-test | Pre-test | Post-test |
| T0 | 76.39 (11.55) | 101.41 (17.14)* | 95.33 (2.45) | 91.06 (6.19)* |
| T1 | 81.40 (14.52) | 108.55 (20.46)* | 94.50 (2.36) | 93.40 (3.85) |
| T2 | 85.05 (17.41) | 112.10 (20.04)* | 94.05 (5.39) | 92.40 (4.13) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



