
Submitted:
16 May 2024
Posted:
17 May 2024
You are already at the latest version
Abstract
Background:
There have been reports of numerous risk factors for Alzheimer's disease. Although widely investigated, some points during the evolution of the disease have been obscure. One of them is a great frustration with therapeutic expectations. Why has there been an increase in suicidal behavior in treatments with anti-beta-amyloid drugs? Interpersonal stress is one of the factors that may be connecting Alzheimer's disease to suicide.
Method:
To observe possible associations between Alzheimer's disease and suicide, two validated questionnaires were selected. We recruited 20 elderly patients over 65 years old to observe the feasibility of further research using these instruments. The study was considered viable if all participants showed no difficulty in understanding the questions and completed both questionnaires in less than 30 minutes with a tendency to homogeneity. A description of the statistical data obtained was made.
Results:
All participants adequately understood the questions and completed the questionnaires in less than 30 minutes. In 10% of the sample, suicide attempts occurred throughout their lives. The average age of respondents was 75 years old. The QoSL Pareto diagram demonstrated a large concentration. The data demonstrated homogeneity.
Conclusions:
The application of the questionnaires in a sample suitable for carrying out analytical statistics was demonstrated. We have two great tools to try to understand the possible association between Alzheimer's disease and suicide.
Keywords:
Alzheimer’s Disease
; suicide
; questionnaire
; pilot study
; feasibility
1. Introduction
As the population ages, new demands are necessary. Seeking to improve the quality of life of the elderly is a task of science.[1] There is a goal of preservation of cognitive functions in the old people.[2] Not just treating, but preventing neurodegenerative diseases is part of the list of every public health service.[3] There are nearly 50 million patients with Alzheimer’s disease (AD) worldwide, 90% of whom develop behavioral and psychological symptoms of dementia (BPSD).[4] AD is the most common dementia type, accounting on its own for almost 70% of all dementia cases.[5] The total annual cost of AD per capita was calculated in U$ 171 752.08.[6]
Many advances in therapies to prevent the progression of AD could already be bringing new resources to clinical practice but were hampered by adverse events, such as suicide.[7] Thus, the great expectation of substances capable of reducing β-amyloid concentration ended in frustration.[8]
What could be behind the increase in suicidal behavior in AD patients undergoing these new treatments?[9] Seeking to understand this topic better, an extensive bibliographic review was carried out.[10] The data from this analysis demonstrates that we have some possible themes to be further investigated as possible interfaces between suicide and AD.
Serotonergic, noradrenergic, and cholinergic neurocircuitry changes are described in the neurochemical interface.[11] In the genetic interface, there are seven serotonin receptor subtypes, and there are different research results on the association between each subtype and BPSD.[4] The presence of allele ε4 of apolipoprotein E was demonstrated to be a probable interface factor between suicide and AD.[12,13] Among other factors, depression stands out as the most likely associated factor, where we can highlight the importance of interpersonal stress in the outbreak of depressive disorders.[14,15,16,17,18,19,20,21,22,23] Impulsivity is a long-known risk factor for suicide attempts. Deficits in decision-making may impair people’s ability to resolve problems and dilemmas.[24,25] This failure is connected to brain systems modulating behavioral inhibitions. Impulsivity is part of the deficits in executive functions, associated with the function of the frontal lobe. In patients with AD, a large commitment in the frontal lobe circuit results in executive dysfunction.[26,27] However, the interpersonal interface between suicide and AD is the least studied to date.
Human relationships can be major causes of existential dissatisfaction and generate countless interpersonal tensions.[28] Interpersonal dysfunctions reflect on quality of life, causing extensive damage to health.[29] Emotional stress consists of physical and psychological reactions to unexpected and, generally, negative situations and it is described as a risk factor for suicide and AD by promoting changes in the hypothalamus-pituitary-adrenal axis (HPA axis).[30] Hyperactivation of the HPA axis leads to greater release of glucocorticoids (GCs).[31] The increased concentration of GCs in the brain promotes a reduction of GCs receptors in the hippocampus and increased DNA methylation with activations and deactivations of gene expressions.[32,33] Certain cascades of epigenetic changes lead to the expression of suicidal phenotypes, such as the reduction of BDNF, and decreased functioning of the cholinergic system with consequent cognitive impairment.[34,35] It has been demonstrated that GCs promote an imbalance in the action of glycogen synthase kinase 3 (GSK-3) and cyclin-dependent kinase 5 (CDK5), which ultimately leads to an increase in the phosphorylation of tau protein and its aggregation into neurofilaments.[36] GSK-3β is the main enzyme in the tau protein phosphorylation process and the PP2A phosphatase of dephosphorylation.[37] GCs increase the function of GSK-3β and reduce the activity of PP2A, leading to the accumulation of hyperphosphorylated tau protein.[38] Neurofibrillary tau protein aggregates appear to exert a braking role against stressful stimuli.[39] However, the long-term persistence of stress triggers the extracellular accumulation of β-amyloid as a synaptic brake.[9] (Figure 1)
Little evidence exists on which specific interpersonal factors may contribute to the onset of AD.[40,41] However, interpersonal theories about suicide are widely described.[42] Adding these concepts to the pathophysiological understanding of AD, we describe Alzheimer’s disease and Suicide associated Theory (ASA Theory): stress promotes a series of organic responses to adapt - the General Adaptation Syndrome (GAS), proposed by Hans Selye.[43] Long-term maintenance of stressful conditions can lead to various diseases. In the case of AD, the adaptive attempt seeks to reduce the overload of pathological stimuli through a neuronal braking mechanism with the accumulation of amyloid beta and tau protein. Suicide is a total non-acceptance of the adversity caused by a stressful situation. Both conditions end up annihilating the existential cognitive condition, described as “Not to be”. (Figure 2)
Beginning from the plane of ideas, where hypotheses are born, we came to look for ways to better assess the phenomenon in question. Our goal is to find evidence about interpersonal factors that are connecting AD and suicide. We started a pilot study to verify the feasibility of selected instruments.
Stress promotes the release of corticotropin-releasing hormone (CRH) from the hippocampus and cascades the release of adrenocorticotropin hormone (ACTH) and glucocorticoids (GCs) from the adrenal gland. GCs increase the function of GSK-3β and reduce the activity of PP2A, leading to the accumulation of hyperphosphorylated tau protein, neurofibrillary tangles, and destabilized microtubules.
ASA Theory: Stress promotes a series of organic responses to adapt - the GAS, proposed by Hans Selye. Long-term maintenance of stressful conditions can lead to various diseases. In the case of Alzheimer’s Disease, the adaptive attempt seeks to reduce the overload of pathological stimuli through a neuronal braking mechanism with the accumulation of amyloid beta and tau protein. Suicide is a total non-acceptance of the adversity caused by a stressful situation. Both conditions end up annihilating the existential cognitive condition, described as “Not to be”.
2. Materials And Methods
2.1. Source Population
The participants in this study are patients treated at the psychogeriatrics outpatient clinic at Unimed Bauru. The city of Bauru is in the geographic center of the state of São Paulo, in Brazil. It has a population of approximately 400,000 inhabitants and is centered around a region of 1 million inhabitants. Unimed is the main private health agency in Brazil and serves a third of the population.
From 9414 patients, those over 65 with cognitive conditions could be included to answer the questionnaires. If they do not accept the free and informed explanation or have a diagnosis of dementia they should be excluded. Our evaluation intends to investigate the suitability of the instruments in the healthy population, which will serve as a control group in comparison with the application in patients with AD in the future. A pilot application was carried out on 20 participants.[44,45,46] Participants were selected by simple random sampling according to the date of their last visit to the clinic.
A free and informed consent form was prepared. The present study was submitted and approved by the ethics and research committee of the Faculty of Medicine of São José do Rio Preto with CAAE: 65514822.2.0000.5415.
2.2. Instruments
Our studies are interested in assessing the interpersonal relationships that may be interconnected between Alzheimer’s disease and suicide. This can be done in several ways, such as by investigating the degree of satisfaction experienced in their personal and social relationships, etc. The level of interpersonal satisfaction is related to quality of life.[47] We chose to use instruments that could give a broad overview of the interpersonal way of life of the old people.
2.3. Data Analysis
A pilot study should not carry out statistical analyses but rather be restricted to describing the data.[44,45,50,51] This pilot aimed to test feasibility and consider the data that matters in this context.
To measure viability, three characteristics were considered in the sample:
- Understanding the questions of research instruments;
- Total response time of fewer than 30 minutes, as taking longer than this for each application of the questionnaires may make data collection for a large sample unfeasible or require many professionals with an exaggerated expenditure of human and financial resources;
- Data tends to be homogeneous, which is suitable for forming a control group.
Continuous variables were summarized as means and SDs; categorical variables were summarized as frequencies and proportions. Data from these participants were described in tables to verify their characteristics. All analyses were carried out using SPSS version 29.
3. Results
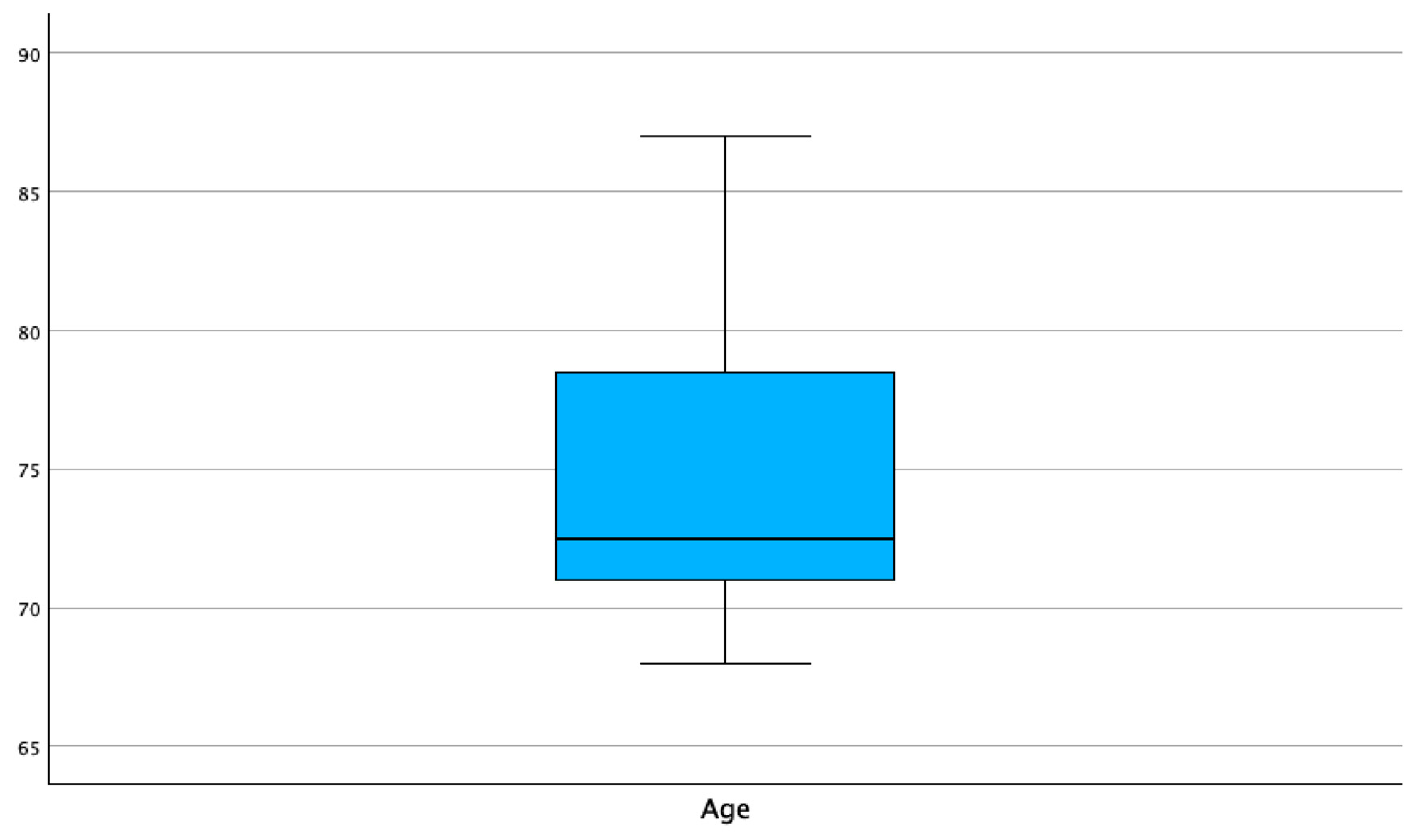
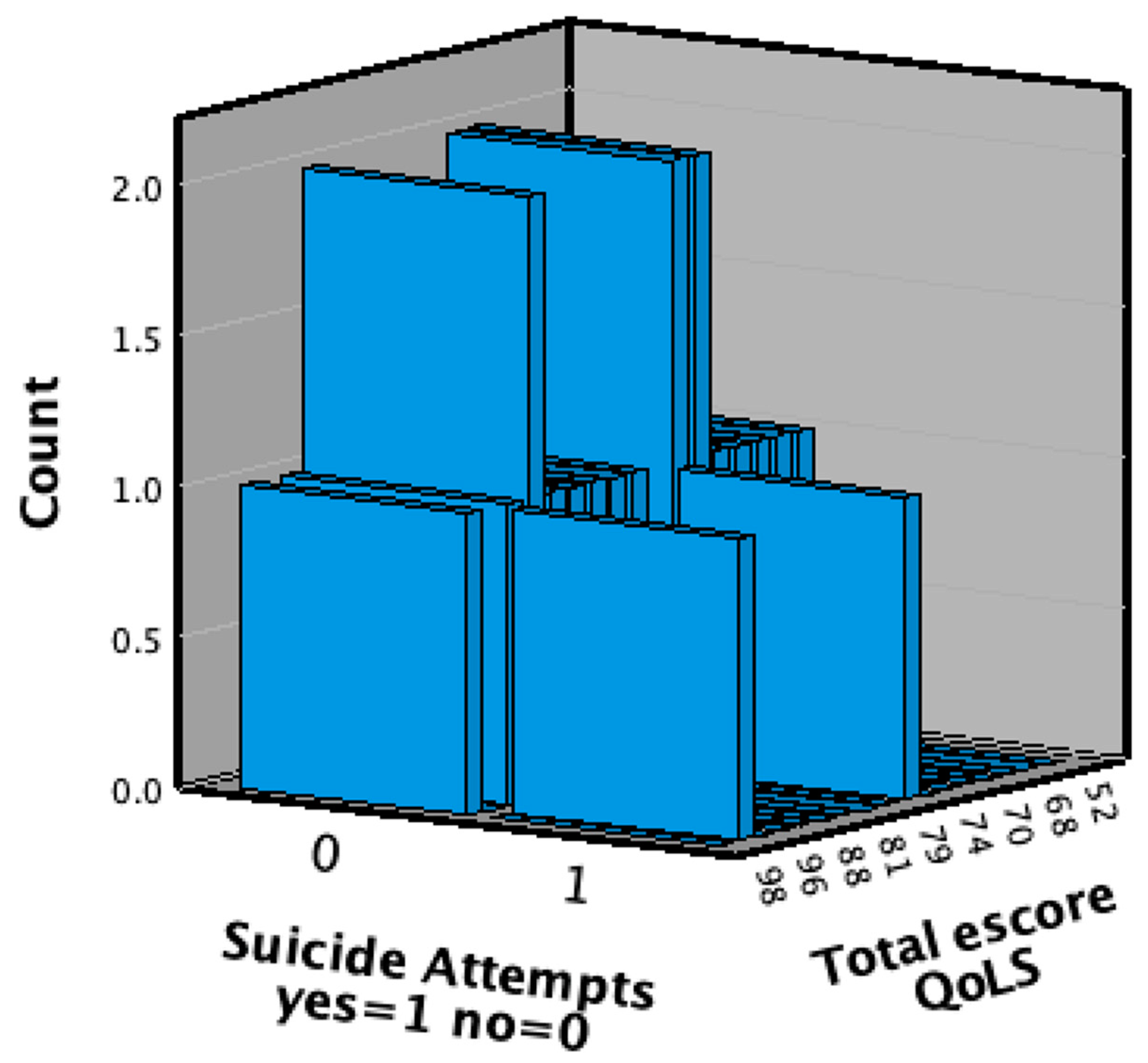
Twenty-one patients were recruited, one of whom was excluded due to a diagnosis of vascular dementia. All those invited to participate in this study agreed, signed the free and informed consent form, and answered the questionnaires. All participants completed both questionnaires in less than 30 minutes. The average age was 75 years (68 – 87) (Table 1, Graphics 2 and 3), with 70% of them having a higher level of education; 70% being women; 80% being treated for depression; 55% being married and 25% being widowed; 20% of whom have already had some suicidal ideation; of those who had suicidal ideation, half had planned and attempted suicide. (Table 2 and Graphic 3)
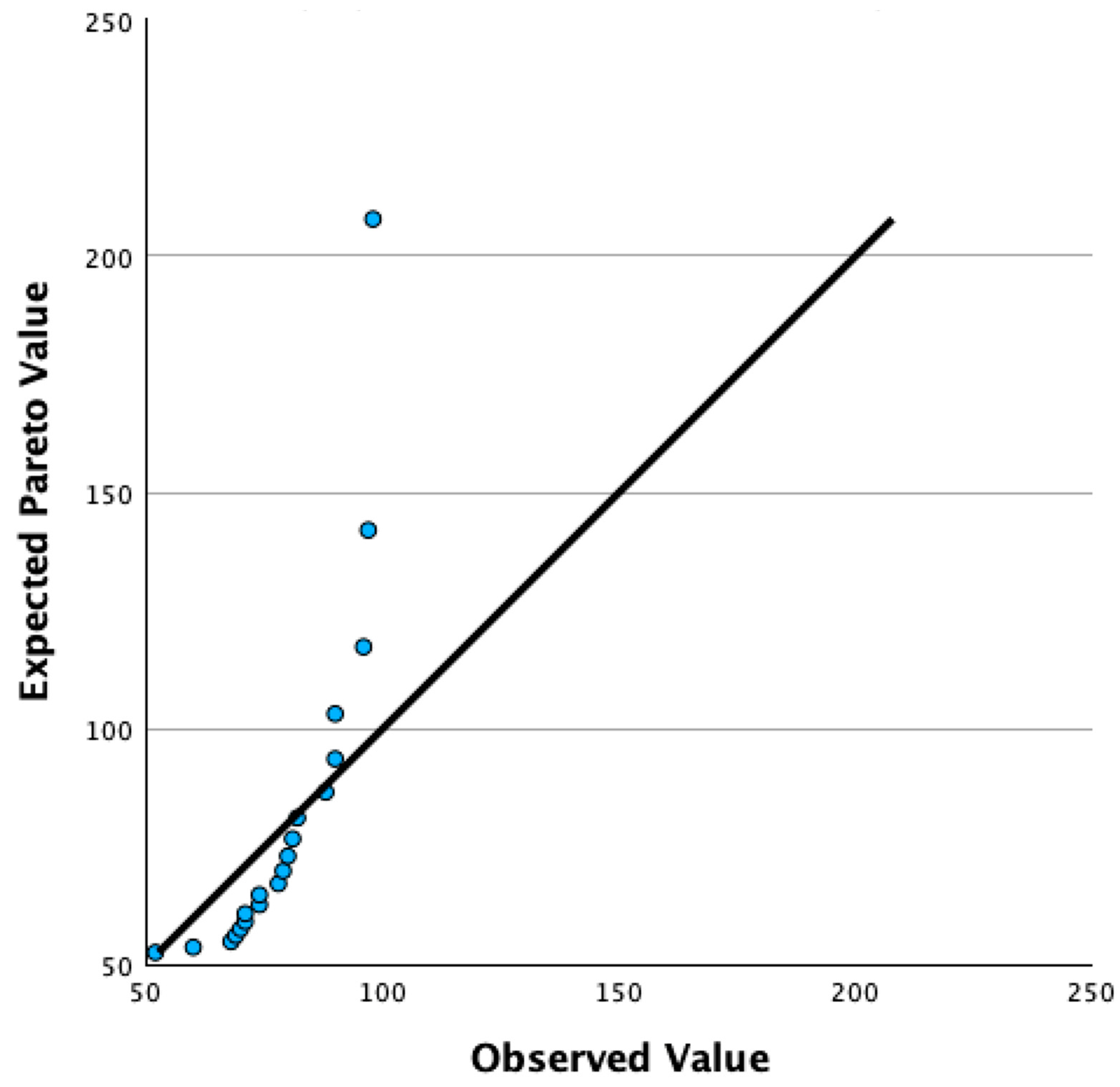
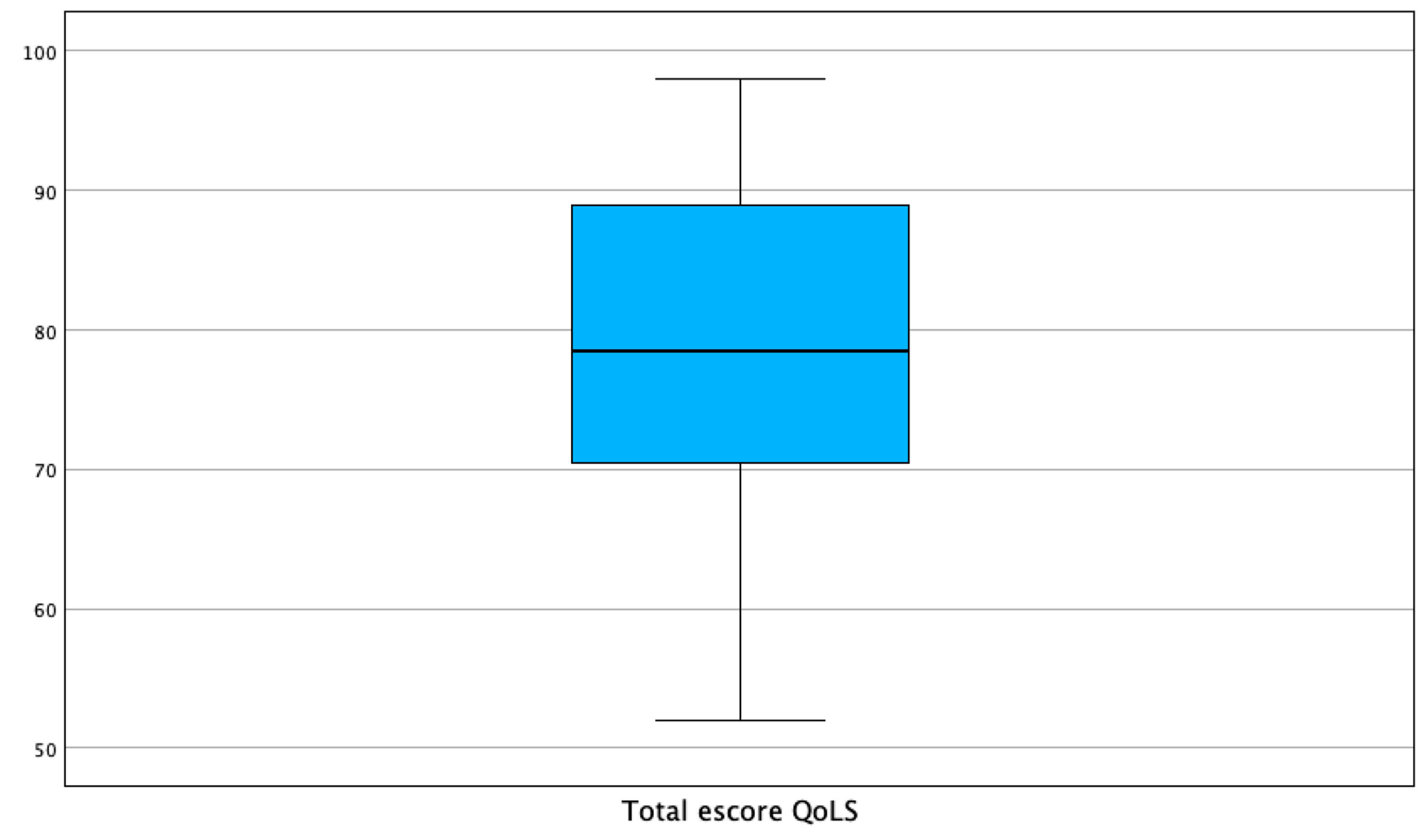
Flanagan’s quality of life scale scores ranged from 52 to 98 (possible minimum values of 15 and maximum of 105), with a median of 78.50 (70.25-89.50). (Graphic 4 and Table 3). The distribution did not demonstrate higher concentrations of a given frequency. (Graphic 5).
In total, we obtained 70 variables. The score for each of the 15 variables in Flanagan’s quality of life scale could vary from one to seven. The mode and median were close to the 75th percentile and the maximum value obtained, suggesting an excellent quality of life and homogeneity of respondents. (Table 3)
The results demonstrate excellent feasibility.
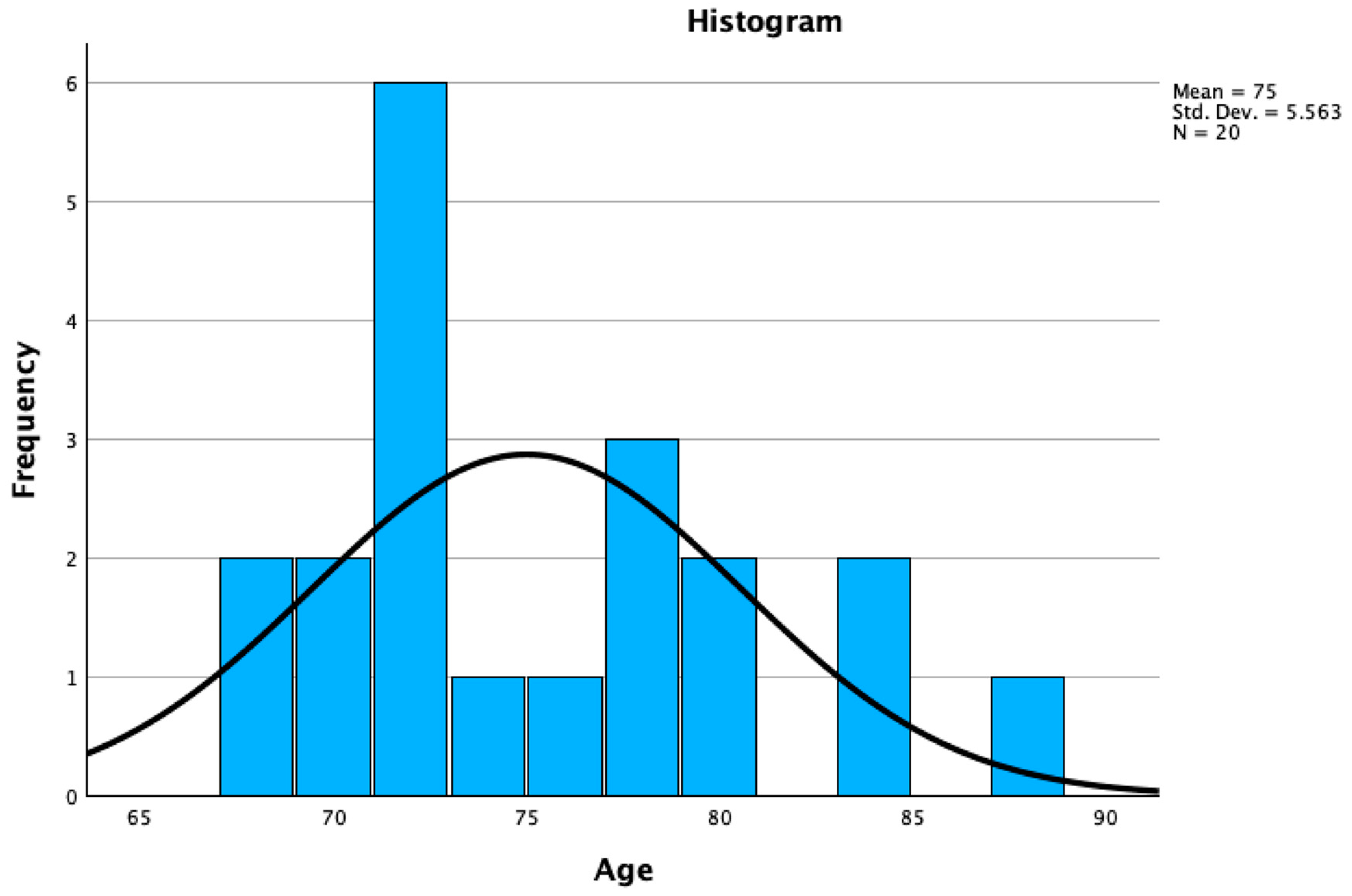
Graphic 1.
Histogram of Age of Participants.
Graphic 2.
Boxplots of Age of Participants.
Graphic 3.
3D Suicide Attempts versus QoSL.
Graphic 4.
Pareto diagram of total QoSL scores.
Graphic 5.
Distribution of Flanagan’s Scale Total scores.
4. Discussion
Carrying out feasibility testing of an instrument to be used is a fundamental step in research.[52] Finding appropriate tools to investigate the behavior of old patients is essential to obtain good results. When dealing with a little-known scenario, such as interpersonal factors that may be related to AD, there is little care in choosing the right instruments.
The suicide questionnaire ensured that it was well understood by healthy old people, which gave us the confidence to test it in states of cognitive impairment. It uses easy-to-understand language and allows a caregiver or close family member to help the patient without interfering and causing bias.
Flanagan developed the quality-of-life scale in 1970.[53] Its validation was carried out three decades later.[54] The QoLS has long been known to Brazilian researchers, having been used in Brazil since 1996.[55,56] It is a simple instrument to apply, and the homogeneous results of this pilot encourage us to use it in patients with cognitive impairment.
Quality of life is directly related to interpersonal well-being and vice versa.[57] Living in a comfortable residence promotes improvement in interpersonal experiences.[58] Being in good economic conditions brings peace of mind to relationships between family members.[59] Having good physical health conditions allows for better experiences between people.[60]
The questionnaire on factors associated with suicide has a broad interpersonal assessment. Its variables added to the QLoS scores can bring important deductions as to which interpersonal factors throughout life connected to suicidal behavior will be most associated with quality of life in old people.
Dysfunctional interpersonal experiences are one of the biggest causes of stress.[61] These are marital conflicts and mistreatment of children and adolescents.[62] Problems adapting to school and work, and the death of loved ones can be stressful in a world that is constantly changing.[63]
The world we live in is complex, dynamic, and full of stress.[64] It is important to seek to detail which experiences have the greatest impact on the health of the old people. Identify interpersonal factors that may be associated.[65] The crusade in the search to minimize the evils of neurodegenerative diseases ranges or computing resources from the search for possible correlated microorganisms to dysfunctional behavioral patterns and biomarkers.[66,67,68,69]
The more we study AD we realize that the breadth of the topic requires the formation of multidisciplinary teams for research.[70] No matter how distant computer science may seem from philosophy, from genetics to psychology, everything is connected in the search for better aging.[71]
Similarly, studying suicide requires an interdisciplinary team. Some countries are already well involved in studies on suicide. Until a decade ago, Brazil had one of the lowest suicide mortality rates. The mortality rate increased from 5/100,000 inhabitants in 2015 to 6.4/100,000 inhabitants in 2021.[72] We need to understand this phenomenon, which may be associated with AD.
Bauru is the most important urban hub in the center of Brazil’s main state.[73] It is historically an interconnection between all national regions. The results of a study of elderly people in this region can be easily generalized to the entire country. Brazil is a country that is experiencing increasing aging, with more than 10% of old people in its population.[74] The Brazilian people are multicultural and data from a broad study on AD in their population are useful for the entire world.[75]
5. Conclusions
In the difficult task of selecting instruments to assess interpersonal factors that may be an interface between AD and suicide, the two questionnaires used demonstrated great potential. They were well understood, quick to apply, and demonstrated homogeneity for a control group compared to patients with cognitive impairment. We will move on to collecting an adequate number of participants to observe which interpersonal complaints are the most relevant.
Answering the questions raised by the associations between suicide and AD can bring significant advances in the treatment of neurodegenerative diseases. We hope that these benefits will multiply for millions of people.
List of Abbreviations
| ACTH | adrenocorticotropin hormone |
| AD | Alzheimer’s Disease |
| ASA Theory | Alzheimer’s Disease and Suicide Associated Theory |
| BPSD | behavioral and psychological symptoms of dementia |
| CRH | corticotropin-releasing hormone |
| CDK5 | cyclin-dependent kinase 5 |
| GAS | General Adaptation Syndrome |
| GCs | glucocorticoids |
| GSK-3 | glycogen synthase kinase 3 |
| GSK-3β | glycogen synthase kinase-3β |
| HPA axis | hypothalamus-pituitary-adrenal axis |
| QoSL | Flanagan quality-of-life scale |
Author Contributions
Conceptualization, Juliano Flávio Rubatino Rodrigues; methodology, Juliano Flávio Rubatino Rodrigues and Moacir Fernandes de Godoy; software, Juliano Flávio Rubatino Rodrigues; validation, Kelly Cristina Atalia da Silva, Edward Goulart Junior, Fernando Victor Martins Rubatino and Pedro Marco Karan Barbosa; formal analysis, Juliano Flávio Rubatino Rodrigues; investigation, Juliano Flávio Rubatino Rodrigues; resources, Juliano Flávio Rubatino Rodrigues; data curation, Juliano Flávio Rubatino Rodrigues writing—original draft preparation, Juliano Flávio Rubatino Rodrigues; writing—review and editing, Lívia Peregrino Rodrigues; visualization, Franciany Cunha Peregrino Rodrigues, Hannes Fischer and Spencer Luiz Marques Payão; supervision, Gerardo Maria de Araújo Filho; project administration, Juliano Flávio Rubatino Rodrigues; funding acquisition, Juliano Flávio Rubatino Rodrigues. All authors have read and agreed to the published version of the manuscript.
Funding
The authors’ own resources were used.
Institutional Review Board Statement
The present study was conducted in accordance with the Declaration of Helsinki, and was submitted and approved by the ethics and research committee of the Faculty of Medicine of São José do Rio Preto with CAAE: 65514822.2.0000.5415.
Informed Consent Statement
All participants signed a free and informed consent agreeing to the publication of the data without revealing their names and or any other form of personal identification, such as address, etc.
Data Availability Statement
The data from the questionnaires used in this research are archived with the main researcher. They cannot be widely publicized to protect the identity of participants. Scientists are available for consultation, please feel free to send an email to julianofrr@terra.com.br and schedule a visit.
Acknowledgements
We thank all the volunteers who contributed to this study and Unimed for the availability of a location for the interviews.
Conflicts of Interest
The authors declare no conflicts of interest with the present study.
References
- Vermeulen, R.J.; Roudijk, B.; Govers, T.M.; Rovers, M.M.; Rikkert, M.G.M.; Wijnen, B.F.M. Prognostic Information on Progression to Dementia: Quantification of the Impacton Quality of Life. Journal of Alzheimer’s Disease 2024, 97, 1829–1840. [Google Scholar] [CrossRef] [PubMed]
- Keenan, H.E.; Czippel, A.; Heydari, S.; Gawryluk, J.R.; Mazerolle, E.L. Alzheimer’s Disease Neuroimaging Initiative. Intrinsic functional connectivity strength of SuperAgers in the default mode and salience networks: Insights from ADNI. Aging Brain 2024, 5, 100114. [Google Scholar] [CrossRef]
- Perneczky, R.; Dom, G.; Chan, A.; Falkai, P.; Bassetti, C. Anti-amyloi antibody treatments for Alzheimer’s disease. Eur J Neurol 2024, 31. [Google Scholar] [CrossRef]
- Li, H.-H.; Yao, X.-Y.; Tao, S.; Sun, X.; Li, P.-p.; Li, X.-x.; Liu, Z.-L.; Ren, C. Serotonin 2 Receptors, Agomelatine, and Behavioral and.
- Psychological Symptoms of Dementia in Alzheimer’s Disease. Behav Neurol 2021, 5533827.
- Calsolaro, V.; Femminella, G.D.; Rogani, S.; Esposito, S.; Franchi, R.; Okoye, C.; Rengo, G.; Monzani, F. Behavioral and Psychological Symptoms in Dementia (BPSD).
- and the Use of Antipsychotics. Pharmaceuticals 2021, 14, 246. [CrossRef] [PubMed]
- Tay, L.X.; Ong, S.C.; Tay, L.J.; Ng, T.; Parumasivam, T. Economic Burden of Alzheimer’s Disease: A Systematic Review. Value Health Reg Issues 2024, 40, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Egan, M.F.; Mukai, Y.; Voss, T.; Kost, J.; Stone, J.; Furtek, C.; Mahoney, E.; Cummings, J.L.; Tariot, P.N.; Aisen, P.S.; et al. Further analyses of the safety of verubecestar in the phase 3 EPOCH trial of mild-to-moderate Alzheimer’s disease. Alzheimers Res Ther 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Asher, S.; Priefer, R. Alzheimer’s disease failed clinical trials. Life Sci 2022, 306. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Lozupone, M.; Bellomo, A.; Imbimbo, B.P. Do anti-amyloid- β drugs affect neuropsychiatric status in Alzheimer’s disease patients? Ageing Research Reviews 2019, 55, 100948. [Google Scholar] [CrossRef]
- Rodrigues, J.F.R.; Rodrigues, L.P.; Araújo Filho, G.M. Alzheimer’s Disease and Suicide: An Integrative Literature Review. Current Alzheimer Research 2023, 20, 758–768. [Google Scholar] [CrossRef]
- !!! INVALID CITATION !!! (11-13).
- Calderón-Garcidueñas, L.; Gónzalez-Maciel, A.; Rreynoso-Robles, R.; Delgado-Chávez, R.; Mukherjee, P.S.; Kulesza, R.J.; Torres-Jardón, R.; Ávila-Ramírez, J.; Villarreal-Ríos, R. Hallmarks of Alzheimer disease are evolving relentlessly in Metropolitan Mexico City infants, children and young adults. APOE4 carries have higher suicide risk and higher odds of reaching NFT stage V at ≤ 40 years of age. Environmental Research 2018, 164, 475–487. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; González-Maciel, A.; Reynoso-Robles, R.; Kuleska, R.J.; Mukherjee, P.S.; Torres-Jardón, R.; Rönkkö, T.; Doty, R.L. Alzheimer’s disease and alpha-synuclein pathology in the olfactory bulbs of infants, children, teens and adults ≤ 40 years in Metropolitan Mexico City. APOE4 carriers at higher risk of suicide accelerate their olfactory bulb pathology. Enviromental Resesearch 2018, 166, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Bracha, H.S.; Kleinman, J.E. Postmortem Studies in Psychiatry. Psychiatr Clin North Am 1984, 7, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Crow, T.J.; Cross, A.J.; Cooper, S.J.; Deakin, J.F.W.; Ferrier, I.N.; Johnson, J.A.; Joseph, M.H.; Owen, F.; Poulter, M.; Lofthouse, R.; et al. Neurotransmitter receptors and monoamine metabolites in the brains of patients with Alzheimer-type Dementia and Depression, and Suicides. Neuropharmacology 1984, 23, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Pearlson, G.D.; Ross, C.A.; Lohr, W.D.; Rovner, B.W.; Chase, G.A.; Folstein, M.F. Association Between Family History of Affective Disorder and the Depressive Syndrome of Alzheimer’s Disease. Am J Psychiatry 1990, 147, 452–456. [Google Scholar] [PubMed]
- Ferris, S.H.; Hofeldt, G.T.; Carbone, G.; Masciandaro, P.; Troetel, W.M.; Imbimbo, B.P. Suicide in Two Patients with a Diagnosis of Probable Alzheimer Disease. Alzheimer Dis Assoc Disord 1999, 13, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Vega, U.; Kishikawa, Y.; Ricanati, E.; Friedland, R.P. Suicide and Alzheimer Disease. Am J Geriatr Psychiatry 2002, 10, 484–485. [Google Scholar] [CrossRef] [PubMed]
- Barak, Y.; Aizenberg, D. Suicide amongst Alzheimer’s Disease Patients: A 10-Year Survey. Dement Geriatr Cogn Disord 2002, 14, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Pagé, V. Cognitive deficits in a suicidal depressed alzheimer’s patient: a specific vulnerability? Int J Geriatric Psychiatry 2014, 29, 326–330. [Google Scholar]
- Hesdorffer, D.C. Comorbidity between neurological illness and psychiatric disorders. CNS Spectrums 2016, 21, 230–238. [Google Scholar] [CrossRef]
- Serafini, G.; Calcagno, P.; Lester, D.; Girardi, P.; Amore, M.; Pompili, M. Suicide Risk in Alzheimer’s Disease: A Systematic Review. Current Alzheimer Research 2016, 13, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Baptista, M.A.T.; Santos, R.L.; Kimura, N.; Lacerda, I.B.; Dourado, M.C.N. Disease awareness may increase risk of suicide in young onset dementia. Dement Nerupsychol 2017, 11, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Gvion, Y.; Levi-Belz, Y.; Hadlaczky, G.; Apter, A. On the role of impulsivity and decision-making in suicidal behavior. World J Psychiatry 2015, 5, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.J.; Currie, D. Biological predictors of suicidal behaviour in mood disorders. In Oxford Textbook of Suicidology and Suicide Prevention, 1 ed ed.; Oxford Universty Press: Oxford, 2009; pp. 335–341. [Google Scholar] [CrossRef]
- Friedman, N.P.; Robbins, T.W. The role of prefontal cortex in cognitive control and executive function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Baudic, S.; D, B.G.; Thibaudet, M.C.; Smagghe, A.; Remy, P.; Traykov, L. Executive function deficits in early Alzheimer’s disease and their relations with episodic memory. Arch Clin Neuropsychol 2006, 21, 15–21. [Google Scholar] [CrossRef]
- Rahioui, H.; Blecha, L.; Bottai, T.; Depuy, C.; Jacquesy, L.; Kochman, F.; Meynard, J.A.; Papeta, D.; Rammouz, I.; Ghachem, R. La thérapie interpersonnelle de la recherche à la pratique [Interpersonal psychotherapy from research to practice]. Encephale 2015, 41, 184–189. [Google Scholar] [CrossRef]
- Siette, J.; Dodds, L.; Surian, D.; Prgomet, M.; Dunn, A.; Westbrook, J. Social interactions and quality of life of residents in aged care facilities: A multi-methods study. PLoS ONE 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Brivio, P.; Sbrini, G.; Tarantini, L.; Parravicini, C.; Gruca, P.; et al. Stress Modifies the Expression of Glucocorticoid-Responsive Genes by Acting at Epigenetic Levels in the Rat Prefrontal Cortex: Modulatory Activity of Lurasidone. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Janthakhin, Y.; Kingtong, S.; Juntapremjit, S. Inhibition of glucocorticoid synthesis alleviates cognitive impairment in high-fat diet-induced obese mice. Compr Psychoneuroendocrinol 2022, 10. [Google Scholar] [CrossRef]
- Dioli, C.; Papadimitriou, G.; Megalokonomou, A.; Marques, C.; Sousa, N.; Sotiropoulos, I. Chronic Stress, Depreesion, and Alzheimer’s Disease: The Triangle of Oblivion. In GeNeDis, Vlamos, P., Ed. Springer: Switzerland, 2023; Vol. 1423, pp. 303-315.
- Turecki, G.; Brent, D. Suicide and suicidal behavior. Lancet 2017, 387, 1227–1239. [Google Scholar] [CrossRef]
- Rodrigues, J.F.R. O que é o suicídio: perfil epidemiológico de suicídio na cidade de Marília: proposições para prevenção; Dialética: São Paulo, 2022; Volume 1, p. 312. [Google Scholar]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B. Suicide and suicide risk. Nat Rev Dis Primers 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Sotiropoulos, I.; Silva, J.M.; Gomes, P.; Sousa, N.; Almeida, O.F.X. Stress and the Etiopathogenesis of Alzheimer’s Disease and Depression. In Tau Biology, Takashima, A., et al., Eds. Springer: Singapore, 2019; Vol. 1184, pp. 241-257.
- Majd, S.; Koblar, S.; Power, J. Compound C enhances tau phosphorylation at Serine 396 via PI3K activation in an AMPK and rapamycin independent way in differentiated SH-SY5Y cells. Neurosci Lett 2018, 670, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Gratuze, M.; Joly-Amado, A.; Buee, L.; Vieau, D.; Blum, D. Tau, Diabetes and Insulin. In Tau Biology, Takashima, A., Ed. Springer: Singapore, 2019; Vol. 1184, pp. 259-287.
- Saeedi, M.; Rashidy-Pour, A. Association between chronic stress and Alzheimer’s disease: Therapeutic effects of Saffron. Biomed Pharmacother 2021, 133, 110995. [Google Scholar] [CrossRef] [PubMed]
- Kalin, N.H. Adverstity, Trauma, Suicide, and Alzheimer’s Disease. Am J Psychiatry 2021, 178, 985–987. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E.; Byers, A.L.; Halpern, J.; Barnes, D.E. Addressing Suicide Risk in Patients Living With Dementia During the COVID-19 Pandemic and Beyond. The Gerontologist 2022, 62, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Orden, K.A.V.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.; Selby, E.A.; Joiner, T.E. The Interpersonal Theory of Suicide. Psychol Rev 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed]
- Seyle, H. Stress and the General Adaptation Syndrome. British Medical Journal 1950, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- Hassan, Z.A.; Schattner, P.; Mazza, D. Doing a pilot study: why is it essential? Malaysian Family Physician 2006, 1, 70–73. [Google Scholar] [PubMed]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: recommendations for good practise. Journal of Evaluation in Clinical Practise 2004, 10, 307–312. [Google Scholar] [CrossRef]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The Role and Interpretation of Pilot Studies in Clinical Research. J Psychiatr Res 2011, 45, 626–629. [Google Scholar] [CrossRef]
- Tokuda, Y.; Jimba, M.; Yanai, H.; Fujii, S.; Inoguchi, T. Interpersonal Trust and Quality-of-Life: A Cross-Sectional Study in Japan. PLoS ONE 2008, 3. [Google Scholar] [CrossRef]
- Rodrigues, J.F.R.; Araújo Filho, G.M.; Rodrigues, L.P.; Rubatino, F.V.M.; Fischer, H.; Payão, S.L.M. Development and validation of a questionnarie to measure association factors with suicide: An instrument for a populational survey. Health Science Reports 2023, 62023;6:e, e1396. [Google Scholar]
- Guewehr, K. Teoria da resposta ao item na avaliação de qualidade de vida de idosos. Universidade Federal do Rio Grande do Sul, 2007.
- In, J. Introduction of a pilot study. Korean Journal of Anesthesiology 2017, 70, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: applications to pratice, 3rd ed.; Hall, P.P., Ed. Pearson Prentice Hall: New Jersey (NJ), 2009; p. 892. [Google Scholar]
- Flanagan, J.C. A Research Approach to Improving Our Quality of Life. American Psychologist 1978, 33, 138–147. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Anderson, K.L.; Archenholtz, B.; Hägg, O. The Flanagan Quality of Life Scale: Evidence of Construct Validity. Health and Quality of Life Outcomes 2003, 1, 59. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Guedes, S.L.; Pereira, V.C. O ostomizado e a qualidade de vida: abordagem fundamentada nas dimensões da qualidade de vida: abordagem fundamentada nas dimensões da qualidade de vida proposta por Flanagan. Universidade de São Paulo, São Paulo, 1996.
- Galisteu, K.J.; Facundim, S.D.; Ribeiro, R.d.C.H.M.; Soler, Z.A.S.G. The Quality of Life of the Elderly in a senior friendly community: measurements with Flanagan’s scale. Arq Ciênc Saúde 2006, 13, 209–214. [Google Scholar]
- Luo, D.; Cai, X.; Wang, H.; Wang, Y.; Xu, J. The role of peer social relationships in psychological distress and quality of life among adolescents with type 1 diabetes mellitus: a longitudinal study. BMC Psychiatry 2024, 24. [Google Scholar] [CrossRef] [PubMed]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. In StatPearls, StatPearls Publishing: Treasure Island (FL), 2024; p https://www.ncbi.nlm.nih.gov/books/NBK565877/.
- Browning, C.J.; Qiu, Z.; Yang, H.; Zhang, T.; Thomas, S.A. Food, Eating, and Happy Aging: The Perceptions of Older Chinese People. Front Public Health 2019, 7. [Google Scholar] [CrossRef]
- B, P. Modeling the effects of physical activity, education, health, and subjective wealth on happiness based on Indonesian national survey data. BMC Public Health 2022, 22. [Google Scholar]
- Brasfield, M.B.; Bui, C.; Patihis, L.; Crowther, M.R.; Allen, R.S.; McDonough, I.M. Self-Reported Chronic Stress Is Unique Across Lifetime Periods: A Test of Competing Structural Equation Models. Gerontologist 2024, 64. [Google Scholar] [CrossRef] [PubMed]
- Owens, S.A.; Helms, S.W.; Rudolph, K.D.; Hastings, P.D.; Nock, M.K.; Prinstein, M.J. Interpersonal Stress Severity Longitudinally Predicts Adolescent Girls’ Depressive Symptoms: the Moderating Role of Subjective and HPA Axis Stress Responses. J Abnorm Child Psycho 2019, 47, 895–905. [Google Scholar] [CrossRef] [PubMed]
- R, S. Coping with stress: a physician’s guide to mental health in aging. Geriatrics 1996, 51, 46–48. [Google Scholar]
- Stickley, A.; Shirama, A.; Sumiyoshi, T. Psychotic experiences, perceived stress, and suicidal ideation among the general population during the COVID-19 pandemic: Findings from Japan. Schizophrenia Research 2023, 260, 49–55. [Google Scholar] [CrossRef] [PubMed]
- SC, S. Pathology in Relationships. Annu Rev Clin Psychol. 2021, 17, 577–601. [Google Scholar]
- Yu, B.; Wan, G.; Cheng, S.; Wen, P.; Yan, X.; Li, J.; Tian, H.; Gao, Y.; Zhong, Q.; Liu, J.; et al. Disruptions of Gut Microbiota are Associated with Cognitive Deficit or Preclinical Alzheimer’s Disease: A Cross-Sectional Study. Current Alzheimer Research 2023, 20, 875–889. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.G.; Coleman, T.; Buciuc, M.; Singh, N.A.; Pham, N.T.T.; Machulda, M.M.; Graff-Radford, J.; Whitwell, J.L.; Josephs, K.A. Behavioral and neuropsychiatric differences across two atypical Alzheimer’s disease variants: Logopenic Aphasia and Posterior Cortical Atrophy. J Alzheimer Dis 2024, 97, 895–908. [Google Scholar] [CrossRef] [PubMed]
- De, A.; Mishra, T.K.; Saraf, S.; Tripathy, B.; Reddy, S.S. A Review on the Use of Modern Computational Methods in Alzheimer’s Disease-Detection and Prediction. Current Alzheimer Research 2023, 20, 845–861. [Google Scholar] [CrossRef] [PubMed]
- Schermer, M.H.N. Preclinical Disease or Risk Factor? Alzheimer’s Disease as a Case Study of Changing Conceptualizations of Disease. The Journal of Medicine and Philosophy: A Forum for Bioethics and Philosophy of Medicine 2023, 48, 322–334. [Google Scholar] [CrossRef]
- Viola, L.F.; Nunes, P.V.; Yassuda, M.S.; Aprahamian, I.; Santos, F.S.; Santos, G.D.; Brum, P.S.; Borges, S.M.; Oliveira, A.M.; Chaves, G.F.; et al. Effects of a multidisciplinary cognitive rehabilitation program for patients with mild Alzheimer’s disease. Clinics (Sao Paulo) 2011, 66, 1395–1400. [Google Scholar] [CrossRef]
- Daniel, K.L.; McConnell, M.; Schuchardt, A.; Peffer, M.E. Challenges facing interdisciplinary researchers: Findings from a professional development workshop. PLoS One 2022, 17. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Suicide mortality and reports of self-harm in Brazil. Saúde, S.d.V.e., Ed. Ministério da Saúde Brasilia (DF), 2021; Vol. 52.
- Rigitano, M.H.C.; Barbassa, A.P. Participation in Bauru master plans.
- Brazil. In Environnement Urbain / Urban Environment, 2010; Vol. 4.
- Kirby, T. Brazil facing ageing population challenges. Lancet 2023, 402. [Google Scholar] [CrossRef] [PubMed]
- Santos, M. Dynamics of Cultural Diversity and Intercultural Communication in the Era of Multiculturalism and Cosmopolitism in Brazil. International Journal of Sociology 2024, 8, 1–13. [Google Scholar] [CrossRef]
Figure 1.
Stress and Brain.
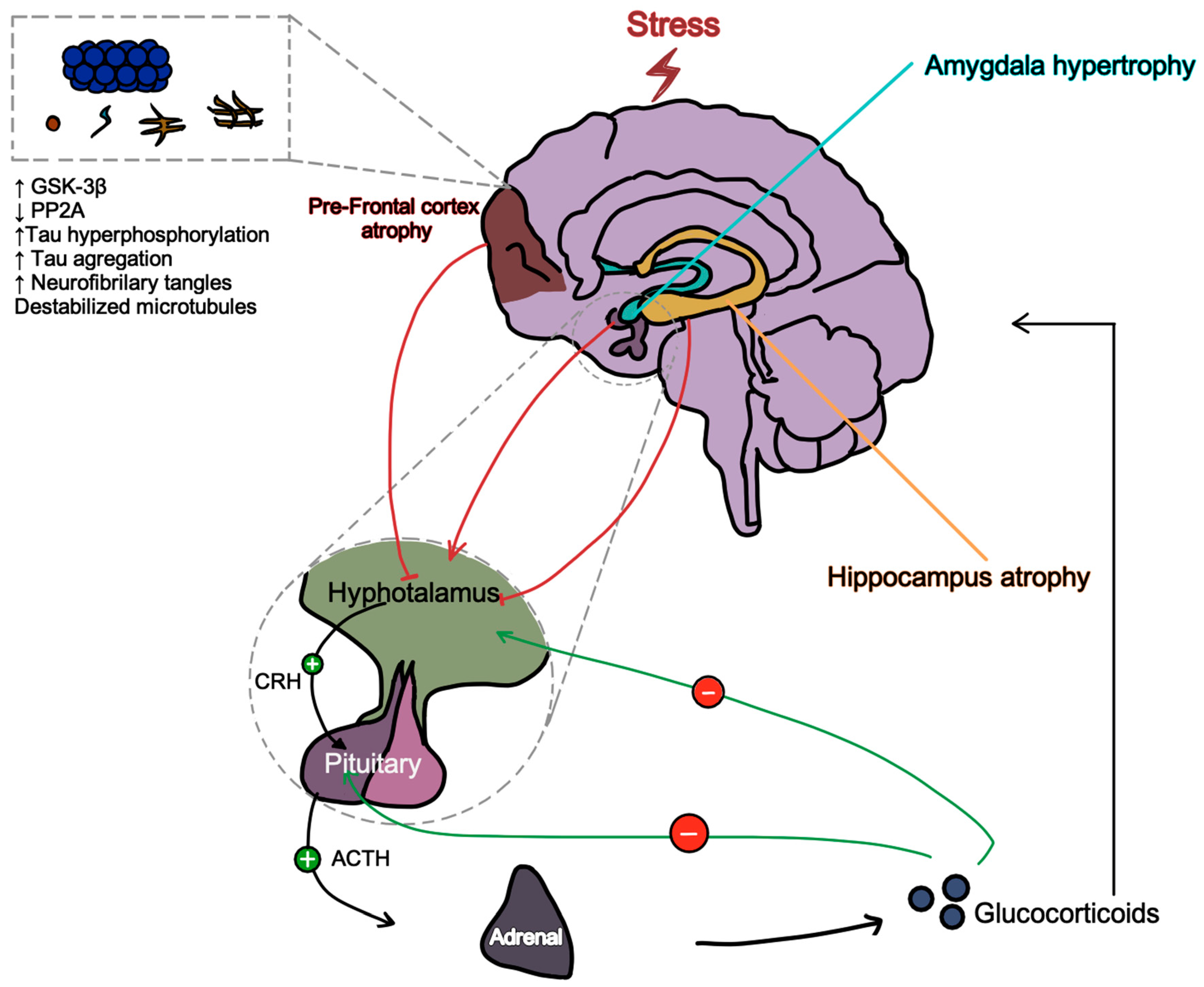
Figure 2.
Alzheimer’s Disease and Suicide Associated Theory.
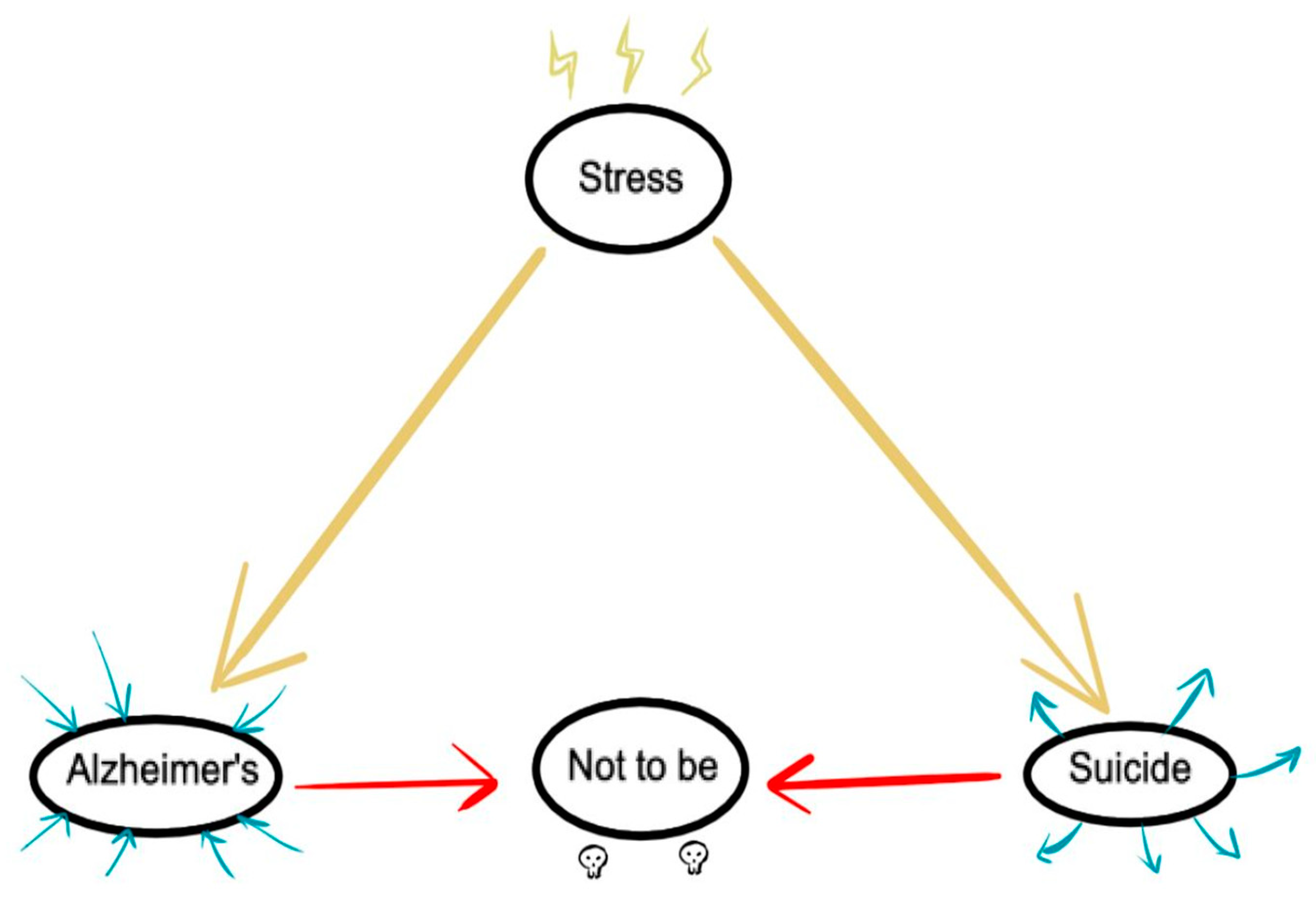

Table 1.
Frequency of Age of Participants.
| Age in years | Frequency | Percent | Valid Percent | Cumulative Percent |
| 68 | 2 | .3 | 10.0 | 10.0 |
| 69 | 1 | .2 | 5.0 | 15.0 |
| 70 | 1 | .2 | 5.0 | 20.0 |
| 71 | 2 | .3 | 10.0 | 30.0 |
| 72 | 4 | .6 | 20.0 | 50.0 |
| 73 | 1 | .2 | 5.0 | 55.0 |
| 75 | 1 | .3 | 5.0 | 60.0 |
| 78 | 3 | .5 | 15.0 | 75.0 |
| 79 | 1 | .2 | 5.0 | 80.0 |
| 80 | 1 | .2 | 5.0 | 85.0 |
| 83 | 1 | .2 | 5.0 | 90.0 |
| 84 | 1 | .2 | 5.0 | 95.0 |
| 87 | 1 | .2 | 5.0 | 100.0 |
| Total | 20 | 3.2 | 100.0 |
Table 2.
Frequency of Suicide Attempts.
| Suicide attempts yes=1 no=0 | |||||
| Frequency | Percent | Valid Percent | Cumulative Percent | ||
| Valid | 0 | 18 | 2.9 | 90.0 | 90.0 |
| 1 | 2 | .3 | 10.0 | 100.0 | |
| Total | 20 | 3.2 | 100.0 | ||
Table 3.
QoLS variables.
| Variable | N | Mode | Median | Minimum | Maximum | Percentil 25 |
Percentil 75 |
|---|---|---|---|---|---|---|---|
| 1 | 20 | 7 | 6.50 | 1 | 7 | 6.00 | 7.00 |
| 2 | 20 | 6 | 5.50 | 1 | 7 | 4.25 | 6.00 |
| 3 | 20 | 7 | 6.00 | 3 | 7 | 5.25 | 7.00 |
| 4 | 20 | 7 | 7.00 | 2 | 7 | 6.00 | 7.00 |
| 5 | 20 | 4 | 5.00 | 2 | 7 | 4.00 | 6.75 |
| 6 | 20 | 6 | 6.00 | 2 | 7 | 5.25 | 7.00 |
| 7 | 20 | 6 | 6.00 | 2 | 7 | 4.00 | 6.75 |
| 8 | 20 | 6 | 5.50 | 3 | 6 | 4.00 | 6.00 |
| 9 | 20 | 4 | 4.00 | 2 | 7 | 4.00 | 6.00 |
| 10 | 20 | 4 | 4.50 | 2 | 7 | 4.00 | 6.00 |
| 11 | 20 | 6 | 6.00 | 2 | 7 | 4.00 | 6.75 |
| 12 | 20 | 4 | 4.00 | 2 | 7 | 3.25 | 6.00 |
| 13 | 20 | 6 | 4.00 | 1 | 6 | 3.25 | 6.00 |
| 14 | 20 | 6 | 6.00 | 4 | 7 | 5.25 | 7.00 |
| 15 | 20 | 6 | 6.00 | 2 | 7 | 3.25 | 6.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



