Submitted:
12 May 2024
Posted:
13 May 2024
You are already at the latest version
Abstract
The endocannabinoid system (ECS) is a complex neuromodulatory network in the human body that have enormous impact in developing the central nervous system, as well as modulates various physiological processes. The ECS is made up of anandamide, 2-arachidonoylglycerol (2-AG), which are responsible for the synthesis and degradation of endocannabinoids, and enzymes such as FAAH and MAGL ensures the precise control over endocannabinoid levels. The ECS relies on CB1 receptors found in the central nervous system (CNS), and CB2 receptors found in the peripheral nervous system and immune cells. Dysregulation of the ECS has been associated with several health conditions, prompting investigations into its association with phytocannabinoids to harness their therapeutic potential. The ECS is intricately linked with the nervous system, and it is known to modulate neuronal activities in the CNS, influencing pain and mood modulation. The ECS is also associated with neuropathies-peripheral nerve damage leading to symptoms such as weakness, numbness and pain as evidenced in diabetic neuropathy, Guillain-Barré Syndrome, carpal tunnel syndrome, peripheral neuropathy, and postherpetic neuralgia. The focus of this review is on the interplay between 2-arachidonoylglycerol and anandamide amidohydrolase in neuropathy, elucidating their roles in pain regulation, inflammation, and specific neuropathies. The knowledge generated is expected to have broad implications, providing comprehensive insights into neuropathic conditions and how to improve on them. Ultimately, this understanding may lead to more effective treatments and improved quality of life for individuals affected by these conditions.
Keywords:
Endocannabinoid system (ECS)
; Anandamide
; 2-arachidonoylglycerol (2-AG)
; CB1 receptors
; CB2 receptors
; Enzymes FAAH and MAGL
; Neuropathies
; Cannabinoids
1. Introduction
The endocannabinoid system (ECS) is a delicate cell-signaling network that has captured enormous recognition in the past few years partly due to its stringent role in modulating various physiological processes in the human dynamic system. ECS acts through a complex association between endogenous compounds known as endocannabinoids, specialized receptors, and key enzymes that modulate these molecules [1,2]. Endocannabinoids are molecules elicited within the body naturally, with anandamide and 2-arachidonylglycerol (2-AG) being the most prevalent studied endocannabinoids. Anandamide and 2-AG are lipid-based molecules produced on demand in response to various physicochemical cues. These two kinds of endocannabinoids play an enormous role in maintaining homeostasis [3,4]. However, ECS effectiveness relies on two specific cannabinoid receptors known as CB1 and CB2 receptors distributed all over the body. CB1 receptors are primarily distributed in the central nervous system, specifically in the brain, whereas CB2 receptors are primarily distributed in the peripheral nervous system, immune cells, and other peripheral tissues. CB1 receptors modulate the release of neurotransmitters, synaptic plasticity, and the succinct regulation of various cognitive and emotional relevance. On the other hand, CB2 receptors are mainly associated with regulating inflammations and immunological responses [1,2,3,4].
Enzymes are crucial for the tight regulation of endocannabinoid levels. Two primary enzymes, fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL), are responsible for the synthesis and degradation of anandamide and 2-AG, respectively. These enzymes ensure that endocannabinoids are synthesized when needed and quickly broken down once their physiological roles are fulfilled [5,6]. The ECS acts as a biological "balancing" system, helping the body maintain homeostasis in response to internal and external stressors. When deviations from the body’s ideal set points, endocannabinoids are produced and activate cannabinoid receptors to change various physiological functions, including pain regulation, immune response modulation, appetite control, mood stabilization, and many other processes [7]. The ECS’s multifaceted nature underscores its importance in maintaining overall health and well-being. Disruptions in this system have been associated with a range of health conditions, including chronic pain, mood disorders, inflammation-related diseases, and more.
Consequently, understanding the ECS and its interactions with exogenous cannabinoids (like those found in cannabis) has become a burgeoning area of research and therapeutic development, with potential applications in the treatment of various medical conditions [8,9,10]. The ECS is connected to the nervous system, with CB1 receptors mainly found in the central nervous system (CNS), including the brain, where they regulate neurotransmitter release and synaptic plasticity. CB2 receptors are more prevalent in the peripheral nervous system and immune cells. Endocannabinoids can modulate neuronal activity in the CNS, affecting processes like pain perception and mood regulation [4,5].
Neuropathies are a group of disorders that involve damage to the peripheral nervous system, leading to various symptoms such as pain, numbness, and weakness. Diabetic neuropathy is a common complication of diabetes, which can lead to pain and numbness in the extremities. Another complication is peripheral neuropathy, which involves various conditions affecting the peripheral nerves, often resulting in tingling, burning, or shooting pain [11]. Furthermore, Guillain-Barré Syndrome, an autoimmune disorder that can lead to muscle weakness and paralysis, is another complication [12]. Carpel tunnel syndrome and postherpetic neuralgia are other known neuropathic complications involving the compression of the median nerves in the wrist, which can result in pain and hand numbness and shingles, which causes severe pain at the site of a previous herpes zoster infection, respectively [13]. The ECS has implications for neuropathic pain, as cannabinoid receptors are involved in pain modulation. Research into how cannabinoids interact with the ECS is ongoing, and cannabinoids like CBD and THC are among the primary compounds explored for their potential to alleviate neuropathic pain and other symptoms associated with neuropathies. However, the use of cannabinoids in neuropathic pain management should be under medical supervision due to potential side effects and variances in individual responses [14,15,16].
This review will comprehensively elaborate on the interplay between 2-Arachidonoylglycerol and Anandamide amidohydrolase in neuropathy and the role they play in pain regulation, inflammation in general, and specific neuropathies, enhancing an enormous role in understanding neuropathy mechanisms, improving pain management, inflammation and immune responses, specific neuropathies, and potential therapeutic targets, and improving our knowledge of medical cannabis.
2. Endocannabinoids
As part of the ECS, endocannabinoids are naturally occurring compounds distributed in the body responsible for modulating various physiological processes. The ECS consists of three primary endogenous cannabinoids (endocannabinoids, cannabinoid receptors, and enzymes), produced by the body [1,2]. The commonly studied endocannabinoids are anandamide (AEA) and 2-arachidonoylglycerol (2-AG). AEA and 2-AG share similar structures with phytocannabinoids (cannabinoids found in cannabis plant), such as cannabidiol (CBD), and tetrahydrocannabinol (THC) (Table 1). The endocannabinoids bind to two specific receptors known as cannabinoid receptors (CB1 and CB2 receptors), distributed throughout the body (central nervous system, immune cells, peripheral nervous system, and other organs). Similarly, monoacylglycerol lipase (MAGL) and fatty acid amide hydrolase (FAAH) are the two enzymes in the ECS responsible for catalyzing endocannabinoids once they have performed their function [2,3,4,5].
2.1. Pain Perception
Endocannabinoids are the intrinsic endogenous compounds elicited by the human system and are endowed with remarkable analgesic qualities via their innate association with the CB1 receptors found across various neural structures [17]. Innumerable sections of the brain, mainly the amygdala, superior colliculus, thalamus, rostral ventromedial medulla, and periaqueductal regions, are involved in initiating cannabinoid-induced analgesia. This pervasive distribution enables endocannabinoids to elicit pain-relieving influence via regulating neural activities within these critical brain regions. CB1 receptors are tactically located in the brain’s lamina X and dorsal horn [17,18]. Here, their primary function is the regulation of pain processing. Additionally, CB1 receptors modulate innate spinal levels’ actions, influencing endocannabinoids’ overall analgesic effects. The delicate interactions of CB1 receptor-mediated regulation aid in fine-tuning pain signaling at the spinal level, bestowing the overall analgesic effects of endocannabinoids.
CB1 receptors are in the ganglia root by peculiar subsets of sensory neurons housing pain-related neuropeptides, including α-calcitonin and P-related gene peptides (CGRP) [19,20]. Regardless of their relative infinitesimal presence, these receptors in the neurons hold profound functional essence. This is paramount in their capacity to regulate CGRP elicitation from the dorsal horn tissue. Immunohistochemically, CB1 receptors are also present in the central terminals and the peripheral peers of primary sensory afferents, expanding the horizon of their influence on pain transmission. Furthermore, Autochthonous application of CB1 receptor agonist to the skin has demonstrated remarkable plasticity and the ability to attenuate riposte to noxious stimuli, emphasizing the prowess and therapeutic implications of targeting peripheral CB1 receptors for pain management [21].
Recent research has provided convincing evidence highlighting the analgesic prowess of CB1 receptor agonists in human subjects, though the preclinical studies are still in their infant stage and ongoing. The preliminary findings underscore the burgeoning delight in capitalizing on the endocannabinoid system as a promising avenue for fabricating novel analgesic drugs, providing hope for more effective and safer pain management in subsequent times [22].
2.2. Inflammation
The paramount role of endocannabinoids is not only limited to the regulation of pain perception but also plays an essential role in immunomodulation and regulation of inflammation throughout the body. These multifaceted roles underscore their essence in maintaining homeostasis and general well-being [23]. The AEA and 2-AG orchestrate the immunomodulation and control of inflammation. Cannabinoid receptors are distributed across the tissues and immune cells. Mainly, CB2 receptors are established in the immune cells, such as macrophages, B and T cells, and monocytes. Immunomodulation occurs are a result of the binding between CB2 receptors and endocannabinoids. The binding also leads to the exertion of anti-inflammatory impacts by lessening the immune cells’ activity and controlling the release of pro-inflammatory molecules. This subsequently curtails chronic inflammation detrimental to the human system [24]. The ECS is commonly referred to as an "immune modulator" as it not only dampens immunological response but strives to keep it at bay to achieve homeostasis. The ECS can help improve immunity when it is invaded and compromised, and on the other hand, they can help temper immune response in cases of inflammation.
Furthermore, ECSs also act as immunological vehicles by conveying immune cells to sites of infection/injury by guiding immune cells to areas of the body where they are most needed. This behavior of the ECS is essential for the proper coordination of immune responses [25]. Another crucial responsibility of the ECS is the link it forms between the immune and the nervous system. The presence of receptors in immune cells to accommodate endocannabinoids influences neural signals, creating a crosstalk between systems in the body, which regulates immune responses in various physiological states [26]. With the dynamic and crucial role ECS plays as an anti-inflammatory and immunomodulatory agent, endocannabinoids and associated compounds have captured the attention of researchers and clinicians at large for their potential therapeutic role in immune-related situations such as arthritis, autoimmune disorders, and organ transplantation to minimize immune rejection [27,28].
2.3. Mood and Emotion
The intriguing part of the ECS is its ability to modulate mood, which emphasizes its role in physiological processes, mental and emotional well-being. The ability of the ECS to exert mood regulation is through influencing the activities of various neurotransmitters, especially dopamine and serotonin, generally recognized for their essential role in emotional and mental states. The ECS enables the homeostasis of these neurotransmitters, which is critical for mood stability [29]. Endocannabinoids affect mood through the regulation of the body’s response to stress. This is achieved when the ECS gets activated and enables the body to withstand the imposed stress, subsequently minimizing anxiety and enabling a sense of well-being. ECS malfunction has been attributed to heightened anxiety, leading to the development of anxiety disorders [30]. Reduced ECS malfunction has also been linked to depression and the inability to manage mood and stress properly. This may lead to an increase in depression. Researchers have garnered keen interest in exploring the association between the ECS and mood regulation and how phytocannabinoids such as CBD and THC can be used in medication targeting the ECS in managing depression and anxiety. The influence of the ECS on mood is extended to the formation of new neurons, a process known as neurogenesis, and the brain’s ability to reorganize itself, a process known as neuroplasticity. Neurogenesis and neuroplasticity are essential in maintaining brain health and mood stability [30,31].
2.4. Appetite and Metabolism
Another interesting area of the ECS that have ignited the interest of cannabinoid researchers is its association with appetite and metabolism. This association has significant implication for understanding physiological process and medical treatments. The ability of the ECS to modulate appetite lies in its intricate association with CB1 receptors which is expressed abundantly in the brain regions linked with appetite modulation [32]. Appetite and the desire to eat is significantly stimulated when endocannabinoid such as AEA binds to CB1 receptors. This is a natural process and it has enormous impact on maintaining energy balance and ensure that the body gets optimum nutrients. The ECS is involved in modulating hunger and satiety, and endocannabinoids are released with interact with receptors to increase appetite when there’s a need for the body to be nourished. Endocannabinoid levels drop when the body’s energy needs are met indicating a sense of satisfaction and fullness. The endocannabinoid system also plays an enormous role in metabolic processes, by influencing the energy expenditure and fat storage, through the regulation of the cellular powerhouse (mitochondria) responsible for fueling the body [33]. ECS dysbiosis can lead to metabolic disorders such as metabolic syndrome and obesity. Understanding of the ECS role in the modulation of appetite and metabolism has led to the key developments in medicine. Various medications are made to target the ECS to enhance appetite, especially in weak immune system as a result of cancer/AIDS where weight and appetite loss are typical [34]. A synthetic THC drug known as dronabinol has been developed to increase appetite and manage body weight. Researchers are further exploring ways the ECS manipulated to help manage weight and obesity. This may be achieved by regulating the ECS’s activity to reduce appetite and enhance the breakdown of adipose tissues [32,33,34].
2.5. Immune Function
The endocannabinoid system is involved in the regulation of immune responses throughout the body. This system operates through interactions between endocannabinoids, cannabinoid receptors (particularly CB1 and CB2 receptors), and enzymes responsible for endocannabinoid synthesis and degradation. CB2 receptors are primarily found in immune cells, while CB1 receptors are also expressed in various immune-related tissues [35]. Endocannabinoids can influence the extent and duration of inflammatory responses. Inflammation is the body’s natural defense mechanism to protect itself against harmful invaders such as bacteria, viruses, and other pathogens. However, excessive or chronic inflammation can be detrimental to health. The endocannabinoid system helps to maintain a balance by regulating the immune system’s response to infection and tissue damage [22].
Endocannabinoids also possess antioxidant properties that can help protect cells from oxidative stress, a common feature of inflammatory processes. This antioxidant activity contributes to the overall regulation of immune responses and helps to prevent excessive damage to healthy tissues. CB2 receptors, primarily found in immune cells, play a vital role in modulating immune cell function [36]. When endocannabinoids bind to CB2 receptors, they can influence immune cell migration, proliferation, and cytokine production. This modulation can significantly impact the outcome of immune responses, especially when the body is dealing with infections. The endocannabinoid system’s role in immune regulation suggests it can impact the body’s ability to fight infections. By influencing the intensity of the immune response, the system can either enhance the body’s defense mechanisms or, in some cases, dampen immune responses to prevent excessive tissue damage [37]. While the endocannabinoid system’s influence on immune responses is promising, striking a cautious balance is essential. Overly suppressing immune responses can be detrimental, as the body’s ability to fight infections is compromised. Therefore, research in this area aims to fine-tune the modulation of immune responses without impairing the body’s overall immune function [38].
2.6. Neuroprotection and Neuropathy
The endocannabinoid system is intricately involved in regulating neurotransmission, the communication process between nerve cells (neurons). It influences the release and uptake of various neurotransmitters, such as dopamine, serotonin, and glutamate. Proper neurotransmitter balance is critical for the normal functioning of the nervous system [6]. Neuroinflammation is a protective response by the brain and spinal cord to injury or infection. However, excessive or chronic neuroinflammation can lead to neuronal damage and neurodegenerative diseases. The endocannabinoid system helps to control neuroinflammatory responses [39,40]. Endocannabinoids like anandamide and 2-arachidonoylglycerol (2-AG) can dampen the release of pro-inflammatory molecules, thereby reducing the harmful effects of neuroinflammation. Endocannabinoids have antioxidant properties that protect neurons from oxidative stress, a process that can damage nerve cells and contribute to neurological disorders. Antioxidants counteract the harmful effects of free radicals and reduce neuronal damage. The endocannabinoid system plays a role in neurogenesis, generating new neurons from neural stem cells. Neurogenesis is particularly important in specific brain regions, such as the hippocampus, linked to memory and learning. Studies suggest that endocannabinoids can enhance neurogenesis and contribute to the brain’s ability to adapt to new information [41]. Dysregulation of the endocannabinoid system has been linked to various neurological disorders, including Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis. In these conditions, the system’s protective mechanisms are compromised. Researchers are investigating how to target the endocannabinoid system to develop therapies for neurodegenerative diseases, as it may enhance neuroprotection and slow disease progression. The endocannabinoid system’s neuroprotective properties have led to research into its potential therapeutic applications. Cannabinoid-based treatments are being explored for conditions like epilepsy, where protecting neurons from damage during seizures is crucial. Additionally, cannabinoid-based therapies are being studied for pain management and mood disorders, as the system’s influence on neurotransmitter balance can play a significant role in these conditions [42].
The human body’s production of endocannabinoids is a tightly regulated process designed to maintain physiological balance or homeostasis. These endocannabinoids are synthesized and used on demand in response to the body’s needs. This regulation is essential to ensure that the endocannabinoid system functions harmoniously and does not lead to imbalances in various physiological processes [10]. Endocannabinoids, such as anandamide and 2-arachidonoylglycerol (2-AG), are typically synthesized and released by neurons in response to specific cues. For example, when there is an injury, inflammation, or another disruption in homeostasis, neurons may produce endocannabinoids to help modulate the body’s response. One of the unique features of the endocannabinoid system is retrograde signaling. This means postsynaptic neurons often produce endocannabinoids and travel backward across synapses to bind with cannabinoid receptors on presynaptic neurons. This retrograde signaling allows endocannabinoids to influence the release of neurotransmitters, essentially providing feedback control over synaptic activity [43]. Endocannabinoid signaling is precise in its temporal and spatial regulation. It acts locally at the synapses where needed and for the time necessary to restore balance. This prevents excessive or prolonged activation of cannabinoid receptors. To prevent excessive or extended signaling, endocannabinoids are rapidly deactivated. Enzymes like fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL) break down anandamide and 2-AG once their job is done.
While the body’s endocannabinoids are precisely regulated, the endocannabinoid system can also be influenced by exogenous cannabinoids, which originate from outside the body [44]. Cannabis, for instance, contains over 100 different cannabinoids, the most well-known being THC (tetrahydrocannabinol) and CBD (cannabidiol). When these exogenous cannabinoids are introduced into the body, they can interact with the endocannabinoid system. THC, for example, can activate CB1 and CB2 receptors, leading to various effects, including altered perception, mood, and appetite. This is due to its psychoactive properties.
On the other hand, CBD does not directly bind to these receptors but can influence the endocannabinoid system in subtler ways. CBD is known for its potential anti-inflammatory and neuroprotective effects, and it may counteract some of the effects of THC, such as anxiety and paranoia [45,46]. Neuropathy, often referred to as peripheral neuropathy, is a medical condition affecting the peripheral nerves, an intricate network of nerves outside the central nervous system—comprising the brain and spinal cord. These peripheral nerves act as vital messengers facilitating communication between the central nervous system and the rest of the body, including muscles, skin, and internal organs [47].
3. Peripheral Nervous System
The Peripheral Nervous System (PNS) is an intricate and expansive network of nerves that acts as the primary communication pathway between the central nervous system (CNS) and the rest of the body. It plays a fundamental role in ensuring that our bodies can sense and interact with the external environment while maintaining essential internal functions.
One of the PNS’s critical functions is to transmit sensory information from various body parts to the brain. This enables us to perceive various sensations, including touch, temperature, pain, pressure, and vibrations. For example, when a hot surface is touched, specialized sensory receptors in the skin send signals through the PNS to the brain, interpreting this information as pain or heat, prompting a quick hand withdrawal to avoid injury [48]. In addition to sensory input, the PNS conveys signals from the brain to execute muscle movements. The PNS consists of motor neurons that transmit commands from the CNS to the muscles, instructing them to contract or relax. This is vital for everyday tasks, such as walking, reaching for objects, or any physical activity involving muscles [49]. The PNS further branches into the autonomic nervous system (ANS), which operates unconsciously and regulates vital processes like heart rate, digestion, respiratory rate, and other involuntary bodily functions. The ANS has two main divisions: the sympathetic and parasympathetic nervous systems. The sympathetic system prepares the body for "fight or flight" responses, while the parasympathetic system promotes "rest and digest" activities. This balance between the two is crucial for maintaining homeostasis in the body. Nerves in the PNS are like the body’s information superhighway. They consist of long, cable-like structures called axons, which can extend from the CNS to various body parts. These axons are coated with a fatty substance called myelin, which acts like insulation on an electrical wire, speeding up the transmission of signals. The PNS ensures signals travel quickly and accurately to and from the brain and spinal cord. The PNS is organized into different nerve plexuses and networks of intersecting nerves. These plexuses are responsible for controlling specific areas and functions of the body. For example, the brachial plexus controls the arm and hand muscles, while the lumbar plexus is associated with the lower back and legs [50,51].
3.1. Manifestations
Many individuals with neuropathy experience tingling sensations, often described as "pins and needles." This is typically due to abnormal nerve signaling, which sends incorrect messages to the brain. Neuropathy often leads to numbness, where affected individuals may have reduced or complete loss of sensation in specific areas. This can be particularly concerning as it increases the risk of unnoticed injuries or burns. Some neuropathy patients report a persistent burning pain, particularly in the hands or feet. This sensation can be chronic and challenging to manage. Nerves affected by neuropathy occasionally send erratic pain signals described as sharp, shooting, or electric shock-like pain [52]. This pain can be sudden and intense. Neuropathy may lead to muscle weakness, causing difficulty in performing specific tasks. For example, individuals may struggle to lift objects or maintain balance. Patients may experience a decline in coordination, making it challenging to perform activities that require fine motor skills, such as buttoning a shirt or writing. It may also affect the autonomic nervous system, leading to digestive problems like diarrhea, constipation, or difficulties in swallowing. Autonomic neuropathy can result in heart rate abnormalities, leading to rapid heartbeat or postural hypotension, where blood pressure drops when moving from sitting to standing [53]. Neuropathy can also result in skin changes like dryness, hair loss, or excessive sweating. Skin can become more prone to injury, and wounds may take longer to heal. Individuals with neuropathy may have difficulty sensing temperature changes, increasing the risk of burns or frostbite. Multiple nerves in various parts of the body are sometimes affected. This is known as polyneuropathy and often results in a combination of symptoms involving sensory, motor, and autonomic nerves.
It can vary from person to person based on its underlying cause. Some common neuropathy causes include diabetes, autoimmune diseases, infections, exposure to toxins, and hereditary factors. The diversity of neuropathy’s clinical presentation underscores the importance of accurate diagnosis and individualized treatment strategies. Management often involves addressing the underlying cause, symptomatic relief, and, in some cases, lifestyle adjustments to enhance overall well-being [11].
3.2. Diagnosis, Treatment and Management
The process of diagnosing neuropathy entails a multifaceted approach, commencing with a meticulous medical history assessment and an exhaustive physical examination, as succinctly explained in a review by Fisse et al., 2020 entitled "Comprehensive approaches for diagnosis, monitoring, and treatment of chronic inflammatory demyelinating polyneuropathy" [54]. To delineate the root cause and gauge nerve function, healthcare professionals commonly integrate nerve conduction studies or electromyography. Blood analyses and imaging investigations may be harnessed to identify causative factors ranging from diabetes to other origins. Neuropathy treatment aims to alleviate symptoms, address the underlying cause when possible, and enhance an individual’s quality of life. Depending on the specific symptoms and causes, treatment may include medications, pain management strategies, physical therapy, and lifestyle adjustments to manage contributing factors such as diabetes or alcohol consumption. The prognosis for neuropathy can be highly variable and largely depends on the underlying cause, early diagnosis, and treatment effectiveness [55]. In some instances, neuropathy can be reversible, while in other cases, it may be a chronic condition necessitating ongoing management. Preventing neuropathy often involves managing and mitigating risk factors. For example, people with diabetes can help prevent diabetic neuropathy by carefully controlling their blood sugar levels through a combination of a healthy diet, exercise, and medication management.
Additionally, practicing safety measures to minimize toxin exposure and adopting a healthy lifestyle can contribute to neuropathy prevention. Neuropathy is a challenging condition that can significantly impact an individual’s quality of life. Early diagnosis and appropriate management are essential for reducing symptoms and preventing further nerve damage [56].
3.3. Anandamide (AEA)
Anandamide (AEA) is a remarkable compound pivotal in the endocannabinoid system. This intricate signaling network is vital for maintaining physiological equilibrium and ensuring the proper functioning of various bodily processes. It has earned the affectionate moniker of the "bliss molecule" due to its remarkable ability to induce sensations of joy and relaxation.
One of its primary roles is in mood regulation. Anandamide can influence one’s emotional state and overall sense of well-being [57,58]. Its interaction with the endocannabinoid system, specifically the CB1 receptors in the central nervous system, allows it to exert its mood-altering effects. By binding to these receptors, anandamide contributes to the delicate balance of neurotransmitters, impacting feelings of happiness and relaxation. AEA also plays a substantial role in pain perception. It can modulate how the body experiences and responds to pain signals. This can have far-reaching implications for pain management and potentially lead to the developing of new analgesic treatments [59].
Moreover, AEA has a hand in appetite modulation. It can influence hunger and the desire to eat, impacting our overall dietary patterns. Understanding this connection is significant in addressing obesity and appetite disorders. Its influence is not limited to emotions, pain, and appetite. It also extends to fertility and reproduction. Its presence and functioning are integral for the reproductive system to work efficiently. One fascinating aspect of anandamide’s name is its origin. "Ananda" is a Sanskrit word that translates to "bliss" or "happiness." This name beautifully encapsulates the feelings of well-being and joy that this endocannabinoid can induce [60]. AEA’s discovery has profoundly enriched our comprehension of the endocannabinoid system’s role in human health and well-being. Its impact on mood, pain, appetite, fertility, and connection to sensations of bliss and relaxation highlights its significance in maintaining our overall physiological balance [61].
3.4. Two-Arachidonoylglycerol (2-AG)
2-Arachidonoylglycerol (2-AG) is one of the two main endocannabinoids produced by the human body, with the other being anandamide. 2-AG is a lipid molecule and part of the endocannabinoid system, a complex cell-signaling system that regulates various physiological processes. The endocannabinoid system is a critical regulator of various physiological functions, including mood, pain perception, immune responses, and more. It consists of endocannabinoids like 2-AG, cannabinoid receptors, and enzymes responsible for their synthesis and degradation [62].
As shown in Figure 1, 2-arachidonoylglycerol (2-AG) is synthesized on membranes of postsynaptic neuron terminals from diacylglycerol (DAG) by hydrolysis by diacylglycerol lipase (DAGL). The 2-AG is then released into the postsynaptic neurons, it activates cannabinoid receptor 1 (CB1). Activated CB1 further activates MAPK signaling cascades or activates K+ channels or inhibits Ca+ signaling. 2-AG finally is broken down into arachidonic acid and glycerol by monoglyceride lipase, thus ending the endocannabinoid signaling event.
2-Arachidonoylglycerol (2-AG) is a vital component of the endocannabinoid system, and its dynamic synthesis and degradation processes play a fundamental role in regulating various physiological functions. 2-AG is synthesized from lipid precursors found in cell membranes. These precursors are typically phospholipids containing arachidonic acid. The phospholipids serve as reservoirs for arachidonic acid, a polyunsaturated fatty acid. Various stimuli or physiological needs can activate enzymes like phospholipase C or phospholipase D. These enzymes cleave the arachidonic acid from the phospholipids, releasing it for further processing. Diacylglycerol lipase (DAGL) enzymes are responsible for the next step in 2-AG synthesis. They catalyze the conversion of diacylglycerol (DAG), produced from the cleaved arachidonic acid, into 2-AG. Unlike anandamide, produced on-demand and released when needed, 2-AG synthesis is considered more constitutive [63,64]. It is present in cells and can be rapidly released to maintain physiological balance. 2-AG is subject to rapid enzymatic degradation to prevent excessive or prolonged signaling. Two primary enzymes in its degradation are monoacylglycerol lipase (MAGL) and alpha-beta hydrolase domain-containing 6 (ABHD6). MAGL is known for its role in hydrolyzing 2-AG into arachidonic acid and glycerol. This degradation process contributes to the termination of 2-AG signaling and the recycling of its components. ABHD6 also plays a role in the enzymatic degradation of 2-AG, but its precise functions and mechanisms may vary between cell types and tissues [65].
2-Arachidonoylglycerol (2-AG) is a pivotal player in the endocannabinoid system, and its interactions with cannabinoid receptors are fundamental to its regulatory functions in the human body. These receptors, particularly CB1 (cannabinoid receptor type 1) and CB2 (cannabinoid receptor type 2) are distributed throughout various tissues and organs, and they contribute to the versatile physiological effects of 2-AG. CB1 receptors are primarily located in the central nervous system (CNS), where they are highly abundant. These receptors are notably present in brain regions responsible for various functions, including mood regulation, pain perception, and memory. Activation of CB1 receptors in the CNS, typically by cannabinoids like Δ9-tetrahydrocannabinol (THC), can induce psychoactive effects. These effects are responsible for the euphoria or "high" associated with cannabis use [66,67].
CB2 receptors are commonly found in peripheral tissues, including the immune system. They are especially prevalent in immune cells such as B, T, and macrophages. Activation of CB2 receptors is associated with immunomodulatory effects. 2-AG’s interaction with CB2 receptors can influence immune responses, including regulating inflammation and the body’s ability to fight infections. 2-AG is an endogenous ligand for both CB1 and CB2 receptors, meaning it is produced within the body and binds to these receptors. In the CNS, 2-AG plays a role in retrograde signaling, where postsynaptic neurons act on presynaptic neurons to synthesize it. This process can modulate the release of neurotransmitters and influence synaptic transmission. The interaction between 2-AG and CB1 receptors in the CNS contributes to pain modulation. By binding to CB1 receptors, 2-AG can influence pain perception and help manage pain. Through its interactions with CB2 receptors in immune cells, 2-AG is involved in immunomodulation and controlling inflammatory responses. The CB1 receptors in the CNS also play a role in mood regulation, and 2-AG’s activation of these receptors can influence emotional states and anxiety levels [68].
2-Arachidonoylglycerol (2-AG) plays a multifaceted role in regulating the immune response and controlling inflammation. Its interactions with cannabinoid receptor type 2 (CB2 receptors) on immune cells significantly affect the body’s ability to manage inflammatory processes and combat infections [4]. CB2 receptors are primarily expressed in immune cells, including B cells, T cells, macrophages, and dendritic cells. When 2-AG binds to these receptors, it can modulate immune responses. The activation of CB2 receptors by 2-AG leads to immunomodulatory effects. This means that 2-AG can regulate the behavior of immune cells. 2-AG can regulate the body’s inflammatory responses by influencing immune cell activity. It can help to reduce inflammation when it is excessive or unnecessary, thus preventing collateral tissue damage and promoting healing.
Furthermore, 2-AG’s role in managing inflammation is vital for controlling the body’s response to infections. Excessive inflammation can cause harm and disrupt the body’s ability to fight infections effectively [69]. 2-AG’s anti-inflammatory effects can help strike a balance between an appropriate immune response and preventing inflammation from spiraling out of control. 2-AG can also influence the production of various signaling molecules called cytokines, which are involved in immune responses. By regulating cytokine production, 2-AG can help maintain a balanced immune reaction. Given 2-AG’s ability to modulate inflammation, it has therapeutic potential for conditions characterized by excessive inflammation, such as autoimmune disorders, chronic inflammatory diseases, and even acute conditions with inflammatory components [70]. The regulation of inflammation and immune responses is essential for the body’s overall homeostasis and well-being. 2-AG, as a component of the endocannabinoid system, contributes to this balance, ensuring that the immune system responds appropriately to various challenges [71].
4. Endocannabinoid Receptor Type 1 (CB1)
CB1 receptors, primarily located within the central nervous system (CNS), are one of the two kinds of receptors in the ECS in the human body. Their primary function lies in their impact on various physiological processes. CB1 receptors are found in the cerebral cortex (the brain’s outermost layer) and are responsible for many higher-order roles, such as decision-making, memory, thoughts, and sensory perception [1]. CB1 receptor’s presence in the cerebral cortex suggests the role they may play in regulating cognitive processes. Within the brain is a seashore-shaped structure called the hippocampus, where CB1 receptors are abundant; the primary role of the hippocampus lies in regulating spatial navigation and memory. This further suggests the role CB1 receptors play in memory consolidation and learning. A review by Terral et al., on cannabinoid control of olfactory processes elucidated that ECS directly modulates olfactory processes, including learning, memory, and odor sensitivity [72]. Therefore, the activation of CB1 receptors in these areas can drastically influence memory processes. CB1 receptors are also found in the basal ganglia (a group of nuclei found deep within the brain known to modulate psychomotor skills such as learning) and have an enormous impact on the regulation of movement. This makes CB1 receptors play an unabated role in Parkinson’s disease and dystonia.
Furthermore, CB1 receptors are also present in the cerebellum, mainly associated with coordination of voluntary motor movements, posture, and balance. CB1 presence in the cerebellum indicates their role in motor coordination control [73] and underscores their function in controlling various cognitive and physiological processes. The activation of CB1 receptors thus has a direct impact on these regions and the associated processes [74]. CB1 receptor’s involvement in pain perception modulation lies in a wide array of functions they play in physiological processes. When these receptors are activated, they influence the transmission of signals in the CNS involved in pain, which in turn influences how the body interprets pains. The potential of CB1 activation in analgesics makes them suitable candidates for fabricating pain relief medications. CB1 receptors are also involved in mood modulation and play an essential role in feelings of pleasure, relaxation, euphoria, decreased anxiety, and general wellness [75].
Nevertheless, excessive activation of CB1 receptors, often associated with external cannabinoids, such as THC, may lead to adverse mood effects like paranoia and anxiety. Appetite and diet intake modulation is another critical function of CB1 receptors. When CB1 receptors are activated, especially by anandamide can stimulate appetite and the enjoyment of meals in a process known as the "munchies effect."
This is why the endocannabinoid system is associated with the "munchies" effect. Consequently, CB1 receptors are explored as potential targets for managing conditions involving appetite loss, like anorexia. CB1 receptors have a significant influence on memory and cognitive processes. They are concentrated in regions of the brain associated with memory formation and learning, such as the hippocampus [76,77]. Activation of CB1 receptors can affect memory consolidation and the ability to acquire new information. This aspect has both therapeutic implications as well as the potential for adverse cognitive effects with cannabinoid use. There is growing evidence that CB1 receptors may be involved in neuroprotection, particularly in response to various neurological insults. Activation of CB1 receptors may help protect nerve cells from damage and promote their survival in certain conditions. The basal ganglia, a brain region rich in CB1 receptors, plays a crucial role in motor control. CB1 receptor activation in this region can influence movement coordination and motor learning. Dysregulation of CB1 receptor function in the basal ganglia is associated with motor disorders like Parkinson’s disease and dystonia. CB1 receptors also have a significant impact on the release of neurotransmitters in the brain. By modulating the release of neurotransmitters like dopamine, serotonin, and gamma-aminobutyric acid (GABA), CB1 receptors regulate mood, motivation, and overall brain function. It is important to note that the effects of CB1 receptor activation can be complex and context-dependent. Excessive and insufficient activation of CB1 receptors can lead to various physiological and psychological effects, making their precise regulation a focus of research and therapeutic development [78].
Exogenous activation of CB1 receptors is a crucial aspect of understanding the effects of cannabinoids like THC, which is a critical component of the cannabis plant. When introduced into the body, THC readily crosses the blood-brain barrier and binds to CB1 receptors, which are abundant in regions associated with sensory perception, such as the cerebral cortex. This interaction leads to altered sensory experiences, including changes in visual, auditory, and tactile perceptions. Users often report heightened sensory sensitivity and alterations in time perception. THC’s binding to CB1 receptors in brain areas linked to mood regulation can induce changes in emotional states. These mood changes can manifest as euphoria, relaxation, and reduced anxiety [79]. However, they can also include undesirable effects such as increased anxiety, paranoia, or mood swings, particularly in individuals’ sensitive to THC or when consumed in excessive amounts. THC stimulates CB1 receptors located in areas related to appetite regulation. This activation often leads to increased appetite, commonly called the "munchies." THC’s influence on appetite is a complex interplay of neurochemical processes, including the release of neurotransmitters like dopamine and the modulation of feeding behavior. The binding of THC to CB1 receptors in regions like the hippocampus, which are crucial for memory and cognitive processes, can result in temporary cognitive impairment. THC’s influence may affect short-term memory, attention, and problem-solving abilities. This is one of the reasons why activities requiring focus and concentration, such as driving, are discouraged under the influence of THC. THC’s activation of CB1 receptors also impacts reward pathways in the brain, particularly the mesolimbic dopamine system. This can lead to the reinforcement of certain behaviors and a perceived sense of reward or pleasure, which contributes to its potential for misuse or addiction.
Additionally, CB1 receptors in the basal ganglia, an area of the brain responsible for motor control, can be activated by THC [80,81]. This can result in altered motor coordination and difficulties with tasks requiring precise movements. These effects can be particularly pronounced in high-dose or inexperienced users. Finally, the interaction between THC and CB1 receptors can produce perceptual distortions, sometimes referred to as hallucinogenic effects. These may include altered visual, auditory, or even olfactory perceptions. Such distortions contribute to the recreational appeal of cannabis but can also lead to unpleasant experiences, especially for those who are not prepared for them.
It is imperative to know that the effects of THC on CB1 receptors can vary widely depending on factors such as the dose consumed, individual sensitivity, and the method of consumption (e.g., smoking, ingestion). Additionally, while the recreational use of cannabis is well-known, the medicinal use of THC and other cannabinoids is also being explored for its potential in managing various health conditions. Knowledge of the intricate interaction between THC and CB1 receptors sheds light on the complexity of cannabis’s effects on the human body and mind [82].
4.1. The Role of CB1 Receptors in Inflammatory Disorders
While CB1 receptors are predominantly known for their presence in the central nervous system (CNS) and their role in regulating neurotransmission and neuromodulatory functions, a growing body of research suggests their potential involvement in mitigating inflammatory disorders. In this context, CB1 receptor activation has shown promise in preclinical and animal studies to address various inflammatory conditions.
Studies have suggested that CB1 receptor activation may have anti-inflammatory properties. In preclinical and animal models, researchers have explored the effects of activating CB1 receptors in the context of various inflammatory disorders. The findings indicate that CB1 receptor activation can reduce inflammatory responses in peripheral tissues [83]. Atherosclerosis is characterized by plaque buildup in arterial walls, leading to inflammation and narrowing of the arteries. Preclinical studies have indicated that CB1 receptor activation may help alleviate inflammation in the arterial walls, potentially slowing down the progression of atherosclerosis. This is significant as atherosclerosis is a major contributor to cardiovascular diseases [84]. Inflammatory processes within the nervous system are implicated in various neuroinflammatory disorders, including multiple sclerosis and neurodegenerative diseases. CB1 receptors have been explored as potential therapeutic targets in managing these conditions. The activation of CB1 receptors may have neuroprotective effects and can help reduce inflammation in the CNS [85]. CB1 receptors play a role in pain modulation, and pain often accompanies inflammation. By reducing inflammation through CB1 receptor activation, it is possible to alleviate inflammatory pain indirectly. This aspect has implications for managing pain associated with inflammatory conditions [86]. CB1 receptors in peripheral tissues and immune cells are key players in regulating the immune response. Activation of these receptors can influence the activity of immune cells, potentially reducing the release of pro-inflammatory signaling molecules. This immunomodulatory effect contributes to the anti-inflammatory potential of CB1 receptor activation [87]. It is essential to consider the psychoactive effects associated with CB1 receptor activation, primarily driven by compounds like THC. The psychoactivity limits the clinical utility of direct CB1 receptor activation, particularly in managing inflammatory disorders. Therefore, research efforts aim to find ways to harness the anti-inflammatory properties of CB1 receptors while minimizing psychotropic effects [88].
4.2. Therapeutic Potential of CB1 Modulation
The therapeutic potential of CB1 (cannabinoid receptor type 1) modulation is a subject of significant research and interest due to its wide-ranging effects on various physiological processes.
CB1 receptors play a crucial role in pain perception and modulation. Modulating CB1 receptors can provide pain relief, especially in chronic pain conditions. This has therapeutic implications for conditions like neuropathic pain, fibromyalgia, and chronic inflammatory pain [89]. CB1 receptors are linked to mood regulation. Modulating CB1 receptors can have antidepressant and anxiolytic effects, making them potential targets for mood disorder treatments. This includes conditions like depression, anxiety, and post-traumatic stress disorder (PTSD) [90]. Activation of CB1 receptors can stimulate appetite. This effect is relevant in medical contexts where appetite loss is a concern, such as cancer-associated anorexia and cachexia. Medications targeting CB1 receptors can help improve appetite and promote weight gain [91]. CB1 receptors influence the emetic reflex, making them a target for antiemetic medications. Drugs that modulate CB1 receptors, such as dronabinol and nabilone, are used to manage chemotherapy-induced nausea and vomiting [92].
CB1 modulation has shown potential in the treatment of neurological disorders. This includes conditions like epilepsy, where cannabinoids like CBD (Cannabidiol) that interact with CB1 receptors have been investigated for their anticonvulsant effects [93]. CB1 receptors are involved in neuroprotection, and their modulation can have a protective effect on nerve cells. This is relevant in conditions like neurodegenerative diseases, including Alzheimer’s disease and Parkinson’s disease [94]. CB1 receptors are present in the eye and play a role in regulating intraocular pressure. Modulating CB1 receptors can be beneficial in the management of glaucoma, a condition characterized by increased intraocular pressure [95]. CB1 modulation is relevant in the treatment of addiction and substance use disorders. Medications that target CB1 receptors can help reduce cravings and withdrawal symptoms associated with addictive substances like opioids [96]. CB1 receptors are involved in the regulation of metabolism and energy balance. Modulating CB1 receptors can affect managing obesity and related metabolic disorders [10]. While CB2 receptors are more directly associated with immune responses, CB1 modulation also shows promise in treating inflammatory disorders. Preclinical and animal studies have demonstrated the potential of CB1 receptor activation in reducing inflammation, especially in peripheral tissues [10,12].
5. Endocannabinoid Receptor Type 2 (CB2)
CB2, or cannabinoid receptor type 2, is one of the two primary types of cannabinoid receptors in the endocannabinoid system. CB2 receptors are distinct from CB1 receptors, with different bodily distribution and functions.
CB2 receptors, or cannabinoid receptor type 2, are primarily in peripheral tissues throughout the body. Unlike CB1 receptors, which are highly concentrated in the central nervous system (CNS), CB2 receptors are not prominently present in the brain and spinal cord. Instead, they are strategically distributed in various peripheral organs and tissues. CB2 receptors are notably abundant in immune cells [97]. They are prevalent in white blood cells, including B, T, and macrophages. This distribution reflects the critical role of CB2 receptors in regulating the immune response. CB2 receptors in immune cells allow them to directly influence immune functions, particularly in response to inflammation and infection [98].
Secondary lymphoid organs, such as the spleen, tonsils, and thymus, also contain CB2 receptors. These organs are essential immune system components, where various immune cells are activated and coordinated to respond to infections and other immune challenges. CB2 receptors in these organs reinforce their involvement in immune function. Besides immune-related sites, CB2 receptors can be found in various peripheral tissues, including the gastrointestinal tract, skin, bone, liver, and more. Their presence in peripheral tissues highlights their role in modulating local physiological processes and maintaining homeostasis. CB2 receptors in peripheral tissues and immune cells indicate their involvement in the endocannabinoid system’s regulation of inflammation and immune responses [99]. Endocannabinoids like 2-arachidonoylglycerol (2-AG) can bind to CB2 receptors, influencing immune cells’ behavior and their role in managing inflammation and immune balance. CB2 receptors in immune cells can affect the immune response by regulating the production and release of various signaling molecules, such as cytokines and chemokines. Activating CB2 receptors on immune cells can help control inflammation, a critical component of the immune response to infections and injuries. The distribution of CB2 receptors in peripheral tissues and immune cells has led to the exploration of CB2-selective compounds as potential therapeutics. Researchers are investigating the development of medications that target CB2 receptors for treating inflammatory disorders and other immune-related conditions while avoiding the psychotropic effects associated with CB1 receptor activation [100].
CB2 receptors, also known as cannabinoid receptor type 2, are primarily associated with modulating the immune response. They are critical components of the endocannabinoid system, a complex cell-signaling system that influences various physiological processes. CB2 receptors are found predominantly on immune cells and immune-related tissues, positioning them as regulators of immune function. One of the central functions of CB2 receptors is to control inflammation. Inflammation is a natural immune response triggered by the body to protect against infections, injuries, and other challenges [101]. However, excessive or prolonged inflammation can lead to chronic inflammatory conditions and tissue damage. CB2 receptors help maintain the balance of the immune response, ensuring that inflammation is appropriately initiated and resolved. CB2 receptors are activated by endocannabinoids, which are naturally occurring compounds within the body. These endocannabinoids, such as 2-arachidonoylglycerol (2-AG), bind to CB2 receptors, initiating signaling pathways that influence immune cell behavior. When CB2 receptors are activated, they can modulate the production and release of various immune signaling molecules, including cytokines and chemokines, essential for coordinating immune responses. Activation of CB2 receptors on immune cells can have anti-inflammatory effects [102]. This means that CB2 receptor activation can help dampen excessive immune responses, reduce the production of pro-inflammatory molecules, and mitigate inflammation-related tissue damage.
Consequently, CB2 receptors are potential targets for the development of anti-inflammatory medications. Given this, CB2 receptors have garnered attention as potential targets for therapeutic interventions. Researchers are exploring the development of CB2-selective compounds to treat various inflammatory conditions, including autoimmune diseases, chronic inflammatory disorders, and neuroinflammatory conditions. CB2 receptors also play a role in pain management. They are involved in modulating pain signals, particularly when pain is associated with inflammation. CB2 receptors indirectly contribute to managing inflammatory pain by controlling the immune response and inflammation. CB2 receptors have been implicated in tissue protection. Their anti-inflammatory effects can help prevent damage to tissues and organs caused by excessive inflammation [103]. This protective function is particularly relevant in conditions where inflammation can destroy tissue, such as autoimmune diseases. In addition to their immune-related functions, CB2 receptors are also found in the central nervous system and are associated with neuroprotection. Their activation can influence processes that support the survival of nerve cells, making them relevant in conditions involving neuroinflammation and neurodegenerative diseases [104].
CB2 receptors, a subtype of cannabinoid receptors, are predominantly found in immune cells, making them a pivotal component of the body’s immune regulation system. These receptors are strategically positioned on immune cells, including white blood cells like B cells, T cells, and macrophages. The immune system is a complex network of cells and molecules that work together to defend the body against infections and other challenges. When the immune system is activated, it triggers various immune responses. During this process, the body produces endocannabinoids [105], such as 2-arachidonoylglycerol (2-AG), as part of the body’s endocannabinoid system. These endocannabinoids act as signaling molecules and bind to CB2 receptors on immune cells. The activation of CB2 receptors on immune cells results in the modulation of immune cell activity. This modulation helps in balancing the immune response and maintaining immune homeostasis. CB2 receptors can control the immune response by influencing the production and release of immune signaling molecules, including cytokines and chemokines. One of the critical functions of CB2 receptor activation is the reduction of pro-inflammatory signaling. When endocannabinoids engage CB2 receptors, they can inhibit the release of pro-inflammatory molecules [106]. This anti-inflammatory effect is crucial in resolving inflammation and preventing excessive immune activation, which can lead to chronic inflammatory conditions. Inflammation is a natural immune response, but it needs to be appropriately initiated and resolved to prevent tissue damage. CB2 receptors play a significant role in the resolution of inflammation by controlling the activities of immune cells. By reducing pro-inflammatory signaling, CB2 receptors help the immune system switch from an inflammatory state to a resolution phase, allowing the body to recover from infections or injuries [107]. CB2 receptors are essential for balancing immune responses. They ensure the immune system responds adequately to threats but does not become overactive or dysfunctional. The modulation of immune cell activity through CB2 receptors is central to this process. Due to their role in immune regulation, CB2 receptors have therapeutic implications. Researchers are exploring the development of CB2-selective compounds to treat various immune-related conditions, including autoimmune diseases, inflammatory disorders, and neuroinflammatory diseases. The goal is to harness the immune-modulating properties of CB2 receptors for therapeutic benefit [108].
Cannabidiol (CBD), a non-psychoactive cannabinoid found in cannabis, has garnered considerable attention for its potential to influence CB2 receptors and the broader endocannabinoid system indirectly. Unlike THC (tetrahydrocannabinol), CBD does not directly bind to CB2 receptors [83]. Instead, it modulates the endocannabinoid system by influencing the levels of endocannabinoids, such as anandamide and 2-arachidonoylglycerol (2-AG). By doing so, CBD can regulate inflammation and immune responses mediated by CB2 receptors. CBD’s mechanism of action involves multiple pathways [85]. One key aspect is its ability to inhibit the enzymes that break down endocannabinoids, such as fatty acid amide hydrolase (FAAH) for anandamide. By blocking these enzymes, CBD increases the availability and activity of endocannabinoids in the body [109]. This is particularly relevant in CB2 receptors, as anandamide and 2-AG are the endocannabinoids that interact with these receptors. CBD has shown promise in reducing inflammation by enhancing endocannabinoid signaling and indirectly impacting CB2 receptors. CB2 receptors, predominantly found in immune cells, regulate the immune response and control inflammatory processes. When endocannabinoids bind to CB2 receptors, they can modulate immune cell activity, potentially reducing the release of pro-inflammatory signaling molecules [110]. CBD’s ability to increase endocannabinoid levels can amplify these effects, contributing to regulating inflammation in the body. The interaction between CBD and the endocannabinoid system, including CB2 receptors, affects immune system balance. By dampening excessive immune responses, CBD may be beneficial in conditions characterized by immune system hyperactivity, such as autoimmune diseases and chronic inflammatory disorders [111]. While more research is needed to fully understand the extent of CBD’s impact on CB2 receptor function, early studies, and preclinical research has provided insights into its potential immunomodulatory effects. The interplay between cannabinoids like CBD and CB2 receptors has clinical relevance. Studies are exploring CBD-based therapies for various conditions linked to immune dysregulation and inflammation, including autoimmune diseases, neuroinflammatory disorders, and chronic pain associated with inflammation. The goal is to harness the therapeutic potential of CBD without the psychoactive effects associated with THC. As research progresses, a better understanding of the specific mechanisms by which CBD influences CB2 receptors may lead to the development of targeted treatments for immune-related conditions. Many studies also explore CBD’s antibiotic properties, especially against gram-negative bacteria [46,112].
5.1. CB2 Receptors and Inflammatory Disorders
Inflammatory Bowel Disease (IBD), such as ulcerative colitis and Crohn’s disease, are characterized by chronic inflammation in the gastrointestinal tract. Recent studies have suggested that CB2 receptors play an enormous role in regulating inflammation. Hence, research into CB2 receptors has ignited the interest of many scientists. With a thorough dive into CB2 receptor agonists, scientists can minimize immune system inflammatory response in the gut [108]. This may subsequently reduce the symptoms and progression of IBD. Furthermore, researchers are also exploring the possibility of employing CB2 receptor agonists in curtailing rheumatoid arthritis autoimmune disease characterized by joint inflammation and damage. By activating CB2 receptors, researchers can regulate immune response, minimizing inflammation and joint pains linked with rheumatoid arthritis. This may offer novel treatment modalities for controlling the symptoms of these life-threatening diseases [107]. CB2 receptors also hold profound role in regulating multiple sclerosis (MS)- a neuroinflammatory disorder characterized by inflammation in the central nervous system (CNS). Studies suggest the possible role CB2 agonists may play in regulating immune responses within the CNS, potentially reducing the progression of MS and associated neurological diseases. Finally, chronic inflammation disorders are another area where CB2 receptors function by reducing persistent inflammation, such as systemic lupus erythematosus (SLE), inflammatory lung disorder, and psoriasis [10]. CB2 receptor’s potential to regulate immune responses and mitigate inflammation holds excellent potential for treating inflammatory diseases. Delving into the intricacies of CB2 receptors, researchers may be able to develop novel therapeutics that provide selective anti-inflammatory effects while eliminating the psychotic side effects incriminated with the activation of CB1 receptors such as THC [11].
5.2. Therapeutic Potential of CB2 Modulation
Researchers are exploring novel ways to develop CB2-selective compounds (CB2 agonists) that target only CB2 receptors. CB2-selective compounds aim at harnessing the immunomodulatory and anti-inflammatory properties of CB2 receptor activation with limited or zero effects on CB1 receptors [113]. The selective approach is paramount for ensuring the tolerability and safety of CB2 receptor-related therapies. By reducing untargeted reactions with CB1 receptors, it is easy to minimize the potential side effects related to psychoactive and cognitive impairment. Beyond inflammatory diseases, CB2 receptors also hold profound potential in autoimmune diseases such as rheumatoid arthritis and inflammatory bowel disease. CB2-selective compounds may regulate the hyperactive immune response and minimize inflammation-related tissue damage [114]. Table 2 explains some therapeutic potential of regulating both CB1 and CB2 receptors.
6. CB1 and CB2 Specific Neuropathies
Investigations into neuropathies associated directly with CB1 and CB2 receptors are still in the infant stage. However, specific neuropathies such as diabetic, peripheral, HIV, Chemotherapy-induced, multiple sclerosis, and cannabis hyperemesis syndrome associated with CB1 and CB2 will be discussed here.
6.1. Diabetic Neuropathy
Diabetic neuropathy is a common complication of diabetes mellitus, affecting a reasonable amount of people suffering from both type 1 and type 2 diabetes. It is a progressive condition associated with nerve damage due to its persistence and high blood glucose levels exposure. The nerve damage often results in numbness, tingling, pain, and weakness in extreme situations. Several factors contribute to the development of diabetic neuropathy. Some of these include inflammation, oxidative stress, and impaired nerve blood flow [128]. Recent studies have elucidated the potential contribution of the ECS, mainly focusing on CB1 and CB2 receptors, in the diabetic neuropathy pathophysiology. The activation of CB1 receptors has been associated with inflammation and pain perception and may lead to pain hypersensitivity common symptom of diabetic neuropathy. Pain perception and relief to individuals with diabetic neuropathy may be minimized by modulating CB1 receptors [129].
CB2 receptors play an enormous role in the modulation of inflammation. Inflammation in nerves and surrounding tissues can worsen nerve damage and pain in diabetic neuropathy. Activating CB2 receptors may minimize inflammatory pain, potentially minimizing tissue damage and protecting neurons. Several studies have explored how the modulation of CB1 and CB2 receptors can potentially impact and correct diabetic neuropathy [130]. Most of the studies have focused on cannabinoid-based compounds like CBD and synthetic cannabinoids. The study also focuses on understanding how cannabinoid levels are changed in individuals with diabetes. Whiles there is so much potential in cannabinoid-based treatments, more research is needed to ascertain the efficacy and safety of these cannabinoid-based approaches for managing diabetic neuropathy [131].
6.2. Peripheral Neuropathy
Peripheral neuropathy is a general term used to describe a wide array of nerve disorders that affect the peripheral nervous system, including those outside the brain and the spinal cord. Peripheral neuropathy manifests as damaged nerves responsible for transmitting sensory information, motor signals, and autonomic function between the CNS and the rest of the body, such as the skin, limbs, internal organs, and muscles [132]. Typical side effects side effect of specific cancer treatments is known as chemotherapy-induced peripheral neuropathy. Chemotherapy-induced neuropathy can lead to nerve damage and cause symptoms such as tingling, numbness, and pain. Studies have demonstrated that viral (HIV/AIDS, Lyme disease, and shingles (herpes zoster)) and bacterial infections can damage peripheral nerves and lead to peripheral neuropathy [133]. Guillain- Barré syndrome is an autoimmune disorder that causes the immune system to mistakenly attack peripheral nerves, leading to damage and neurological symptoms. There has been growing interest in recent years in accessing the potential role of CB1 and CB2 receptors in controlling neuropathic pain related to peripheral neuropathy. Several studies have explored the role of cannabinoids and other related compounds that interact with the ECS as potential remedies for neuropathic pain [14]. Especially studies have explored the role of CBD and synthetic cannabinoids in modulating neuropathic pain perception, reduced inflammation, and neuropathic pain. Multiple sclerosis (MS) is another chronic autoimmune disorder that targets and affects the CNS, resulting in a wide range of neurological symptoms. Neuropathic pain is a common complication of MS, which has a significant impact on the quality of life of individuals suffering from this infection [134].
CB1 and CB2 receptors have emerged as promising areas of interest in managing MS due to their dynamic role in modulating immune responses and inflammation. Whiles the exact mechanisms/pathophysiology of MS are complex and require demyelination and inflammation in the CNS, the immune system involvement is crucial for the disease progression. CB1 and CB2 receptors distributed across the CNS and the peripheral immune system have become potential targets for modulating MS-related neuropathic symptoms [135]. Specifically, CB2 receptors play a crucial role in regulating immune responses and inflammation due to their abundance in the immune cells. Hence, modulating CB2 receptors has been explored extensively as a potential remedy for preventing inflammatory processes seen in MS. The activation of CB2 receptors may suppress the immune system’s inappropriate activation against the CNS. Similarly, activating CB1 receptors may also prevent neuropathic pain related to MS [136].
6.3. HIV-Associated Neuropathy
HIV-associated neuropathy affects individuals living with HIV/AIDS, and this condition can be excruciating and have a tremendous impact on the victim’s quality of life. Several studies are underway aiming at exploring the impact of CB1 and CB2 receptors in managing inflammation and pain related to HIV neuropathy [137]. A common symptom of HIV-associated neuropathy is neuropathic pain. CB1 receptors are involved in managing pain perception. Hence, the activation of CB1 receptors can significantly impact neuropathic pain by modulating pain signaling trajectories. HIV/AIDS negatively impacts the immune system where CB2 receptors are predominantly located, leading to chronic inflammation [138]. Regulating CB2 receptors could minimize the immune system’s hyperactive inflammatory responses associated with HIV infection. HIV elicits both indirect and direct effects on the central nervous system, and CB1 receptors are specifically associated with the survival of nerve cells and neuroprotection, which is essential in preserving nerve function regarding HIV-associated neuropathy [139]. The activation of CB2 receptors in the immune system may lead to the release of anti-inflammatory signaling molecules. Excessive inflammation may cause nerve damage and pain. Hence, managing inflammation is crucial [140].
6.4. Chemotherapy-Induced Neuropathy
Cancer patients undergoing chemotherapy are often afflicted with chemotherapy-induced neuropathy. Chemotherapy-induced neuropathy is a distressing condition associated with nerve damage, resulting in various neuropathic symptoms such as numbness, tingling sensation, and pain. CB1 and CB2 receptors have gained significant attention for modulating chemotherapy-induced neuropathy and improving neuroprotection [141]. A primary symptom of chemotherapy-induced neuropathy is neuropathic pain. It is a severe, burning pain and shooting in its extremities. Activation of CB1 receptors in the central nervous system is the major player in regulating pain perception and plays a crucial role in alleviating pain and distressing symptoms. Tetrahydrocannabinol (THC) is the main phytocannabinoids with tremendous potential in pain management, even though THC’s psychoactive effects have limited this potential [142]. Never cells can be damaged with chemotherapy agents and subsequently, compromise the nervous system’s integrity associated with neuroprotection. Hence, the activation of CB1 receptors may help in the proliferation and health of nerve cells, potentially eliminating the severity of neuropathy related to inflammation and oxidative stress. Additionally, the activation of CB2 receptors may also lead to the release of anti-inflammatory molecules and antioxidants. The ECS may contribute to reducing or protecting neuropathic symptoms by regulating inflammation and oxidative stress. Neuropathic symptoms can significantly impact a patient’s quality of life. Therefore, properly managing these conditions is essential to ensure that individuals may continue their chemotherapy without any deleterious side effects. The ECS capacity in pain management, neuroprotection, and inflammation is explored to improve the quality of life of people undergoing chemotherapy [143].
6.5. Cannabis Hyperemesis Syndrome (CHS)
Prolonged and heavy cannabis indulgence has been attributed to the development of a condition known as cannabis hyperemesis (CHS), characterized by recurrent instances of vomiting, abdominal pains, and severe nausea. CHS is not a neuropathy; it is nonetheless relevant to discussion because of its association with the CB1 receptor activation in the gastrointestinal tract. CHS can be manifested in different phases [144]. The prodromal phase is when individuals experience early morning nausea and discomfort attributed to cannabis withdrawal. The second phase is the hyperemic phase, characterized by abdominal pain and severe vomiting. People experiencing this symptom seek relief through frequent baths or hot showers. The final phase is the recovery phase, which follows the cessation of cannabis indulgence, and it is characterized by resolution [145]. The cyclic occurrences may cause rampant dehydration, complications, and weight loss. The ECS plays a central role in modulating gastrointestinal function where CB1 receptors are present and contribute to regulating nausea, vomiting, and appetite. Neurotransmitters such as serotonin and dopamine involved in vomiting reflexes are modulated with the activation of CB1 receptors. Studies stipulate that chronic indulgence in cannabis and CB1 receptor activation in the gut can lead to the development of CHS [146]. Additionally, the balance of neurotransmitters may be disrupted by overstimulating CB1 receptors. This claim is based on the observation that CHS manifestation tends to influence the cessation of cannabis use. The diagnosis of CHS is challenging because it has symptoms overlapping/similar to various other situations, such as recurring vomiting syndrome and gastrointestinal disorders [147]. Differential diagnosis is often used to rule out other potential issues. Primarily, CHS’s best treatment is stopping cannabis use completely. Furthermore, symptoms can be managed through supportive care measures, such as intravenous fluids to cater for dehydration. Antiemetic medications may also be employed to tackle issues with vomiting and nausea or hospitalization in severe cases [148]. Research on CHS remains limited, and severally scientists are still exploring this area. This is to say that the association between heavy and prolonged cannabis use, CB1 receptors, and their involvement in the development of CHS is poorly elucidated. It does, however, underscore the enormous role the ECS plays in modulating gastrointestinal functions and its possible influence on its dysregulation due to cannabis indulgence [149].
References
- Ramirez, C.E.M.; Ruiz-Pérez, G.; Stollenwerk, T.M.; Behlke, C.; Doherty, A.; Hillard, C.J. Endocannabinoid signaling in the central nervous system. Glia 2022, 71, 5–35. [Google Scholar] [CrossRef] [PubMed]
- Lutz, B. Neurobiology of cannabinoid receptor signaling. Dialog- Clin. Neurosci. 2020, 22, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; Demartini, C.; Zanaboni, A.M.; Francavilla, M.; De Icco, R.; Ahmad, L.; Tassorelli, C. The endocannabinoid system and related lipids as potential targets for the treatment of migraine-related pain. Headache J. Head Face Pain 2022, 62, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Chanda, D., Neumann, D. and Glatz, J.F., 2019. The endocannabinoid system: Overview of an emerging multi-faceted therapeutic target. Prostaglandins, Leukotrienes and Essential Fatty Acids, 140, pp.51-56.
- Komarnytsky, S.; Rathinasabapathy, T.; Wagner, C.; Metzger, B.; Carlisle, C.; Panda, C.; Le Brun-Blashka, S.; Troup, J.P.; Varadharaj, S. Endocannabinoid System and Its Regulation by Polyunsaturated Fatty Acids and Full Spectrum Hemp Oils. Int. J. Mol. Sci. 2021, 22, 5479. [Google Scholar] [CrossRef] [PubMed]
- Kilaru, A. and Chapman, K.D., 2020. The endocannabinoid system. Essays in Biochemistry, 64(3), pp.485-499.
- Finn, D.P.; Haroutounian, S.; Hohmann, A.G.; Krane, E.; Soliman, N.; Rice, A.S. Cannabinoids, the endocannabinoid system, and pain: A review of preclinical studies. Pain 2021, 162, S5–S25. [Google Scholar] [CrossRef] [PubMed]
- Schultz, S., Gould, G.G., Antonucci, N., Brigida, A.L. and Siniscalco, D., 2021. Endocannabinoid system dysregulation from acetaminophen use may lead to autism spectrum disorder: Could cannabinoid treatment be efficacious? Molecules, 26(7), p.1845.
- Petrie, G., Balsevich, G., Fuzesi, T., Aukema, R., Wouter, D., Van der Stelt, M., Bains, J.S. and Hill, M.N., 2022. Disruption of Tonic Endocannabinoid Signaling Triggers the Generation of a Stress Response. bioRxiv, pp.2022-09.
- Lowe, H.; Toyang, N.; Steele, B.; Bryant, J.; Ngwa, W. The Endocannabinoid System: A Potential Target for the Treatment of Various Diseases. Int. J. Mol. Sci. 2021, 22, 9472. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, H.C., Wunderlich, G., Fink, G.R. and Sommer, C., 2020. Diagnosis of peripheral neuropathy. Neurological research and practice, 2, pp.1-7.
- Khan, Z.; Ahmad, U.; Ualiyeva, D.; Amissah, O.B.; Khan, A.; Noor, Z.; Zaman, N. Guillain-Barre syndrome: An autoimmune disorder post-COVID-19 vaccination? Clin. Immunol. Commun. 2022, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Karjalanen, T.; Raatikainen, S.; Jaatinen, K.; Lusa, V. Update on Efficacy of Conservative Treatments for Carpal Tunnel Syndrome. J. Clin. Med. 2022, 11, 950. [Google Scholar] [CrossRef] [PubMed]
- Campos, R.M.P.; Aguiar, A.F.L.; Paes-Colli, Y.; Trindade, P.M.P.; Ferreira, B.K.; Reis, R.A.d.M.; Sampaio, L.S. Cannabinoid Therapeutics in Chronic Neuropathic Pain: From Animal Research to Human Treatment. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Behl, T.; Sharma, L.; Shah, O.P.; Yadav, S.; Sachdeva, M.; Rashid, S.; Bungau, S.G.; Bustea, C. Exploring the molecular pathways and therapeutic implications of angiogenesis in neuropathic pain. Biomed. Pharmacother. 2023, 162, 114693. [Google Scholar] [CrossRef] [PubMed]
- Svensson, C.K., 2020. CBD for the treatment of pain: What is the evidence? Journal of the American Pharmacists Association, 60(6), pp.e80-e83.
- Prospéro-García, O.; Contreras, A.E.R.; Gómez, A.O.; Herrera-Solís, A.; Méndez-Díaz, M. Endocannabinoids as Therapeutic Targets. Arch. Med Res. 2019, 50, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-López, A.; Pastor, A.; de la Torre, R.; La Porta, C.; Ozaita, A.; Cabañero, D.; Maldonado, R. Role of the endocannabinoid system in a mouse model of Fragile X undergoing neuropathic pain. Eur. J. Pain 2021, 25, 1316–1328. [Google Scholar] [CrossRef]
- Fowler, C.J. The endocannabinoid system – current implications for drug development. J. Intern. Med. 2020, 290, 2–26. [Google Scholar] [CrossRef] [PubMed]
- Wołyniak, M.; Małecka-Wojciesko, E.; Zielińska, M.; Fabisiak, A. A Crosstalk between the Cannabinoid Receptors and Nociceptin Receptors in Colitis—Clinical Implications. J. Clin. Med. 2022, 11, 6675. [Google Scholar] [CrossRef] [PubMed]
- Finn, D.P.; Haroutounian, S.; Hohmann, A.G.; Krane, E.; Soliman, N.; Rice, A.S. Cannabinoids, the endocannabinoid system, and pain: a review of preclinical studies. Pain 2021, 162, S5–S25. [Google Scholar] [CrossRef] [PubMed]
- Osafo, N., Yeboah, O.K. and Antwi, A.O., 2021. The endocannabinoid system and its modulation of the brain, gut, joint, and skin inflammation. Molecular biology reports, 48(4), pp.3665-3680.
- Hryhorowicz, S.; Kaczmarek-Ryś, M.; Zielińska, A.; Scott, R.J.; Słomski, R.; Pławski, A. Endocannabinoid System as a Promising Therapeutic Target in Inflammatory Bowel Disease – A Systematic Review. Front. Immunol. 2021, 12, 790803. [Google Scholar] [CrossRef] [PubMed]
- Scheau, C.; Draghici, C.; Ilie, M.A.; Lupu, M.; Solomon, I.; Tampa, M.; Georgescu, S.R.; Caruntu, A.; Constantin, C.; Neagu, M.; et al. Neuroendocrine Factors in Melanoma Pathogenesis. Cancers 2021, 13, 2277. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, I.; Syamala, S.; Ayariga, J.A.; Xu, J.; Robertson, B.K.; Meenakshisundaram, S.; Ajayi, O.S. Modulatory Effect of Gut Microbiota on the Gut-Brain, Gut-Bone Axes, and the Impact of Cannabinoids. Metabolites 2022, 12, 1247. [Google Scholar] [CrossRef] [PubMed]
- Garani, R., Watts, J.J. and Mizrahi, R., 2021. The endocannabinoid system in psychotic and mood disorders, a review of human studies. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 106, p.110096.
- Pinna, G. Endocannabinoids and Precision Medicine for Mood Disorders and Suicide. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Stasiulewicz, A.; Znajdek, K.; Grudzień, M.; Pawiński, T.; Sulkowska, J.I. A Guide to Targeting the Endocannabinoid System in Drug Design. Int. J. Mol. Sci. 2020, 21, 2778. [Google Scholar] [CrossRef] [PubMed]
- Arjmand, S.; Behzadi, M.; Kohlmeier, K.A.; Mazhari, S.; Sabahi, A.; Shabani, M. Bipolar disorder and the endocannabinoid system. Acta Neuropsychiatr. 2019, 31, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Myers, M.N.; Zachut, M.; Tam, J.; Contreras, G.A. A proposed modulatory role of the endocannabinoid system on adipose tissue metabolism and appetite in periparturient dairy cows. J. Anim. Sci. Biotechnol. 2021, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Chadha, S.; Sachdeva, M.; Sehgal, A.; Kumar, A.; Dhruv; Venkatachalam, T.; Hafeez, A.; Aleya, L.; Arora, S.; et al. Understanding the possible role of endocannabinoid system in obesity. Prostaglandins Other Lipid Mediat. 2020, 152, 106520. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V. and Silvestri, C., 2019. Lifestyle and metabolic syndrome: Contribution of the endocannabinoidome. Nutrients, 11(8), p.1956.
- McDew-White, M.; Lee, E.; Premadasa, L.S.; Alvarez, X.; Okeoma, C.M.; Mohan, M. Cannabinoids modulate the microbiota–gut–brain axis in HIV/SIV infection by reducing neuroinflammation and dysbiosis while concurrently elevating endocannabinoid and indole-3-propionate levels. J. Neuroinflammation 2023, 20, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Shu, Z.; Gu, X.; Wu, Y.; Yang, J.; Deng, H. The Endocannabinoid System as a Potential Therapeutic Target for HIV-1-Associated Neurocognitive Disorder. Cannabis Cannabinoid Res. 2023, 8, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Costiniuk, C.T. and Jenabian, M.A., 2019. Cannabinoids and inflammation: Implications for people living with HIV. Aids, 33(15), pp.2273-2288.
- Argenziano, M.; Tortora, C.; Bellini, G.; Di Paola, A.; Punzo, F.; Rossi, F. The Endocannabinoid System in Pediatric Inflammatory and Immune Diseases. Int. J. Mol. Sci. 2019, 20, 5875. [Google Scholar] [CrossRef] [PubMed]
- Kopustinskiene, D.M.; Masteikova, R.; Lazauskas, R.; Bernatoniene, J. Cannabis sativa L. Bioactive Compounds and Their Protective Role in Oxidative Stress and Inflammation. Antioxidants 2022, 11, 660. [Google Scholar] [CrossRef] [PubMed]
- Patil, A.P., Patil, T.M., Shinde, A.R., Vakhariya, R.R., Mohite, S.K. and Magdum, C.S., 2021. Nutrition, lifestyle, and immunity: Maintaining optimal immune function and boosting our immunity. Asian Journal of Pharmaceutical Research and Development, 9(3), pp.129-136.
- Dokalis, N. and Prinz, M., 2019, November. Resolution of neuroinflammation: Mechanisms and potential therapeutic option. In Seminars in immunopathology (Vol. 41, No. 6, pp. 699-709). Berlin/Heidelberg: Springer Berlin Heidelberg.
- Yang, H.; Zeng, Q.; Silverman, H.A.; Gunasekaran, M.; George, S.J.; Devarajan, A.; Addorisio, M.E.; Li, J.; Tsaava, T.; Shah, V.; et al. HMGB1 released from nociceptors mediates inflammation. Proc. Natl. Acad. Sci. 2021, 118. [Google Scholar] [CrossRef] [PubMed]
- O’Brien. K., Blair, P., O’Brien, K. and Blair, P., 2021. Endocannabinoid System. Medicinal Cannabis and CBD in Mental Healthcare.
- Cristino, L.; Bisogno, T.; Di Marzo, V. Cannabinoids and the expanded endocannabinoid system in neurological disorders. Nat. Rev. Neurol. 2020, 16, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.M. and Piomelli, D., 2022. Cannabinoids and endocannabinoids. In Neuroscience in the 21st Century: From Basic to Clinical (pp. 2129-2157). Cham: Springer International Publishing.
- van Egmond, N., Straub, V.M. and van der Stelt, M., 2021. Targeting endocannabinoid signaling: FAAH and MAG lipase inhibitors. Annual Review of Pharmacology and Toxicology, 61, pp.441-463.
- Ibrahim, I., Ayariga, J.A., Xu, J., Adebanjo, A., Robertson, B.K., Samuel-Foo, M. and Ajayi, O.S., 2023. CBD-resistant Salmonella strains are susceptible to epsilon 34 phage tailspike protein. Frontiers in Medicine, 10, p.1075698.
- Spiller, K.J., Bi, G.H., He, Y., Galaj, E., Gardner, E.L. and Xi, Z.X., 2019. Cannabinoid CB1 and CB2 receptor mechanisms underlie cannabis reward and aversion in rats. British Journal of Pharmacology, 176(9), pp.1268-1281.
- Feldman, E.L., Callaghan, B.C., Pop-Busui, R., Zochodne, D.W., Wright, D.E., Bennett, D.L., Bril, V., Russell, J.W. and Viswanathan, V., 2019. Diabetic neuropathy. Nature Reviews Disease primers, 5(1), p.41.
- Sloan, G.; Selvarajah, D.; Tesfaye, S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat. Rev. Endocrinol. 2021, 17, 400–420. [Google Scholar] [CrossRef] [PubMed]
- Evans-Martin, F., 2022. The nervous system. Infobase Holdings, Inc.
- Oaklander, A.L.; Mills, A.J.; Kelley, M.; Toran, L.S.; Smith, B.; Dalakas, M.C.; Nath, A. Peripheral Neuropathy Evaluations of Patients With Prolonged Long COVID. Neurol. - Neuroimmunol. Neuroinflammation 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Selvarajah, D.; Kar, D.; Khunti, K.; Davies, M.J.; Scott, A.R.; Walker, J.; Tesfaye, S. Diabetic peripheral neuropathy: Advances in diagnosis and strategies for screening and early intervention. Lancet Diabetes Endocrinol. 2019, 7, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic Pain: From Mechanisms to Treatment. Physiol. Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.S.; Karlsson, P.; Gylfadottir, S.S.; Andersen, S.T.; Bennett, D.L.; Tankisi, H.; Finnerup, N.B.; Terkelsen, A.J.; Khan, K.; Themistocleous, A.C.; et al. Painful and non-painful diabetic neuropathy, diagnostic challenges and implications for future management. Brain 2021, 144, 1632–1645. [Google Scholar] [CrossRef] [PubMed]
- Fisse, A.L., Motte, J., Grüter, T., Sgodzai, M., Pitarokoili, K. and Gold, R., 2020. Comprehensive approaches for diagnosing, monitoring, and treating chronic inflammatory demyelinating polyneuropathy. Neurological research and practice, 2(1), pp.1-14.
- Pop-Busui, R.; Ang, L.; Boulton, A.; Feldman, E.L.; Marcus, R.; Mizokami-Stout, K.; Singleton, J.R.; Ziegler, D. Diagnosis and Treatment of Painful Diabetic Peripheral Neuropathy. ADA Clin. Compend. 2022, 2022, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, M., 2023. Assessing Neuropathy Risk and Quality of Life in Sedentary Obese, Prediabetic, and Type 2 Diabetic Populations: A Comprehensive Questionnaire-Based Approach. Clinical Images and Case Reports, 1(01), pp.29-38.
- Matei, D.; Trofin, D.; Iordan, D.A.; Onu, I.; Condurache, I.; Ionite, C.; Buculei, I. The Endocannabinoid System and Physical Exercise. Int. J. Mol. Sci. 2023, 24, 1989. [Google Scholar] [CrossRef] [PubMed]
- Bryk, M.; Chwastek, J.; Kostrzewa, M.; Mlost, J.; Pędracka, A.; Starowicz, K. Alterations in Anandamide Synthesis and Degradation during Osteoarthritis Progression in an Animal Model. Int. J. Mol. Sci. 2020, 21, 7381. [Google Scholar] [CrossRef] [PubMed]
- Yagin, N.L.; Aliasgharzadeh, S.; Alizadeh, M.; Aliasgari, F.; Mahdavi, R. The association of circulating endocannabinoids with appetite regulatory substances in obese women. Obes. Res. Clin. Pr. 2020, 14, 321–325. [Google Scholar] [CrossRef]
- Bowen, D., Ramesh, S., Deruiter, J., Govindarajulu, M., Lowery, P., Moore, T., Agrawal, D.C. and Dhanasekaran, M., 2022. Neuropharmacological Approaches to Modulate Cannabinoid Neurotransmission. In Cannabis/Marijuana for Healthcare (pp. 35-52). Singapore: Springer Nature Singapore.
- Silveira, K.M.; Wegener, G.; Joca, S.R.L. Targeting 2-arachidonoylglycerol signalling in the neurobiology and treatment of depression. Basic Clin. Pharmacol. Toxicol. 2021, 129, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, U., Pelzer, M., Kleine, J., Hohmann, T., Ghadban, C. and Dehghani, F., 2019. Opposite effects of neuroprotective cannabinoids, palmitoylethanolamide, and 2-arachidonoylglycerol on function and morphology of microglia. Frontiers in Neuroscience, 13, p.1180.
- Agrawal, I.; Lim, Y.S.; Ng, S.-Y.; Ling, S.-C. Deciphering lipid dysregulation in ALS: From mechanisms to translational medicine. Transl. Neurodegener. 2022, 11, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Kokona, D., Spyridakos, D., Tzatzarakis, M., Papadogkonaki, S., Filidou, E., Arvanitidis, K.I., Kolios, G., Lamani, M., Makriyannis, A., Malamas, M.S. and Thermos, K., 2021. The endocannabinoid 2-arachidonoylglycerol and dual ABHD6/MAGL enzyme inhibitors display neuroprotective and anti-inflammatory actions in the in vivo retinal model of AMPA excitotoxicity. Neuropharmacology, 185, p.108450.
- Pete, D.D. and Narouze, S.N., 2021. Endocannabinoids: Anandamide and 2-arachidonoylglycerol (2-AG). In Cannabinoids and Pain (pp. 63-69). Cham: Springer International Publishing.
- Maia, J.; Fonseca, B.M.; Cunha, S.C.; Braga, J.; Gonçalves, D.; Teixeira, N.; Correia-Da-Silva, G. Impact of tetrahydrocannabinol on the endocannabinoid 2-arachidonoylglycerol metabolism: ABHD6 and ABHD12 as novel players in human placenta. Biochim. et Biophys. Acta (BBA) - Mol. Cell Biol. Lipids 2020, 1865, 158807. [Google Scholar] [CrossRef] [PubMed]
- Simard, M.; Rakotoarivelo, V.; Di Marzo, V.; Flamand, N. Expression and Functions of the CB2 Receptor in Human Leukocytes. Front. Pharmacol. 2022, 13, 826400. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, O.; Ganguly, D. Endocannabinoids in immune regulation and immunopathologies. Immunology 2021, 164, 242–252. [Google Scholar] [CrossRef]
- Sharma, D.S.; Paddibhatla, I.; Raghuwanshi, S.; Malleswarapu, M.; Sangeeth, A.; Kovuru, N.; Dahariya, S.; Gautam, D.K.; Pallepati, A.; Gutti, R.K. Endocannabinoid system: Role in blood cell development, neuroimmune interactions and associated disorders. J. Neuroimmunol. 2021, 353, 577501. [Google Scholar] [CrossRef] [PubMed]
- Cuddihey, H.; MacNaughton, W.K.; Sharkey, K.A. Role of the Endocannabinoid System in the Regulation of Intestinal Homeostasis. Cell. Mol. Gastroenterol. Hepatol. 2022, 14, 947–963. [Google Scholar] [CrossRef] [PubMed]
- Terral, G.; Marsicano, G.; Grandes, P.; Soria-Gómez, E. Cannabinoid Control of Olfactory Processes: The Where Matters. Genes 2020, 11, 431. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Moncada, I.; Rodrigues, R.S.; Fundazuri, U.B.; Bellocchio, L.; Marsicano, G. Type-1 cannabinoid receptors and their ever-expanding roles in brain energy processes. J. Neurochem. 2023. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.T.; Mackie, K.; Chiou, L. Alternative pain management via endocannabinoids in the time of the opioid epidemic: Peripheral neuromodulation and pharmacological interventions. Br. J. Pharmacol. 2022, 180, 894–909. [Google Scholar] [CrossRef]
- Andrade, A.K., Renda, B. and Murray, J.E., 2019. Cannabinoids, interoception, and anxiety. Pharmacology Biochemistry and Behavior, 180, pp.60-73.
- Sideli, L.; Quigley, H.; La Cascia, C.; Murray, R.M. Cannabis Use and the Risk for Psychosis and Affective Disorders. J. Dual Diagn. 2019, 16, 22–42. [Google Scholar] [CrossRef] [PubMed]
- Niloy, N.; Hediyal, T.A.; Vichitra, C.; Sonali, S.; Chidambaram, S.B.; Gorantla, V.R.; Mahalakshmi, A.M. Effect of Cannabis on Memory Consolidation, Learning and Retrieval and Its Current Legal Status in India: A Review. Biomolecules 2023, 13, 162. [Google Scholar] [CrossRef] [PubMed]
- Schurman, L.D., Lu, D., Kendall, D.A., Howlett, A.C. and Lichtman, A.H., 2020. Molecular mechanism and cannabinoid pharmacology. Substance Use Disorders: From Etiology to Treatment, pp.323-353.
- O’Sullivan, S.E., Yates, A.S. and Porter, R.K., 2021. The peripheral cannabinoid receptor type 1 (CB1) is a molecular target for modulating body weight in men. Molecules, 26(20), p.6178.
- Hurel, I., Muguruza, C., Redon, B., Marsicano, G. and Chaouloff, F., 2021. Cannabis and exercise: Effects of Δ9-tetrahydrocannabinol on mice’s preference and motivation for wheel-running. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 105, p.110117.
- Zhornitsky, S.; Pelletier, J.; Assaf, R.; Giroux, S.; Li, C.-S.R.; Potvin, S. Acute effects of partial CB1 receptor agonists on cognition – A meta-analysis of human studies. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2020, 104, 110063. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M. The Impact of CB1 Receptor on Inflammation in Skeletal Muscle Cells. J. Inflamm. Res. 2021, 14, 3959–3967. [Google Scholar] [CrossRef] [PubMed]
- Guillamat-Prats, R.; Rami, M.; Herzig, S.; Steffens, S. Endocannabinoid Signalling in Atherosclerosis and Related Metabolic Complications. Arthritis Res. Ther. 2019, 119, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Rehman, S.U.; Shahmohamadnejad, S.; Zia, M.A.; Ahmad, M.; Saeed, M.M.; Akram, Z.; Iqbal, H.M.N.; Liu, Q. Therapeutic Attributes of Endocannabinoid System against Neuro-Inflammatory Autoimmune Disorders. Molecules 2021, 26, 3389. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Poe, A.R.; Wiese, B.; Kibaly, C.; Lueptow, L.; Garcia, J.; Anand, P.; Cahill, C.; Moron, J.A. Effects of inflammatory pain on CB1 receptor in the midbrain periaqueductal gray. PAIN Rep. 2021, 6, e897. [Google Scholar] [CrossRef]
- Anthony, A.T.; Rahmat, S.; Sangle, P.; Sandhu, O.; Khan, S. Cannabinoid Receptors and Their Relationship With Chronic Pain: A Narrative Review. Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.Y.; Cha, H.J.; Min, H.K.; Yun, J. Pharmacology and adverse effects of new psychoactive substances: Synthetic cannabinoid receptor agonists. Arch. Pharmacal Res. 2021, 44, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Thapa, D.; Cairns, E.A.; Szczesniak, A.-M.; Kulkarni, P.M.; Straiker, A.J.; Thakur, G.A.; Kelly, M.E.M. Allosteric Cannabinoid Receptor 1 (CB1) Ligands Reduce Ocular Pain and Inflammation. Molecules 2020, 25, 417. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, E. The Role of the Cannabinoid System in Opioid Analgesia and Tolerance. Mini-Reviews Med. Chem. 2020, 20, 875–885. [Google Scholar] [CrossRef] [PubMed]
- Hua, T., Li, X., Wu, L., Iliopoulos-Tsoutsouvas, C., Wang, Y., Wu, M., Shen, L., Brust, C.A., Nikas, S.P., Song, F. and Song, X., 2020. Activation and signaling mechanism revealed by cannabinoid receptor-Gi complex structures. Cell, 180(4), pp.655-665.
- Kędziora, M.; Boccella, S.; Marabese, I.; Mlost, J.; Infantino, R.; Maione, S.; Starowicz, K. Inhibition of anandamide breakdown reduces pain and restores LTP and monoamine levels in the rat hippocampus via the CB1 receptor following osteoarthritis. Neuropharmacology 2023, 222, 109304. [Google Scholar] [CrossRef] [PubMed]
- Mielnik, C.A.; Lam, V.M.; Ross, R.A. CB1 allosteric modulators and their therapeutic potential in CNS disorders. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2020, 106, 110163. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, J.M.; Cservenka, A. Emotion Dysregulation Moderates the Association Between Stress and Problematic Cannabis Use. Front. Psychiatry 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Tarragon, E. and Moreno, J.J., 2019. Cannabinoids, chemical senses, and regulation of feeding behavior. Chemical senses, 44(2), pp.73-89.
- Ibrahim, N.A.M., Mansour, Y.S.E. and Sulieman, A.A., 2019. Antiemetic medications: Agents, current research, and future directions. International Journal of Pharmacy and Pharmaceutical Sciences, pp.7-14.
- Landucci, E.; Berlinguer-Palmini, R.; Baccini, G.; Boscia, F.; Gerace, E.; Mannaioni, G.; Pellegrini-Giampietro, D.E. The Neuroprotective Effects of mGlu1 Receptor Antagonists Are Mediated by an Enhancement of GABAergic Synaptic Transmission via a Presynaptic CB1 Receptor Mechanism. Cells 2022, 11, 3015. [Google Scholar] [CrossRef] [PubMed]
- Lindner, T.; Schmidl, D.; Peschorn, L.; Pai, V.; Popa-Cherecheanu, A.; Chua, J.; Schmetterer, L.; Garhöfer, G. Therapeutic Potential of Cannabinoids in Glaucoma. Pharmaceuticals 2023, 16, 1149. [Google Scholar] [CrossRef] [PubMed]
- Navarrete, F.; García-Gutiérrez, M.S.; Gasparyan, A.; Navarro, D.; López-Picón, F.; Morcuende, Á.; Femenía, T.; Manzanares, J. Biomarkers of the Endocannabinoid System in Substance Use Disorders. Biomolecules 2022, 12, 396. [Google Scholar] [CrossRef]
- Rakotoarivelo, V.; Sihag, J.; Flamand, N. Role of the Endocannabinoid System in the Adipose Tissue with Focus on Energy Metabolism. Cells 2021, 10, 1279. [Google Scholar] [CrossRef] [PubMed]
- Marsicano, G. and Kuner, R., 2008. Anatomical distribution of receptors, ligands, and enzymes in the brain and the spinal cord: Circuitries and neurochemistry. In Cannabinoids and the Brain (pp. 161-201). Boston, MA: Springer US.
- Zhang, J.; Hoffert, C.; Vu, H.K.; Groblewski, T.; Ahmad, S.; O’Donnell, D. Induction of CB2 receptor expression in the rat spinal cord of neuropathic but not inflammatory chronic pain models. Eur. J. Neurosci. 2003, 17, 2750–2754. [Google Scholar] [CrossRef] [PubMed]
- Onaivi, E.S.; Ishiguro, H.; Gong, J.P.; Patel, S.; Perchuk, A.; Meozzi, P.A.; Myers, L.; Mora, Z.; Tagliaferro, P.; Gardner, E.; et al. Discovery of the Presence and Functional Expression of Cannabinoid CB2 Receptors in Brain. Ann. N. Y. Acad. Sci. 2006, 1074, 514–536. [Google Scholar] [CrossRef]
- Sugiura, T.; Kishimoto, S.; Oka, S.; Gokoh, M. Biochemistry, pharmacology and physiology of 2-arachidonoylglycerol, an endogenous cannabinoid receptor ligand. Prog. Lipid Res. 2006, 45, 405–446. [Google Scholar] [CrossRef] [PubMed]
- Pascual, A.C.; Gaveglio, V.L.; Giusto, N.M.; Pasquaré, S.J. Cannabinoid receptor-dependent metabolism of 2-arachidonoylglycerol during aging. Exp. Gerontol. 2014, 55, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Toguri, J.T., Lehmann, C., Laprairie, R.B., Szczesniak, A.M., Zhou, J., Denovan-Wright, E.M. and Kelly, M.E.M., 2014. Anti-inflammatory effects of cannabinoid CB2 receptor activation in endotoxin-induced uveitis. British Journal of Pharmacology, 171(6), pp.1448-1461.
- Capozzi, A.; Caissutti, D.; Mattei, V.; Gado, F.; Martellucci, S.; Longo, A.; Recalchi, S.; Manganelli, V.; Riitano, G.; Garofalo, T.; et al. Anti-Inflammatory Activity of a CB2 Selective Cannabinoid Receptor Agonist: Signaling and Cytokines Release in Blood Mononuclear Cells. Molecules 2021, 27, 64. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, C.; Blanchet, M.-R.; LaViolette, M.; Flamand, N. The CB2 receptor and its role as a regulator of inflammation. Cell. Mol. life Sci. 2016, 73, 4449–4470. [Google Scholar] [CrossRef] [PubMed]
- Benito, C.; Tolón, R.M.; Pazos, M.R.; Núñez, E.; I Castillo, A.; Romero, J. Cannabinoid CB2 receptors in human brain inflammation. Br. J. Pharmacol. 2008, 153, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J.C.; Glass, M. The Cannabinoid CB2 Receptor as a Target for Inflammation-Dependent Neurodegeneration. Curr. Neuropharmacol. 2007, 5, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Park, Y. and Watkins, B.A., 2021. Endocannabinoids and aging—inflammation, neuroplasticity, mood and pain. In Vitamins and Hormones (Vol. 115, pp. 129-172). Academic Press.
- Cravatt, B.F.; Demarest, K.; Patricelli, M.P.; Bracey, M.H.; Giang, D.K.; Martin, B.R.; Lichtman, A.H. Supersensitivity to anandamide and enhanced endogenous cannabinoid signaling in mice lacking fatty acid amide hydrolase. Proc. Natl. Acad. Sci. 2001, 98, 9371–9376. [Google Scholar] [CrossRef] [PubMed]
- Blesching, U., 2020. Your Cannabis CBD: THC Ratio: A Guide to Precision Dosing for Health and Wellness. Ed Rosenthal.
- Aziz, A.-I.; Nguyen, L.C.; Oumeslakht, L.; Bensussan, A.; Ben Mkaddem, S. Cannabinoids as Immune System Modulators: Cannabidiol Potential Therapeutic Approaches and Limitations. Cannabis Cannabinoid Res. 2022, 8, 254–269. [Google Scholar] [CrossRef]
- Gildea, L., Ayariga, J.A., Ajayi, O.S., Xu, J., Villafane, R. and Samuel-Foo, M., 2022. Cannabis sativa CBD extract shows promising antibacterial activity against Salmonella Typhimurium and S. newington. Molecules, 27(9), p.2669.
- Hashiesh, H.M.; Sharma, C.; Goyal, S.N.; Jha, N.K.; Ojha, S. Pharmacological Properties, Therapeutic Potential and Molecular Mechanisms of JWH133, a CB2 Receptor-Selective Agonist. Front. Pharmacol. 2021, 12, 702675. [Google Scholar] [CrossRef] [PubMed]
- Docagne, F.; Mestre, L.; Loría, F.; Hernangómez, M.; Correa, F.; Guaza, C. Therapeutic potential of CB2 targeting in multiple sclerosis. Expert Opin. Ther. Targets 2008, 12, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.P., 2014. Cannabinoids in pain management: CB1, CB2 and non-classic receptor ligands. Expert opinion on investigational drugs, 23(8), pp.1123-1140.
- Guindon, J.; Hohmann, A.G. Cannabinoid CB2 receptors: a therapeutic target for the treatment of inflammatory and neuropathic pain. Br. J. Pharmacol. 2008, 153, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Desroches, J.; Beaulieu, P. Opioids and Cannabinoids Interactions: Involvement in Pain Management. Curr. Drug Targets 2010, 11, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Docagne, F.; Muñetón, V.; Clemente, D.; Ali, C.; Loría, F.; Correa, F.; Hernangómez, M.; Mestre, L.; Vivien, D.; Guaza, C. Excitotoxicity in a chronic model of multiple sclerosis: Neuroprotective effects of cannabinoids through CB1 and CB2 receptor activation. Mol. Cell. Neurosci. 2007, 34, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Morcuende, A.; García-Gutiérrez, M.S.; Tambaro, S.; Nieto, E.; Manzanares, J.; Femenia, T. Immunomodulatory Role of CB2 Receptors in Emotional and Cognitive Disorders. Front. Psychiatry 2022, 13, 866052. [Google Scholar] [CrossRef]
- Hill, M.N. and Gorzalka, B.B., 2009. The endocannabinoid system and the treatment of mood and anxiety disorders. CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders), 8(6), pp.451-458.
- Preet, A., Qamri, Z., Nasser, M.W., Prasad, A., Shilo, K., Zou, X., Groopman, J.E. and Ganju, R.K., 2011. Cannabinoid receptors, CB1 and CB2, are novel targets for inhibiting non–small cell lung cancer growth and metastasis. Cancer prevention research, 4(1), pp.65-75.
- Nasser, M.W.; Qamri, Z.; Deol, Y.S.; Smith, D.; Shilo, K.; Zou, X.; Ganju, R.K. Crosstalk between Chemokine Receptor CXCR4 and Cannabinoid Receptor CB2 in Modulating Breast Cancer Growth and Invasion. PLoS ONE 2011, 6, e23901. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V., Piscitelli, F. and Mechoulam, R., 2011. Cannabinoids and endocannabinoids in metabolic disorders with a focus on diabetes. Diabetes-Perspectives in Drug Therapy, pp.75-104.
- Scheen, A.J.; Paquot, N. Use of cannabinoid CB1 receptor antagonists for the treatment of metabolic disorders. Best Pr. Res. Clin. Endocrinol. Metab. 2009, 23, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Steffens, S.; Pacher, P. Targeting cannabinoid receptor CB2 in cardiovascular disorders: Promises and controversies. Br. J. Pharmacol. 2012, 167, 313–323. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, S.E., 2015. Endocannabinoids and the cardiovascular system in health and disease. Endocannabinoids, pp.393-422.
- Elmes, S.J.; Winyard, L.A.; Medhurst, S.J.; Clayton, N.M.; Wilson, A.W.; Kendall, D.A.; Chapman, V. Activation of CB1 and CB2 receptors attenuates the induction and maintenance of inflammatory pain in the rat. Pain 2005, 118, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Ikegami, M.; Kai, M.; Ohsawa, M.; Kamei, J. Activation of spinal cannabinoid CB2 receptors inhibits neuropathic pain in streptozotocin-induced diabetic mice. Neuroscience 2013, 250, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Vera, G.; López-Miranda, V.; Herradón, E.; Martín, M.I.; Abalo, R. Characterization of cannabinoid-induced relief of neuropathic pain in rat models of type 1 and type 2 diabetes. Pharmacol. Biochem. Behav. 2012, 102, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Toth, C.C.; Jedrzejewski, N.M.; Ellis, C.L.; Frey, W.H. Cannabinoid-Mediated Modulation of Neuropathic Pain and Microglial Accumulation in a Model of Murine Type I Diabetic Peripheral Neuropathic Pain. Mol. Pain 2010, 6, 16. [Google Scholar] [CrossRef]
- Zhang, F.; Challapalli, S.C.; Smith, P.J. Cannabinoid CB1 receptor activation stimulates neurite outgrowth and inhibits capsaicin-induced Ca2+ influx in an in vitro model of diabetic neuropathy. Neuropharmacology 2009, 57, 88–96. [Google Scholar] [CrossRef]
- Lin, X.; Xu, Z.; Carey, L.; Romero, J.; Makriyannis, A.; Hillard, C.J.; Ruggiero, E.; Dockum, M.; Houk, G.; Mackie, K.; et al. A peripheral CB2 cannabinoid receptor mechanism suppresses chemotherapy-induced peripheral neuropathy: Evidence from a CB2 reporter mouse. Pain 2021, 163, 834–851. [Google Scholar] [CrossRef] [PubMed]
- Cavaletti, G., Alberti, P., Frigeni, B., Piatti, M. and Susani, E., 2011. Chemotherapy-induced neuropathy. Current treatment options in neurology, 13, pp.180-190.
- Maldonado, R.; Baños, J.E.; Cabañero, D. The endocannabinoid system and neuropathic pain. Pain 2016, 157, S23–S32. [Google Scholar] [CrossRef] [PubMed]
- Svíženská, I., Dubový, P. and Šulcová, A., 2008. Cannabinoid receptors 1 and 2 (CB1 and CB2), their distribution, ligands and functional involvement in nervous system structures—a short review. Pharmacology Biochemistry and Behavior, 90(4), pp.501-511.
- Benito, C.; Romero, J.P.; Tolón, R.M.; Clemente, D.; Docagne, F.; Hillard, C.J.; Guaza, C.; Romero, J. Cannabinoid CB1and CB2Receptors and Fatty Acid Amide Hydrolase Are Specific Markers of Plaque Cell Subtypes in Human Multiple Sclerosis. J. Neurosci. 2007, 27, 2396–2402. [Google Scholar] [CrossRef] [PubMed]
- Aly, E.; Masocha, W. Targeting the endocannabinoid system for management of HIV-associated neuropathic pain: A systematic review. IBRO Neurosci. Rep. 2021, 10, 109–118. [Google Scholar] [CrossRef]
- Eibach, L., Scheffel, S., Cardebring, M., Lettau, M., Özgür Celik, M., Morguet, A., Roehle, R. and Stein, C., 2021. Cannabidivarin for HIV-associated neuropathic pain: a randomized, blinded, controlled clinical trial. Clinical Pharmacology & Therapeutics, 109(4), pp.1055-1062.
- Munawar, N.; Oriowo, M.A.; Masocha, W. Antihyperalgesic Activities of Endocannabinoids in a Mouse Model of Antiretroviral-Induced Neuropathic Pain. Front. Pharmacol. 2017, 8, 136. [Google Scholar] [CrossRef] [PubMed]
- Rahn, E.J.; Zvonok, A.M.; Thakur, G.A.; Khanolkar, A.D.; Makriyannis, A.; Hohmann, A.G. Selective Activation of Cannabinoid CB2 Receptors Suppresses Neuropathic Nociception Induced by Treatment with the Chemotherapeutic Agent Paclitaxel in Rats. J. Pharmacol. Exp. Ther. 2008, 327, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Mulpuri, Y.; Marty, V.N.; Munier, J.J.; Mackie, K.; Schmidt, B.L.; Seltzman, H.H.; Spigelman, I. Synthetic peripherally-restricted cannabinoid suppresses chemotherapy-induced peripheral neuropathy pain symptoms by CB1 receptor activation. Neuropharmacology 2018, 139, 85–97. [Google Scholar] [CrossRef]
- A Galli, J., Andari Sawaya, R. and K Friedenberg, F., 2011. Cannabinoid hyperemesis syndrome. Current drug abuse reviews, 4(4), pp.241-249.
- Wallace, E.A., Andrews, S.E., Garmany, C.L. and Jelley, M.J., 2011. Cannabinoid hyperemesis syndrome: Literature review and proposed diagnosis and treatment algorithm. South Med J, 104(9), pp.659-664.
- Sorensen, C.J.; DeSanto, K.; Borgelt, L.; Phillips, K.T.; Monte, A.A. Cannabinoid Hyperemesis Syndrome: Diagnosis, Pathophysiology, and Treatment—a Systematic Review. J. Med Toxicol. 2016, 13, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.R.; Gordon, B.K.; Danielson, A.R.; Moulin, A.K. Pharmacologic Treatment of Cannabinoid Hyperemesis Syndrome: A Systematic Review. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, S.E.; Denysenko, L.; Mulcare, J.L.; Vito, J.P.; Chabon, B. Cannabinoid Hyperemesis Syndrome: A Case Series and Review of Previous Reports. Psychosomatics 2012, 53, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Lapoint, J.; Meyer, S.; Yu, C.K.; Koenig, K.L.; Lev, R.; Thihalolipavan, S.; Staats, K.; Kahn, C.A. Cannabinoid Hyperemesis Syndrome: Public Health Implications and a Novel Model Treatment Guideline. WestJEM 21.2 March Issue 2018, 19, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.B.; Spooner, C.; May, L.; Leslie, R.; Whiteley, V.L. Cannabinoid Hyperemesis Syndrome Survey and Genomic Investigation. Cannabis Cannabinoid Res. 2022, 7, 336–344. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cartoon depiction of 2-AG interactions at the synapses. 2-arachidonyl glycerol (2-AG); cannabinoid receptor 1 (CB1); diacylglycerol (DAG); diacylglycerol lipase (DAGL); mitogen- activated protein kinase (MAPK), adenyl cyclase (AC).
Figure 1.
Cartoon depiction of 2-AG interactions at the synapses. 2-arachidonyl glycerol (2-AG); cannabinoid receptor 1 (CB1); diacylglycerol (DAG); diacylglycerol lipase (DAGL); mitogen- activated protein kinase (MAPK), adenyl cyclase (AC).
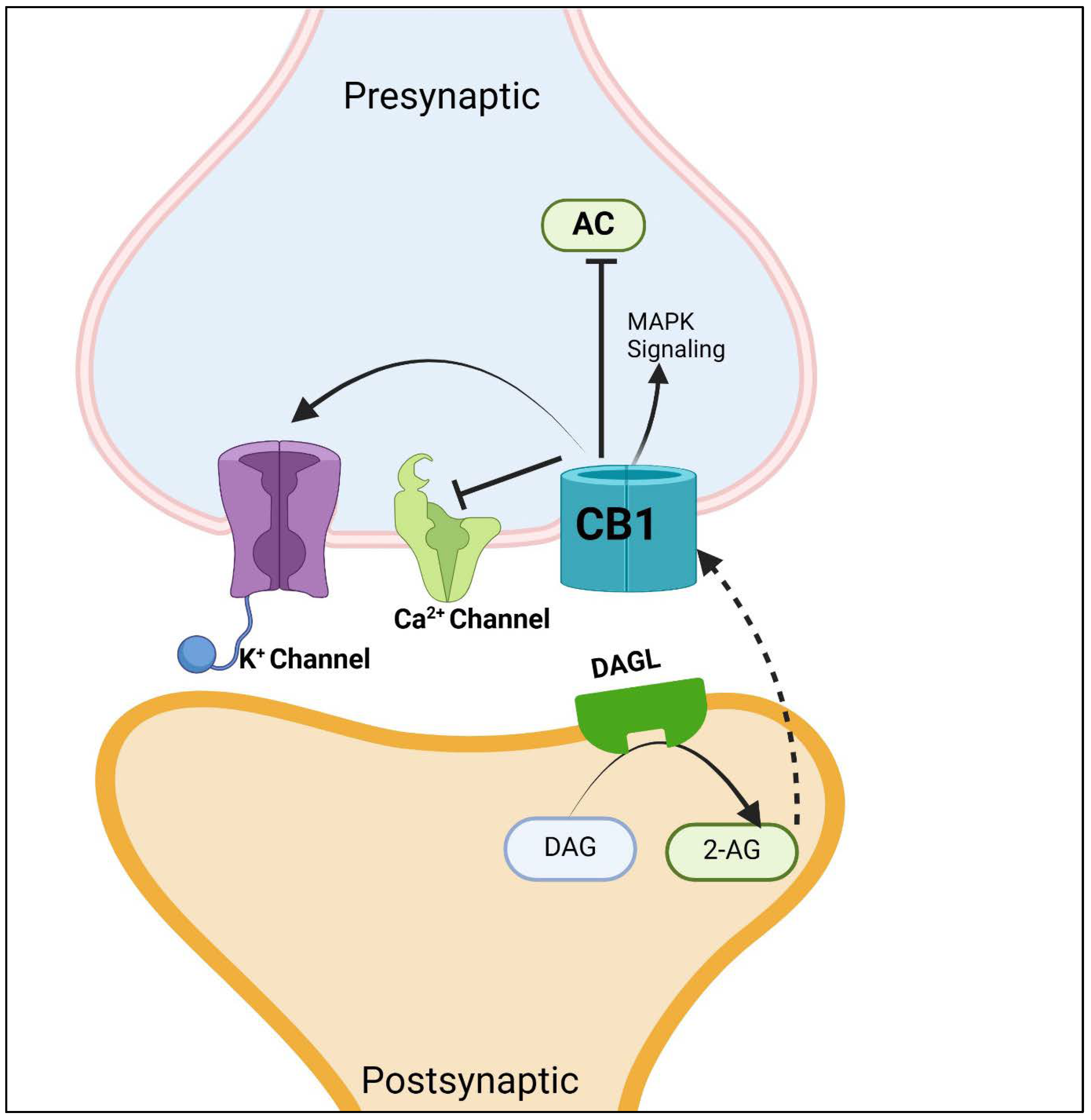

Table 1.
Chemical properties of endocannabinoids/phytocannabinoids.
| Endocannabinoids/Phytocannabinoids | Structure | Molecular Formula | Molecular weight |
|---|---|---|---|
| Anandamide amidohydrolase (AEA) | 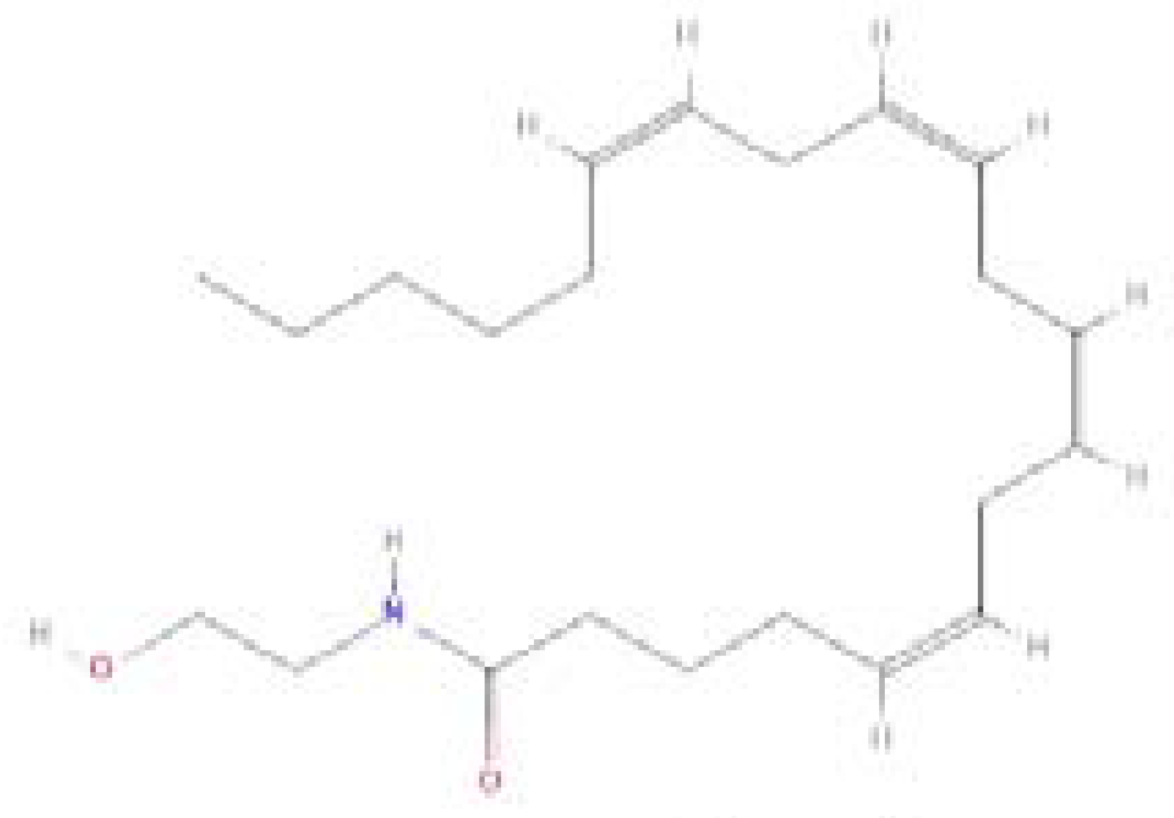 |
C22H37NO2 | 347.5 g/mol |
| 2-Arachidonoylglycerol (2-AG) | 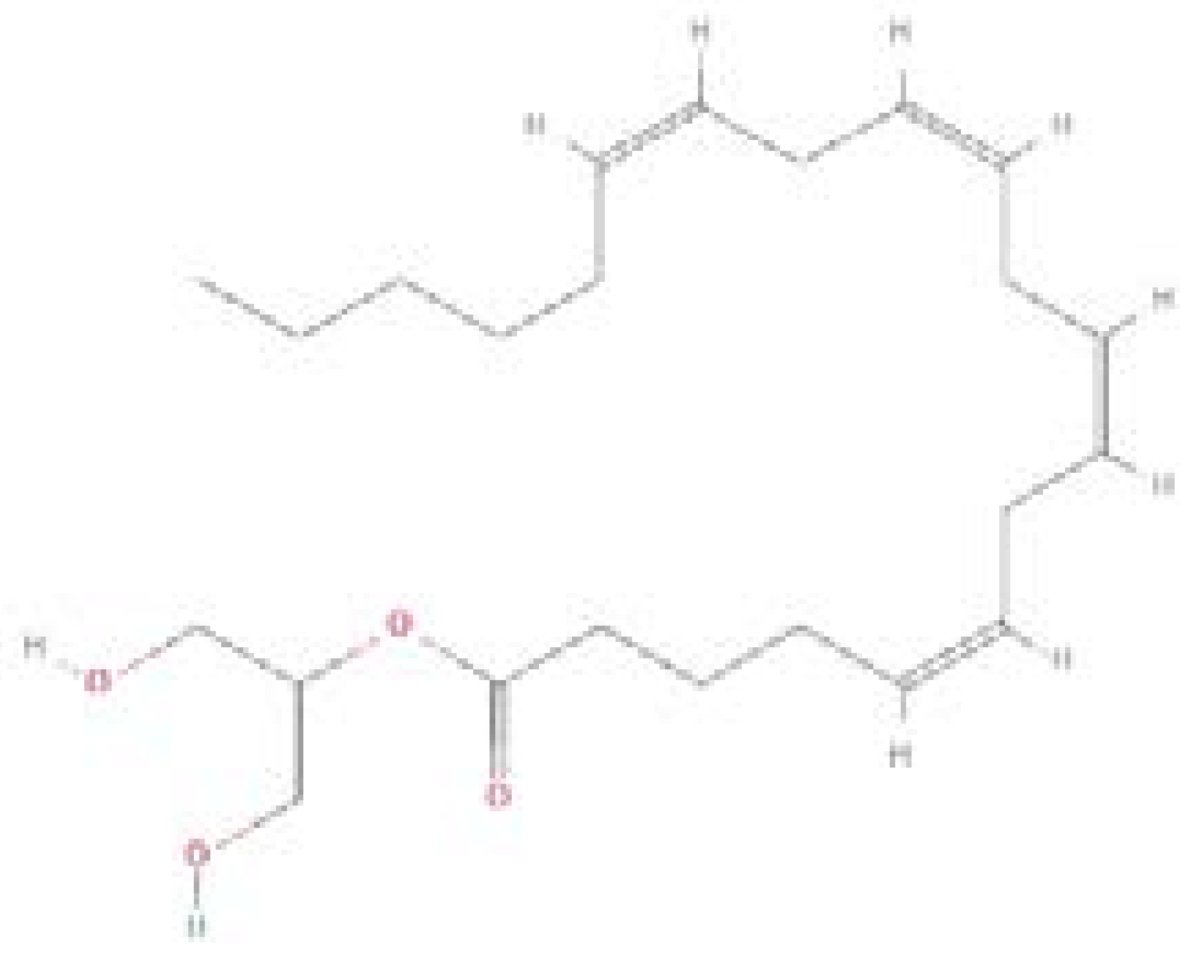 |
C23H38O4 | 378.5 g/mol |
| Cannabinoid (CBD) | 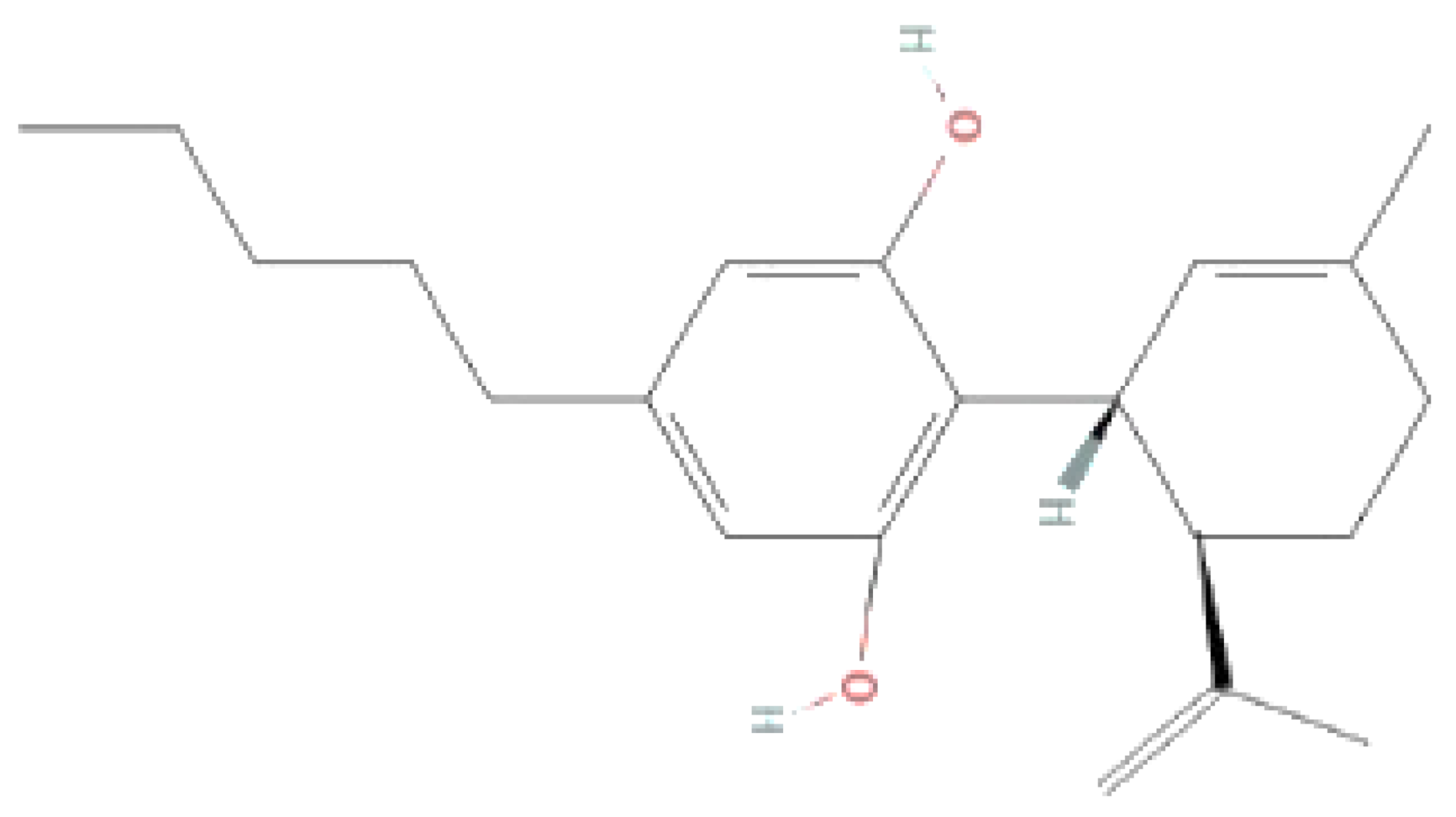 |
C21H30O2 | 314.5 g/mol |
| Delta-9 tetrahydrocannabinol (THC) |  |
C21H30O2 | 314.5 g/mol |
Structures obtained from PubChem.
Table 2.
Therapeutic Potential of CB2 and CB1 Modulation with specific examples.
| Therapeutic Potential | Description | Specific Examples | Reference |
|---|---|---|---|
| Pain Management (CB2) | CB2 modulation shows promise in alleviating various types of pain, particularly neuropathic pain, inflammatory pain, and chronic pain conditions. It may offer an alternative or adjunct to traditional analgesics, with potentially fewer side effects. | - Neuropathic pain relief#break#- Alleviation of inflammatory pain#break#-Management of chronic pain conditions | [115,116] |
| Inflammation (CB2) | CB2 receptors play a crucial role in regulating immune responses and inflammation. Modulating CB2 activity has been investigated for its therapeutic effects in inflammatory diseases such as arthritis, inflammatory bowel disease (IBD), and neuroinflammatory conditions. | - Reduction of arthritis symptoms#break#- Management of inflammatory bowel disease#break#- Attenuation of neuroinflammation | [110,111,113] |
| Neuroprotection (CB2) | Activation of CB2 receptors has been linked to neuroprotection in various neurodegenerative diseases, including Alzheimer’s disease, Parkinson’s disease, and multiple sclerosis. CB2 modulation may help reduce neuroinflammation, oxidative stress, and neuronal damage, thereby slowing disease progression and preserving cognitive function. | - Protection against neuronal damage in Alzheimer’s disease #break#- Attenuation of neuroinflammation in Parkinson’s disease#break#- Preservation of cognitive function in multiple sclerosis | [117,118] |
| Mood Disorders (CB2) | CB2 modulation has shown potential in regulating mood and emotional responses, suggesting a role in the treatment of mood disorders such as anxiety, depression, and post-traumatic stress disorder (PTSD). Emerging research indicates that CB2 activation may exert anxiolytic and antidepressant effects through modulation of neurotransmitter systems and neuroinflammatory pathways. | - Reduction of anxiety symptoms#break#- Alleviation of depressive symptoms#break#- Improvement in PTSD symptoms | [119,120] |
| Cancer (CB2) | CB2 receptors are overexpressed in certain cancer types, and their modulation has been explored for anticancer effects. Preclinical studies suggest that CB2 activation inhibits tumor growth, metastasis, and angiogenesis, while inducing apoptosis in cancer cells. CB2 agonists may also enhance the efficacy of chemotherapy and radiation therapy, offering potential synergistic effects in cancer treatment. | - Inhibition of tumor growth and metastasis#break#- Induction of cancer cell apoptosis#break#- Enhancement of chemotherapy efficacy | [121,122] |
| Metabolic Disorders (CB2) | CB2 activation has been implicated in regulating metabolic processes such as appetite, energy balance, and glucose metabolism. Modulating CB2 activity may hold therapeutic potential in metabolic disorders like obesity, type 2 diabetes, and metabolic syndrome. CB2 agonists have been shown to reduce food intake, body weight, and adiposity, as well as improve insulin sensitivity and lipid profiles in preclinical models. | - Reduction of food intake and body weight#break#- Improvement of insulin sensitivity#break#- Regulation of lipid metabolism | [123,124] |
| Cardiovascular Health (CB2) | Modulation of CB2 receptors may have protective effects on the cardiovascular system. CB2 activation has been associated with reduced inflammation, oxidative stress, endothelial dysfunction, and atherosclerotic plaque formation, suggesting potential therapeutic benefits for cardiovascular diseases such as atherosclerosis, hypertension, and myocardial infarction. | - Reduction of inflammation and oxidative stress in atherosclerosis#break#- Improvement of endothelial function#break#- Prevention of atherosclerotic plaque formation | [125,126] |
| Pain Management (CB1) | CB1 receptors are involved in the modulation of pain perception, particularly in the central nervous system. Activation of CB1 receptors can suppress pain signaling pathways, offering potential therapeutic benefits in the management of acute and chronic pain conditions. | - Suppression of pain signaling pathways in the CNS | [115,127] |
| Neuroprotection (CB1) | CB1 receptor activation has been associated with neuroprotective effects in various neurological conditions, including epilepsy, ischemic stroke, and traumatic brain injury. CB1 modulation may help mitigate neuronal damage, excitotoxicity, and neuroinflammation, thereby preserving neuronal integrity and function. | - Protection against neuronal damage in epilepsy#break#- Attenuation of neuroinflammation in stroke#break#- Preservation of neuronal function in traumatic brain injury | [120,121] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



