
Submitted:
22 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
The present study describes a comprehensive analysis of the Adverse Drug Reactions (ADRs) documented in the Database of the Spanish Pharmacovigilance System (FEDRA) concerning the use of biological medications used for severe refractory asthma, specifically omalizumab, mepolizumab, reslizumab, benralizumab, dupilumab, and tezepelumab. Emphasis was placed on ADRs not documented in the Technical Sheet (Summary of Product Characteristics, SmPC) of the respective specialties (Xolair®, Nucala®, Cinqaero®, Fasenra®, Dupixent®, and Tezspire®), which could potentially trigger a warning signal in Pharmacovigilance, indicating previously unidentified risks. The analysis encompassed data from the inception of each drug ́s marketing until January 22, 2024, including cases originating from various sources: direct submissions to the Spanish Pharmacovigilance System, communications from the Pharmaceutical Industry, and findings from literature review. Notifications were analyzed independently of their origin, so a complete review of all ADRs associated with these medications was ensured. In essence, this investigation highlights the critical role of post-marketing safety information, emphasizing the relevance of comprehensive reporting by healthcare professionals to facilitate a robust Pharmacovigilance system, ultimately advancing patient care and safety.
Keywords:
Severe asthma
; Biologic Therapy
; Safety
; Adverse event
; Pharmacovigilance.
1. Introduction
1.1. Background
Asthma, a significant non-transmissible respiratory condition affects 1–18% of the world population [1,2] and stands as the most prevalent chronic disease among children globally. Despite advancements in asthma management, 3.5% to 5% of individuals with asthma prove challenging to treat, leading to increased medication usage, frequent emergency department visits and hospitalizations, representing >50% of the direct total asthma cost [3,4,5]. Current guidelines indicate that subjects with the severe forms of the disease require treatment with high dose inhaled corticosteroids (ICSs) along with a second controller medication -and/or systemic corticosteroids- to prevent asthma from becoming uncontrolled or which remains uncontrolled despite strictly adhering to therapy [6]. This approach reflects a departure from the traditional model of asthma as a singular entity towards a more intricate biological network where severe asthma (SA) is categorized based on observable features resulting from complex interaction between hereditary, environmental, and behavioral influences. Moreover, the enhanced comprehension of SA immunopathogenesis has progressed to the characterization of distinct endotypes classified as either type 2 (T2) high or T2-low, according to the varying levels of expression of specific cytokines like IL-4, IL-5, and IL-13 [7]. Clinically, T2-high asthma has been categorized into three distinct phenotypes, comprising early-onset allergic asthma, late-onset eosinophilic asthma, and nonsteroidal anti-inflammatory drugs (NSAIDs)-exacerbated respiratory disease (NERD) [8,9,10,11,12]. In contrast T2 Low asthma, has been clinically grouped based on factors such as exposure to smoking, obesity and/or age, being immunologically distinguished by the activation of inflammatory pathways involving T helper-lymphocytes type 1 (Th1) and Th17 cells as well as cytokines like IL-6, IL-8, IL-17, and IL-22 along with epithelial derived cytokines [13,14,15,16]. Despite T2 inflammation being preponderant in SA, the assignment to a specific asthma phenotype may not remain consistent over time because there is often substantial overlap (>70%) observed among different asthma traits [17,18,19,20] . The advantage of classifying severe asthma, first discussed in 2008, lies in the possibility of targeting each endotype with specifically tailored therapy to address the underlying pathogenic molecular mechanisms [17,21].
1.2. Overview of Biological Agents for Asthma
In recent decades, the advent of biologics, defined by the European Medicines Agency (EMA) as a medicine whose active substance is made by a living organism [22], has revolutionized the management of SA particularly in those individuals with the T2 endotype [23,24,25]. This transformative shift has altered our expectations for SA, enabling exploration of the potential to alter the disease trajectory and even induce remission [26,27].
In Spain, the available biologics -formerly approved by the EMA- for severe uncontrolled asthma include 6 monoclonal antibodies, which are briefly described as follows:
- -
- Omalizumab (Xolair®) is a recombinant monoclonal antibody specifically designed to target free IgE, preventing its interaction with the high-affinity FcεRI receptors found on the surface of basophils and mast cells [28,29]. Omalizumab treatment should be considered only for patients 6 years of age and older with asthma convincingly mediated by IgE -i.e., a positive skin test or in vitro reactivity to a perennial aeroallergen- and whose symptoms are inadequately controlled with inhaled corticosteroids [30].
- -
- Mepolizumab (Nucala®) is a humanized IgG1 monoclonal antibody that directly binds to IL-5, preventing its interaction with the alpha-chain of the IL-5 receptor from eosinophils and basophils [31,32]. First authorized in Spain in 2015, and currently indicated as additional treatment for severe refractory eosinophilic asthma in patients 6 years of age and older [33].
- -
- Reslizumab (Cinqaero®), the second available anti-IL5 biological agent in 2016, is indicated as an additional treatment in adult patients with severe eosinophilic asthma inadequately controlled with high-dose inhaled corticosteroids plus another maintenance treatment medication [34]. Reslizumab is solely designated for hospital use due to its requirement for intravenous administration.
- -
- Benralizumab (Fasenra®) is a humanized and afucosylated monoclonal antibody that binds with high affinity and specificity to the alpha-subunit of the receptors for IL-5 specifically expressed on the surface of eosinophils and basophils [35]. Authorized in Spain in 2018, it serves as an additional treatment in adult patients with severe eosinophilic asthma who are not adequately controlled despite high-dose corticosteroid treatment and long-acting beta-2 agonists [36].
- -
- Tezepelumab (Tezspire®), a human monoclonal antibody produced in Chinese hamster ovary (CHO) cells using recombinant DNA technology that Blocks circulating thymic stromal lymphopoietin (TLSP) and prevents receptor binding. Authorized in Spain in 2022, tezepelumab is indicated as an additional maintenance treatment in adults and adolescents aged 12 years and older with severe asthma who are not adequately controlled despite high-dose inhaled corticosteroids in combination with another maintenance treatment [37].
- -
- Dupilumab (Dupixent®) is a recombinant monoclonal antibody that inhibits signaling of interleukin-4 (IL-4) and interleukin-13 (IL-13) which are involved in type-2 inflammation. Authorized in Spain in 2017, it is indicated as an additional maintenance treatment in adults and adolescents aged 12 years and older with severe asthma characterized by type-2 inflammation, evidenced by elevated blood eosinophils and/or elevated FeNO, who are not controlled with high-dose inhaled corticosteroids in combination with another maintenance treatment [38].
1.3. Post-Approval Pharmacovigilance of Biological Drug in Asthma
While these agents are deemed safe upon authorization by the EMA, it should be noted that the use of any drug can lead to an increase in frequency of reported adverse drug reactions (ADRs) and may reveal previously unknown risks, emphasizing the need for continued surveillance, especially given the lack of long-term safety data [39,40]. The Spanish System of Human Use Medicines Pharmacovigilance (SEFV-H, for its acronym in Spanish), the organization responsible for pharmacovigilance activities in Spain, gathers data of notifications (or reports) on suspected ADRs to medicines, registering all in a database named Farmacovigilancia Española, Datos de Reacciones Adversas (FEDRA, for its acronym in Spanish).This information leads to the generation of so called Signals, which represents an association between a drug and an ADR previously unknown but considered plausible based on quantitative and qualitative data, judged to have sufficient likelihood to warrant further verification action [41]. Pharmacovigilance Signals allow the generation of new hypotheses about medication safety post-marketing [42,43,44], underscoring the essential importance of healthcare professionals’ participation in spontaneous reporting programs for suspected ADRs.
1.4. Justification and Aim of the Study
The Allergy Department at Canary Islands University Hospital, Tenerife, Spain, identified three cases of severe arthralgia related to the use of mepolizumab and reported them to the Autonomous Pharmacovigilance Center (CAFV, for its acronym in Spanish). In February 2023, the Canary Islands CAFV presented a Signal titled "Mepolizumab and arthralgia" to the Technical Committee of SEFV-H, as this association was not reflected in the Nucala® Summary of Product Characteristics (SmPC), and arthralgia was considered as a new risk. This signal was communicated to the Pharmacovigilance Risk Assessment Committee (PRAC) of the EMA, prompting a request for all available information from the pharmaceutical laboratory that markets mepolizumab for evaluation in the next Periodic Safety Report (PSR).
Consequently, it was considered of interest to know the profile of notifications of suspected ADRs to biological medications specifically designated for SA. Thus, the objective of this study is to examine all reports of suspected ADRs related to any of the biological medications approved for SA in Spain, providing a complete summary of the most significant ADRs that are not currently included in their SmPC, and which, due to their severity, are likely to generate a pharmacovigilance signal.
2. Materials and Methods
2.1. Biological Medicines under Study
It is important to note that while this analysis encompasses all biological drugs used in the treatment of severe refractory asthma, the current selection of cases has solely focused on the medication used, disregarding the indication, thereby facilitating the investigation of the complete profile of reactions associated with its use (Table 1).
2.2. Data Source and Analysis of Cases Registered in the FEDRA Database
The Database of the Spanish Pharmacovigilance System (FEDRA) is a computerized database containing Individual Case Safety Reports (ICSRs) of suspected ADRs submitted by healthcare professionals, citizens, and Marketing Authorization Holders (MAH), also known as the pharmaceutical industry, and cases from Medical Literature Monitoring (MLM Service) conducted by the EMA. FEDRA encompasses notifications accumulated since 1983, containing only reports of ADRs detected post-drug authorization (n > 590.000). The primary goal of spontaneous reporting of suspected ADRs is to operate as a responsive and swift system for identifying potential adverse events that were not identified during the pre-commercialization clinical trials conducted with the drugs.
For an adequate understanding of the results, it is essential to consider that the same case may originate from multiple sources of information (i.e., patients, and or health professionals including Pharmacists, Primary or Specialty Care physicians, nurses, etc.). Additionally, each case often describes the use of several medications in the same patient, as well as several ADRs or symptoms resulting from the same ADR. Therefore, the number of cases is not equivalent to the number of ADRs, nor will the number of medications involved be equal to the number of reported cases.
In the evaluation of a pharmacovigilance signal, both quantitative and qualitative analysis are conducted, based solely on spontaneous reporting data. The statistical results should be interpreted as the "degree of imputability of the case series", indicating whether the association warrants further investigation. Subsequently, an epidemiological evaluation is performed, assessing factors such as the presence of a compatible temporal sequence, improvement of symptoms upon medication withdrawal, reasonable exclusion of alternative causes, and identification of confounding factors and biases. If a case exhibits positive re-exposure, the imputability of that signal would be further strengthened [44].
The quantitative analysis involves calculating the disproportionality of reporting, which assesses whether the frequency of the reporting of a particular association is significantly higher than expected. This comparison considers how often an association between an ADR and a drug is reported compared to the reporting of either the drug or the ADR alone, relative to the total number of cases in the database. This metric is known as the Reporting Odds Ratio (ROR). Similarly, the Information Component (IC) utilizes a logarithmic basis to compare the expected and reported cases, providing insight into the unexpectedness of the association while shrinking the confidence interval [42]. Additionally, the Chi-Square (X2) calculation offers supplementary information about the association between reported cases and drugs [45]. Despite a greater disproportionality of notification, it should be mentioned that this does not necessarily indicate a stronger association, as observed in epidemiological studies [43].
The SEFV-H has developed guidelines for the correct interpretation of data obtained from the FEDRA Database, which are briefly enumerated as follows [46]:
- Each notification of suspected ADRs does not establish certainty that the suspected drug caused the ADR; individual evaluation of each reported case is essential, considering factors like temporal sequence and positive re-exposure effect, among others, without leading to an unequivocal diagnostic judgment of causality.
- The accumulation of reported cases cannot be utilized to calculate incidence or estimate the risk of ADRS; instead, these data should be interpreted cautiously as notification rates, precluding comparisons of the safety of different drugs.
- The overall evaluation of reported cases of a drug-reaction association aims solely to identify potential signals of unknown risks within an epidemiological case history context.
2.3. Medical Dictionary for Regulatory Activities (MedDRA)
FEDRA utilizes the MedDRA terminological dictionary (Medical Dictionary for Regulatory Activities) for the coding of reported cases. This dictionary organizes reaction terms into a hierarchical structure consisting of five levels: the highest hierarchical level being the System Organ (SOC), encompassing 28 categories, while the lowest level comprises clinical symptoms known as Lowest Level Term (LLT), totaling 80,000. Preferred Terms (PT) sit one level above and initially analyzed. Higher than PT are High Level Term (HLT) and High-Level Group Term (HLGT), which categorize terms based on different clinical characteristics. It should be noted that a term may be included in multiple hierarchical groupings, known as a “multiaxial structure” (Figure 1).
Additionally, the dictionary provides Standardized MedDRA Queries (SMQ) for specific clinical and analytical purposes that can be expressly defined for specific scenarios. Therefore, the results of this study are presented not only based on MedDRA´s hierarchical structure but also on the combination of terms most relevant from a clinical perspective.
2.4. Institutional Review Board Statement
This article is derived from reviews of existing databases, guidelines, and literature, and does not involve any studies regarding human participants or animals. These data are anonymized data, and its use has been carried out in accordance with the procedures of the Spanish Pharmacovigilance System and the Guide for the use of FEDRA data by the Autonomic Centers of the SEFV-H [47].
3. Results
3.1. Global Findings from the Analysis of Overall Data
Suspected ADRs reported in FEDRA up to January 22, 2024, involving drugs categorized under ATC group RO3DX + D11AH05_dupilimab account for 2,280 cases, constituting 0.38% of the total FEDRA case pool. The origin of communication of the cases, which may come from multiple sources (SEFV-H, MAH and MLM Service), the majority are from the MAH.
Regarding the type of notifier, physicians account for most notifications, comprising 48%, originating both from the SEFV-H and the Pharmaceutical Industry. Secondly, 34% of the cases are notified by users themselves, primarily through the MAH. Since these are considered “only-hospital prescribed drugs”, most notifications from health professionals originate from such centers, both physicians and pharmacists. As expected, the distribution by age group and sex, most patients fell within the adult range (between 18 and 65 years old), with twice as many women as men.
In terms of seriousness of the reported ADRs, out of the total cases, 36% (n = 840) were regarded as serious by the notifier, health professional, or patient, primarily due to clinically relevant conditions (n = 669; 29%). Among these cases, 23 were fatal, 65 endangered the patient's life, 35 resulted in persistent disability, and 239 required hospital admission or prolonged it (Table 2).
When considering the evolution or clinical outcome of the reactions, a notable discrepancy was observed in the available information between notifications originating from MAH and those originating from SEFV-H (Table 3).
3.2. Active Ingredient
Table 4 displays the number of cases recorded in FEDRA for each active ingredient, along with the percentage of serious ADRs and warning cases. Additionally, the distribution of patients with ADRs by sex for each suspected drug is presented. It should be noted that the variation in the number of serious and warning cases among active ingredients shown in Table 4 does not indicate a superior or inferior safety profile; rather, it reflects differences in frequency reporting.
While these data do not directly derive from the present FEDRA case review, it was imperative to evaluate assess the safety data outlined in the SmPC for each drug. Hence, we conducted a comprehensive review of ADRs (Table 5), emphasizing that all ADRs documented in the SmPC have also been reported.
Moreover, Table 6 delineates additional ADRs that have been reported but are not documented in the SmPC, highlighting potential gaps in the current safety information.
3.2.1. Omalizumab
As per details provided in the Xolair® SmPC, the most frequent ADR associated with omalizumab (occurring in up to 1 patient in 10) include headache and reactions at the injection site, predominantly characterized by pain, swelling, redness and itching. In children aged between 6 and 12 years with allergic asthma, the occurrence of fever and upper abdominal pain was very common. Moreover, in patients with chronic urticaria, the most reported ADRs encompassed joint pain, sinusitis, and upper respiratory tract infections. Similar ADRs were noted in patients with chronic rhinosinusitis with nasal polyps, with upper abdominal pain, dizziness and joint pain being the predominant concerns in their safety profile.
Below are described the most relevant reported adverse reactions not currently included in the Xolair® SmPC:
- -
- Cutaneous Disorders were reported in 25% of cases in FEDRA: there are 166 cases (of 672) related to skin disorders. In addition to the ADRs described in SmPC, have been reported: atopic dermatitis, purpura, and hyperhidrosis.
- -
- In addition to headache, syncope, paresthesia, dizziness, and drowsiness, known in SmPC as ADRs of Nervous System, there were 122 cases registered with any of these in FEDRA, which represent 18% of those notified. It is worth highlighting vascular disorders of the central nervous system (Cerebrovascular accident, Transient ischemic attack, and Ischemic stroke); Tremor, Dyskinesias and movement disorders; and Seizure disorders.
- -
- Musculoskeletal and Connective Tissue Disorders are known for omalizumab (arthralgias, myalgia, swelling of the joints and systemic lupus erythematosus). In FEDRA the reactions that affect this SOC represent almost 16% n = 105. Back pain is the most reported ADR among those not described in SmPC, along with extremity pain, muscle weakness, muscle spasms, musculoskeletal stiffness, and discomfort in limbs.
- -
- Neoplastic Disorders: No formal carcinogenicity studies have been performed with omalizumab, nor are any benign or malignant adverse reactions described in the SmPC for Xolair®. However, in FEDRA there are 67 cases registered that link omalizumab with a neoplastic disorder, which represents 10% of its total cases. All these cases should be considered of interest and likely to generate a signal in pharmacovigilance. Malignant neoplasms of the breast are the most reported, although malignant neoplasms have also been reported in other locations: Colorectal neoplasms malignant; Lymphomas unspecified NEC; Respiratory tract and pleural neoplasms malignant cell type unspecified NEC.
- -
- The adverse reactions of the Immune System are known (local and systemic type I allergic reactions, anaphylaxis and anaphylactic shock, and appearance of antibodies against omalizumab). In FEDRA, it represented 9% (n = 59) of the total reported. Among those not included in SmPC, three cases of optic neuritis, three of multiple sclerosis and three cases of Sjögren's Syndrome stand out.
- -
- Complementary Explorations: The Xolair® SmPC does not contain a section on reactions linked to additional investigations, however the possibility of an increase in body weight as a consequence of treatment with omalizumab is described. In this series of cases, in FEDRA, there are 45 notifications that describe some disorder at the level of Complementary Examinations: the only term that could be of interest (n = 4) is decreased weight.
- -
- Infections or infestations are uncommon (pharyngitis) or rare (parasitic infections) according to SmPC. In FEDRA there are 43 cases of suspected ADRs to omalizumab related to the appearance of infections, which represent 6%. Herpes zoster virus infections may be of interest, as it is the most frequently reported infection.
- -
- Vascular Disorders described in SmPC with omalizumab are rare and limited to postural hypotension and flushing. But in FEDRA there are 34 cases that represent 5% of the total. Deep vein thrombosis was the most reported term not in SmPC.
- -
- Cardiac Disorders: While not mentioned in the Xolair® SmPC, omalizumab was associated with 29 cases registered in FEDRA, 4% of those reported including increased heart rate and coronary ischemic disorders (angina pectoris and myocardial infarction) as the most reported ADR terms.
- -
- Blood and Lymphatic System Disorders: The SmPC for Xolair® indicates that omalizumab may lead, with an unknown frequency, to the development of idiopathic thrombocytopenia, including severe cases. In FEDRA, a total of 25 cases (4%) were reported with suspected adverse events of omalizumab on blood parameters (anemic disorders and lymphadenopathy, not described in SmPC).
- -
- Pregnancy, puerperium, and perinatal diseases. Omalizumab crosses the placental barrier, but there is no risk of malformations or associated fetal/neonatal toxicity in SmPC, if clinically necessary, use during pregnancy may be considered. In FEDRA there are 19 cases (3%). The most numerous cases reported are related to abortion (n = 6).
- -
- Eye Disorders: Although not described in the Xolair® SmPC, 19 cases (3%) including eye and eyelid edema were reported in FEDRA.
- -
- Psychiatric Disorders. There are no adverse reactions related to any psychiatric disorder described in the Xolair® SmPC. However, there are 15 cases registered in FEDRA linking omalizumab to some psychiatric disorder, 2% of the total notifications. Anxiety-related disorders and symptoms are the most frequently reported ADRs.
- -
- In FEDRA, there are 13 cases linking the use of omalizumab to the appearance of disorders of the reproductive system and breast, 2% of the total. The Xolair® SmPC does not include terms related to this system or organ. There were found reactions that could be of interest, such as menstrual cycle disorders.
- -
- No mention of metabolic and nutritional disorders is made in the information contained in the Xolair® SmPC either. These reactions accounted for almost 2% of the cases in FEDRA (n=11). Decreased appetite was the only one to be considered of interest.
- -
- FEDRA contains 8 cases associating the use of omalizumab with some disorder of the ear and labyrinth, accounting for 1% of the total notifications of this drug. Hearing loss was the most reported ADR with 5 out of the 8 cases in this SOC. No ADRs with this type of disorder are currently described in the Xolair® SmPC.
3.2.2. Mepolizumab
The most commonly ADR described in the Nucala® SmPC was headache, followed by infections (lower respiratory tract infections, urinary tract infections, and pharyngitis), hypersensitivity reaction, nasal congestion, pain in the upper abdomen and back, eczema, injection site reactions, fever, and rare cases of anaphylaxis are also mentioned.
FEDRA database reported 499 cases of adverse reactions linked to mepolizumab; with symptoms categorized by frequency:
- -
- Respiratory issues, constituting 30% of cases, include known reactions and exacerbation of treated conditions (n = 166).
- -
- Skin and subcutaneous reactions, also 30%, mostly align with hypersensitivity described in product info. There are 8 cases of alopecia that may be of interest.
- -
- Neurological symptoms, totaling 26%, mostly headaches and dizziness. Not specified in product info were: 15 cases of Paresthesia, Hypoesthesia or Dysesthesia (5 of them in a context of Severity); Muscle weakness and atrophy 6 cases (3 severe); Tremor 5 cases (3 severe); CNS vascular disorders: 4 cases (all 4 serious).
- -
- Regarding the Immune System, 105 cases (21%): our series predominantly included reactions already described in SmPC of hypersensitivity (systemic allergic reaction) and Anaphylaxis. But it can be explored if there is any relationship with other diseases or autoimmune symptoms (n = 5 cases): Lichen planus, Vasculitis, Telangiectasia, Pemphigoid, Disease related to immunoglobulin G4.
- -
- Musculoskeletal symptoms. There were 27 cases of arthralgia (5% of all cases reported with mepolizumab), 7 of them severe.
- -
- Cardiac issues are presently not outlined in the Mepolizumab® SmPC. Nonspecific symptoms (55 cases) whose alternative cause could be related to the underlying disease were noted, with 7 cases of arrhythmias reported as serious.
- -
- Vascular disorders (13%) exhibited 67 cases coded with 30 ADR terms including vasculitis, thrombosis, purpura, cyanosis, telangiectasia, hypertension, etc., all also described in hyper-eosinophilic conditions. In 9 cases, at least one of the following three terms were reported: Deep vein thrombosis, stroke, and /or pulmonary embolism.
- -
- Infections and infestations (13%) included upper respiratory infections and a case of visceral leishmaniasis. Herpes zoster infection stands out with statistical significance of notification.
- -
- Gastrointestinal symptoms (13%) are not mentioned in the mepolizumab SmPC. Of the 64 cases describing some GI symptom, 21 were regarded as serious clinical conditions.
- -
- Psychiatric issues were not covered in the mepolizumab SmPC and reported cases (n=29) in FEDRA were insufficient to delineate a clear ADR pattern.
- -
- Neoplasms reported to FEDRA included 24 cases (5%) encompassing male breast cancer (2), lung (3), and five cases gastrointestinal tract cancers that were particularly noteworthy.
3.2.3. Benralizumab
FEDRA contains 588 cases reporting adverse reactions from both spontaneous notification programs and observational studies, where benralizumab was the suspected drug. Consistent with what is described in the benralizumab SmPC, headaches (including migraine) were the most frequently reported ADR, accounting for 14.6% (86 cases), followed by pharyngitis (including aphonia, tonsillitis, dysphagia, oropharyngeal pain, throat dryness, nasopharyngitis, and laryngeal irritation), with 16.15% (95 cases).
- -
- General Disorders and Administration Site Conditions: This was the most frequently reported category, comprising 42% (246 cases) of all cases. Fatigue was mentioned in 55 cases, with 9 cases being classified as severe asthenia.
- -
- Respiratory, Thoracic, and Mediastinal Disorders: These accounted for 34% (200 cases) of the total cases, but the symptoms described could be related to the underlying disease being treated, so they are not detailed.
- -
- Neurological Disorders symptoms were present in 26% of the cases (151 cases). However, most of these terms corresponded to headache (82 cases), a reaction already documented in the SmPC. The rest were too nonspecific and scattered for analysis.
- -
- Skin and Subcutaneous Tissue Disorders accounted for 16% of the cases (116 cases), with most falling under hypersensitivity reactions described in the product information. However, there were 6 cases of alopecia that may be of interest.
- -
- Musculoskeletal and Connective Tissue Disorders: They represented 15% of all cases (86 cases) with myalgia being the most notable (29 cases, 14% of them severe), followed by arthralgia (18 cases of which 22% were regarded as severe).
- -
- Gastrointestinal Disorders were 14% of all cases (85 cases), most corresponding to disorders listed in the product information or being too scattered for analysis. However, there were 14 cases with terms related to abdominal pain: 7 of abdominal discomfort, 5 of abdominal pain (one severe), and 5 of upper abdominal discomfort.
- -
- Immune System Disorders: This accounted for 13% of cases (75 cases), primarily comprising hypersensitivity reactions (systemic allergic reaction and cutaneous manifestations) and anaphylaxis.
- -
- Infections represented 11% of cases (68 cases). While many terms referred to pharyngeal infections already described in the SmPC, other infection-related terms appeared in 39 cases (more than half of all infections), with 19 of them being severe. The most relevant among them are those related to pneumonia: Unspecified pneumonia was reported in 5 cases, but it can be grouped together with other terms of specific pneumonia such as streptococcal pneumonia, fungal pneumonia, pneumonia due to COVID-19 (one case each) or even with another terms suggestive of pneumonia (pleural, productive cough...etc) reaching an important clinical meaning.
- -
- Cardiac disorders accounted for 11% of all notified cases (66 cases), with symptoms possibly related to coronary ischemia being notable: 7 cases of chest pain, 9 of chest discomfort and one Kounis´syndrome.
- -
- Vascular disorders: The terminology dispersion in this category hinders interpretation, but blood pressure disorders stand out: hypertension (5 cases) and hypotension (5 cases).
- -
- Psychiatric disorders: Although not described in the product information, there were 45 reported cases (8%), with sleep disorders being notable, accounting for 22 of the 52 terms (nearly half) grouped under psychiatric disorders. Other remarkable terms were those related to anxiety -anxiety (4), nervousness (4)- or mood disorders (4)
- -
- Not described in the SmPC were also weight increase (3 cases) and decreased appetite (3 cases)
3.2.4. Dupilumab
In FEDRA, we found 537 cases associated with the drug dupilumab. Upon reviewing the SmPC, the most frequent adverse reactions included injection site reactions (including erythema, swelling, itching, pain, and swelling), conjunctivitis, allergic conjunctivitis, arthralgia, oral herpes, and eosinophilia. An additional adverse reaction of bruising at the injection site was reported in the US. Rare cases of serum sickness, serum sickness-like reaction, anaphylactic reaction, and ulcerative keratitis have also been reported.
- -
- Skin and subcutaneous tissue disorders were the most frequent suspected ADRs, with 29% (159 cases) of all notified cases. Adverse reactions not described in the SmPC included alopecia /alopecia areata with 21 cases and psoriasis with 11 cases respectively.
- -
- The second most reported category was infections and infestations, with 28% (153 cases) of the cases recorded in FEDRA. Despite the dupilumab SmPC mentions a section on infections and infestations, detailing conjunctivitis, oral herpes, and the potential impact on responses to helminthic infections, FEDRA reported additional cases such as pneumonia (11 cases), lower respiratory tract infections (3 cases), and cellulitis (3 cases).
- -
- FEDRA records 136 cases (25%) of General disorders and conditions at the local administration site. These types of disorders are addressed in the dupilumab SmPC; FEDRA highlights pyrexia (14 cases), malaise (12 cases), asthenia (9 cases) and fatigue (9 cases).
- -
- In FEDRA, 88 cases (16%) of ocular disorders secondary to dupilumab were reported, although the SmPC already lists conditions such as allergic conjunctivitis, keratitis, blepharitis, ocular pruritus, dry eye, and ulcerative keratitis. FEDRA reports additional symptoms like tearing, discomfort, and hyperemia, which may indicate the presence of already described ADRs.
- -
- FEDRA records 67 cases (12%) of nervous system disorders, not covered in the dupilumab SmPC, FEDRA highlights headaches (25 cases), dizziness (10 cases), and syncope (5 cases).
- -
- Furthermore, FEDRA lists 58 cases (10%) of musculoskeletal and connective tissue disorders, with arthralgia being the most common, consistent with the SmPC. Other reported symptoms include myalgia (5 cases), bone pain (5 cases), and limb pain (5 cases).
- -
- There were also 47 cases (8%) describing abnormalities in Investigations, with decreased weight (5 cases), not mentioned in the SmPC, being noteworthy.
- -
- While gastrointestinal disorders were not listed as possible ADRs in the SmPC, FEDRA associated 35 cases (6%) with dupilumab, including vomiting and nausea (13 cases), diarrhea (5 cases), and 3 cases reported Crohn's disease as an adverse event.
- -
- Blood and lymphatic system disorders, described in the SmPC, were reported in FEDRA with 35 cases (6%), most of which involved eosinophilia (18 cases) already mentioned in the SmPC, and lymphadenopathy (11 cases) not previously described.
- -
- FEDRA also documented 23 cases (4%) of vascular disorders, including erythema (7 cases) and vasculitis (5 cases), none of which were previously reported in the SmPC.
- -
- Psychiatric disorders were noted with 21 (3%) cases, the most prevalent being anxiety, stress, and nervousness, totaling 11 cases together.
- -
- The results of immune system disorders in FEDRA included 16 cases (2%), with the most characteristic being eosinophilic granulomatosis with polyangiitis (EGPA) with 3 cases.
- -
- Additionally, 11 cases (2%) of cardiac disorders were reported in FEDRA, with tachycardia (5 cases) being the most frequent.
- -
- Metabolic and nutritional disorders were described in 6 cases (1%), with abnormal weight loss (2 cases) and decreased appetite (2 cases) being notable and absent in the SmPC.
3.2.5. Reslizumab
As the sole biologic drug in our group designated for intravenous administration, its usage is notably lower compared to other alternatives, even in the absence of consumption data. Currently, there have been only 30 suspected ADRs reported with this biologic, among which 19 were classified as serious. These cases encompassed several instances of arthralgia, some of which were clinically severe, along with 7 reports of neoplasms, including 2 cases of glioma, and occurrences of two thrombosis or pulmonary embolism.
3.2.6. Tezepelumab
With its recent market introduction in September 2023, up to April 1, 2024, there have been only eleven cases of suspected ADRs associated with this biologic drug. Among them, 5 were deemed serious, with 2 requiring hospital admissions and 3 exhibited clinically significant symptoms. The reported reactions align with those described in the Tezspire® SmPc, encompassing arthralgia, myalgia, bronchospasm, cough, dyspnea, pruritus, erythema, and wheezing.
Additionally, Table 7 displays the values of the mentioned reporting disproportion of associations drug-ADR reported to FEDRA and not contained in the SmPC.
4. Discussion
This is to our knowledge the first investigation to evaluate the real-life safety profile of approved asthma biologics using the FEDRA database in Spain. Considering the substantial variations in asthma phenotypes [12,48,49] and the heterogeneity in the use of asthma biologics across different regions and populations [50,51], obtaining an overview of ADRs that may be locally prevalent but are not currently addressed in the biological therapies SmPC is of utmost importance.
4.1. Industry Reporting
It is worth highlighting the preeminent place occupied by industry notifications, since it represents almost 90% of the cases notified to FEDRA concerning these biologicals. Among them, nearly 40% are cases from studies. However, as the SEFV-H does not consider this type of reports in its statistical analysis to avoid bias a significant portion of unexpected adverse effects, although detected, will not be included into the analysis for signal generation. Furthermore, the information provided by MAH and SEFV-H exhibits distinct profiles, particularly evident in the clinical evolution or outcome of ADRs. In over 40% of cases, the industry classifies these outcomes as unknown, whereas SEFV-H accounts for less than 20% such cases. This discrepancy extends to other data such as age, sex, dates of medication use, and the onset and resolution of reported ADRs. Consequently, the data obtained from industry sources may be less conclusive compared to that typically provided directly to health system pharmacovigilance programs.
4.2. SmPC and Risk
The review of the reports within FEDRA has facilitated the identification of numerous risks not included in the SmPC. Additionally, it is noteworthy that ADRs documented in the SmPC were often reported, frequently in significant quantities. The substantial disparity between the limited safety information provided in the SmPC for these medications and the comprehensive data yielded by the Pharmacovigilance system is remarkable. Moreover, the inconsistency in the representation of ADR content among various SmPC is also striking.
Both mepolizumab and omalizumab include myalgia and arthralgia in their ADR profiles. Notably, myalgia and arthralgia have been newly listed in the mepolizumab SmPC based on research conducted by the Canary Islands-CAFV and the Allergy Department at our Institution that originated a signal on this association that was approved by PRAC of EMA in 2024 April. In contrast, reslizumab lists only myalgia, while tezepelumab and dupilumab exclusively mention arthralgia in their respective SmPC. Surprisingly, despite some drugs of this group include all these symptoms and others only some of them, benralizumab´s SmPC does not include musculoskeletal adverse effects at all yet reports of both ADRs have been reported with statistically significance in FEDRA, with many cases being serious (Table 8).
Although pyrexia is mentioned in the SmPCs of omalizumab, mepolizumab and benralizumab, it is notably absent in dupilumab´s, yet it has been equally reported across these medications. Alopecia is described in the omalizumab SmPC, but not for the rest of the evaluated biologics, although it has been reported with each of them, even in a statistically significant manner with mepolizumab, benralizumab and dupilumab [52,53]. The mechanism of action of dupilumab may contribute to sebaceous gland atrophy and subsequent alopecia [54,55]. This may be similar for the other drugs studied. Infections of the lower respiratory tract are solely listed in mepolizumab´s SmPC, despite being also widely reported with omalizumab, benralizumab and dupilumab.
These discrepancies highlight the importance of comprehensive reporting and analysis within pharmacovigilance systems. Although it is a striking finding we do not expect identical information in each document nor suggest a class effect as each medication operates through distinct mechanisms, leading to differences in their adverse event profiles [56,57]. Understanding these distinctions may enhance comprehension of medication safety profiles and inform clinical decision-making.
4.3. ADR and Underlying Disease
The ADRs reported with these medicines indicate that some symptoms occur with each active ingredient in this group. This finding prompts us to consider whether the symptoms may be related to the underlying disease, any biological therapy, or if they are attributable to each drug. For instance, fatigue and asthenia, frequently reported with these drugs, may be related to the underlying disease. Similarly, the avoidance of discussing respiratory-related symptoms underlines the importance of considering any ADR likely to occur in patients with severe uncontrolled asthma.
4.4. Eosinophilic Granulomatosis with Polyangiitis (EGPA)
The reports concerning immune system disorders in FEDRA included 3 cases of EGPA with dupilumab, 3 with benralizumab, 2 with mepolizumab and 11 with omalizumab. The SmPC of dupilumab mentions EGPA cases in both drug-treated and placebo-treated patients, suggesting a possible relationship with corticosteroid reduction, which could serve as an alternative explanation applicable to all drugs [58]. However, this implies that unless the clinician confirms the discontinuation of corticosteroids use in a patient, the case of EGPA may be considered potentially linked to the drug under scrutiny. The disruption produced by dupilumab may induce excessive eosinophilic inflammation, contributing to the development of EGPA [54]. A similar mechanism may be valid for the other drugs, but this has not been assessed. To further complicate matters, certain biological drugs not only may have the potential to trigger EGPA but can also serve as treatments for the condition [59,60,61]. And, although causality has not been established, caution has been recommended when prescribing dupilumab for uncontrolled asthma with characteristics that may indicate EGPA [54,62]
4.5. Neoplastic Disorders and Biological Therapy
While the potential for tumor development when using a drug that impacts the immune response is concerning, the SmPC of omalizumab states that “No formal carcinogenicity studies have been performed with omalizumab”, and neither benign nor malignant neoplasms are described in the SmPC. However, some controversies have been raised as its long-term use has recently been linked to potential cancer risk [63,64,65,66]. Furthermore, a statistical association between malignancy and these drugs was found in FEDRA:
Sixty-seven cases were registered that linked omalizumab with a neoplastic disorder, representing 10% of its total cases. Anyway, the evidence from literature is inconclusive [67]. The same situation occurred with mepolizumab, where neoplasms reported to FEDRA accounted for 24 cases encompassing male breast cancer (two cases), lung (three cases), and gastrointestinal tract cancers in 5 cases. With benralizumab and dupilumab the situation was similar, with different types of neoplasms being reported, but without any available reference in the SmPC. For benralizumab there were 11 cases, and for dupilumab 10 cases were described, both accounting for 2% of the total cases.
4.6. Vascular Disorders
Central nervous system vascular disorders, including cerebrovascular accidents, transient ischemic attacks, and ischemic strokes, have been reported with both omalizumab and mepolizumab. However, these events, included in the product information for the USA by the FDA several years ago, were not incorporated in the SmPC for either drug [68,69]. Cases of deep vein thrombosis have also been reported with both omalizumab and mepolizumab. Additionally, pulmonary embolism has been described with the latter, and occasionally reported with reslizumab as well [70] . In addition, omalizumab has been associated with cardiac disorders, notably ischemic alterations of coronary arteries. Similarly, there are cases of ischemic coronary disorder with benralizumab; however, this information was not included in the SmPC for either drug.
Some of the cases of vascular disorders associated with mepolizumab exhibited terms including vasculitis, thrombosis, purpura, cyanosis, telangiectasia, hypertension, etc. These manifestations are also described in hyper-eosinophilic conditions, suggesting another instance of overlap with the underlying condition [71,72].
4.7. ADR Comments for Specific Biological Agents in Severe Asthma
Omalizumab
Safety issues with omalizumab accumulate the most cases, possibly due to its status as the oldest drug among those reviewed. In addition to the vascular conditions already described, the association with deafness [73] and various autoimmune conditions (Multiple Sclerosis, Sjögren's syndrome and optic neuritis) stands out, requiring more specific studies due to their clinical relevance. Moreover, the association of spontaneous abortion with omalizumab also exhibits a statistical association, demanding further investigation, a situation that was not observed with the rest of the biological drugs for SA [74].
Mepolizumab
Among the cases reported with mepolizumab, the association of paresthesias, dysesthesias, and hypoesthesias stands out, as it is not described with the rest of biologics in this group [63]. Moreover, and in line with former research, it is also worth highlighting the occurrence of Herpes zoster (6 cases) which holds statistical significance [67,75,76,77], PRAC of April 2024 has already included this ADR in the Side Effects section of the SmPC of mepolizumab. The appearance of alopecia, arthralgia, asthenia, and vascular alterations (including cerebrovascular accidents, deep vein thrombosis and pulmonary thromboembolism) has already been discussed in previous sections.
Benralizumab
Safety concerns regarding benralizumab appear to have been underestimated. The SmPC provides scant information: the ADRs table includes only 7 terms grouped into 4 SOC. However, ADR reporting associated with this drug presents a different narrative in this study, something that also has been reported by former research [78,79]. It is particularly striking that infections, a significant concern for a drug affecting the immune system, accounted for 11% of reported cases. Conversely, the benralizumab SmPC describes only pharyngitis, while other types of infections have been previously overlooked [75,80,81] despite some studies addressing them [82,83]. Another type of reaction that should be noted are sleep disorders due to benralizumab, a condition that may be easily assessed during the clinical interview with a simple question. However, it should be noted that all these findings may not align the conclusions drawn in other scientific literature [84].
Dupilumab
The proportion of male to females in reporting suspected ADRs to all these drugs follows the sex distribution of patients with SA, being more frequent in females (3:1). However, a different sex distribution was found for dupilumab (1:1), likely due to its initial indication for uncontrolled severe atopic dermatitis, which may exhibit a different sex distribution [85] . Also, the unusually high reporting of conjunctivitis and eye symptoms with dupilumab, may be preferentially linked to its initial indication for atopic dermatitis [38], as conjunctivitis is not typically associated with asthma but with atopic eczema. Nevertheless, it should be noted that conjunctivitis has been described in patients treated with dupilumab for atopic dermatitis when compared to placebo or other immunosuppressants [86,87,88]. The same overlapping phenomenon may occur with skin and subcutaneous tissue disorders, which were most frequent ADR reported with this drug. However, the reporting of alopecia/alopecia areata (21 cases), not described in the SmPC, may not be attributable to underlying atopic eczema [53,89,90] while a causative mechanism, very different from the dermatitis, has been proposed for the conjunctivitis [(67)]. Metabolic and nutritional disorders were described in 6 cases (1%) with dupilumab, with notable occurrences of abnormal weight loss (2 cases) and decreased appetite (2 cases), which are absent in the SmPC. Surprisingly, weight gain, described in former research but not in the SmPC has been addressed [91]. Additionally, benralizumab has also been related to these findings, albeit in a low number (3 cases of weight increase and 3 of appetite loss).
5. Limitations of the Study
Underreporting: Studies relying on spontaneous reporting of ADRs face several limitations, notably underreporting to the pharmacovigilance system, leading to an underestimation of the true frequency of drug-related adverse events. Additionally, reporting rates may fluctuate due to factors such as the type and severity of the reaction, the medications involved, and whether the drug is newly marketed or established in the market [42,92,93].
Indication: It should be noted that the cases analyzed correspond to patients under treatment with these drugs whatever it may be the indication, so the ADR reported is independent of the underlying condition. This perceived limitation may not as a significant drawback, considering the following facts:
- We aimed to span our knowledge of the security profile of these approved drugs, avoiding as much as possible the bias resulting from an underlying condition.
- The biologic drug indication data are often sparsely documented. Studies focusing solely on indication may overlook a significant number of reports, potentially up to 70% in some cases) [94]. However, studies utilizing that approach failed to identify any ADR that were not already described in the present investigation. We interpret this finding as supportive evidence for our approach.
- All the elucidated facts highlight the necessity for this type of data to be routinely included by any professional in their reporting.
Selection of ADR: The clinical importance of an ADR is given by many factors, among them, the number of cases involved. This number is largely subjective, as an ADR can be defined by a single term or a grouping of terms, so the number of cases needed to consider an ADR to be clinically significant cannot be easily established. However, a significant number of the ADRs described exhibit have statistical significance, as indicated by the disproportionality analysis revealing a statistical association. Given that many cases from so-called studies are not included in this type of analysis, it can be inferred that all mentioned ADRs in this study hold clinical relevance.
6. Conclusions and Future Research Directions
Pharmacovigilance activity, based on spontaneous reporting programs for suspected ADR, serves as an effective system for gaining accurate and early insights into the profile of ADR in real-world settings. The generation and validation of signals in pharmacovigilance enable the generation of new safety hypotheses and contribute to ongoing safety surveillance of drugs post-marketing. Real-world studies offer a valuable tool for post-marketing monitoring of biological drugs, enhancing our understanding of their effectiveness and safety in everyday clinical practice, thereby bolstering clinicians´ confidence among clinicians in their utilization of biologics in SA.
Despite the biologics´ overall safety, this review of the Spanish Pharmacovigilance database reveals numerous serious cases not documented in the SmPC, warranting detailed investigation as pharmacovigilance signals. Addressing these associations is a commitment for our research team in the future. Furthermore, for future reviews, exploring adverse effects following prolonged use of these biological medications, particularly with usage periods exceeding 2 years post-marketing, appears worthwhile.
Considering the relevance of enhancing drug safety knowledge, it is imperative to encourage active participation and engagement of patients, healthcare professionals, pharmaceutical companies, and regulatory bodies in reporting suspected ADRs through the promotion of side-effect reporting programs. The collaboration between CAFV and clinical areas like the Allergy Department at our Institution has proven instrumental in achieving clinically relevant results, emphasizing the significance of such partnership in advancing drug safety knowledge.
Author Contributions
Conceptualization, C.B-F., M.G-S., E.F-Q., and R.G-P.; methodology, C.B-F., M.G-S., and E.F-Q.; investigation, C.B-F., M.G-S., E.F-Q., L.R-L., and R.G-P.; resources, P.P-G., and I.S-M.; data curation, C.B-F., M.G-S., E.F-Q., and L.R-L.; writing—original draft preparation, C.B-F., M.G-S., E.F-Q., L.R-L., and R.G-P.; writing—review and editing, P.P-G., and I.S-M.; supervision, P.P-G., and I.S-M.; project administration, C.B-F., and R.G-P.; funding acquisition, R.G-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. It should be noted that this article is derived from reviews of existing databases, guidelines, and literature, and does not involve any studies regarding human participants or animals.
Informed Consent Statement
Not applicable. It should be noted that this article is derived from reviews of existing databases, guidelines, and literature, and does not involve any studies regarding human participants or animals.
Data Availability Statement
The data that support the findings of this study are available from Servicio Canario de la Salud, however, restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with the permission of Servicio Canario de la Salud.
Conflicts of Interest
The authors declare no conflicts of interest in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
FEDRA database of the Spanish System of Pharmacovigilance of Human Medicines (SEFV-H) disclaimer
The data for the completion of this study come from the FEDRA database of the SEFV-H, managed by the Spanish Agency of Medicines and Medical Devices (AEMPS). The results, discussion, and conclusions of the study are solely those considered by the authors and do not represent in any way the position of the SEFV-H or the AEMPS regarding this topic.
References
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2023 [Internet]. https://ginasthma.org/.
- Ferkol T, Schraufnagel D. The Global Burden of Respiratory Disease. Ann Am Thorac Soc. 2014 March;11(3):404-6. [CrossRef]
- Price D, Fletcher M, van der Molen T. Asthma control and management in 8,000 European patients: the REcognise Asthma and LInk to Symptoms and Experience (REALISE) survey. NPJ Prim Care Respir Med. 2014 June 12th d;24:14009. [CrossRef]
- Levy ML. The national review of asthma deaths: what did we learn and what needs to change? Breathe Sheff Engl. 2005 March;11(1):14-24.
- Sadatsafavi M, Rousseau R, Chen W, Zhang W, Lynd L, FitzGerald JM. The preventable burden of productivity loss due to suboptimal asthma control: a population-based study. Chest. 2014 April;145(4):787-93.
- Rogliani P, Calzetta L, Matera MG, Laitano R, Ritondo BL, Hanania NA, et al. Severe Asthma and Biological Therapy: When, Which, and for Whom. Pulm Ther. 2020 June;6(1):47-66. [CrossRef]
- Habib N, Pasha MA, Tang DD. Current Understanding of Asthma Pathogenesis and Biomarkers. Cells. 2022 September 5th;11(17):2764. [CrossRef]
- Anderson GP. Endotyping asthma: new insights into key pathogenic mechanisms in a complex, heterogeneous disease. Lancet Lond Engl. 2008 September 20th;372(9643):1107-19. [CrossRef]
- Kuruvilla ME, Lee FEH, Lee GB. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin Rev Allergy Immunol. 2019 April;56(2):219-33. [CrossRef]
- Ray A, Camiolo M, Fitzpatrick A, Gauthier M, Wenzel SE. Are We Meeting the Promise of Endotypes and Precision Medicine in Asthma? Physiol Rev. 2020 July 1st;100(3):983-1017.
- McDowell PJ, Heaney LG. Different endotypes and phenotypes drive the heterogeneity in severe asthma. Allergy. 2020 February;75(2):302-10. [CrossRef]
- Espuela-Ortiz A, Martin-Gonzalez E, Poza-Guedes P, González-Pérez R, Herrera-Luis E. Genomics of Treatable Traits in Asthma. Genes. 2023 September 20th;14(9):1824. [CrossRef]
- Sze E, Bhalla A, Nair P. Mechanisms and therapeutic strategies for non-T2 asthma. Allergy. 2020 February;75(2):311-25. [CrossRef]
- Kim SR. Next-Generation Therapeutic Approaches for Uncontrolled Asthma: Insights Into the Heterogeneity of Non-Type 2 Inflammation. Allergy Asthma Immunol Res. 2024;16(1):1.
- Xie Y, Abel PW, Casale TB, Tu Y. TH17 cells and corticosteroid insensitivity in severe asthma. J Allergy Clin Immunol. 2022 February;149(2):467-79. [CrossRef]
- Carr TF, Peters MC. Novel potential treatable traits in asthma: Where is the research taking us? J Allergy Clin Immunol Glob. 2022 May;1(2):27-36.
- Stokes JR, Casale TB. Characterization of asthma endotypes: implications for therapy. Ann Allergy Asthma Immunol. 2016 August;117(2):121-5.
- Han YY, Zhang X, Wang J, Wang G, Oliver BG, Zhang HP, et al. Multidimensional Assessment of Asthma Identifies Clinically Relevant Phenotype Overlap: A Cross-Sectional Study. J Allergy Clin Immunol Pract.2021 January ;9(1):349-362.e18. [CrossRef]
- Ricciardolo FLM, Guida G, Bertolini F, Di Stefano A, Carriero V. Phenotype overlap in the natural history of asthma. Eur Respir Rev. 2023 June 30th;32(168):220201. [CrossRef]
- Fouka E, Domvri K, Gkakou F, Alevizaki M, Steiropoulos P, Papakosta D, et al. Recent insights in the role of biomarkers in severe asthma management. Front Med. 2022;9:992565. [CrossRef]
- Fahy JV. Type 2 inflammation in asthma — present in most, absent in many. Nat Rev Immunol.2015 January;15(1):57-65.
- EMA medical terms simplifier [Internet]. 2023. www.ema.europa.eu/en/documents/other/ema-medical-terms-simplifier_en.pdf.
- Lommatzsch M, Brusselle GG, Canonica GW, Jackson DJ, Nair P, Buhl R, et al. Disease-modifying anti-asthmatic drugs. Lancet Lond Engl. 2022 April 23th;399(10335):1664-8. [CrossRef]
- Farne HA, Wilson A, Milan S, Banchoff E, Yang F, Powell CV. Anti-IL-5 therapies for asthma. Cochrane Database Syst Rev. 2022 July 12th;7(7):CD010834.
- González-Pérez R, Poza-Guedes P, Mederos-Luis E, Sánchez-Machín I. Real-Life Performance of Mepolizumab in T2-High Severe Refractory Asthma with the Overlapping Eosinophilic-Allergic Phenotype. Biomedicines. 19 de octubre de 2022 October 19th;10(10):2635. [CrossRef]
- Papaioannou AI, Fouka E, Bartziokas K, Kallieri M, Vontetsianos A, Porpodis K, et al. Defining response to therapy with biologics in severe asthma: from global evaluation to super response and remission. Expert Rev Respir Med. 2023;17(6):481-93. [CrossRef]
- Thomas D, McDonald VM, Pavord ID, Gibson PG. Asthma remission: what is it and how can it be achieved? Eur Respir J. 2022 November;60(5):2102583.
- Humbert M, Beasley R, Ayres J, Slavin R, Hébert J, Bousquet J, et al. Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATE. Allergy. 2005 March;60(3):309-16. [CrossRef]
- Chang TW. The pharmacological basis of anti-IgE therapy. Nat Biotechnol. febrero de 2000;18(2):157-62. [CrossRef]
- BIFIMED: Buscador de la Información sobre la situación de financiación de los medicamentos - Nomenclátor de ABRIL - 2024 [BIFIMED: Information Search Engine on the financing situation of medicines - Nomenclátor APRIL - 2024]. www.sanidad.gob.es/profesionales/medicamentos.do?metodo=verDetalle&cn=652563.
- McGregor MC, Krings JG, Nair P, Castro M. Role of Biologics in Asthma. Am J Respir Crit Care Med. 2019 February 15th;199(4):433-45.
- Corren J. New Targeted Therapies for Uncontrolled Asthma. J Allergy Clin Immunol Pract. mayo de 2019;7(5):1394-403. [CrossRef]
- Nucala: EPAR - Product Information [Internet].www.ema.europa.eu/en/documents/product-information/nucala-epar-product-information_en.pdf.
- Cinqaero : EPAR - Product Information [Internet].: www.ema.europa.eu/en/documents/product-information/cinqaero-epar-product-information_en.pdf.
- Fasenra : EPAR - Product Information [Internet].https://www.ema.europa.eu/en/documents/product-information/fasenra-epar-product-information_en.pdf.
- Informe de Posicionamiento Terapéutico de benralizumab (Fasenra®) como tratamiento adicional en el asma grave no controlada eosinofílica [Internet].: /www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/IPT-benralizumab-Fasenra-asma_EPOC.pdf.
- Tezspire : EPAR - Product Information [Internet]. www.ema.europa.eu/en/documents/product-information/tezspire-epar-product-information_en.pdf.
- Dupixent : EPAR - Product Information [Internet]. https://www.ema.europa.eu/en/search?f%5B0%5D=ema_search_entity_is_document%3ADocument&search_api_fulltext=Dupixent%3A%20EPAR%20-%20Product%20Information.
- Bavbek S, Pagani M, Alvarez-Cuesta E, Castells M, Dursun AB, Hamadi S, et al. Hypersensitivity reactions to biologicals: An EAACI position paper. Allergy. 2022 January;77(1):39-54. [CrossRef]
- Sitek A, Chiarella SE, Pongdee T. Hypersensitivity reactions to biologics used in the treatment of allergic diseases: clinical features, diagnosis and management. Front Allergy. 2023 August 11th;4:1219735. [CrossRef]
- Real Decreto 577/2013, de 26 de julio, por el que se regula la farmacovigilancia de medicamentos de uso humano. [Internet]. https://www.boe.es/buscar/doc.php?id=BOE-A-2013-8191.
- Bate A, Evans SJW. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol Drug Saf. 2009 June;18(6):427-36. [CrossRef]
- Guideline on good pharmacovigilance practices (GVP) Module IX Addendum I – Methodological aspects of signal detection from spontaneous reports of suspected adverse reactions.
- Grupo de trabajo Guía de señales del SEFV-H. Guía de señales del SEFV-H. Draft version. 2024.
- Evans SJ, Waller PC, Davis S. Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol Drug Saf. 2001;10(6):483-6. [CrossRef]
- ANEXO-005 Normas para la correcta interpretación y utilización de los datos del Sistema Español de Farmacovigilancia Humana (SEFV-H) [ANNEX-005 Standards for the correct interpretation and use of data from the Spanish Human Pharmacovigilance System (SEFV-H)]. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/file:///C:/Users/cboada/Downloads/ANEXO_SEFV-H-005%20v1-%20Normas%20correcta%20interpretaci%C3%B3n%20y%20utilizaci%C3%B3n%20datos%20del%20SEFV-H.pdf.
- ANEXO-008 v1- Campos que no se pueden liberar desde FEDRA 3 a personas ajenas al SEFV-H.pdf. [ANNEX-008 v1- Fields that cannot be released from FEDRA 3 to people outside the SEFV-H.pdf.].
- González-Pérez R, Poza-Guedes P, Pineda F, Galán T, Mederos-Luis E, Abel-Fernández E, et al. Molecular Mapping of Allergen Exposome among Different Atopic Phenotypes. Int J Mol Sci. 2023 June 21st;24(13):10467. [CrossRef]
- Garcia-Marcos L. Grand challenges in genetics and epidemiology of allergic diseases: from genome to exposome and back. Front Allergy. 2024 February 5th;5:1368259. [CrossRef]
- Frix AN, Heaney LG, Dahlén B, Mihaltan F, Sergejeva S, Popović-Grle S, et al. Heterogeneity in the use of biologics for severe asthma in Europe: a SHARP ERS study. ERJ Open Res. 2022 October;8(4):00273-2022.
- Casas-Maldonado, F, Álvarez-Gutiérrez, FJ, Blanco-Aparicio, M, Domingo-Ribas, C, Cisneros-Serrano, C, Soto-Campos, G, et al. Monoclonal antibody treatment for severe uncontrolled asthma in Spain: analytical map. J Asthma.2022 October 3rd;59(10):1997-2007. [CrossRef]
- Nixon R, Despiney R, Pfeffer P. Case of paradoxical adverse response to mepolizumab with mepolizumab-induced alopecia in severe eosinophilic asthma. BMJ Case Rep. 2020 February 20th;13(2):e233161. [CrossRef]
- Park S. Short communication: Comments on hair disorders associated with dupilumab based on VigiBase. PLoS One. 2022;17(7).
- Suzaki I, Tanaka A, Yanai R, Maruyama Y, Kamimura S, Hirano K, et al. Eosinophilic granulomatosis with polyangiitis developed after dupilumab administration in patients with eosinophilic chronic rhinosinusitis and asthma: a case report. BMC Pulm Med.2023 April 19th;23(1):130. [CrossRef]
- Flanagan K, Sperling L, Lin J. Drug-induced alopecia after dupilumab therapy. JAAD Case Rep. 2019 January;5(1):54-6. [CrossRef]
- Agache I, Beltran J, Akdis C, Akdis M, Canelo-Aybar C, Canonica GW, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020 May;75(5):1023-42.
- Casas-Maldonado F, Álvarez-Gutiérrez FJ, Blanco Aparicio M, Domingo Ribas C, Cisneros Serrano C, Soto Campos G, et al. Treatment Patterns of Monoclonal Antibodies in Patients With Severe Uncontrolled Asthma Treated by Pulmonologists in Spain. Open Respir Arch. 2023 July;5(3):100252. [CrossRef]
- Caminati M, Fassio A, Alberici F, Baldini C, Bello F, Cameli P, et al. Eosinophilic granulomatosis with polyangiitis onset in severe asthma patients on monoclonal antibodies targeting type 2 inflammation: Report from the European EGPA study group. Allergy.2024 February;79(2):516-9. [CrossRef]
- Bachert C, Han JK, Desrosiers MY, Gevaert P, Heffler E, Hopkins C, et al. Efficacy and safety of benralizumab in chronic rhinosinusitis with nasal polyps: A randomized, placebo-controlled trial. J Allergy Clin Immunol. 2022 April;149(4):1309-1317.e12. [CrossRef]
- Yonezawa H, Ohmura S ichiro, Ohkubo Y, Otsuki Y, Miyamoto T. New-onset of eosinophilic granulomatosis with polyangiitis without eosinophilia and eosinophilic infiltration under benralizumab treatment: A case report. Mod Rheumatol Case Rep. 29 de diciembre de 2023;8(1):145-9. [CrossRef]
- Caminati M, Menzella F, Guidolin L, Senna G. Targeting eosinophils: severe asthma and beyond. Drugs Context. 2019;8:212587. [CrossRef]
- Kai M, Vion PA, Boussouar S, Cacoub P, Saadoun D, Le Joncour A. Eosinophilic granulomatosis polyangiitis (EGPA) complicated with periaortitis, precipitating role of dupilumab? A case report a review of the literature. RMD Open. 2023 September;9(3):e003300. [CrossRef]
- Mota D, Rama TA, Severo M, Moreira A. Potential cancer risk with omalizumab? A disproportionality analysis of the WHO’s VigiBase pharmacovigilance database. Allergy.2021 October;76(10):3209-11.
- Ferastraoaru D, Gross R, Rosenstreich D. Increased malignancy incidence in IgE deficient patients not due to concomitant Common Variable Immunodeficiency. Ann Allergy Asthma Immunol. 2017 September;119(3):267-73. [CrossRef]
- Ferastraoaru D, Rosenstreich D. IgE deficiency and prior diagnosis of malignancy. Ann Allergy Asthma Immunol. 018 November;121(5):613-8. [CrossRef]
- Bagnasco D, Canevari RF, Del Giacco S, Ferrucci S, Pigatto P, Castelnuovo P, et al. Omalizumab and cancer risk: Current evidence in allergic asthma, chronic urticaria, and chronic rhinosinusitis with nasal polyps. World Allergy Organ J. 2022 December;15(12):100721. [CrossRef]
- Jackson K, Bahna SL. Hypersensitivity and adverse reactions to biologics for asthma and allergic diseases. Expert Rev Clin Immunol.2020 March 3rd;16(3):311-9. [CrossRef]
- FDA Drug Safety Communication: FDA approves label changes for asthma drug Xolair (omalizumab), including describing slightly higher risk of heart and brain adverse events [Internet]. 2014. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-approves-label-changes-asthma-drug-xolair-omalizumab-including.
- Iribarren C, Rahmaoui A, Long AA, Szefler SJ, Bradley MS, Carrigan G, et al. Cardiovascular and cerebrovascular events among patients receiving omalizumab: Results from EXCELS, a prospective cohort study in moderate to severe asthma. J Allergy Clin Immunol. 2017 May;139(5):1489-1495.e5. [CrossRef]
- Oblitas CM, Galeano-Valle F, Vela-De La Cruz L, Del Toro-Cervera J, Demelo-Rodríguez P. Omalizumab as a Provoking Factor for Venous Thromboembolism. Drug Target Insights. 2019;13:1177392819861987.
- Satake Y, Sakai S, Takao T, Saeki T. A case of subarachnoid associated with MPO-ANCA-positive eosinophilic granulomatosis with polyangiitis, successfully treated with glucocorticoid, cyclophosphamide, and mepolizumab. Mod Rheumatol Case Rep.2023 December 8th;rxad071.
- Mutoh T, Shirai T, Sato H, Fujii H, Ishii T, Harigae H. Multi-targeted therapy for refractory eosinophilic granulomatosis with polyangiitis characterized by intracerebral hemorrhage and cardiomyopathy: a case-based review. Rheumatol Int. 2022 November;42(11):2069-76. [CrossRef]
- Park HT, Park S, Jung YW, Choi SA. Is Omalizumab Related to Ear and Labyrinth Disorders? A Disproportionality Analysis Based on a Global Pharmacovigilance Database. Diagn Basel Switz. 8 de octubre de 2022 October 8th;12(10):2434. [CrossRef]
- Namazy JA, Blais L, Andrews EB, Scheuerle AE, Cabana MD, Thorp JM, et al. Pregnancy outcomes in the omalizumab pregnancy registry and a disease-matched comparator cohort. J Allergy Clin Immunol. 2020 February;145(2):528-536.e1. [CrossRef]
- Sitek AN, Li JT, Pongdee T. Risks and safety of biologics: A practical guide for allergists. World Allergy Organ J. 2023 January;16(1):100737. [CrossRef]
- Khurana S, Brusselle GG, Bel EH, FitzGerald JM, Masoli M, Korn S, et al. Long-term Safety and Clinical Benefit of Mepolizumab in Patients With the Most Severe Eosinophilic Asthma: The COSMEX Study. Clin Ther. 2019 October;41(10):2041-2056.e5. [CrossRef]
- Jackson DJ, Korn S, Mathur SK, Barker P, Meka VG, Martin UJ, et al. Safety of Eosinophil-Depleting Therapy for Severe, Eosinophilic Asthma: Focus on Benralizumab. Drug Saf. 2020 May;43(5):409-25. [CrossRef]
- Morikawa K, Toyoshima M, Koda K, Kamiya Y, Suda T. Cryptogenic organizing pneumonia after withdrawal of systemic corticosteroids for chronic eosinophilic pneumonia and severe asthma under benralizumab treatment. Respir Investig. 2024 March;62(2):231-3. [CrossRef]
- Tanaka A, Fujimura Y, Fuke S, Izumi K, Ujiie H. A case of bullous pemphigoid developing under treatment with benralizumab for bronchial asthma. J Dermatol. 2023 September;50(9):1199-202. [CrossRef]
- Akenroye A, Lassiter G, Jackson JW, Keet C, Segal J, Alexander GC, et al. Comparative efficacy of mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis. J Allergy Clin Immunol. 2022 November;150(5):1097-1105.e12.
- Korn S, Bourdin A, Chupp G, Cosio BG, Arbetter D, Shah M, et al. Integrated Safety and Efficacy Among Patients Receiving Benralizumab for Up to 5 Years. J Allergy Clin Immunol Pract. 2021 December;9(12):4381-4392.e4. [CrossRef]
- Kavanagh JE, Hearn AP, Dhariwal J, d’Ancona G, Douiri A, Roxas C, et al. Real-World Effectiveness of Benralizumab in Severe Eosinophilic Asthma. Chest. 2021 February;159(2):496-506.
- Mishra AK, Sahu KK, James A. Disseminated herpes zoster following treatment with benralizumab. Clin Respir J. 2019 March;13(3):189-91. [CrossRef]
- Jackson DJ, Pavord ID. Living without eosinophils: evidence from mouse and man. Eur Respir J.2023 January;61(1):2201217. [CrossRef]
- Bylund S, Kobyletzki L, Svalstedt M, Svensson A. Prevalence and Incidence of Atopic Dermatitis: A Systematic Review. Acta Derm Venereol. 2020;100(12):adv00160. [CrossRef]
- Akinlade B, Guttman-Yassky E, de Bruin-Weller M, Simpson EL, Blauvelt A, Cork MJ, et al. Conjunctivitis in dupilumab clinical trials. Br J Dermatol. 2019 September;181(3):459-73.
- De Bruin-Weller M, Thaçi D, Smith CH, Reich K, Cork MJ, Radin A, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical t. Br J Dermatol.2018 May;178(5):1083-101.
- Blauvelt A, Teixeira HD, Simpson EL, Costanzo A, De Bruin-Weller M, Barbarot S, et al. Efficacy and Safety of Upadacitinib vs Dupilumab in Adults With Moderate-to-Severe Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol. 2021 September 1st;157(9):1047-55.
- Sachdeva M. Alopecia areata related paradoxical reactions in patients on dupilumab therapy: a systematic review. J Cutan Med Surg. 2021;25(4):451-2. [CrossRef]
- Beaziz J, Bouaziz JD. Dupilumab-induced psoriasis and alopecia areata: case report and review of the literature. Ann Dermatol Venereol. 2021;148(3):198-201. [CrossRef]
- Johansson EK, Ivert LU, Bradley B, Lundqvist M, Bradley M. Weight gain in patients with severe atopic dermatitis treated with dupilumab: a cohort study. BMC Dermatol. 2020 September 22th;20(1):8. [CrossRef]
- Gonzalez-Gonzalez C, Lopez-Gonzalez E, Herdeiro MT, Figueiras A. Strategies to improve adverse drug reaction reporting: a critical and systematic review. Drug Saf. 2013 May;36(5):317-28. [CrossRef]
- Avedillo-Salas A, Pueyo-Val J, Fanlo-Villacampa A, Navarro-Pemán C, Lanuza-Giménez FJ, Ioakeim-Skoufa I, et al. Prescribed Drugs and Self-Directed Violence: A Descriptive Study in the Spanish Pharmacovigilance Database. Pharmaceuticals.2023 May 22th;16(5):772. [CrossRef]
- Cutroneo PM, Arzenton E, Furci F, Scapini F, Bulzomì M, Luxi N, et al. Safety of Biological Therapies for Severe Asthma: An Analysis of Suspected Adverse Reactions Reported in the WHO Pharmacovigilance Database. BioDrugs Clin Immunother Biopharm Gene Ther. 2024 March 15th; [CrossRef]
Figure 1.
The multiaxial structure of MedDRA. Abbreviations: SOC: System Organ Classes. HLGT: High-Level Group Term. HLT: High-Level Term. PT: Preferred Term. LLT: Low Level Term.
Figure 1.
The multiaxial structure of MedDRA. Abbreviations: SOC: System Organ Classes. HLGT: High-Level Group Term. HLT: High-Level Term. PT: Preferred Term. LLT: Low Level Term.
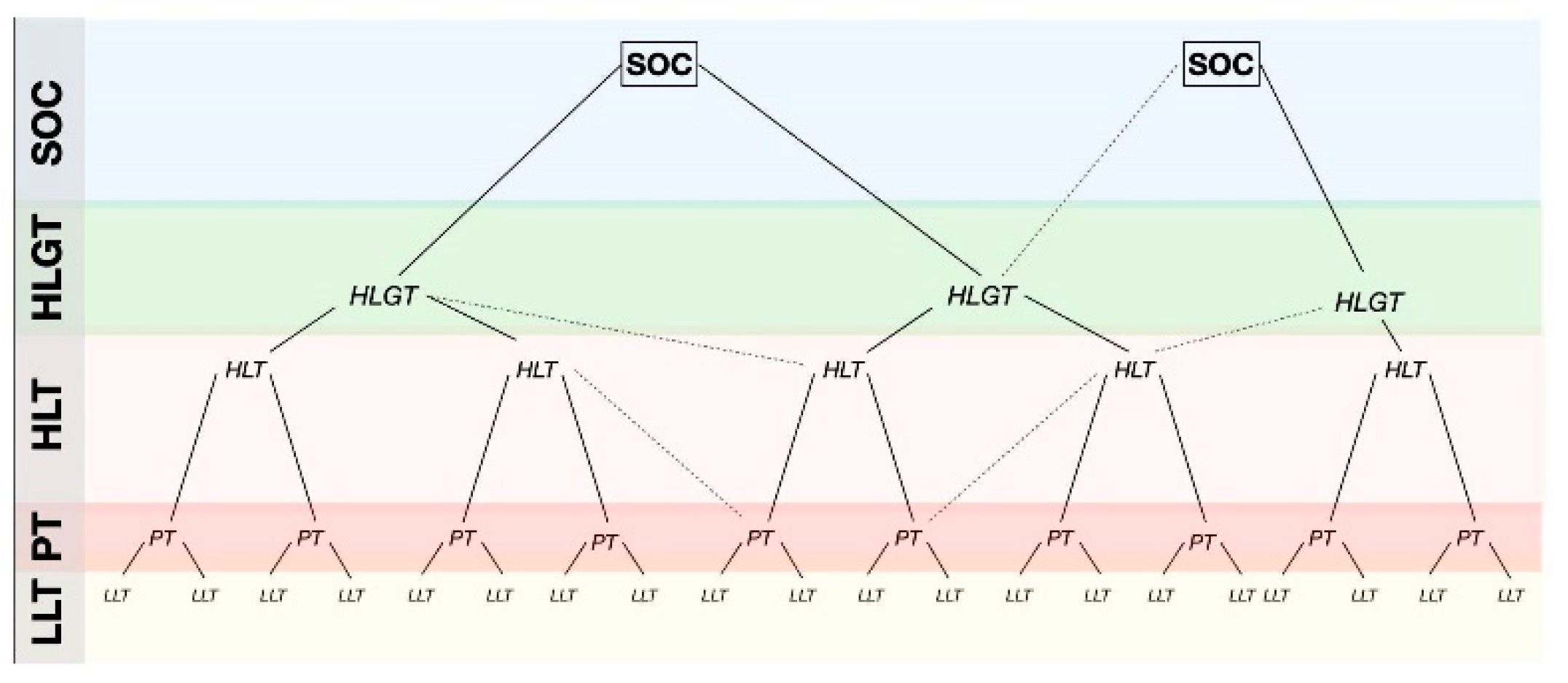

Table 1.
Biological drugs under study.
| Biological Drugs (Date of Approval) |
ATC – GTER Classification | Approved Indications | Brand Name |
|---|---|---|---|
| Omalizumab (10/25/2005) |
R03DX05 -Other systemic drugs for obstructive airway diseases | Allergic asthma convincingly mediated by IgE | Xolair® |
| Mepolizumab (12/02/2015) |
R03DX09 | Severe refractory eosinophilic asthma Chronic rhinosinusitis with nasal polyps Eosinophilic granulomatosis with polyangiitis Hypereosinophilic syndrome |
Nucala® |
| Reslizumab (05/15/2016) |
R03DX08 | Insufficiently controlled severe eosinophilic asthma | Cinqaero® ▼ |
| Benralizumab (02/12/2018) |
R03DX10 | Severe uncontrolled eosinophilic asthma | Fasenra® |
| Tezepelumab (09/19/2022) |
R03DX11 | Severe asthma | Tezspire® ▼ |
| Dupilumab (09/26/2017) |
D11AH -Agents for dermatitis, excluding corticosteroids | Moderate to severe atopic dermatitis Severe uncontrolled eosinophilic asthma Chronic rhinosinusitis with nasal polyps Prurigo nodularis Eosinophilic esophagitis |
Dupixent® |
▼ Medicines under additional monitoring in the European Union.
Table 2.
Origin of cases and seriousness.
| Origin of Cases (n) | Non-Serious n (%) |
Serious* n (%) |
|---|---|---|
| SEFV-H (361) | 154 (43 %) | 207 (57 %) |
| MAH (1,985) | 1,506 (76 %) | 479 (24 %) |
*Seriousness Criteria: A case is considered serious if it accomplished at least one of the following: it causes death (Fatal) ; It endangers the patient's life; Requires admission or prolonged hospital stay; Disability or persistent disability; Congenital anomaly or defect; It has not caused any of the above but is considered clinically or medically significant. SEFV-H: Spanish System of Human Use Medicines Pharmacovigilance; MAH: Marketing Authorization Holders.
Table 3.
Outcome of adverse drug reactions according to the origin of data.
| Unknown | Mortal | Not Recovered | Recovered with after-Effects | In Recovery | Recovered | Origin of Cases (n) |
|---|---|---|---|---|---|---|
| 17 % | 1 % | 16 % | 2 % | 25 % | 40 % | SEFV-H (361) |
| 43 % | 1 % | 22 % | 0,4 % | 8 % | 25 % | MAH (1,985) |
SEFV-H: Spanish System of Human Use Medicines Pharmacovigilance; MAH: Marketing Authorization Holders.
Table 4.
Number of reported cases and seriousness for each active ingredient.
| Biological Drug | FEDRA (n) | Serious* Cases | Males | Females | Warning** Cases |
|---|---|---|---|---|---|
| Omalizumab | 672 | 61% | 27% | 65% | 10,1% |
| Mepolizumab | 497 | 32% | 24% | 66% | 3,6% |
| Reslizumab | 35 | 54% | 17% | 74% | 17% |
| Benralizumab | 588 | 18% | 23% | 75% | 2,2% |
| Tezepelumab | 3 | 33% | 33% | 66% | - |
| Dupilumab | 536 | 29% | 47% | 45% | 5,6% |
*Seriousness Criteria: A case is considered serious if it accomplished at least one of the following: it causes death (Fatal) ; It endangers the patient's life; Requires admission or prolonged hospital stay; Disability or persistent disability; Congenital anomaly or defect; It has not caused any of the above but is considered clinically or medically significant. ** Warning cases: Cases that contain unknown adverse reactions (not included in the SmPC) and that due to their severity are likely to generate a Pharmacovigilance Signal.
Table 5.
Adverse drug reactions currently described in the Summary of Product Characteristics.
| Symptoms grouping | Omalizumab | Mepolizumab | Reslizumab | Benralizumab | Tezepelumab | Dupilumab |
|---|---|---|---|---|---|---|
| Blood and lymphatic system disorders | Idiopathic thrombocytopenia | Eosinophilia | ||||
| Eye disorders | Allergic conjunctivitis. Keratitis Blepharitis Eye pruritus Dry eye Ulcerative keratitis |
|||||
| Gastrointestinal disorders | Upper abdominal pain | Upper abdominal pain | ||||
| General disorders and administration site conditions | Pyrexia Injection site reactions: swelling erythema, pain, and pruritus Influenza-like illness Swelling arms Weight increase Fatigue |
Pyrexia Injection site reactions Systemic non allergic administration- related reactions |
Pyrexia Injection site reactions |
Injection site reactions |
Injection site reactions: swelling, oedema, erythema, pain, hematoma, and pruritus |
|
| Immune system disorders | Anaphylactic reaction and other serious allergic conditions. Anti-omalizumab antibody development Serum sickness, may include fever lymphadenopathy |
Anaphylactic reaction and other serious allergic conditions |
Anaphylactic reaction | Anaphylactic reaction Hypersensitivity reactions |
Anaphylactic reaction and other serious allergic conditions | Anaphylactic reaction Angioedema Serum sickness |
| Infections and infestations | Pharyngitis Parasitic infection |
Pharyngitis Lower respiratory tract infection Urinary tract infections |
Pharyngitis | Pharyngitis | Conjunctivitis Oral herpes |
|
| Investigations | Blood creatine phosphokinase increased | |||||
| Musculoskeletal and connective tissue disorders | Myalgia Arthralgia Joint swelling Systemic lupus erythematosus |
Myalgia Back pain |
Myalgia |
Arthralgia |
Arthralgia |
|
| Nervous system disorders | Headache Syncope Paresthesia Somnolence Dizziness |
Headache | Headache | |||
| Respiratory, thoracic, and mediastinal disorders | Allergic bronchospasm Coughing Laryngoedema Allergic granulomatous vasculitis |
Nasal congestion | ||||
| Skin and subcutaneous tissue disorders | Photosensitivity Urticaria, Rash Pruritus Alopecia |
Eczema, Rash |
Rash |
Rash |
||
| Vascular disorders | Flushing Postural hypotension |
Flushing |
Table 6.
Reported ADRs not collected in SmPC. Bold characters reflect disproportionally reported data, indicating statistically significant associations.
Table 6.
Reported ADRs not collected in SmPC. Bold characters reflect disproportionally reported data, indicating statistically significant associations.
| Omalizumab | Mepolizumab | Reslizumab | Benralizumab | Dupilumab | |
|---|---|---|---|---|---|
| Blood and lymphatic system disorders | Anemic disorders Lymphadenopathy |
Lymphadenopathy |
|||
| Cardiac disorders |
Acute myocardial infarction Pericarditis |
Ischemic coronary artery disorders | |||
| Ear and labyrinth disorders |
Deafness Deafness. neurosensory |
||||
| Eye disorders | Eyelid oedema | ||||
| Gastrointestinal disorders | Abdominal pain or discomfort | Vomiting and nausea Diarrhea Crohn's disease |
|||
| General disorders and administration site conditions | Asthenic conditions |
|
Asthenia or Fatigue | Asthenia or Fatigue Pyrexia Malaise |
|
| Immune system disorders |
Multiple Sclerosis Sjögren Syndrome |
||||
| Infections and infestations |
Herpes viral infect. Lung and lower resp. tract infection |
Herpes viral infect* |
Pneumonia |
Infective Pneumonia Cellulitis |
|
| Metabolism and nutrition disorders | Decreased appetite Decreased weight |
Decreased appetite Decreased weight |
|||
| Musculoskeletal and connective tissue disorders | Back pain Muscular weakness Muscle spasms Musculoskeletal stiffness |
Arthralgia* |
Arthralgia |
Arthralgia Myalgia Muscle spasms |
Myalgia Bone pain Limb pain |
| Neoplasms benign, malignant, and unspecified (incl cysts and polyps) |
Breast and nipple neoplasm malignant Lymphomas unspecified Colorectal neoplasm malignant Respiratory tract neoplasm malignant cell type unspecified. |
Breast and nipple neoplasm malignant Breast cancer male Malignant neo.GI NEC Respiratory tract neoplasm malignant cell type unspecified. |
Glial tumors malignant |
Malignant neo.GI NEC Malignant Respiratory neoplasm |
|
| Nervous system disorders |
Vascular disorders CNS Gait disturbance, Gait inability, Mobility decreased and Hypokinesia Optic neuritis |
Cerebrovascular accident Paraesthesias, Dysaesthesias Hypoaesthesias Tremor |
Headaches Dizziness Syncope |
||
| Pregnancy, puerperium, and perinatal conditions | Abortion spontaneous | ||||
| Psychiatric disorders | Anxiety | Sleep disorders | Anxiety, Stress and Nervousness | ||
| Reproductive system and breast disorders | Menstrual cycle disorders | . | |||
| Respiratory, thoracic, and mediastinal disorders | Pulmonary embolism and thrombosis | Pulmonary embolism and thrombosis | Pulmonary embolism and thrombosis | Eosinophilic Pneumonia |
|
| Skin and subcutaneous tissue disorders |
Atopic dermatitis Purpura Hyperhidrosis |
Alopecia |
Alopecia | Alopecia | Alopecia |
| Vascular disorders | Deep Vein Thrombosis | Deep Vein Thrombosis | Hypertension Hypotension |
Vasculitis |
* The EMA Pharmacovigilance Committee (PRAC) of April 2024 has already included these adverse drug reactions in the side effects section of the summary of product of mepolizumab.
Table 7.
Value of the disproportion of reporting for each of the associations drug-ADR signaled as statistically significant.
Table 7.
Value of the disproportion of reporting for each of the associations drug-ADR signaled as statistically significant.
| Association | N | Lower Limit ROR* | Lower Limit CI^ | X2` |
|---|---|---|---|---|
| Omalizumab-Acute myocardial infarction (PT: acute myocardial infarction, acute coronary syndrome, Kounis´ syndrome) |
6 | 1.48 | 0.23 | 9.25 |
| Omalizumab-Angina pectoris (PT) | 4 | 2.97 | 0.45 | 23.05 |
| Omalizumab-Pericarditis (PT: pericarditis; pleuropericarditis) | 4 | 2.86 | 0.43 | 21.95 |
| Omalizumab-Deafness (PT: deafness; neurosensorial deafness) | 4 | 3.69 | 0.54 | 30.19 |
| Omalizumab-Multiple Sclerosis (PT) | 3 | 2.75 | 0.13 | 18.45 |
| Omalizumab-Sjögren Syndrome (PT) | 3 | 15.15 | 0.42 | 122.99 |
| Omalizumab-Optic Neuritis (PT) | 3 | 3.28 | 0.19 | 22.95 |
| Omalizumab-Herpes viral infection (PT: oral herpes, herpes zoster, eczema herpeticum, herpes virus infections.) |
8 | 1.10 | 0.00 | 5.7 |
| Omalizumab-Muscular weakness; Back pain; Muscle spasms; Joint stiffness. (PTs) | 18 | 1.11 | 0.09 | 5.85 |
| Omalizumab-Breast and nipple neoplasm malignant (PTs: hormone receptor-positive breast cancer, breast cancer, invasive lobular breast carcinoma, invasive breast carcinoma, invasive ductal breast cancer) |
16 |
23.33 | 2.84 | 540.78 |
| Omalizumab-Colon cancer (PT) | 7 | 12.49 | 1.62 | 162.52 |
| Omalizumab-Lymphoma (PT) | 4 | 1.64 | 0.10 | 9.78 |
| Omalizumab-Lung adenocarcinoma, Lung malignant neoplasm (PTs) | 7 | 8.27 | 1.48 | 104.16 |
| Omalizumab-Cerebrovascular accident, Ischemic stroke, Transient ischemic attack (PTs) | 8 | 2.48 | 0.82 | 24.74 |
| Omalizumab-Gait disturbance, Gait inability, Mobility decreased and Hypokinesia (PTs) | 8 | 1.44 | 0.29 | 9.54 |
| Omalizumab-Abortion spontaneous, gestational fetal death (PTs) | 8 | 4.05 | 1.21 | 48.52 |
| Omalizumab-Atopic dermatitis (PT) | 4 | 8.06 | 0.77 | 73.97 |
| Omalizumab-Deep Vein Thrombosis (PT) | 5 | 1.47 | 0.14 | 8.71 |
| Omalizumab-Embolic and thrombotic events (SMQ) | 25 | 1.51 | 0.50 | 16.69 |
| Mepolizumab-Arthralgia (PT)** | 27 | 2.22 | 0.95 | 39.15 |
| Mepolizumab-Herpes zoster (PT)** | 6 | 2.42 | 0.63 | 20.81 |
| Mepolizumab-Breast and nipple neoplasm. malignant (HLT) Breast malignant tumors (SMQ) |
3 | 5.36 | 0.32 | 40.85 |
| Mepolizumab-Gastrointestinal neoplasms malignant and unspecified (HLGT) | 4 | 5.41 | 0.67 | 47.55 |
| Mepolizumab-Respiratory and mediastinal neoplasms malignant and unspecified (HLGT) | 3 | 5.98 | 0.34 | 46.21 |
| Mepolizumab-Malignancies (SMQ) | 16 | 2.86 | 1.19 | 44.32 |
| Mepolizumab-Alopecia (PT) | 8 | 3.88 | 1.17 | 45.66 |
| Reslizumab-Arthralgia (PT) | 10 | 6.28 | 1.42 | 77.96 |
| Benralizumab-Alopecia (PT) | 4 | 2.68 | 0.38 | 20.05 |
| Dupilumab-Crohn's disease (PT) | 3 | 3.67 | 0.22 | 26.23 |
| Dupilumab-Infective Pneumonia (SMQ) [excluded COVID-19] | 7 | 1.92 | 0.52 | 15.47 |
| Dupilumab-Bone pain (PT) | 4 | 2.02 | 0.23 | 13.52 |
| Dupilumab-Alopecia (PT) | 15 | 5.00 | 1.76 | 92.92 |
*The Reporting Odds Ratio (ROR) must be above 1 to have statistical significance. ^The Information Component (CI) must be above 0 to have statistical significance. ‘The Chi-Square (X2) has no interval limits and gives information about the strength of the association (the higher the value, the higher the strength). Above 4 it´s considered to be statistically significant, sustaining the association. ** The EMA Pharmacovigilance Committee (PRAC) of April 2024 has already included this ADR in the Side Effects section of the FT of Mepolizumab. SMQ: Standardized MedDRA Queries. PT: Preferred Terms. HLGT: High-Level Group Term. HLT: High Level Term.
Table 8.
Variations regarding arthralgia and myalgia in the summary of product characteristics.
| Present in SmPC | Present in Reports | |||
|---|---|---|---|---|
| Omalizumab | Arthralgia | Myalgia | Arthralgia | Myalgia |
| Mepolizumab | Arthralgia | Myalgia | Arthralgia | Myalgia |
| Dupilumab | Arthralgia | Arthralgia | Myalgia | |
| Tezepelumab | Arthralgia | Arthralgia | Myalgia | |
| Reslizumab | Myalgia | Arthralgia | Myalgia | |
| Benralizumab | Arthralgia | Myalgia | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



