
Submitted:
07 April 2024
Posted:
08 April 2024
You are already at the latest version
Abstract
BK polyomavirus (BKPyV) is still a real threat in the management of kidney transplantation. Immunosuppressive treatment disrupts the equilibrium between virus replication and immune response, and uncontrolled BKPyV replication leads to nephropathy (BKPyV nephropathy). The first evidence of BKPyV reactivation in transplant recipients is the detection of viral shedding in urine, which appears in 20% to 60% of patients, followed by BKPyV viremia in 10-20% of kidney transplant recipients. BKPyV nephropathy eventually occurs in 1-10% of this population, mainly within the first 2 years post-transplantation, causing graft loss in about half of those patients. Few data exist regarding the pediatric population and we focus on them.
In this paper, we review the existing diagnostic methods, we summarize the evidences on the role of BKPyV humoral and cellular immunity in the modulation of the clinical course of BKPyV infection and as potential predictors of the outcome. We look at the known risk factors of BKPyV nephropathy in the immunosuppressed patient. Finally, we propose a sensible clinical attitude in order to screen and manage BKPyV infection in kidney transplant children.
Keywords:
BK polyomavirus
; BKPyV nephropathy
; kidney transplantation
1. Introduction
The Polyomaviridae is a family of small, non-enveloped viruses with circular dsDNA genomes of approximately 5 kbp. This family includes four genera whose members have restricted host range, infecting almost exclusively mammals and birds [1]. The first polyomavirus was identified in 1953 as filterable tumor-causing agent in mice, followed by Simian vacuolating virus (SV40) isolated from rhesus monkey kidney cells that had been used for poliovirus vaccine preparation in the sixties [2]. The first two human polyomavirus species, both named after the index case patients, were identified in 1971 independently in two different patients. BK polyomavirus (BKPyV) was isolated from a urine sample of a renal transplant patient [3] and JC virus was isolated from the brain tissue of a patient with progressive multifocal leukoencephalopathy [4]. BK and JC viruses have been the only well-known human polyomaviruses for decades. However, more than 50 years of research have provided crucial insights into the cellular and molecular biology of these viruses, and up to now at least 13 human polyomavirus species have been identified [1,5].
2. Pathogenesis
Primary BKPyV infection is mainly acquired early in life and is most likely transmitted horizontally by direct contact, by aerosol or fecal–oral routes [6]. Approximately 80% of the general population has detectable antibodies to BKPyV, which appear at a point in childhood and persist throughout life [7]. The mechanisms of persistence and reactivation of the virus remain poorly understood. The BKPyV is believed to firstly replicate in the respiratory tract and then to spread to other organs through the bloodstream, notably in renal tubular epithelial and urothelial cells [8]. BKPyV remains clinically latent in immunocompetent hosts, but after kidney transplantation, immunosuppressive treatment disrupts the equilibrium between virus replication and immune response resulting in potentially severe clinical complications.
3. Kidney Graft Involvement
Uncontrolled BKPyV replication leads to nephropathy (BKPyV nephropathy) which continues to be a real threat in the management of kidney transplantation. The first evidence of BKPyV reactivation in kidney transplant recipients is the detection of viral shedding in urine, which appears in 20% to 60% of patients [9]. BKPyV viremia may follow the replication in urine, and it is detected in 10-20% of kidney transplant recipients. BKPyV nephropathy occurs in 1-10% of renal allograft recipients, mainly within the first 2 years post-transplantation, causing graft loss in about half of those patients [10,11].
Virological and immunological determinants of the progression from self-limited BKPyV viruria or viremia to BKPyV nephropathy in kidney transplant recipients are poorly understood and the source of BKPyV could be either the urinary tract of the donor or the recipient, although both sources may not be mutually exclusive [12,13,14].
4. Immune Response
4.1. Humoral Immune Response
The role of BKPyV humoral immunity in the modulation of the clinical course of BKPyV infection is still debated. In 1983, Rosen et al. have reported a severe case of end-stage-renal-disease due to a BKPyV infection in a six-year-old immunocompromised boy with congenital dysgammaglobulinemia [15]. Renal biopsy at the time of his presentation revealed tubulo-interstitial lesions with mononuclear infiltrates and numerous BKPyV inclusions. A hypothesis raised that the humoral immune deficiency was responsible for the severity of the BKPyV infection in this child.
Pre-transplant serologies for cytomegalovirus and Epstein–Barr virus in donor and recipient are now performed routinely with the aim to estimate the risk of infection and to plan the prophylactic treatment. Similarly, could pre-transplant serology for BKPyV be used as a screening tool to evaluate the individual risk for BKPyV infection?
Serotypes I and IV represent more than 90% of strains found in kidney transplant patients. Studies have suggested that high BKPyV-specific antibody titers against the donor strain before transplantation might have a protective role. Wunderink et al. found that higher level of serotype I antibodies before transplantation was strongly correlated with a lower risk of BKPyV infection [16]. A study by Solis et al. in 2018 revealed the key role of the anti-BKPyV genotype–specific neutralizing antibody titers in protecting against BKPyV infection [17]. Recently, Dakroub et al. used a commercial antibody for enzyme-linked immunosorbent assay (ELISA) in order to assess the BKPyV serostatus of 329 adult kidney transplant recipients and 222 matched donors [18]. Their results showed a higher risk of developing post-transplantation BKPyV viremia in the R-/D+ group.
4.2. Cellular Immune Response
Already 40 years ago, Drummond and al showed that BKPyV-specific cell-mediated immune response was the main mechanism in controlling viral replication [24]. This finding was further supported by a study on the cellular immune response to JC virus in patients with progressive multifocal leuko encephalopathy. In those patients, JC virus-specific cytotoxic T lymphocytes were found to be a key factor in containing the disease [25].
Impairment of cell-mediated immune response allows the BKPyV reactivation, which begins with the active viral replication in the graft, followed by viral shedding in the urine, and eventually viremia, nephropathy and, in the worst-case scenario, graft loss [21,26]. In kidney transplant recipients low levels of BKPyV-specific interferon gamma-producing T cells correlate with progression to BKPyV nephropathy [27].
Currently the plasma BKPyV-DNA load is used after kidney transplantation to identify patients at risk of BKPyV nephropathy. However, some authors advocate that the BKPyV viremia alone is not an accurate predictor of the clinical outcome and that more reliable parameters are needed to distinguish patients with self-limiting viremia from those with higher risk of BKPyV nephropathy [28]. Therefore, monitoring pre- and post-transplant BKPyV-specific T cells was suggested as a potential accurate marker to identify those kidney transplant recipients at increased risk.
Data on children are very scarce. As for the adult population, in a recent pediatric study high levels of BKPyV-specific CD4 and/or CD8 T-cells were found in cases of self-limiting viremia, whereas lack or low levels of BKPyV-specific T cells were associated with long-term viremia and florid BKPyV nephropathy [29].
5. Diagnosis
5.1. Urine Cytology
Decoy cells are characterized by a ground-glass appearance with intra-nuclear inclusions. Their presence in urine has been used for decades as a marker for BKPyV infection, although their predictive value is limited by the high intraobserver variability [10]. Moreover, urine decoy cells are not specific for BKPyV infection, having also been described in adenovirus and cytomegalovirus infections [30]. However, many institutions continue to screen renal transplant recipients through the detection of decoy cells and they measure BKPyV-DNA in the plasma only if decoy cells persist. The main reason is that in many countries the public health system and/or insurance policy's do not cover the cost of PCR testing [31].
5.2. BKPyV Viruria
Urine BKPyV-PCR has been proposed as a more reliable screening tool in renal transplant recipients, as this method could detect the infection at an early stage. Thresholds used for the risk of viremia and BKPyV nephropathy are commonly > 107 copies/mL [32]. Adult data shown that a BKPyV viruria was associated with BKPyV nephropathy in only one third of cases, while no patients with a viruria under this cut-off developed the disease [33]. Therefore, this test is only useful when it is negative, as it makes the diagnosis of BKPyV nephropathy improbable.
Few data concern the pediatric population. In the CERTAIN Registry study, about one quarter of children developed a high level BKPyV viruria within the first post-transplantation year, while only 3% ended with a BKPyV nephropathy [34]. In our ongoing Belgian study on 55 transplanted children between 2010 and 2022, 18% developed a high level BKPyV viruria already within the first 6 months post-tranplantation, while during the same early period, 6% progressed towards a high-level viremia and none to BKPyV nephropathy (Data presented at the 37th congress of the French Pediatric Nephrology Society, Nice 15-17 November 2023).
5.3. BKPyV Viremia
Regular screening for BKPyV replication by plasma viral load is now universally recommended in kidney transplant recipients [35,36]. A recent Belgian study with systematic biopsy and BKPyV-DNA load follow-up has shown a very high negative predictive value (0.989) when the plasma viral load was below 104 copies/mL. Performing a biopsy for confirmation of BKPyV nephropathy is therefore not necessary in cases of low viral load [37].
Conversely, persistent high-level BKPyV viremia, (> 104 copies/mL) is associated with an increased risk of BKPyV nephropathy, and it currently even defines a presumptive BKPyV nephropathy [9,37,38]. Therefore, in this scenario, guidelines universally recommend a reduction of maintenance immunosuppression [38].
As regards as the children population, in the CERTAIN Registry study 14% of patients developed a high-level viremia (presumptive BKPyV nephropathy) within the first year and needed a therapeutic intervention [34]. However, many reports have observed self-limiting BKPyV viremia in kidney recipients without any immunosuppression reduction [38,39,40]. Therefore, in these cases, pre-emptive reduction and/or modification of immunosuppressive drugs could not only be unnecessary but potentially at increased risk of rejection.
5.4. BKPyV-Specific Cell Immune Monitoring
BKPyV-specific cell-mediated immune response has been a recent area of research as BKPyV-specific cellular immunity seems to play an important role in controlling viral replication. Adult and pediatric studies observed that an increase in BKPyV-specific T cells was correlated with the viral clearance in kidney transplant recipients [27,29]. BKPyV-specific cell immune monitoring has been therefore suggested as a prognostic tool to identify patients who are at risk of BKPyV nephropathy [40].
Recently, Ahlenstiel-Grunow and colleagues performed a detailed analysis of the BKPyV-specific cellular immune response in a German cohort of transplanted children at the onset of BKPyV viremia [29]. They found that lack or low levels of BKPyV-specific CD4 and CD8 T cells were associated with an increased risk of persistent viremia, florid BKPyV nephropathy, and the urgent need of a reduction of immunosuppression. Whereas patients with adequate BKPyV-specific CD4 T cells (≥ 0.5 cells/µL) and/or CD8 T cells (≥ 0.1 cells/µL) showed transient, self-limiting viremia without BKPyV-associated complications.
Although the analysis of BKPyV-specific CD4 and CD8 T cells might offer an accurate prognostic tool in order to tailor the level of immunosuppression in kidney transplant recipients, up to now, the price, availability and technical hitches make these tests impractical for use in routine care.
5.5. Allograft Biopsy
Standardized graft biopsy using immunohistochemistry (SV40 T antigen staining or in situ hybridization) remains the gold standard to confirm a BKPyV nephropathy [35,36]. The Banff working group on BKPyV nephropathy classified the disease into 3 grades based on histology to allow comparative analyses and improvement in predicting clinical presentation and outcome [41]. Typical findings are focal interstitial mononuclear inflammatory cell infiltrates, necrotic tubular epithelium, and presence of homogenous intra- nuclear inclusions. Tubular atrophy and interstitial fibrosis remain the most important predictors of poor outcome [42].
In the CERTAIN Registry study, biopsy-proven BKPyV nephropathy was diagnosed in 4.5% of children during a 5-year post-transplantation period [34]. Unlike in adults, more than 20% of these patients developed a BKPyV nephropathy beyond the second year post-transplant [34]. Although current guidelines recommend to screen for BKPyV replication only once per year after the second year post-transplant, these pediatric observations suggest a more vigilant approach.
Negative biopsy results do not necessarily rule out BKPyV nephropathy, as the disease can be focal at start, and sampling errors are always possible [43]. Two cores containing medulla are required for an adequate biopsy sample [36]. Therefore, in patients with a negative kidney biopsy and a BKPyV viremia (> 104 copies/mL) for more than 4 weeks, the diagnosis of “presumptive BKPyV nephropathy” should be retained [35].
6. Risk Factors of BKPyV Nephropathy in the Immunosuppressed Patient
It is widely agreed that the introduction of more potent immunosuppression, both for the induction and the maintenance phase, has increased the risk of BKPyV nephropathy in transplanted kidneys [29,34,44].
6.1. Immunosuppression
Thymoglobuline (ATG): As for the induction therapy, ATG has been clearly incriminated when compared to no induction or induction with IL-2 receptor blockers [9,44].
Tacrolimus (TAC): Results from the large Organ Procurement and Transplantation Network (OPTN) Registry found an association between the TAC-based maintenance regimens and a higher incidence of treatment for BKPyV nephropathy within the first 2 years post-transplantation; and this when compared to cyclosporine (CsA)-based regimens [44]. TAC has also been incriminated in more recent prospective studies on the adult population [45,46].
The pediatric cohort analysis of the United Network for Organ Sharing (UNOS) database on children followed for 5 years post-transplantation, found that TAC therapy at the time of discharge was significantly associated with graft failure due to BKPyV nephropathy as compared to graft failure due to other causes [47]. The CERTAIN Registry study also found that TAC-based immunosuppression was independently associated with presumptive BKPyV nephropathy in transplanted children [34].
Mycophenolate mofetil (MMF): The OPTN registry study found an association between the MMF-based regimen and a higher incidence of treatment for BKPyV nephropathy within the first 2 years post-transplantation when compared to azathioprine-based regimen [44].
Not surprisingly, the combination TAC-MMF has been associated with a particularly higher risk of BKPyV infection [9,44], even in children [34].
Inhibitors of mammalian target of rapamycin (mTORi): Studies have found that mTORi have an antiviral effect without losing their immunosuppressive action against graft rejection [48]. In vitro experiments using BKPyV-infected renal epithelial cell lines, found that sirolimus reduces BKPyV large T-antigen expression and its genome replication by blocking the protein-kinase Akt/mTOR pathway [49,50]. In clinics, an important role of mTORi in decreasing BKPyV infection has been observed [44,51], especially when combined with low-dose calcineurin inhibitors CNI [51,52,53,54,55]. Up to now, no reliable data exist in transplanted children.
6.2. Other Risk Factors
In addition to immunosuppression, other independent risk factors for BKPyV infection have been suggested, mainly recipient characteristics such as male gender [45], young [44] and advanced age [45], obstructive uropathy [34], and prior graft loss due to BKPyV nephropathy [28]. Also specific graft characteristics have been suspected such as organs from BKPyV seropositive donors to seronegative recipients, number of HLA mismatches, ischemic injury and ureteral stent placement at transplantation [19,34].
Transplanted children have an increased risk of developing a BKPyV serious infection. The possible explanation is that those patients have not been previously exposed to the virus, and when immunosuppressed, they acquire a primary and more severe infection [34,44]. On the contrary, the increased rate of BKPyV nephropathy in the elderly is plausible because of the reduction with increasing age in global humoral and cellular immunity to viruses [45]. It is therefore strongly recommended a more frequent surveillance in these two extreme age populations.
7. How to Manage BKPyV in Pediatric Kidney Transplantation
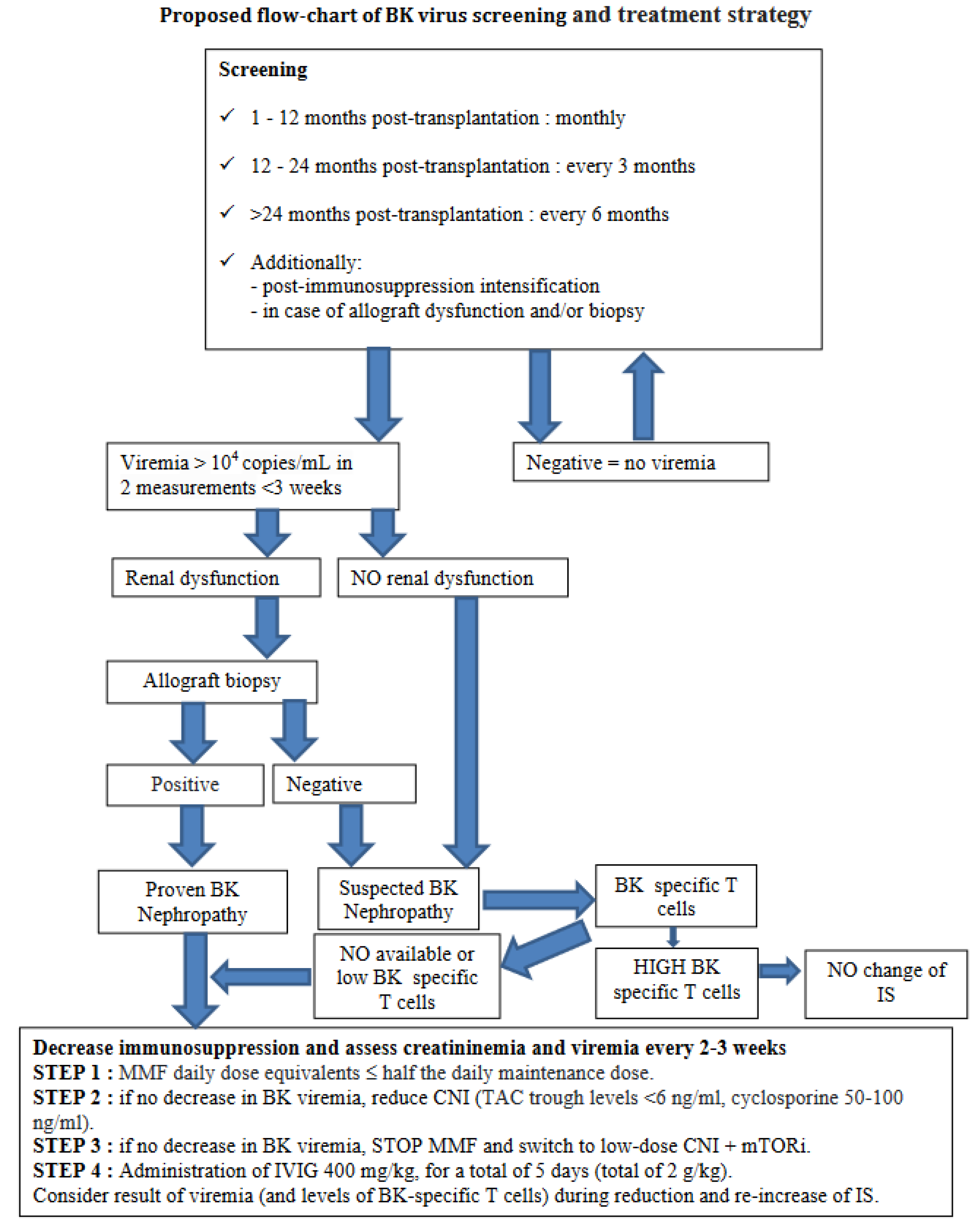
BKPyV screening: Our own experience on 55 transplanted children between 2010 and 2022, showed that 12% of patients progressed towards a high-level viremia (presumptive BKPyV nephropathy) within the first 2 post-transplant years, with 50% of them already affected within the first 6 months and nearly 85% within the first year [Data presented at the 37th congress of the French Pediatric Nephrology Society, Nice 15-17 November 2023].
Therefore, we suggest that kidney transplanted children should be screened for plasma BKPyV-DNA monthly the first year, then every 3 months the second year, and afterward every 6 months.
If BKPyV viremia load is > 103 copies/mL in two measurements at less than 3 weeks of interval, BKPyV load should be monitored for potential infection with frequent plasma sampling, at least every two weeks. If the viremia load is > 104 copies/mL in two measurements, a presumptive BKPyV nephropathy should be considered even in the absence of renal biopsy and the first step of management should be taken [37] (Figure 1).
Immunosuppression management: The first step in the management of presumptive or proven BKPyV nephropathy is reducing maintenance immunosuppression as CNI and/or MMF. TAC trough levels are commonly targeted to <6 ng/ml, cyclosporine to <150 ng/ml, and MMF equal or less than half the daily maintenance dose. During reduction of immunosuppressive therapy, plasma BKPyV-DNA should be tested every 2-3 weeks, as well as the levels of BKPyV-specific T cells when possible.
If necessary, a following step could be switching to mTORi plus low-dose CNI after cessation of MMF [56]. Unfortunately, this aggressive reduction in immunosuppression may inevitably lead to acute rejection and/or graft loss [57].
Adjunctive therapies: In patients with persistent BKPyV nephropathy, despite adequately reduced immunosuppression, the use of adjunctive therapies may be considered [28,35,36]. However, no randomized controlled trials could provide evidence that their use alone or in combination, is superior to the reduction of immunosuppression alone [28].
Intravenous immunoglobulin (IVIG): IVIG could play a broad anti-inflammatory, immunomodulator role or directly neutralize viral activity. Clinical studies showing clearance of plasma BKPyV-DNA following IVIG administration do exist [58], though their real efficacy is difficult to evaluate as other antiviral interventions are always performed concomitantly [28]. IVIG have been administered in doses ranging from 0.1 to 2 g/Kg in conjunction with reduced immunosuppression.
Cidofovir: Cidofovir is a nucleoside analog of cytosine which has an antiviral activity inhibiting the DNA polymerase. Although randomized clinical trials assessing its efficacy are pending, few adult studies did report a stabilization of renal function and/or clearance of viremia [59]. In addition, several side effects have been reported, including nephrotoxicity, myelosuppression, nausea, diarrhea, anterior uveitis [28]. At our best knowledge, no robust pediatric studies have been published up to now [60].
Leflunomide: Leflunomide has unique antiviral and immunosuppressive properties, inhibiting the pyrimidin synthesis and protein kinase activity. It has been orally administered as a replacement for discontinued MMF, with a loading dose of 100 mg for 3 to 5 days, followed by a maintenance dose de 20 to 60 mg daily [61]. Significant toxic effects have been reported, including hepatitis, hemolysis, thrombotic microangiopathy, bone marrow suppression [9,28]. In children, very scarce case reports reporting the efficacy of Leflunomide have been published [62,63].
In order to avoid rejection, return to routine maintenance immunosuppression after successful clearance of BKPyV viremia should be considered under careful monitoring plasma viral loads. In case rejection appears, it should be treated according to standard protocol.
8. Conclusion
Due to limited number of pediatric studies, diagnosis and treatment of BKPyV-infections vary considerably between centers and countries [64]. The vast majority of children are managed according to adult guidelines. We have nevertheless attempted in the following flow-chart to summarize a sensible clinical attitude in order to screen and manage BKPyV infection in kidney transplant children (Figure 1).
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moens U, Calvignac-Spencer S, Lauber C, Ramqvist T, Feltkamp MCW, Daugherty MD, Verschoor EJ, Ehlers B, Ictv Report Consortium. ICTV Virus Taxonomy Profile: Polyomaviridae. J Gen Virol. 2017 Jun;98(6):1159-1160. [CrossRef] [PubMed] [PubMed Central]
- Vilchez RA, Butel JS. Emergent human pathogen simian virus 40 and its role in cancer. Clin Microbiol Rev. 2004 Jul;17(3):495-508, table of contents. [CrossRef] [PubMed] [PubMed Central]
- Gardner SD, Field AM, Coleman DV, Hulme B. New human papovavirus (B.K.) isolated from urine after renal transplantation. Lancet. 1971 Jun 19;1(7712):1253-7. [CrossRef] [PubMed]
- Padgett BL, Walker DL. Prevalence of antibodies in human sera against JC virus, an isolate from a case of progressive multifocal leukoencephalopathy. J Infect Dis. 1973 Apr;127(4):467-70. [CrossRef] [PubMed]
- DeCaprio JA, Garcea RL. A cornucopia of human polyomaviruses. Nat Rev Microbiol. 2013 Apr;11(4):264-76. [CrossRef] [PubMed] [PubMed Central]
- Goudsmit J, Wertheim-van Dillen P, van Strien A, van der Noordaa J. The role of BK virus in acute respiratory tract disease and the presence of BKV DNA in tonsils. J Med Virol. 1982;10(2):91-9. [CrossRef] [PubMed]
- Stolt A, Sasnauskas K, Koskela P, Lehtinen M, Dillner J. Seroepidemiology of the human polyomaviruses. J Gen Virol. 2003 Jun;84(Pt 6):1499-1504. [CrossRef] [PubMed]
- Boldorini R, Veggiani C, Barco D, Monga G. Kidney and urinary tract poyomavirus infection and distribution: molecular biology investigation of 10 consecutive autopsies. Arch Pathol Lab Med. 2005 Jan;129(1):69-73. [CrossRef] [PubMed]
- Sharma R, Tzetzo S, Patel S, Zachariah M, Sharma S, Melendy T. BK Virus in Kidney Transplant: Current Concepts, Recent Advances, and Future Directions. Exp Clin Transplant. 2016 Aug;14(4):377-84. [CrossRef] [PubMed]
- Hirsch HH, Knowles W, Dickenmann M, Passweg J, Klimkait T, Mihatsch MJ, Steiger J. Prospective study of polyomavirus type BK replication and nephropathy in renal-transplant recipients. N Engl J Med. 2002 Aug 15;347(7):488-96. [CrossRef] [PubMed]
- Kuypers DR. Management of polyomavirus-associated nephropathy in renal transplant recipients. Nat Rev Nephrol. 2012 Apr 17;8(7):390-402. [CrossRef] [PubMed]
- Schmitt C, Raggub L, Linnenweber-Held S, Adams O, Schwarz A, Heim A. Donor origin of BKV replication after kidney transplantation. J Clin Virol. 2014 Feb;59(2):120-5. [CrossRef] [PubMed]
- Gras J, Nere ML, Peraldi MN, Bonnet-Madin L, Salmona M, Taupin JL, Desgrandchamps F, Verine J, Brochot E, Amara A, Molina JM, Delaugerre C. BK virus genotypes and humoral response in kidney transplant recipients with BKV associated nephropathy. Transpl Infect Dis. 2023 Apr;25(2):e14012. [CrossRef] [PubMed]
- Mineeva-Sangwo O, Martí-Carreras J, Cleenders E, Kuypers D, Maes P, Andrei G, Naesens M, Snoeck R. Polyomavirus BK Genome Comparison Shows High Genetic Diversity in Kidney Transplant Recipients Three Months after Transplantation. Viruses. 2022 Jul 14;14(7):1533. [CrossRef] [PubMed] [PubMed Central]
- Rosen S, Harmon W, Krensky AM, Edelson PJ, Padgett BL, Grinnell BW, Rubino MJ, Walker DL. Tubulo-interstitial nephritis associated with polyomavirus (BK type) infection. N Engl J Med. 1983 May 19;308(20):1192-6. [CrossRef] [PubMed]
- Wunderink HF, van der Meijden E, van der Blij-de Brouwer CS, Mallat MJ, Haasnoot GW, van Zwet EW, Claas EC, de Fijter JW, Kroes AC, Arnold F, Touzé A, Claas FH, Rotmans JI, Feltkamp MC. Pretransplantation Donor-Recipient Pair Seroreactivity Against BK Polyomavirus Predicts Viremia and Nephropathy After Kidney Transplantation. Am J Transplant. 2017 Jan;17(1):161-172. [CrossRef] [PubMed]
- Solis M, Velay A, Porcher R, Domingo-Calap P, Soulier E, Joly M, Meddeb M, Kack-Kack W, Moulin B, Bahram S, Stoll-Keller F, Barth H, Caillard S, Fafi-Kremer S. Neutralizing Antibody-Mediated Response and Risk of BK Virus-Associated Nephropathy. J Am Soc Nephrol. 2018 Jan;29(1):326-334. [CrossRef] [PubMed] [PubMed Central]
- Dakroub F, Touzé A, Sater FA, Fiore T, Morel V, Tinez C, Helle F, François C, Choukroun G, Presne C, Guillaume N, Duverlie G, Castelain S, Akl H, Brochot E. Impact of pre-graft serology on risk of BKPyV infection post-renal transplantation. Nephrol Dial Transplant. 2022 Mar 25;37(4):781-788. Erratum in: Nephrol Dial Transplant. [CrossRef] [PubMed]
- Hariharan S, Cohen EP, Vasudev B, Orentas R, Viscidi RP, Kakela J, DuChateau B. BK virus-specific antibodies and BKV DNA in renal transplant recipients with BKV nephritis. Am J Transplant. 2005 Nov;5(11):2719-24. [CrossRef] [PubMed]
- Chen Y, Trofe J, Gordon J, Du Pasquier RA, Roy-Chaudhury P, Kuroda MJ, Woodle ES, Khalili K, Koralnik IJ. Interplay of cellular and humoral immune responses against BK virus in kidney transplant recipients with polyomavirus nephropathy. J Virol. 2006 Apr;80(7):3495-505. [CrossRef] [PubMed] [PubMed Central]
- Schachtner T, Stein M, Sefrin A, Babel N, Reinke P. Inflammatory actvation and recovering BKV-specific immunity correlate with self-limited BKV replication after renal transplantation. Transpl Int. 2014 Mr;27(3):290-301. [CrossRef] [PubMed]
- Leboeuf C, Wilk S, Achermann R, Binet I, Golshayan D, Hadaya K, Hirzel C, Hoffmann M, Huynh-Do U, Koller MT, Manuel O, Mueller NJ, Mueller TF, Schaub S, van Delden C, Weissbach FH, Hirsch HH; Swiss Transplant Cohort Study. BK Polyomavirus-Specific 9mer CD8 T Cell Responses Correlate With Clearance of BK Viremia in Kidney Transplant Recipients: First Report From the Swiss Transplant Cohort Study. Am J Transplant. 2017 Oct;17(10):2591-2600. [CrossRef] [PubMed]
- Kaur A, Wilhelm M, Wilk S, Hirsch HH. BK polyomavirus-specific antibody and T-cell responses in kidney transplantation: update. Curr Opin Infect Dis. 2019 Dec;32(6):575-583. [CrossRef] [PubMed]
- Drummond JE, Shah KV, Donnenberg AD. Cell-mediated immune responses to BK virus in normal individuals. J Med Virol. 1985 Nov;17(3):237-47. [CrossRef] [PubMed]
- Koralnik IJ, Du Pasquier RA, Letvin NL. JC virus-specific cytotoxic T lymphocytes in individuals with progressive multifocal leukoencephalopathy. J Virol. 2001 Apr;75(7):3483-7. [CrossRef] [PubMed] [PubMed Central]
- Leung AY, Chan M, Tang SC, Liang R, Kwong YL. Real-time quantitative analysis of polyoma BK viremia and viruria in renal allograft recipients. J Virol Methods. 2002 May;103(1):51-6. [CrossRef] [PubMed]
- Prosser SE, Orentas RJ, Jurgens L, Cohen EP, Hariharan S. Recovery of BK virus large T-antigen-specific cellular immune response correlates with resolution of bk virus nephritis. Transplantation. 2008 Jan 27;85(2):185-92. [CrossRef] [PubMed]
- Ahlenstiel-Grunow T, Pape L. Diagnostics, treatment, and immune response in BK polyomavirus infection after pediatric kidney transplantation. Pediatr Nephrol. 2020 Mar;35(3):375-382. [CrossRef] [PubMed]
- Ahlenstiel-Grunow T, Sester M, Sester U, Hirsch HH, Pape L. BK Polyomavirus-specific T Cells as a Diagnostic and Prognostic Marker for BK Polyomavirus Infections After Pediatric Kidney Transplantation. Transplantation. 2020 Nov;104(11):2393-2402. [CrossRef] [PubMed]
- Fogazzi GB, Cantú M, Saglimbeni L. 'Decoy cells' in the urine due to polyomavirus BK infection: easily seen by phase-contrast microscopy. Nephrol Dial Transplant. 2001 Jul;16(7):1496-8. [CrossRef] [PubMed]
- Yamada Y, Tsuchiya T, Inagaki I, Seishima M, Deguchi T. Prediction of Early BK Virus Infection in Kidney Transplant Recipients by the Number of Cells With Intranuclear Inclusion Bodies (Decoy Cells). Transplant Direct. 2018 Feb 2;4(2):e340. [CrossRef] [PubMed] [PubMed Central]
- Randhawa P, Vats A, Shapiro R. Monitoring for polyomavirus BK And JC in urine: comparison of quantitative polymerase chain reaction with urine cytology. Transplantation. 2005 Apr 27;79(8):984-6. [CrossRef] [PubMed]
- Viscount HB, Eid AJ, Espy MJ, Griffin MD, Thomsen KM, Harmsen WS, Razonable RR, Smith TF. Polyomavirus polymerase chain reaction as a surrogate marker of polyomavirus-associated nephropathy. Transplantation. 2007 Aug 15;84(3):340-5. [CrossRef] [PubMed]
- Höcker B, Schneble L, Murer L, Carraro A, Pape L, Kranz B, Oh J, Zirngibl M, Dello Strologo L, Büscher A, Weber LT, Awan A, Pohl M, Bald M, Printza N, Rusai K, Peruzzi L, Topaloglu R, Fichtner A, Krupka K, Köster L, Bruckner T, Schnitzler P, Hirsch HH, Tönshoff B. Epidemiology of and Risk Factors for BK Polyomavirus Replication and Nephropathy in Pediatric Renal Transplant Recipients: An International CERTAIN Registry Study. Transplantation. 2019 Jun;103(6):1224-1233. [CrossRef] [PubMed]
- Hirsch HH, Babel N, Comoli P, Friman V, Ginevri F, Jardine A, Lautenschlager I, Legendre C, Midtvedt K, Muñoz P, Randhawa P, Rinaldo CH, Wieszek A; ESCMID Study Group of Infection in Compromised Hosts. European perspective on human polyomavirus infection, replication and disease in solid organ transplantation. Clin Microbiol Infect. 2014 Sep;20 Suppl 7:74-88. [CrossRef] [PubMed]
- Hirsch HH, Randhawa PS; AST Infectious Diseases Community of Practice. BK polyomavirus in solid organ transplantation-Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019 Sep;33(9):e13528. [CrossRef] [PubMed]
- Cleenders E, Koshy P, Van Loon E, Lagrou K, Beuselinck K, Andrei G, Crespo M, De Vusser K, Kuypers D, Lerut E, Mertens K, Mineeva-Sangwo O, Randhawa P, Senev A, Snoeck R, Sprangers B, Tinel C, Van Craenenbroeck A, van den Brand J, Van Ranst M, Verbeke G, Coemans M, Naesens M. An observational cohort study of histological screening for BK polyomavirus nephropathy following viral replication in plasma. Kidney Int. 2023 Nov;104(5):1018-1034. [CrossRef] [PubMed]
- Elfadawy N, Flechner SM, Schold JD, Srinivas TR, Poggio E, Fatica R, Avery R, Mossad SB. Transient versus persistent BK viremia and long-term outcomes after kidney and kidney-pancreas transplantation. Clin J Am Soc Nephrol. 2014 Mar;9(3):553-61. [CrossRef] [PubMed] [PubMed Central]
- Alméras C, Foulongne V, Garrigue V, Szwarc I, Vetromile F, Segondy M, Mourad G. Does reduction in immunosuppression in viremic patients prevent BK virus nephropathy in de novo renal transplant recipients? A prospective study. Transplantation. 2008 Apr 27;85(8):1099-104. [CrossRef] [PubMed]
- Schachtner T, Stein M, Babel N, Reinke P. The Loss of BKV-specific Immunity From Pretransplantation to Posttransplantation Identifies Kidney Transplant Recipients at Increased Risk of BKV Replication. Am J Transplant. 2015 Aug;15(8):2159-69. [CrossRef] [PubMed]
- Nickeleit V, Singh HK, Randhawa P, Drachenberg CB, Bhatnagar R, Bracamonte E, Chang A, Chon WJ, Dadhania D, Davis VG, Hopfer H, Mihatsch MJ, Papadimitriou JC, Schaub S, Stokes MB, Tungekar MF, Seshan SV; Banff Working Group on Polyomavirus Nephropathy. The Banff Working Group Classification of Definitive Polyomavirus Nephropathy: Morphologic Definitions and Clinical Correlations. J Am Soc Nephrol. 2018 Feb;29(2):680-693. [CrossRef] [PubMed] [PubMed Central]
- Masutani K, Shapiro R, Basu A, Tan H, Wijkstrom M, Randhawa P. The Banff 2009 Working Proposal for polyomavirus nephropathy: a critical evaluation of its utility as a determinant of clinical outcome. Am J Transplant. 2012 Apr;12(4):907-18. [CrossRef] [PubMed] [PubMed Central]
- Drachenberg CB, Papadimitriou JC, Hirsch HH, Wali R, Crowder C, Nogueira J, Cangro CB, Mendley S, Mian A, Ramos E. Histological patterns of polyomavirus nephropathy: correlation with graft outcome and viral load. Am J Transplant. 2004 Dec;4(12):2082-92. [CrossRef] [PubMed]
- Dharnidharka VR, Cherikh WS, Abbott KC. An OPTN analysis of national registry data on treatment of BK virus allograft nephropathy in the United States. Transplantation. 2009 Apr 15;87(7):1019-26. [CrossRef] [PubMed]
- Gately R, Milanzi E, Lim W, Teixeira-Pinto A, Clayton P, Isbel N, Johnson DW, Hawley C, Campbell S, Wong G. Incidence, Risk Factors, and Outcomes of Kidney Transplant Recipients With BK Polyomavirus-Associated Nephropathy. Kidney Int Rep. 2022 Dec 30;8(3):531-543. [CrossRef] [PubMed] [PubMed Central]
- Hirsch HH, Vincenti F, Friman S, Tuncer M, Citterio F, Wiecek A, Scheuermann EH, Klinger M, Russ G, Pescovitz MD, Prestele H. Polyomavirus BK replication in de novo kidney transplant patients receiving tacrolimus or cyclosporine: a prospective, randomized, multicenter study. Am J Transplant. 2013 Jan;13(1):136-45. [CrossRef] [PubMed] [PubMed Central]
- Patel H, Rodig N, Agrawal N, Cardarelli F. Incidence and risk factors of kidney allograft loss due to BK nephropathy in the pediatric population: A retrospective analysis of the UNOS/OPTN database. Pediatr Transplant. 2021 Aug;25(5):e13927. [CrossRef] [PubMed]
- Ferrer IR, Wagener ME, Robertson JM, Turner AP, Araki K, Ahmed R, Kirk AD, Larsen CP, Ford ML. Cutting edge: Rapamycin augments pathogen-specific but not graft-reactive CD8+ T cell responses. J Immunol. 2010 Aug 15;185(4):2004-8. [CrossRef] [PubMed] [PubMed Central]
- McCabe MT, Low JA, Imperiale MJ, Day ML. Human polyomavirus BKV transcriptionally activates DNA methyltransferase 1 through the pRb/E2F pathway. Oncogene. 2006 May 4;25(19):2727-35. [CrossRef] [PubMed]
- Liacini A, Seamone ME, Muruve DA, Tibbles LA. Anti-BK virus mechanisms of sirolimus and leflunomide alone and in combination: toward a new therapy for BK virus infection. Transplantation. 2010 Dec 27;90(12):1450-7. [CrossRef] [PubMed]
- Jouve T, Rostaing L, Malvezzi P. Place of mTOR inhibitors in management of BKV infection after kidney transplantation. J Nephropathol. 2016 Jan;5(1):1-7. [CrossRef] [PubMed] [PubMed Central]
- Suwelack B, Malyar V, Koch M, Sester M, Sommerer C. The influence of immunosuppressive agents on BK virus risk following kidney transplantation, and implications for choice of regimen. Transplant Rev (Orlando). 2012 Jul;26(3):201-11. [CrossRef] [PubMed]
- Mallat SG, Tanios BY, Itani HS, Lotfi T, McMullan C, Gabardi S, Akl EA, Azzi JR. CMV and BKPyV Infections in Renal Transplant Recipients Receiving an mTOR Inhibitor-Based Regimen Versus a CNI-Based Regimen: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. Clin J Am Soc Nephrol. 2017 Aug 7;12(8):1321-1336. [CrossRef] [PubMed] [PubMed Central]
- Berger SP, Sommerer C, Witzke O, Tedesco H, Chadban S, Mulgaonkar S, Qazi Y, de Fijter JW, Oppenheimer F, Cruzado JM, Watarai Y, Massari P, Legendre C, Citterio F, Henry M, Srinivas TR, Vincenti F, Gutierrez MPH, Marti AM, Bernhardt P, Pascual J; TRANSFORM investigators. Two-year outcomes in de novo renal transplant recipients receiving everolimus-facilitated calcineurin inhibitor reduction regimen from the TRANSFORM study. Am J Transplant. 2019 Nov;19(11):3018-3034. [CrossRef] [PubMed]
- Moscarelli L, Caroti L, Antognoli G, Zanazzi M, Di Maria L, Carta P, Minetti E. Everolimus leads to a lower risk of BKV viremia than mycophenolic acid in de novo renal transplantation patients: a single-center experience. Clin Transplant. 2013 Jul-Aug;27(4):546-54. [CrossRef] [PubMed]
- Yilmaz VT, Kisaoglu A, Avanaz A, Dandin O, Ozel D, Mutlu D, Akkaya B, Aydinli B, Kocak H. Predictive Factors of BK Virus Development in Kidney Transplant Recipients and the Effect of Low-Dose Tacrolimus Plus Everolimus on Clinical Outcomes. Exp Clin Transplant. 2023 Sep;21(9):727-734. [CrossRef] [PubMed]
- Karatas M, Tatar E, Okut G, Yildirim AM, Kocabas E, Tasli Alkan F, Simsek C, Dogan SM, Uslu A. Efficacy of mTOR Inhibitors and Intravenous Immunoglobulin for Treatment of Polyoma BK Nephropathy in Kidney Transplant Recipients: A Biopsy-Proven Study. Exp Clin Transplant. 2024 Jan;22(Suppl 1):118-127. [CrossRef] [PubMed]
- Sener A, House AA, Jevnikar AM, Boudville N, McAlister VC, Muirhead N, Rehman F, Luke PP. Intravenous immunoglobulin as a treatment for BK virus associated nephropathy: one-year follow-up of renal allograft recipients. Transplantation. 2006 Jan 15;81(1):117-20. [CrossRef] [PubMed]
- Wu SW, Chang HR, Lian JD. The effect of low-dose cidofovir on the long-term outcome of polyomavirus-associated nephropathy in renal transplant recipients. Nephrol Dial Transplant. 2009 Mar;24(3):1034-8. [CrossRef] [PubMed]
- Aksoy G, Erkan M, Koyun M, Çomak E, Toru HS, Mutlu D, Akkaya B, Akman S. Treatment of BK Polyomavirus-Associated Nephropathy in Paediatric Kidney Transplant Recipients: Leflunomide Versus Cidofovir. Exp Clin Transplant. 2024 Jan;22(1):29-34. [CrossRef] [PubMed]
- Faguer S, Hirsch HH, Kamar N, Guilbeau-Frugier C, Ribes D, Guitard J, Esposito L, Cointault O, Modesto A, Lavit M, Mengelle C, Rostaing L. Leflunomide treatment for polyomavirus BK-associated nephropathy after kidney transplantation. Transpl Int. 2007 Nov;20(11):962-9. [CrossRef] [PubMed]
- Jung YH, Moon KC, Ha JW, Kim SJ, Ha IS, Cheong HI, Kang HG. Leflunomide therapy for BK virus allograft nephropathy after pediatric kidney transplantation. Pediatr Transplant. 2013 Mar;17(2):E50-4. [CrossRef] [PubMed]
- Araya CE, Garin EH, Neiberger RE, Dharnidharka VR. Leflunomide therapy for BK virus allograft nephropathy in pediatric and young adult kidney transplant recipients. Pediatr Transplant. 2010 Feb;14(1):145-50. [CrossRef] [PubMed]
- Pape L, Tönshoff B, Hirsch HH; Members of the Working Group ‘Transplantation’ of the European Society for Paediatric Nephrology. Perception, diagnosis and management of BK polyomavirus replication and disease in paediatric kidney transplant recipients in Europe. Nephrol Dial Transplant. 2016 May;31(5):842-7. [CrossRef] [PubMed]
Figure 1.
Proposed flow-chart of BK virus screening and treatment strategy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



