Submitted:
02 April 2024
Posted:
03 April 2024
Read the latest preprint version here
Abstract
Background and Objectives:
Medulloblastoma is the most common malignant brain tumor in children. In recent decades, the therapeutic landscape has undergone significant changes, with stereotactic radiosurgery (SRS) emerging as a promising treatment for recurrent cases. Our study provides a comprehensive analysis of the long-term efficacy and safety of SRS in recurrent medulloblastomas across both pediatric and adult patients at a single institution.
Methods:
We retrospectively reviewed the clinical and radiological records of patients who underwent CyberKnife SRS for recurrent cranial medulloblastomas at our institution between 1998 and 2023. Follow-up data were available for 15 medulloblastomas in 10 patients. The cohort comprised 8 pediatric patients (ages 3-18) and 2 adult patients (ages 19-75). Median age at the time of SRS was 13 years, median tumor volume accounted for 1.9 cc, median biologically equivalent dose (BED) was 126 Gy, and single-fraction equivalent dose (SFED) was 18 Gy. The SRS was administered at 75% of the median isodose line.
Results:
Following a median follow-up of 39 months (range: 6-78), 53.3% of the medulloblastomas progressed, 13.3% regressed, and 33.3% remained stable. The 3-year local tumor control (LTC) rate for all medulloblastomas was 65%, with lower rates observed in the adult cohort (50%) and higher rates in pediatric patients (67%). The 3-year overall survival (OS) rate was 70%, with significantly higher rates in pediatric patients (75%) compared to adult patients (50%). The 3-year progression-free survival (PFS) rate was 58.3%, with higher rates in pediatric patients (60%) compared to adult patients (50%). Two pediatric patients developed radiation-induced edema, while two adult patients experienced radiation necrosis at the latest follow-up, with both adult patients passing away.
Conclusion:
Our study provides a complex perspective on the efficacy and safety of CyberKnife SRS in treating recurrent cranial medulloblastomas across pediatric and adult populations. The rarity of adverse radiation events (ARE) underscores the safety profile of SRS, reinforcing its role in enhancing treatment outcomes. The intricacies of symptomatic outcomes, intertwined with factors such as age, tumor location, and prior surgeries, emphasize the need for personalized treatment approaches. Our findings underscore the imperative for ongoing research and the development of more refined treatment strategies for recurrent medulloblastomas. Given the observed disparities in treatment outcomes, a more meticulous tailoring of treatment approaches becomes crucial.
Keywords:
Stereotactic radiosurgery
; CyberKnife Radiosurgery
; Medulloblastoma
1. Introduction
First described in 1925, medulloblastoma remains as a significant malignant brain neoplasm predominantly affecting the pediatric population [1]. Manifesting with a peak age of diagnosis between 6 to 8 years, the traditional therapeutic triad of surgery, chemotherapy (CT) and radiation therapy (RT) has been the mainstay[2,3]. Notably, recent decades have ushered substantial transformations in therapeutic strategies, marked by an enhanced understanding of molecular subgroups influencing both prognosis and treatment modalities [4]. Despite these strides, the absence of clear guidelines for managing recurrent cases underscores the persistent clinical challenges, especially given the aggressive nature of recurrent medulloblastoma [5].
The intricate interplay between the infiltrative nature of medulloblastoma and the intricacies of neural architecture demands precise and efficacious therapeutic strategies [6]. Within this context, stereotactic radiosurgery (SRS) has emerged as a focal point in the management of recurrent medulloblastoma [7]. Leveraging targeted ionizing radiation, SRS strategically engages the biological vulnerabilities of the pathology. Bolstered by advancements in radiological imaging, radiation delivery platforms, and an evolving comprehension of radiobiology, SRS has assumed a pivotal role in combating this challenging adversary[8,9].
In our study, we demonstrate the efficacy and safety of SRS over the long term, specifically for both pediatric and adult patients grappling with the formidable burden of recurrent medulloblastoma. Situated within a single institution, our investigation uniquely integrates clinical expertise with research acumen, providing a nuanced perspective on the multifaceted dimensions of SRS application in the context of the recurrent nature of medulloblastoma.
2. Methods
Patient Selection and Characteristics
Between 1998 and 2023, we identified and treated 15 cases of recurrent medulloblastomas in 10 patients at Stanford University Medical Center using CyberKnife SRS. The selection criteria included a minimum follow-up period of 6 months. Clinical data were stored in a database approved by the Institutional Review Board (IRB) and complied with the Helsinki Declaration. The detailed overview of the patient demographics is presented in Table 1.
The study cohort comprised 8 (80%) pediatric patients (ages 3-18) and 2 (20%) adult patients (ages 19-75). The median age at the time of SRS was 13 years, with the pediatric group having a median age of 12 years (range: 9-16) and the adult group with a median age of 27 years (range: 25-29). Nine (90%) patients underwent prior surgery prior to SRS, with histological confirmation of WHO grade IV recurrent medulloblastomas. Additionally, one (10%) adult patient received RT as primary treatment based on radiographic diagnosis. Symptoms were correlated with lesion location and included headaches, ataxia, nausea, vomiting, seizures, visual impairment, and motor impairment (Table 1).
Tumor Characteristics
The overall study included 10 patients with 15 recurrent cranial medulloblastomas. The median tumor volume was 1.9 cc (mean: 2.7; range: 0.02-8.7); with the pediatric group having a median of 1.9 cc (range: 0.02-8.7) and the adult group having 1.5 cc (range: 0.5-2.5). Most lesions (86.7%) occurred in pediatric patients, primarily located in the cerebellum (n = 5, 33.3%), followed by ventricular (n=2, 13.3%), parietal (n=2, 13.3%), and frontal (n=2, 13.3%) regions (Table 1).
Treatment
Cranial recurrent medulloblastomas were treated with CyberKnife SRS (Accuray, Inc., Sunnyvale, CA) utilizing the established method previously outlined by Shi et al. [10]. The median time between initial diagnosis and SRS was 30 months (range: 12-108); 39 months (range: 12-108) in the pediatric group and 24.5 months (range: 24-25) in the adult group. SRS was administered with a median single-fraction equivalent dose (SFED) of 18 Gy to the 75% median isodose line (range: 65-81). Marginal dose, maximum dose, isodose line, and the number of fractions did not significantly differ between cohorts (Table 2).
Biologically Effective Dose (BED), Single-Fraction Equivalent Dose (SFED), and Equivalent Total Doses in 2-Gy Fractions (EQD2)
The biologically effective dose (BED) was calculated using the linear-quadratic (LQ) model with a α/β ratio of 3 Gy[11,12]. The BED was converted to SFED and the equivalent total doses in 2-Gy fractions (EQD2) using LQ model [13]. Median BED, SFED, and EQD2 for the entire cohort were 126 Gy (range: 66.7-153.3), 18 Gy (range: 12.7-20), and 75.6 Gy (range: 40-92), respectively, with no significant differences observed between groups (Table 2).
Follow-up
Patients underwent clinical evaluation and MRI follow-up semi-annually for the first two years after SRS, followed by annual assessments. Tumor volume was measured in axial, sagittal, and coronal planes and analyzed using Kaplan-Meier analysis. Graphical representations were generated using standard statistical software (IBM SPSS Statistics 29.0, Chicago, IL).
3. Results:
Patient Demographics and Characteristics
Following the exclusion of patients lost to follow-up, 15 lesions in 10 patients were included in the study. The cohort consisted of 8 (80%) were pediatric and 2 (20%) adult patients, while 5 (50%) patients succumbed during the evaluation period. The median follow-up after SRS was 39 months (range: 6-78) (Table 2).
Local Tumor Control
Among the 15 recurrent medulloblastomas, 8 (53.3%) demonstrated progression, 2 (13.3%) exhibited radiographic regression, and 5 (33.3%) remained stable. LTC rates for all medulloblastomas were 86%, 65%, and 31% at 1, 3, and 5 years, with a higher rate observed in pediatric patients (67%) at 3 years compared to the adult cohort (50%) (Table 3, Figure 1A).
Analysis of LTC rates revealed interesting patterns related to the location of tumors. Cerebellar lesions demonstrated a favorable response with a 78% LTC rate at 3 years compared to 50% for ventricular lesions. Furthermore LTC rates correlated with the number of prior surgeries, with a higher rate in patients who had undergone a single surgery (75%) compared to those with multiple surgeries (66.7%) (Table 1 and Table 3).
Patient Survival
Progression-Free Survival
PFS rates were 90%, 58%, and 29% for all patients at 1, 3, and 5 years, with a higher rate observed in the pediatric cohort at 3 years (60%) (Table 3, Figure 1C).
PFS was notably influenced by the age at treatment, with pediatric patients experiencing a 60% PFS rate at 3 years compared to 50% in adults. Additionally, a positive correlation was observed between PFS and target tumor volume, with larger volumes exhibiting a slightly higher PFS rate (Table 2 and Table 3).
Symptomatic Outcome
In the entire cohort, one (10%) pediatric patient was asymptomatic, allowing the evaluation of symptomatic outcomes for 9 (90%) patients with 14 (93.3%) symptomatic medulloblastomas. Overall, 7 (77.8%) patients demonstrated symptomatic improvements following SRS (Table 3). Notably, symptomatic improvement was more significant in the pediatric cohort (75%) compared to the adult cohort (50%) (p=0.05). The improvements were observed in headaches, nausea, vomiting, ataxia, and visual impairment. However, one (12.5%) pediatric patient and one (50%) adult patient experienced worsening headaches, and one (50%) adult patient presented with new symptoms, including dizziness and vomiting after treatment with SRS (Table 3).
Symptomatic outcomes were associated with the location of tumors, with cerebellar lesions showing the highest rate of improvement (80%). Furthermore, improvements in symptoms were more pronounced in cases with a single prior surgery compared to multiple surgeries (81.3% vs. 57.1%) (Table 1, Table 2 and Table 3).
Adverse Radiation Effect (ARE)
Among the entire cohort, 2 (20%) pediatric patients experienced radiation-induced edema and 2 (20%) adult patients confirmed radiation necrosis. Patients who experienced ARE had similar dose parameters as the overall cohort, highlighting the need for further investigation into individual susceptibility factors.
4. Discussion
Our investigation into the outcomes of SRS for recurrent cranial medulloblastomas presents a thorough analysis of treatment efficacy and patient management (Figure 2). In light of the identified variations in treatment outcomes between pediatric and adult patients, a nuanced customization of treatment strategies emerges as imperative. This divergence may stem from enhanced central nervous system (CNS) plasticity in pediatric patients or the presence of less aggressive tumor types [14]. By integrating demographic, clinical, and treatment factors, our study provides a nuanced understanding of the intricate landscape associated with recurrent medulloblastomas.
Local Tumor Control
The observed LTC rates, notably the substantial 67% rate at 3 years in the pediatric cohort, emphasize the potential efficacy of SRS in managing recurrent medulloblastomas. Our findings align with existing literature, underscoring the significance of precision in targeting specific tumor locations, particularly cerebellar lesions, to optimize treatment outcomes[7,15,16,17,18].
Pediatric patients, who constitute a majority in our cohort, exhibit a higher prevalence of cerebellar lesions, possibly contributing to the enhanced LTC rates observed in this subgroup (Table 1). Conversely, the prevalence of multiple prior surgeries in the adult cohort may be linked to comparatively lower LTC rates, suggesting a potential association between prior surgical intervention and LTC outcomes[19,20,21]. Further exploration of associations between the number of fractions, BED, and LTC rates, considering factors such as age and tumor location, could enhance our understanding of the interplay influencing LTC outcomes.
Patient Survival and Progression-Free Survival
The OS rates of 90%, 70%, and 35% at 1, 3, and 5 years underscore the potential long-term benefits of SRS in managing recurrent cranial medulloblastomas, especially given their aggressive nature [22]. The discernibly elevated survival rates in pediatric patients compared to their adult counterparts emphasize age as a pertinent prognostic factor[23,24]. The prevalence of multiple prior surgeries in the adult cohort may contribute to the lower OS rates, emphasizing the impact of prior treatment history on long-term survival outcomes [25]. Shorter intervals between diagnosis and SRS may be associated with more favorable outcomes, suggesting that prompt initiation of SRS after diagnosis could contribute to improved survival rates. Smaller tumor volumes may correlate with greater OS and PFS outcomes, highlighting the importance of accurately defining and targeting tumor boundaries during SRS [26]. Optimal margin doses contribute to improved OS and PFS, and deviations from this may impact outcomes [27]. The nuanced interplay of these factors underscores the need for personalized treatment strategies, tailoring therapeutic approaches based on individual patient characteristics to optimize treatment outcomes.
Symptomatic Outcomes
Our investigation of symptomatic outcomes post-SRS reveals notable improvements, particularly in the pediatric patient cohort. With a higher percentage experiencing SI and lower rates of SW and NS, a potential correlation between clinical response and long-term survival outcomes is suggested [28]. Pediatric patients, constituting 80% of our cohort, demonstrate a particularly encouraging trend in symptomatic outcomes[29,30]. The SI percentage of 75% in the pediatric group, compared to 50% in adults, underscores the positive impact of SRS on symptom relief in younger patients [31]. The correlation between tumor location and SI emphasizes the need for tailored treatment approaches, with targeting cerebellar lesions yielding favorable symptomatic outcomes. The influence of the number of prior surgeries on symptomatic outcomes necessitates a critical examination of the optimal timing and extent of surgical interventions in managing recurrent medulloblastomas[30,32]. While SRS contributes to SI, understanding the interplay between prior surgeries and post-SRS symptoms is crucial for refining treatment strategies [33]. Our findings suggest that a judicious approach to surgical interventions, considering factors such as timing and extent, may contribute to more favorable symptomatic outcomes in the context of recurrent medulloblastomas.
Adverse Radiation Effects
The identification of radiation-induced edema and necrosis, albeit in a subset of patients, accentuates the critical role of meticulous dose planning[29,34]. These occurrences in both pediatric and adult patients underscore the imperative for personalized treatment strategies to mitigate ARE. [1] The absence of myelopathy provides reassurance and aligns with the safety profile reported in the existing literature[35,36].
Integration with Previous Studies
Our findings harmonize with prior studies exploring the role of SRS in recurrent medulloblastomas, emphasizing the indispensability of a multidisciplinary approach in patient care[4,31]. The alignment with established literature buttresses the generalizability of our results and contributes substantially to the burgeoning body of evidence supporting the efficacy of SRS in recurrent cranial medulloblastomas.
Limitations and Future Directions
Notwithstanding the promising results, our study is not immune to limitations. The retrospective nature of the analysis and the relatively modest sample size warrant cautious interpretation. Prospective studies with larger cohorts are imperative to validate our findings. Additionally, sustained long-term follow-up is pivotal for assessing the durability of treatment responses and potential late effects. These considerations acknowledge the current limitations and provide a foundation for future research to build upon our initial insights.
5. Conclusion
Our study offers a nuanced perspective on the efficacy and safety of CyberKnife SRS in addressing recurrent cranial medulloblastomas in both pediatric and adult demographics. The infrequency of ARE accentuates the favorable safety profile associated with CyberKnife SRS, thus affirming its contributory role in optimizing treatment outcomes. The intricacies of symptomatic responses, entangled with variables such as age, tumor localization, and prior surgical interventions, underscore the imperative for individualized therapeutic strategies. Our results underscore the need for ongoing research endeavors and the development of more refined and effective treatment strategies for recurrent medulloblastomas. Given the observed disparities in treatment outcomes between pediatric and adult cohorts, a more meticulous tailoring of treatment modalities becomes crucial.
Funding
Not applicable.
Ethics approval
Not applicable.
Consent for publication
Not applicable.
Acknowledgments
The authors express their gratitude for the valuable contributions of SDC, AM, DPJ, NJM, and KHY to the conception and design of this article. KHY played a pivotal role in data collection, analysis, manuscript composition, and the creation of figures and tables. SDC provided crucial resources and project supervision. The collaborative efforts of all authors were integral to shaping the article, and their approval has been obtained for the submitted version.
Conflicts of interest/Competing interests
Nothing to report.
Code availability
Not applicable.
Consent to participate
Not applicable.
Conference Presentations
This research has been presented as a poster at several prestigious conferences, including the American Association of Neurological Surgeons (AANS) Annual Meeting 2023 in Los Angeles, USA, the European Association of Neuro-Oncology (EANO) Annual Meeting 2023 in Rotterdam, Netherlands, the Congress of Neurological Surgeons (CNS) Annual Meeting 2023 in Washington, D.C., and the Radiosurgery Society (RSS) Scientific Meeting 2024 in Chicago, IL.
References
- Martin, A.M.; Raabe, E.; Eberhart, C.; Cohen, K.J. Management of pediatric and adult patients with medulloblastoma. Curr Treat Options Oncol. 2014, 15, 581–594. [Google Scholar] [CrossRef] [PubMed]
- Northcott, P.A.; Robinson, G.W.; Kratz, C.P. , et al. Medulloblastoma. Nat Rev Dis Primers. 2019, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.H.; Park, D.J.; Choi, J.H. , et al. Optimizing the synergy between stereotactic radiosurgery and immunotherapy for brain metastases. Front Oncol. 2023, 13, 1223599. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Noël, G. Medulloblastoma: optimizing care with a multidisciplinary approach. J Multidiscip Healthc. 2019, 12, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, V.; Remke, M.; Bouffet, E. , et al. Recurrence patterns across medulloblastoma subgroups: an integrated clinical and molecular analysis. Lancet Oncol. 2013, 14, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- van Bree, N.F.H.N.; Wilhelm, M. The Tumor Microenvironment of Medulloblastoma: An Intricate Multicellular Network with Therapeutic Potential. Cancers . 2022, 14, 5009. [Google Scholar] [CrossRef]
- Yoo, K.H.; Park, D.J.; Marianayagam, N.J., et al. Stereotactic Radiosurgery for Cranial and Spinal Hemangioblastomas: A Single-Institution Retrospective Series. Neurosurgery. 2023. [CrossRef]
- Zeng, M.; Han, L.F. Stereotactic radiosurgery: a “targeted” therapy for cancer. Chin J Cancer. 2012, 31, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.Y.H.; Soltys, S.G.; Gibbs, I.C. , et al. Stereotactic radiosurgery of cranial nonvestibular schwannomas: results of single- and multisession radiosurgery. Neurosurgery. 2011, 68, 1200–1208, discussion 1208. [Google Scholar] [CrossRef]
- Shi, S.; Jin, M.C.; Koenig, J. , et al. Stereotactic Radiosurgery for Pediatric and Adult Intracranial and Spinal Ependymomas. Stereotact Funct Neurosurg. 2019, 97, 189–194. [Google Scholar] [CrossRef]
- Fowler, J.F. 21 years of biologically effective dose. Br J Radiol. 2010, 83, 554–568. [Google Scholar] [CrossRef]
- Verma, V.; Kulkarni, R.R.; Bhirud, A.R.; Bennion, N.R.; McComb, R.D.; Lin, C. Metachronous medulloblastoma and glioblastoma: Implications for clinical and technical aspects of re-irradiation. Rep Pract Oncol Radiother. 2016, 21, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Joiner, M.C.; van der Kogel, A.J. Basic Clinical Radiobiology. CRC Press; 2018.
- Anderson, V.; Spencer-Smith, M.; Wood, A. Do children really recover better? Neurobehavioural plasticity after early brain insult. Brain. 2011, 134, 2197–2221. [Google Scholar] [CrossRef] [PubMed]
- Roussel, M.F.; Hatten, M.E. Cerebellum development and medulloblastoma. Curr Top Dev Biol. 2011, 94, 235–282. [Google Scholar] [PubMed]
- Peyrl, A.; Chocholous, M.; Sabel, M. , et al. Sustained Survival Benefit in Recurrent Medulloblastoma by a Metronomic Antiangiogenic Regimen: A Nonrandomized Controlled Trial. JAMA Oncol. 2023, 9, 1688–1695. [Google Scholar] [CrossRef]
- Cooney, T.; Lindsay, H.; Leary, S.; Wechsler-Reya, R. Current studies and future directions for medulloblastoma: A review from the pacific pediatric neuro-oncology consortium (PNOC) disease working group. Neoplasia. 2023, 35, 100861. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.H.; Barnett, G.H. Stereotactic radiosurgery for brain tumors in pediatric patients. Technol Cancer Res Treat. 2003, 2, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Management and Long-term Outcomes of Adults With Medulloblastoma. Neurology. Accessed January 2, 2024. https://www.neurology.org/doi/full/10.1212/WNL.0000000000207631?casa_token=IwzRtTLffBMAAAAA:qD0QXqjsWZuJ20jlSRUZVTswiTOE_-_2NFRy3c-BrecfeltHpGRIby9NtCpkigblcAVwd-xS_zP3. January.
- Edelstein, K.; Spiegler, B.J.; Fung, S. , et al. Early aging in adult survivors of childhood medulloblastoma: long-term neurocognitive, functional, and physical outcomes. Neuro Oncol. 2011, 13, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tarbell, N.J.; Black, P.M. , et al. Adult medulloblastoma: prognostic factors and patterns of relapse. Neurosurgery. 2000, 47, 623–631. [Google Scholar]
- King, D.; Connolly, D.; Zaki, H.; Lee, V.; Yeomanson, D. Successful treatment of metastatic relapse of medulloblastoma in childhood with single session stereotactic radiosurgery: a report of 3 cases. J Pediatr Hematol Oncol. 2014, 36, 301–304. [Google Scholar] [CrossRef]
- Yoo, K.H.; Marianayagam, N.J.; Park, D.J. , et al. P11. 48. A STEREOTACTIC RADIOSURGERY FOR EPENDYMOMA IN PEDIATRIC AND ADULT PATIENTS: A SINGLE-INSTITUTION EXPERIENCE. Neuro Oncol. 2023, 25, ii84–ii85. [Google Scholar] [CrossRef]
- Wooley, J.R.; Penas-Prado, M. Pediatric versus Adult Medulloblastoma: Towards a Definition That Goes beyond Age. Cancers . 2021, 13, 6313. [Google Scholar] [CrossRef] [PubMed]
- Gregory, T.A.; Mastall, M.; Lin, H. , et al. Characterization of recurrence patterns and outcomes of medulloblastoma in adults: The University of Texas MD Anderson Cancer Center experience. Neurooncol Adv. 2023, 5, vdad032. [Google Scholar] [PubMed]
- Peña-Pino, I.; Chen, C.C. Stereotactic Radiosurgery as Treatment for Brain Metastases: An Update. Asian J Neurosurg. 2023, 18, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Osuna-Marco, M.P.; Martín-López, L.I.; Tejera, Á.M.; López-Ibor, B. Questions and answers in the management of children with medulloblastoma over the time. How did we get here? A systematic review. A systematic review. Front Oncol. 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.Y.; Rosenblum, J.S.; Ho, W.S.; Heiss, J.D. New Developments in the Pathogenesis, Therapeutic Targeting, and Treatment of Pediatric Medulloblastoma. Cancers . 2022, 14, 2285. [Google Scholar] [CrossRef] [PubMed]
- Wetmore, C.; Herington, D.; Lin, T.; Onar-Thomas, A.; Gajjar, A.; Merchant, T.E. Reirradiation of recurrent medulloblastoma: does clinical benefit outweigh risk for toxicity? Cancer. 2014, 120, 3731–3737. [Google Scholar] [CrossRef]
- Hill, R.M.; Plasschaert, S.L.A.; Timmermann, B. , et al. Relapsed Medulloblastoma in Pre-Irradiated Patients: Current Practice for Diagnostics and Treatment. Cancers . 2021, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Napieralska, A.; Brąclik, I.; Radwan, M.; Mandera, M.; Blamek, S. Radiosurgery or hypofractionated stereotactic radiotherapy after craniospinal irradiation in children and adults with medulloblastoma and ependymoma. Childs Nerv Syst. 2019, 35, 267–275. [Google Scholar] [CrossRef]
- Chin, A.L.; Moding, E.J.; Donaldson, S.S. , et al. Survival impact of postoperative radiotherapy timing in pediatric and adolescent medulloblastoma. Neuro Oncol. 2018, 20, 1133–1141. [Google Scholar] [CrossRef]
- Hodgson, D.C.; Goumnerova, L.C.; Loeffler, J.S. , et al. Radiosurgery in the management of pediatric brain tumors. Int J Radiat Oncol Biol Phys. 2001, 50, 929–935. [Google Scholar] [CrossRef]
- Murphy, E.S.; Merchant, T.E.; Wu, S. , et al. Necrosis after craniospinal irradiation: results from a prospective series of children with central nervous system embryonal tumors. Int J Radiat Oncol Biol Phys. 2012, 83, e655–e660. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.W.; Rudneva, V.A.; Buchhalter, I. , et al. Risk-adapted therapy for young children with medulloblastoma (SJYC07): therapeutic and molecular outcomes from a multicentre, phase 2 trial. Lancet Oncol. 2018, 19, 768–784. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.E.; Duffner, P.K.; Terplan, K.L. Myelopathy with severe structural derangement associated with combined modality therapy. Cancer. 1983, 52, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Summary of patient outcome according to Kaplan-Meier method after treatment with CyberKnife SRS. A. Local tumor control (LTC) rate, B. Overall Survival (OS) rate, and C. Progression-free survival (PFS) rate of the adult (black, solid) and pediatric (blue, dash) series with recurrent medulloblastomas with number of lesions (A) and patients (B+C) at risk.
Figure 1.
Summary of patient outcome according to Kaplan-Meier method after treatment with CyberKnife SRS. A. Local tumor control (LTC) rate, B. Overall Survival (OS) rate, and C. Progression-free survival (PFS) rate of the adult (black, solid) and pediatric (blue, dash) series with recurrent medulloblastomas with number of lesions (A) and patients (B+C) at risk.
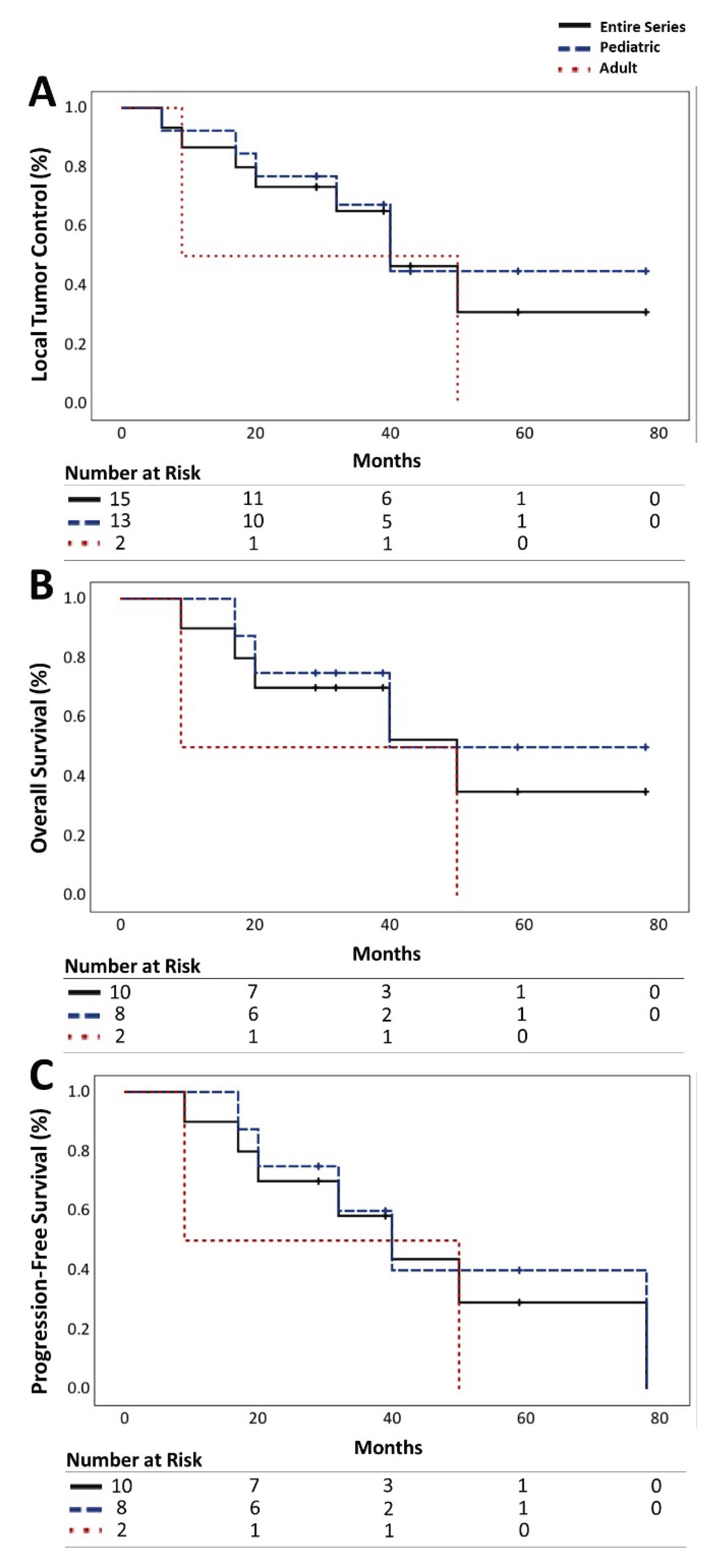
Figure 2.
Comparison of A. a baseline CyberKnife treatment plan and B. the most recent radiographic follow-up evaluation of a 11-year-old male patient with a cervicomedullary recurrent medulloblastoma status post surgical resection and adjuvant radiation therapy. A marginal dose of 18 Gy was delivered with the maximum dose of 24.16 Gy in a single fraction to 75% of the isodose line (A). A substantial reduction in tumor size was evident in the 41-month follow-up MRI (B).
Figure 2.
Comparison of A. a baseline CyberKnife treatment plan and B. the most recent radiographic follow-up evaluation of a 11-year-old male patient with a cervicomedullary recurrent medulloblastoma status post surgical resection and adjuvant radiation therapy. A marginal dose of 18 Gy was delivered with the maximum dose of 24.16 Gy in a single fraction to 75% of the isodose line (A). A substantial reduction in tumor size was evident in the 41-month follow-up MRI (B).
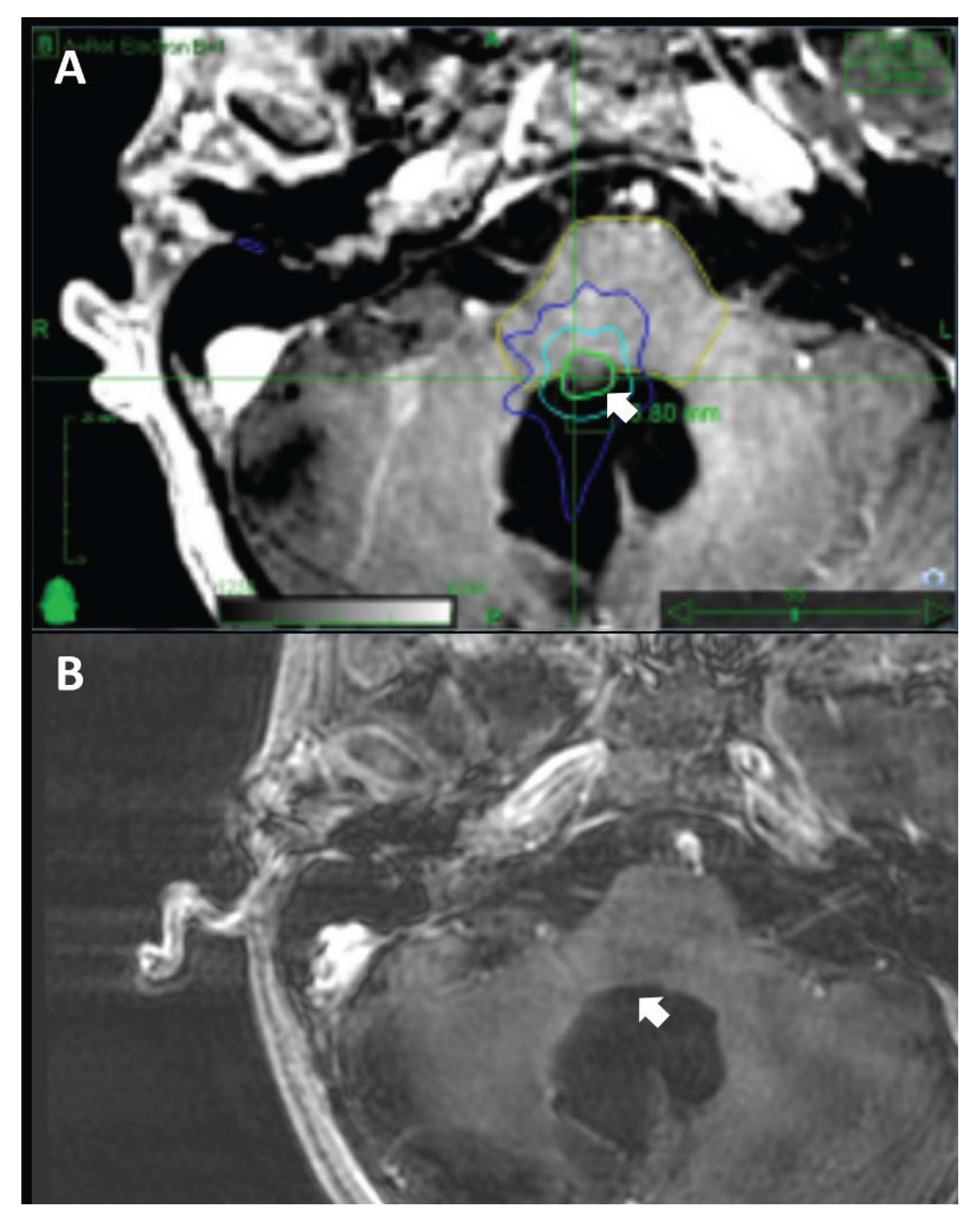

Table 1.
Demographic characteristics in 10 patients with 15 recurrent cranial medulloblastomas.
| Characteristics | Entire Cohort | Pediatric | Adult |
|---|---|---|---|
| # patients | 10 (100%) | 8 (80%) | 2 (20%) |
| Sex | |||
| Male | 8 (80%) | 6 (75%) | 2 (100%) |
| Female | 2 (20%) | 2 (25%) | 0 (0%) |
| Prior Surgery | |||
| Single | 6 (60%) | 6 (75%) | 0 (0%) |
| Multiple | 3 (30%) | 1 (12.5%) | 2 (100%) |
| Symptoms | |||
| Headaches | 6 (60%) | 4 (50%) | 2 (100%) |
| Nausea | 4 (40%) | 4 (50%) | 1 (50%) |
| Vomiting | 5 (50%) | 4 (50%) | 1 (50%) |
| Ataxia | 3 (30%) | 1 (12.5%) | 2 (100%) |
| Visual impairment | 3 (30%) | 2 (25%) | 1 (50%) |
| Seizure | 2 (20%) | 2 (25%) | 0 (0%) |
| Left-sided dysmetria | 1 (10%) | 1 (12.5%) | 0 (0%) |
| Peripheral rigidity | 1 (10%) | 1 (12.5%) | 0 (0%) |
| # tumors | 15 (100%) | 13 (86.7%) | 2 (13.3%) |
| Location | |||
| Cerebellar | 5 (33.3%) | 4 (30.8%) | 1 (50%) |
| Ventricular | 2 (13.3%) | 1 (7.7%) | 1 (50%) |
| Frontal | 2 (13.3%) | 2 (15.4%) | 0 (0%) |
| Parietal | 2 (13.3%) | 2 (15.4%) | 0 (0%) |
| Temporal | 1 (6.7%) | 1 (7.7%) | 0 (0%) |
| Thalamic | 1 (6.7%) | 1 (7.7%) | 0 (0%) |
| Cervicomedullary | 1 (6.7%) | 1 (7.7%) | 0 (0%) |
| Medullary | 1 (6.7%) | 1 (7.7%) | 0 (0%) |
| Clinical Presentation | |||
| Symptomatic | 14 (93.3%) | 12 (92.3%) | 2 (100%) |
| Asymptomatic | 1 (6.7%) | 1 (7.7%) | 0 (0%) |
| #, numbers | |||
Table 2.
Treatment characteristics in 10 patients with 15 recurrent cranial medulloblastomas.
| Characteristics | Entire Cohort | Pediatric | Adult | Statistical Significance (p Values) |
|---|---|---|---|---|
| # tumors per patient | 0.4 | |||
| Mean | 1.5 | 1.6 | 1 | |
| Median | 1 | 1 | 1 | |
| Range | 1-4 | 1-4 | 1 | |
| Age at Treatment, yrs | ||||
| Mean | 14.3 | 12.4 | 27 | < 0.001 |
| Median | 13 | 12 | 27 | |
| Range | 9-29 | 9-16 | 25-29 | |
| Interval between Diagnosis to SRS, mo | ||||
| Mean | 42.7 | 45.5 | 24.5 | |
| Median | 30 | 39 | 24.5 | 0.4 |
| Range | 12-108 | 12-108 | 24-25 | |
| Target Tumor Volume, cc | ||||
| Mean | 2.7 | 2.9 | 1.5 | 0.51 |
| Median | 1.9 | 1.8 | 1.5 | |
| Range | 0.02-8.7 | 0.02-8.7 | 0.5-2.5 | |
| Margin Dose, Gy | ||||
| 1 Fraction | 0.8 | |||
| Mean | 17.8 | 17.8 | 18 | |
| Median | 18 | 18 | 18 | |
| Range | 14-20 | 14-20 | 18 | |
| 2 Fractions | ||||
| Mean | 20 | 20 | N/A | |
| Median | 20 | 20 | N/A | |
| Range | 20 | 20 | N/A | |
| 3 Fractions | ||||
| Mean | N/A | N/A | N/A | |
| Median | N/A | N/A | N/A | |
| Range | N/A | N/A | N/A | |
| 4 Fractions | ||||
| Mean | N/A | N/A | N/A | |
| Median | N/A | N/A | N/A | |
| Range | N/A | N/A | N/A | |
| 5 Fractions | ||||
| Mean | 25 | 25 | N/A | |
| Median | 25 | 25 | N/A | |
| Range | 25 | 25 | N/A | |
| Maximum Dose, Gy | ||||
| 1 Fraction | 0.9 | |||
| Mean | 23.3 | 23.1 | 24.2 | |
| Median | 24.2 | 24.2 | 24.2 | |
| Range | 19.7-25 | 19.7-25 | 24.2-24.3 | |
| 2 Fractions | ||||
| Mean | 30.8 | 65 | N/A | |
| Median | 30.8 | 65 | N/A | |
| Range | 30.8 | 65 | N/A | |
| 3 Fractions | ||||
| Mean | N/A | N/A | N/A | |
| Median | N/A | N/A | N/A | |
| Range | N/A | N/A | N/A | |
| 4 Fractions | ||||
| Mean | N/A | N/A | N/A | |
| Median | N/A | N/A | N/A | |
| Range | N/A | N/A | N/A | |
| 5 Fractions | ||||
| Mean | 35.7 | 70 | N/A | |
| Median | 35.7 | 70 | N/A | |
| Range | 35.7 | 70 | N/A | |
| # Fraction | ||||
| Mean | 1.3 | 1.4 | 1 | |
| Median | 1 | 1 | 1 | 0.6 |
| Range | 1-5 | 1-5 | 1 | |
| BED, Gy | ||||
| Mean | 118.1 | 117 | 126 | |
| Median | 126 | 126 | 126 | 0.7 |
| Range | 66.7-153.3 | 66.7-153.3 | 126 | |
| SFED | ||||
| Mean | 17.2 | 17.1 | 18 | |
| Median | 18 | 18 | 18 | 0.6 |
| Range | 12.7-20 | 12.7-20 | 18 | |
| EQD2 | ||||
| Mean | 70.8 | 70.2 | 75.6 | |
| Median | 75.6 | 75.6 | 75.6 | 0.7 |
| Range | 40-92 | 40-92 | 75.6 | |
| Isodose Line, % | ||||
| Mean | 74.9 | 74.9 | 74.5 | 0.9 |
| Median | 75 | 75 | 74.5 | |
| Range | 65-81 | 65-81 | 74-75 | |
| Follow Up, mo | ||||
| Mean | 35.6 | 36.5 | 29.5 | 0.6 |
| Median | 39 | 39 | 29.5 | |
| Range | 6-78 | 6-78 | 9-50 | |
| #, number; BED, biologically effective dose; SFED, single-fraction equivalent dose; EQD2, equivalent total doses in 2-Gy fractions; N/A, not applicable; cc, cubic centimeter; Gy, Gray; mo, months; yrs, years | ||||
Table 3.
Radiological and clinical outcomes.
| Variables | Entire Series | Pediatric | Adult | Statistical Significance(p Value) |
|---|---|---|---|---|
| LTC | ||||
| 3 yrs, % | 65 | 67 | 50 | 0.05 |
| OS | ||||
| 3 yrs, % | 70 | 75 | 50 | 0.24 |
| mean, mo | 47.4 | 47.4 | 0 | |
| PFS | ||||
| 3 yrs, % | 58 | 60 | 50 | 0.46 |
| mean, mo | 42.3 | 42.3 | 0 | |
| SI, % | 70 | 75 | 50 | 0.05 |
| SW, % | 10 | 12.5 | 50 | 0.03 |
| NS, % | 10 | 0 | 50 | < 0.001 |
| LTC, local tumor control; OS, overall survival; PFS, progression-free survival; SI, symptomatic improvement; SW, symptomatic worsening; NS, new symptoms; yrs, years; mo, months | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



