
Submitted:
30 March 2024
Posted:
01 April 2024
You are already at the latest version
Abstract
Introduction: Chronic wounds caused by diabetes or lower-extremity artery disease are intractable because the wound healing mechanism is no longer effective due to the poor environment of the wound bed. Biosheet obtained using in-body tissue architecture (iBTA) is a collagen-based membranous tissue that is created within the body and autologously contains various growth factors and somatic stem cells including pluripotent stem cells. When applied to a wound, granulation formation can be promoted and even epithelialization may be achieved. Hearin, we report our clinical treatment experience with seven cases of intractable diabetic foot ulcers. Cases: From 46- to 93-year-old 7 patients had large foot ulcers including heel area, which was failed to heal with standard wound treatment. Methods: Two or four Biosheet-forming molds were implanted subcutaneously in the chest or abdomen, and after 3 to 6 weeks, the molds were removed. Biosheets that formed inside the mold were obtained and applied directly to the wound surface. Results: In all cases, there were no problems with the mold embedding and removal procedures, and Biosheets were formed without any infection or inflammation during the implantation period. The Biosheets were simply applied to the wounds, and in all cases, they adhered within one week, did not fall of, and became integrated with the wound surface Complete wound closure was achieved within 8 weeks in two cases and within 5 months in two cases. One patient was lost due to infective endocarditis from septic colitis. One case required lower leg amputation due to the wound recurrence, and one case achieved wound reduction and wound healing in approximately 9 months. Conclusion: Biotube obtained via iBTA promoted wound healing and were extremely useful for intractable diabetic foot ulcers involving heel area.
Keywords:
Diabetic foot ulcer
; Tissue-engineered biosheet
; in-body tissue architecture
; wound repaire
1. Introduction
Diabetic foot ulcers are some of the most significant diabetic complications. Approximately 25% of people with diabetes will develop a lower-extremity ulcer over their lifetimes [1]. Concomitant conditions associated with diabetes, such as peripheral artery disease causing limb ischemia, neuropathy causing sensory disturbance and foot deformity, and high blood glucose increasing the risk of infection, contribute to causing foot ulcers and gangrene. In addition, the delayed healing of ulcers increases the need for amputation, which, in turn, increases morbidity and healthcare costs and simultaneously reduces an individual’s productivity and quality of life. Wound healing is an intricate and complex process. Chronic wounds caused by diabetes or lower-extremity artery disease are intractable, as the wound-healing mechanism is no longer effective because of the poor environment of the wound bed. Moist dressings, debridement, wound offloading, and infection control are standard in the management of lower-extremity ulcers, yet even with the best conservative care, these wounds are notoriously slow to heal, requiring many months of treatment [2]. The ideal therapeutic product would need to work for multiple targets in the wound repair process.
We developed an in vivo tissue-engineering technique called in-body tissue architecture (iBTA), enabling tissue preparation for autologous implantation by subcutaneously embedding a specifically designed mold [3,4,5,6,7,8,9,10]. A “Biosheet” can be obtained using iBTA, a collagen-based membranous tissue that is created within the body and autologously contains various growth factors and somatic stem cells, including pluripotent stem cells. When applied to a wound, granulation formation can be promoted and even epithelialization can be achieved. Herein, we report our clinical treatment experiences with seven cases of intractable diabetic foot ulcers.
2. Cases
All seven cases were diagnosed with type 2 diabetes mellitus, and four of these cases also had peripheral artery disease (Table 1). In addition, six cases were undergoing dialysis treatment for end-stage renal disease.
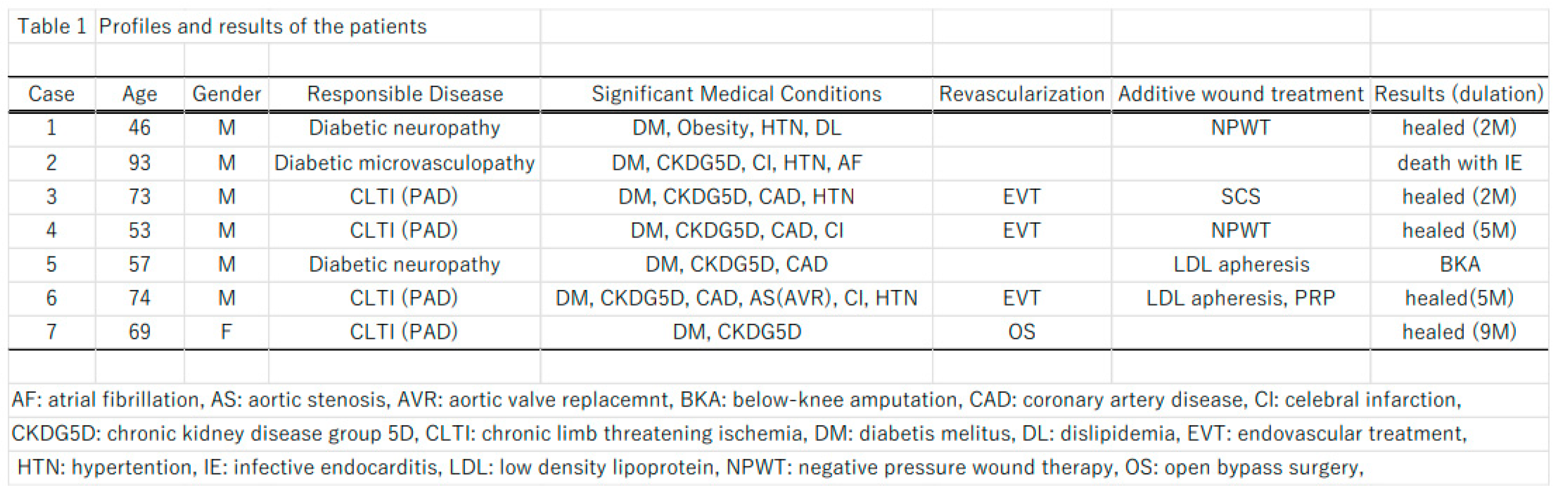
Revascularization and standard wound treatment had been performed, and spinal cord stimulation was performed for Case 3, negative pressure wound therapy was performed for Case 4, and LDL apheresis was performed for Cases 4 and 5 as an additive wound treatment; however, foot ulcers are difficult to cure.
Two or four Biosheet-forming molds for each patient were implanted subcutaneously in the chest or abdomen, and after 3 to 6 weeks, the molds were removed. Biosheets that formed inside the mold were obtained and applied directly to the wound surface. Then, the Biosheets were covered with a nonadherent silicon dressing (Mepitel-One; Moneliche Health Care, Germany) or an acetylcellulose dressing (Sorbact: ABIGO Medical AB, Sweden), and were then overlapped with an antimicrobial non-woven hydrofiber fabric (Aquacel Ag Advantage: ConvaTec Inc, USA).
Following the application of the Biosheets, dressings were exchanged weekly.
3. Results
In all cases, there were no problems with the mold implantation and removal techniques, and the Biosheets formed without any infection or inflammation during the implantation period. The Biosheets were simply applied to the wounds, and in all cases, they adhered within one week, did not fall off, and became integrated with the wound surface. Specific case examples are shown below.
Case 1 (Figure 1 and Figure 2): A 46-year-old man was obese with a height of 180 cm and a weight of 135 kg. He has had diabetes since his 20s, which was complicated by retinopathy, nephrotic syndrome, hypertension, and dyslipidemia. Both of his fifth toes had already been amputated because of diabetic ulcers. At the beginning of December 202X, an ulcer formed on the dorsum and heel of his left foot. By mid-December, the patient had developed a fever and redness and swelling of the entire left foot. Thus, he visited our wound care center on December 23.
A blood test showed a high inflammatory state (WBC was 15700/mm3, CRP was 16.23 mg/dl). Antibiotic treatment was started and then debridement was performed. Negative pressure wound therapy was performed on January 18th, and when the wound bed preparation was completed, two molds were implanted. Three weeks later, Biosheets were attached to the wound. The wound was epithelialized in about 2 months.
Case 3 (Figure 3 and Figure 4): A 72-year-old man presented with chronic limb-threatening ischemia with gangrene of the left first toe and bilateral heel ulcers. He had diabetes, end-stage renal disease, and high blood pressure and had already undergone right metatarsal amputation and coronary artery bypass surgery. In January 202X, the patient was referred for intractable bilateral heel ulcers and left first-toe gangrene. Lower-extremity angiography revealed occlusion of the right posterior tibial artery, 90% stenosis of the anterior tibial artery, occlusion of the left posterior tibial artery and peroneal artery, and 90% stenosis of the anterior tibial artery. His ischemic pain was also severe; therefore, spinal cord stimulation therapy was used to alleviate the pain and improve his peripheral microcirculation. After endovascularly treating the left lower limb, amputating the left thumb, and endovascularly treating the right lower limb, four molds were placed subcutaneously in the patient’s abdomen. After 4 weeks, four Biosheets were applied to the wound. The small heel ulcer healed in 3 weeks, and the large heel ulcer healed in 2 months.
Case 6 (Figure 5 and Figure 6): A 74-year-old man with chronic limb-threatening ischemia presented with gangrene of the right thumb and left forefoot. The patient had diabetes, end-stage renal disease, and hypertension; had a history of coronary artery disease, cerebral infarction, colon polyps, and thyroid cancer; and had undergone coronary artery intervention, open polypectomy, and thyroid cancer removal. During his previous hospitalization, he underwent lower-extremity endovascular treatment four times and was also given LDL apheresis treatment, but it was refractory. After admission to our hospital, antibiotics were administered, and left transverse total metatarsal amputation was performed to control the infection. Additional endovascular treatment was performed, and LDL apheresis was continued to improve blood flow. However, the wound separated, and the metatarsal bones were exposed; therefore, we performed a left Chopard joint disarticulation, and at the same time, the right big toe was amputated, and a stump was created. The right big toe wound healed, but the left stump wound dehisced again. Four molds were implanted subcutaneously in the abdomen, and 6 weeks later, Biosheets obtained from these molds were implanted into the left stump wound. Wound granulation progressed, and healing was achieved after 5 months.
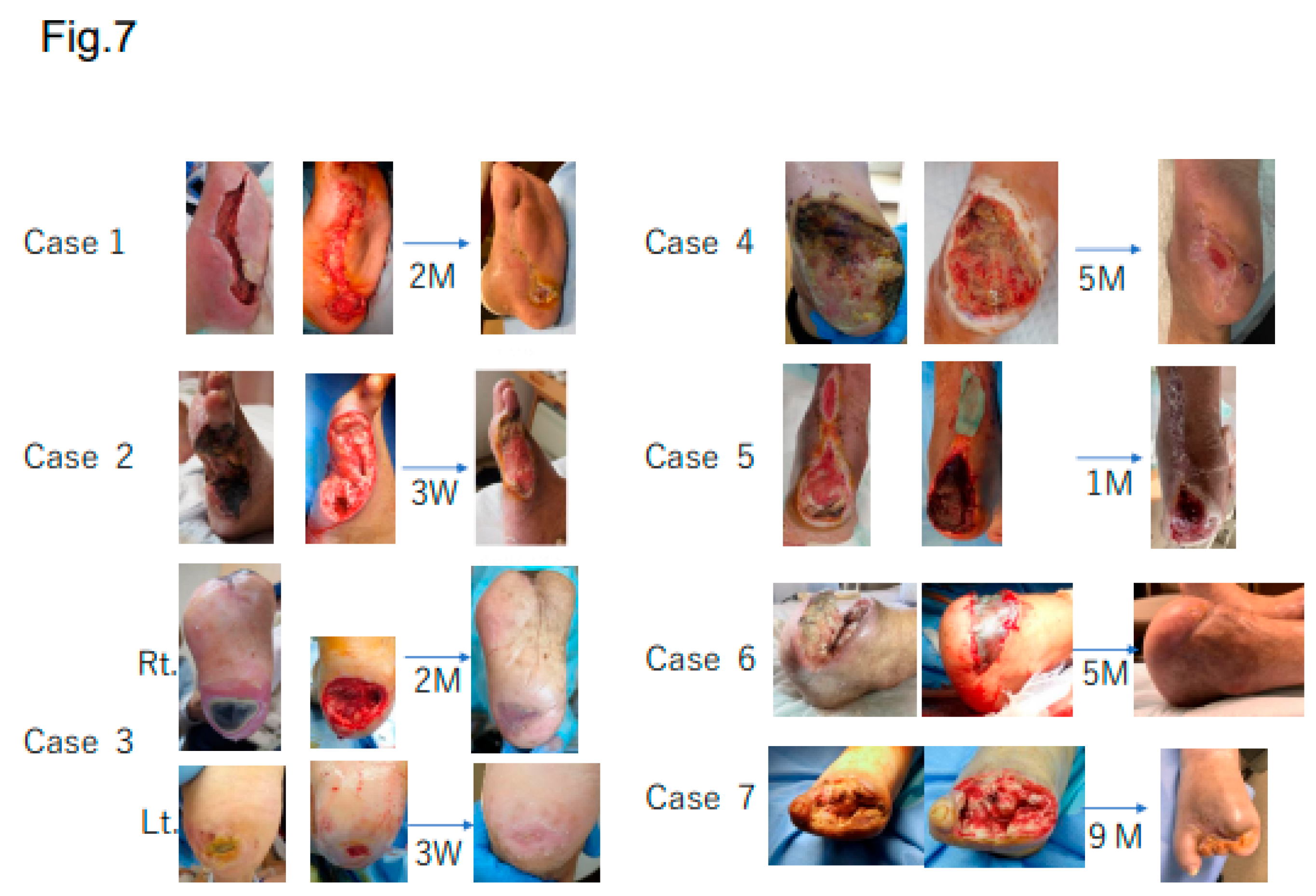
In summary, complete wound closure was achieved within 8 weeks in two cases (Cases 1 and 3) and within 5 months in two cases (Cases 4 and 6). Case 2 was lost due to infective endocarditis from septic colitis. Case 5 required lower leg amputation due to wound recurrence, and Case 7 achieved wound reduction and wound healing in approximately 9 months because of significant edema in her lower leg (Figure 7).
4. Discussion
It is difficult to treat ulcers and gangrene located on the heel, and it is recommended that primary amputation be carried out in select individuals with heel necrosis [11,12].
Soderstorm et al. [13] showed that ischemic tissue lesions located on the mid- and hindfoot had significantly prolonged ulcer healing times; Kobayashi et al. [14] indicated that the healing rate of heel wounds was lower than that of toe wounds and that they took a considerably longer time to heal. The wounds in all of our cases were located on the heel or mid- or hindfoot and seemed to be hard to heal; however, Biosheets were effective in promoting healing.
A tissue analysis of Biosheets used in a previous animal experiment showed that 560,000 CD90-positive mesenchymal stem cells/cm2 and 160,000 SEEA-positive pluripotent stem cells/cm2. In addition, component analysis showed platelet-derived growth factor, fibroblast growth factor, vascular endothelial growth factor, hepatocyte growth factor, and epidermal growth factor, which are thought to have considerable effects on wound healing.
Advanced therapies such as bioengineered skin substitutes, xenografts, and allografts have been shown to promote wound closures, resulting in more consistent and faster healing of diabetic ulcers compared with standard therapies [15,16,17,18,19]; however, even though net cost savings can be achieved through increased healing rates, a faster time to healing, and reduced incidences of infection and amputation, these advanced therapies are expensive. Biosheets are much less expensive and safer because they are autologously produced and do not require factory instruments, cell culture, or labor. In addition, wound management costs include supplies and dressings (15–20%), nursing time (30–35%), and hospitalization (more than 50%) [20]. Frequent dressing changes increase the cost of wound care; in comparison, Biosheets can be single-use and dressing changes may only be required about once a week.
5. Conclusions
Biotubes obtained via iBTA promoted wound healing and were extremely useful for intractable diabetic foot ulcers involving the heel area.
References
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic foot ulcers and their recurrence. N Engl J Med 2017, 376, 2367-75. [Google Scholar] [CrossRef] [PubMed]
- Zhan LX, Branco BC, Armstrong DG, et al. The society for vascular surgery lower extremity threatened limb classification system based on wound, ischemia, and foot infection (WIfI) correlates with risk of major amputation and time wound healing. J Vasc Surg 2015, 61, 939-44. [Google Scholar]
- Nakayama, Y.; Ishibashi-Ueda, H.; Takamizawa, K. In vivo tissue-engineered small-caliber arterial graft prosthesis consisting of autologous tissue (Biotube). Cell Transplant 2004, 13, 439-49. [Google Scholar] [CrossRef] [PubMed]
- Takiyama N, Mizuno T, Iwai R, et al. In-body tissue-engineered collagenous connective tissue membranes (BIOSHEETs) for potential corneal stromal substitution. J Tissue Eng Regen Med 10: E518-26, 2013.
- Nakayama Y, Takewa Y, Sumikura H, et al. In-body tissue-engineered aortic valve (Biovalve type VII) architecture based on 3D printer molding. J Biomed Mater Res B Appl Biomater 103: 1-11, 2015.
- Furukoshi M, Moriwaki T, Nakayama Y. Development of an in vivo tissue-engineered vascular graft with designed wall thickness (biotube type C) based on a novel caged mold. J Artif Organs 19: 54-61, 2016.
- Nakayama Y, Kaneko Y, Takewa Y, et al. Mechanical properties of human autologous tublar connective tissues (human biotubes) obtained from patients undergoing peritoneal dialysis. J Biomed Mater Res Part B 2016 104B: 1431-1437.
- Ishii D, Enmi J, Moriwaki T, et al. Development of in vivo tissue-engineered maicrovascular grafts with an ultra small diameter of 0.6 mm (MicroBiotubes): acute phase evaluation by optical coherence tomography and magunetic resonance angiology. J Artif Organs (2016) 19: 262-269.
- Satake R, Komura M, Komura H, et al. Patch tracheoplasty in body tissue engineering using collagenous connective tissue membranes (biosheets). J Pediatr Surg 51(2016) 244-248.
- Nakayama Y, Furukoshi M, Terazawa T, et al. Development of long in vivo tissue-engineered “Biotube” vascular grafts. Biomaterials 185 (2018) 232-239.
- Carsten CG 3rd, Taylor SM, Langan EM 3rd, et al. Factors associated with limb loss despite a patient infrainguinal bypass graft. Am Surg 1998; 64: 33-37; discussion 37-38.
- Edwards JM, Taylor LM Jr, Porter JM. Limb salvage in end-stage renal disease (ESRD). Comparison of modern results in patients with and without ESRD. Arch Surg 1998; 123: 1164-1168.
- Soderstrom M, Aho PS, Lepnatalo M, et al. The influence of the characteristics of ischemic tissue lesion on ulcer healing time after infrainguinal bypass for critical leg ischemia. J Vasc Surg 2009; 49: 932-937.
- Kobayashi N, Hirano K, Nakano M, et al. Wound healing and wound location in critical limb ischemia following endovascular treatment. Circ J 2014; 78: 1746-1753.
- Veves A, Falanga V, Armstrong DG, et al. Graftskin, a human skin equivalent, is effective in the management of noninfected neuropathic diabetic foot ulcers: a prospective randomized multicenter clinical trial. Diabetes Care 2001; 24: 290-5.
- Marston WA, Hanft J, Norwood P, et al. The efficacy and safety of dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care; 2003; 26:1701-5.
- Zelen CM, Serena TE, Denoziere G, et al. A prospective randomized comparative parallel study of amniotic membrane wound graft in the management of diabetic foot ulcers. Int Wound J 2013; 10: 502-7.
- Fetterolf DE, Istwan NB, Stanziano GJ. An evaluation of healing metrics associated with commonly used advanced wound care products for treatment of chronic foot ulcers. Manag Care 2014; 23: 31-8.
- Zelen CM, Gould L, Serena TE, et al. A prospective, randomized, controlled, multi-centre comparative effectiveness study of healing using dehydrated human amnion/chorion membrane allograft, bioengineered skin substitute or standard of care for treatment of chronic lower extremity diabetic ulcers. Int Wound J 2015; 12: 724-732.
- Tiscar-Gonzalez V, Menor-Rodriguez MJ, Rabadan-Sainz C, et al. Clinical and economic impact of wound care using a polyurethane foam multilayer dressing. Adv Skin Wound Care 2021; 10: 13-23.
Figure 1.
(A) Left-foot ulcers at admission: a. ulcer on dorsal pedis; b. medial part; c. heel ulcer on left foot. (B) a. Wounds after debridement; b. negative-pressure wound treatment. (C) Subcutaneous mold-embedding procedure—a. the mold is 5 centimeter in length, 2 centimeter in diameter, and has numerous small round holes in the outer part; b. subcutaneous embedding of the mold; c. closed wound over embedding; d. air removal of the inside mold through a needle puncture. (D) Biosheet patch therapy—a. removing the mold from the subcutaneous space; b. obtained Biosheet; c. patch therapy using the opened Biosheet; d. wound covered by a siliconsheet (Mepitel One).
Figure 1.
(A) Left-foot ulcers at admission: a. ulcer on dorsal pedis; b. medial part; c. heel ulcer on left foot. (B) a. Wounds after debridement; b. negative-pressure wound treatment. (C) Subcutaneous mold-embedding procedure—a. the mold is 5 centimeter in length, 2 centimeter in diameter, and has numerous small round holes in the outer part; b. subcutaneous embedding of the mold; c. closed wound over embedding; d. air removal of the inside mold through a needle puncture. (D) Biosheet patch therapy—a. removing the mold from the subcutaneous space; b. obtained Biosheet; c. patch therapy using the opened Biosheet; d. wound covered by a siliconsheet (Mepitel One).
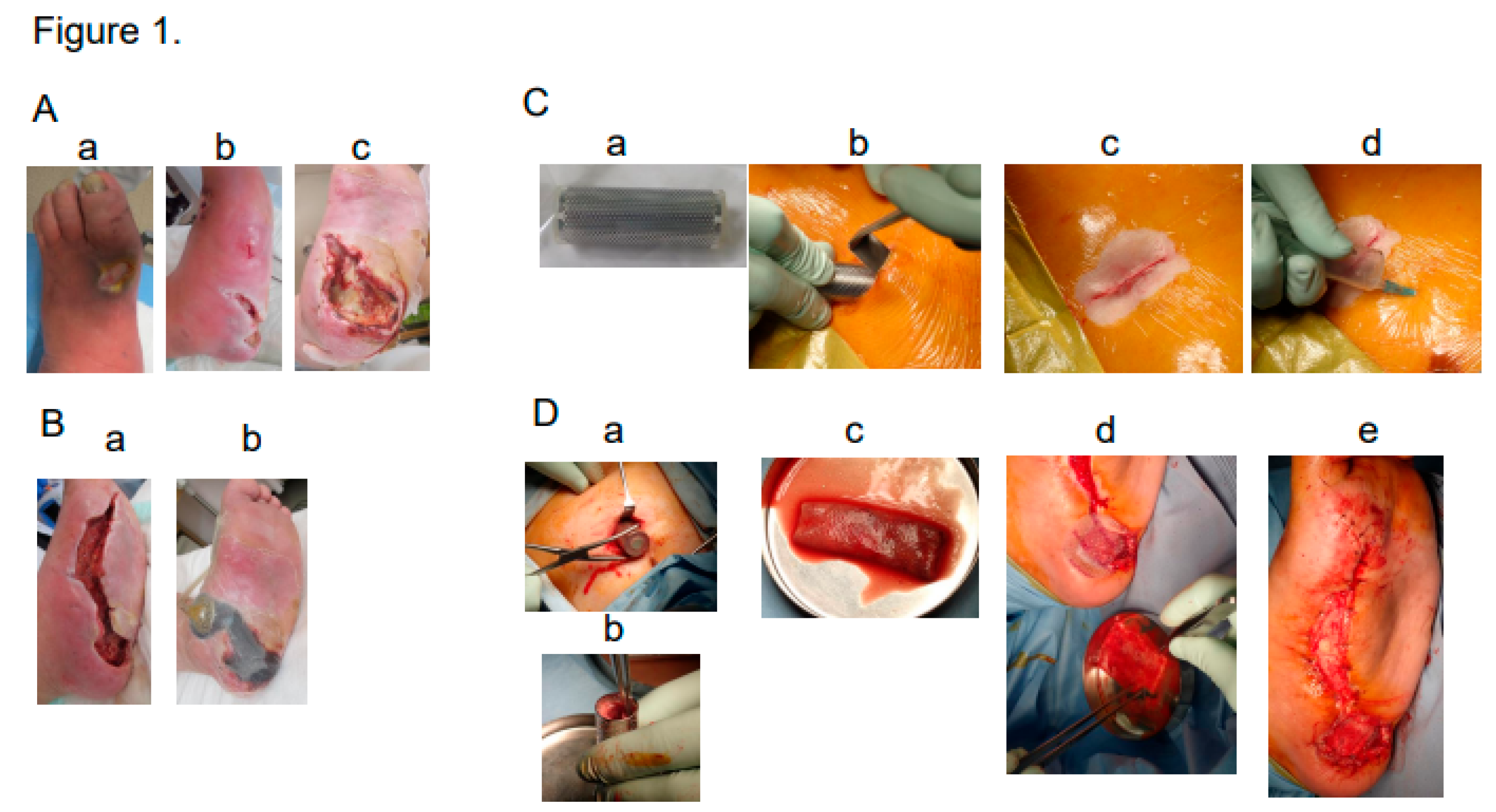
Figure 2.
Post-operative course in Case 1. Wound healed in three months.
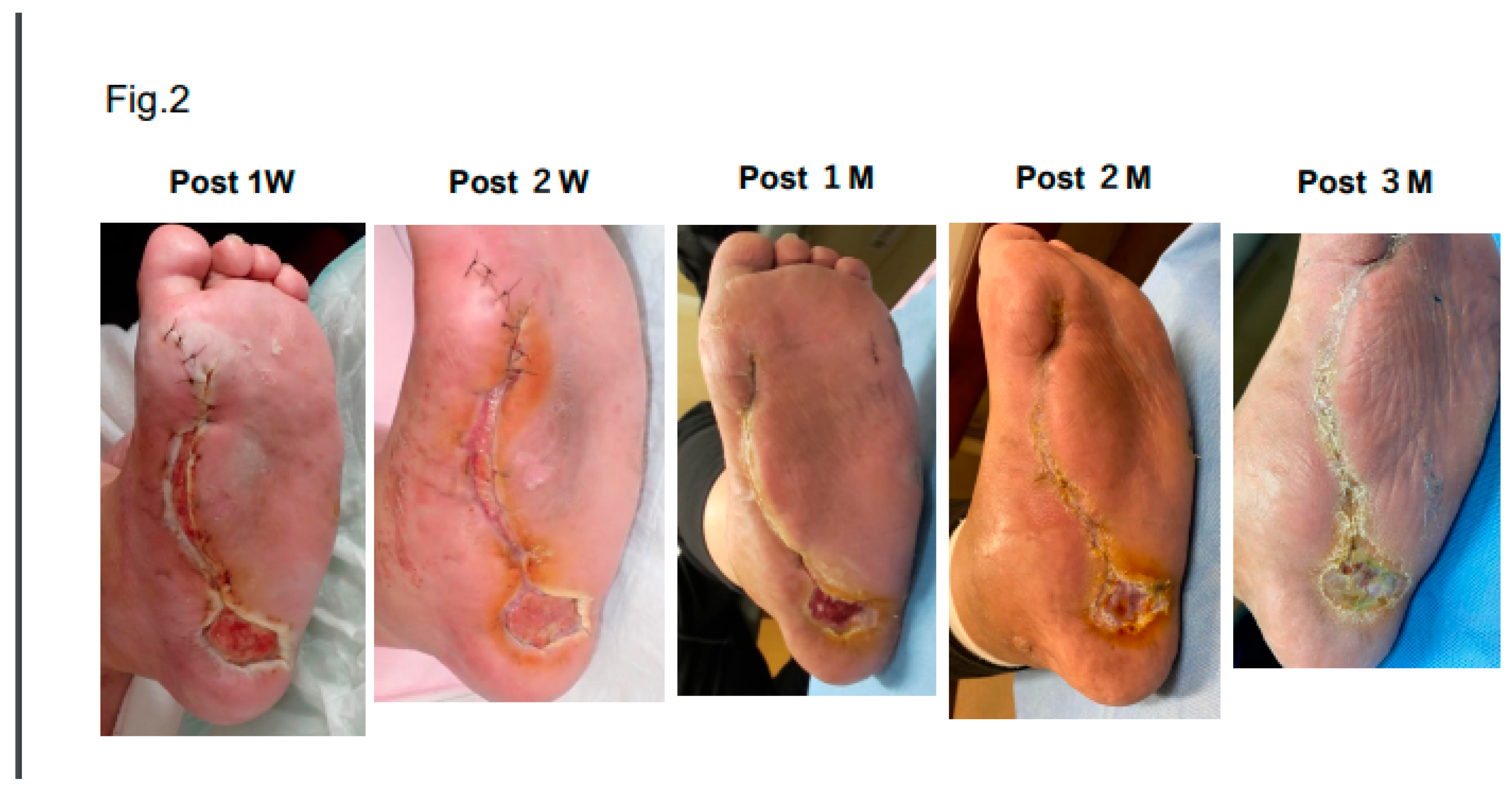
Figure 3.
(A) Foot ulcers and gangrene in Case 3 upon admission—a. Left 2nd-and 3rd-toe gangrene; b. left-heel ulcer; c. right-heel ulcer. (B) Subcutaneous mold-embedding procedure—a. the plan of the mold embedding; b. embedding procedure using a sizer; c. air removal from the subcutaneous space and inside mold through a drainage tube after embedding; d. X-ray photograph after embedding the four molds. The white arrow indicates the spinal code stimulation generator. (C) Biosheet patch therapy—a. four Biosheets obtained after removing the mold from the subcutaneous space; b. Biosheets applied to the debrided wounds.
Figure 3.
(A) Foot ulcers and gangrene in Case 3 upon admission—a. Left 2nd-and 3rd-toe gangrene; b. left-heel ulcer; c. right-heel ulcer. (B) Subcutaneous mold-embedding procedure—a. the plan of the mold embedding; b. embedding procedure using a sizer; c. air removal from the subcutaneous space and inside mold through a drainage tube after embedding; d. X-ray photograph after embedding the four molds. The white arrow indicates the spinal code stimulation generator. (C) Biosheet patch therapy—a. four Biosheets obtained after removing the mold from the subcutaneous space; b. Biosheets applied to the debrided wounds.
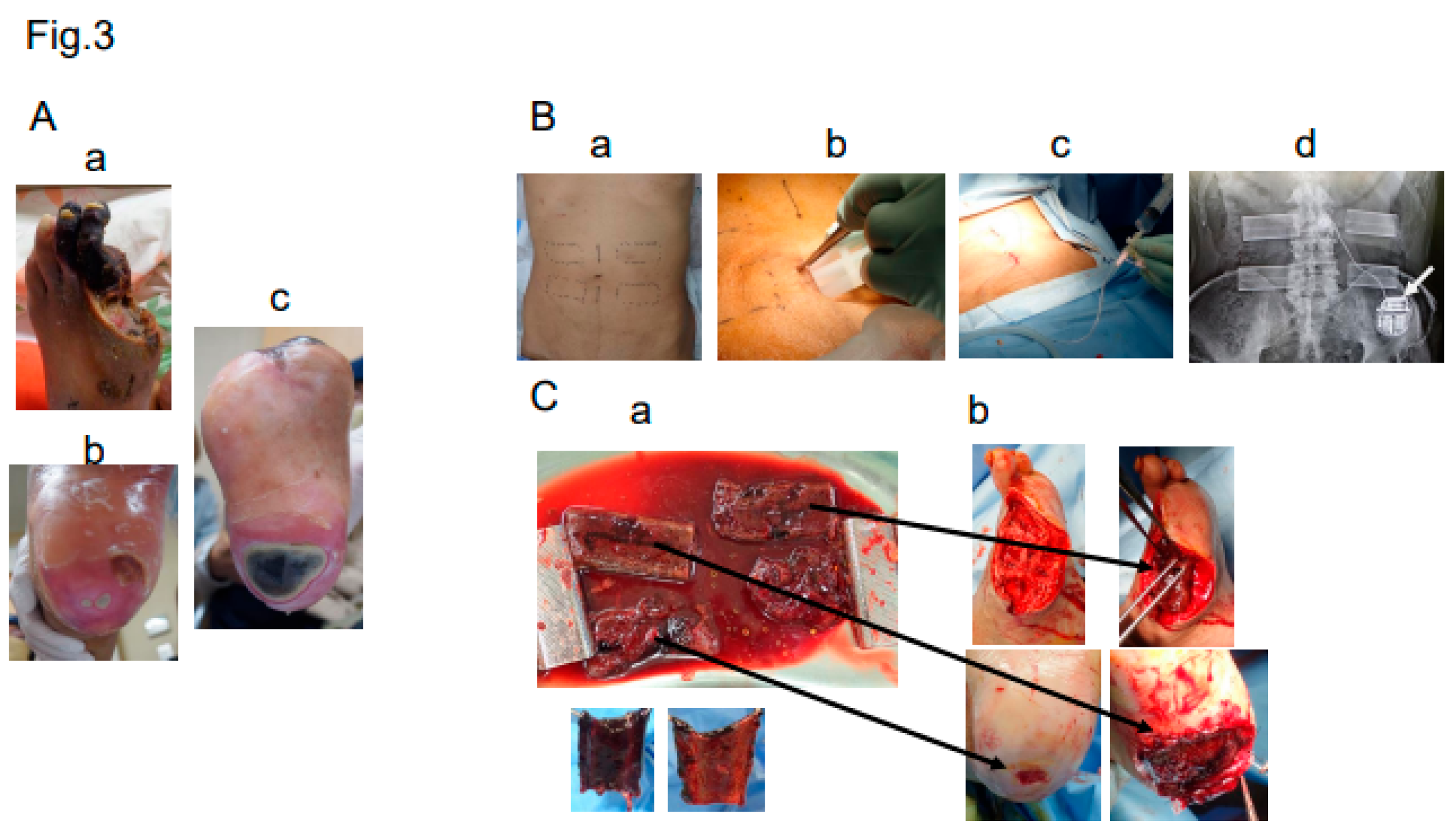
Figure 4.
Post-operative course in Case 3. (a) After the toes were debrided, the wound healed in ten weeks. (b) Small wound on the left heel healed in three weeks. (c) Large wound on the right heel healed in eight weeks.
Figure 4.
Post-operative course in Case 3. (a) After the toes were debrided, the wound healed in ten weeks. (b) Small wound on the left heel healed in three weeks. (c) Large wound on the right heel healed in eight weeks.
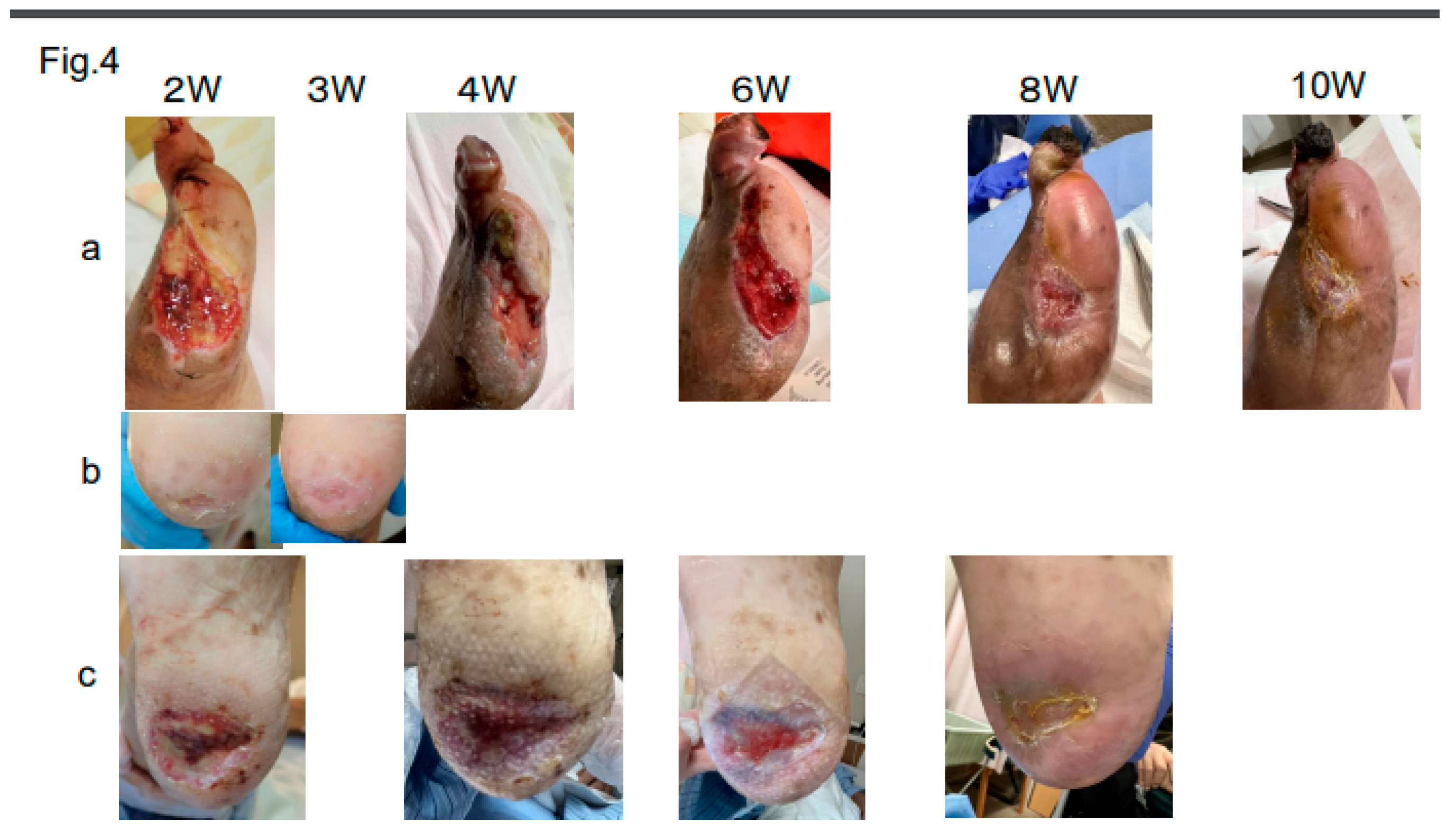
Figure 5.
(A) Opened wound after Chopart amputation in Case 6. (B) a. Removed mold; b. Biosheet cut and opened. Upper right shows inner surface and lower right shows outer surface. (C) a. Debrided wound; b. three Biosheets applied; c. wound covered by an antimicrobial acetylcellulose dressing (Sorbact).
Figure 5.
(A) Opened wound after Chopart amputation in Case 6. (B) a. Removed mold; b. Biosheet cut and opened. Upper right shows inner surface and lower right shows outer surface. (C) a. Debrided wound; b. three Biosheets applied; c. wound covered by an antimicrobial acetylcellulose dressing (Sorbact).
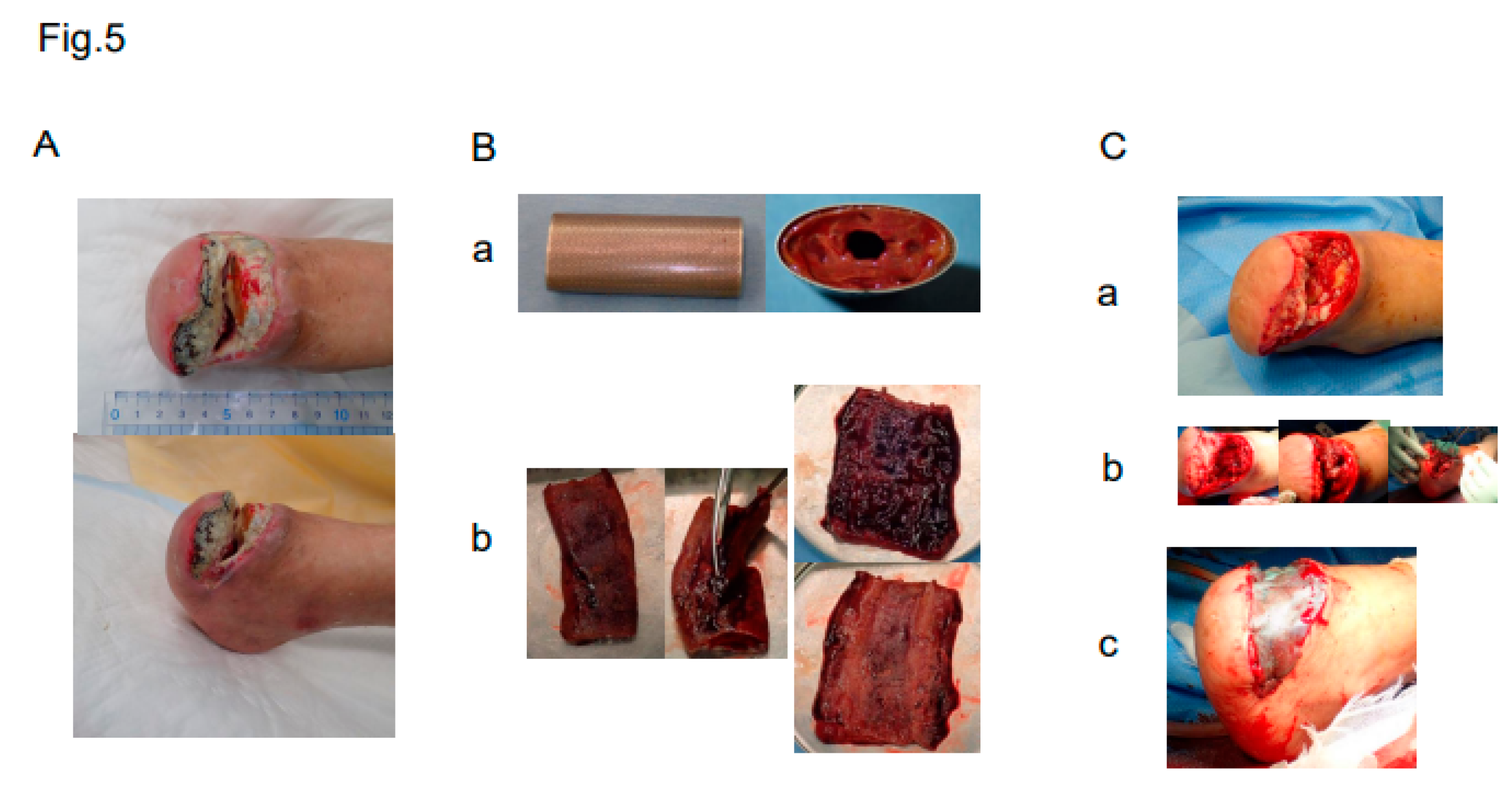
Figure 6.
Post-operative course in Case 6. Wound closed in five months.
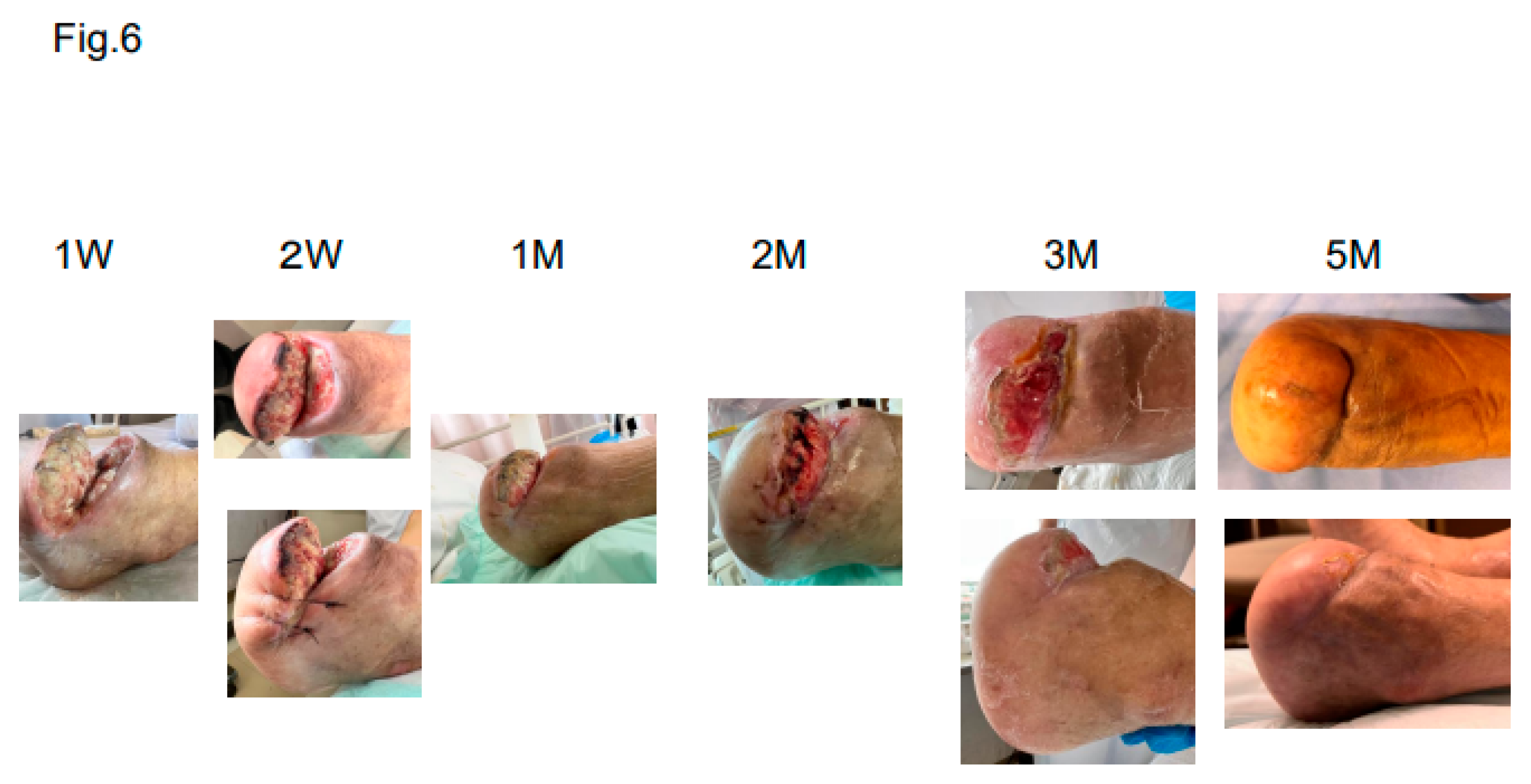
Figure 7.
Summary of 7 Cases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



