Submitted:
21 February 2024
Posted:
25 February 2024
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Vaccine hesitancy was one of the problems India faced after the COVID-19 vaccine roll-out. Earlier studies carried out to understand the perception of people towards the vaccine were mainly based on online or offline community-based surveys. These studies do not help to understand the actions taken by people towards vaccination. Hence, this study has been designed to understand the exact behaviour of people toward the vaccine. Methods: The study population is divided into three age groups, 18+ years, 12-14 years, and 15-18 years. The data analysis has been done using cumulative coverage of vaccines in the said age groups. Results: The study shows a substantial population has missed second and booster doses of vaccine at the state, regional, and national levels in all three three-age groups. Even for the states that have shown the smallest number of people who missed their dose, their number is in the thousands. Conclusion: Further research is needed to know, in total population, how many people have not even taken a single dose of vaccine. Policy-level efforts are needed to cover the entire population of the country for at least a single dose and vulnerable population, not only for the primary series (1st and 2nd dose) but also for the booster dose of the COVID-19 vaccine.
Keywords:
COVID-19
; India
; pandemic
; viruses
; vaccines
Introduction
COVID 19-vaccines are effective at protecting people from getting seriously ill, being hospitalized, and dying (1, 2, 3). India began its vaccination program on 16 January 2021 with the AstraZeneca vaccine (Covishield) and the indigenous Covaxin. Later on, other vaccines like Sputnik V and Corbevax were also approved for emergency use (4).
COVID-19 incidence rate was ninefold higher in the unvaccinated than those who received two doses (76 per 1000 person-months). One-dose recipients had shown 25 cases per 1000 person-months whereas two-dose recipients showed 9 per 1000 person-months (5). This shows taking a second dose of the COVID-19 vaccine is important to bring down the incidence rate of the disease.
Vaccine effectiveness may wane over time since the receipt of the second dose of the vaccines (6, 7, 8, 9, 10). Waning is greater in older adults and in those in a clinical risk group (11, 12). The real-world evidence suggests substantially increased protection from the booster vaccine dose against mild and severe disease irrespective of the primary course-1st and 2nd Covid vaccine doses (13,14). This shows that people need to take not only a second dose of their vaccine course but also a booster dose.
Vaccine rollout in India faced many practical problems like political polarization (15), vaccine shortage (16), misinformation and rumours (17), and challenges with registration and appointments (18, 19).
Vaccination coverage is a widely used indicator of vaccination programme strengths and weaknesses and of access to health care (20). Hesitancy towards the newly developed COVID-19 vaccines was a global phenomenon (21, 22, 23, 24, 25). Approximately eighteen systematic studies were carried out to understand the perception of Indian people toward the COVID-19 vaccine.
Most of these studies were pan-India studies carried out by online surveys (26, 27, 28, 29, 30, 31, 32). Few studies were carried out at the community level for specific states (33, 34, 35, 36, 37, 38, 39). There were a couple of studies focused on healthcare workers to understand their perception of the COVID-19 vaccine (40, 41).
Online surveys have their own set of limitations, inability to connect with people from remote areas (42, 43), high chances of survey fraud (44, 45), sampling issues (46, 47), response bias (48, 49), survey fatigue (50), increase in errors (51), a large number of unanswered questions (52), and difficult to interpret the sentiments behind answers (53).
All the earlier studies carried out to understand the perception of people towards the COVID-19 vaccine are questionnaire-based online surveys which do not help to understand the exact action taken by people towards immunization. It is not clear whether the person who took the first dose of the vaccine has taken the second and booster dose or not. In this study, the number of doses of the COVID-19 vaccine administered in the population will help us to understand the exact behaviour of the people towards the vaccine.
All the earlier studies carried out on the Indian population to understand their perception towards the COVID-19 vaccine have shown varying degrees of hesitancy towards the vaccine. Even if the majority of Indians would accept the vaccine, given the large population of India, a small proportion of hesitant individuals would translate to millions of unvaccinated individuals. It remains unclear exactly how many individuals have taken their primary course and booster of vaccines in India.
Earlier studies in the Indian population were focused on the acceptance or hesitancy of the people towards vaccines. Here systematic study has been carried out to understand the attitude of people towards the first dose, second dose, and booster dose of the COVID-19 vaccine. In this study, the number of doses administered in the population is used to understand the behaviour of the people towards COVID-19 vaccine which will give us a better idea than questionnaire-based surveys. Earlier studies were mostly regional or state-specific. In this paper, a nationwide study is carried out for every state and union territory. The study population here is not random but it is divided into subgroups like 18+ years, 15-18 years, and 12-14 years for primary courses whereas they are broadly divided into 18-59 years and 60+, HCW, and FLW for a booster dose.
The data derived from this study will help in planning strategic measures and policy decisions to enhance the rate of COVID-19 vaccination in India. The results of this study will be of great help in the future emergency of COVID-19. The national level and state level analysis done here can be used to develop targeted behaviour change communication campaigns.
Materials and Methods
The cumulative Coverage Report of COVID-19 vaccination is taken from the Ministry of Health and Family Welfare (MoHFW), Government of India. The data for the study was collected on 23rd December 2022 (At IST 7 am). https://www.mohfw.gov.in/pdf/CummulativeCovidVaccinationReport23Dec2022.pdf.
From 24th December 2022, the Ministry of Health & Family Welfare has implemented fresh guidelines for international arrivals in the context of COVID-19 in light of the increasing trajectory of COVID-19 cases being noted in some countries across the world, mainly neighbouring China.
For ease of analysis, the country is divided into seven main regions- 1)The northern region- six states- Himachal Pradesh, Punjab, Uttarakhand, Haryana, Delhi, and Uttar Pradesh; 2) the Southern region contains five states- Andhra Pradesh, Karnataka, Kerala, Tamil Nadu, and Telangana; 3)Eastern region is consisting of the states of Bihar, Jharkhand, Odisha and West Bengal; 4)Western region states are Rajasthan, Maharashtra Gujarat and Goa; 5) Central region consists of two states- Madhya Pradesh and Chhattisgarh; 6)North-East region includes-eight States viz. Arunachal Pradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim, and Tripura; 7)Union territories-Andaman and Nicobar islands, Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Lakshadweep, Puducherry, Ladakh and Jammu & Kashmir.
The population under the study is divided based on doses of vaccine administered. The population in which the first and second dose of vaccine is administered is divided into the sub-groups)18+ yrs, 2)15-18 yrs, 3)12-14 years. For the third or precautionary or booster dose, the population is divided into two sub-categories -1) 18-59 years and 2) Vulnerable population- 60+ years, Health Care Workers (HCW) and Front-Line Workers (FLW). The data for miscellaneous doses has been added in a separate table to avoid confusion during analysis.
The difference between the first dose and second dose of the COVID-19 vaccine administered in the population is calculated by simple mathematical operations. Total booster doses given to the 18-59 years population and vulnerable population are calculated by adding their values. The values obtained after calculations are rounded off to the nearest place value.
Results
When the COVID-19 vaccine coverage data was analyzed at the country level, it showed that ~920 million doses had been administered in 18+ years age group as the first dose (Table 1). But out of this 920 million, only 870 million have taken the second dose (Figure 1). That means 60 million people have missed their second dose of the vaccine. The difference in first and second doses administered in the 15-18 years and 12-14 years age group categories has shown a difference of around 8.5 million and 8.8 million respectively.
The results for total booster doses administered in the population showed only 220 million as compared to ~920 million for the first dose of vaccine. Only 70 million booster doses were administered in vulnerable populations all over the country (Figure 2).
When the vaccine coverage for the northern region of India is analyzed, the data entry error for 18+ population has been observed for Jammu and Kashmir. For these states, the number of second doses is more than the first one. Hence that reading was ignored. Out of 6 states of North India, Uttar Pradesh has administered the highest number (390 million) of total vaccines. Whereas the state of Himachal Pradesh has administered the lowest number of doses (15 million). In all the states of northern India, a considerable population in every age group has missed the second dose of vaccine. The highest number is seen in people of Uttar Pradesh (6.3 million) missed the second dose in the age group 18+, 0.9 million and 0.83 million missed their second dose in 15-18 years and 12-14 years respectively. These numbers are quite high if compared to the rest of the states of the northern region of India. The next state to Uttar Pradesh which missed the second dose in 18+ population is Haryana (3.2 million) followed by Punjab (2.8 million) and then Delhi (2.25 million). Uttarakhand (20 million) and Himachal Pradesh (15 million) have comparatively lower numbers for total doses administered as well as lower population (0.2 million per state) who missed the second dose of vaccine (Table 2).
When the data was analyzed for total booster doses administered in the population, Uttar Pradesh showed the highest number (45 million) in the northern region of India. But these doses are just one-third of the first dose. A more or less similar trend is noticed for the other states of the Northern region for booster doses. The highest number of booster doses in the vulnerable population (9.2 million) is seen in Uttar Pradesh only. This number is almost eight to nine times higher as compared to other states of north India.
In the southern region of India, a total of 491 million COVID-19 vaccine doses were administered (Table 3). For the states of Andhra Pradesh and Karnataka, the number of second doses administered in the age group 18+ population is more, hence considering it as a data error by MoHFW, these readings were ignored. In Kerala, a total 57 million doses were administered but 3.2 million in 18+ population, 0.36 million in 15-18 years and 0. 29 million in the 12-14 years population have missed the second dose of vaccine. A total of 3.06 million booster doses were administered in Kerala which is far less compared to the first dose of vaccine.
In Tamil Nādu, 127 million total vaccine doses were administered. 3.2 million people missed the second dose in the 18+ population. Whereas 0.4 million and 0.45 million people in the age group 15-18 years and 12-14 years have missed their second dose respectively. 9 million people in the 18+ population and vulnerable population have taken booster doses in Tamil Nādu.
In Telangana, a total of 77 million vaccine doses were administered. 29 million people in the 18+ population took the first dose but out of those who took the first dose, 0.55 million people missed their second dose. In the age group 15-18 years, 0.1 million people missed their second dose whereas 0.2 million missed the second dose in the 12-14 years of age group. In Telangana, the total booster doses administered were 13 million.
A total of 436 million COVID-19 vaccine doses were administered in the eastern region of India (Table 4). In Bihar and West Bengal, 155 million doses in each state were administered followed by Odisha (81 million) and Jharkhand (43 million). In Bihar and West Bengal, approximately 15 million booster doses in each state were administered followed by Odisha (13 million) and Jharkhand (1.95 million). In Bihar, 3.8 million, 0.89 million, and 0.88 million missed their second dose in the age group 18+, 15-18 years, and 12-14 years respectively.
In Jharkhand, 5.26 million, 0.49 million, and 0.44 million have missed the second dose in the age group 18+, 15-18 years, and 12-14 years respectively. In Odisha, the number who missed the second dose (1.5 million) is less as compared to the other three states of the region. In West Bengal, in contrast, 5.7 million people in the age group 18+ have missed their second dose. 0.56 million people in the age group 15-18 years and 12-14 years have missed their second dose of vaccine.
A total of 421 million vaccine doses have been administered in the western region of India (Table 5). The numbers of Gujarat for the second dose in the 18+ population are higher than the first dose. Considering it as an error, these figures are ignored. The highest doses in the western region 177 million were administered in the state of Maharashtra. It is followed by Gujarat (127 million) and then Rajasthan (115 million). Only 2.8 million doses were administered in Goa.
In Rajasthan, 51.1 million doses were administered as first dose but 4.59 million in 18+ population, 0.66 million in 15-18 years, and 0.84 million in 12-14 years missed their second dose. In Maharashtra, 13 million in 18+ population, 1.01 million in 15-18 years, and 1.02 million in 12-14 years have missed their second vaccine dose. In Goa, only 1.35 million people in the 18+ population took the first dose of the vaccine but 0.13 million missed their second dose. 7181 and 6626 respectively in the age group 15-18 years and 12-14 years missed the second dose. Only 0.13 million people took the booster dose in Goa.
The central region of India consists of Chhattisgarh and Madhya Pradesh where collectively 182 million doses were administered (Table 6). In Chhattisgarh (18 million) and in Madhya Pradesh (54 million) first doses were administered, out of which 0.4 million and 0.1 million people respectively missed their second doses of the COVID-19 vaccine. In Chhattisgarh, 0.18 million people in the age group 15-18 years and 0.32 million in 12-14 years have missed their second dose. In Madhya Pradesh, 0.7 million in 15-18 years and 0.71 million in 12-14 years have missed their second dose. In Chhattisgarh, 7.5 million people and in Madhya Pradesh, 13 million people were immunized with booster doses.
In the North-East region of India (Table 7), the highest COVID-19 vaccine doses (50 million) were administered in Assam whereas the lowest doses (1.36 million) were administered in Sikkim. Out of all the eight states except Sikkim, populations ranging from 0.11 million to 2.0 million have missed their second dose in the 18+ population. Assam is the state that has missed the highest number of second doses in the age group 15-18 years (0.29 million) and 12-14 years (0.39 million).
Among India's seven Union Territories, a data entry error has been noticed for the Andaman & Nicobar Islands. The highest number of vaccine doses were administered in Chandigarh (2.28 million) followed by Puducherry (2.27 million). The lowest numbers were administered in Lakshadweep (0.14 million). The highest booster doses (0.4 million) were administered in the population of Puducherry out of all the Union territories of India (Table 8). A total of 5295713 miscellaneous doses were given in the entire country which was used only for country-level analysis and not for regional-level analysis (Table 9).
Discussion
In the present analysis, we first explored the number of vaccine doses administered in the population at the country level as primary courses in the age groups, 18+ population, 15-18 years population, and 12-14 years population. A significant number of the population missed the second dose of the COVID-19 vaccine administered in all three age groups. Similar results were noticed in the other studies where persons who start the primary series are presumably amenable to initial vaccination but may then either delay completing or may fail to complete the series (54).
Delayed or missed recommended COVID-19 vaccine doses can hamper national efforts to reduce COVID–19–associated illness, hospitalization, and death (55,56,57). More information about this population is valuable for addressing second-dose vaccination barriers and devising interventions to increase primary series completion.
When the data for booster doses administered at the national level was studied, a considerable number of people from vulnerable populations like the 60+ population, Health Care Workers, and Front-Line Workers have not taken booster doses. The total booster doses in the overall population of 18+ and vulnerable populations is far lower as compared to the first vaccine dose (Table 1).
Compared with booster dose recipients in 18–59 years of age, recipients >60 years of age, HCW, and FLW were less likely to have missed a second dose. Persons in older age groups had more time to complete their vaccination, given the prioritization when the COVID-19 vaccine first became available. Older adults also are at higher risk for severe COVID-19 illness and may have been more motivated to become fully vaccinated (58). Compared with unvaccinated HCWs, HCWS who have had either one or two doses of vaccines were less likely to have moderate to severe disease or seek treatment at the hospital (59).
The findings of this study clearly show that people in any age group including vulnerable groups are reluctant to take a second dose as well as a booster dose of COVID-19. This trend is worrisome especially for the vulnerable population as there is clear evidence from the studies of Horne et. al., 2022 and Nanishi et.al, 2022 that waning vaccine effectiveness is greater in older adults and in those in a clinical risk group. Andrews et.al, 2022 and Shekhar et. al., 2021 have proved that booster doses give substantially increased protection against mild and severe disease.
In the region-wise analysis, the trend in northern, southern, western, eastern, central, and north-east regions of India matches with a national trend of vaccine coverage. Where a substantial population has missed the second dose in all three age groups. At the same time, a substantial population has not taken their booster doses, including vulnerable populations.
In Uttar Pradesh under the northern region, the highest number of total vaccine doses as well as booster doses were administered. But this is the same state which has shown the highest population in the region which missed the second dose of vaccine. In Uttar Pradesh, two-thirds population out of those who took the first dose have missed the booster dose. The reason behind the highest number of vaccine doses administered in Uttar Pradesh may be that it is the country's highest populated state (60). Another possible reason might be, that Uttar Pradesh was one of the ten worst-hit states of India during the second wave of COVID-19, and in the wake of a resurgence in the number of new cases, the decision to speed up the process of vaccination has been taken by the government (61).
The results for Delhi, being the national capital were, expected to be better, but the large population there too missed their second and booster dose. This result might be supported by the study where 39.1% of the population of Delhi has shown concern about the safety of the vaccine (62). Himachal Pradesh and Uttarakhand have shown the lowest number of doses administered compared to the other states of the northern region of the country. The possible reason behind the small number might be the small population of these states.
Seeing the geographical difficulties of the North-East region of the country, accessibility of the vaccine to the people of this area was an issue, which makes the data of the region important. Here delivering the vaccine was a bigger challenge for the government than the perception of the people towards the COVID-19 vaccine. Similar challenges were also seen for the Union territory of Andaman & Nicobar Islands. However, analysis of this study shows that enough total vaccine doses were administered throughout the North-East region as well as in challenging Union Territories. The reason behind this might be the Indian Council of Medical Research’s drone (i-Drone) response and outreach in North East delivered doses of COVID-19 vaccine (63).
This finding is consistent with the reports from other studies where when compared with first-dose recipients were more likely to have delayed or missed the second dose (64). Our research findings are also consistent with the Government of India’s Economic Survey, 2023. As per the survey report, till December 2022, overall, 91.65 l million people were vaccinated with the first dose and 76.565 million with the second dose (65). This report clearly shows the substantial population has missed the second dose when compared with the first dose. Many factors may contribute to this disparity. Fear of side effects is one of the reasons attributed to the higher percentage of delayed second doses among the recipients (66). Another possibility behind the lower second dose mentioned is that lower-income persons may be concerned about taking time off work to get vaccinated and to recuperate should they experience side effects (67,68).
Previous research found that COVID-19 vaccine coverage was lower in rural areas than in urban areas (69). A similar possibility might be there in the case of the Indian scenario. Also, these observations of the present study highlight the value of knowing which barriers prevent timely second-dose completion or booster dose for recipients.
One peculiar problem of data has been noticed for some of the states where the number of second doses is higher than the first one. There is a possibility of human error during data entry at MoHFW website. Unfortunately, data entry errors can have deleterious effects on research results. Simple data entry errors – such as typing an incorrect number can ruin the results of a statistical analysis (70). Hence the data for these states is mentioned but not considered for the conclusion. This needs further correction by MoHFW.
This is a systematic study based on data on the total number of vaccines administered at the national, regional, and state levels. This study highlights the number of people who took their first dose of the vaccine but missed their second dose in three age groups, 18+, 15-18 years, and 12-14 years. This also gives the idea of how many people have taken booster doses in the 18-59 years population and vulnerable population. But there is a need to further carry out the research to understand out of the total population of the state, how many people have not taken even a single dose of COVID-19 vaccine.
Conclusion
The national, regional, and state-level analyses of COVID-19 vaccine coverage have shown that a substantial population has missed the second dose of the vaccine. Even for the states where this number is smallest, that number is in thousands. In every state, 50-75% of the population has not taken booster doses out of those who took the first dose of primary series. One of the limitations we noticed here is discrepancies in data for some states. There is a need for further research to know how many people have not even taken a single dose of vaccine. The policy level changes are needed to cover the entire population of the country for at least a single dose and vulnerable populations for booster doses of the COVID-19 vaccine.
Ethics Approval and Consent to Participate
Not Applicable.
Supplementary Materials
Metadata-Cumulative Coverage Report of COVID-19 vaccination is taken from the Ministry of Health and Family Welfare (MoHFW), Government of India. https://www.mohfw.gov.in/pdf/CummulativeCovidVaccinationReport23Dec2022.pdf.
Author Contributions
All authors have agreed to the submission of this manuscript.
Funding
Not Applicable.
Acknowledgments
Not Applicable.
Conflicts of Interest
The authors declare no competing interests.
References
- Cabezas C, Coma E, Mora-Fernandez N, Li X, Martinez-Marcos M, Fina F et al. Associations of BNT162b2 vaccination with SARS-CoV-2 infection and hospital admission and death with COVID-19 in nursing homes and healthcare workers in Catalonia: prospective cohort study. BMJ. 2021;374:n1868. [CrossRef]
- Hyams C, Marlow R, Maseko Z, King J, Ward L, Fox K, et al. Effectiveness of BNT162b2 and ChAdOx1 nCoV-19 COVID-19 vaccination at preventing hospitalisations in people aged at least 80 years: a test-negative, case-control study. Lancet Infect Dis. 2021;21(11):1539-48. [CrossRef]
- Lopez Bernal J, Andrews N, Gower C, Gallagher E, Simmons R, Thelwall S, et al. Effectiveness of COVID-19 vaccines against the B.1.617.2 (delta) variant. N Engl J Med. 2021;385(7):585-94. [CrossRef]
- VaccinationMoHFWhttps:. Available from: http://www.mohfw.gov.in/pdf/COVIDVaccinationBooklet14SEP.pdf.
- Tsundue T, Namdon T, Tsewang T, Topgyal S, Dolma T, Lhadon D, et al. First and second doses of Covishield vaccine provided high level of protection against SARS-CoV-2 infection in highly transmissible settings: results from a prospective cohort of participants residing in congregate facilities in India. BMJ Glob Health. 2022;7(5):e008271. [CrossRef]
- Goldberg Y. Yair, Mandel, Micha, Bar-On, Yinon M, Bodenheimer Omri, Freedman Laurence, et al. Waning immunity of the BNT162b2 vaccine: a nationwide study from Israel. N Engl J Med. 2021;385:e85.
- Khoury DS, Cromer D, Reynaldi A, Schlub TE, Wheatley AK, Juno JA, et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med. 2021;27(7):1205-11. [CrossRef]
- Levin EG, Lustig Y, Cohen C, Fluss R, Indenbaum V, Amit S et al. Waning immune humoral response to BNT162b2 COVID-19 vaccine over 6 months. N Engl J Med. 2021;385(24):e84. [CrossRef]
- Tang P, Hasan MR, Chemaitelly H, Yassine HM, Benslimane FM, Al Khatib HA et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nat Med. 2021;27(12):2136-43. [CrossRef]
- Chemaitelly H, Yassine HM, Benslimane FM, Al Khatib HA, Tang P, Hasan MR et al. mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar. Nat Med. 2021;27(9):1614-21. [CrossRef]
- Horne EMF, Hulme WJ, Keogh RH, Palmer TM, Williamson EJ, Parker EPK et al. Waning effectiveness of BNT162b2 and ChAdOx1 COVID-19 vaccines over six months since second dose: OpenSAFELY cohort study using linked electronic health records. BMJ. 2022;378:e071249. [CrossRef]
- Nanishi E, Levy O, Ozonoff A. Waning effectiveness of SARS-CoV-2 mRNA vaccines in older adults: a rapid review. Hum Vaccin Immunother. 2022 Nov 30;18(5):2045857. [CrossRef]
- Shekhar R, Garg I, Pal S, Kottewar S, Sheikh AB. COVID-19 vaccine booster: to boost or not to boost. Infect Dis Rep. 2021;13(4):924-9. [CrossRef]
- Andrews N, Stowe J, Kirsebom F, Toffa S, Sachdeva R, Gower C et al. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat Med. 2022;28(4):831-7. [CrossRef]
- Sarkar J. Is lockdown an effective strategy to control infections like COVID-19? Might be! – shows this new study from Pune. Analysis. 2022.
- Ravi D. COVID-19 in India vaccine shortages are leading to discrimination in access. BMJ. 2021:1-5.
- Vaghela G, Narain K, Isa MA, Kanisetti V, Ahmadi A, Lucero-Prisno DE III. World’s largest vaccination drive in India: challenges and recommendations. Health Sci Rep. 2021;4(3):e355. [CrossRef]
- Thiagarajan K. Why is India having a COVID-19 surge? Br Med J. 2021;373:n1124. [CrossRef]
- Chakraborty C, Sharma AR, Bhattacharya M, Agoramoorthy G, Lee SS. The current second wave and COVID-19 vaccination status in India. Brain Behav Immun. 2021;96:1-4. [CrossRef]
- Cutts FT, Claquin P, Danovaro-Holliday MC, Rhoda DA. Monitoring vaccination coverage: defining the role of surveys. Vaccine. 2016;34(35):4103-9. [CrossRef]
- Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775-9. [CrossRef]
- Sallam M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines. 2021;9(2):160. [CrossRef]
- Kreps S, Dasgupta N, Brownstein JS, Hswen Y, Kriner DL. Public attitudes toward COVID-19 vaccination: the role of vaccine attributes, incentives, and misinformation. npj Vaccines. 2021;6(1):73. [CrossRef]
- Rzymski P, Zeyland J, Poniedziałek B, Małecka I, Wysocki J. The perception and attitudes toward COVID-19 vaccines: A cross-sectional study in Poland. Vaccines. 2021;9(4):382. [CrossRef]
- Dhalaria P, Arora H, Singh AK, Mathur M, S AK. COVID-19 Vaccine Hesitancy and Vaccination Coverage in India: an Exploratory Analysis. Vaccines (Basel). 2022 May 9;10(5):739. [CrossRef]
- Chandani S, Jani D, Sahu PK, Kataria U, Suryawanshi S, Khubchandani J et al. COVID-19 vaccination hesitancy in India: state of the nation and priorities for research. Brain Behav Immun Health. 2021 Dec;18:100375. [CrossRef]
- Kishore J, Venkatesh U, Ghai G, Heena KP, Kumar P. Perception and attitude towards COVID-19 vaccination: A preliminary online survey from India. J Fam Med Prim Care. 2021 Aug;10(8):3116-21. [CrossRef]
- Bharadwaj AH, Ramachandra SC, Devaraju A, Nataraj SM, Vishwanath P, Prashant A. Perception of Indian citizens toward the available COVID-19 vaccines: need to create increased awareness. Perspect Clin Res. 2021 Oct-Dec;12(4):236-7. [CrossRef]
- Goel, Priya, Bansal, Monika. Perception and attitude of Indian population towards COVID-19 vaccines. J Cardiovasc Dis Res (J Cardiovasc Dis Res). 2021;12(5):343-50.
- Das B, Padhye A. Public perception and potential acceptance of COVID-19 vaccine in India. public Health Rev: Int J Public Health Res. 2021;8(2):23-31. [CrossRef]
- Mishra S, Verma A, Meena K, Kaushal R. Public reactions towards COVID-19 vaccination through twitter before and after second wave in India. Soc Netw Anal Min. 2022;12(1):57. [CrossRef]
- Sanghavi N, Neiterman E. COVID-19 vaccine hesitancy in middle-aged and older adults in India: A mixed-methods study. Cureus. October 16, 2022;14(10):e30362. [CrossRef]
- Danabal KGM, Magesh SS, Saravanan S, Gopichandran V. Attitude towards COVID 19 vaccines and vaccine hesitancy in urban and rural communities in Tamil Nadu, India – a community based survey. BMC Health Serv Res. 2021;21(1):994. [CrossRef]
- Raju GodasiG, Raj Kiran D, Salaam MA, Sankar PasamR, Sri Lakshmi T. Attitude towards COVID-19 vaccine among the general public in south India: A cross sectional study. 2021;22(1):28-35.
- Barigela SK, Galimudi RK, Kadarla S, Rani DN, Reddy PP, Jangala M et al. Knowledge, attitude and perceptions towards COVID-19 vaccination among south Indian (Telangana) population - A cross sectional study. Arch Clin Med Case Rep. 2022;6:350-69.
- Surapaneni KM, Kaur M, Kaur R, Grover A, Joshi A. The impact of COVID-19 vaccine communication, acceptance, and practices (CO-VIN-CAP) on vaccine hesitancy in an Indian setting: protocol for a cross-sectional study. JMIR Res Protoc. 2021;10(6):e29733. [CrossRef]
- Leelavathy M, Messaline S, Ramachandran D, Sukumaran A, Jose R, Noufel AN, Sunitha2, Divija1. Attitude towards COVID-19 vaccination among the public in Kerala: a cross sectional study. J Fam Med Prim Care, Anilbindu1, Regi1, Ahmed N.1. November 2021;10(11):4147-52. [CrossRef]
- Anil A, Sharafudeen S, Krishna A, Rajendran R, James JM, Kuruvilla S et al. Acceptance and concerns regarding COVID-19 vaccination in Kerala, India. Public Health Toxicol. 2021;1(1):5. [CrossRef]
- Mundackal R, Agarwal T, Murali K, Isaac NV, Hu P, Dhayal V et al. Prevalence & correlates of COVID-19 vaccine hesitancy in a rural community of Bengaluru district, southern India: A preliminary cross-sectional study. Indian J Med Res. May-June 2022;155(5&6):485-90. [CrossRef]
- Jain J, Saurabh S, Kumar P, Verma MK, Goel AD, Gupta MK et al. COVID-19 vaccine hesitancy among medical students in India. Epidemiol Infect. 2021;149:e132. [CrossRef]
- Bassi S, Bahl D, Thapliyal N, Maity H, Marathe SD, Prakshale BB, et al. COVID-19 vaccine knowledge, attitudes, perceptions and uptake among healthcare workers of Pune district, Maharashtra. J Glob Health Rep. 2022;6:e2022041. [CrossRef]
- Oliveri S, Lanzoni L, Petrocchi S, Janssens R, Schoefs E, Huys I et al. Opportunities and challenges of web-based and remotely administered surveys for patient preference studies in a vulnerable population. Patient Prefer Adherence. 2021 Nov 15;15:2509-17. [CrossRef]
- Wright KB. Researching Internet-based populations: advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J Comput Mediated Commun. Apr 1 2005;10(3):JCMC1034. [CrossRef]
- Teitcher JE, Bockting WO, Bauermeister JA, Hoefer CJ, Miner MH, Klitzman RL. Detecting, preventing, and responding to ”fraudsters” in internet research: ethics and tradeoffs. J Law Med Ethics. 2015 Spring;43(1):116-33. [CrossRef]
- Singh S, Sagar R. A critical look at online survey or questionnaire-based research studies during COVID-19. Asian J Psychiatry. 2021 Nov;65:102850. [CrossRef]
- Andrews D, Nonnecke B, Preece J. Electronic survey methodology: A case study in reaching hard-to-involve Internet users. Int J Hum Comput Interact. 2003;16(2):185-210. [CrossRef]
- Howard PEN, Rainie L, Jones S. Days and nights on the Internet: the impact of a diffusing technology. Am Behav Sci. 2001;45(3):383-404. [CrossRef]
- Andrade C. The limitations of online surveys. Indian J Psychol Med. 2020;42(6):575-6. [CrossRef]
- Menachemi N. Assessing response bias in a web survey at a university faculty. Eval Res Educ. 2010;24:1.
- de Koning R, Egiz A, Kotecha J, Ciuculete AC, Ooi SZY, Bankole NDA et al. Survey fatigue during the COVID-19 Pandemic: an analysis of neurosurgery survey response rates. Front Surg. 2021;8. [CrossRef]
- Bradley VC, Kuriwaki S, Isakov M, Sejdinovic D, Meng XL, Flaxman S. Unrepresentative big surveys significantly overestimated US vaccine uptake. Nature. 2021;600(7890):695-700. [CrossRef]
- Manfreda KL, Bosnjak M, Berzelak J, Haas I, Vehovar V. Web surveys versus other survey modes: A meta-analysis comparing response rates. Int J Mark Res. 2008;50(1):79-104. [CrossRef]
- Einola K, Alvesson M. Behind the numbers: questioning questionnaires. J Manag Inq. 2021;30(1):102-14. [CrossRef]
- Anders C. 15 million people in the U.S. have missed their second dose of the coronavirus vaccine, CDC says [cited Jan 30 2022]. Available from: https://www.washingtonpost.com/health/2021/07/02/missed-second-dose-covid19-vaccine.
- Bradley T, Grundberg E, Selvarangan R, LeMaster C, Fraley E, Banerjee D, et al. Antibody responses after a single dose of SARS-CoV-2 mRNA vaccine. N Engl J Med. 2021;384(20):1959-61. [CrossRef]
- Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, Kalkstein N, et al. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N Engl J Med. 2021;385(15):1393-400. [CrossRef]
- Doria-Rose N, Suthar MS, Makowski M, O’Connell S, McDermott AB, Flach B, et al. Antibody persistence through 6 months after the second dose of mRNA-1273 vaccine for COVID-19. N Engl J Med. 2021;384(23):2259-61. [CrossRef]
- Barek MdA, Aziz MdA, Islam MS. Impact of age, sex, comorbidities and clinical symptoms on the severity of COVID-19 cases: A meta-analysis with 55 studies and 10014 cases. Heliyon. 2020;6(12). [CrossRef]
- Jamil M, Bhattacharya PK, Barman B, Lynrah KG, Lyngdoh M, Tiewsoh I et al. COVID-19 vaccination status among healthcare workers and its effect on disease manifestations: A study from Northeast India. Cureus. 2022 May 20;14(5):e25159. [CrossRef]
- . [CrossRef]
- Juyal D, Pal S, Thaledi S, Pandey HC. COVID-19: the vaccination drive in India and the Peltzman effect. J Fam Med Prim Care. Nov 2021;10(11):3945-7. [CrossRef]
- Sharma A, Srivastava A. Perceptions and beliefs on vaccination for COVID-19 in Delhi: A cross-sectional study. Indian J Med Spec. 2021;12(3):151-4. [CrossRef]
- World Health Organization. India deploys drones to deliver COVID-19 vaccines; 2021.
- Meng L, Murthy NC, Murthy BP, Zell E, Saelee R, Irving M et al. Factors associated with delayed or missed Second-Dose mRNA COVID-19 vaccination among persons >12 years of Age, United States. Emerg Infect Dis. 2022 Aug;28(8):1633-41. [CrossRef]
- Government of India. p. 2022-23; 2023. Economic Survey. Available from: https://www.indiabudget.gov.in/economicsurvey/.
- Ismail L. Doctors say some are opting out of second vaccine dose in fear of side effects [cited Mar 4 2022]. Available from: https://www.newschannel5.com/news/doctors-say-some-are-opting-out-of-second-vaccine-dose-in-fear-of-side-effects.
- Goldman N, Pebley AR, Lee K, Andrasfay T, Pratt B. Racial and ethnic differentials in COVID-19-related job exposures by occupational standing in the US. PLOS ONE. 2021;16(9):e0256085. [CrossRef]
- Hamel L, Lopes L, Sparks G, Kirzinger A, Kearney A, Strokes M, et al. Kaiser Family Foundation. KFF COVID-19 vaccine monitor; October 2021 [cited Jan 30 2022]. Available from: https://www.kff.org/coronavirus-COVID-19/poll-finding/kff-COVID-19-vaccine-monitor-october-2021.
- Saelee R, Zell E, Murthy BP, Castro-Roman P, Fast H, Meng L, et al. Disparities in COVID-19 vaccination coverage between urban and rural counties—United States, December 14, 2020-January 31, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(9):335-40. [CrossRef]
- Barchard KA, Pace LA. Preventing human error: the impact of data entry methods on data accuracy and statistical results. Comput Hum Behav. 2011;27(5, September):1834-9. [CrossRef]
Figure 1.
Pie chart showing total number of COVID-19 vaccine doses administered in 18+ population (1st and 2nd doses).
Figure 1.
Pie chart showing total number of COVID-19 vaccine doses administered in 18+ population (1st and 2nd doses).
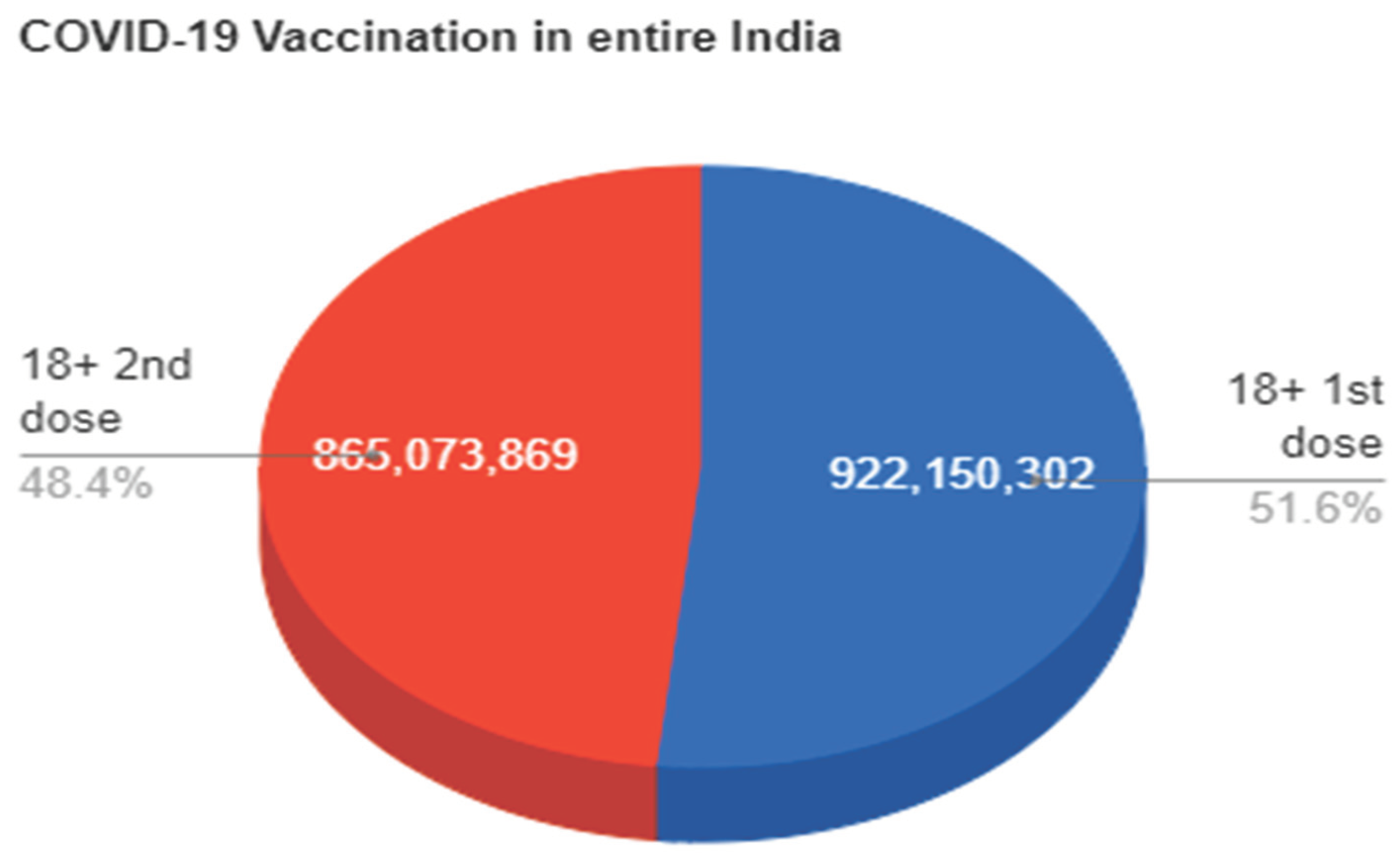
Figure 2.
Bar graph showing the total number of COVID-19 vaccine doses administered in the Indian population.
Figure 2.
Bar graph showing the total number of COVID-19 vaccine doses administered in the Indian population.
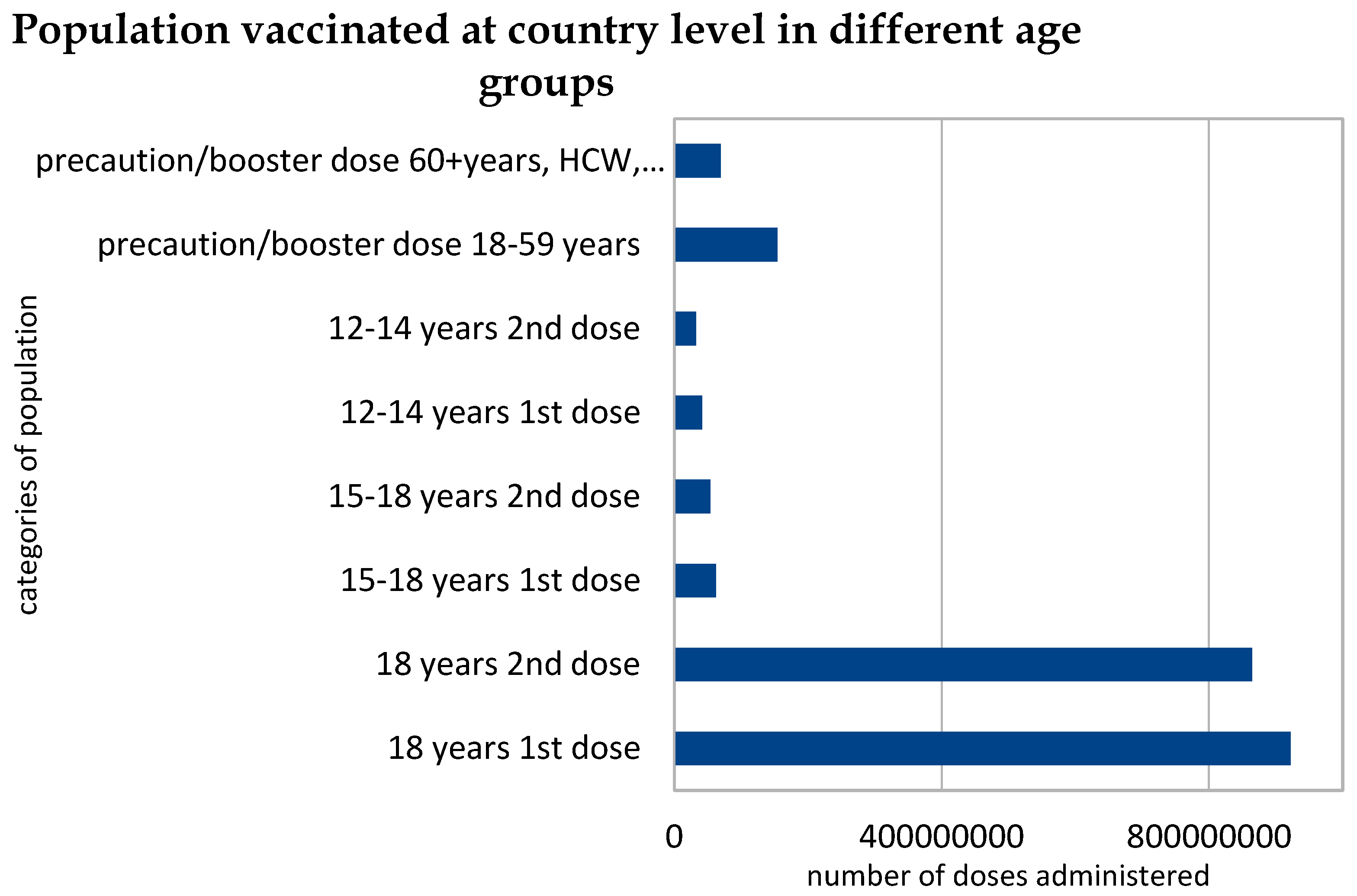

Table 1.
Cumulative coverage report of COVID-19 vaccination in entire India.
| India | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | ||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | ||
| 922150302 | 865073869 | 57076433 | 62111781 | 53629741 | 8482040 | 41288312 | 32518122 | 8770190 | 153962383 | 69565391 | 223527774 | 2200299901 | |
Table 2.
Cumulative coverage report of COVID-19 vaccination in the northern region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Himachal Pradesh | 6041524 | 5779764 | 261760 | 331637 | 308731 | 22906 | 272064 | 235002 | 37062 | 1480474 | 822929 | 2303403 | 15272125 |
| 2 | Punjab | 22351896 | 19601010 | 2750886 | 1116705 | 874903 | 241802 | 684126 | 497377 | 186749 | 794809 | 1039692 | 1834501 | 46960518 |
| 3 | Uttarakhand | 8179978 | 7940252 | 239726 | 532593 | 466493 | 66100 | 402309 | 315984 | 86325 | 1341674 | 866468 | 2208142 | 20045751 |
| 4 | Haryana | 21954733 | 18731652 | 3223081 | 1157529 | 767491 | 390038 | 559418 | 327204 | 232214 | 1249641 | 700969 | 1950610 | 45448637 |
| 5 | Delhi | 16599587 | 14348233 | 2251354 | 1008405 | 870305 | 138100 | 682753 | 489523 | 193230 | 2307012 | 1052355 | 3359367 | 37358173 |
| 6 | Uttar Pradesh | 154054737 | 147709294 | 6345443 | 14192132 | 13221527 | 970605 | 8708556 | 7874893 | 833663 | 35581131 | 9235711 | 44816842 | 390577981 |
Table 3.
Cumulative coverage report of COVID-19 vaccination in the southern region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Andhra Pradesh | 40642902 | 43548909 | -2906007 | 2535297 | 2527591 | 7706 | 1523355 | 1495429 | 27926 | 11700256 | 6579067 | 18279323 | 110552806 |
| 2 | Karnataka | 50014221 | 50452205 | -437984 | 2814308 | 2709721 | 104587 | 2324463 | 2149980 | 174483 | 5644638 | 4717480 | 10362118 | 120827016 |
| 3 | Kerala | 27013330 | 23790740 | 3222590 | 1322406 | 956252 | 366154 | 810901 | 511928 | 298973 | 850965 | 2215064 | 3066029 | 57471586 |
| 4 | Tamil Nadu | 56657297 | 53494530 | 3162767 | 2627003 | 2221961 | 405042 | 1916056 | 1460282 | 455774 | 6024065 | 3019271 | 9043336 | 127420465 |
| 5 | Telangana | 29606569 | 29051472 | 555097 | 1723557 | 1580580 | 142977 | 1106831 | 900504 | 206327 | 10512313 | 2700120 | 13212433 | 77181946 |
Table 4.
Cumulative coverage report of COVID-19 vaccination in the eastern region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Bihar | 62942587 | 59142450 | 3800137 | 6227260 | 5329417 | 897843 | 4287681 | 3402619 | 885062 | 11975634 | 3867313 | 15842947 | 157174961 |
| 2 | Jharkhand | 21297837 | 16037741 | 5260096 | 1586108 | 1091508 | 494600 | 1062295 | 621850 | 440445 | 1291246 | 662290 | 1953536 | 43650875 |
| 3 | Odisha | 31453540 | 29949586 | 1503954 | 2195508 | 1844375 | 351133 | 1600839 | 1206527 | 394312 | 9991894 | 3199032 | 13190926 | 81441301 |
| 4 | West Bengal | 67299545 | 61592577 | 5706968 | 3599204 | 3038845 | 560359 | 2621997 | 2058910 | 563087 | 10245585 | 5489990 | 15735575 | 155946653 |
Table 5.
Cumulative coverage report of COVID-19 vaccination in the western region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Rajasthan | 51101129 | 46504169 | 4596960 | 3570406 | 2905664 | 664742 | 2343781 | 1496486 | 847295 | 4362850 | 2993986 | 7356836 | 115278471 |
| 2 | Maharashtra | 84640930 | 71589342 | 13051588 | 4110678 | 3091658 | 1019020 | 2888879 | 1868124 | 1020755 | 4986703 | 4444638 | 9431341 | 177620952 |
| 3 | Gujrat | 49312972 | 49426218 | -113246 | 3131238 | 2903246 | 227992 | 1940872 | 1677615 | 263257 | 13419812 | 5931642 | 19351454 | 127743615 |
| 4 | Goa | 1354815 | 1224166 | 130649 | 51727 | 44546 | 7181 | 33265 | 26639 | 6626 | 60755 | 76549 | 137304 | 2872462 |
Table 6.
Cumulative coverage report of COVID-19 vaccination in the central region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Chhattisgarh | 18954784 | 18532212 | 422572 | 1234608 | 1050135 | 184473 | 1076048 | 752552 | 323496 | 5724368 | 1803871 | 7528239 | 49128578 |
| 2 | Madhya Pradesh | 54139637 | 54034786 | 104851 | 4194075 | 3469035 | 725040 | 2410903 | 1698621 | 712282 | 9846394 | 3786020 | 13632414 | 133579471 |
Table 7.
Cumulative coverage report of COVID-19 vaccination in north-east region of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Arunachal Pradesh | 860420 | 747123 | 113297 | 59080 | 44796 | 14284 | 40792 | 28406 | 12386 | 72076 | 58524 | 130600 | 1911217 |
| 2 | Assam | 22549847 | 20561284 | 1988563 | 1261430 | 965279 | 296151 | 999552 | 602277 | 397275 | 2081769 | 1259676 | 3341445 | 50281114 |
| 3 | Manipur | 1463972 | 1225590 | 238382 | 109282 | 68171 | 41111 | 75418 | 44329 | 31089 | 113999 | 165096 | 279095 | 3265857 |
| 4 | Meghalaya | 1332102 | 1024901 | 307201 | 76875 | 42605 | 34270 | 37364 | 19512 | 17852 | 30704 | 56987 | 87691 | 2621050 |
| 5 | Mizoram | 785749 | 668814 | 116935 | 60098 | 47010 | 13088 | 48360 | 33595 | 14765 | 79573 | 67619 | 147192 | 1790818 |
| 6 | Nagaland | 837775 | 684305 | 153470 | 59731 | 40145 | 19586 | 26012 | 19885 | 6127 | 26060 | 43640 | 69700 | 1737553 |
| 7 | Sikkim | 539927 | 509134 | 30793 | 30049 | 26515 | 3534 | 21899 | 19007 | 2892 | 158276 | 55637 | 213913 | 1360444 |
| 8 | Tripura | 2658796 | 2328462 | 330334 | 144797 | 115099 | 29698 | 112965 | 79612 | 33353 | 270651 | 204535 | 475186 | 5914917 |
Table 8.
Cumulative coverage report of COVID-19 vaccination in union territories of India.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Andaman and Nicobar Islands | 313284 | 320383 | -7099 | 19208 | 18860 | 348 | 15124 | 14041 | 1083 | 236936 | 53427 | 290363 | 991263 |
| 2 | Chandigarh | 1089211 | 917560 | 171651 | 57635 | 42055 | 15580 | 38117 | 25941 | 12176 | 48174 | 62852 | 111026 | 2281545 |
| 3 | Dadra & Nagar Haveli | 430279 | 332452 | 97827 | 19655 | 16329 | 3326 | 12365 | 7989 | 4376 | 69607 | 10342 | 79949 | 899018 |
| 4 | Daman & Diu | 300463 | 262473 | 37990 | 11852 | 10612 | 1240 | 7623 | 6937 | 686 | 67317 | 12142 | 79459 | 679419 |
| 5 | Lakshadweep | 56908 | 55992 | 916 | 2911 | 2780 | 131 | 1988 | 1723 | 265 | 15757 | 6949 | 22706 | 145008 |
| 6 | Ladakh | 219560 | 186920 | 32640 | 10068 | 9228 | 840 | 8627 | 7758 | 869 | 68544 | 53920 | 122464 | 564625 |
| 7 | Jammu & Kashmir | 9941538 | 10386743 | -445205 | 876032 | 861659 | 14373 | 553841 | 517810 | 36031 | 928479 | 669391 | 1597870 | 24735493 |
| 8 | Puducherry | 912821 | 801311 | 111510 | 50694 | 44614 | 6080 | 30873 | 21251 | 9622 | 302242 | 106698 | 408940 | 2270504 |
Table 9.
Cumulative coverage report of COVID-19 vaccination miscellaneous.
| S. No | State | Beneficiaries Vaccinated | Total doses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18+ population | 15-18 years | 12-14 years | Precaution/booster dose | |||||||||||
| 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 1st dose | 2nd dose | Difference | 18-59 years | 60 + years HCW, FLW | Total booster doses | |||
| 1 | Miscellaneous | 2243100 | 1579114 | 1473499 | 5295713 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



