
Submitted:
18 February 2024
Posted:
20 February 2024
You are already at the latest version
Abstract
Introduction: The trophoblast derived angiogenic factors are considered to play an important role in the pathophysiology of various complications of pregnancy. The aim of this study was to establish relationship between concentrations of soluble Human Leukocyte Antigen-G (sHLA-G) in maternal serum and amniotic fluid at 16-22 weeks of gestation and the sonographic measurements of the fetal and placental growth.
Materials and methods: sHLA-G in serum and amniotic fluid, as well as fetal biometric data and placental volume and perfusion indices were determined in 41 uncomplicated singleton pregnancies.
Results: The sHLA-G levels were unchanged both in amniotic fluid and in serum during mid-pregnancy. The sHLA-G level in serum correlated positively with amniotic sHLA-G level (β=0.63, p<0.01). Significant correlation was found between serum sHLA-G level and abdominal measurement (β=0.41, p<0.05) and estimated fetal weight (β=0.41, p<0.05). The amniotic sHLA-G level and placental perfusion (VI: β = -0.34, p<0.01 and VFI: β = -0.44, p<0.01, respectively) were negatively interrelated. A low amniotic sHLA-G level was significantly associated with nuchal translucency (r = -0.102, p<0.05).
Conclusions: sHLA-G assayed in amniotic fluid might be a potential indicator for placental function, whereas the sHLA-G level in serum can be a prognostic modality for feto-placental insufficiency.
Keywords:
soluble Human Leukocyte Antigen-G
; serum
; amniotic fluid
; fetus
; placenta
; sonography
1. Introduction
Human Leukocyte Antigen-G (HLA-G) is a member of non-classical human major histocompatibility complex class Ib family human major histocompatibility complex exhibiting a limited polymorphism. HLA-G is a key molecule in maternal-fetal immune tolerance maintaining immune homeostasis [1]. It has been described initially in extravillous trophoblast (EVT), but later has been identified cornea, erythroid precursors, pancreatic islets, endothelial cell precursors and erythroblasts and thymus, and displays different characteristics that of classical HLA-A, HLA-B and HLA-C (class Ia) molecules.
The HLA-G molecule constitutes of a heavy chain subunit comprised of three extracellular domains, located on chromosome 6, associated non-covalently with β2-microglobulin, encoded on chromosome 15. The HLA-G gene has 8 exons and 7 non-coding intervening sequences. Depending on the localization, membrane- bound and soluble HLA-G molecules are known due to seven different isoforms resulting from alternative splicing and differential association with 𝛽2-microglobulin. The membrane-bound subtypes are HLA-G1-4, which are expressed by ET cells in the placenta. The soluble forms released from the cell (HLA-G1, -G5, -G6, and -G7), due to the lack of the transmembrane and intracellular domains of membrane-bound HLA-G. The soluble subtypes are produced by various cells such as extravillous and villous cytotrophoblasts, chorion and amnion membranes, syncytiotrophoblasts, decidual stromal cells, fetal endothelial cells, and immune cells in the placenta [2,3].
Basically, HLA-G exhibits an immune tolerant function by direct inhibition of different immune-competent cells. The suppressing potential is mediated by HLA-G binding to its target receptors. The HLA-G receptors are inhibitory receptors such as killer cell immunoglobulin-like receptor 2DL4 (KIR2DL4) and immunoglobulin-like transcription receptor type 2 and type 4 (ILT2 and ILT4 respectively) [4,5].
Killer-cell immunoglobulin-like receptor (KIR) belongs to the family of type I transmembrane glycoproteins, which are mainly expressed on the plasma membrane of two subtypes of the natural killer (NK) cells: decidual natural killer (dNK) and peripherial blood natural killer (pbNK) cells. The ligands for several KIR proteins are subsets of HLA class I molecules, therefore KIR proteins are thought to play a significant role in down-regulation of maternal immune response. KIR2DL4 is a member of unusual killer cell immunoglobulin-like receptor (KIR) family in terms of its structure, expression, cellular localization and signaling properties. Unlike all other KIRs, which are expressed on the surface of NK cells, KIR2DL4 resides in endosomes. HLA-G, particularly the sHLA-G isoforms are solely ligands of the KIR2DL4 [4,5]. Importantly, HLA-G inhibits NK cell cytotoxicity and required to protect trophoblasts against NK cell-induced lysis [6] yet the mechanism by which EVTs uniquely express HLA-G remains unknown. Since NK cells constitute the predominant lymphocyte subset in the placenta, the pro-inflammatory/pro-angiogenic outcome of the interaction between KIR2DL4 and soluble HLA-G supports the role of KIR2DL4 in extensive remodeling of maternal vasculature during early weeks of pregnancy [7]. The ligand-receptor interaction activates the angiogenesis and vasculogenesis-related processes and inhibits the cytotoxic activity of the NK cells. sHLA-G isoforms induce trophoblast invasion and remodeling of spiral arteries by producing pro-inflammatory cytokines (IL-6, TNF-alfa) and proangiogenic factors (VEGF-A, MMP) by the NK cells [1,8]. sHLA-G promotes the secretion of IL-8 in NK cells and machrophages manifesting in trophoblast invasion. The activation processes encompass production of interferon- γ (IFN- γ) by the non-activated NK cells enhancing the paracrine secretion of HLA-G. The HLA-G induced NK-derived IFN-γ is essential for the decidual disorganization, vessel modification through promoting cell adhesion, smooth muscle proliferation [9].
Moreover, HLA-G interacts with ILT2 and ILT4 receptors, thereby inhibits cytotoxicity and enhances the production of anti-inflammatory cytokines (IL-4, IL-10, TGF-beta). ILT2 is on the surface of T cells, B cells, natural killer (NK) cells and antigen presenting cells (APCs), whereas ILT4 is exclusive to dendritic cells, macrophages/monocytes and APCs. HLA-G molecule binds with high affinity to both ILT2 and ILT4 inhibiting the maternal immune response [10]. The direct interaction of HLA-G with different immune cell subpopulations and endothel cells is accompanied by the generation and maintenance of tolerance at different stages of the immune response, e.g., differentiation, proliferation, cytolysis and cytokine secretion. On the other hand, HLA-G can be bound to ILT2 on dNK-cells and activates the PI3K-ACT signal transmission path. This interaction stimulates the production of growth promoting factors, such as pleiotrophin, osteoglycin and osteopontin, which are crucial for embryonic and fetal development [1,8]. Soluble forms have an antiproliferative effect on CD8+ T lymphocytes through promoting their apoptosis. Furthermore, they trigger the Th1-Th2 and Th17-regulatory T cells shift to reduce the maternal immune reaction [1,2].
Its major immunosuppression effected is exerted via bounding to its receptors appearing on the surface of immunocompetent cells (CD14+ monocytes NK, B, T cells and APCs) in any other organs as well apart from the placenta. HLA-G has been implicated in immune modulatory processes in organ transplantation, viral infections, cancer progression, autoimmunity, and even embryonic tissues. Both soluble and membrane-bound HLA-G have immunosuppressive effect and may contribute to tissue remodelling in both the maternal decidua and in tumors as it is protective against a graft-versus-host reaction since play a role in avoiding immune surveillance [11,12]. Both in cancers and in throphoblasts, the HLA-G may be important in tissue remodelling [1,11].
Under pathophysiological conditions HLA-G antigens are expressed on various types of malignant cells signifying that HLA-G antigen expression on tumors is a potent strategy to avoid immune surveillance. Several polymorphisms in the 3’UTR region condition changes in HLA-G expression (14bp and +3142C/G, among others), which have been associated with both the development and outcome of patients with different tumor types [11]. Since HLA-G antigens can be expressed on immune cells (including macrophages, neutrophils and NK cells) that infiltrates the tumor mass by chemoattraction to pro-inflammatory cytokines secreted by the cancer cells. The peripheral blood from cancer patients includes also HLA-G presenting cells [13], and HLA-G is suggested to impair the immune response to the tumor. HLA-G+ APC can inhibit the function of CD4+ T cells and induce their differentiation into regulatory T cells [14]. These immune cells contribute to tissue remodelling within cancer, including promotion of metastasis of tumor cells and angiogenesis, furthermore NK cells exhibit citotoxicity towards tumor cells [15]. The depletion of NK cells increases tumor growth and low pbNK cytotoxic activity is associated with increased risk of cancer [16], whereas NK cell presence in tumor is positively associated with prognosis [17]. Recent research describes the potential use of membrane-bound and soluble HLA-G as a prognostic biomarker to identify tumors and to assess disease stage, as well as on the use of HLA-G as a novel therapeutic target in cancer.
Some studies have found a reduced expression and polymorphism of HLA-G in pregnancy pathologies such as preeclampsia [18] or recurrent spontaneous abortion [19] in comparison with healthy placentas.
Soluble HLA-G can be detected both in maternal blood [7,8,9] and amniotic fluid [20]. In this study, we have investigated sHLA-G (sHLA-G1 and sHLA-G5) concentration in amniotic fluid and in maternal serum in mid-pregnancy. Considering uncomplicated pregnancies, we have investigated the correlations of sHLA-G levels and fetoplacental growth during mid-pregnancy.
2. Materials and Methods
2.1. Study Design
A prospective, cross-sectional cohort study was conducted in pregnant women undergoing amniocentesis at the Department of Obstetrics and Gynecology, University of Szeged, Hungary between January 2021 and May 2021. The demography of the study group was homogenic (Caucasian female subjects). During the study period, all singleton pregnancies with increased risk of chromosomal abnormality, where amniocentesis (AC) was performed between 16+0 and 22+0 weeks of gestation, were recruited into our study. The indications for AC were increased nuchal translucency (NT) at first trimester scan (≥2 MoM for gestational age (GA)) (n=2), chromosome aberration or gene disorder concerning the previous pregnancy (n=2), and advanced maternal age (n=37).
Exclusion criteria of the study were identified as follows: multiple pregnancies; fetal or neonatal structural or genetic anomaly, improper localization of the placenta for sonography (placenta praevia, posterior placenta), pathological placentation (placenta accreta spectrum), self-reported drug, alcohol, caffeine or nicotine abuse or exposure to circulatory medication (oxerutins, calcium dobesilate) and systemic disease (e.g., essential hypertension, any type of pregestational diabetes mellitus, autoimmune disease, vasculitis, hemophylia, thrombophylia, chronic infections).
In addition, women with complications during late pregnancy (gestational diabetes mellitus treated with diet, hypertension-related diseases, small for gestational age at delivery, large for gestational age at delivery) were excluded from the study. Therefore 41 healthy pregnancies were included in our study.
The study protocol was approved by the Clinical Research Ethics Committee of the University of Szeged (date of approval: 10 February 2017, reference number: SZTE 09/2017). The study was carried out according to the Principles of the Declaration of Helsinki. We obtained written informed consent from all participants.
2.2. Conventional 2-Dimensional (2-D) Sonographic Examinations
All pregnancies were dated by using the measurement of crown rump length (CRL) at nuchal screening. NT and anatomic assessment between 11+0 and 13+6 weeks were performed by utilizing conventional methods. Ultrasound examination took place before measuring AC to determine the number of fetuses, fetal biometry, fetal anomalies, placental location and the amount of amniotic fluid. Fetal weight was estimated according to the method of Hadlock et al.[21]. after measuring the necessary sonographic parameters (biparietal diameter, head circumference, abdominal circumference and femur length). Estimated fetal weight percentile was calculated according to the local standards [22]. The ultrasound investigations were conducted by J. S. and A. S.
2.3. Volume Acquisition
The images used for the determination of placental volume and 3-dimensional Power Doppler (3-DPD) indices were acquired at the time of the visit. All 3-D scans were performed by A. S. Voluson 730 Expert ultrasound machine (GE Medical Systems, Kretztechnik GmbH & Co OHG, Tiefenbach, Austria) equipped with a multifrequency probe (2–5 MHz) was used to acquire all images. Each sample was examined using 3D rendering mode, in which the color and gray value information was processed and combined to give a 3D image (mode cent; smooth: 4/5; FRQ: low; quality: 16; density: 6; enhance: 16; balance: 150; filter: 2; actual power: 2 dB; pulse repetition frequency: 0.9). We used fast low-resolution acquisition to avoid any kind of artifacts. The 3-D static volume box was placed over the highest villous vascular density zone at the umbilical cord insertion [23]. Each image was recovered from the disc in succession for processing. We recorded one sample from each patient during gestation.
2.4. Determination of Power Doppler Indices
The stored volumes were further analyzed using the virtual organ computer-aided analysis (VOCAL) program pertaining to computer software 4DView (GE Medical Systems, Zipf, Austria, version 10.4) by the same expert in 3-D analysis (A. S.). The image used for recovering from the hard disc was captured and processed using multiplanar system. The spherical sample volume was consistently 28 mL. The VOCAL program calculated automatically the grey- and color scale values from the acquired spherical sample volume in a histogram in all cases. The combined use of power Doppler with three-dimensional ultrasound provides the possibility of quantifying blood in motion within a volume of interest. Three indices were calculated, namely the vascularization index (VI), flow index (FI), and vascularization flow index (VFI), as estimates of the percentage of the volume filled with detectably moving blood. VI (expressed as a percentage) is the proportion of color voxels in the studied volume, representing the proportion of blood vessels within the tissue. FI (expressed as a scale of 0–100) is the average value of all color voxels, representing the average power Doppler amplitude within blood vessels. VFI (expressed as a scale of 0–100) is the average color value of all grey and color voxels, a product of the number of color voxels as a percentage and the relative amplitude of these voxels [24,25].
The intra-observer errors were evaluated by repeated measurements of 3-DPD indices at initiation of the study. The intra-class correlation coefficients for all Doppler indices were excellent (0.99) in case of all indices.
2.5. Amniocentesis Procedure
The patients were informed about the procedure and possible complications before a consent form was signed prior to the procedure. All procedures were performed by the same operator expert (J.S.) at the outpatient unit, who followed the standard protocol. A local antiseptic was applied to the skin. A 22-gauge spinal needle was inserted under continuous ultrasound guidance, and needle insertion through the placenta was avoided. Amniotic fluid (8–10 mL) was taken, and the first 2 mL of each sample was discarded to prevent contamination with maternal cells. Blood-contaminated amniotic fluid was not utilized. Fetal heart rate was evaluated after the procedure, and no stillbirth or premature rupture was observed. Following amniocentesis, anti-D immunoglobulin was administered, when it was necessary.
2.6. Samples
Amniotic fluid and maternal venous blood were collected from each patient at the time of amniocentesis. Blood samples were centrifuged at 3400 rpm for 15 minutes. Serum and amniotic fluid samples were stored at −80 °C until assay.
2.7. Enzyme-Linked Immunosorbent Assay (ELISA)
Human sHLA-G in maternal serum and amniotic fluid were determined by ELISA. The laboratory staff members who performed the assays were blinded to pregnancy outcome, and the clinician recruiting women did not participate at analyzing the samples.
Concentration of sHLA-G was measured using the kits from Elabscience Biotechnology Corporation (Houston, TX, USA). The sensitivity of assay was 0.38 ng/ml. The intra- and inter-assay coefficients of variation were <10% according to the manufacturer.
2.8. Data and Statistical Analysis
Statistical analyses were performed using SPSS version 23 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and categorical variables were expressed as numbers and percentages. The relationship between the level of sHLA-G and other continuous variables was assessed using univariate and multivariate regression analyses characterized by correlation coefficient (ß) and 95% confidence interval (CI). Multiple linear regression was adjusted for well-known confounders such as maternal age, body mass index (BMI) at the time of amniocentesis, number of previous pregnancies and gestational age at the time of amniocentesis, as these factors determine the actual placental volume and fetal weight. Paired samples t-test was applied to analyze the differences between serum and amniotic levels of the analytes. The two-tailed statistical significance level was set at 5% and p-values were adjusted using Holm–Bonferroni correction for multiple comparisons.
3. Results
Descriptive statistics are shown in Table 1. As expected by guidelines, amniocentesis has been proposed for pregnant women with advanced maternal age (above 37 years) and suspicion of aneuploidy. Mean maternal age (33.63 years) in our case group was minimally higher compared to the national average reference age at delivery, which was 29.1 years for primiparous women and 30.4 years for the total number of pregnant women in 2021 [26]. Women who participated in our study had a mean BMI of 26.4 kg/m2 and slightly overweighted and 29.3% of the participants were primiparous. Birth weights of our sample was also near to that of the national average of healthy pregnant. As expected, the birth weight of the offsprings very without extremities. Ultrasound characteristics are demonstrated in Table 2. Large NT was scarcely observed in our group (n=2). Mean gestational age at the time of amniocentesis was 18.4 weeks and mean gestational age at the time of delivery was 39.0 weeks (range: 37.0-41.0 weeks). Typically, all of the fetal sonographic measurements were with no outliers and with a low standard deviation (<1) explicating that the data are clustered tightly around the mean.
Table 3 gives an overview of the levels of angiogenic factors. The mean concentration was 53.39 ng/ml for sHLA-G in amniotic fluid and 51.05 ng/ml for sHLA-G in serum.
Figure 1 presents the levels of angiogenic factors in body fluids adjusted to the gestational age. The sHLA-G levels were steady during the gestational period, which was investigated in our study. The sHLA-G level in serum was significantly associated with sHLA-G level in amniotic fluid, both in the unadjusted (β=0.63, 95% CI= 0.30-0.72, p<0.01) and in the adjusted model (β=0.66, 95% CI= 0.32-0.74, p<0.01) controlled for age, BMI, previous parity and gestational age at amniocentesis.
Table 4 displays the sonographic correlates of sHLA-G levels. The sHLA-G serum concentration was significantly correlated positively with abdominal circumference percentiles in the unadjusted analysis (β=0.41, 95% CI= -0.08-0.75, p<0.05). Similarly, we found a significant interaction between sHLA-G levels in serum and the estimated fetal weight percentile (β=0.41, 95% CI= -0.02-0.84, p<0.05). An inverse correlation could be detected between sHLA-G level in serum and FI in the unadjusted linear regression model (β=-0.34, 95% CI= -3.58-0.46, p<0.05). Reduced nuchal translucency appears to be correlated with high sHLA-G level in amniotic fluid (β=-0.30, 95% CI= -21,73-0.04, p<0.05). Indirect correlations were observed between sHLA-G concentrations in amniotic fluid and placental perfusion [VI: univariate analysis: β=-0.34, 95% CI= -2.13-0.06, p<0.05, multivariate analysis: β=-0.38, 95% CI= -2.47-0.03, p<0.05; and VFI: univariate analysis: β=-0.44, 95% CI= -3.28-0.63, p<0.05, multivariate analysis: β=-0.51, 95% CI= -3.79-0.72, p<0.05].
4. Discussion
HLA-G is a molecule that was first known to confer protection to the fetus from destruction by maternal immune system, thus critically contributing to maternal-fetal immune tolerance. The appropriate vasculogenesis and angiogenesis have an important role in placental development. The trophoblast invasion and remodeling of spiral arteries are regulated by the balance and interaction between pro-angiogenic and anti-angiogenic factors. The imbalance of angiogenic factors can lead to gestational pathological conditions, such as gestational hypertension, preeclampsia and prematurity [8,20,27,28,29]
We have found a positive correlation between sHLA-G levels in serum and amniotic fluid, even when adjusted for confounders. sHLA-G in maternal circulation is secreted by EVT cells, while sHLA-G expressed by amniotic membrane is detectable in amniotic fluid, ensuring that it is involved in both local and systemic maternal immune modulation, which is in line with previous reports [19,20]. The association can be explained that the local and systemic immune response is in concordance in its extent. However, why the amniotic membrane cells secret the sHLA-G into the amniotic fluid is in line with the sHLA-G serum level is not understood, but maybe it is related to the size of the fetus. A larger of amniotic epithel cells area may present a higher cell mass that is interacting with a larger amount of immune cells.
Furthermore, HLA-G is primarily a checkpoint molecule. In our research, we have realized that sHLA-G levels in maternal serum and amniotic fluid are constant during mid-pregnancy, although maternal serum level has been decreased slightly and non-significantly.
Maternal serum level exhibits a positive correlation with fetal growth in terms of abdominal circumference and estimated fetal weight, which is expressed in percentiles after sonographic measurement. HLA-G levels in serum have a wide range of variety in a relatively short time period during gestation as published by others [30]. Furthermore, fetal growth percentiles in our sample are constant and independent of gestation between 16th and 22nd weeks. However, our study supports the idea that sHLA-G in serum is able to predict the weight percentile among fetuses with normal weight during this short time period of the study. Moreover, a previous study has revealed that sHLA-G is significantly decreased in maternal blood of patients having the diagnosis of fetal growth restriction [31]. The possible molecular explanation can be that sHLA-G stimulates decidual NK cells that promotes fetal growth and controls trophoblast invasion during mid-pregnancy [1,32]. Another explanation could be that HLA-G has been found to facilitate fetal growth by stimulating secretion of growth promoting factors (GPFs) in NK cells, according to recent studies [32,33,34].
One can speculate that a higher EVT mass can coordinate a larger amount of spiral arteries that can supply the higher demand of gas and nutrition exchange of a larger fetus.
In contrast with our former article where the dataset on normal and pathologic pregnancies altogether was interpreted [35], our current results show no association between serum sHLA-G levels and placental volume. An explanation could be that our new sample was included only asymptomatic, healthy pregnancies with no extreme values which should correspond to pathologic pregnancies.
HLA-G is unusual among HLA molecules in its unique pattern of expression in healthy individuals [36]. Similar to our former results among healthy and complicated pregnancies [28], sHLA-G level in amniotic fluid exhibited a negative correlation with the vascular perfusion of placenta. In this study we have explored an inverse correlation between HLA-G level in maternal serum and the placental blood perfusion with regard to healthy pregnancies. We assume that sHLA-G secretion may be reactive to reduced blood flow and vascular network in the expanding placenta, since sHLA-G facilitates the process of vasculogenesis [30]. The expansion of placental volume may outweigh the increase in capillary branching. In order to evaluate the placental perfusion, we used “Mercé-type sonobiopsy”, which is a reproducible and validated method [37,38], and by obtaining a representative sample of the placental tree, it is applicable throughout the entire pregnancy, unlike other methods [24], when the entire placenta needs to be visualized [39,40]. It can be also hypothesized that the HLA-G specific interaction of decidual natural killer cells and macrophages provides the secretion of angiogenic and pro-inflammatory factors implicated in vascular remodeling and the extent of trophoblast invasion, which is connected to lower perfusion indices as previously detected by ultrasound examinations.
Interestingly, we have unraveled an indirect correlation between NT measurements during 11-14 weeks of gestation and sHLA-G levels in amniotic fluid during 16 and 22 weeks of gestation. Our results support the assumption that low vascularization and perfusion of the placenta with high sHLA-G level in amniotic fluid during second trimester is preceded by an impaired placental 3D-PD indices and higher NT in the first trimester. This is in line with the results of Metzenbauer et al.[41], who found that trisomies are associated with higher NT and smaller placental volume between 11 to 14 weeks of gestation. Based on the literature we can confirm that low sHLA-G expression is commonly associated with implantation failure and miscarriage [42,43], which is supported by our results as well, since an obvious correlation exists between increased nuchal translucency and fetal loss [44].
Our study is focused on a relatively large number of amniotic samples deriving from a single center, where the ultrasound measurements were performed by two highly skilled sonographers.
In conclusion, increasing amount of data are collected concerning the impact of HLA-G polymorphism on the quantity of HLA-G expression and the correlation with complications in pregnancy. sHLA-G is unchanged in serum and amniotic fluid during second trimester in high-risk, but non-complicated pregnancies. Furthermore, our results indicate the role of decreased amniotic concentration of sHLA-G in the pathogenesis of increased nuchal translucency. It is of clinical importance that serum sHLA-G might be utilized as a predictor of anomaly of fetal growth and sHLA-G in amniotic fluid and maternal serum can be a potent biomarker of placental perfusion. To establish sHLA-G as a meaningful clinical biomarker, it is of paramount importance to trace back the structural diversity to tolerance-mediating functions.
Author Contributions
Conceptualization: M.V., Z.K. and J.S.; methodology: M.V., Z.K. and J.S.; formal analysis: A.M. writing—original draft preparation, M.V. and Z.K.; writing—review and editing, M.V., Z.K., A.S., J.S., J.S.J., G.N. and S.V.; supervision: I.F., G.N. and S.V.; data collection: M.V., J.S.J. and A.S. All authors have read and agreed to the published version of the manuscript.
Funding
Hetényi Grant of Albert Szent-Györgyi Medical School of the University of Szeged, Szeged, Hungary (Number: 5S 724 (A202).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of the University of Szeged (the protocol code: 09/2017 and the date of approval: 10 February 2017).
Informed Consent Statement
Informed consent was obtained from all subjects, who were involved in the study.
Data Availability Statement
The data can be made available by corresponding authors on request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Xu X, Zhou Y, Wei H. Roles of HLA-G in the Maternal-Fetal Immune Microenvironment. Front Immunol. 2020, 11. [CrossRef]
- Tantengco OAG, Richardson L, Lee A, Kammala A, Silva M de C, Shahin H, et al. Histocompatibility antigen, class i, g (Hla-g)’s role during pregnancy and parturition: A systematic review of the literature. Life 2021, 11(10). [CrossRef]
- Mao J, Feng Y, Zhu X, Ma F. The Molecular Mechanisms of HLA-G Regulatory Function on Immune Cells during Early Pregnancy. Biomolecules 2023, 13(8). [CrossRef]
- Li C, Houser BL, Nicotra ML, Strominger JL. HLA-G homodimer-induced cytokine secretion through HLA-G receptors on human decidual macrophages and natural killer cells. Proc Natl Acad Sci U S A. 2009, 106(14). [CrossRef]
- Rajagopalan S, Bryceson YT, Kuppusamy SP, Geraghty DE, Van Der Meer A, Joosten I, et al. Activation of NK cells by an endocytosed receptor for soluble HLA-G. PLoS Biol. 2006, 4(1). [CrossRef]
- Pazmany L, Mandelboim O, Valés-Gómez M, Davis DM, Reyburn HT, Strominger JL. Protection from natural killer cell-mediated lysis by HLA-G expression on target cells. Science (1979). 1996, 274(5288). [CrossRef]
- Rajagopalan S, Long EO. KIR2DL4 (CD158d): An activation receptor for HLA-G. Front Immunol. 2012, 3(AUG). [CrossRef]
- Le Bouteiller, P. HLA-G in human early pregnancy: Control of uterine immune cell activation and likely vascular remodeling. Biomed J. 2015, 38(1). [CrossRef]
- Murphy SP, Tayade C, Ashkar AA, Hatta K, Zhang J, Croy BA. Interferon gamma in successful pregnancies. Biol Reprod. 2009;80(5). [CrossRef]
- Shiroishi M, Tsumoto K, Amano K, Shirakihara Y, Colonna M, Braud VM, et al. Human inhibitory receptors Ig-like transcript 2 (ILT2) and ILT4 compete with CD8 for MHC class I binding and bind preferentially to HLA-G. Proc Natl Acad Sci U S A. 2003, 100(15). [CrossRef]
- Amiot L, Ferrone S, Grosse-Wilde H, Seliger B. Biology of HLA-G in cancer: A candidate molecule for therapeutic intervention? Cellular and Molecular Life Sciences. 2011, 68(3). [CrossRef]
- Poehlmann TG, Schaumann A, Busch S, Fitzgerald JS, Aguerre-Girr M, Le Bouteiller P, et al. Inhibition of term decidual NK cell cytotoxicity by soluble HLA-G1. American Journal of Reproductive Immunology. 2006, 56(5–6). [CrossRef]
- Wagner SN, Rebmann V, Willers CP, Grosse-Wilde H, Goos M. Expression analysis of classic and non-classic HLA molecules before interferon alfa-2b treatment of melanoma. Lancet 2000, 356(9225). [CrossRef]
- Lemaoult JL, Ne Krawice-Radanne I, Dausset J, Carosella ED. HLA-G1-expressing antigen-presenting cells induce immunosuppressive CD4 T cells. 2004. Available from: www.pnas.orgcgidoi10.1073pnas.0401922101.
- De Visser KE, Eichten A, Coussens LM. Paradoxical roles of the immune system during cancer development. Nat Rev Cancer. 2006, 6(1). [CrossRef]
- Imai C, Iwamoto S, Campana D. Genetic modification of primary natural killer cells overcomes inhibitory signals and induces specific killing of leukemic cells. Blood 2005, 106(1). [CrossRef]
- Mordoh J, Levy EM, Roberti MP. Natural killer cells in human cancer: From biological functions to clinical applications. J Biomed Biotechnol. 2011, 2011. [CrossRef]
- Yie SM, Li LH, Li YM, Librach C. HLA-G protein concentrations in maternal serum and placental tissue are decreased in preeclampsia. Am J Obstet Gynecol. 2004, 191(2). [CrossRef]
- Peng B, Zhang L, Xing A yun, Hu M, Liu S yun. The expression of human leukocyte antigen G and E on human first trimester placenta and its relationship with recurrent spontaneous abortion. Journal of Sichuan University (Medical Science). 2008, 39(6).
- Kusanovic JP, Romero R, Jodicke C, Mazaki-Tovi S, Vaisbuch E, Erez O, et al. Amniotic fluid soluble human leukocyte antigen-G in term and preterm parturition, and intra-amniotic infection/inflammation. Journal of Maternal-Fetal and Neonatal Medicine. 2009, 22(12). [CrossRef]
- Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with the use of head, body, and femur measurements--a prospective study. Am J Obstet Gynecol. 1985 Feb, 151(3), 333–337.
- K. Joubert. Magyar születéskori testtömeg- és testhossz-standardok az 1990-96. évi országos élveszületési adatok alapján. Magy Noorv Lapja. 2000, 63(12), 155–163.
- Suranyi A, Kozinszky Z, Molnar A, Nyari T, Bito T, Pal A. Placental three-dimensional power Doppler indices in mid-pregnancy and late pregnancy complicated by gestational diabetes mellitus. Prenat Diagn. 2013 Oct, 33(10), 952–958.
- Molnar A, Suranyi A, Nyari T, Nemeth G, Pal A. Examination of placental three-dimensional power Doppler indices and perinatal outcome in pregnancies complicated by intrauterine growth restriction. Int J Gynaecol Obstet. 2015 Apr, 129(1), 5–8.
- Lai PK, Wang YA, Welsh AW. Reproducibility of regional placental vascularity/perfusion measurement using 3D power Doppler. Ultrasound Obstet Gynecol. 2010 Aug, 36(2), 202–209.
- Központi Statisztikai Hivatal (Central Statistical Office H. KSH database 22.1.1.7. Live births by main characteristics of mother and newborn 1980-2022] [Internet]. 2023.
- Beneventi F, Locatelli E, De Amici M, Simonetta M, Cavagnoli C, Bellingeri C, et al. Soluble HLA-G concentrations in maternal blood and cervical vaginal fluid of pregnant women with preterm premature rupture of membranes. J Reprod Immunol. 2016, 116. [CrossRef]
- Vincze M, Sikovanyecz J, Molnár A, Földesi I, Surányi A, Várbíró S, et al. Predictive Capabilities of Human Leukocyte Antigen-G and Galectin-13 Levels in the Amniotic Fluid and Maternal Blood for the Pregnancy Outcome. Medicina (B Aires). 2024 Jan, 60(1), 85.
- Umapathy A, Chamley LW, James JL. Reconciling the distinct roles of angiogenic/anti-angiogenic factors in the placenta and maternal circulation of normal and pathological pregnancies. Angiogenesis. 2020, 23(2). [CrossRef]
- Rizzo R, Andersen AS, Lassen MR, Sørensen HC, Bergholt T, Larsen MH, et al. Soluble Human Leukocyte Antigen-G isoforms in maternal plasma in early and late pregnancy. American Journal of Reproductive Immunology. 2009, 62(5). [CrossRef]
- Steinborn A, Varkonyi T, Scharf A, Bahlmann F, Klee A, Sohn C. Early detection of decreased soluble HLA-G levels in the maternal circulation predicts the occurrence of preeclampsia and intrauterine growth retardation during further course of pregnancy. American Journal of Reproductive Immunology. 2007, 57(4). [CrossRef]
- Fu B, Zhou Y, Ni X, Tong X, Xu X, Dong Z, et al. Natural Killer Cells Promote Fetal Development through the Secretion of Growth-Promoting Factors. Immunity. 2017, 47(6). [CrossRef]
- Yockey LJ, Iwasaki A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity. 2018, 49(3). [CrossRef]
- Andreotti JP, Paiva AE, Prazeres PHDM, Guerra DAP, Silva WN, Vaz RS, et al. The role of natural killer cells in the uterine microenvironment during pregnancy. Cell Mol Immunol. 2018, 15(11). [CrossRef]
- Vincze M, Sikovanyecz J, Molnár A, Földesi I, Surányi A, Várbíró S, et al. Predictive Capabilities of Human Leukocyte Antigen-G and Galectin-13 Levels in the Amniotic Fluid and Maternal Blood for the Pregnancy Outcome. Medicina (B Aires). 2024 Jan, 60(1), 85.
- Nardi F da S, König L, Wagner B, Giebel B, Santos Manvailer LF, Rebmann V. Soluble monomers, dimers and HLA-G-expressing extracellular vesicles: the three dimensions of structural complexity to use HLA-G as a clinical biomarker. HLA. 2016, 88(3). [CrossRef]
- Merce LT, Barco MJ, Bau S. Reproducibility of the study of placental vascularization by three-dimensional power Doppler. J Perinat Med. 2004, 32(3), 228–233.
- Merce LT, Barco MJ, Bau S, Kupesic S, Kurjak A. Assessment of placental vascularization by three-dimensional power Doppler “vascular biopsy” in normal pregnancies. Croat Med J. 2005 Oct, 46(5), 765–771.
- Rizzo G, Capponi A, Pietrolucci ME, Aiello E, Arduini D. First trimester placental volume and three dimensional power doppler ultrasonography in type I diabetic pregnancies. Prenat Diagn. 2012 May;32(5):480–4.
- de Paula CFS, Ruano R, Campos JADB, Zugaib M. Quantitative analysis of placental vasculature by three-dimensional power Doppler ultrasonography in normal pregnancies from 12 to 40 weeks of gestation. Placenta. 2009 Feb, 30(2), 142–148.
- Metzenbauer M, Hafner E, Schuchter K, Philipp K. First-trimester placental volume as a marker for chromosomal anomalies: Preliminary results from an unselected population. Ultrasound in Obstetrics and Gynecology. 2002, 19(3). [CrossRef]
- Barbaro G, Inversetti A, Cristodoro M, Ticconi C, Scambia G, Di Simone N. HLA-G and Recurrent Pregnancy Loss. Int J Mol Sci. 2023, 24(3). [CrossRef]
- Arnaiz-Villena A, Juarez I, Suarez-Trujillo F, López-Nares A, Vaquero C, Palacio-Gruber J, et al. HLA-G: Function, polymorphisms and pathology. Int J Immunogenet. 2021, 48(2). [CrossRef]
- Bilardo CM, Pajkrt E, De Graaf I, Mol BW, Bleker OP. Outcome of fetuses with enlarged nuchal translucency and normal karyotype. Ultrasound in Obstetrics and Gynecology. 1998, 11(6). [CrossRef]
Figure 1.
HLA-G concentrations between 16th and 22nd gestational weeks.
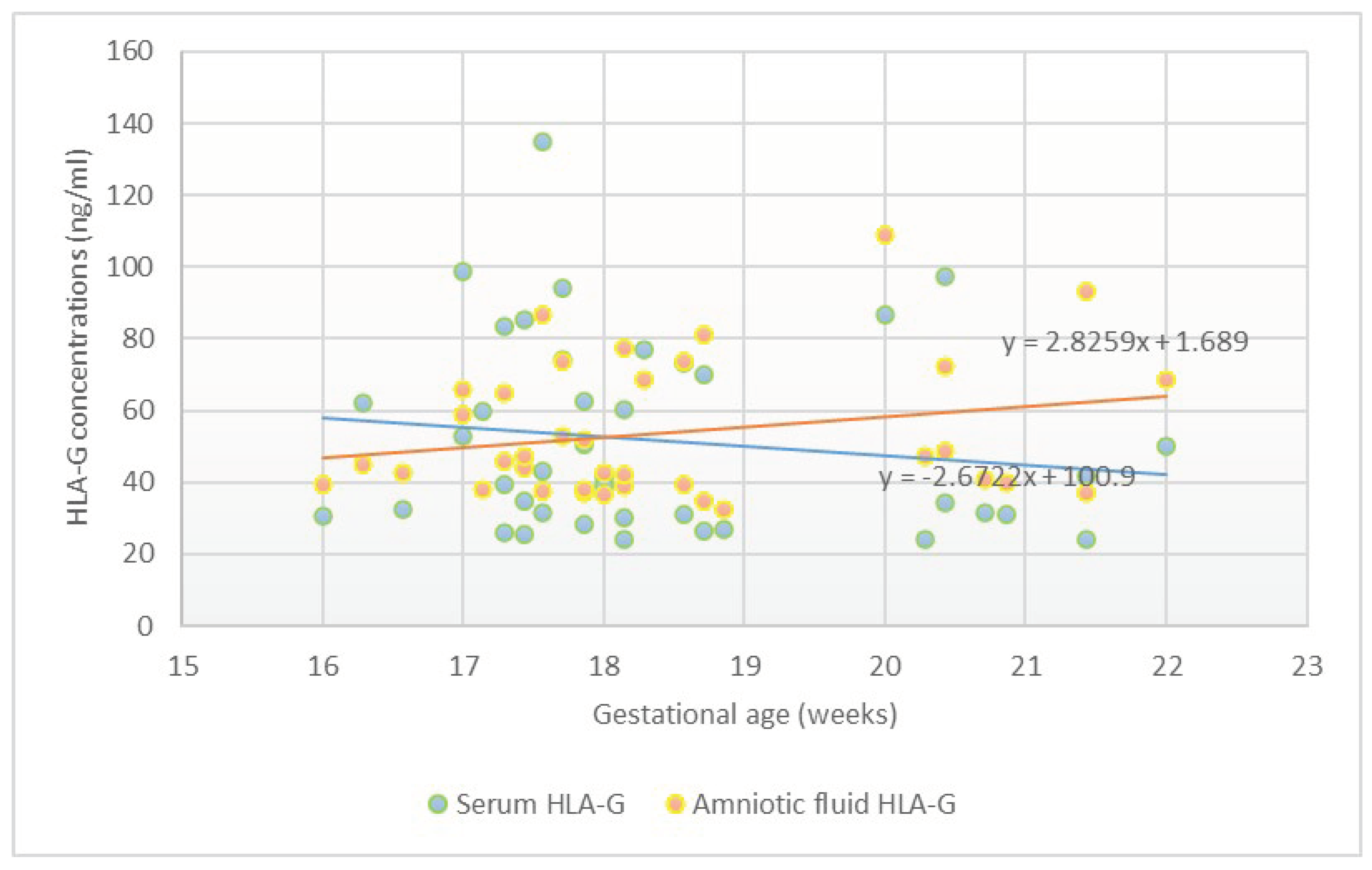

Table 1.
Clinical and obstetric data of pregnant women with amniocentesis (N=41).
| Maternal age (years)* | 33.63 ± 6.51 |
|---|---|
| Number of nulliparous women in the study** | 12 (29.3) |
| BMI at the time of genetic consultation (kg/m2)* | 26.35 ± 6.19 |
| Birth weight (grams)* | 3351.22 ± 370.10 |
| Birth weight (percentile)* | 54.34 ± 24.39 |
| Gestational age at the time of delivery (weeks)* | 39.01 ± 1.32 |
*Continuous variables are displayed as mean ± standard deviation (SD). ** Categorical variables are presented as number and %.
Table 2.
Ultrasound data (N=41)*.
| Data on genetic ultrasound examination in the first trimester | |
|---|---|
| NT (mm) | 1.88 ± 0.66 |
| CRL at NT (mm) | 63.90 ± 6.54 |
| Gestational age at nuchal translucency (weeks) | 12.62 ± 0.55 |
| Fetal biometry at the time of amniocentesis | |
| Gestational age at the time of amniocentesis (weeks) | 18.37 ± 1.49 |
| Head circumference (mm) | 153.62 ± 15.89 |
| Head circumference (percentile) | 56.70 ± 29.21 |
| Abdominal circumference (mm) | 134.10 ± 17.06 |
| Abdominal circumference (percentile) | 55.25 ± 27.57 |
| Femur length (mm) | 27.71 ± 4.99 |
| Femur length (percentile) | 57.54 ± 27.46 |
| Estimated fetal weight (grams) | 260.71 ± 81.26 |
| Estimated fetal weight (percentile) | 53.50 ± 26.11 |
| Placental sonography | |
| Placental volume (mm3) | 214.80 ± 94.67 |
| VI | 14.38 ± 5.67 |
| FI | 43.27 ± 8.76 |
| VFI | 8.46 ± 4.20 |
NT: Nuchal Translucency, CRL: Crown-Rump Length, VI: Vascularization Index, FI: Flow Index, VFI: Vascularization Flow Index.
Table 3.
Levels of HLA-G in samples of amniotic fluid and serum (N=41)*.
| sHLA-G concentration in amniotic fluid (ng/ml) | 53.39 ± 19.00 |
|---|---|
| sHLA-G concentration in serum (ng/ml) | 51.05 ± 26.99 |
sHLA-G: soluble Human Leukocyte Antigen-G. *Continuous variables are displayed as mean ± standard deviation (SD).
Table 4.
Correlation between maternal as well as sonographic data and levels of sHLA-G in maternal serum and amniotic fluid (N=41).
Table 4.
Correlation between maternal as well as sonographic data and levels of sHLA-G in maternal serum and amniotic fluid (N=41).
| sHLA-G level in serum | sHLA-G in amniotic fluid | |||||||
| Univariate linear regression | Multivariate linear regression | Univariate linear regression | Multivariate linear regression | |||||
| β | CI | β | CI | β | CI | β | CI | |
| Clinical and obstetric characteristics | ||||||||
| Maternal age | 0.01 | -1.31-1.38 | 0.01 | -1.71-1.74 | -0.20 | -1.51-0.39 | -0.17 | -1.75-0.79 |
| Previous parity | -0.12 | -13.18-6.00 | -0.15 | -16.17-7.50 | -0.08 | -8.54-5.33 | 0.08 | -7.21-10.43 |
| BMI at the time of genetic consultation (kg/m2) | 0.19 | -0.57-2.21 | 0.15 | -0.82-2.16 | -0.04 | -1.22-0.93 | 0.00 | -1.10-1.11 |
| Birth weight (grams) | -0.02 | -0.03-0.02 | -0.01 | -0.03-0.02 | 0.01 | -0.02-0.02 | -0.01 | -0.02-0.02 |
| Birth weight (percentile) | 0.05 | -0.30-0.40 | 0.18 | -0.31-0.42 | -0.02 | -0.27-0.24 | -0.00 | -0.27-0.27 |
| NT | -0.11 | -17.87-8.79 | -0.17 | -22.29-8.50 | -0.30 | -17.78-0.86 | -0.38* | -21.73-0.04* |
| CRL at NT | 0.30 | -0.08-2.52 | 0.76 | -0.38-2.69 | 0.10 | -0.71-1.32 | 0.14 | -0.75-1.60 |
| GA at the time of delivery | -0.11 | -8.85-4.34 | -0.06 | -1.14-0.81 | 0.02 | -4.45-5.08 | 0.03 | -0.63-0.77 |
| GA at the time of amniocentesis (weeks) | -0.13 | -8.22-3.45 | 0.46 | -1.30-0.55 | 0.24 | -1.12-7.10 | 0.20 | -0.31-1.02 |
| Fetal sonography at the time of amniocentesis | ||||||||
| Head circumference (mm) | -0.12 | -0.75-0.35 | -0.09 | -1.12-0.83 | 0.26 | -0.08-0.69 | 0.19 | -0.49-0.95 |
| Head circumference (percentile) | -0.03 | -0.32-0.28 | -0.16 | -0.51-0.21 | -0.08 | -0.27-0.17 | 0.08 | -0.24-0.34 |
| Abdominal circumference (mm) | 0.01 | -0.71-0.71 | 0.70 | -0.30-2.77 | 0.33 | -0.08-0.86 | 0.93 | -0.14-2.32 |
| Abdominal circumference (percentile) | 0.41* | -0.08-0.75* | 0.35 | -0.07-0.84 | 0.26 | -0.12-0.51 | 0.35 | -0.08-0.61 |
| Femur length (mm) | 0.07 | -2.54-1.74 | -0.18 | -7.88-5.78 | 0.23 | -0.61-2.53 | -0.28 | -6.89-4.61 |
| Femur length (percentile) | 0.20 | -0.18-0.59 | -0.02 | -0.49-0.45 | -0.00 | -0.30-0.29 | -0.12 | -0.49-0.31 |
| Estimated fetal weight (grams) | -0.04 | -0.16-0.14 | 0.64 | -0.22-0.69 | 0.26 | -0.04-0.17 | 0.73 | -0.17-0.53 |
| Estimated fetal weight (percentile) | 0.41* | -0.02-0.84* | 0.31 | -0.15-0.85 | 0.24 | -0.14-0.52 | -0.31 | -0.12-0.63 |
| Placental sonography at the time of amniocentesis | ||||||||
| Placental volume (mm3) | 0.02 | -0.09-0.10 | -0.03 | -0.11-0.10 | -0.09 | -0.09-0.05 | 0.01 | -0.07-0.08 |
| VI | -0.10 | -2.00-1.08 | -0.16 | -2.56-1.03 | -0.34* | -2.13-0.06* | -0.38* | -2.47-0.03* |
| FI | 0.05 | -0.86-1.14 | 0.04 | -0.92-1.17 | -0.18 | -1.12-0.34 | -0.13 | -1.06-0.50 |
| VFI | -0.34* | -3.58-0.46* | -0.32 | -4.32-0.20 | -0.44* | -3.28-0.63* | -0.52* | -3.79-0.72* |
sHLA-G: soluble Human Leukocyte Antigen-G, BMI: body mass index, GA: Gestational age, VI: Vascularization Index, FI: Flow Index, VFI: Vascularization Flow Index. *p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



