Submitted:
18 January 2024
Posted:
19 January 2024
You are already at the latest version
Abstract
Dendritic cells (DCs) are the most specialized antigen-presenting cells and lymph nodes (LNs) play an important role in the DC-mediated T-cell response. We evaluated the infiltration of CD1a-positive DCs (CD1a-DCs) i.e. immature DCs, and S100-positive dendritic cells (S100-DCs), a mixture of immature- and mature DCs, in 73 cases of laryngeal cancer and its regional LNs. Among them, 31 patients underwent radiotherapy (RT) or chemoradiotherapy (CRT) prior to surgery. No significant difference was found for CD1a-DC infiltration in the primary tumor, metastatic LNs and non-metastatic LNs, while S100-DCs were significantly fewer in number in the primary tumor and metastatic LNs compared to non-metastatic LNs. Cases which showed a high infiltration of S100-DCs in metastatic LNs appeared to show a favorable prognosis although statistical significance was not reached. In the RT/CRT group, infiltration of CD1a-DCs and S100-DCs were fewer in the primary tumor and metastatic LNs compared to the treatment naive group. Conversely, the RT/CRT group showed higher CD1a-DCs and S100-DCs numbers in non-metastatic LNs compared to the treatment naïve group. Thus, DC maturation in metastatic LNs plays an important role in tumor immunity in laryngeal cancer, and infiltration of DCs into the primary tumor and metastatic LNs is impaired by RT/CRT.
Keywords:
dendritic cell
; CD1a
; S100
; lymph node
; chemoradiotherapy
1. Introduction
Laryngeal cancer is a common malignancy of the head and neck. Although the prognosis of early laryngeal cancer is favorable, that for advanced laryngeal cancer is poor, despite much progress being made with regard to multidisciplinary therapy, such as the combined use of chemoradiotherapy and surgery [1].
The treatment strategy for laryngeal cancer is different according to the tumor stage. Local resection or radiation therapy is the first choice for patients with early-stage cancer [2] but for advanced cancer, larynx-preserving surgery or total laryngectomy is performed. Cervical LN dissection may be carried out depending on the presence of LN metastases. Chemoradiotherapy is usually required when the postoperative pathology shows positive margins or LN metastasis with extracapsular extension [3]. If surgery is not an option, chemoradiotherapy is the first treatment of choice, but if residual tumor is observed after treatment, salvage surgery is performed [4]. In cases with T4 or LN metastases, induction chemotherapy should be given first, followed by chemoradiotherapy if a response is elicited. If there is no response, surgery is considered [5]. Thus, there is a wide range of treatment options for laryngeal cancer, which may be modified by the patient's desire to preserve their larynx or surgical risk due to an underlying condition. Currently, there is no unified treatment strategy for laryngeal cancer, and it is often difficult to decide between surgery and chemoradiotherapy. In recent years, immune checkpoint inhibitors have been administered to patients with recurrent or unresectable tumors, contributing to improved prognosis. The importance of tumor immunity research and immunotherapy is expected to increase. However, there are many unknowns about the immune microenvironment of laryngeal cancer, and elucidating the immune environment may lead to the development of effective immunotherapy and improved treatment outcomes for laryngeal cancer.
DCs play important roles in cancer immune responses. First, they phagocytose necrotic cancer cell antigens. Subsequent T-cell responses require signals, such as inflammatory cytokines released by tumor cells to prevent immune tolerance to the tumor antigen in the periphery. DCs then present the antigen captured on major histocompatibility complex (MHC) I or MHC II molecules to T-cells. The T-cell response to the cancer-specific antigen is then primed and activated. The ratio of effector T-cells to regulatory T-cells is determined and influences the outcome. Activated effector T-cells migrate to and infiltrate tumor sites, where they interact with antigens bound to T-cell receptors and MHC I molecules which then specifically recognize and bind to cancer cells destroying them [6]. T-cells recognize lipid antigens in a complex with CD1 antigen-presenting molecules. Humans have five CD1 genes encoding five proteins, CD1a, b, c, d, and e. The CD1 isoforms overlap but have distinct lipid-binding specificities, which affect the repertoire of lipid antigens that stimulate T-cells. CD1a expression declines as DCs mature and acquire the ability to present antigen [7,8].
Several studies on various types of carcinomas focused on infiltration of DCs into tumor tissue [9,10,11,12,13,14,15,16], but no unanimous opinion was reached. In a previous study conducted in our laboratory, CD1a-DCs were found to be associated with unfavorable clinical outcomes in patients with advanced laryngeal cancer who had underwent total laryngectomy as the initial treatment [17]. However, only a small number of studies have focused on DC infiltration into laryngeal cancer tissue but the results differed [18,19,20,21,22,23], so that the role of DC infiltration in laryngeal cancer remains unclear.
LNs play a very important role in the DC-mediated T-cell response. After antigen phagocytosis, DCs are activated and express C-chemokine receptor 7 (CCR7), a specific chemokine receptor that promotes their migration to LNs, and they are directed by chemokines to the draining lymph vessels and to T-cell areas of LNs, where they initiate T-cell responses [24,25]. To the best of our knowledge, there has been no specific study that focused on DCs infiltration into the LNs of cancer patients.
In the present study, the aim was to elucidate the trend of DCs in tumor immunity in laryngeal cancer by analyzing DC infiltration into the regional LNs and tumor tissue. Furthermore, we also evaluated the status of DC infiltration after radiotherapy and/or chemoradiotherapy.
2. Results
2.1. Clinicopathological Features of 73 Patients with Laryngeal Cancer
The clinical and pathological findings of the cohort of 73 laryngeal cancer patients (70 males (95.9%), 3 females (4.1%)) are summarized in Table 1. The median age at initial diagnosis was 68.9 years. The primary tumor sites were glottic in 36 (49.3%) patients, supraglottic in 36 (49.3%) and subglottal in 1 (1.4%). The T-stages at initial diagnosis were T1 in 8 (11.0%), T2 in 21 (28.8%), T3 in 21 (28.8%) and T4 in 23 (31.5%) patients, respectively. Forty-six (37.0%) patients had metastatic LNs and 1 patient had no non-metastatic LN specimens. The Stages at initial diagnosis were: Stage I, 5 patients (6.8%); Stage II, 11 patients (15.1%); Stage III, 16 patients (21.9%); and Stage IV, 41 patients (56.2%). The histology of the patient tumors were squamous cell carcinoma (SCC) except for 1 case of carcinosarcoma containing a SCC component.
Forty-two (57.5%) patients underwent surgical resection as their initial treatment. Two (2.7%) patients underwent preoperative radiotherapy (RT) and then underwent surgery, and 29 (39.7%) were given chemoradiotherapy (CRT) before surgery. The primary tumor was not detectable after CRT in 8 cases. In these cases, biopsy specimens obtained prior to CRT were defined as treatment naïve primary tumor tissue. Thus, 50 cases of primary tumor tissue were finally evaluated as treatment naïve.
2.2. Assessment of DCs in Primary Tumor and Regional LNs
The results of CD1a-DCs and S100-DCs, which were evaluated for each primary tumor, metastatic LNs and non-metastatic LNs, are shown in Figure 1. The average number ± standard deviation (SD) of CD1a-DCs, which are considered to be immature DCs, in primary tumor was 35.1 ± 38.9 (median: 21). The average number of CD1a-DCs in metastatic LNs and non-metastatic-LNs were 44.9 ± 47.7 and 34.3 ± 49.0, respectively. There were no significant statistical differences in the numbers of CD1a-DCs found in primary tumor, metastatic LNs and non-metastatic LNs.
The average numbers ± SD of S100-DCs, which are considered to be a mixture of immature-DCs and mature DCs, in primary tumor was 49.2 ± 36.0 (median: 43). The average numbers of S100-DCs in metastatic LNs and non-metastatic LNs were 45.1 ± 33.7 and 89.5 ± 49.1, respectively. The numbers of S100-DCs in non-metastatic LNs were significantly greater than in metastatic LNs (P < 0.000) or primary tumor (P < 0.000).
2.3. Comparison of DCs in Primary Tumor and Regional LNs between the RT/CRT and Treatment Naïve Groups
In the analysis of the RT/CRT and treatment naïve groups, the average number ± SD of CD1a-DCs in primary tumor, metastatic LNs and non-metastatic LNs of the RT/CRT group were 23.4 ± 36.7, 25.1 ± 35.2 and 43.2 ± 61.2, and in the treatment naïve group 40.4 ± 39.0, 60.1 ± 51.0 and 27.6 ± 36.7, respectively. The numbers of CD1a-DCs in the primary tumor and metastatic LNs in the RT/CRT group were fewer than in the treatment naïve group. A statistically significant difference was found for metastatic LNs (P = 0.008) but not for the primary tumor (P = 0.128). Conversely, the number of CD1a-DCs in non-metastatic LNs in the RT/CRT group appeared to be greater than in the treatment naïve group, but statistical significance was not reached (P = 0.140).
The average number ± SD of S100-DCs in primary tumor, metastatic LNs and non-metastatic LNs of the RT/CRT group were 33.0 ± 25.5, 33.2 ± 26.0 and 101.0 ± 52.8, and for the treatment naïve group 56.6 ± 37.9, 54.3 ± 36.4 and 80.8 ± 44.7, respectively. The numbers of S100-DCs detected in primary tumor and metastatic LNs in the RT/CRT group were fewer than in the treatment naïve group. Statistical significance was found after analysis of the primary tumor (P = 0.020) but not for metastatic LNs (P = 0.077). Conversely, the numbers of S100-DCs in non-metastatic LNs in the RT/CRT group was significantly greater than in the treatment naïve group (P = 0.034).
2.4. Clinicopathological Features per CD1a-DCs Infiltration in Primary Tumor, Metastatic LNs and Non-Metastatic LNs
In primary tumor, the patient cohort was divided into a CD1a-low group (n = 37) and a CD1a-high group (n = 36) with regard to infiltration of CD1a-DCs. No significant differences were found in age, gender and the TNM stage between the CD1a-low and CD1a-high groups. Patients who received RT/CRT had significantly fewer CD1a-DCs (P = 0.043).
For the analysis of metastatic LNs, the patient cohort was divided into a CD1a-low group (n = 23) and a CD1a-high group (n = 23). No significant differences were found with regard to age, gender and the TNM stage. Patients who received RT/CRT had significantly fewer CD1a-DCs (P = 0.036).
For the analysis of non-metastatic LNs, the patient cohort was divided into a CD1a-low group (n = 40) and a CD1a-high group (n = 32) according to the cut-off. The non-metastatic LNs of older patients tended to have fewer CD1a-DCs (P = 0.074). However, no significant differences were observed in age, gender, the TNM stage or RT/CRT (Table 2).
2.5. Clinicopathological Features per S-100 DC Infiltration in Primary Tumor, Metastatic LNs and Non-Metastatic LNs
According to the cutoff value for the primary tumor, the patient cohort was divided in a S100-low group (n = 37) and a S100-high group (n = 36). No significant differences were found with regard to age and the TNM stage in the S100-low and S100-high groups. Patients who received RT/CRT had significantly fewer S100-DCs (P = 0.011).
In the analysis of metastatic LNs, the patient cohort was divided into a S100-low group (n = 25) and a S100-high group (n = 21) according to the cut-off value (median of S100-DC numbers). No significant difference was found with regard to age, gender or the TNM stage. Patients who received RT/CRT had significantly fewer S100-DCs (P = 0.019).
For the analysis of non-metastatic LNs, the patient cohort was divided into a S100-low group (n = 14) and a S100-high group (n = 58) according to the cut-off. In non-metastatic LNs, patients who had distant metastasis had significantly fewer S100-DCs (P = 0.036). No significant difference were found for age, gender, the TNM stage or RT/CRT (Table 3).
2.6. Kaplan-Meier Survival Curves According to the Infiltration of CD1a- and S100- DCs
Kaplan-Meier curves, based on the status of CD1a-DCs infiltration, are shown in Figure 2. In the primary tumor, the CD1a-high group appeared to exhibit a worse prognosis in disease-specific survival (DSS), although statistical significance was not achieved (P = 0.090). However, no tendency was observed in the analyses of overall survival (OS) for primary tumor (P = 0.468), DSS in metastatic LNs (P = 0.969) and non-metastatic LNs (P = 0.580), or for each analysis of OS for the primary tumor (P = 0.468), metastatic LNs (P = 0.581), and non-metastatic LNs (P = 0.737).
Kaplan-Meier curves, based on the status of S100-DCs infiltration, are displayed in Figure 3. In metastatic LNs, the S100-high group appeared to show a favorable prognosis in DSS and OS, although statistical significance was not reached (P = 0.165, P = 0.067, respectively). However, no tendency was observed in the analysis of DSS for the primary tumor (P = 0.535) and non-metastatic LNs (P = 0.865), or in the analysis of OS for the primary tumor (P = 0.994) and non-metastatic LNs (P = 0.487).
2.7. Univariate Analyses for DSS and OS in All Patients (n = 73)
The results of the univariate analyses for DSS and OS in all patients are summarized in Table 4. The factor significantly correlated with DSS was only the N stage (P = 0.025). The factors significantly correlated with OS were the T stage (P = 0.031) and the N stage (P = 0.037). The status of both CD1a-DCs and S100-DCs infiltration in each primary tumor, metastatic LNs and non-metastatic LNs showed no significant correlation with both DSS and OS, although tendencies were observed in DSS for CD1a-DCs infiltration in primary tumor (P = 0.098), DSS for S100-DCs infiltration in metastatic LNs (P = 0.177, and OS for S100-DCs infiltration in metastatic LNs (P = 0.077).
3. Discussion
DCs are derived from common myeloid progenitors (CMPs) in the bone marrow and are comprised of two subtypes. In inflammatory conditions, they differentiate into monocytes and then into monocyte DCs through expression of the transcription factor Nur77. In the absence of Nur77, CMPs differentiate into dendritic cell progenitors, which differentiate into plasmacytoid DCs (pDCs) or conventional DCs (cDCs). cDCs are immature at first but can differentiate into mature DCs following injury, exposure to pathogen-associated factors or inflammatory cytokines. DCs express CCR7 and migrate to LNs. In LNs, mature DCs activate naive T cells to initiate an immune response [26,27].
Several factors have been implicated in DC differentiation and maturation [28]. Several cytokines affect DCs: IL-6 inhibits DCs differentiation and maturation [29,30] and IL-10 inhibits DCs differentiation, maturation and certain functions [31,32]. M-CSF inhibits their differentiation into DCs from CD34-positive CMPs [29]. GM-CSF produced by tumors has an inhibitory effect on immature DCs [33] while VEGF inhibits differentiation of DCs and affects the differentiation of the multiple hematopoietic lineage [34]. These research findings raise the possibility that activation and maturation of DCs are affected by various cytokines and that not all tumor-infiltrating DCs function as antigen-presenting cells. It is possible that the maturation, activation and T-cell response of DCs may be significantly affected by the histological type or by the progression of the tumor.
In the present study, the infiltration of CD1a-DCs was not significantly different in the primary lesion, metastatic LNs or non-metastatic LNs. However, the infiltration of S100-DCs was significantly different: infiltration of S-100DCs in non-metastatic LN was significantly greater than for the primary lesion and metastatic LNs. As S100-DCs are considered to label both immature and mature DCs, these results support the hypothesis that the maturation of DCs was prevented by the presence of cancer cells.
Our previous research indicated that infiltration of CD1a-DCs into the primary lesion was associated with an unfavorable prognosis for patients with advanced laryngeal cancer who had underwent a total laryngectomy as their initial treatment [17]. A similar tendency was observed in the present study for a different cohort of patients. The high-CD1a-DCs infiltrating group in the primary lesion indicated an unfavorable prognosis compared to the low-CD1a-DCs infiltrating group, although statistical significance was not reached. Conversely, while infiltration of S100- DCs into primary lesions and non-metastatic LNs did not affect the prognosis, a higher infiltration of S100-DCs in metastatic LNs was correlated with better outcomes. These findings highlight the importance of maturation of DCs in metastatic LNs for an immune response against laryngeal cancer.
Our study had the following limitations, namely a small sample size and that assessment of mature DCs was only an indirect marker of S100. However, the results produced important hints for understanding the immune response mediated by DCs in laryngeal cancer. It is likely that the cancer cells play some important roles in both infiltration and maturation of DC at the primary sites and in metastatic LNs. Unraveling the mechanism of the induction and maturation of DCs by cancer cells may well lead to the development of new immunotherapies. Therefore, the analysis of various cytokines and chemokines in cancer tissue that are associated with infiltration and maturation of DCs is an important research area, as well as an examination of the characteristics of CD1a-DC regarding their interaction with cancer cells. This research will provide new insights into our understanding of cancer immune responses mediated by DCs.
It has been shown that antigen phagocytosis and maturation of DCs are processes affected by RT and chemotherapy [35,36,37,38]. Radiotherapy, in particular, has been reported to have an inhibitory effect on DC functions, suggesting that the presence or absence of radiotherapy may make a difference to DC infiltration and maturation [39,40].
RT exerts its therapeutic effect through DNA damage. It is now recognized that the nucleic acid species produced from this DNA damage are inflammatory and potentially immunogenic. RT enhances antigenicity through the release of antigens associated with tumor cell death, radiation-induced neoantigens and upregulation of MHC-I molecules. On the other hand, RT initiates immunoregulatory and homeostatic actions that reduce the functions of DCs in the tumor microenvironment. In short, RT promotes antitumor immunity through DCs while simultaneously counteracting their functions [41,42,43,44].
The present research also focused on the status of DC-infiltration and maturation in primary tumor and LNs after RT/CRT. Our results indicated that infiltration of CD1a-DCs were fewer in numbers in primary lesions and metastatic LNs in the RT/CRT group compared to the treatment naïve group. Conversely, the RT/CRT group showed a higher CD1a-DC infiltration into non-metastatic LNs than the treatment naïve group. Similar results were also obtained in analyses of S100-DCs. These results support the following working hypothesis: the ability of DCs induction in cancer cells and the surrounding stroma are impaired by necrosis and/or degeneration of the tumor cells and microenvironmental changes due to RT/CRT. On the other hand, the ability of DC induction remains in non-metastatic LNs, which are relatively unaffected by RT/CRT. The infiltration of DC numbers into non-metastatic LNs, both CD1a-DCs and S100-DCs, was higher in RT/CT cases than in treatment naïve cases. This result was also predictable considering the enhanced immune-reaction elicited by RT/CRT.
In conclusion, our study suggested that DCs maturation in metastatic LNs plays an important role in tumor immunity in laryngeal cancer. Additionally, the results confirmed DC induction in tumor tissue impaired by RT/CRT in clinically resected specimens. Understanding these phenomena could open avenues for novel immunotherapies. Further accumulation of clinicopathological and basic research data will be necessary to clarify the mechanisms underlying tumor-immune responses involving DCs.
4. Materials and Methods
4.1. Patients
A total of 333 patients with laryngeal cancer treated at Saga University Hospital between 2000 and 2020 were initially enrolled in the study. Among these, cases without lymphadenectomy or lymph node biopsy, and those with histological types other than squamous cell carcinoma were excluded. Finally, 73 patients were enrolled. Comprehensive informed consent for the use of resected tissue for this research was obtained from all patients, and the study protocol was approved by the Ethics Committee of Saga University (2023-02-R-09).
4.2. Immunohistochemistry
Immunohistochemistry (IHC) of CD1a and S-100 was carried out on representative primary tumors and regional LNs. In the cases with nodal metastasis, both representative metastatic and non-metastatic LNs were subjected to IHC. For patients without nodal metastasis, only non-metastatic LNs were analyzed using IHC. As one patient had no non-metastatic LNs, only metastatic nodes were subjected to IHC in that case. The specimens were sectioned into 4 µm slices from Formalin-Fixed Paraffin-Embedded (FFPE) blocks. The primary antibodies used were CD1a (Clone 010, prediluted; Dako, Glostrup, Denmark), and S100 (GA50461–2 J; prediluted; Dako). IHC was performed using an Autostainer plus automatic stainer (Dako). The Envision System (Dako) was employed as the secondary antibody. Specimens on slides were visualized by diaminobenzidine tetrahydrochloride and nuclei were counterstained with hematoxylin.
4.3. Assessment of CD1a- and S100-DCs
The IHC sections were scanned and converted to digital slides by NanoZoomer S360 (Hamamatsu Photonics, Shizuoka, Japan). CD1a-DCs and S100-positive DCs (S100-DCs) were evaluated in 3 random hot spots at a magnification of × 100 (Figure 4). The median values of CD1a-DCs and S100-DCs in the primary tumor were used as the cut-off values and the patient cohort was divided into a high-group and a low-group. The same cut-off value, determined for the primary tumor, was used in the evaluation of LNs. Patients were also divided into high- and low-groups according to the degree of DC infiltration into LNs.
4.4. Statistical Analysis
All statistical analyses were performed using JMP Pro 13.1.0 software (SAS Institute, Cary, NC, US). Student’s t-test, Pearson’s chi-squared test and a linear regression analysis were used when appropriate for comparisons between two groups. Disease-specific survival (DSS) was defined as the period from surgery to cancer-related death or the last follow-up. Overall survival (OS) was defined as the period from surgery to death or the last follow-up. The maximum follow-up period during the study was 120 months, with a median follow-up time of 45.0 months. The survival curve was calculated by the Kaplan-Meier method, and a log-rank test was conducted.
Author Contributions
Conceptualization and design, K.K., A.M. and K.K.; diagnoses and treatment of patients, M.Y. and Y.K.; acquisition of data, K.K., A.M. and K.K.; writing of the original draft of the manuscript, K.K. and K.K.; material preparation and pathological assessments, K.K., S.M., A.M. and K.K.; analysis and interpretation of data, K.K. and K.K.
Funding
The study was financially supported by the Japan Society for the Promotion of Science KAKENHI Grant-in-Aid for Scientific Research (research project no. 22K16913). This study was also funded by The Soda Toyoji Memorial Foundation (research project no. JS20220057).
Institutional Review Board Statement
The study protocols were approved by the Ethics Committee of Saga University Hospital (approval number: 2023-02-R-09).
Informed Consent Statement
Written informed consent was obtained from all patients for permission to use their clinical data and tissue samples for research purposes.
Data Availability Statement
Data contained within the article will be provided by the authors upon reasonable request.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Abbreviations
CCR7, C-chemokine receptor 7; CMP, common myeloid progenitor; CRT, chemoradiotherapy; DC, dendritic cell; DSS, disease specific survival; FFPE, formalin-fixed paraffin-embedded; GM-CSF, granulocyte macrophage colony stimulating factor; IHC, immunohistochemistry; LN, lymph node; M-CSF, macrophage colony stimulating factor; MHC, major histocompatibility complex; Nur77, nuclear receptor 77; OS, overall survival; RT, radiotherapy; VEGF, vascular endothelial growth factor
References
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; Colevas, A.D.; Eisele, D.W.; Fenton, M.; Foote, R.L.; Galloway, T.; Gillison, M.L.; Haddad, R.I.; Hicks, W.L.; Hitchcock, Y.J.; Jimeno, A.; Leizman, D.; Maghami, E.; Mell, L.K.; Mittal, B.B.; Pinto, H.A.; Ridge, J.A.; Rocco, J.W.; Rodriguez, C.P.; Shah, J.P.; Weber, R.S.; Weinstein, G.; Witek, M.; Worden, F.; Yom, S.S.; Zhen, W.; Burns, J.L.; Darlow, S.D. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Nibu, K.; Hayashi, R.; Asakage, T.; Ojiri, H.; Kimata, Y.; Kodaira, T.; Nagao, T.; Nakashima, T.; Fujii, T.; Fujii, H.; Homma, A.; Matsuura, K.; Monden, N.; Beppu, T.; Hanai, N.; Kirita, T.; Kamei, Y.; Otsuki, N.; Kiyota, N.; Zenda, S.; Omura, K.; Omori, K.; Akimoto, T.; Kawabata, K.; Kishimoto, S.; Kitano, H.; Tohnai, I.; Nakatsuka, T. Japanese Clinical Practice Guideline for Head and Neck Cancer. Auris Nasus Larynx. 2017, 44, 375–380. [Google Scholar] [CrossRef]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; Glabbeke, M.V.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.K.; Lefebvre, J.L. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Head Neck. 2005, 27, 843–850. [Google Scholar] [CrossRef]
- Maruo, T.; Zenda, S.; Shinozaki, T.; Tomioka, T.; Okano, W.; Sakuraba, M.; Tahara, M.; Hayashi, R. Comparison of salvage surgery for recurrent or residual head and neck squamous cell carcinoma. Jpn. J. Clin. Oncol. 2020, 50, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Okano, S.; Homma, A.; Kiyota, N.; Tahara, M.; Hanai, N.; Asakage, T.; Matsuura, K.; Ogawa, T.; Saito, Y.; Sano, D.; Kodaira, T.; Motegi, A.; Yasuda, K.; Takahashi, S.; Tanaka, K.; Onoe, T.; Yokota, T.; Imamura, Y.; Ariizumi, Y.; Akimoto, T.; Hayashi, R. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck. Jpn. J. Clin. Oncol. 2021, 51, 173–179. [Google Scholar] [CrossRef]
- Chen, D.S.; Mellman, I. Oncology Meets Immunology: The Cancer-Immunity Cycle. Immunity. 2013, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Coventry, B.J.; Lee, P.L.; Gibbs, D.; Hart, D.N.J. Dendritic cell density and activation status in human breast cancer- CD1a, CMRF-44, CMRF-56 and CD-83 expression. Br. J. Cancer. 2002, 86, 546–551. [Google Scholar] [CrossRef]
- Mori, L.; Libero, G.D. Presentation of lipid antigens to T cells. Immunol. Lett. 2008, 117, 1–8. [Google Scholar] [CrossRef]
- Hilly, O.; Rath-Wolfson, L.; Koren, R.; Mizrachi, A.; Hamzany, Y.; Bachar, G.; Shpitzer, T. CD1a-positive dendritic cell density predicts disease-free survival in papillary thyroid carcinoma. Pathol. Res. Pract. 2015, 211, 652–656. [Google Scholar] [CrossRef]
- Kai, K.; Tanaka, T.; Ide, T.; Kawaguchi, A.; Noshiro, H.; Aishima, S. Immunohistochemical analysis of the aggregation of CD1a-positive dendritic cells in resected specimens and its association with surgical outcomes for patients with gallbladder cancer. Transl. Oncol. 2021, 14, 100923. [Google Scholar] [CrossRef]
- Giorello, M.B.; Matas, A.; Marenco, P.; Davies, K.M. , Borzone, F.R.; Calcagno, M.D.L.; Garcia-Rivello, H; Wernicke, A.; Martinez, L.M.; Labovsky, V.; Chasseing, N.A. CD1a- and CD83-positive dendritic cells as prognostic markers of metastasis development in early breast cancer patients. Breast Cancer. 2021, 28, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Coventry, B.J.; Morton, J. CD1a- positive infiltrating-dendritic cell density and 5-year survival from human breast cancer. Br. J. Cancer. 2003, 89, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Gulubova, M.V.; Ananiev, J.R.; Vlaykova, T.I.; Yovchev, Y.; Tsoneva, V.; Manolova, I.M. Role of dendritic cell in progression and clinical outcome of colon cancer. Int. J. Colorectal Dis. 2012, 27, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Hilly, O.; Strenov, Y.; Rath-Wolfson, L.; Hod, R.; Shkedy, Y.; Mizrachi, A.; Koren, R.; Shpitzer, T. The predictive of dendritic cells in early squamous cell carcinoma of tongue. Pathol. Res. Pract. 2016, 212, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Malietzis, G.; Lee, G.H.; Jenkins, J.T.; Bernardo, D.; Moorghen, M.; Knight, S.C.; Al-Hassi, H.O. Prognostic Value of the Tumour-Infiltrating Dendritic Cells in Colorectal Cancer: A Systematic Review. Cell Commun. Adhes. 2015, 22, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Nagorsen, D.; Voigt, S.; Berg, E.; Stein, H.; Thiel, E.; Loddenkemper, C. Tumor-Infiltrating macrophages and dendritic cells in human colorectal cancer: Relation to local regulatory T cells, systemic T-cell response against tumor-associated antigens and survival. J. Transl. Med. 2007, 5, 62. [Google Scholar] [CrossRef] [PubMed]
- Minesaki, A.; Kai, K.; Kuratomi, Y.; Aishima, S. Infiltration of CD1a-positive dendritic cells in advanced laryngeal cancer correlates with unfavorable outcomes post-laryngectomy. BMC Cancer. 2021, 21, 973. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, T.; Gedikoglu, G.; Celik, A.; Onerci, M.; Turan, E. Prognostic significance of Langerhans cell infiltration in cancer of the larynx. Otolaryngol. Head Neck Surg. 2005, 132, 309–316. [Google Scholar] [CrossRef]
- Gallo, O.; Libonati, G.A.; Gallina, E.; Fini-Storchi, O.; Giannini, A.; Urso, C.; Bondi, R. Langerhans cells related to prognosis in patients with laryngeal carcinoma. Arch. Otolaryngol. Head Neack Surg. 1991, 117, 1007–1010. [Google Scholar] [CrossRef]
- Karakök, M.; Bayazit, Y.A.; Ucak, R.; Ozer, E.; Kanlikama, M.; Mumbuc, S.; Sari, I. Langerhans cell related inflammatory reaction in laryngeal squamous cell carcinoma. Auris Nasus Larynx. 2003, 30, 81–84. [Google Scholar] [CrossRef]
- Esteban, F.; Ruiz-Cabello, F.; Gonzalez-Moles, M.A.; Lopez-Gonzalez, M.A.; Funez, R.; Redondo, M. Clinical Significance of Langerhans Cells in Squamous Cell Carcinoma of the larynx. J. Oncol. 2012, 2012, 753296. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, C.S.; Ceausu, A.R.; Gaje, N.P.; Raica, M. Profile and Potential Significance of Dendritic Cells in Head and Neck Squamous Cell Carcinoma. Cancer Diagn. Progn. 2022, 6, 758–763. [Google Scholar] [CrossRef]
- Descamps, G.; Furgiuele, S.; Mhaidly, N.; Journe, F.; Saussez, S. Immune Cell Density Evaluation Improves the Prognostic Values of Staging and p16 in Oropharyngeal Cancer. Cancers. 2022, 14, 5560. [Google Scholar] [CrossRef] [PubMed]
- Binnewies, M.; Mujal, A.M.; Pollack, J.L.; Combes, A.J.; Hardison, E.A.; Barry, K.C.; Tsui, J.; Ruhland, M.K.; Kersten, K.; Abushawish, M.A.; Spasic, M.; Giurintano, J.P.; Chan, V.; Daud, A.I.; Ha, P.; Ye, C.J.; Roberts, E.W.; Krummel, M.F. Unleashing Type-2 Dendritic cells to Drive Protective Antitumor CD4+ Tcell Immunity. Cell. 2019, 177, 556–571. [Google Scholar] [CrossRef]
- Gerhard, G.M.; Bill, R.; Messemaker, M.; Klein, A.M.; Pettet, M.J. Tumor-infiltrating dendritic cell states are conserved across solid human cancers. J. Exp. Med. 2021, 218, e20200264. [Google Scholar] [CrossRef]
- Gardner, A.; Pulido, A.D.M.; Ruffell, B. Dendritic cells and Their Role in Immunotherapy. Front. Immunol. 2020, 11, 924. [Google Scholar] [CrossRef]
- Suzuki, S.; Honma, K.; Matsuyama, T.; Suzuki, K.; Toriyama, K.; Ichinose, A.; Yamamoto, K.; Suematsu, T.; Nakamura, M.; Yui, K.; Kumatori, A. Critical roles of interferon regulatory factor 4 in CD11bhighCD8α⁻dendritic cell development. Proc. Natl. Acad. Sci. USA. 2004, 101, 8981–8986. [Google Scholar] [CrossRef] [PubMed]
- Pinzon-Charry, A.; Maxwell, T.; Lopez, J.A. Dendritic cell dysfunction in cancer: A mechanism for immunosuppression. Immunol. Cell Biol. 2005, 83, 451–461. [Google Scholar] [CrossRef]
- Menetrier-Caux, C.; Montmain, G.; Dieu, M.C.; Bain, C.; Favrot, M.C.; Caux, C.; Blay, J.Y. Inhibition of the Differentiation of Dendritic Cells From CD34+ Progenitors by Tumor Cells: Role of Interleukin-6 and Macrophage Colony-Stimulating Factor. Blood, 1998, 92, 4778–4791. [Google Scholar] [CrossRef]
- Park, S.J.; Nakagawa, T.; Kitamura, H.; Atsumi, T.; Kamon, H.; Sawa, S.; Kamimura, D.; Ueda, N.; Iwakura, Y.; Ishihara, K.; Murakami, M.; Hirano, T. IL-6 Regulates In Vivo Dendritic Cell Differentiation through STAT3 Activation. J. Immunol. 2004, 173, 3844–3854. [Google Scholar] [CrossRef]
- Buelens, C.; Verhasselt, V.; Groote, D.D.; Thielemans, K.; Goldman, M.; Willems, F. Interleukin-10 prevents the generation of dendritic cells from human peripheral blood mononuclear cells cultured with interleukin-4 and granulocyte/macrophage-colony stimulating factor. Eur. J. Immunol. 1997, 27, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Beckebaum, S.; Zhang, X.; Chen, X.; Yu, Z.; Frilling, A.; Dworacki, G.; Grosse-Wilde, H.; Broelsch, C.E.; Gerken, G.; Cicinnati, V.R. Increased Levels of Interleukin-10 in Serum from Patients with Hepatocellular Carcinoma Correlate with Profound Numerical Deficiencies and Immature Phenotype of Circulating Dendritic Cell Subsets. Clin. Cancer Res. 2004, 10, 7260–7269. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V.; Chappell, D.B.; Apolloni, E.; Cabrelle, A.; Wang, M.; Hwu, P.; Restifo, N.P. Unopposed Production of Granulocyte- Macrophage Colony-Stimulating Factor by Tumors Inhibits CD8+ T cell Responses by Dysregulating Antigen-Presenting Cell Maturation. J. Immunol. 1999, 162, 5728–5737. [Google Scholar] [CrossRef] [PubMed]
- Gabrilovich, D.; Ishida, T.; Oyama, T.; Ran, S.; Kravtsov, V.; Nadaf, S.; Carbone, D.P. Vascular Endothelial Growth Factor Inhibits the Development of Dendritic Cells and Dramatically Affects the Differentiation of Multiple Hematopoietic Lineages In Vivo. Blood, 1998, 92, 4150–4166. [Google Scholar] [CrossRef] [PubMed]
- Baysal, H.; Siozopoulou, V.; Zaryouh, H.; Hermans, C.; Lau, H.W.; Lambrechts, H.; Fransen, E.; Pauw, I.D.; Jacobs, J.; Peeters, M.; Pauwels, P.; Vermorken, J.B.; Smits, E.; Lardon, F.; Waele, J.D.; Wouters, A. The prognostic impact of the immune signature in head and neck squamous cell carcinoma. Front. Immunol. 2022, 13, 1001161. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Askari, A.; Malietzis, G.; Bernardo, D.; Clark, S.K.; Knight, S.C.; Al-Hassi, H.O. The role of CD40 expression in dendritic cells in cancer biology; a systemic review. Curr. Cancer Drug Targets. 2014, 14, 610–620. [Google Scholar] [CrossRef]
- Almond, B.; Resser, J.R.; Lindman, B.; Nadaf, S.; Clark, J.I.; Kwon, E.D.; Carbone, D.P.; Gabrilovich, D.I. Clinical significance of defective dendritic cell differentiation in cancer. Clin. Cancer Res. 2000, 5, 1755–66. [Google Scholar]
- Marciscano, A.E.; Anandasabapathy, N. The role of dendritic cells in cancer and anti-tumor immunity. Semin. Immunol. 2021, 52, 101481. [Google Scholar] [CrossRef]
- Vanpouille-Box, C.; Alard, A.; Aryankalayil, M.J.; Sarfraz, Y.; Diamond, J.M.; Schneider, R.J.; Inghirami, G.; Coleman, C.N.; Formenti, S.C.; Demaria, S. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat. Commun. 2017, 8, 15618. [Google Scholar] [CrossRef]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; Yang, H.; Amigorena, S.; Ryffel, B.; Barrat, F.J.; Saftig, P.; Levi, F.; Lidereau, R.; Nogues, C.; Mira, J.P.; Chompret, A.; Joulin, V.; Clavel-Chapelon, F.; Bourhis, J.; Andre, F.; Delaloge, S.; Tursz, T.; Kroemer, G.; Zitvogel, L. Toll-like receptor 4-dependent contribution of the immune system to anticancer chemotherapy and radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef]
- Liang, H.; Deng, L.; Hou, Y.; Meng, X.; Huang, X.; Rao, E.; Zheng, W.; Mauceri, H.; Mack, M.; Xu, M.; Fu, Y.X.; Weichselbaum, R.R. Host STING-dependent MDSC mobilization drives extrinsic radiation resistance. Nat. Commun. 2017, 8, 1736. [Google Scholar] [CrossRef] [PubMed]
- Widau, R.C.; Parekh, A.D.; Ranck, M.C.; Golden, D.W.; Kumar, K.A.; Sood, R.F.; Pitroda, S.P.; Liao, Z.; Huang, X.; Darga, T.E.; Xu, D.; Huang, L.; Andrade, J.; Roizman, B.; Weichselbaum, R.R.; Khodarev, N.N. RIG-I-like receptor LGP2 protects tumor cells from ionizing radiation. Proc. Natl. Acad. Sci. USA. 2014, 111, E484–491. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Liang, H.; Rao, E.; Zheng, W.; Huang, X.; Deng, L.; Zhang, Y.; Yu, X.; Xu, M.; Mauceri, H.; Arina, A.; Weichselbaum, R.R.; Fu, Y.X. Non-canonical NF-κB Antagonizes STING Sensor-Mediated DNA Sensing in Radiotherapy. Immunity. 2018, 49, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Obeid, M.; Tesniere, A.; Ghiringhelli, F.; Fimia, G.M.; Apetoh, L.; Perfettini, J.L.; Castedo, M.; Mignot, G.; Panaretakis, T.; Casares, N.; Metivier, D.; Larochette, N.; Endert, P.V.; Ciccosanti, F.; Piacentini, M.; Zitvogel, L.; Kroemer, G. Calreticulin exposure dictates the immunogenicity of cancer cell death. Nat. Med. 2007, 13, 54–61. [Google Scholar] [CrossRef]
Figure 1.
The average number of infiltrating DCs in primary tumor, metastatic LNs and non-metastatic LNs, respectively. The left figure shows the evaluation for all patients (n = 73), the right figure shows the evaluation for patients after RT/CRT (n = 31) vs. treatment naïve patients (n = 42).
Figure 1.
The average number of infiltrating DCs in primary tumor, metastatic LNs and non-metastatic LNs, respectively. The left figure shows the evaluation for all patients (n = 73), the right figure shows the evaluation for patients after RT/CRT (n = 31) vs. treatment naïve patients (n = 42).
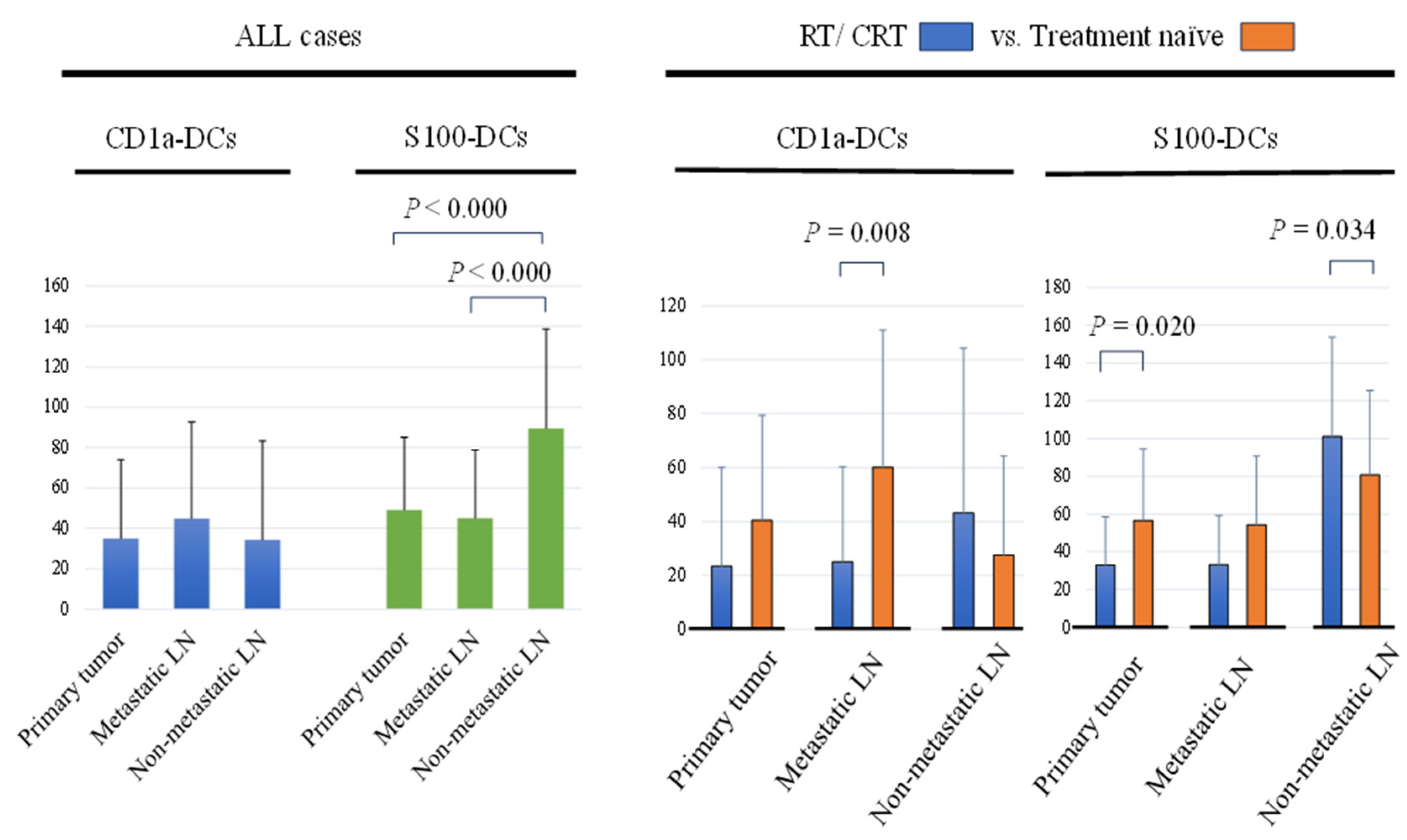
Figure 2.
Kaplan-Meier survival curves according to CD1a-DCs infiltration status in primary tumor, metastatic LNs and non-metastatic LNs. (a-c): Kaplan-Meier survival curves by disease-specific survival (DSS). (d-f): Kaplan-Meier survival curves by overall survival (OS).
Figure 2.
Kaplan-Meier survival curves according to CD1a-DCs infiltration status in primary tumor, metastatic LNs and non-metastatic LNs. (a-c): Kaplan-Meier survival curves by disease-specific survival (DSS). (d-f): Kaplan-Meier survival curves by overall survival (OS).
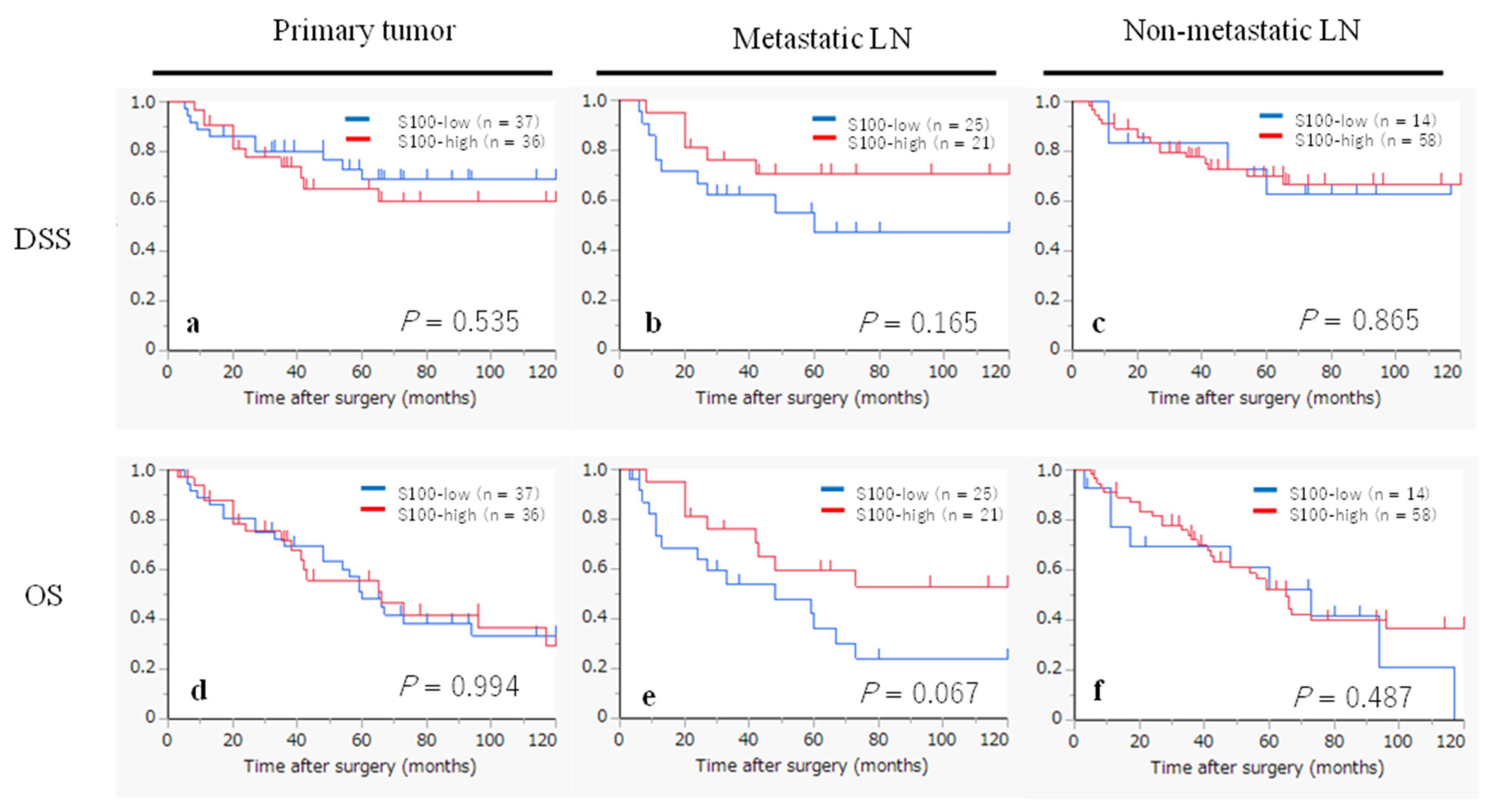
Figure 3.
Kaplan-Meier survival curves according to the S100-DC infiltration status in primary tumor, metastatic LNs and non-metastatic LNs. (a-c): Kaplan-Meier survival curves by disease-specific survival (DSS). (d-f): Kaplan-Meier survival curves by overall survival (OS).
Figure 3.
Kaplan-Meier survival curves according to the S100-DC infiltration status in primary tumor, metastatic LNs and non-metastatic LNs. (a-c): Kaplan-Meier survival curves by disease-specific survival (DSS). (d-f): Kaplan-Meier survival curves by overall survival (OS).
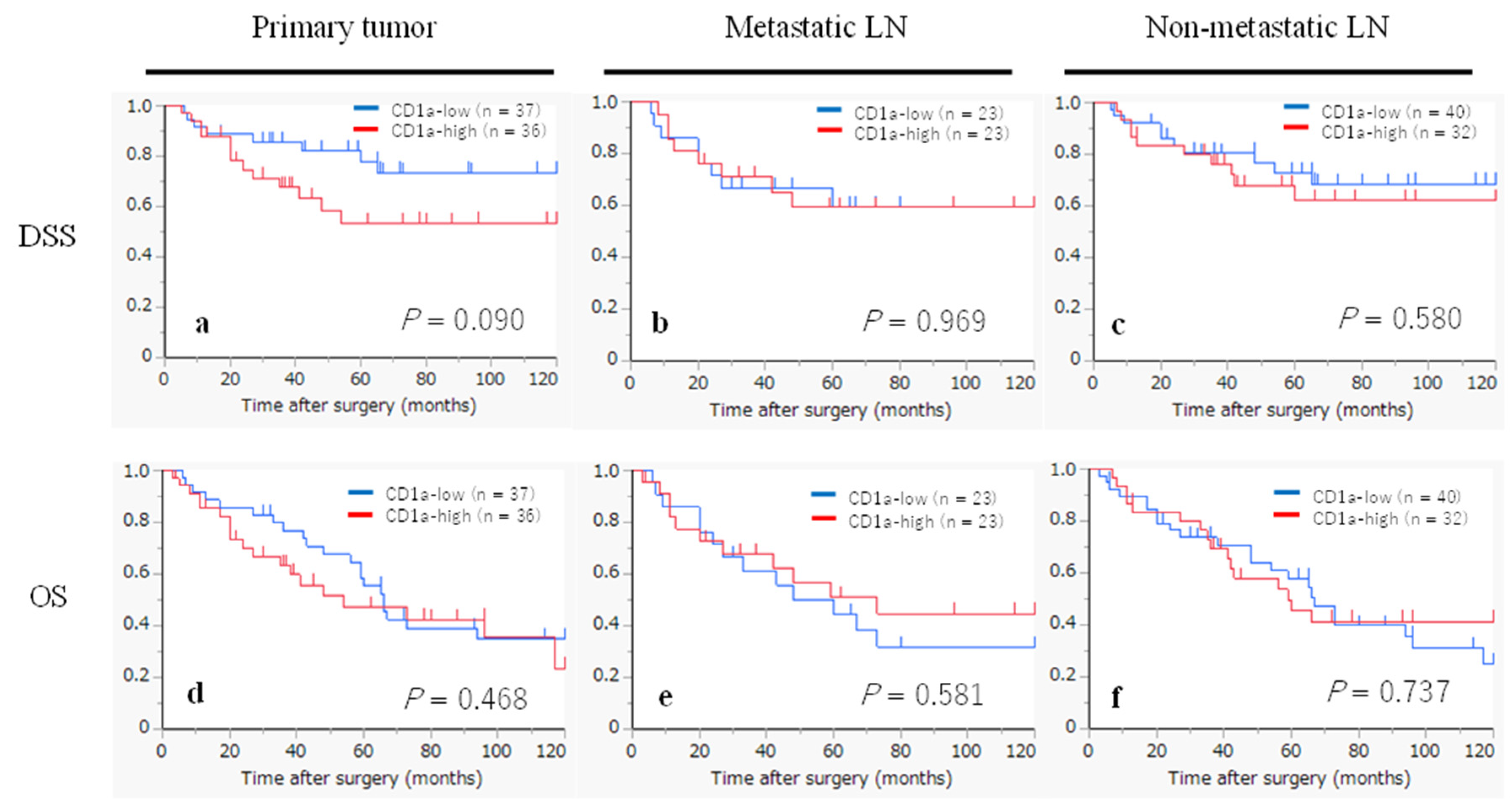
Figure 4.
Immunohistochemistry of CD1a (a-c) and S100 (d-f). Original magnification of each photo was × 200. a, d: primary tumor, b, e: metastatic LN, c, f: non-metastatic LN.
Figure 4.
Immunohistochemistry of CD1a (a-c) and S100 (d-f). Original magnification of each photo was × 200. a, d: primary tumor, b, e: metastatic LN, c, f: non-metastatic LN.
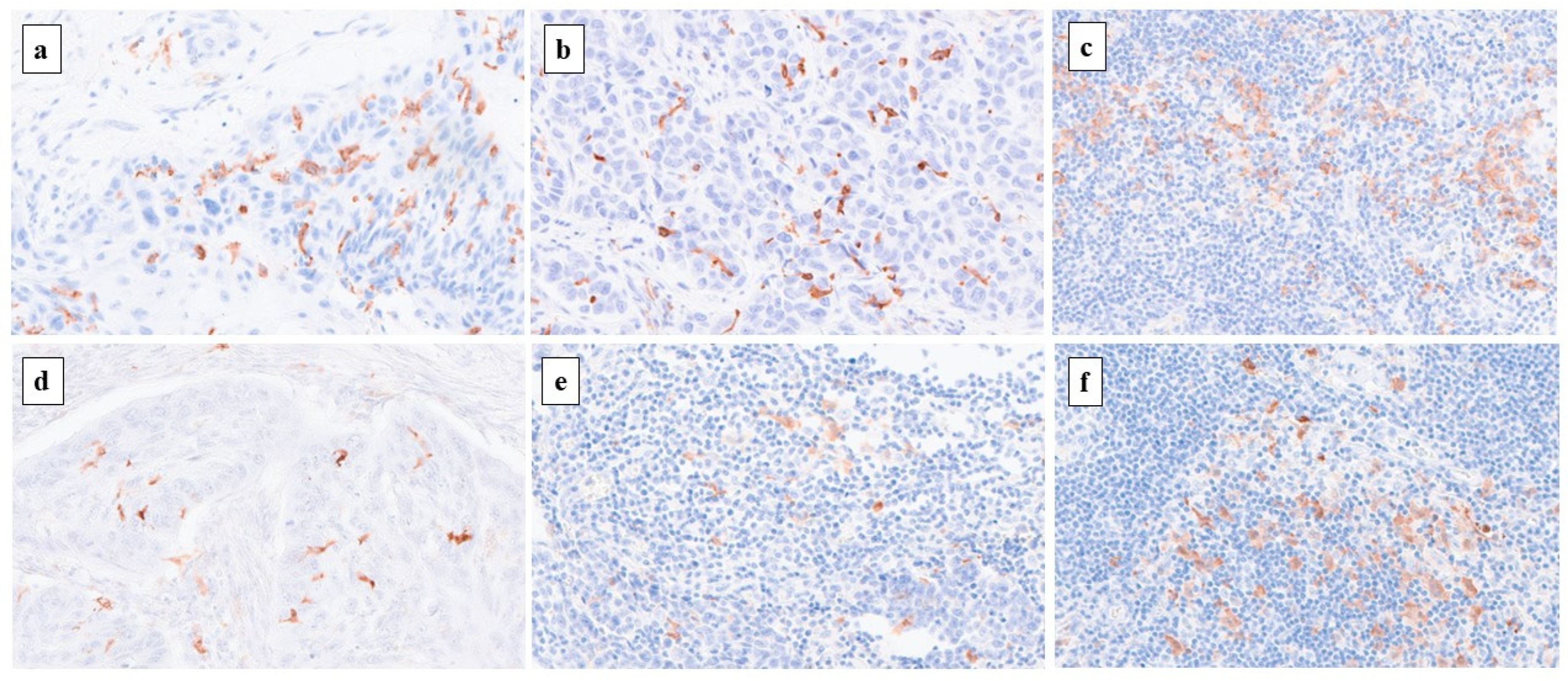

Table 1.
Clinicopathological features of 73 patients with laryngeal cancer.
| Age, years (mean ± SD) | 68.9 ± 9.4 |
| Sex | |
| Male / Female | 70 (95.9%) / 3 (4.1%) |
| Smoking habit | |
| Never / Ex / Current | 8 (11.0%) / 15 (20.5%) / 50 (68.5%) |
| Alcohol abuse | |
| (-) / (+) | 22 (30.1%) / 51 (69.9%) |
| Subsite | |
| Glottis / Supraglottis / Subglottis | 36 (49.3%) / 36 (49.3%) / 1 (1.4%) |
| Histology and differentiation | |
| Well / Mode / Poor / Carcinosarcoma | 33 (45.2%) / 35 (47.9%) / 4 (5.5%) / 1 (1.4%) |
| Primary T stage | |
| T1 / T2 / T3 / T4 | 8 (11.0%) / 21 (28.8%) / 21 (28.8%) / 23 (31.5%) |
| N | |
| (-) / (+) | 27 (63.0%) / 46 (37.0%) |
| Primary M stage | |
| M0 / M1 | 71 (97.3%) / 2 (2.7%) |
| Stage | |
| I / II / III / IV | 5 (6.8%) / 11 (15.1%) / 16 (21.9%) / 41 (56.2%) |
| Treatment background | |
| Surgery without RT / CRT | 42 (57.5%) |
| Surgery after RT | 2 (2.7%) |
| Surgery after CRT | 29 (39.7%) |
Abbreviations: SD, standard deviation; RT, Radiotherapy; CRT, Chemoradiotherapy.
Table 2.
Clinicopathological features per CD1a-DC infiltration.
| Primary tumor (n = 73) |
Metastatic LN (n = 46) |
Non-metastatic LN (n = 72*) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CD1a- low (n = 37) | CD1a- high (n = 36) | P | CD1a -low (n = 23) | CD1a- high (n = 23) | P | CD1a-low (n = 40) | CD1a- high (n = 32) | P | ||
| Age, years (mean ± SD) |
67.1 ± 8.9 | 70.5 ± 9.7 | 0.124 | 68.3 ± 9.5 | 67.5 ± 9.8 | 0.772 | 70.6 ± 8.4 | 66.6 ± 10.3 | 0.074 | |
| Sex | ||||||||||
| Male | 36 (97.3%) | 34 (94.4%) | 0.615 | 23 (100.0%) | 20 (87.0%) | 0.233 | 39 (97.5%) | 30 (93.8%) | 0.582 | |
| Female | 1 (2.7%) | 2 (5.6%) | 0 (0.0%) | 3 (13.0%) | 1 (2.5%) | 2 (6.3%) | ||||
| Primary T stage | ||||||||||
| T1/2 | 17 (46.0%) | 12 (33.3%) | 0.341 | 12 (52.2%) | 10 (43.5%) | 0.768 | 19 (47.5%) | 10 (31.3%) | 0.227 | |
| T3/4 | 20 (54.1%) | 24 (66.7%) | 11 (47.8%) | 13 (56.5%) | 21 (52.5%) | 22 (68.8%) | ||||
| N | ||||||||||
| N (-) | 12 (32.4%) | 15 (41.7%) | 0.473 | 0 (0.0%) | 0 (0.0%) | n/a | 14 (35.0%) | 13 (40.6%) | 0.634 | |
| N (+) | 25 (67.6%) | 21 (58.3%) | 23 (100%) | 23 (100%) | 26 (65.0%) | 19 (59.4%) | ||||
| Primary M stage | ||||||||||
| M0 | 36 (97.3%) | 35 (97.2%) | 1.000 | 22 (95.7%) | 22 (95.7%) | 1.000 | 40 (100.0%) | 30 (93.8%) | 0.194 | |
| M1 | 1 (2.7%) | 1 (2.8%) | 1 (4.4%) | 1 (4.4%) | 0 (0.0%) | 2 (6.3%) | ||||
| Timing of the resected samples | ||||||||||
| After RT or CRT | 16 (43.2%) | 7 (19.4%) | 0.043 | 14 (60.9%) | 6 (26.1%) | 0.036 | 18 (45.0%) | 12 (37.5%) | 0.632 | |
| Treatment naïve** | 21 (56.8%) | 29 (80.6%) | 9 (39.1%) | 17 (73.9%) | 22 (55.0%) | 20 (62.5%) | ||||
* One patient had no non-metastatic LNs. ** Eight cases are biopsy specimens obtained prior to CRT. Abbreviations: DC, dendritic cell; SD, standard deviation; n/a, not available; RT, radiotherapy; CRT, chemoradiotherapy.
Table 3.
Clinicopathological features per S100-DC infiltration.
| Primary tumor (n = 73) |
Metastatic LN (n = 46) |
Non-metastatic LN (n = 72*) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| S100-low (n = 37) | S100-high (n = 36) | P | S100-low (n = 25) | S100- high (n = 21) | P | S100- low (n = 14) | S100- high (n = 58) | P | |
| Age, years (mean ± SD) | 68.0 ± 9.3 | 69.7 ± 9.6 | 0.445 | 68.5 ± 10.5 | 67.2 ± 8.3 | 0.654 | 72.1 ± 9.3 | 68.0 ± 9.4 | 0.150 |
| Sex | |||||||||
| Male | 36 (97.3%) | 34 (94.4%) | 0.615 | 24 (96.0%) | 19 (90.5%) | 0.585 | 13 (92.9%) | 56 (96.6%) | 0.483 |
| Female | 1 (2.7%) | 2 (5.6%) | 1 (4.0%) | 2 (9.5%) | 1 (7.1%) | 2 (3.5%) | |||
| Primary T stage | |||||||||
| T1/2 | 15 (40.5%) | 14 (38.9%) | 1.000 | 7 (28.0%) | 15 (71.4%) | 0.007 | 5 (35.7%) | 24 (41.4%) | 0.770 |
| T3/4 | 22 (59.5%) | 22 (61.1%) | 18 (72.0%) | 6 (28.6%) | 9 (64.3%) | 34 (58.6%) | |||
| N | |||||||||
| N (-) | 15 (40.5%) | 12 (33.3%) | 0.630 | 0 (0.0%) | 0 (0.0%) | n/a | 5 (35.7%) | 22 (37.9%) | 1.000 |
| N (+) | 22 (59.5%) | 24 (66.7%) | 25 (100%) | 21 (100%) | 9 (64.3%) | 36 (62.1%) | |||
| Primary M stage | |||||||||
| M0 | 36 (97.3%) | 35 (97.2%) | 1.000 | 23 (92.0%) | 21 (100.0%) | 0.493 | 12 (85.7%) | 58 (100.0%) | 0.036 |
| M1 | 1 (2.7%) | 1 (2.8%) | 2 (8.0%) | 0 (0.0%) | 2 (14.3%) | 0 (0.0%) | |||
| Timing of resected samples | |||||||||
| After CRT or RT | 17 (45.9%) | 6 (16.7%) | 0.011 | 15 (60.0%) | 5 (23.8%) | 0.019 | 3 (21.4%) | 27 (46.6%) | 0.131 |
| Treatment naïve** | 20 (54.1%) | 30 (83.3%) | 10 (40.0%) | 16 (76.2%) | 11 (78.6%) | 31 (53.5%) | |||
* One patient had no non-metastatic LNs. **Eight cases are biopsy specimens obtained prior to CRT. Abbreviations: DC, dendritic cell; SD, standard deviation; n/a, not available ; RT, radiotherapy; CRT, chemoradiotherapy.
Table 4.
Univariate analyses for DSS and OS in all patients (n = 73).
| Characteristic | n | DSS | OS | ||
|---|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | ||
| Age | 0.683 | 0.783 | |||
| ≤68years | 38 | 1 | 1 | ||
| >68years | 35 | 0.84 (0.35-1.98) | 1.09 (0.59-2.03) | ||
| Sex | 0.473 | 0.470 | |||
| Female | 3 | 1 | 1 | ||
| Male | 70 | 0.48 (0.06-3.58) | 0.59 (0.14-2.47) | ||
| T stage | 0.109 | 0.031 | |||
| T1/T2 | 29 | 1 | 1 | ||
| T3/T4 | 44 | 2.18 (0.84-5.63) | 2.09 (1.07-4.08) | ||
| N stage | 0.025 | 0.037 | |||
| N0 | 27 | 1 | 1 | ||
| N1-3 | 46 | 2.96 (1.14-7.67) | 1.97 (1.04-3.72) | ||
| M stage | 0.050 | 0.179 | |||
| M0 | 71 | 1 | 1 | ||
| M1 | 2 | 4.32 (1.00-18.69) | 2.68 (0.64-11.25) | ||
| CD1a-DCs in primary tumor | 0.098 | 0.472 | |||
| low | 37 | 1 | 1 | ||
| high | 36 | 2.11 (0.87-5.12) | 1.25 (0.67-2.35) | ||
| CD1a-DCs in metastatic LN | 0.969 | 0.586 | |||
| low | 23 | 1 | 1 | ||
| high | 23 | 0.98 (0.36-2.61) | 0.80 (0.36-1.79) | ||
| CD1a-DCs in non-metastatic LN | 0.582 | 0.739 | |||
| low | 40 | 1 | 1 | ||
| high | 32 | 1.28 (0.53-3.08) | 0.90 (0.47-1.70) | ||
| S100-DCs in primary tumor | 0.538 | 0.994 | |||
| low | 37 | 1 | 1 | ||
| high | 36 | 1.31 (0.55-3.09) | 1.00 (0.54-1.87) | ||
| S100-DCs in metastatic LN | 0.177 | 0.077 | |||
| low | 25 | 1 | 1 | ||
| high | 21 | 0.50 (0.18-1.37) | 0.47 (0.21-1.08) | ||
| S100-DCs in non-metastatic LN | 0.866 | 0.490 | |||
| low | 14 | 1 | 1 | ||
| high | 58 | 0.91 (0.30-2.73) | 0.77 (0.36-1.62) |
Abbreviations: DSS, disease specific survival; OS, overall survival; HR, hazard ratio; CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



