
Submitted:
14 December 2023
Posted:
15 December 2023
You are already at the latest version
Abstract
We aimed to evaluate the survival benefits of coadministering statins and multityrosine kinase inhibitors (TKIs) in patients with advanced hepatocellular carcinoma (HCC). Data from the Health Insurance Review and Assessment Service in Korea (2010–2020) were utilized. Statin use (≥28 cumulative defined daily doses) was analyzed, with 1,534 statin users matched to 6,136 non-users (1:4 ratio) using propensity scores. Primary and secondary outcomes were overall survival (OS) and progression-free survival (PFS). Statin use significantly improved OS (hazard ratio [HR] 0.77, 95% confidence interval [CI] 0.72–0.82, P<0.001) and PFS (HR 0.78, 95% CI 0.74–0.84, P<0.001). Continuous or post-TKI statin users had better OS, while discontinuation after TKI use led to poorer OS. Both lipophilic and hydrophilic statins improved OS and PFS, particularly with ≥730 cumulative defined daily doses. In conclusion, combining statins and TKIs in patients with advanced HCC yielded significant survival benefits, influenced by statin dosage and duration. Continuous statin administration post-TKI treatment is crucial for improving outcomes in patients with HCC.
Keywords:
statin
; multityrosine kinase inhibitor
; sorafenib resistance
; hepatocellular carcinoma
; lipophilic statin
; hydrophilic statin
1. Introduction
Hepatocellular carcinoma (HCC), the most common type of primary liver cancer, is one of the leading causes of cancer mortality worldwide [1]. Most patients with HCC are at an advanced stage at the time of diagnosis, and systemic therapy is the only feasible treatment modality at this stage [2].
Sorafenib and lenvatinib, multityrosine kinase inhibitors (TKIs), were used as first-line treatment for patients with advanced HCC for almost 10 years, until immune checkpoint inhibitor-based immunotherapy was introduced [3,4]. TKIs are still considered as an alternative for patients with contraindications to atezolizumab plus bevacizumab (Atezo+Bev) therapy or for sequential therapy after Atezo+Bev treatment failure. In a previous study, although TKIs resulted in improved overall survival (OS) compared to that with placebo, the survival benefit on average was 3 months [3,5]. Thus, resistance to TKIs has been a major challenge in the systemic treatment of HCC [6].
Statins are competitive inhibitors of 3-hydroxy-3-methylglutaryl-CoA reductase (HMG-CoA), and they also have potential chemopreventive and cytotoxic effects on cancer cells in different types of cancers, independent of their lipid-lowering effect [7,8,9]. Moreover, statin use may be associated with a lower risk of HCC development in patients with hepatitis B or C infection and diabetes mellitus (DM) [10,11,12,13,14]. Molecular evidence shows that statins might potentiate the anticancer effects of TKIs, specifically in chronic myeloid leukemia, non-small cell lung cancer (NSCLC), renal cell cancer, and head and neck squamous cell cancer (HNSCC) [15,16,17,18]. Additionally, two retrospective cohort studies verified that statins could improve clinical outcomes in patients with NSCLC and HNSCC treated with TKIs [19,20].
The Health Insurance Review and Assessment Service (HIRA) in Korea is responsible for claims review and quality assessment of the National Health Insurance (NHI). HIRA research database provides information on age, sex, codes for diagnosis, prescribed drugs, and treatment, including surgical history and procedures.
We aimed to verify the potential clinical benefits of statins in patients with advanced HCC treated with sorafenib or lenvatinib by analyzing large-scale data from HIRA in Korea. We also investigated the impact of the timing of statin administration (pre-TKI use, continuous use, and post-TKI use) and optimal statin type and dose on the survival outcomes of these patients.
2. Materials and Methods
2.1. Data Source
More than 98% of Koreans are obligated to join the NHI Service. HIRA is a national institution that reviews and evaluates medical costs and the quality of medical care. In the present study, information from the HIRA database, including data on patient demographics, prescriptions, treatments, and diagnoses, was reviewed. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Ajou University Hospital (AJIRB MED-EXP-2021-552). The requirement for prior consent was waived because of the retrospective nature of the study. De-identification processing was performed, and the data were approved by the national health information data request review committee of HIRA.
2.2. Study Population and Definition of Terms
Overall, 22,144 patients, aged ≥18 years, who were diagnosed with HCC and took sorafenib or lenvatinib for more than 1 day between January 1, 2010 and December 31, 2020 were initially screened. Considering that the treatment response is evaluated every 2–3 months in patients with advanced HCC treated with sorafenib or lenvatinib, we defined sorafenib- or lenvatinib-treated patients as those who had received TKIs for >60 days without interruption. Patients who received sorafenib or lenvatinib for <60 days (n= 9,548) were excluded. Thus, 12,596 patients were included in the analysis. Statin dose was measured using the cumulative defined daily dose (cDDD). Statin use was defined as ≥28 cDDDs of filled statin prescriptions and nonuse was defined as <28 cDDDs. Of the 12,596 patients, 11,062 were statin nonusers and 1,534 were statin users (Figure 1). Statin dose was subclassified as follows: 28–180 cDDDs, 181–365 cDDDs, 366–730 cDDDs, 731–1095 cDDDs, and ≥1096 cDDDs.
2.3. Data collection
Using the Korea Classification of Disease (KCD), based on the International Classification of Diseases, 11th Revision (ICD-11), we collected research data as codes for all diseases, prescriptions, and procedures. Diseases diagnosed within 1 year before HCC diagnosis were identified as comorbidities. We collected anthropometric and demographic data such as age, sex, and region. Clinical data included a history of chronic hepatitis B or C, nonalcoholic fatty liver disease, alcoholic liver disease, or other liver diseases such as primary biliary cirrhosis (PBC) and comorbidities such as liver cirrhosis, hypertension (HTN), DM, cerebrovascular disease, and cardiovascular disease. Additional data were collected as follows: history of statin exposure, including the dose and type of statin, timing of statin use, duration of statin administration (cDDD), history of HCC treatment before sorafenib or lenvatinib use, and history of aspirin and antidiabetic medications such as dipeptidyl peptidase-4 (DPP-4) inhibitor, insulin, metformin, sodium glucose cotransporter-2 (SGLT-2) inhibitor, sulfonylurea, and thiazolidinedione (TZD).
2.4. Outcomes
The primary outcome was OS, defined as the time between the index date (first day of TKI treatment) and death from any cause. The secondary outcome was progression-free survival (PFS), defined as the time between the first prescription and last administration of TKIs.
2.5. Statistical analysis
All statistical analyses were performed using R version 4.1.3 (http://www.r-project.org; R Foundation for Statistical Computing, Vienna, Austria), with a P-value of <0.05 considered statistically significant. Continuous variables with normal distribution are expressed as mean ± standard deviation, and categorical variables are expressed as numbers with percentages. Statin users were matched with nonusers in a 1:4 ratio using propensity score matching to balance baseline characteristics and minimize potential confounding. Variables included in propensity score matching were age, sex, etiology (chronic hepatitis B or C, nonalcoholic fatty liver disease, alcoholic liver disease, and PBC), and DM. Kaplan–Meier analysis was performed to compare OS and PFS between groups. Univariate and multivariate Cox regression analyses were performed to identify the risk factors associated with all-cause death and tumor progression. The results are presented as hazards ratios (HRs) with 95% confidence intervals (CIs).
3. Results
3.1. Comparing Baseline Characteristics between Statin Users and Nonusers in Unmatched and PS-matched Cohorts
The study compared baseline characteristics between statin users and nonusers in unmatched and propensity score-matched cohorts. Initially, 12,596 participants were involved, and after propensity score matching for age, sex, etiology, and DM, 1,534 statin users (including 973 using lipophilic statins and 561 using hydrophilic statins) were matched in a 1:4 ratio with 6,136 nonusers. Table 1 summarizes the baseline characteristics of statin users and nonusers. The median follow-up period was 95 months (range: 56–190 months) for statin nonusers and 119.5 months (range: 63–250 months) for statin users. The baseline characteristics revealed that statin users tended to be older and had a higher prevalence of alcoholic liver disease but a lower frequency of chronic hepatitis B virus infection compared to nonusers. Additionally, statin users were more likely to have comorbid conditions such as DM, fatty liver, cirrhosis, PBC, HTN, cardiovascular disease, and cerebrovascular disease. Moreover, a larger proportion of statin users were using aspirin and antidiabetic medications. After propensity score matching, both groups showed no significant differences in the proportion of patients with a history of alcoholic liver disease and DM. The majority of both statin users (91.4%) and nonusers (93.1%) were being treated with sorafenib (Table 1).
3.2. Statin Use and Survival Outcome
Both OS and PFS were significantly better for statin users than for statin nonusers in the PS-matched cohort (log rank P<0.001; Figure 3a,b). The positive impact of statin use was noticeable among patients treated with sorafenib (log rank P<0.001 and P=0.001, respectively; Figure S1a,b), but not in those treated with lenvatinib (shown in Figure S2a,b).
Multivariate Cox regression analysis was performed to identify factors associated with OS and PFS. Statin use was linked to improved OS (HR, 0.77; 95% CI, 0.72–0.82; P<0.001), as were other factors like aspirin, metformin, SGLT-2 inhibitors, sulfonylurea use, and a history of HTN and cardiovascular disease. However, insulin use (HR, 1.24; 95% CI, 1.16–1.33; P<0.001; Table 2) was associated with worse OS. For PFS, factors associated with better outcomes included living in an urban region, having a history of HTN, cardiovascular disease, cerebrovascular disease, and using statins (HR, 0.78; 95% CI, 0.74–0.84; P<0.001), aspirin (HR, 0.63; 95% CI, 0.55–0.73; P <0.001), metformin (HR, 0.72; 95% CI, 0.62–0.84; P<0.001), and sulfonylureas (HR, 0.83; 95% CI, 0.69–1.00; P = 0.049). On the other hand, age > 60 years (HR, 1.01; 95% CI, 1.00–1.01; P=0.006) and insulin use (HR, 1.26; 95% CI, 1.18–1.35; P<0.001) were associated with poorer PFS (Table 3).
3.3. Timing of Statin Use and Survival Outcome
In multivariate analysis for OS, it was found that continuous statin use (HR, 0.87; 95% CI, 0.80–0.95; P=0.002) and post-TKI statin use (HR, 0.43; 95% CI, 0.38–0.50; P<0.001) were significantly associated with improved OS. However, pre-TKI statin use was identified as an independent risk factor for poorer OS (HR, 1.33; 95% CI, 1.14–1.54; P<0.001). Other factors associated with better OS included a history of DM, fatty liver, HTN, cardiovascular disease, and the use of aspirin, metformin, SGLT-2 inhibitors, and sulfonylureas. Conversely, insulin use significantly deteriorated OS (HR, 1.23; 95% CI, 1.15–1.32; P<0.001). In the analysis for PFS, only post-TKI statin use (HR, 0.42; 95% CI, 0.38–0.48; P<0.001) significantly improved PFS, while continuous statin use did not (HR, 0.94; 95% CI, 0.87–1.02; P=0.122). Other factors influencing PFS were consistent with those for OS. Factors such as living in an urban region, a history of DM, HTN, cardiovascular disease, and cerebrovascular disease, as well as the use of aspirin, DPP-4 inhibitors, metformin, and sulfonylureas, were associated with better PFS. Pre-TKI statin use (HR, 1.56; 95% CI, 1.35–1.80; P<0.001) and insulin use (HR, 1.25; 95% CI, 1.17–1.33; P<0.001) were identified as independent risk factors for an unfavorable outcome in terms of PFS. In summary, the timing of statin use had a significant impact on survival outcomes, with post-TKI statin use showing the most favorable results, while pre-TKI statin use had a detrimental effect on survival. Multiple other factors, including comorbidities and medication use, also influenced survival outcomes.
3.4. Statin Type and Survival Outcome
Regarding statin type, hydrophilic statins showed a more favorable outcomes in both OS and PFS compared to lipophilic statins (log rank P<0.001 and P=0.006, respectively; Figure 3c,d). Notably, both types of statins led to significant improvements in survival despite significant differences in survival outcomes. For users of lipophilic statins, HR for PFS was 0.74 (95% CI, 0.69–0.80; P<0.001) and for OS, it was 0.75 (95% CI, 0.69–0.81; P<0.001). For users of hydrophilic statins, HR for PFS was 0.63 (95% CI, 0.57–0.69; P<0.001), and for OS, it was 0.59 (95% CI, 0.53–0.66; P<0.001; Table S1). This indicates that while both statin types had a positive impact on survival, hydrophilic statins appeared to offer even greater benefits.
3.5. Statin Dose and Survival Outcome
In the PS-matched cohort, the administration of a high cumulative dose of statins (>730 cDDD) had a substantial positive impact on both OS and PFS. In the group receiving 731 to 1095 cDDD, the HR was 0.46 (95% CI, 0.46–0.69; P<0.001) for tumor progression and 0.48 (95% CI, 0.48–0.75; P<0.001) for all-cause death, both indicating significant benefits (P<0.001). In the group with more than 1,096 cDDD, the HR was even lower at 0.34 (95% CI, 0.28–0.41; P<0.001) for tumor progression and 0.34 (95% CI, 0.28–0.42; P<0.001) for all-cause death, underlining a strong association between higher cumulative statin doses and improved survival outcomes (shown in Table S2 and Figure 4). This suggests that higher cumulative doses of statins are linked to more favorable results in terms of survival, emphasizing the importance of the dose in achieving positive effects.
3.6. Multivariate Stratified Analysis
Multivariate stratified analysis is summarized in Figure 5. In the OS analysis, statin users demonstrated significantly favorable outcomes after adjustment for most covariates, including age, sex, etiology, comorbidities, and comedications. However, statin use was not associated with a lower risk of mortality in patients receiving lenvatinib, patients with underlying PBC, and in SGLT-2 inhibitor and TZD users (Figure 5a). Similar results were observed in PFS analysis (Figure 5b).
3.7. Subgroup Analysis According to Sorafenib or Lenvatinib Treatment
For patients receiving sorafenib treatment, the analysis revealed that statin use was an independent factor associated with improved OS and PFS, with HR of 0.76 (95% CI, 0.71–0.82; P<0.001) for OS. Other factors associated with better OS in this subgroup included living in an urban area, having a history of HTN, cardiovascular disease, cerebrovascular disease, and the use of aspirin, metformin, and sulfonylurea. On the contrary, insulin use was associated with a poorer OS (HR, 1.20; 95%CI, 1.12–1.28; P<0.001; Table S3). PFS analysis yielded similar results, except that older age (>60 years) was associated with poor PFS, and sulfonylurea use did not have a meaningful effect on PFS (Table S4).
In the sorafenib-treated group, both continuous (HR, 0.87; 95% CI, 0.80–0.95; P=0.002) and post-TKI statin use (HR, 0.44; 95% CI, 0.38–0.51; P<0.001) significantly improved OS, along with a history of cerebrovascular and cardiovascular disease and the use of aspirin and antidiabetic medications. In contrast, pre-TKI statin use (HR, 1.28; 95% CI, 1.10–1.49; P=0.002) and insulin use increased the risk of tumor progression (Table S5). For PFS in the sorafenib-treated group, post-TKI statin use was beneficial in reducing the risk of tumor progression (HR, 0.43; 95% CI, 0.38–0.48; P<0.001), along with other factors such as living in urban region and histories of DM, HTN, and vascular disease, as well as the use of aspirin and most antidiabetic medications (Table S6). In the subgroup analysis of patients treated with lenvatinib, the results were less clear, with only insulin use significantly impacting survival outcomes (Table S7 and S8). When assessing the timing of statin use in the lenvatinib group, post-TKI statin use was associated with favorable outcomes in OS (HR, 0.29; 95% CI, 0.11–0.79; P=0.015), while pre-TKI statin use (HR, 2.27; 95% CI, 1.23–4.22; P=0.009), older age (>60 years), and insulin use were independent risk factors for poor OS (Table S9). For PFS, only post-TKI statin use was beneficial (HR, 0.36; 95% CI, 0.17–0.77; P=0.009) with age >60 years, but insulin use remained a risk factor for tumor progression. Overall, the subgroup analysis showed disparities between sorafenib and lenvatinib treatment groups, possibly due to the smaller number of participants in the lenvatinib group (Table S10).

Table 5.
Univariate and multivariate cox regression analysis for PFS according to statin use pattern.
Table 5.
Univariate and multivariate cox regression analysis for PFS according to statin use pattern.
| Variables | Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | |||
| Statin use pattern | ||||||||
| Non-user | reference | reference | ||||||
| pre-TKI use | 1.53 | 1.33–1.77 | <0.001 | 1.56 | 1.35–1.80 | <0.001 | ||
| continuous use from TKI treatment | 0.86 | 0.80–0.93 | <0.001 | 0.94 | 0.87–1.02 | 0.122 | ||
| post-TKI use | 0.38 | 0.34–0.43 | <0.001 | 0.42 | 0.38–0.48 | <0.001 | ||
| Age ≥60 yr | 1.04 | 0.99–1.09 | 0.156 | 1.00 | 1.00–1.01 | 0.032 | ||
| Sex, female | 0.98 | 0.91–1.06 | 0.603 | 1.02 | 0.95–1.10 | 0.571 | ||
| Region, urban | 0.88 | 0.82–0.94 | <0.001 | 0.86 | 0.80–0.92 | <0.001 | ||
| DM, yes | 0.91 | 0.85–0.98 | 0.007 | 0.92 | 0.86–0.99 | 0.023 | ||
| Fatty liver, yes | 0.94 | 0.89–1.00 | 0.054 | |||||
| Cirrhosis, yes | 0.82 | 0.79-0.86 | <0.001 | |||||
| HTN, yes | 0.80 | 0.75–0.84 | <0.001 | 0.86 | 0.81–0.91 | <0.001 | ||
| cardiovascular disease, yes | 0.84 | 0.79–0.88 | <0.001 | 0.91 | 0.86–0.96 | 0.001 | ||
| cerebrovascular disease, yes | 0.81 | 0.76–0.87 | <0.001 | 0.91 | 0.85–0.98 | 0.012 | ||
| Aspirin use, yes | 0.57 | 0.50–0.65 | <0.001 | 0.68 | 0.59–0.77 | <0.001 | ||
| DPP-4 inhibitor use, yes | 0.78 | 0.70–0.88 | <0.001 | 0.88 | 0.78–0.99 | 0.035 | ||
| Insulin use, yes | 1.13 | 1.06–1.20 | <0.001 | 1.25 | 1.17–1.33 | <0.001 | ||
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.75 | 0.64–0.87 | <0.001 | ||
| SGLT-2 inhibitor use, yes | 0.70 | 0.50–0.98 | 0.038 | 0.74 | 0.53–1.03 | 0.077 | ||
| Sulfonylurea use, yes | 0.73 | 0.61–0.86 | <0.001 | 0.81 | 0.67–0.97 | 0.022 | ||
| Thiazolidinedione use, yes | 0.64 | 0.49–0.85 | 0.002 | |||||
Abbreviations: CI, confidence interval; HR = hazard ratio; DM, diabetes mellitus; HTN, hypertension; DPP, dipeptidyl peptidase; PFS, progression free survival; SGLT, sodium-glucose cotransporter; TKI, tyrosine kinase inhibitor.
4. Discussion
This study is noteworthy because it is the first to investigate the potential survival benefits of statins in patients with advanced HCC treated with TKIs using nationwide and multicenter data from the HIRA in Korea. The study begins by acknowledging that statins have previously been associated with a reduced risk of HCC development in patients with chronic liver disease and a decreased risk of tumor recurrence after curative resection in early-stage HCC [10-14However, statin use is often limited due to safety concerns, particularly in patients with cirrhotic liver. While a cirrhotic liver is vulnerable to drug-induced liver injury or statin associated muscle symptoms because of impaired hepatic metabolism of statins via cytochrome P 268 (CYP)3A4 and reduced multi-drug resistance protein 2 membrane transporter activity, fatal cases are rare [23,24]. The clinical benefits of statins in advanced cirrhosis need to be emphasized beyond potential risks [25,26,27]. Additionally, statins have been shown to induce antitumor effects through various mechanisms, such as apoptosis, regulation of autophagy, and interaction with the tumor microenvironment [28,29,30,31,32,33,34]. These mechanisms are linked to pathways associated with sorafenib resistance, making statins a potential strategy to overcome resistance to TKIs.
Simvastatin can re-sensitize sorafenib-resistant HCC cells by inhibiting the hypoxia-inducible 280 factor-1α/PPAR-γ/PKM2 axis and suppressing PKM2-mediated glycolysis, as demonstrated in vitro [35]. Fluvastatin combined with sorafenib induced apoptosis and inhibited hepatic stellate cell activation, showing a synergistic antitumor effect in vivo [36,37,38]. Similarly, in vivo studies, pravastatin combined with sorafenib was shown to further inhibit cancer cell proliferation and exhibit greater efficacy against HCC compared to sorafenib alone [39]. However, the effective role of pravastatin combined with sorafenib in clinical studies is inconsistent [40,41,42,43]. Despite this, statins have been proposed as potential therapeutic agents to overcome sorafenib resistance based on previous experimental and epidemiological evidence. Interestingly, continuous use of statins, whether initiated before or after TKI treatment, was associated with better survival outcomes, emphasizing the importance of maintaining consistent statin administration even after an HCC diagnosis, consistent with previous findings[44].
The study further explored the impact of the type of statin, revealing that both lipophilic and hydrophilic statins provide survival benefits for patients with advanced HCC undergoing sorafenib treatment, contrary to previous studies favoring lipophilic statins [12,14]. The effects of statins may vary based on their type and underlying liver disease. In cirrhotic liver, intrahepatic angiogenesis, sinusoidal remodeling, and reduced liver perfusion can impair the functionality of CYP enzymes. In particular, hepatic expression of CYP3A, a key enzyme involved in the metabolism of both sorafenib and lipophilic statins, was found to be reduced in cirrhotic liver. While lipophilic statins passively diffuse through tissues and are metabolized by CYP450, hydrophilic statins are only minimally affected by CYP450, are taken up by hepatic transporters, and can more selectively disrupt lipid metabolism in HCC cells compared to lipophilic statins [45]. In this context, combining hydrophilic statins with sorafenib may offer added benefits for patients with advanced HCC or cirrhosis. In this study, hydrophilic statins exhibited superior survival benefits compared to lipophilic statins, challenging previous preferences for lipophilic statins.
The relationship between various medications and survival outcomes in patients with HCC has been investigated in this study. Aspirin, DPP-4 inhibitors, and metformin are associated with improved outcomes [46,47,48,49], while insulin use and pre-TKI statin use are linked to an increased risk of mortality and tumor recurrence in statin users. In advanced cirrhosis, exogenous insulin is frequently used to prevent hepatoxicity from other diabetes medications. Increased levels of free serum IGF-1 due to insulin resistance in these patients may promote hepatocarcinogenesis via autophagy, leading to poor prognosis in HCC patients with type II DM [50]. The presence of cardiovascular or cerebrovascular disease in statin users was found to ameliorate all-cause mortality and tumor recurrence, suggesting that statins may have a preventive effect on the survival of HCC patients, particularly those with a history of vascular events.
We emphasize that statins, when coadministered with sorafenib, can offer significant survival benefits in higher cumulative dose of statins, specifically exceeding 730 cDDD for patients with advanced HCC. The study underscores the importance of maintaining statin administration consistently, even after an HCC diagnosis. This approach can be considered as a promising combination therapy, taking into account factors such as cost, effectiveness, and tolerability.
We acknowledge several limitations in this study. First, the study is retrospective in nature and was conducted on a health insurance claims database lacking information on certain risk factors of HCC, such as anthropometric information (including body mass index and waist circumference), laboratory findings assessing hepatic reserve function (e.g., Child-Pugh or modified albumin-bilirubin grade), and clinical details related to cirrhosis complications (such as ascites, hepatic encephalopathy, and variceal bleeding). Although we acknowledge these missing data could be critical for assessing patient prognosis and outcomes, we were unable to control these potential confounding factors. Second, the study considered all-cause death as the primary outcome, which may not provide insights into liver-related mortality, a more specific and relevant endpoint for HCC patients. Third, although liver function of patients with advanced HCC may be initially favorable at the timing point of statin administration, the progressive decline in functional reserve volume of liver and portal HTN due to tumor thrombosis, can lead to a rapid deterioration of liver function, necessitating the discontinuation of statin use. Insufficient details regarding tumor staging, specifically the absence of information on factors such as tumor volume or the extent of portal vein invasion and distant metastasis, could potentially limit conclusive insights of statin dosage and duration in this study. Further exploration on the relationships between effectiveness and dosages of statins is warranted to offer valuable contributions in real-world practices. Finally, given the distinct underlying factors for HCC in Korea compared to Western countries, the generalizability of our findings to other healthcare systems may be limited. Regional variations in HCC etiology should be considered when interpreting the study results.
In summary, the study highlights that statins, when coadministered with sorafenib, can substantially improve OS and PFS in patients with advanced HCC. It emphasizes the importance of continuous statin administration, even after an HCC diagnosis. However, more research, including in vitro studies to understand the molecular mechanisms, and well-designed prospective clinical trials, are needed to establish a solid basis for combining sorafenib and statins as a treatment strategy for advanced HCC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Survival outcomes according to statin type; Table S2. Survival outcomes according to statin dose; Table S3. Univariate and multivariate cox regression analysis for OS treated with sorafenib according to statin use in a PS-matched cohort; Table S4. Univariate and multivariate cox regression analysis for PFS treated with sorafenib according to statin use in a PS-matched cohort; Table S5. Univariate and multivariate cox regression analysis for OS treated with sorafenib according to statin use pattern in a PS-matched cohort; Table S6. Univariate and multivariate cox regression analysis for PFS treated with sorafenib according to statin use pattern in a PS-matched cohort; Table S7. Univariate and multivariate cox regression analysis for OS treated with lenvatinib according to statin use in a PS-matched cohort; Table S8. Univariate and multivariate cox regression analysis for PFS treated with lenvatinib according to statin use in a PS-matched cohort; Table S9. Univariate and multivariate cox regression analysis for OS treated with lenvatinib according to statin use pattern in a PS-matched cohort; Table S10. Univariate and multivariate cox regression analysis for the PFS treated with lenvatinib according to the statin use pattern in a PS-matched cohort; Figure S1. Kaplan–Meier curves of OS and PFS according to statin use and statin type in the sorafenib subgroup; Figure S2. Kaplan–Meier curves of OS and PFS according to statin use and statin type in the lenvatinib subgroup.
Author Contributions
Cho H.J. conceived the idea of the study and planned statistical analysis. Han J.E. and Cho H.J. drafted the manuscript. Park B.H and Kim J.S did statistical analysis. Han J.E., Cho H.J., Kim S.S., and Cheong J.Y. contributed to the interpretation of the results; All authors reviewed the manuscript draft and revised it critically on intellectual content. All authors approved the final version of the manuscript to be published.
Funding
This research was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (Grant number: HR22C1734 and HR21C1003), as well as the Bio and Medical Technology Development Program of the National Research Foundation funded by the Korean government Ministry of Science and ICT (Grant Number NRF-2021R1C1C1009619, NRF-2022R1H1A2093189, 2022R1A2C2092422).
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Ajou University Hospital (AJIRB MED-EXP-2021-552).
Informed Consent Statement
The requirement for prior consent was waived because of the retrospective nature of the study. De-identification processing was performed, and the data were approved by the national health information data request review committee of HIRA.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol 2022, 77, 1598–1606. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009, 10, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Blanco, C.; Fondevila, F.; García-Palomo, A.; González-Gallego, J.; Mauriz, J.L. Sorafenib resistance in hepatocarcinoma: role of hypoxia-inducible factors. Exp Mol Med 2018, 50, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Göbel, A.; Zinna, V.M.; Dell’Endice, S.; Jaschke, N.; Kuhlmann, J.D.; Wimberger, P.; Rachner, T.D. Anti-tumor effects of mevalonate pathway inhibition in ovarian cancer. BMC Cancer 2020, 20, 703. [Google Scholar] [CrossRef]
- Ricco, N.; Flor, A.; Wolfgeher, D.; Efimova, E.V.; Ramamurthy, A.; Appelbe, O.K.; Brinkman, J.; Truman, A.W.; Spiotto, M.T.; Kron, S.J. Mevalonate pathway activity as a determinant of radiation sensitivity in head and neck cancer. Mol Oncol 2019, 13, 1927–1943. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.L.; E, J.Y.; Lin, Y.; Rebbeck, T.R.; Lu, S.E.; Shang, M.; Kelly, W.K.; D’Amico, A.; Stein, M.N.; Zhang, L.; et al. Individual and joint effects of metformin and statins on mortality among patients with high-risk prostate cancer. Cancer Med 2020, 9, 2379–2389. [Google Scholar] [CrossRef] [PubMed]
- Goh, M.J.; Sinn, D.H.; Kim, S.; Woo, S.Y.; Cho, H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; et al. Statin use and the risk of hepatocellular carcinoma in patients with chronic hepatitis B. Hepatology 2020, 71, 2023–2032. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.Y.; Zhu, G.Q.; Wang, Y.; Zheng, J.N.; Ruan, L.Y.; Cheng, Z.; Hu, B.; Fu, S.W.; Zheng, M.H. Systematic review with network meta-analysis: statins and risk of hepatocellular carcinoma. Oncotarget 2016, 7, 21753–21762. [Google Scholar] [CrossRef]
- Lai, S.W.; Liao, K.F.; Lai, H.C.; Muo, C.H.; Sung, F.C.; Chen, P.C. Statin use and risk of hepatocellular carcinoma. Eur J Epidemiol 2013, 28, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Joo, Y.S.; Kang, S.C.; Koh, H.B.; Han, S.H.; Yoo, T.H.; Kang, S.W.; Park, J.T. Association of statin treatment with hepatocellular carcinoma risk in end-stage kidney disease patients with chronic viral hepatitis. Sci Rep 2022, 12, 10807. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Duberg, A.S.; Aleman, S.; Hagstrom, H.; Nguyen, L.H.; Khalili, H.; Chung, R.T.; Ludvigsson, J.F. Lipophilic statins and risk for hepatocellular carcinoma and death in patients with chronic viral hepatitis: results from a nationwide Swedish population. Ann Intern Med 2019, 171, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Su, V.Y.; Yang, K.Y.; Huang, T.Y.; Hsu, C.C.; Chen, Y.M.; Yen, J.C.; Chou, Y.C.; Chang, Y.L.; He, C.H. The efficacy of first-line tyrosine kinase inhibitors combined with co-medications in Asian patients with EGFR mutation non-small cell lung cancer. Sci Rep 2020, 10, 14965. [Google Scholar] [CrossRef] [PubMed]
- Matusewicz, L.; Czogalla, A.; Sikorski, A.F. Attempts to use statins in cancer therapy: an update. Tumour Biol 2020, 42, 1010428320941760. [Google Scholar] [CrossRef] [PubMed]
- Woodard, J.; Joshi, S.; Viollet, B.; Hay, N.; Platanias, L.C. AMPK as a therapeutic target in renal cell carcinoma. Cancer Biol Ther 2010, 10, 1168–1177. [Google Scholar] [CrossRef]
- Jang, H.J.; Woo, Y.M.; Naka, K.; Park, J.H.; Han, H.J.; Kim, H.J.; Kim, S.H.; Ahn, J.S.; Kim, T.; Kimura, S.; et al. Statins enhance the molecular response in chronic myeloid leukemia when combined with tyrosine kinase inhibitors. Cancers (Basel) 2021, 13, 5543. [Google Scholar] [CrossRef]
- Hung, M.S.; Chen, I.C.; Lee, C.P.; Huang, R.J.; Chen, P.C.; Tsai, Y.H.; Yang, Y.H. Statin improves survival in patients with EGFR-TKI lung cancer: a nationwide population-based study. PLOS ONE 2017, 12, e0171137. [Google Scholar] [CrossRef]
- Lebo, N.L.; Griffiths, R.; Hall, S.; Dimitroulakos, J.; Johnson-Obaseki, S. Effect of statin use on oncologic outcomes in head and neck squamous cell carcinoma. Head Neck 2018, 40, 1697–1706. [Google Scholar] [CrossRef]
- Singh, S.; Singh, P.P.; Roberts, L.R.; Sanchez, W. Chemopreventive strategies in hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol 2014, 11, 45–54. [Google Scholar] [CrossRef]
- Yang, S.Y.; Wang, C.C.; Chen, K.D.; Liu, Y.W.; Lin, C.C.; Chuang, C.H.; Tsai, Y.C.; Yao, C.C.; Yen, Y.H.; Hsiao, C.C.; et al. Statin use is associated with a lower risk of recurrence after curative resection in BCLC stage 0-A hepatocellular carcinoma. BMC Cancer 2021, 21, 70. [Google Scholar] [CrossRef]
- Pose, E.; Trebicka, J.; Mookerjee, R.P.; Angeli, P.; Ginès, P. Statins: old drugs as new therapy for liver diseases? J Hepatol 2019, 70, 194–202. [Google Scholar] [CrossRef]
- Björnsson, E.; Jacobsen, E.I.; Kalaitzakis, E. Hepatotoxicity associated with statins: reports of idiosyncratic liver injury post-marketing. J Hepatol 2012, 56, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, D.E.; Serper, M.A.; Mehta, R.; Fox, R.; John, B.; Aytaman, A.; Baytarian, M.; Hunt, K.; Albrecht, J.; Njei, B.; et al. Effects of hypercholesterolemia and statin exposure on survival in a large national cohort of patients with cirrhosis. Gastroenterology 2019, 156, 1693–1706.e12. [Google Scholar] [CrossRef] [PubMed]
- Abraldes, J.G.; Villanueva, C.; Aracil, C.; Turnes, J.; Hernandez-Guerra, M.; Genesca, J.; Rodriguez, M.; Castellote, J.; García-Pagán, J.C.; Torres, F.; et al. Addition of simvastatin to standard therapy for the prevention of variceal rebleeding does not reduce rebleeding but increases survival in patients with cirrhosis. Gastroenterology 2016, 150, 1160–1170.e3. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, N.; Chapin, S.; Goldberg, D.S.; Reddy, K.R.; Taddei, T.H.; Kaplan, D.E. Statin exposure is associated with reduced development of acute-on-chronic liver failure in a Veterans Affairs cohort. J Hepatol 2022, 76, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kundu, M.; Viollet, B.; Guan, K.L. AMPK and mTOR regulate autophagy through direct phosphorylation of Ulk1. Nat Cell Biol 2011, 13, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.F.; Chen, H.L.; Tai, W.T.; Feng, W.C.; Hsu, C.H.; Chen, P.J.; Cheng, A.L. Activation of phosphatidylinositol 3-kinase/Akt signaling pathway mediates acquired resistance to sorafenib in hepatocellular carcinoma cells. J Pharmacol Exp Ther 2011, 337, 155–161. [Google Scholar] [CrossRef]
- Wang, H.; Xu, L.; Zhu, X.; Wang, P.; Chi, H.; Meng, Z. Activation of phosphatidylinositol 3-kinase/Akt signaling mediates sorafenib-induced invasion and metastasis in hepatocellular carcinoma. Oncol Rep 2014, 32, 1465–1472. [Google Scholar] [CrossRef]
- Liu, L.P.; Ho, R.L.; Chen, G.G.; Lai, P.B. Sorafenib inhibits hypoxia-inducible factor-1α synthesis: implications for antiangiogenic activity in hepatocellular carcinoma. Clin Cancer Res 2012, 18, 5662–5671. [Google Scholar] [CrossRef]
- Zhao, D.; Zhai, B.; He, C.; Tan, G.; Jiang, X.; Pan, S.; Dong, X.; Wei, Z.; Ma, L.; Qiao, H.; et al. Upregulation of HIF-2α induced by sorafenib contributes to the resistance by activating the TGF-α/EGFR pathway in hepatocellular carcinoma cells. Cell Signal 2014, 26, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Zou, X.; Song, Y.; Duan, Z.; Liu, L. PFKFB3/HIF-1α feedback loop modulates sorafenib resistance in hepatocellular carcinoma cells. Biochem Biophys Res Commun 2019, 513, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.; Dong, Z.; Cai, X.; Shen, J.; Xu, Y.; Zhang, M.; Li, H.; Yu, W.; Chen, W. Hypoxia induces sorafenib resistance mediated by autophagy via activating FOXO3a in hepatocellular carcinoma. Cell Death Dis 2020, 11, 1017. [Google Scholar] [CrossRef] [PubMed]
- Blanc, J.F.; Khemissa, F.; Bronowicki, J.P.; Monterymard, C.; Perarnau, J.M.; Bourgeois, V.; Obled, S.; Abdelghani, M.B.; Mabile-Archambeaud, I.; Faroux, R.; et al. Phase 2 trial comparing sorafenib, pravastatin, their combination or supportive care in HCC with Child-Pugh B cirrhosis. Hepatol Int 2021, 15, 93–104. [Google Scholar] [CrossRef]
- Feng, J.; Dai, W.; Mao, Y.; Wu, L.; Li, J.; Chen, K.; Yu, Q.; Kong, R.; Li, S.; Zhang, J.; et al. Simvastatin re-sensitizes hepatocellular carcinoma cells to sorafenib by inhibiting HIF-1α/PPAR-γ/PKM2-mediated glycolysis. J Exp Clin Cancer Res 2020, 39, 24. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Doudican, N.A.; Quay, E.; Orlow, S.J. Fluvastatin enhances sorafenib cytotoxicity in melanoma cells via modulation of AKT and JNK signaling pathways. Anticancer Res 2011, 31, 3259–3265. [Google Scholar]
- Cheng, Y.; Luo, R.; Zheng, H.; Wang, B.; Liu, Y.; Liu, D.; Chen, J.; Xu, W.; Li, A.; Zhu, Y. Synergistic anti-tumor efficacy of sorafenib and fluvastatin in hepatocellular carcinoma. Oncotarget 2017, 8, 23265–23276. [Google Scholar] [CrossRef]
- Hisada, T.; Ayaori, M.; Ohrui, N.; Nakashima, H.; Nakaya, K.; Uto-Kondo, H.; Yakushiji, E.; Takiguchi, S.; Terao, Y.; Miyamoto, Y.; et al. Statin inhibits hypoxia-induced endothelin-1 via accelerated degradation of HIF-1α in vascular smooth muscle cells. Cardiovasc Res 2012, 95, 251–259. [Google Scholar] [CrossRef]
- Hijona, E.; Banales, J.M.; Hijona, L.; Medina, J.F.; Arenas, J.; Herreros-Villanueva, M.; Aldazabal, P.; Bujanda, L. Pravastatin inhibits cell proliferation and increased MAT1A expression in hepatocarcinoma cells and in vivo models. Cancer Cell Int 2012, 12, 5. [Google Scholar] [CrossRef]
- Riaño, I.; Martín, L.; Varela, M.; Serrano, T.; Núñez, O.; Mínguez, B.; Rodrigues, P.M.; Perugorria, M.J.; Banales, J.M.; Arenas, J.I. Efficacy and safety of the combination of pravastatin and sorafenib for the treatment of advanced hepatocellular carcinoma (ESTAHEP clinical trial). Cancers (Basel) 2020, 12, 1900. [Google Scholar] [CrossRef] [PubMed]
- Jouve, J.L.; Lecomte, T.; Bouché, O.; Barbier, E.; Khemissa Akouz, F.; Riachi, G.; Nguyen Khac, E.; Ollivier-Hourmand, I.; Debette-Gratien, M.; Faroux, R.; et al. Pravastatin combination with sorafenib does not improve survival in advanced hepatocellular carcinoma. J Hepatol 2019, 71, 516–522. [Google Scholar] [CrossRef]
- Kawata, S.; Yamasaki, E.; Nagase, T.; Inui, Y.; Ito, N.; Matsuda, Y.; Inada, M.; Tamura, S.; Noda, S.; Imai, Y.; et al. Effect of pravastatin on survival in patients with advanced hepatocellular carcinoma. A randomized controlled trial. Br J Cancer 2001, 84, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P.; Natarajan, Y.; Liu, Y.; El-Serag, H.B. Statin use after diagnosis of hepatocellular carcinoma is associated with decreased mortality. Clin Gastroenterol Hepatol 2019, 17, 2117–2125.e3. [Google Scholar] [CrossRef] [PubMed]
- Lauschke, V.M.; Ingelman-Sundberg, M. The importance of patient-specific factors for hepatic drug response and toxicity. Int J Mol Sci 2016, 17, 1714. [Google Scholar] [CrossRef]
- Goh, M.J.; Sinn, D.H. Statin and aspirin for chemoprevention of hepatocellular carcinoma: time to use or wait further? Clin Mol Hepatol 2022, 28, 380–395. [Google Scholar] [CrossRef]
- Zeng, R.W.; Yong, J.N.; Tan, D.J.H.; Fu, C.E.; Lim, W.H.; Xiao, J.; Chan, K.E.; Tan, C.; Goh, X.L.; Chee, D.; et al. Meta-analysis: chemoprevention of hepatocellular carcinoma with statins, aspirin and metformin. Aliment Pharmacol Ther 2023, 57, 600–609. [Google Scholar] [CrossRef]
- Hsu, W.H.; Sue, S.P.; Liang, H.L.; Tseng, C.W.; Lin, H.C.; Wen, W.L.; Lee, M.Y. Dipeptidyl peptidase 4 inhibitors decrease the risk of hepatocellular carcinoma in patients with chronic hepatitis C infection and type 2 diabetes mellitus: a nationwide study in Taiwan. Front Public Health 2021, 9, 711723. [Google Scholar] [CrossRef]
- Nishina, S.; Yamauchi, A.; Kawaguchi, T.; Kaku, K.; Goto, M.; Sasaki, K.; Hara, Y.; Tomiyama, Y.; Kuribayashi, F.; Torimura, T.; et al. Dipeptidyl peptidase 4 inhibitors reduce hepatocellular carcinoma by activating lymphocyte chemotaxis in mice. Cell Mol Gastroenterol Hepatol 2019, 7, 115–134. [Google Scholar] [CrossRef]
- Shan, Y.; Lu, C.; Wang, J.; Li, M.; Ye, S.; Wu, S.; Huang, J.; Bu, S.; Wang, F. IGF-1 contributes to liver cancer development in diabetes patients by promoting autophagy. Ann Hepatol 2022, 27, 100697. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study population. DM, diabetes mellitus; PBC, primary biliary cholangitis.In terms of statin administration timing, pre-TKI statin use was defined as statin use before TKI treatment with discontinuation after TKI treatment initiation. Post TKI use was defined as statin administration initiated after TKI administration, given concurrently for more than 30 days. Continuous statin use was defined as statin use from the period before TKI treatment to the period after TKI treatment (Figure 2) Lipophilic statins included lovastatin, simvastatin, atorvastatin, fluvastatin, and pitavastatin, whereas hydrophilic statins included pravastatin and rosuvastatin. Regional distribution was subclassified to determine urban–rural differences in the survival outcomes of patients; urban regions included Seoul, Gyeonggi province, and Special cities, whereas others were classified as rural regions.
Figure 1.
Flow chart of the study population. DM, diabetes mellitus; PBC, primary biliary cholangitis.In terms of statin administration timing, pre-TKI statin use was defined as statin use before TKI treatment with discontinuation after TKI treatment initiation. Post TKI use was defined as statin administration initiated after TKI administration, given concurrently for more than 30 days. Continuous statin use was defined as statin use from the period before TKI treatment to the period after TKI treatment (Figure 2) Lipophilic statins included lovastatin, simvastatin, atorvastatin, fluvastatin, and pitavastatin, whereas hydrophilic statins included pravastatin and rosuvastatin. Regional distribution was subclassified to determine urban–rural differences in the survival outcomes of patients; urban regions included Seoul, Gyeonggi province, and Special cities, whereas others were classified as rural regions.
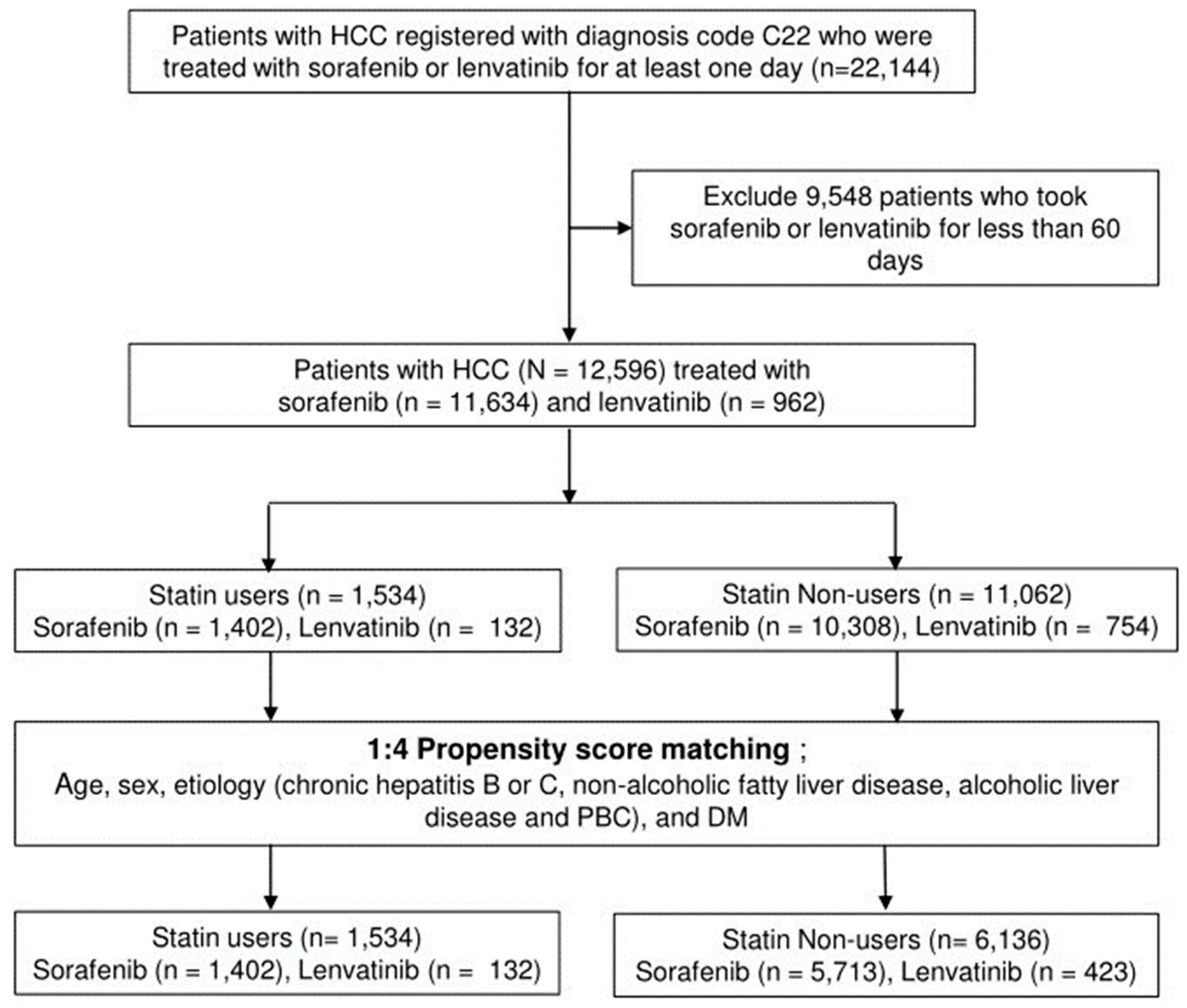
Figure 2.
Definitions of statin use regarding the timing of statin administration.
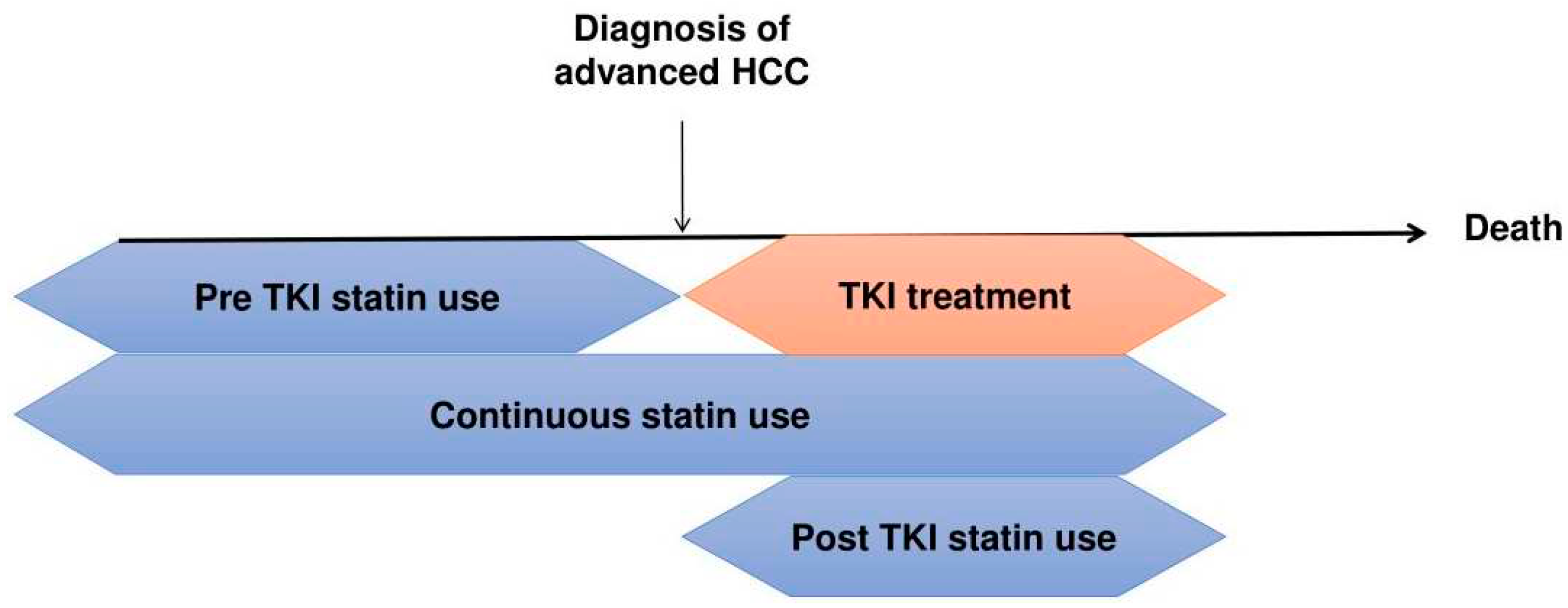
Figure 3.
Kaplan-Meier curves of OS and PFS according to statin use and statin type in the PS-matched cohort. (a) Comparison of OS between statin users and non-users. (b) Comparison of PFS between statin users and non-users. (c) Comparison of OS according to statin type (hydrophilic vs lipophilic). (d) Comparison of PFS according to statin type (hydrophilic vs lipophilic). OS; overall survival, PFS; progression-free survival, PS; propensity score.
Figure 3.
Kaplan-Meier curves of OS and PFS according to statin use and statin type in the PS-matched cohort. (a) Comparison of OS between statin users and non-users. (b) Comparison of PFS between statin users and non-users. (c) Comparison of OS according to statin type (hydrophilic vs lipophilic). (d) Comparison of PFS according to statin type (hydrophilic vs lipophilic). OS; overall survival, PFS; progression-free survival, PS; propensity score.
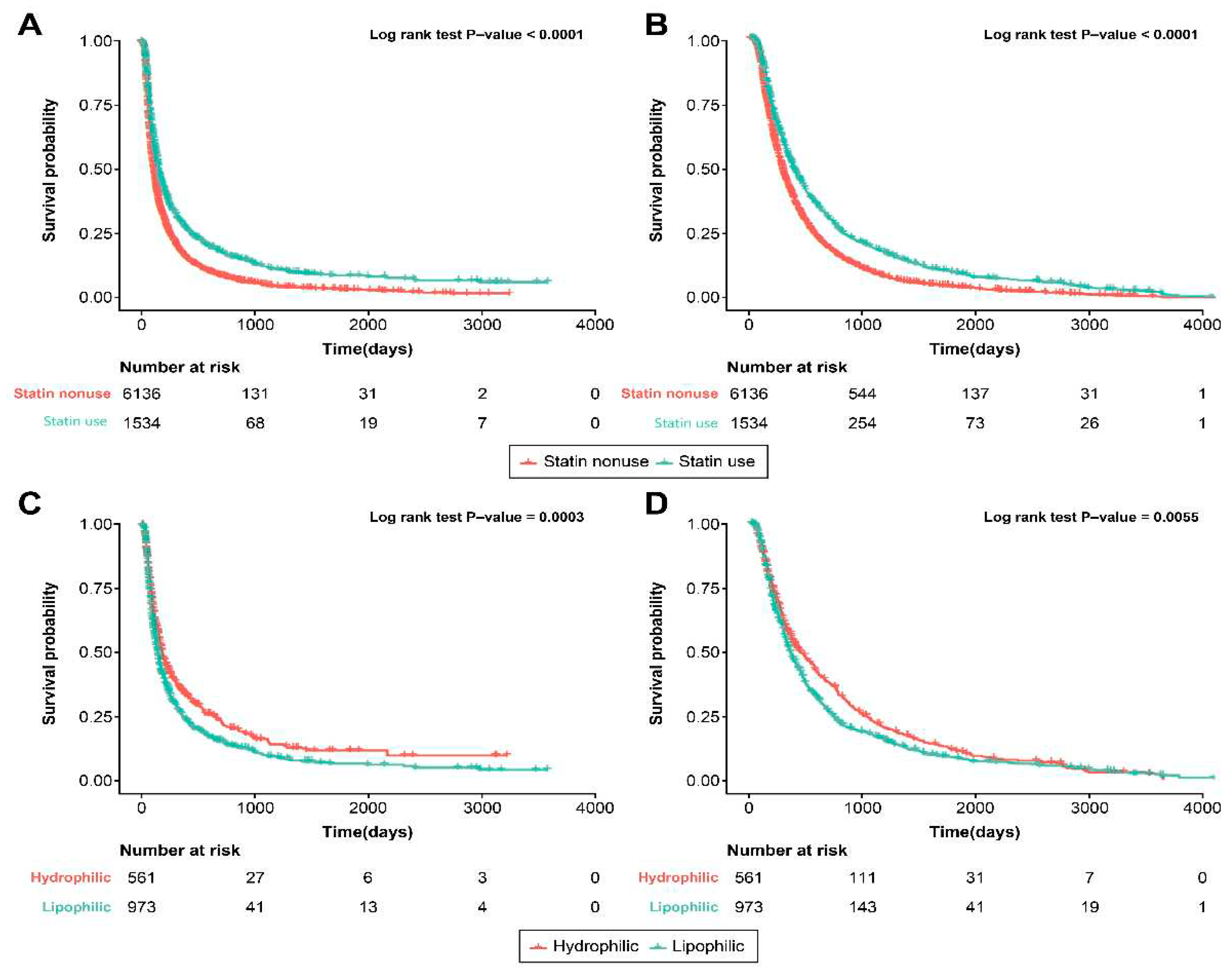
Figure 4.
Kaplan-Meier curves for OS and PFS according to cumulative statin dose in PS-matched cohort. (a) OS of patients with HCC treated with sorafenib or lenvatinib according to cumulative statin dose. (b) PFS of patients with HCC treated with sorafenib or lenvatinib according to cumulative statin dose. HCC, hepatocellular carcinoma; OS; overall survival, PFS; progression-free survival, PS; propensity score.
Figure 4.
Kaplan-Meier curves for OS and PFS according to cumulative statin dose in PS-matched cohort. (a) OS of patients with HCC treated with sorafenib or lenvatinib according to cumulative statin dose. (b) PFS of patients with HCC treated with sorafenib or lenvatinib according to cumulative statin dose. HCC, hepatocellular carcinoma; OS; overall survival, PFS; progression-free survival, PS; propensity score.
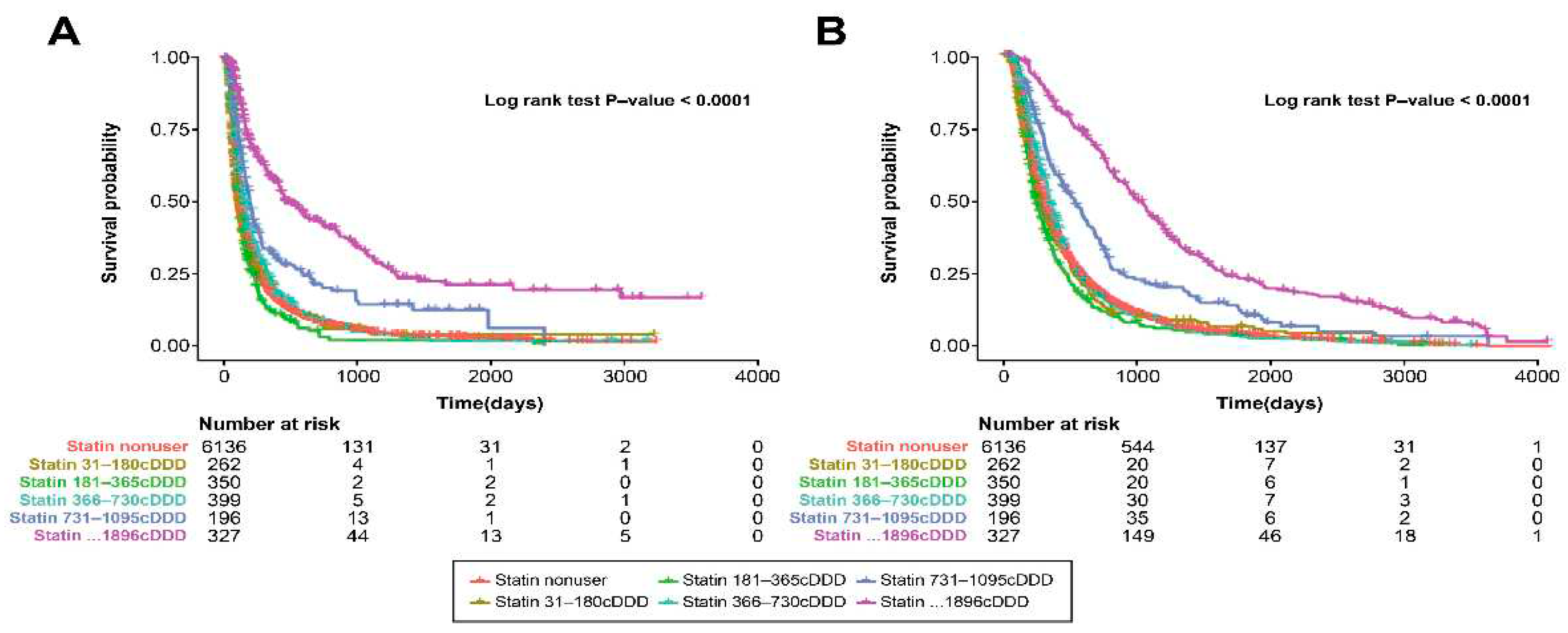
Figure 5.
Multivariate stratified analyses for the association between statin usage and OS/PFS in patients with HCC treated with sorafenib or lenvatinib. HR and 95% CI of the difference in mortality and tumor progression risk between statin users and non-users were determined using multivariate Cox regression hazard models based on adjusted covariates. (a) Multivariable stratified analyses for the association between statin use and OS in patients with HCC treated with sorafenib or lenvatinib. (b) Multivariate stratified analyses for the association between statin use and PFS in patients with HCC treated with sorafenib or lenvatinib. HCC, hepatocellular carcinoma; CI; confidence interval, HR; hazard ratio, OS; overall survival, PFS; progression-free survival, PS; propensity score.
Figure 5.
Multivariate stratified analyses for the association between statin usage and OS/PFS in patients with HCC treated with sorafenib or lenvatinib. HR and 95% CI of the difference in mortality and tumor progression risk between statin users and non-users were determined using multivariate Cox regression hazard models based on adjusted covariates. (a) Multivariable stratified analyses for the association between statin use and OS in patients with HCC treated with sorafenib or lenvatinib. (b) Multivariate stratified analyses for the association between statin use and PFS in patients with HCC treated with sorafenib or lenvatinib. HCC, hepatocellular carcinoma; CI; confidence interval, HR; hazard ratio, OS; overall survival, PFS; progression-free survival, PS; propensity score.
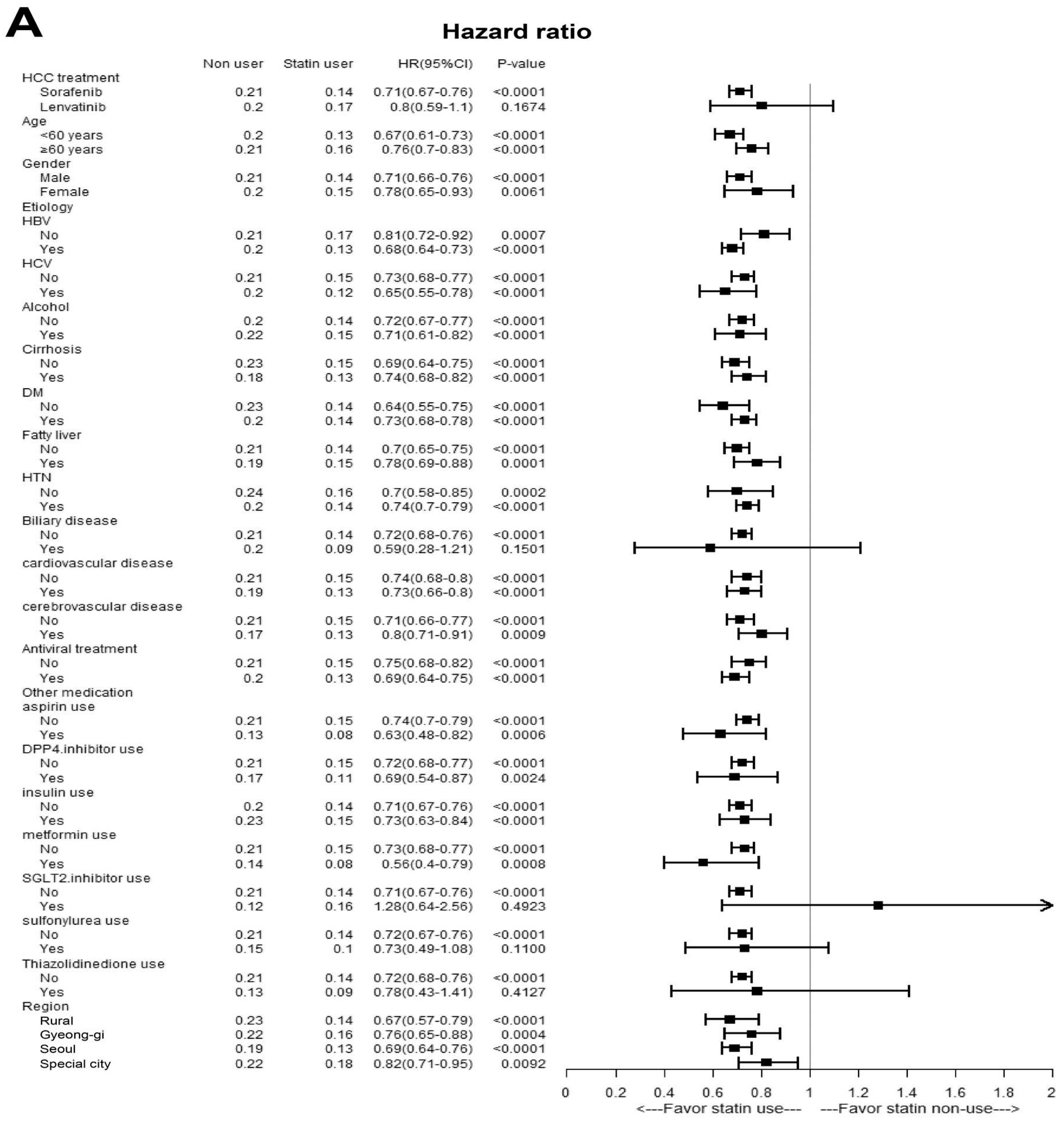
Table 1.
Baseline characteristics of statin users and non-users.
| Before PS-matching | After PS-matching | |||||
|---|---|---|---|---|---|---|
| Non-users (n=11062) | Statin users (n=1534) | P-value | Non-users (n=6136) | Statin users (n=1534) | P-value | |
| Age | 56.48 (8.28) | 59.87 (7.29) | <0.001 | 59.363 (7.013) | 59.870 (7.290) | 0.012 |
| Sex, male, No. (%) | 9652 (87.3%) | 1359 (88.6%) | 0.139 | 5439 (88.6%) | 1359 (88.6%) | 0.957 |
| Region, No. (%) | 0.033 | 0.004 | ||||
| Rural | 1542 (13.9%) | 202 (13.2%) | 912 (14.9%) | 202 (13.2%) | ||
| Gyeong-gi | 1721 (15.6%) | 242 (15.8%) | 906 (14.8%) | 242 (15.8%) | ||
| Seoul | 5590 (50.5%) | 826 (53.8%) | 3066 (50.0%) | 826 (53.8%) | ||
| Special city | 2209 (20.0%) | 264 (17.2%) | 1252 (20.4%) | 264 (17.2%) | ||
| HCC treatment, No. (%) | 0.010 | 0.021 | ||||
| Sorafenib | 10308 (93.2%) | 1402 (91.4%) | 5713 (93.1%) | 1402 (91.4%) | ||
| Lenvatinib | 754 (6.8%) | 132 (8.6%) | 423 (6.9%) | 132 (8.6%) | ||
| Statin use pattern, No. (%) | - | - | ||||
| pre-TKI use | - | 218 (14.2%) | - | 218 (14.2%) | ||
| continuous use from TKI treatment | - | 950 (61.9%) | - | 950 (61.9%) | ||
| post-TKI use | - | 366 (23.9%) | - | 366 (23.9%) | ||
| Etiology, No. (%) | ||||||
| HBV | 9363 (84.6%) | 1109 (72.3%) | <0.001 | 4818 (78.5%) | 1109 (72.3%) | <0.001 |
| HCV | 1368 (12.4%) | 185 (12.1%) | 0.732 | 793 (12.9%) | 185 (12.1%) | 0.364 |
| Alcoholic | 1472 (13.3%) | 263 (17.1%) | <0.001 | 972 (15.8%) | 263 (17.1%) | 0.214 |
| History of comorbidities | ||||||
| History of DM, No. (%) | 6413 (58.0%) | 1303 (84.9%) | <0.001 | 5163 (84.1%) | 1303 (84.9%) | 0.442 |
| History of fatty liver, No. (%) | 1735 (15.7%) | 415 (27.1%) | <0.001 | 1352 (22.0%) | 415 (27.1%) | <0.001 |
| History of cirrhosis, No. (%) | 4832 (43.7%) | 713 (46.5%) | 0.0385 | 2892(47.1%) | 713(46.5%) | 0.6473 |
| History of HTN, No. (%) | 7067 (63.9%) | 1397 (91.1%) | <0.001 | 4433 (72.2%) | 1397 (91.1%) | <0.001 |
| History of PBC, No. (%) | 52 (0.5%) | 17 (1.1%) | 0.002 | 45 (0.7%) | 17 (1.1%) | 0.143 |
| History of cardiovascular disease, No. (%) | 2448 (22.1%) | 717 (46.7%) | <0.001 | 1614 (26.3%) | 717 (46.7%) | <0.001 |
| History of cerebrovascular disease, No. (%) | 970 (8.8%) | 437 (28.5%) | <0.001 | 718 (11.7%) | 437 (28.5%) | <0.001 |
| Antiviral treatment, No. (%) | ||||||
| HBV treatment | 7752 (70.1%) | 842 (54.9%) | <0.001 | 3905 (63.6%) | 842 (54.9%) | <0.001 |
| HCV treatment | 248 (2.2%) | 47 (3.1%) | 0.046 | 793 (12.9%) | 185 (12.1%) | 0.364 |
| Other medication, No. (%) | ||||||
| aspirin use | 264 (2.4%) | 106 (6.9%) | <0.001 | 158 (2.6%) | 106 (6.9%) | <0.001 |
| DPP-4 inhibitor use | 279 (2.5%) | 109 (7.1%) | <0.001 | 241 (3.9%) | 109 (7.1%) | <0.001 |
| insulin use | 1717 (15.5%) | 285 (18.6%) | 0.002 | 1010 (16.5%) | 285 (18.6%) | 0.048 |
| metformin use | 229 (2.1%) | 54 (3.5%) | <0.001 | 173 (2.8%) | 54 (3.5%) | 0.147 |
| SGLT-2 inhibitor use | 27 (0.2%) | 18 (1.2%) | <0.001 | 25 (0.4%) | 18 (1.2%) | <0.001 |
| sulfonylurea use | 131 (1.2%) | 38 (2.5%) | <0.001 | 109 (1.8%) | 38 (2.5%) | 0.073 |
| Thiazolidinedione use | 43 (0.4%) | 21 (1.4%) | <0.001 | 36 (0.6%) | 21 (1.4%) | 0.001 |
| Median treatment duration (days) | 260.00 (149.00, 498.00) | 337.00 (180.00, 708.00) | <0.001 | 269.00 (152.00, 512.00) | 337.00 (180.00, 708.00) | <0.001 |
| Median follow-up period (months) | 95.00 (56.00, 190.00) | 119.50 (63.00, 250.00) | <0.001 | 96.00 (56.00, 199.00) | 119.50 (63.00, 250.00) | <0.001 |
Abbreviations: DM, diabetes mellitus; DPP, dipeptidyl peptidase; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HTN, hypertension; PBC, primary biliary cholangitis; PS, propensity score; SGLT, sodium-glucose cotransporter; TKI, tyrosine kinase inhibitor.
Table 2.
Univariate and multivariate cox regression analysis for OS according to statin use in the entire PS-matched cohort.
Table 2.
Univariate and multivariate cox regression analysis for OS according to statin use in the entire PS-matched cohort.
| Variables | Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | ||
| Statin use, yes | 0.71 | 0.66–0.76 | <0.001 | 0.77 | 0.72–0.82 | <0.001 | |
| Age, ≥60 yr | 0.99 | 0.94–1.04 | 0.624 | 1.00 | 1.00–1.01 | 0.469 | |
| Sex, female | 0.93 | 0.86–1.01 | 0.080 | 0.95 | 0.88–1.03 | 0.205 | |
| Region, urban | 0.96 | 0.89–1.03 | 0.249 | ||||
| DM, yes | 0.92 | 0.86–0.99 | 0.022 | 0.94 | 0.87–1.01 | 0.086 | |
| HTN, yes | 0.80 | 0.75–0.85 | <0.001 | 0.87 | 0.82–0.92 | <0.001 | |
| Cardiovascular disease, yes | 0.86 | 0.81–0.91 | <0.001 | 0.93 | 0.88–0.98 | 0.010 | |
| Cerebrovascular disease, yes | 0.86 | 0.80–0.92 | <0.001 | ||||
| Fatty liver, yes | 0.90 | 0.84–0.96 | 0.001 | 0.95 | 0.89–1.01 | 0.081 | |
| Cirrhosis, yes | 0.80 | 0.76-0.84 | <0.001 | ||||
| Aspirin, yes | 0.61 | 0.53–0.70 | <0.001 | 0.64 | 0.55–0.74 | <0.001 | |
| DPP-4 inhibitor use, yes | 0.85 | 0.75–0.95 | 0.006 | ||||
| Insulin use, yes | 1.14 | 1.07–1.22 | <0.001 | 1.24 | 1.16–1.33 | <0.001 | |
| Metformin use, yes | 0.75 | 0.65–0.87 | <0.001 | 0.78 | 0.67–0.91 | 0.002 | |
| SGLT-2 inhibitor use, yes | 0.60 | 0.41–0.88 | 0.01 | 0.67 | 0.45–0.99 | 0.044 | |
| Sulfonylurea use, yes | 0.76 | 0.63–0.91 | 0.003 | 0.81 | 0.67–0.99 | 0.037 | |
| Thiazolidinedione use, yes | 0.65 | 0.47–0.89 | 0.007 | 0.79 | 0.57–1.09 | 0.150 | |
Abbreviations: CI, confidence interval; HR, hazard ratio; DM, diabetes mellitus; HTN, hypertension; DPP, dipeptidyl peptidase; OS, overall survival; PS, propensity score; SGLT, sodium-glucose cotransporter.
Table 3.
Univariate and multivariate cox regression analysis for PFS according to statin use in PS-matched cohort.
Table 3.
Univariate and multivariate cox regression analysis for PFS according to statin use in PS-matched cohort.
| Variables | Univariate analysis | Multivariate analysis | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | ||
| Statin use, yes | 0.72 | 0.67–0.76 | <0.001 | 0.78 | 0.74–0.84 | <0.001 | |
| Age, ≥60 yr | 1.04 | 0.99–1.09 | 0.156 | 1.01 | 1.00–1.01 | 0.006 | |
| Sex, female | 0.98 | 0.91–1.06 | 0.603 | 1.01 | 0.94–1.09 | 0.825 | |
| Region, urban | 0.88 | 0.82–0.94 | <0.001 | 0.87 | 0.81–0.93 | <0.001 | |
| DM, yes | 0.91 | 0.85–0.98 | 0.007 | 0.95 | 0.88–1.01 | 0.104 | |
| Fatty liver, yes | 0.94 | 0.89–1.00 | 0.054 | ||||
| Cirrhosis, yes | 0.82 | 0.79-0.86 | <0.001 | ||||
| HTN, yes | 0.80 | 0.75–0.84 | <0.001 | 0.86 | 0.81–0.91 | <0.001 | |
| Cardiovascular disease, yes | 0.84 | 0.79–0.88 | <0.001 | 0.90 | 0.86–0.96 | <0.001 | |
| Cerebrovascular disease, yes | 0.81 | 0.76–0.87 | <0.001 | 0.90 | 0.84–0.97 | 0.004 | |
| Aspirin use, yes | 0.57 | 0.50–0.65 | <0.001 | 0.63 | 0.55–0.73 | <0.001 | |
| DPP-4 inhibitor use, yes | 0.78 | 0.70–0.88 | <0.001 | 0.90 | 0.80–1.01 | 0.085 | |
| Insulin use, yes | 1.13 | 1.06–1.20 | <0.001 | 1.26 | 1.18–1.35 | <0.001 | |
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.72 | 0.62–0.84 | <0.001 | |
| SGLT-2 inhibitor use, yes | 0.70 | 0.50–0.98 | 0.038 | 0.77 | 0.54–1.07 | 0.123 | |
| Sulfonylurea use, yes | 0.73 | 0.61–0.86 | <0.001 | 0.83 | 0.69–1.00 | 0.049 | |
| Thiazolidinedione use, yes | 0.64 | 0.49–0.85 | 0.002 | 0.80 | 0.60–1.06 | 0.114 | |
Abbreviations: CI, confidence interval; HR, hazard ratio; DM, diabetes mellitus; HTN, hypertension; DPP, dipeptidyl peptidase; PFS, progression free survival; PS, propensity score; SGLT, sodium-glucose cotransporter.
Table 4.
Univariate and multivariate cox regression analysis for OS according to statin use pattern.
Table 4.
Univariate and multivariate cox regression analysis for OS according to statin use pattern.
| Variables | Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | |||
| Statin use pattern | ||||||||
| Non-user | reference | reference | ||||||
| pre-TKI use | 1.31 | 1.13–1.52 | <0.001 | 1.33 | 1.14–1.54 | <0.001 | ||
| continuous use from TKI treatment | 0.80 | 0.74–0.87 | <0.001 | 0.87 | 0.80–0.95 | 0.002 | ||
| post-TKI use | 0.40 | 0.35–0.46 | <0.001 | 0.43 | 0.38–0.50 | <0.001 | ||
| Age, ≥60 yr | 0.99 | 0.94–1.04 | 0.624 | 1.00 | 1.00–1.00 | 0.767 | ||
| Sex, female | 0.93 | 0.86–1.01 | 0.080 | 0.95 | 0.88–1.03 | 0.246 | ||
| Region, urban | 0.96 | 0.89–1.03 | 0.249 | |||||
| DM, yes | 0.92 | 0.86–0.99 | 0.022 | 0.93 | 0.87–1.00 | 0.048 | ||
| Fatty liver, yes | 0.90 | 0.84–0.96 | <0.001 | 0.94 | 0.88–1.00 | 0.050 | ||
| Cirrhosis, yes | 0.80 | 0.76-0.84 | <0.001 | |||||
| HTN, yes | 0.80 | 0.75–0.85 | <0.001 | 0.87 | 0.82–0.92 | <0.001 | ||
| Cardiovascular disease, yes | 0.86 | 0.81–0.91 | <0.001 | 0.93 | 0.88–0.99 | 0.016 | ||
| Cerebrovascular disease, yes | 0.86 | 0.80–0.92 | <0.001 | |||||
| Aspirin use, yes | 0.61 | 0.53–0.70 | <0.001 | 0.69 | 0.59–0.79 | <0.001 | ||
| DPP-4 inhibitor use, yes | 0.85 | 0.75–0.95 | 0.006 | 0.90 | 0.80–1.03 | 0.119 | ||
| Insulin use, yes | 1.14 | 1.07–1.22 | <0.001 | 1.23 | 1.15–1.32 | <0.001 | ||
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.83 | 0.71–0.97 | 0.022 | ||
| SGLT-2 inhibitor use, yes | 0.60 | 0.41–0.88 | 0.010 | 0.66 | 0.45–0.98 | 0.038 | ||
| Sulfonylurea use, yes | 0.76 | 0.63–0.91 | 0.003 | 0.79 | 0.65–0.96 | 0.020 | ||
| Thiazolidinedione use, yes | 0.65 | 0.47–0.89 | 0.007 | |||||
Abbreviations: CI, confidence interval; HR = hazard ratio; DM, diabetes mellitus; HTN, hypertension; DPP, dipeptidyl peptidase; OS, overall survival; SGLT, sodium-glucose cotransporter; TKI, tyrosine kinase inhibitor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



