
Submitted:
13 December 2023
Posted:
13 December 2023
You are already at the latest version
Abstract
Background: We aimed to evaluate whether baseline GLS and NT-proBNP and their changes after cardiac resynchronization therapy (CRT) can predict the long-term clinical outcomes and the echocardiographic-based response to CRT (defined by 15% relative reduction in left ventricular end-systolic volume). Methods: We enrolled 143 patients with stable, ischemic heart failure (HF) undergoing CRT-D implantation. NT-proBNP and echocardiogram were obtained before and 6 months after. The patients were followed-up (median: 58 months) for HF-related deaths and/or HF hospitalizations (primary endpoint) or HF-related deaths (secondary endpoint) Results: 84 patients achieved the primary and 53 the secondary endpoint, while 104 patients were considered as CRT-responders and 39 as non-responders. At baseline, event-free patients had higher absolute GLS values (p<0.001) and lower NT-proBNP serum levels (p<0001) than those achieving primary endpoint. A similar pattern was observed in favor of CRT-responders vs non-responders. In Cox regression analysis, lower baseline absolute GLS value (HR=0.77;95%CI, 0.51-1.91; p=0.002), higher baseline NT-proBNP levels (HR=1.55;95%CI, 1.43-2.01;p=0.002) and diabetes (HR=1.27;95%CI, 1.12-1.98;p=0.003) were associated with lower incidence of primary endpoint. Conclusions: In HF patients undergoing CRT-D, baseline GLS and NT-proBNP concentrations may serve as prognostic factors, while they may predict the echocardiographic-based response to CRT.
Keywords:
cardiac resynchronization therapy-CRT
; global longitudinal strain-GLS
; natriuretic peptides
; heart failure
1. Introduction
Patients with symptomatic (NYHA II-IV) heart failure (HF), reduced left ventricular ejection fraction (LVEF), and wide QRS complex are good candidates for cardiac resynchronization therapy (CRT), since it is associated with significant improvements in symptoms and morbidity and mortality (Level of evidence IA or IIaB) [1,2]. Unfortunately, a significant proportion of CRT recipients (~30%) do not experience the expected clinical benefits despite the fulfilment of classical selection criteria [3]. That proportion is almost similar between registries, despite the application of several approaches. The characteristics of those patients, so-called “non-responders”, have been put under investigation in order to maximize the efficacy of this costly therapy. The site of LV electrode implantation and the post-intervention management may determine the response to CRT in a predictable way, but the most challenging parameter remains patients’ selection [4]. Although the response to CRT is clinically judged, which requires a long-term clinical follow-up, there is a growing body of evidence investigating the echocardiographic-based response, as a surrogate marker of clinical response [5]. Over and above other indices, a significant reduction (by ≥15%) in LV end-systolic volume (LVESV) has been proposed as an echocardiographic-derived index of effective response to CRT-D implantation [6]. Patients achieving the aforementioned ESV decline are considered as “CRT-responders”. That change requires 6 months to become recognizable and according to most, but not all, previous studies has shown a significant association with clinical outcomes in CRT-D receivers, supporting its application as a surrogate prognostic factor [7,8]. This is an attempt to shorten the follow-up time and facilitate the early recognition of HF patients who will not take advantage from CRT (non-responders) who should search for optimum medical therapy.
Regarding this gap, several investigators have proposed supplementary echocardiographic indices to predict clinical response to CRT [9]. Global longitudinal strain (GLS), an index quantifying active global myocardial deformation, has commonly been reported as a valid predictor of CRT response [10]. In particular, a high absolute baseline GLS and the amount of its change post-intervention have been related to favorable clinical outcomes of CRT in HF patients. Most, but not all, studies have supported the prognostic power of GLS in CRT recipients [11]. However, there is still insufficient evidence to support its use as a single prognostic factor.
Biomarkers have also been proposed as predictors of clinical outcomes in patients with HF [12]. Growing body of evidence supports its usage for tailoring CRT implantation and candidate’s selection [13]. Among those biomarkers, N-terminal pro hormone of B-type natriuretic peptide (NT-proBNP) have emerged as the most promising prognostic factors, but the available data about their application in CRT guiding are limited and controversial [14,15].
The aim of the present study was to investigate whether the baseline values of GLS and NT-proBNP and/or their changes after implantation in patients with HF fulfilling the criteria for CRT can predict: 1) the long-term morbidity and mortality, 2) the response to CRT-D based on echocardiographic criteria. For comparison reasons, we examined our cohort using either clinical criteria [(event-free patients versus patients with at least one event (hospitalization and/or death)], or echocardiographic criteria (CRT responders versus CRT non-responders).
2. Materials and Methods
2.1. Study design
This is a prospective, observational study conducted in two hospitals from 2016 to 2019. We initially recruited 147 patients with ischemic HF [NYHA class II/III, ejection fraction ≤35%] referred for CRT-D, according to the international criteria and despite the already optimum HF therapy [16]. The ischemic aetiology was defined by the history of myocardial infarction and/or coronary revascularization procedure (percutaneous coronary angioplasty, coronary artery bypass grafting). At baseline and before CRT-D implantation, all patients underwent initial evaluation including: medical history, NYHA class assessment, blood pressure, blood sampling for NT-proBNP assay and echocardiographic examination. That evaluation was repeated 6 months after implantation by the same cardiologists. After the second assessment, we continued follow-up of all alive participants by retrieving records from the National Healthcare operation systems of our countries or hospital records or, when they were not available, by telephone interview of patients or their siblings. In case of patients’ deaths, we searched for medical records to clarify the reason of death and endpoints achievement.
Based on echocardiographic criteria, patients presenting ≥15% reduction in their LVESV from baseline to 6 months were considered as “CRT-responders”, the rest as “CRT-non-responders”. During the whole study period we evaluated the achievement of primary endpoints: HF-related deaths and/or hospitalizations and secondary endpoint: 1) HF-related deaths or 2) all-cause mortality. We searched for other endpoints, like myocardial infarction or cardiovascular morbidity, but we realized that the low number of recorded events prevented us from any further analysis or were overlapped by other events. Among all potential prognostic factors, we evaluated baseline GLS and NT-proBNP and their changes after implantation in patients with HF undergoing CRT-D.
Informed consent was obtained from all subjects involved in the study.
2.2. Echocardiography
Using a standard imaging system (iE33 ultrasound scanner equipped with a S5-1 transducer (Philips Healthcare, Andover, MA, USA) two independent operators performed the echocardiographic studies at baseline and 6 months after implantation. The offline imaging analysis was performed on a single PC workstation by two cardiologists, blinded to patients’ data. Standard echocardiographic measurements included LVEF, LV end-diastolic volume (LVEDV) and LVESV.
Speckle tracking echocardiography has been developed for the assessment of myocardial deformation. The motion of speckles in a certain region of interest is traced frame by frame throughout the cardiac cycle. In a normal individual, the strain curves reach its peak strain at peak systole, in a coordinated manner. GLS has been recommended as an index of speckle tracking echocardiography with high accuracy for the quantification of LV systolic dysfunction [17]. We acquired all images at the maximum possible frame rates using the same vendor for image analysis. GLS was derived from speckle tracking, and analyzed by post-processing of all 3 apical images of the LV (4-chamber, 2-chamber, 3-chamber). In all the three apical images, the echocardiography software divided each wall in 3 segments in which peak systolic longitudinal strain values were calculated. Then, the mean peak longitudinal strain of each imaging plane and the mean of the peak global longitudinal strain values from all segments were obtained. A GLS value < -18% usually falls within the normal range, while an increasing GLS from > -16% parallels the degree of LV systolic dysfunction.
2.3. Statistical analysis
Data are expressed as mean and ± SD. Normality of distribution was assessed by Kolmogorov-Smirnov test. Based on primary endpoint, we divided patients into event-free and those experiencing an event. Based on echocardiographic criterion of CRT response we compared CTR-responders with non-responders. Paired-samples t-test and student’s t-test were used for comparison of continuous parameters within and between groups, respectively. Differences between groups were assessed using Mann Whitney U test for variables with non-normal distribution, and the χ2 test for categorical variables as appropriate. Paired samples t-test was used to compare changes of echocardiographic parameters from baseline to follow-up. Cox regression analysis was used for prediction of the primary and secondary clinical endpoints. Hazard ratios (HR) and 95% confidence intervals (CIs) were calculated for each factor via the Cox proportional hazards analysis. All baseline variables with p<0.05, in univariate analyses were integrated into the Cox multivariate model to determine the independent predictors of primary and secondary endpoints. Logistic regression analysis was used to assess the association of baseline variables with echocardiographic-based CRT response at 6 months after implantation. Survival analysis using the Kaplan-Meier method with log-rank test was used to analyze the cumulative survival starting from baseline. Receiver operating characteristic (ROC) curves were used to assess the diagnostic accuracy for discriminating the achievement of clinical endpoints or not. Area under the curve (AUC), sensitivity and specificity were calculated. Two-tailed p value <0.05 was defined as statistically significant. We used for analyses the statistical software SPSS-25.0 (SPSS Inc, Chicago, IL, USA).
3. Results
3.1. Groups at baseline
One hundred forty-seven patients initially entered analysis. We further excluded two patients, who were lost during follow-up for personal reasons and another 2 patients, who died just after CRT-D implantation and before discharge due to infection and acute heart failure, respectively.
We got full data from 143 patients. During a median follow-up of 58 months, 84 patients achieved the primary endpoint (death and/or hospitalization due to HF). The group achieving the primary endpoint was a substantial expansion of that of the secondary one. Notably, almost all patients before HF-related death had at least one hospitalization for HF decompensation. In the whole cohort at baseline, 56 patients died from any cause. Among them, 53 deaths were attributed to HF (secondary endpoint), while 3 patients died due to other reasons: myocardial infarction, newly diagnosed lung cancer and car accident. The all-cause mortality was predominantly driven by HF-related mortality which remained the secondary endpoint
3.2. Prognostic value of GLS and NT-proBNP at baseline
Based on clinical endpoints we assessed the prognostic value of GLS and NT-proBNP. Regarding that hospitalization for HF preceded almost all HF-related deaths, we paid attention to the group achieving the primary endpoint. That group appeared with higher NT-proBNP, and lower absolute GLS values at baseline compared to event-free group (Table 1). Notably, those groups did not differ in other significant parameters, like demographic characteristics, QRS duration, pharmaceutical therapy etc. In Cox regression analysis, lower GLS absolute value, higher NT-proBNP and the presence of diabetes mellitus at baseline were associated with higher incidence of death and/or hospitalization due to HF in multivariate analysis (Table 2). In ROC curve analysis a cut-off value of GLS < -7.92% predicted primary endpoint with modest sensitivity (69.0%) and specificity (70.4%) (AUC R2=0.75, p<0.001) (Figure 1).
Regarding the secondary endpoint, with smaller group achieving it, baseline NT-proBNP, along with atrial fibrillation and kidney dysfunction emerged as independent predictors of secondary endpoint (Table 3).
3.3. Prediction of CRT response by GLS and NT-proBNP
As expected, CRT-responders had better survival and experienced less hospitalizations (p<0.001) compared to non-responders (Table 4 & Figure 2). At baseline, CRT-responders appeared with higher absolute GLS values (p<0.001), larger left atrium volumes (p=0.029) and lower NT-proBNP serum levels (p<0001) than non-responders. There was a marginal, non-significant difference between groups in QRS duration (p=0.061) with responders having a non-significantly broader QRS-complex. There were no significant differences in the rest of clinical, pharmaceutical or echocardiographic parameters (p>0.05) (Table 4). Although CRT-responders had higher baseline absolute GLS values and lower NT-proBNP levels, we failed to find any independent association of neither absolute GLS (OR=1.11; 95%CI, 1.01-1.32; p=0.660) nor NT-proBNP (OR=1.35; 95% CI, 1.19-1.75; p=0.088,) at baseline with CRT response at 6 months in logistic regression analysis.
3.4. Changes of GLS and NT-proBNP with CRT and their prognostic value
Regarding the prognostic value of the CRT-induced changes of GLS and NT-proBNP in the 6-month post-intervention period, we further evaluated them in relation to HF-related hospitalization. Event-free group had a larger increase in absolute GLS (ΔGLS: 4.1±0.8% vs 0.55±0.3%, p<0.001) and remarkable decrease in NT-proBNP levels (ΔNT-proBNP: -588±281pg/ml vs -101±78pg/ml, p=0.003) than those who had at least one hospitalization.
Using echocardiographic-based response, at 6-months’ time CRT-responders showed significant improvement in QRS duration, NYHA class and NT-proBNP levels compared to non-responders. Notably, the usage of diuretics was also reduced in the former group, implicating functional improvement. Similarly, CRT-responders had significantly larger increase in absolute GLS (ΔGLS: 3.5±0.6% vs 0.23.5±0.5%, p<0.001) and remarkable decrease in NT-proBNP levels (ΔNT-proBNP: -651±98pg/ml vs -43±8pg/ml, p<0.001) than non-responders.
Based on a previous publication [18], we performed a subgroup analysis, looking at patients with > 25% reduction in NT-proBNP concentration and concomitant >30% improvement in GLS. All patients fulfilling those criteria belonged to responders’ group (n=45). Notably, compared to remaining responders (n=59); mortality rate was comparable; however, fewer patients achieved the primary endpoint during follow-up (7 versus 24, p<0.001).
4. Discussion
In the present prospective, observational study, pre-intervention baseline low values of both absolute GLS and NT-proBNP at baseline independently predicted the primary clinical endpoint, while low circulating NT-proBNP levels independently predicted secondary clinical endpoint, in the long-term follow-up (almost 6 years). In addition to this, higher absolute GLS and lower NT-proBNP levels predicted the echocardiographic-based CRT-response. Both event-free patients and CRT-D responders had significantly ameliorated GLS and NT-proBNP levels within 6 months of CRT-D implantation, but that effect did not determine prognosis.
The identification of patients who may not benefit from CRT implantation (non-responders) using feasible and easily assessed parameters is of crucial importance. Several factors have been recommended, but no single factor has been remarkably powered to identify potential non-responders and guide the exclusion of them prior to CRT. Among them, shorter QRS duration (<130ms), an ischemic origin of HF, male gender and non-LBBB pattern have been proposed as negative predictors of CRT clinical response [19]. Regarding that LV dyssynchrony is the target of CRT, several conventional echocardiographic indices with potential prognostic value have been proposed, but the long-term results are very modest and not yet clinically applicable [20]. The assessment of LV deformation, using GLS, seems to be a good tool to adequately predict and monitor the response to CRT device implantation [21]. The echocardiographic response to CRT has been associated with clinical improvement and reduced morbidity and mortality [22]. Most, but not all, researchers have demonstrated a strong association of significant decrease in ESV after CRT implantation with beneficial outcomes in the long-term proposing it as a surrogate marker of CRT clinical response. An advantage of using surrogate markers is an early and highly accurate estimation of a therapy’s efficacy, before the occurrence of all cardiovascular events. From the methodological point of view, this study evaluated the relationship of baseline GLS and NT-proBNP with CRT response using both criteria: clinical outcomes during follow-up and the echocardiographic-based index. Our findings are consistent with previous studies reporting higher absolute value of GLS in responders than non-responders defined by both criteria [23]. A recent meta-analysis using either clinical or echocardiographic characteristics of CRT response confirmed better resting GLS values in CRT responders than non-responders (Bazoukis et al 2022). That meta-analysis used a mixed definition of CRT response, which may be confounding. Presumably, a higher absolute GLS at baseline expresses less burden of non-viable, scarred myocardium, with potential higher response rate.
Despite the documented relationship between GLS and beneficial changes in ESV after CRT, there is still not consistent, direct relationship of GLS with clinical outcomes. Almost all previous studies have documented a link between baseline GLS and echocardiographic-based CRT response, however a surprisingly small number of them, all from the same research centre, have confirmed a direct relationship of baseline GLS with clinical outcomes [6,24,25]. The conventional, echocardiographic-defined CRT response, consists of a surrogate marker, but it may not entirely reflect the clinical course of CRT receivers. In our study, the event-free patients had higher absolute GLS levels at baseline, implicating an indirect relationship between variables. Most importantly, we demonstrated a direct, independent relationship of GLS with the combined clinical endpoint (death and HF hospitalization) in Cox regression analysis. Our study supports the application of GLS for the detection of patients who may get benefit from CRT device implantation affecting the decision-making process. The clinical relevance should be further investigated because in multivariate models the characteristics of studied cohorts, the homogeneity and the power of the study may determine the independent relationship of any variable within groups. On the other hand, the relationship of GLS with clinical endpoints in HF patients not requiring CRT has been long demonstrated [26]. Despite accumulated data, there is not yet a widely accepted cut-off value for either resting GLS or GLS change to predict clinical response. Based on ROC analysis, we drew a cut-off value of GLS < -7.92% for the prediction of combined clinical endpoint in CRT receivers, but with modest sensitivity and specificity. A single previous study has also proposed almost equivalent discriminatory value of GLS for clinical outcomes, but it has not been validated yet [27].
Despite the remarkable difference in GLS between CRT-responders and non-responders, we failed to find an independent association of baseline GLS with the change of ESV values at 6 months. Contrary to previous study we did not confirm the prognostic value of echocardiographic-based CRT response and hence its relationship with GLS [28]. Perhaps GLS may not be able to serve as a predictor of another echocardiographic index (ESV change) in the selected time-frame of 6 months and in our cohort with specific characteristics. This raises questions about the clinical applicability of echocardiographic-based CRT response. In parallel, we demonstrated that CRT responders appeared with improved GLS at a larger extent than non-responders, which agrees to previous meta-analysis. This is an expected result, but the percentage of GLS change which could predict clinical improvement and survival has not yet been determined. Therefore, more studies are required to investigate the clinical impact of GLS in decision-making in patients undergoing CRT.
To our knowledge, this is the second study demonstrating the inverse relationship of NT-proBNP, at baseline, with favourable clinical outcomes in the long-term and CRT response. The CARE-HF trial with their extensions of follow-up was the first and largest trial supporting the prognostic value of NT-proBNP in CRT receivers [29,30]. Growing body of evidence implicates the prognostic power of NT-proBNP, which may significantly influence in the future therapeutic decisions in HF [31]. Therefore, NT-proBNP may become a significant biomarker predicting the efficacy of CRT and identifying candidates, which will gain benefits from this interventional therapy [32]. Despite those promising results, there are some important limitations for widespread application of biomarkers [33]. First of all, this is a multifaceted biomarker, which may be affected by concomitant pharmaceutical therapy and co-morbidities attenuating its prognostic value. Second, there is not yet a cut-off value to predict event-free clinical course or CRT response. Inversely, CRT favourably reduced NT-proBNP circulating levels in responders, however, its changes alone did not have any prognostic value for CRT receivers. Nevertheless, NT-proBNP remains a cheap, well-established, easily measured biomarker with potential application for the detection of appropriate CRT candidates.
In agreement to previous reports, our CRT responders appeared with higher improvement of GLS compared to non-responders. Notably, patients with >30% increase of GLS concomitant with >25% reduction in NT-proBNP were all assigned to responders’ group. Those patients had the best clinical course compared not only to non-responders, but also to responders with less amount of improvement in both GLS and NT-proBNP. Perhaps, a combined approach of echocardiographic assessment of deformation and natriuretic peptides may further enhance the early discrimination of super-responders. Our study was not powered to quantify the clinical impact of such combination.
Among the most important limitations of the present study were its relatively small sample and the short-term, 6-months, monitoring of echocardiographic performance and NT-proBNP levels. We could not control parameters for the whole follow-up period, focusing solely on clinical endpoints. On the other hand, we recruited a more homogeneous cohort by involving patients with ischemic HF, receiving only CRT-D. The threshold defining response to CRT is a matter of debate. It is predominantly based on echocardiographic than clinical assessment and its calculation is vendor-dependent, so it may vary across different vendor platforms.
In conclusion, lower absolute value of GLS and higher NT-proBNP levels predicted the primary endpoint of death and HF hospitalization in HF patients undergoing CRT-D and the echocardiographic-assessed non-response. Moreover, low baseline NT-proBNP was independently associated with survival in the long-term. Finally, a significant amelioration of concomitant GLS and NT-proBNP after CRT-D implantation did not add prognostic value in our cohort.
Author Contributions
Conceptualization, Formal analysis, Methodology, Project administration, Visualization, writing original draft, writing -review and editing N.K. Investigation, A.L. Investigation, Writing—review and editing M.K., I.H., A.B., F.B., T.S. Writing—review and editing, I.K. Conceptualization, Formal analysis, Methodology, Project administration, writing -review and editing P.H. All authors have read and agreed to the published version of the manuscript and the completed authorship form has been submitted.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Catharina Hospital, Eindhoven, The Netherlands (protocol code Niet-WMO 2015-34 and date of approval 29/5/2015) and the National Bioethical Committee of Cyprus (protocol code NBECC 2021/34 and date of approval 11/6/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I, Tolosana JM; ESC Scientific Document Group. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021 Sep 14;42(35):3427-3520.
- Wang Z, Wu Y, Zhang J. Cardiac resynchronization therapy in heart failure patients: tough road but clear future. Heart Fail Rev. 2021 May;26(3):735-745.
- Bazoukis G, Thomopoulos C, Tse G, Tsioufis K, Nihoyannopoulos P. Global longitudinal strain predicts responders after cardiac resynchronization therapy-a systematic review and meta-analysis. Heart Fail Rev. 2021 Mar 30. [CrossRef]
- Zhu H, Zou T, Zhong Y, Yang C, Ren Y, Wang F. Prevention of non-response to cardiac resynchronization therapy: points to remember. Heart Fail Rev. 2020 Mar;25(2):269-275. [CrossRef]
- Martins R, António N, Donato H, Oliveiros B. Predictors of echocardiographic response to cardiac resynchronization therapy: A systematic review with Meta-Analysis. Int J Cardiol Heart Vasc. 2022 Feb 28;39:100979. [CrossRef]
- Mele D, Luisi GA, Malagù M, Laterza A, Ferrari R, Bertini M. Echocardiographic evaluation of cardiac dyssynchrony: Does it still matter? Echocardiography. 2018 May;35(5):707-715.
- Hu X, Xu H, Hassea SRA, Qian Z, Wang Y, Zhang X, Hou X, Zou J. Comparative efficacy of image-guided techniques in cardiac resynchronization therapy: a meta-analysis. BMC Cardiovasc Disord. 2021 May 24;21(1):255. [CrossRef]
- Bazoukis G, Naka KK, Alsheikh-Ali A, Tse G, Letsas KP, Korantzopoulos P, Liu T, Yeung C, Efremidis M, Tsioufis K, Baranchuk A, Stavrakis S. Association of QRS narrowing with response to cardiac resynchronization therapy-a systematic review and meta-analysis of observational studies. Heart Fail Rev. 2020 Sep;25(5):745-756. [CrossRef]
- Dal Ferro M, De Paris V, Collia D, Stolfo D, Caiffa T, Barbati G, Korcova R, Pinamonti B, Zovatto L, Zecchin M, Sinagra G, Pedrizzetti G. Left Ventricular Response to Cardiac Resynchronization Therapy: Insights From Hemodynamic Forces Computed by Speckle Tracking. Front Cardiovasc Med. 2019 May 14;6:59. [CrossRef]
- van der Bijl P, Kostyukevich MV, Khidir M, Ajmone Marsan N, Delgado V, Bax JJ. Left ventricular remodelling and change in left ventricular global longitudinal strain after cardiac resynchronization therapy: prognostic implications. Eur Heart J Cardiovasc Imaging. 2019 Oct 1;20(10):1112-1119. [CrossRef]
- Menet A, Guyomar Y, Ennezat PV, Graux P, Castel AL, Delelis F, Heuls S, Cuvelier E, Gevaert C, Le Goffic C, Tribouilloy C, Maréchaux S. Prognostic value of left ventricular reverse remodeling and performance improvement after cardiac resynchronization therapy: A prospective study. Int J Cardiol. 2016 Feb 1;204:6-11. [CrossRef]
- Vazquez-Montes MDLA, Debray TPA, Taylor KS, Speich B, Jones N, Collins GS, Hobbs FDRR, Magriplis E, Maruri-Aguilar H, Moons KGM, Parissis J, Perera R, Roberts N, Taylor CJ, Kadoglou NPE, Trivella M; proBHF group. UMBRELLA protocol: systematic reviews of multivariable biomarker prognostic models developed to predict clinical outcomes in patients with heart failure. Diagn Progn Res. 2020 Aug 26;4:13. [CrossRef]
- Asgardoon MH, Vasheghani-Farahani A, Sherafati A. Usefulness of Biomarkers for Predicting Response to Cardiac Resynchronization Therapy. Curr Cardiol Rev. 2020;16(2):132-140. [CrossRef]
- Debska-Kozlowska A, Ksiazczyk M, Warchol I, Lubinski A. Clinical Usefulness of N-terminal Prohormone of Brain Natriuretic Peptide and High Sensitivity Troponin T in Patients with Heart Failure Undergoing Cardiac Resynchronization Therapy. Curr Pharm Des. 2019;25(14):1671-1678. [CrossRef]
- McAloon CJ, Barwari T, Hu J, Hamborg T, Nevill A, Hyndman S, Ansell V, Musa A, Jones J, Goodby J, Banerjee P, O'Hare P, Mayr M, Randeva H, Osman F. Characterisation of circulating biomarkers before and after cardiac resynchronisation therapy and their role in predicting CRT response: the COVERT-HF study. Open Heart. 2018 Oct 18;5(2):e000899. [CrossRef]
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Authors/Task Force Members; Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016 Aug;18(8):891-975.
- Kato T, Harada T, Kagami K, Obokata M. The roles of global longitudinal strain imaging in contemporary clinical cardiology. J Med Ultrason (2001). 2022 Apr;49(2):175-185.
- Bakos Z, Chatterjee NC, Reitan C, Singh JP, Borgquist R. Prediction of clinical outcome in patients treated with cardiac resynchronization therapy - the role of NT-ProBNP and a combined response score. BMC Cardiovasc Disord. 2018 Apr 24;18(1):70.
- European Society of Cardiology (ESC); European Heart Rhythm Association (EHRA), Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J, Deharo JC, Delgado V, Elliott PM, Gorenek B, Israel CW, Leclercq C, Linde C, Mont L, Padeletti L, Sutton R, Vardas PE. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace. 2013 Aug;15(8):1070-118.
- Mele D, Trevisan F, Fiorencis A, Smarrazzo V, Bertini M, Ferrari R. Current Role of Echocardiography in Cardiac Resynchronization Therapy: from Cardiac Mechanics to Flow Dynamics Analysis. Curr Heart Fail Rep. 2020 Dec;17(6):384-396. [CrossRef]
- Stătescu C, Ureche C, Enachi Ș, Radu R, Sascău RA. Cardiac Resynchronization Therapy in Non-Ischemic Cardiomyopathy: Role of Multimodality Imaging. Diagnostics (Basel). 2021 Mar 30;11(4):625. [CrossRef]
- Rijks J, Ghossein MA, Wouters PC, Dural M, Maass AH, Meine M, Kloosterman M, Luermans J, Prinzen FW, Vernooy K, van Stipdonk AMW. Comparison of the relation of the ESC 2021 and ESC 2013 definitions of left bundle branch block with clinical and echocardiographic outcome in cardiac resynchronization therapy. J Cardiovasc Electrophysiol. 2023 Apr;34(4):1006-1014. [CrossRef]
- Zhu M, Chen H, Fulati Z, Liu Y, Su Y, Shu X. Left ventricular global longitudinal strain and mechanical dispersion predict response to multipoint pacing for cardiac resynchronization therapy. J Clin Ultrasound. 2019 Jul;47(6):356-365. [CrossRef]
- Khidir MJH, Abou R, Yilmaz D, Ajmone Marsan N, Delgado V, Bax JJ. Prognostic value of global longitudinal strain in heart failure patients treated with cardiac resynchronization therapy. Heart Rhythm. 2018 Oct;15(10):1533-1539. [CrossRef]
- Delgado-Montero A, Tayal B, Goda A, Ryo K, Marek JJ, Sugahara M, Qi Z, Althouse AD, Saba S, Schwartzman D, Gorcsan J 3rd. Additive Prognostic Value of Echocardiographic Global Longitudinal and Global Circumferential Strain to Electrocardiographic Criteria in Patients With Heart Failure Undergoing Cardiac Resynchronization Therapy. Circ Cardiovasc Imaging. 2016 Jun;9(6):e004241.
- Haugaa KH, Edvardsen T. Global longitudinal strain: the best biomarker for predicting prognosis in heart failure? Eur J Heart Fail. 2016 Nov;18(11):1340-1341.
- Bax JJ, Delgado V, Sogaard P, Singh JP, Abraham WT, Borer JS, Dickstein K, Gras D, Brugada J, Robertson M, Ford I, Krum H, Holzmeister J, Ruschitzka F, Gorcsan J. Prognostic implications of left ventricular global longitudinal strain in heart failure patients with narrow QRS complex treated with cardiac resynchronization therapy: a subanalysis of the randomized EchoCRT trial. Eur Heart J. 2017 Mar 7;38(10):720-726. [CrossRef]
- van der Bijl P, Kostyukevich MV, Khidir M, Ajmone Marsan N, Delgado V, Bax JJ. Left ventricular remodelling and change in left ventricular global longitudinal strain after cardiac resynchronization therapy: prognostic implications. Eur Heart J Cardiovasc Imaging. 2019 Oct 1;20(10):1112-1119. [CrossRef]
- Richardson M, Freemantle N, Calvert MJ, Cleland JG, Tavazzi L; CARE-HF Study Steering Committee and Investigators. Predictors and treatment response with cardiac resynchronization therapy in patients with heart failure characterized by dyssynchrony: a pre-defined analysis from the CARE-HF trial. Eur Heart J. 2007 Aug;28(15):1827-34. [CrossRef]
- Cleland J, Freemantle N, Ghio S, Fruhwald F, Shankar A, Marijanowski M, Verboven Y, Tavazzi L. Predicting the long-term effects of cardiac resynchronization therapy on mortality from baseline variables and the early response a report from the CARE-HF (Cardiac Resynchronization in Heart Failure) Trial. J Am Coll Cardiol. 2008 Aug 5;52(6):438-45. [CrossRef]
- Kadoglou NPE, Parissis J, Karavidas A, Kanonidis I, Trivella M. Assessment of acute heart failure prognosis: the promising role of prognostic models and biomarkers. Heart Fail Rev. 2022 Mar;27(2):655-663. [CrossRef]
- Pitzalis MV, Iacoviello M, Di Serio F, Romito R, Guida P, De Tommasi E, Luzzi G, Anaclerio M, Varraso L, Forleo C, Pansini N. Prognostic value of brain natriuretic peptide in the management of patients receiving cardiac resynchronization therapy. Eur J Heart Fail. 2006 Aug;8(5):509-14. [CrossRef]
- Vazquez-Montes MDLA, Debray TPA, Taylor KS, Speich B, Jones N, Collins GS, Hobbs FDRR, Magriplis E, Maruri-Aguilar H, Moons KGM, Parissis J, Perera R, Roberts N, Taylor CJ, Kadoglou NPE, Trivella M; proBHF group. UMBRELLA protocol: systematic reviews of multivariable biomarker prognostic models developed to predict clinical outcomes in patients with heart failure. Diagn Progn Res. 2020 Aug 26;4:13. [CrossRef]
Figure 1.
The ROC curve showing cut-off of GLS < -7.92% for primary endpoint.
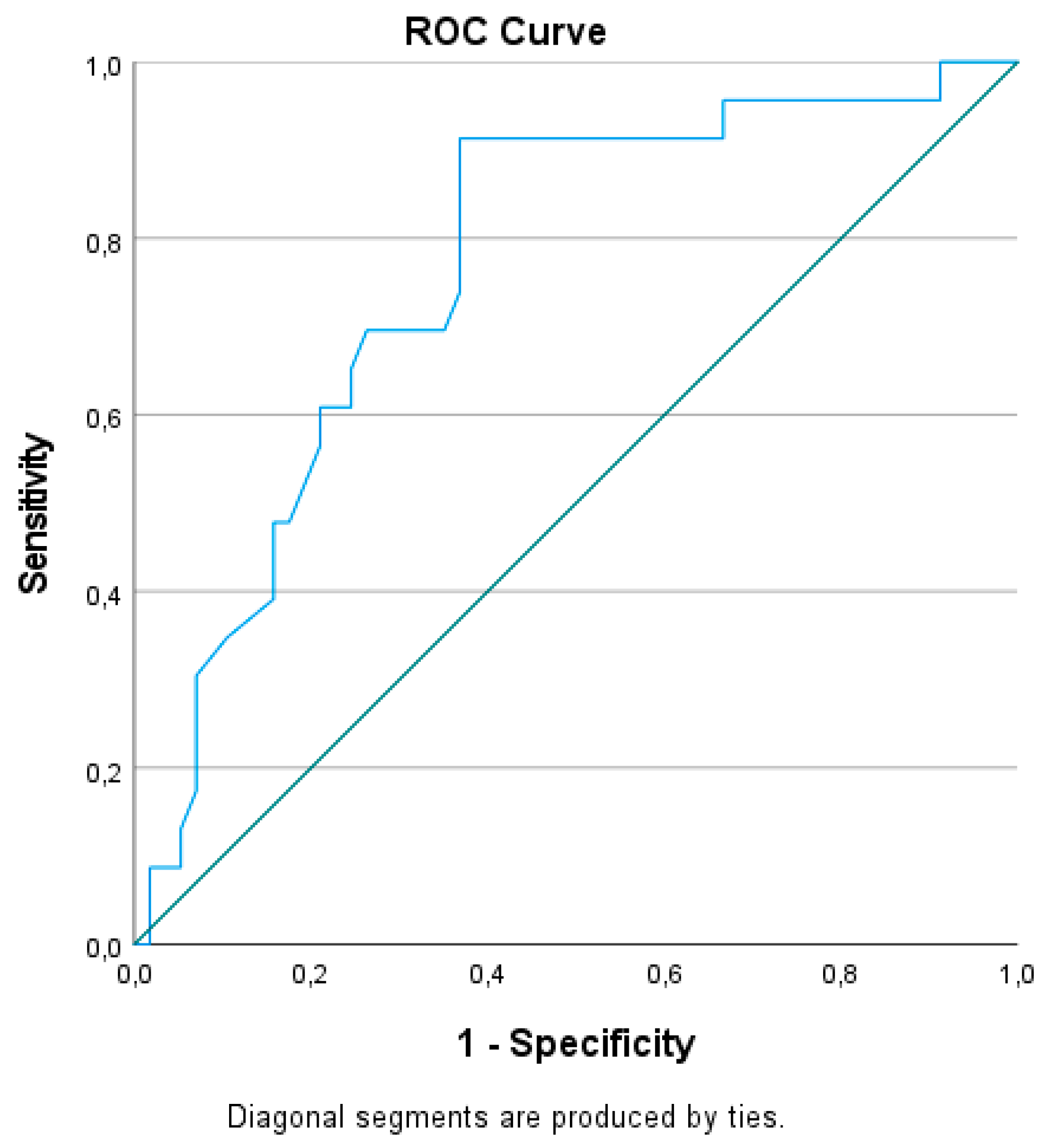
Figure 2.
Kaplan Meier survival curve between responders and non-responders from 6 months to the end of follow-up.
Figure 2.
Kaplan Meier survival curve between responders and non-responders from 6 months to the end of follow-up.
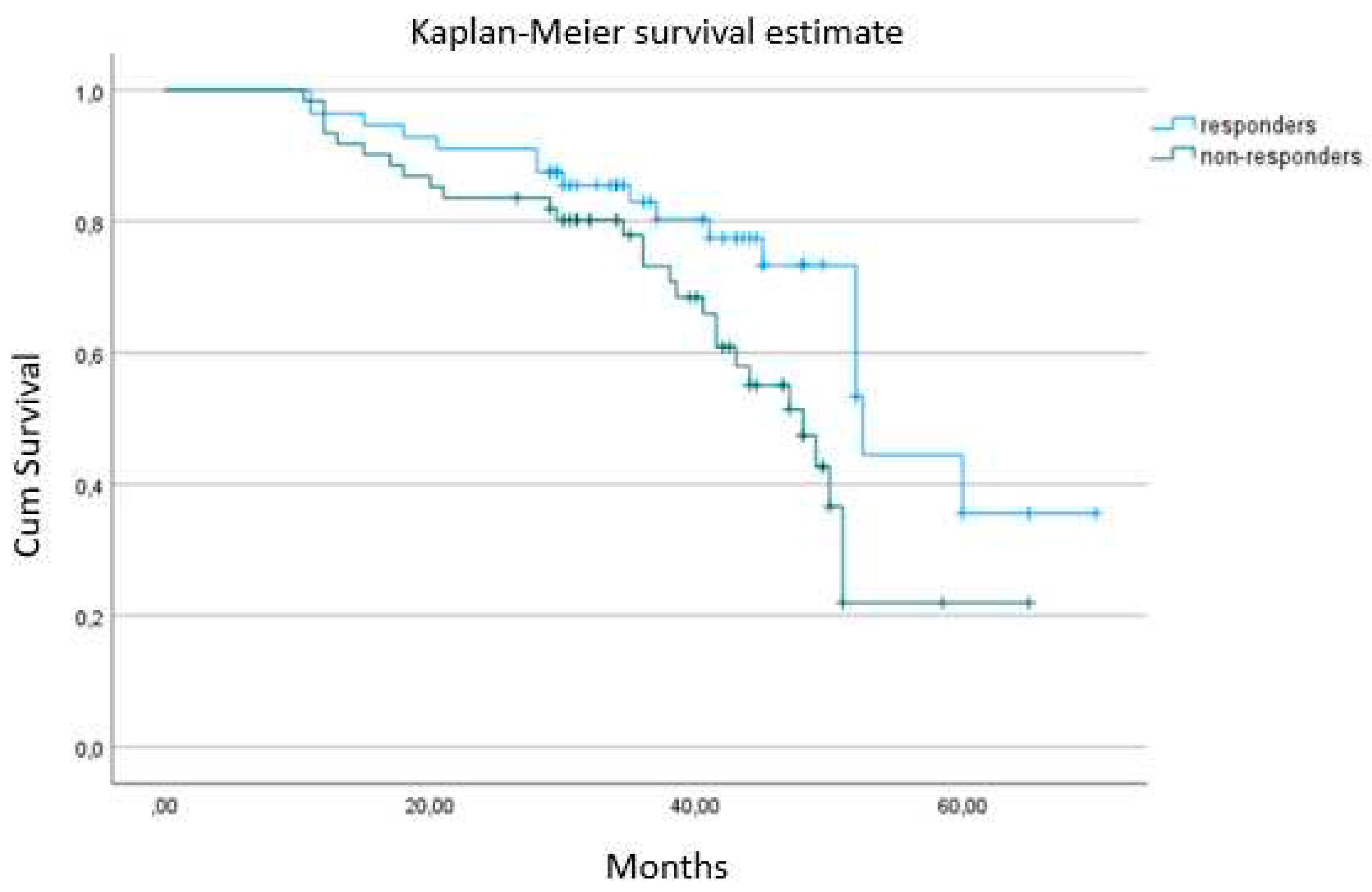

Table 1.
Baseline characteristics of event-free patients compared to those achieved primary clinical endpoint during follow-up.
Table 1.
Baseline characteristics of event-free patients compared to those achieved primary clinical endpoint during follow-up.
| No events (N=58) |
Secondary endpoint (N=84) |
p | |
|---|---|---|---|
| Age, y | 71±10 | 73±9 | 0.578 |
| Males, n | 43 (73%) | 60 (71%) | 0.789 |
| LVEF (%) | 29 ± 9 | 26 ± 10 | 0.777 |
| LVESV (ml) | 142 ± 61 | 156 ± 54 | 0.403 |
| LAVI (ml/m2) | 34 ± 8 | 38 ± 8 | 0.122 |
| GLS (%) | -8.8±2 | -6.1±2.2* | <0.001 |
| QRS duration (ms) | 157 ± 25 | 155 ± 21 | 0.061 |
| NYHA II | 18 (31%) | 21 (25%) | 0.411 |
| NYHA III | 40 (69%) | 63 (75%) | 0.173 |
| Diabetes, n | 12 (20.7%) | 23 (27.4%) | 0.125 |
| Atrial Fibrillation | 9 (15.5%) | 19 (22.6%) | 0.101 |
| CKD (stage IV-V),n | 2 (3.4%) | 4 (4.8%) | 0.535 |
| NT-proBNP (pg/ml) | 1449±288 | 2210±420 | <0.001 |
| Diuretics, n | 56 | 82 | 0923 |
| ACEIs/ARBs, n | 50 | 64 | 0.875 |
| MRA, n | 44 | 62 | 0.813 |
| B-blockers, n | 53 | 78 | 0.819 |
ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; CKD, chronic kidney disease; GLS, global longitudinal strain; LAVI, left atrial volume index; LVEF, left-ventricular ejection fraction; LVESV, left-ventricular end-systolic volume; MRA, mineralocorticoid receptor antagonists n, number; y, years.
Table 2.
Uni- and multi-variable Cox proportional hazard models of HF-related deaths and/or hospitalizations.
Table 2.
Uni- and multi-variable Cox proportional hazard models of HF-related deaths and/or hospitalizations.
| Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age (years) | 1.04 (1-1.08) | 0.891 | ||
| Male gender | 0.93 (0.77-1.13) | 0.770 | ||
| NYHA | 1.04 (0.95-1.18) | 0.441 | ||
| QRS (ms) | 1.15 (1.01-1.29) | 0.126 | ||
| Diabetes mellitus | 1.52 (1.28 – 2.05) | <0.001 | 1.27 (1.12-1.98) | 0.003 |
| Chronic kidney disease (eGFR<45mL/min/1.73 m2 ) | 1.88 (1.39-2.74) | 0.009 | 1.29 (1.10-2.12) | 0.068 |
| CRT response | 1.30 (1.03 – 1.85) | 0.033 | 1.12 (0.98 – 1.43) | 0.394 |
| GLS (absolute value %) | 0.48 (0.32-2.1) | <0.001 | 0.77 (0.51-1.91) | 0.002 |
| NT-proBNP | 1.78 (1.59-245) | <0.001 | 1.55 (1.43-2.01) | 0.002 |
Table 3.
Uni- and multi-variable Cox proportional hazard models of secondary endpoint (HF-related deaths).
Table 3.
Uni- and multi-variable Cox proportional hazard models of secondary endpoint (HF-related deaths).
| Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age (years) | 1.01 (0.99-1.03) | 0.932 | ||
| Male gender | 1.05 (0.91-1.19) | 0.690 | ||
| NYHA | 1.11 (1.01-1.25) | 0.702 | ||
| QRS (ms) | 1.15 (1.01-1.29) | 0.126 | ||
| Diabetes mellitus | 1.28 (1.10 – 1.88) | 0.008 | 1.27 (1.12-1.98) | 0.087 |
| Atrial fibrillation | 1.89 (1.51 – 2.67) | <0.001 | 1.66 (1.31-2.22) | <0.001 |
| Chronic kidney disease (eGFR<45mL/min/1.73 m2 ) | 1.66 (1.33-2.55) | 0.006 | 1.41 (1.17-1.98) | <0.001 |
| CRT response | 1.91 (1.23 – 3.05) | 0.012 | 1.22 (1.15 – 2.43) | 0.132 |
| GLS (absolute value %) | 0.67 (0.56-1.05) | 0.015 | 0.96 (0.81-1.11) | 0.091 |
| NT-proBNP | 1.64 (1.23-2.22) | <0.001 | 1.23 (1.01-1.69) | <0.001 |
Table 4.
Characteristics of CRT responders and non-responders at baseline.
| CRT-responders (N=104) |
CRT non-responders (N=39) |
p | |
|---|---|---|---|
| Age, y | 70±11 | 74±7 | 0.423 |
| Males, n | 74 (71.2%) | 29 (74.4%) | 0.831 |
| LVEF (%) | 28 ± 6 | 26 ± 8 | 0.891 |
| LVESV (ml) | 148 ± 55 | 153 ± 52 | 0.790 |
| LAVI (ml/m2) | 37 ± 7 | 33 ± 5 | 0.029 |
| GLS (%) | -8.2±2.4 | -6.2±1.8* | <0.001 |
| QRS duration (ms) | 167 ± 29 | 151 ± 22 | 0.061 |
| NYHA II | 31 (30%) | 15 (38.5%) | 0.309 |
| NYHA III | 73 (70.2%) | 24 (61.5%) | 0.298 |
| Diabetes, n | 25 (24%) | 10 (25.6%) | 0.925 |
| Atrial Fibrillation | 21 (20.2%) | 7 (17.9%) | 0.881 |
| CKD (stage IV-V), n | 4 (7.7%) | 2 (5.1%) | 0.123 |
| NT-proBNP (pg/ml) | 1589±232 | 1998±308 | <0.001 |
| Diuretics, n | 101 | 37 | 0.955 |
| ACEIs/ARBs, n | 88 | 32 | 0.906 |
| MRA, n | 74 | 32 | 0.881 |
| B-blockers, n | 95 | 36 | 0.984 |
| Primary endpoint,n | 52 (50%) | 32 (82%) | <0.001 |
| Secondary endpoint, n | 35 (33.6%) | 18 (46.2%) | 0.007 |
ACEIs, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blockers; CKD, chronic kidney disease; GLS, global longitudinal strain; LAVI, left atrial volume index; LVEF, left-ventricular ejection fraction; LVESV, left-ventricular end-systolic volume; MRA, mineralocorticoid receptor antagonists n, number; y, years.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



