
Submitted:
24 November 2023
Posted:
27 November 2023
You are already at the latest version
Abstract
This study aimed to investigate the efficacy of probiotics in elderly hospitalized tube-fed patients undergoing antibiotic therapy for Clostridium difficile-associated diarrhea (CDAD). Probiotics were administered to 29 patients, with twice-daily doses for 7 days following the completion of antibiotic treatment. In the probiotic group, while stool form showed no significant change, there was a significant decrease in stool frequency. Conversely, the control group exhibited improved stool form but not frequency. The probiotic group maintained a significant difference in stool form during the follow-up period. Additionally, the control group showed a positive correlation between stool form, frequency, antibiotic therapy, and intensive care unit admission, which was not observed in the probiotic group. These findings suggest that supplementing with probiotics can effectively normalize stool form in elderly hospitalized tube-fed patients undergoing antibiotic treatment for CDAD, highlighting the potential benefits of probiotic intervention in this specific population.
Keywords:
Antibiotic-associated diarrhea (AAD)
; Clostridium difficile-associated diarrhea (CDAD)
; Probiotic
; Tube-fed elderly
; Infectious disease
1. Introduction
Antibiotics have significant benefits in treating many infectious diseases, but they often cause gastrointestinal (GI) side effects. Among them, antibiotic-associated diarrhea (AAD) is the most commonly experienced symptom by hospitalized patients, due to disruption of the GI microbiota and mucosal integrity, leading to overgrowth of pathogens and a metabolic imbalance. The incidence of AAD ranges 5% to 49%, and it can occur any time after antibiotic exposure [1]. About 10%~25% of AAD cases were attributed to Clostridium difficile infection (CDI), which is commonly implicated with antibiotics including fluoroquinolones, clindamycin, penicillins, and third- or fourth-generation cephalosporins. Clostridium difficile is a gram-positive, spore-forming bacillus that was first isolated in 1935 from the fecal flora of healthy neonates and was identified as the pathogen responsible for pseudomembranous colitis in 1978 [2,3,4].
Clostridium difficile-associated diarrhea (CDAD) results in symptoms ranging from mild diarrhea to colitis, toxic megacolon, and death, and is the most common healthcare-associated diarrhea in developed countries. According to a study conducted at National Cheng Kung University Hospital, Taiwan, the proportion of hospitalized patients with CDAD was 42.6 cases per 100,000 patient-days, and was highest in intensive care units (ICUs) (110.6 cases per 100,000 patient-days) [5]. Risk factors for CDAD include an advanced age and hospitalization, in addition to antibiotics. Research on outbreaks of C. difficile in Quebec found that individuals aged over 65 years had a ten-fold higher incidence rate compared to younger individuals [6]. The incidence rate of CDAD among outpatient was 3%, while in hospitalized adults, it ranged 20% to 30% [7]. It was also reported that 61% of tube feeding-related diarrhea was caused by medications, and 17% of the cases were attributed to C. difficile [8].
Several studies showed that specific strains of probiotics have various beneficial health effects, suggesting that providing probiotics may be helpful in controlling or preventing AAD. Common probiotic strains associated with GI health include Lactobacillus rhamnosus GG, Bifidobacterium ssp., Streptococcus ssp., the yeast Saccharomyces boulardii, and other Lactobacillus species such as L. reuteri, L. acidophilus, and L. casei, and the use of multiple strains of probiotics had more-significant effects against CDAD compared to using a single probiotic strain. Two studies revealed that an intervention with a combination of L. acidophilus and L. casei showed improvements in decreasing incidence rates of AAD and CDAD among hospitalized patients [9]. Furthermore, the suitable dosage of probiotics given is also crucial, as previous studies found that administering probiotic products with different dosages (5×1010 colony-forming units (CFU) vs. 1011 CFU) to elderly hospitalized patients significantly reduced the incidence rates of AAD and CDAD, while the highest dose had a better effect compared to the lower dose [10,11]. Another study that used a combination of L. acidophilus, L. paracasei, and B. lactis found that the high-dose group had significantly lower incidence rates of AAD and CDAD compared to the control group, and further discovered that for each one-unit increase in the body-mass index (BMI), the odds of AAD incidence decreased 0.9-fold [12]. Although several studies indicated the beneficial effects of probiotics against the incidence of AAD in hospitalized patients, the use of probiotics in elderly tube-fed patients treated with antibiotics was not investigated. Furthermore, the prolonged effects of probiotics after patients are discharged remain unknown. Therefore, the aim of our study was to investigate the effects of probiotics in elderly hospitalized tube-fed patients with antibiotic use, and further evaluate its prolonged effects after patients are discharged.
2. Materials and Methods
This study was conducted at Taipei Medical University Hospital (TMUH). All research procedures performed in this trial were in strict accordance with a predefined protocol that was approved by all researchers and the local ethics committee. The ethics committee approved the study protocol on 23 September 2020 (certificate no.: N202008008), and all participants provided informed consent before participation.
Subjects
Eligible patients were hospitalized, were aged ≥ 65 years, were being tube-fed, and had been prescribed antibiotic therapy for a minimum of 3 days and a maximum of 14 days. Exclusion criteria were the existence of a bowel disease such as a short bowel disease or inflammatory bowel disease, use of total parenteral nutrition, documented CDI within 3 months before enrollment, immunotherapy, and immunosuppressive disease such as hematological disease or acquired immunodeficiency syndrome (AIDS), antibiotics use within 30 days before enrollment, other probiotics use or participation in other clinical therapy.
Study design
This was a single-center, case-controlled study. Each enrolled subject was matched with a contemporary control. Control patients were chronologically recruited at the same time as the probiotic patients were being enrolled. If they met all inclusion and exclusion criteria, they served as a study control. Reasons that patients were not included in the treatment group were due to the time to obtain consent was greater than 48 h. Probiotic patients received an initial dose of the assigned intervention within 48 h of their prescribed antibiotic therapy, and daily use of the product continued for 7 additional days after completion of their antibiotics. The study product was commercially purchased and contained 109 CFU of L. plantarum, L. rhamnosus, L. acidophilus, B. lactis, S. thermophiles, L. casei, and B. longum. The intervention was administered twice daily (3 g per package), approximately 2 h after the antibiotic and meals. The investigators followed the subjects via a weekly telephone call for 4 weeks after finishing the antibiotic course to inquire about the stool form, adverse events, and compliance with the study protocol.
Data collection
We collected anthropometric data, laboratory data, medication records, stool form, and nutritional status. All patients received a standard nutrition care process under a registered dietitian. The Bristol Stool Form Scale form was used to assess the stool status (types 1 and 2 indicate constipation, types 3 and 4 are ideal stools as they are easier to pass, and types 5~7 may indicate diarrhea and urgency), and the Nutritional Risk Screening (NRS) 2002 score was used to assess the nutritional risk (score 0 as well-nourished, scores 1 and 2 as mild malnutrition risk, scores 3 and 4 as moderate malnutrition risk, and scores of ≥ 5 as a high malnutrition risk). Subjects were supplied with diary cards and instructed by the physician to record any diarrhea and the number of liquid stools per day during the experimental period. Subjects who had not completed their full antibiotic treatment and/or study product during their stay in the hospital received the appropriate amount of each to complete treatment on an outpatient basis.
Statistical methods
Data are expressed as the mean ± standard deviation (SD). A two-tailed χ2 test or Fisher’s exact test was used to compare between the groups. Continuous data were analyzed by nonparametric tests (Wilcoxon’s rank-sum or Mann-Whitney U test). The correlation between variables in the study groups used Spearman’s correlation. p<0.05 was considered statistically significant. SPSS version 26.0 was used to perform all statistical analyses.
3. Results
In total, 165 patients were screened, and 121 patients were excluded. In total, 44 patients were eligible to participate in the study, and 29 patients agreed and signed the consent form, and these served as probiotic group. The other 15 patients served as control group. Failure to complete the study was due to the use of antibiotics for more than 14 days or personal reasons (Figure 1). Average ages of the control and probiotic groups were 83.1 and 80.0 years, respectively. No significant differences were observed in baseline characteristics between the two groups (Table 1).
Compliance with the study product was 100%, as there were no returned study products, and they were consumed according to the patients' notes. The mean stool forms at the beginning of the antibiotic therapy in the control and antibiotic group were 5.5 ± 0.8 and 5.6 ± 1.4, with frequencies of 2.7 ± 2.1 and 2.0 ± 1.0 times, respectively, with no significant differences between the two groups. In the probiotic group, no significant difference was found in stool form between the beginning and end of antibiotic therapy (5.5 ± 0.8 vs. 5.1 ± 1.1), but the frequency significantly decreased (2.0 ± 0.7 vs. 1.6 ± 0.7), whereas in the control group, although the stool form between beginning and end of antibiotic therapy significantly improved (5.6 ± 1.4 vs. 4.5 ± 1.4), the frequency did not significantly differ (2.7 ± 2.1 vs. 2.4 ± 1.5). During the follow-up period for the probiotic group (a total of 4 weeks), the stool form significantly differed compared to both the beginning and end of antibiotic therapy. The frequency during the follow-up period also significantly decreased compared to the beginning of antibiotic therapy (2.0 ± 1.0 vs. 1.6 ± 0.8). Members of the control group were discharged 2 weeks after the end of antibiotic treatment and were unable to be followed up via phone calls as control patients disagreed and did not sign the consent forms; hence, the stool form only had 2 weeks of data from in-house medical records. The stool form and frequency during the follow-up period in the control group did not significantly differ compared to the beginning or end of antibiotic therapy (Table 2 & Figure 2).
The average number of days that probiotics were given was 16.0 ± 2.8 days. Both the control and probiotic groups had similar nutritional requirements, and percentages of calorie requirements that were met for the control and probiotic groups were 91.2% and 98.1%, and percentages of protein requirements that were met were 88.1% and 91.7%, respectively. No significant differences were found between the groups (Table 3).

Table 1.
Basic characteristics of the study groups.
| Control (N=11) | Probiotic (N=11) | |
|---|---|---|
| Male sex (%) | 63.6% | 54.5% |
| Body-mass index (kg/m2) | 22.1 ± 4.2 | 21.9 ± 2.6 |
| Age (years) | 83.1 ± 10.3 | 80.0 ± 10.2 |
| Length of hospitalization (days) | 14.9 ± 6.9 | 12.1 ± 6.4 |
| NRS score_initial | 3.7 ± 1.8 | 3.6 ± 1.7 |
| NRS score_discharge | 2.9 ± 1.3* | 2.6 ± 0.9* |
| ICU admission (%) | 27.3% | 45.5% |
| Duration of antibiotic therapy (days) | 10.8 ± 2.9 | 10.3 ± 4.4 |
| Numbers of antibiotics | 1.9 ± 0.8 | 2.2 ± 1.0 |
| Antibiotic type, n (%) | ||
| Frequently associated CDI | ||
| Broad-spectrum penicillin | 6 (54.5) | 6 (54.5) |
| Lincosamide | 1 (9.1) | 0 (0.0) |
| 2nd-generation cephalosporin | 3 (27.3) | 4 (36.4) |
| 3rd-generation cephalosporin | 0 (0.0) | 7 (63.6) |
| 4th-generation cephalosporin | 0 (0.0) | 2 (18.2) |
| Occasionally associated CDI | ||
| 1st-generation cephalosporin | 2 (18.2) | 0 (0.0) |
| Macrolide | 3 (27.3) | 1 (9.1) |
| Penicillinase-sensitivity penicillin | 1 (9.1) | 1 (9.1) |
| Rarely associated CDI | ||
| Aminoglycoside | 2 (18.2) | 2 (18.2) |
| Vancomycin | 3 (27.3) | 0 (0.0) |
| Laboratory data | ||
| Hemoglobin (g/dL) | 10.1 ± 1.7 | 11.6 ± 1.9 |
| White blood cells (103/µL) | 8.9 ± 3.9 | 10.9 ± 6.6 |
| % neutrophils | 70.7 ± 14.8 | 75.9 ± 12.0 |
| % lymphocytes | 18.3 ± 11.0 | 13.7 ± 9.3 |
| Cr (mg/dL) | 1.3 ± 1.7 | 0.9 ± 0.6 |
| Albumin (g/dL) | 3.2 ± 0.7 | 3.5 ± 0.8 |
| C-reactive protein (mg/dL) | 5.4 ± 4.1 | 6.3 ± 8.7 |
| Na (mEq/L) | 136.0 ± 8.3 | 136.7 ± 10.9 |
| K (mEq/L) | 4.6 ± 1.0 | 3.8 ± 0.4§ |
| CDI occurrence rate | 9.0 % | 0.0% |
| ICU, intensive care unit; NRS, Nutrition Risk Screening; Cr, creatinine; CDI, Clostridium difficile infection.* p<0.05 compared to the NRS score_initial within a group. § p<0.05 showed a significant difference between groups. | ||
Table 2.
Stool form and frequency in the study groups.
| Stool form | Stool frequency | |||
| Control group | Probiotic group | Control group | Probiotic group | |
| Antibiotic therapy | 5.6 ± 1.4 | 5.5 ± 0.8 | 2.7 ± 2.1 | 2.0 ± 1.0 |
| End of antibiotic therapy | 4.5 ± 1.4a | 5.1 ± 1.1 | 2.4 ± 1.5 | 1.6 ± 0.7a |
| f/u week 1 | 4.3 ± 1.0 | 4.6 ± 1.3ab | 3.0 ± 2.2 | 1.6 ± 0.8a |
| f/u week 2 | 4.3 ± 1.2 | 4.8 ± 1.0ab | 3.0 ± 2.6 | 1.6 ± 0.8a |
| f/u week 3 | - | 4.5 ± 1.3ab | - | 1.6 ± 0.8a |
| f/u week 4 | - | 4.2 ± 1.1ab | - | 1.6 ± 0.8a |
| Antibiotic therapy and end of antibiotic therapy in the probiotic group were with the study product. Stool form: types 1 and 2 indicate constipation, 3 and 4 are ideal stools as they are easier to pass, and 5~7 may indicate diarrhoea and urgency. f/u, follow up. Sample numbers for f/u weeks 1 and 2 in the control group were 4 and 3, respectively. a p<0.05 compared to the beginning of antibiotic therapy within a group using the Wilcoxon signed-rank test. b p<0.05 compared to the end of the antibiotic therapy within a group using the Wilcoxon signed-rank test. | ||||
Figure 2.
Stool form (left) and stool frequency (right) in the probiotic group. Stool form: types 1 and 2 indicate constipation, 3 and 4 are ideal stools as they are easier to pass, and 5~7 may indicate diarrhea and urgency. f/u, follow up; wk, week. a p<0.05 compared to the beginning of antibiotic therapy within a group using the Wilcoxon signed-rank test. b p<0.05 compared to the end of the antibiotic therapy within a group using the Wilcoxon signed-rank test.
Figure 2.
Stool form (left) and stool frequency (right) in the probiotic group. Stool form: types 1 and 2 indicate constipation, 3 and 4 are ideal stools as they are easier to pass, and 5~7 may indicate diarrhea and urgency. f/u, follow up; wk, week. a p<0.05 compared to the beginning of antibiotic therapy within a group using the Wilcoxon signed-rank test. b p<0.05 compared to the end of the antibiotic therapy within a group using the Wilcoxon signed-rank test.
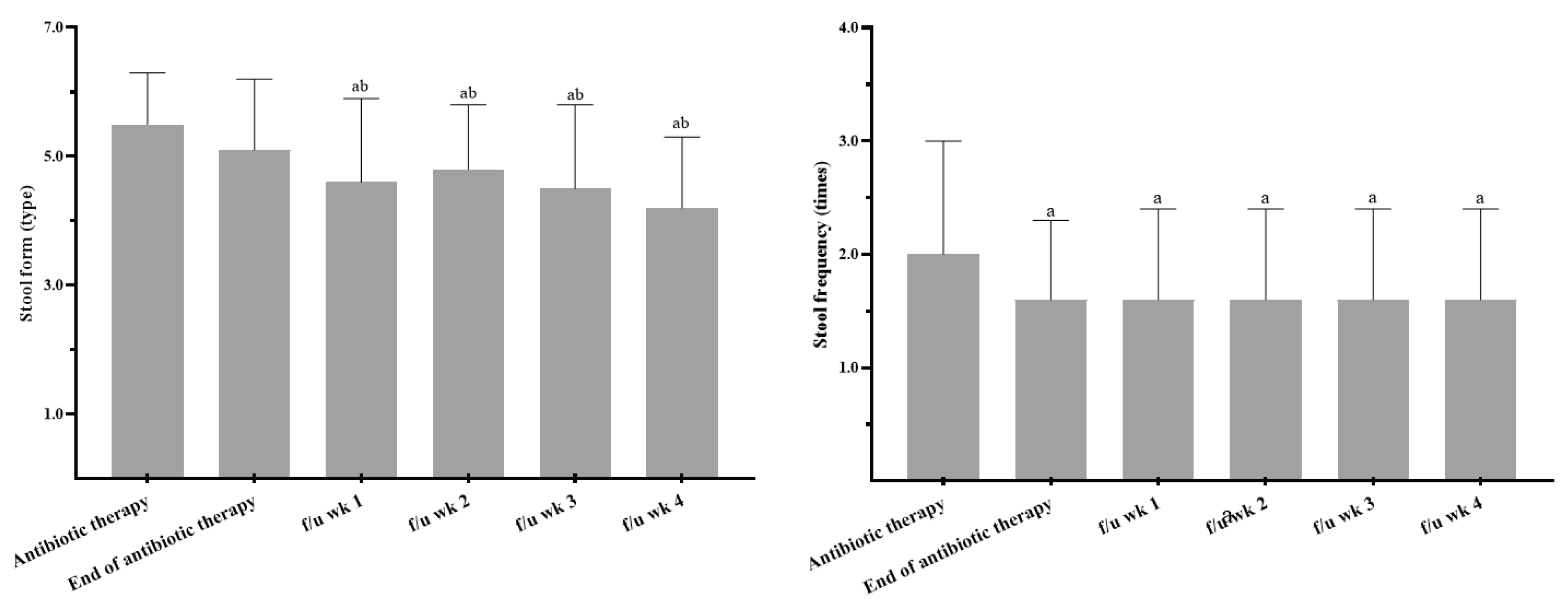
Table 3.
Nutrition requirements and actual intake in the study groups (2nd visit).
| Control | Probiotic | |
|---|---|---|
| Estimate calorie requirement (kcal) | 1512.5 ± 155.3 | 1455.6 ± 113.0 |
| Actual calorie intake (kcal) | 1380.1 ± 289.1 | 1428.6 ± 180.8 |
| Estimate protein requirement (g) | 67.9 ± 9.0 | 68.5 ± 11.5 |
| Actual protein intake (g) | 59.8 ± 15.7 | 62.8 ± 13.4 |
Variables such as ICU admission, duration of antibiotic therapy, and numbers of antibiotics used were assessed using Spearman’s correlation. In the control group, the stool form at the beginning of antibiotic therapy was moderately correlated (R=0.67, p<0.001), and the stool frequency at the beginning of antibiotic therapy and initial NRS score were highly correlated (R=0.84, p<0.001; R=0.81, p<0.001) with ICU admission. The stool form during the follow-up period (weeks 1 and 2) was negatively correlated with the duration of antibiotic therapy. The stool frequency during the follow-up period (week 1) was highly correlated with the duration of antibiotic therapy. In the probiotic group, the stool frequency was correlated with ICU admission, but the duration of antibiotic therapy and numbers of antibiotics were not significantly correlated (Table 4).
4. Discussion
Use of antibiotics is an effective option for treating infectious diseases, but inappropriate use of broad-spectrum antibiotics and the emergence of drug-resistant bacteria have raised significant clinical concerns, such as CDAD which is one of the most frequent consequences leading by inappropriate use of antibiotic treatment [13]. In a meta-analysis that reviewed 5496 hospitalized patients (in 20 studies) with the majority of studies conducted in Asia (14 studies), the frequency of CDAD among AAD was 20% (95% confidence interval [CI] 13.0%–28.0%) [14]. A review mentioned that AAD complications could prolong the length of stay, and increase mortality rates and medical costs. Moreover, complications of CDI are much more severe than those of AAD, as there are higher rates of colectomy surgeries and chances of readmission [15]. Probiotics are defined as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” [16]. In a systematic review, the use of probiotics could reduce the risk of CDI by 60.5% in both adults and children treated with antibiotics as inpatients and outpatients [17]. The Bristol Stool Form Scale can be used to monitor changes in intestinal function, as such scales have been widely utilized in both clinical practice and research [18]. Furthermore, this scale demonstrates the validity and reliability in diarrhea-predominant irritable bowel syndrome [19]. In our study, we found the stool form in the probiotic group was much closer to the ideal form during follow-up compared to the beginning or end of antibiotic therapy, which was not observed in the control group. A triple-blind randomized control trial (RCT) that used capsules containing L. acidophilus, L. paracasei, and B. lactis found that liquid stools occurred less often in both probiotic groups (low dose: 4.17 × 109 CFU and high dose: 1.70 × 1010 CFU) [12]. Another double-blind RCT that used fermented milk containing L. acidophilus CL1285® and L. casei observed that the incidence of loose stools was lower in the high-dose group (1011 CFU) who were aged 50~70 years [11], but 5 × 1010 CFU of the same product produced no significant decreases in the incidence or adverse effects of CDAD [10].
The US Centers for Disease Control revealed that 55% of hospitalized patients had received at least one antibiotic during hospitalization, and this number increased to 70% in the ICU with multiple antibiotics [20]. Increasing evidence indicates that critical illnesses and widespread antibiotic use have resulted in gut dysbiosis in ICU patients, which is associated with higher rates of ICU infections, sepsis, and multiple organ dysfunction syndrome [21]. We found a positive correlation between the stool form and frequency during antibiotic therapy and ICU admission in the control group but not in the probiotic group, indicating that the use of probiotics could be used to prevent diarrhea in ICU patients. A case-controlled trial also demonstrated that fermented milk containing 10 billion L. casei could be provided to ICU patients with no serious adverse effects, such as insertion of a rectal tube for diarrhea control, emesis, requirement for parenteral nutrition, or the need for surgical management of the GI tract, suggesting its safety and stability for use in ICU patients [22].
Our study revealed that no CDI occurred in the probiotic group, whereas there was only one case in the control group. An individual patient data meta-analysis suggested that probiotics may be useful and safe for CDI prevention. Those participants were male (over 50%), were taking two or more antibiotics, had lengths of hospital stay of 7 (4~15) days, had durations of antibiotic therapy of 10 (7~14) days, and used probiotics for 15 (11~21) days [23], and we had similar characteristics in our study groups. Both inadequate or excessive feeding may be harmful in adult hospitalized patients, hence consultation from dietitians or other experts on feeding prescription is crucial [24]. According to the European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines, calorie delivery should subsequently be increased up to 80%~100% of the measured energy expenditure after 3 days in the ICU [25]. In this study, subjects in both group met 80% of their nutritional requirements at the second visit.
In a retrospective study performed in France, it was found that populations with malnutrition were correlated with CDI. But its definition was based on body weight loss, a lower BMI, low calorie intake, and low albumin and high C-reactive protein (CRP) levels [26], and such definitions are vague and may not clarify the severity of malnutrition. In our study, we used the NRS 2002 which is a summed total of the nutritional score, severity of disease score, and age adjustment score that may provide a clearer statement of malnutrition, by giving a total number of points ranging 0 to 7 [27]. Our study demonstrated that patients in both groups had a moderate malnutrition risk as both had scores of > 3. After discharge, their nutritional statuses significantly improved.
The reason for the different results is that some strains of our probiotics are not commonly used for CDI, and Lactobacillus and B. longum are more commonly investigated in the study of inflammatory bowel disease and colitis [28,29], and Streptococcus thermophiles was used to reduce symptoms of lactose intolerance [30]. There are a few limitations in our study. First, the small sample size due to the reduced number of hospitalized patients during the COVID-19 pandemic and the inability to contact and obtain informed consent from family members due to visiting restrictions resulted in a lower enrollment rate. Second, the incomplete experimental design was due to inclusion of patients in the control group who either declined to participate or were unable to provide consent within the specified timeframe. As a result, it was hard to track the stool form and frequency during the follow-up period, leading to incomplete experimental data that could not be analyzed. Last, we did not design a comparison between different compositions of probiotic strains.
5. Conclusions
This study demonstrates that supplementing probiotics can help normalize the stool form in elderly hospitalized tube-fed patients using antibiotics and is considered safe for use in ICUs.
Author Contributions
C.H.H., H.Y.S and Y.W.C. were involved in the conceptualization and the design of this study. C.H.H. conducted this study and biochemical analyses. C.H.H. wrote the original draft preparation. C.H.H. and Y.W.C reviewed and edited this study. Y.H.C., H.Y.S and H.C.C. supervised this study. Y.W.C. visualized and supervised this study. All authors provided critical inputs to data analyses and the inter-pretation of the data. All authors read and approved the final version for submission.
Funding
This study was funded by TMUH, grant no. 109TMU-TMUH-30.
Acknowledgements
We would like to express our sincere gratitude to our advisor, Dr. Chang, for her invaluable guidance and support throughout the research process. We also wish to thank the Taipei Medical University Hospital for their financial support. Finally, we are grateful to all of the research participants who generously gave their time and effort to this project.
Declaration of Competing Interest:
All authors declare no conflict of interests.
References
- Cai, J.; Zhao, C.; Du, Y.; Zhang, Y.; Zhao, M.; Zhao, Q. Comparative efficacy and tolerability of probiotics for antibiotic-associated diarrhea: Systematic review with network meta-analysis. United European Gastroenterol J. 2018, 6, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Kyne, L.; Farrell, R.J.; Kelly, C.P. Clostridium difficile. Gastroenterol Clin North Am. 2001, 30, 753–777. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Lamont, J.T. Clostridium difficile Infection. New England Journal of Medicine. 2015, 372, 1539–1548. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Hamill, R.J.; Musher, D.M. Treatment of Clostridium difficile-associated disease: old therapies and new strategies. Lancet Infect Dis. 2005, 5, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Wu, C.J.; Lee, H.C.; Yan, J.J.; Chang, C.M.; Lee, N.Y.; et al. Clostridium difficile infection at a medical center in southern Taiwan: incidence, clinical features and prognosis. J Microbiol Immunol Infect. 2010, 43, 119–125. [Google Scholar] [CrossRef]
- Pepin, J.; Valiquette, L.; Cossette, B. Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. CMAJ. 2005, 173, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G. Antibiotic-Associated Diarrhea. New England Journal of Medicine. 2002, 346, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Edes, T.E.; Walk, B.E.; Austin, J.L. Diarrhea in tube-fed patients: feeding formula not necessarily the cause. Am J Med. 1990, 88, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Yap, C.; Lytvyn, L.; Lo, C.K.; Beardsley, J.; Mertz, D.; et al. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst Rev. 2017, 12, CD006095. [Google Scholar] [CrossRef] [PubMed]
- Beausoleil, M.; Fortier, N.; Guenette, S.; L'Ecuyer, A.; Savoie, M.; Franco, M.; et al. Effect of a fermented milk combining Lactobacillus acidophilus Cl1285 and Lactobacillus casei in the prevention of antibiotic-associated diarrhea: a randomized, double-blind, placebo-controlled trial. Can J Gastroenterol. 2007, 21, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.W.; Mubasher, M.; Fang, C.Y.; Reifer, C.; Miller, L.E. Dose-response efficacy of a proprietary probiotic formula of Lactobacillus acidophilus CL1285 and Lactobacillus casei LBC80R for antibiotic-associated diarrhea and Clostridium difficile-associated diarrhea prophylaxis in adult patients. Am J Gastroenterol. 2010, 105, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Ouwehand, A.C.; DongLian, C.; Weijian, X.; Stewart, M.; Ni, J.; Stewart, T.; et al. Probiotics reduce symptoms of antibiotic use in a hospital setting: a randomized dose response study. Vaccine. 2014, 32, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Larcombe, S.; Hutton, M.L.; Lyras, D. Involvement of Bacteria Other Than Clostridium difficile in Antibiotic-Associated Diarrhoea. Trends in Microbiology. 2016, 24, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Nasiri, M.J.; Goudarzi, M.; Hajikhani, B.; Ghazi, M.; Goudarzi, H.; Pouriran, R. Clostridioides (Clostridium) difficile infection in hospitalized patients with antibiotic-associated diarrhea: A systematic review and meta-analysis. Anaerobe. 2018, 50, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Abad, C.L.R.; Safdar, N. A Review of Clostridioides difficile Infection and Antibiotic-Associated Diarrhea. Gastroenterol Clin North Am. 2021, 50, 323–340. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. Are Probiotics Money Down the Toilet? Or Worse? Are Probiotics Money Down the Toilet? Or Worse? Are Probiotics Money Down the Toilet? Or Worse? JAMA. 2019, 321, 633–635. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.S.; Chamberlain, R.S. Probiotics are effective at preventing Clostridium difficile-associated diarrhea: a systematic review and meta-analysis. International journal of general medicine. 2016, 9, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scandinavian journal of gastroenterology. 1997, 32, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.R.; Raker, J.M.; Whelan, K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. 2016, 44, 693–703. [CrossRef]
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; et al. International study of the prevalence and outcomes of infection in intensive care units. Jama. 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; McDonald, D.; Knight, R. Role of the microbiome, probiotics, and 'dysbiosis therapy' in critical illness. Current opinion in critical care. 2016, 22, 347–353. [Google Scholar] [CrossRef]
- Alberda, C.; Marcushamer, S.; Hewer, T.; Journault, N.; Kutsogiannis, D. Feasibility of a Lactobacillus casei Drink in the Intensive Care Unit for Prevention of Antibiotic Associated Diarrhea and Clostridium difficile. Nutrients. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Lytvyn, L.; Lo, C.K.; Allen, S.J.; Wang, D.; Szajewska, H.; et al. Microbial Preparations (Probiotics) for the Prevention of Clostridium difficile Infection in Adults and Children: An Individual Patient Data Meta-analysis of 6,851 Participants. Infect Control Hosp Epidemiol. 2018, 39, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Stroud, M.; Duncan, H.; Nightingale, J. Guidelines for enteral feeding in adult hospital patients. 2003; 52, (Suppl. S7), vii1–vii12. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Khanafer, N.; Vanhems, P.; Barbut, F.; Luxemburger, C.; group CDIS; Demont, C.; et al. Factors associated with Clostridium difficile infection: A nested case-control study in a three year prospective cohort. Anaerobe. 2017, 44, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z.; Ad Hoc, E.W.G. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Zhao, Z.; Wang, W.; Liu, X. Bifidobacterium Longum: Protection against Inflammatory Bowel Disease. Journal of immunology research. 2021, 2021, 8030297. [Google Scholar] [CrossRef] [PubMed]
- Quigley, E.M.M. Chapter 16 - Bifidobacterium longum. In The Microbiota in Gastrointestinal Pathophysiology; Floch, M.H., Ringel, Y., Allan Walker, W., Eds.; Academic Press: Boston, 2017; pp. 139–141. [Google Scholar]
- Hutkins, R.; Goh, Y.J. STREPTOCOCCUS|Streptococcus thermophilus. In Encyclopedia of Food Microbiology (Second Edition); Batt, C.A., Tortorello, M.L., Eds.; Academic Press: Oxford, 2014; pp. 554–559. [Google Scholar]
Figure 1.
Participant enrollment through the study.
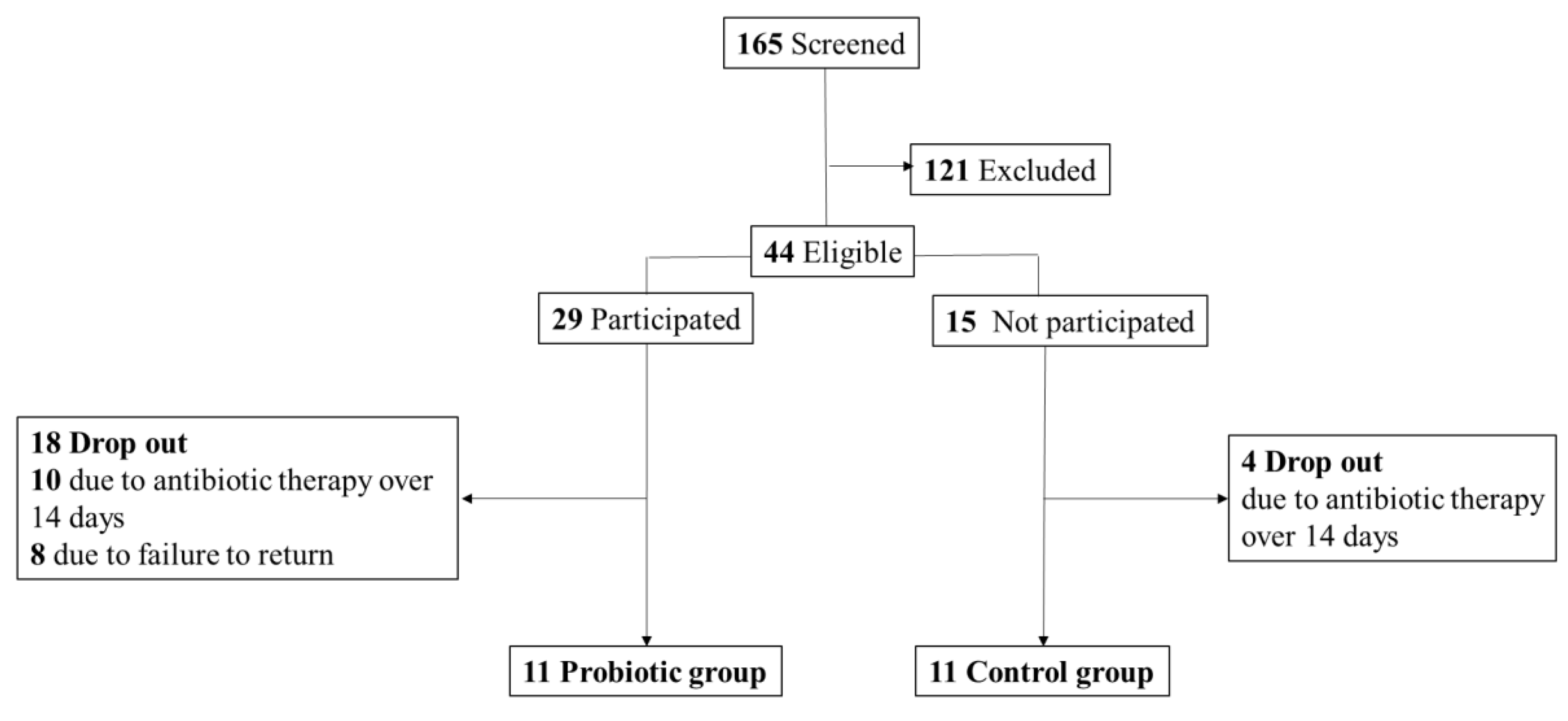
Table 4.
Correlations between variables in the study groups.
| Control | Probiotic | ||||
|---|---|---|---|---|---|
| Variable | R | p | R | p | |
| ICU admission | Length of hospitalization | 0.23 | 0.54 | 0.33 | 0.32 |
| Duration of antibiotic therapy | 0.30 | 0.38 | 0.21 | 0.54 | |
| Kinds of antibiotics | 0.55 | 0.08 | 0.22 | 0.51 | |
| Stool form_antibiotic therapy | 0.67* | 0.00 | -0.06 | 0.85 | |
| Stool frequency_antibiotic therapy | 0.84* | 0.00 | 0.16 | 0.65 | |
| Stool form_end of antibiotic therapy | -0.27 | 0.43 | -0.4 | 0.22 | |
| Stool frequency_end of antibiotic therapy | 0.49 | 0.13 | 0.00 | 1.00 | |
| NRS score_initial | 0.81* | 0.00 | 0.38 | 0.24 | |
| NRS score_discharge | 0.43 | 0.19 | -0.14 | 0.68 | |
| Duration of antibiotic therapy | Stool form_antibiotic therapy | 0.20 | 0.56 | 0.31 | 0.35 |
| Stool frequency_antibiotic therapy | 0.04 | 0.90 | 0.50 | 0.11 | |
| Stool form_end of antibiotic therapy | 0.13 | 0.70 | 0.01 | 0.98 | |
| Stool frequency_end of antibiotic therapy | 0.12 | 0.71 | 0.08 | 0.82 | |
| Stool form_f/u week 1 | -1.00* | 0.00 | -0.18 | 0.60 | |
| Stool frequency_f/u week 1 | 0.95* | 0.05 | 0.09 | 0.79 | |
| Stool form_f/u week 2 | -1.00* | 0.00 | -0.06 | 0.09 | |
| Stool frequency_f/u week 2 | 0.87 | 0.33 | 0.09 | 0.79 | |
| Numbers of antibiotics | Stool form_antibiotic therapy | 0.52 | 0.10 | -0.22 | 0.51 |
| Stool frequency_antibiotic therapy | 0.52 | 0.10 | 0.16 | 0.64 | |
| Stool form_end of antibiotic therapy | -0.15 | 0.67 | 0.19 | 0.59 | |
| Stool frequency_end of antibiotic therapy | 0.29 | 0.39 | 0.08 | 0.81 | |
| Stool form_f/u week 1 | -0.09 | 0.06 | 0.24 | 0.48 | |
| Stool frequency_f/u week 1 | 0.89 | 0.10 | 0.30 | 0.36 | |
| Stool form_f/u week 2 | -1.00* | 0.00 | 0.08 | 0.81 | |
| Stool frequency_f/u week 2 | 0.87 | 0.33 | 0.31 | 0.36 | |
| *p<0.05 indicates the correlation is significant using Spearman’s correlation. ICU, intensive care unit; NRS, Nutritional Risk Screening; f/u, follow-up. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



