
Submitted:
18 November 2023
Posted:
21 November 2023
You are already at the latest version
Abstract
Background: Bacterial conjunctivitis is one of the most commonly encountered eye complications in medicine, particularly in developing nations. In Hadhramout Governorate-Yemen, there is no data about bacterial conjunctivitis among patients. Aim: The present study aimed to determine the prevalence rate of bacterial conjunctivitis among patients seeking hospitals in Hadhramout Governorate, Yemen. Methods: A total of 1722 eye swabs were collected from patients attending different Hadhramout hospitals over a period of April to December 2018. The isolation and identification of bacteria are performed using standard bacteriological procedures. In addition, structured questionnaires were used to gather data from patients. Results: Out of 1722 eye swabs, 198 (11.49%) were positive for bacterial conjunctivitis, while 1524 (88.5%) were negative. The high prevalence rate of infection was among female participants and the age group between 31 and 40 years, at 15.25% and 29.29%, respectively. In addition, the prevalence of gram-positive bacteria was significantly greater among study patients than gram-negative bacteria (58.59% vs. 41.41%). The most predominant Gram-positive bacteria were Staphylococcus aureus (26.26%), followed by Streptococci pneumoniae (17.18%), Alpha-hemolytic Streptococci (8.08%), and Staphylococcus epidermidis (7.07%). Whereas the gram-negative bacteria were Pseudomonas aeruginosa (12.1%), followed by Moraxella catarrhalis (10.1%), Haemophilus influenza (7.07%), Klebsiella sp. (6.06%), Enterobacter agglomerans (4.04%), and Neisseria gonorrhoeae (2.02%). Additionally, the majority of study patients suffered from red eyes (100%), tearing eyes (93.93%), itching (90.9%), painful eyes (87.87%), purulent eyes (56.56%), and eye discharge (38.38%). Conclusion: The prevalence rate of bacterial conjunctivitis among patients in Hadhramout, Yemen, is relatively low compared with international investigations. Further investigation is required to assess and identify the antibiotic resistance to these agents that cause conjunctivitis.
Keywords:
Bacteria
; Conjunctivitis
; Hadhramout
; Yemen
Introduction
Bacterial conjunctivitis most commonly affects otherwise healthy people worldwide, particularly in developing countries. Bacterial conjunctivitis can be transmitted from person to person through respiratory droplets, hand-to-eye contact, and eye contact with fomite, as well as exposure to infected persons, immunodeficiency states, past ocular disease, trauma, and birth exposure to agents of sexually transmitted disease [1,2].
Factors such as hygiene practices, living conditions, and access to healthcare can influence the incidence of the infection. Patients with bacterial conjunctivitis frequently complain of redness, tearing, and discharge from one or both eyes [3]. Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis are the most frequent causes of acute bacterial conjunctivitis. While Neisseria gonorrhoeae or Neisseria meningitides, Chlamydia trachomatis, Moraxella lacunata, or Gram-negative enteric flora, and Chlamydia trachomatis are extremely rare or less commonly [3].
H. influenzae is the most frequent causal organism for bacterial conjunctivitis in children, followed by S. pneumoniae and M. catarrhalis [5,6]. Adults are more frequently infected with staphylococcal types of bacteria, with a smaller percentage of cases being caused by H. influenzae and S. pneumoniae. S. aureus is more frequently detected in adults and the elderly, but it is also present in cases of bacterial conjunctivitis in children [7].
Most bacterial conjunctivitis is self-limiting. One systematic review found a clinical cure or significant improvement with a placebo within 2–5 days in 65% of people. Some organisms cause corneal or systemic complications, or both. Otitis media may develop in 25% of children with H. influenzae conjunctivitis, and systemic meningitis may complicate primary meningococcal conjunctivitis in 18% of people [5].
According to estimates, 23% of bacterial conjunctivitis cases in the United States occur in children under the age of two, 28% in children between the ages of three and nine, 13% in adolescents between the ages of 10 and 19 years old, and 36% in adults [8].
Yemen is considered to be among the world's poorest low-income nations. Recent data indicates that over 79% of the population is estimated to be living below the poverty line, with about 65 percent of these individuals being considered extremely poor. Furthermore, the majority of Yemenis lack access to clean drinking water; poor hygiene practices; unstable institutions; food insecurity; and restricted access to healthcare services are all factors that raise the risk of contracting infectious diseases [9,10,11,12,13].
There is only one study conducted in Sana’a City that revealed the prevalence rate of bacterial conjunctivitis among neonates was 51.7% [14]. There is currently no information available about the prevalence of bacterial conjunctivitis in Hadhramout Governorate, Yemen. Therefore, this study aimed to determine the prevalence rate of bacterial conjunctivitis among patients seeking hospitals in Hadhramout Governorate, Yemen.
Materials and Methods
This study is a cross-sectional study conducted among 1722 patients with bacterial conjunctivitis in Hadhramout Governorate between April and December 2018. Hadhramout is the largest governorate of Yemen by area and is located in the southeastern part of the Republic of Yemen, 794 kilometers east of the capital of Sana’a, between Al-Mahra to the east and Al-Jawf, Marib, and Shabwah to the west. The governorate is divided administratively into 28 districts, with the city of Mukalla as its capital. It borders the Kingdom of Saudi Arabia in the north (Figure 1).
Patients study
The patients included in this study are newborns, infants, children, and adults. Conjunctivitis cases were defined by a clinical diagnosis of conjunctivitis or an episode of one of the following symptoms: red or itchy eyes, pain, purulent eyes, eye discharge, and tearing. All identified cases underwent a bio-microscopic check with a slit lamp. Patients suspected of having or with a positive culture for fungal, viral, or Acanthamoeba infections were also excluded.
Data Collection
A questionnaire was designed to collect relevant data from each participant. Demographic data such as age, sex, signs, and symptoms were collected by interviewing them face-to-face.
Samples Collection
The conjunctival swabs were collected by trained healthcare staff using a cotton swab moistened with sterile saline. Two swabs from each patient were collected, one for each eye, even if the infection was in only one eye. Specimens were transported directly to the laboratory within half an hour for culture and other bacteriological analysis.
Microbiological Laboratory Analysis
The collected swabs were inoculated onto Blood agar (5% sheep blood), MacConkey agar, and Chocolate agar (HiMedia Lab., India). The inoculated Blood and MacConkey agar were aerobically incubated at 37 °C for 27 hours, while the Chocolate agar plates were incubated under anaerobic conditions within a candle jar (7% CO2 atmosphere) at 37 °C for 27 hours. Bacteria were identified using routine standard microbiological methods: culture characters of pure colonies, Gram staining, enzyme production, and biochemical tests. Biochemical tests such as the catalase test, coagulase test, and optochin test were applied for gram-positive bacteria, while carbohydrate tests were applied for gram-negative bacteria [15].
Ethical Approval
The project's ethical permission was approved by the Hadhramout University Ethics Committee. Before any data or specimens were collected, the patient participants were fully informed of the investigation's goals, and they gave their consent to participate in this investigation. In addition, the collected data was treated with confidentiality and was only used for research purposes within the scope of this study.
Statistical Analysis
The obtained data was analyzed using descriptive analyses. The frequency and percentage representations of categorical variables are shown in tables and figures.
Results
Out of 1722 patients enrolled in this study, it was found that 198 (11.49%) eye swabs were positive for bacterial growth in culture media, while 1524 (88.5%) eye swabs were negative (Figure 2).
In this result, it was noticed that the female participants had a higher rate of bacterial conjunctivitis (15.25%) when compared with the males (8.04%), as illustrated in Table 1.
Regarding age group, in general, a higher rate of bacterial conjunctivitis was observed among study subjects ages 31–40 years (29.29%), while the lowest rate was reported among babies younger than one year (2.02%). Additionally, the prevalence rate of bacterial conjunctivitis is significantly greater in males aged between 1 and 10 years (27.78%) compared to other age groups. While the females in the age group of 31–40 years had a higher rate of bacterial conjunctivitis (31.75%) when compared to other age groups (Table 2).
The current findings showed that the gram-positive bacteria were the most isolated from 116 patients (58.59%), while the gram-negative bacteria were isolated from 82 patients (41.41%). S. aureus was the most Gram-positive bacteria at 52 (26.26%), followed by S. pneumoniae 34 (17.18%), Alpha-hemolytic Streptococci 16 (8.08%), and S. epidermidis 14 (7.07%). In addition, P. aeruginosa was the most Gram-negative bacteria observed at 24 (12.1%), followed by Moraxella catarrhalis 20 (10.1%), H. influenzae 14 (7.07%), Klebsiella sp. 12 (6.06%), E. agglomerans 8 (4.04%), and N. gonorrhoeae 4 (2.02%), as shown in Figure 3.
According to signs and symptoms associated with infected eyes, 100% of the study participants had red eyes; 93.93% had a tearing eye; 90.9% of them had itching; 87.87% had painful eyes; 56.56% had purulent eyes; and 38.38% had eye discharge (Table 3).
Discussion
This study is the first to describe the clinical pattern of bacterial conjunctivitis in Hadhramout Governorate. In this study, the prevalence of bacterial conjunctivitis was 11.5% among participants. This result is lower than what was in a previous study that showed the prevalence rate of bacterial conjunctivitis at 14.2% in Nigeria [16], 15.8% in the UK [17], 51.7% in Sana'a, Yemen [14], 60% in Saudi Arabia [18], 69% in Iraq [19], 81.5% in the United Arab Emirate [20], and 80.5% in Iran [21].
The variation in prevalence rate might be due to variations in geographic regions, study population, sample size, racial and ethnic variations, environmental and behavioral patterns, economic status, and the methods of diagnosis used in this study.
Regarding the sex variable, the present finding showed that bacterial conjunctivitis was higher among females (15.25%) compared to males (8.04%). This result is similar to those documented in different countries [22,23,24]. In different statements, males and females have equal natural resistance to bacterial conjunctivitis [2]. Sex has less influence than age on the ocular microbiota composition. In fact, several studies have shown that there is no difference between males and females [25].
The fact that Yemeni customs and traditions obligate women in Yemen to wear the Islamic hijab, which covers their faces during activities outside their homes, may have contributed to the spreading of eye infections. This explains why bacterial conjunctivitis increased among females in this study.
Concerning the age group, study participants aged 31–40 years in this study had the highest rate of bacterial conjunctivitis (29.29%), whilst infants under one year old had the lowest rate (2.02%). The results align with those of other workers who reported that ocular infections are rising with increasing age [24,26,27]. In addition, Wen et al. noticed that older participants had a higher diversity of Shannon index values than younger individuals when analyzing the diversity of the ocular microbiome in people aged 28 to 84 years [28].
In contrast, the United States has a higher incidence of bacterial conjunctivitis in children than in adults; 23% of cases have been reported in children ages 0–2, 28% in children ages 3–9, 13% in children ages 10–19, and 36% in adults [8,29].
Additionally, compared to other age groups, males between the ages of 1 and 10 years had a considerably higher prevalence rate of bacterial conjunctivitis (27.78%). In contrast to other age groups, the females in the 31–40-year-old age group had a greater risk of bacterial conjunctivitis (31.75%). Depending on the age range, different bacteria can cause bacterial conjunctivitis, which affects children significantly more frequently than adults [30,31].
In this finding, gram-positive bacteria were found to be significantly more prevalent in patients than gram-negative bacteria (58.59% vs. 41.41%). This result is in compliance with findings regarding the most common isolated bacteria being gram-positive bacteria [32,33].
In this study, S. aureus was the most common pathogen isolated from participants (26.26%). This result is in consonance with other studies in South Florida [32], the UK [17], Nigeria [34], and Saudi Arabia [33]. The high prevalence of S. aureus in this study indicates that this bacterium is one of the normal resident flora of the conjunctiva, eyelids, and skin in a small number. In addition, this bacterium can spread through hand-to-eye contact or by colonizing nearby mucosal tissues, like the sinus or nasal mucosa [35]. Moreover, the high prevalence of S. aureus in the hospital environment is another reason for its transmission to patients during hospitalization [36,37,38].
These data showed that S. pneumoniae was the second bacteria isolated from study subjects (17.18%), and this is in line with reports [14,33,39]. S. pneumoniae is one of the top three most commonly isolated microorganisms from normal conjunctival flora [40]. S. pneumoniae kills an estimated 317,300 children aged 1–59 months, mostly in lower-income countries [41]. It is responsible for 7–44% of acute conjunctivitis and for 12–20% of conjunctivitis-otitis syndrome [42].
Overall, P. aeruginosa was the third one recovered, and most gram-negative bacteria were detected in the participants’ study (12.1%). This result is in accordance with the results of Cavuoto et al. [32] and Alhazmi et al. [33]. In addition, several studies reported that the proportion rate of P. aeruginosa was reported at 11.4% in Ethiopia [43], 24.2% in Iran [44], 21% in Australia [45], and 20% between 2014 and 2015 in Baghdad [46].
P. aeruginosa is resistant to lens cleaning solutions, where they adhere and spread through the formation of lipid rafts in contact lens users [47]. P. aeruginosa is an opportunistic human pathogen and is a common cause of bacterial keratitis, which is more progressive with large infiltrations and scarring [48]. This type of bacteria has been noticed in several studies conducted among healthcare workers [49,50,51].
The prevalence rate of S. epidermidis was reported at 7.07% in this study. S. epidermidis inhabits the ocular surface, specifically the conjunctival sac [52]. Additionally, high incidences of ocular infection by S. epidermidis have been reported, even in some cases superior to those achieved by S. aureus. The previous reports are considerable because S. epidermidis does not have a variety of virulence factors such as S. aureus [53,54].
Furthermore, the other Gram-negative bacteria recovered in this work were Moraxella catarrhalis (10.1%), H. influenzae (7.07%), Klebsiella sp. (6.06%), E. agglomerans (4.04%), and N. gonorrhoeae (2.02%). In previous studies, H. influenzae and M. catarrhalis had a frequency rate of 61.8% and 19.1%, respectively, in children with infective conjunctivitis [42]. In a study by Bharathi et al. [55] in India, the prevalence of M. catarrhalis, M. lacunata, Haemophilus sp., and Enterobacter sp. was recorded at 53.17%, 63.83%, 25.5%, and 35.7%, respectively. A report by Cavuoto et al. [32] revealed that H. influenzae was the most frequent isolate recovered from patients under 7 years old (59.8%).
The transmission of N. gonorrhoeae occurs when the eyes come into contact with infected genital secretions from a person with genital gonorrhea [56]. H. influenzae is a frequent cause of conjunctivitis in children ages 6–36 months. Children younger than 2 years were the most vulnerable population to this syndrome, and H. influenzae was the most correlative pathogen [57].
The most common symptoms of bacterial conjunctivitis in the current study are red eye, tearing, and itching with 100%, 93.93%, and 90.9%, respectively. Other signs and symptoms include pain, purulent eyes, and eye discharge. A history of infectious conjunctivitis and itch both made the probability of current bacterial involvement less likely [58].
Conclusion
From this study, it can be concluded that the prevalence of bacterial conjunctivitis among patients in the study area is low compared to other countries. S. aureus bacterium was the most predominant as well, and gram-positive cocci are still the most common isolates. Public education regarding eye health is necessary, as is the prompt referral of any occurrences of eye infections to an eye specialist to avoid complications that could result in blindness. Future studies that include a larger population and antibiotic profiles are warranted to provide a better understanding of bacterial conjunctivitis in Hadhramout.
Funding
The authors received no financial support.
Acknowledgments
The author's thanks go to the physicians, nurses, and laboratory technicians in the different governmental and private hospitals in Hadhramout Governorate who have helped them in conducting the study. Finally, yet importantly, they are extremely grateful to the patients for their cooperation with them to undergo the various tests achieved during this study.
Conflict of Interest
The authors declare that they have no competing interests.
References
- G. Høvding, “Acute bacterial conjunctivitis,” Acta Ophthalmologica, 86, 1: 5–17, Feb. 2008. [CrossRef]
- K. K. Y. O. Faao, “Bacterial conjunctivitis (pink eye): practice essentials, background, pathophysiology.”. Available online: https://emedicine.medscape.com/article/1191730-overview#showall.
- C. Beal and B. Giordano, “Clinical evaluation of red eyes in pediatric patients,” Journal of Pediatric Health Care, 30, 5, : 506–514, Sep. 2016. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Pinkeye (Conjunctivitis). January 4, 2019. Available online: https://www.cdc.gov/conjunctivitis/about/causes.html#print.
- J. Epling, “Bacterial conjunctivitis,” BMJ Clin Evid. 2012, 0704. Feb 20;2012.
- K. C. Leung, K. L. Hon, A. H. C. Wong, and A. S. Wong, “Bacterial conjunctivitis in childhood: etiology, clinical manifestations, diagnosis, and management,” Recent Patents on Inflammation & Allergy Drug Discovery, 12, 2: 120–127, Sep. 2018. Sep. [CrossRef]
- Azari and N., P. Barney, “Conjunctivitis,” JAMA, 310, 16; 1721, Oct. 2013. [CrossRef]
- F. Smith and C. Waycaster, “Estimate of the direct and indirect annual cost of bacterial conjunctivitis in the United States,” BMC Ophthalmology, 9, 1, Nov. 2009. [CrossRef]
- W. H. Edrees, “Seroprevalence and risk factors for Helicobacter pylori infection among school students in Sana'a City, Yemen,” Universal J Pharm Res, 7, 2: 67–73, May 15 2022. [CrossRef]
- W. H. Edrees, A. A. Al-Asbahi, W. A. Al-Shehari, and E. A. Qasem, “Vulvovaginal candidiasis prevalence among pregnant women in different hospitals in Ibb, Yemen,” Universal J Pharm Res, 5, 4: 1–5, Sep. 15, 2020. [CrossRef]
- W. H. Edrees, A. A. Anbar, “Prevalence and antibacterial susceptibility of bacterial uropathogens isolated from pregnant women in Sana'a, Yemen,” PSM Biol Res, 5, 4: 157–165, Oct. 31, 2020.
- Al-Halani, A.A.; Edrees, W.H.; Alrahabi, L.M.; Thabit, J.M.; Al-Bahloul, S.M.; Alwashali, F.A.; Al-Qhali, R.M.; Morshed, M.M.; Alـhossainy, A.S.; Al-Maflhi, E.A.; et al. “Prevalence of intestinal parasites, malnutrition, anemia and their risk factors among orphaned children in Sana'a City, Yemen,” Universal J Pharm Res, 8, 2: 32-39. May, 2023. [CrossRef]
- Abdullah, Q.Y.; Al-Helali, M.F.; Al-Mahbashi, A.; Qaaed, S.T.; Edrees, W.H. “Seroprevalence of dengue fever virus among suspected patients in Taiz Governorate-Yemen,” Universal J Pharm Res, 5, 5: 21–26, Nov. 15, 2020. [CrossRef]
- Al-Arosi, S.A.H.; Al-Shamahi, E.Y.; Al-Kholani, A.I.M.; Al-Jawfi, A.Y.; Al-Shamahy, H.A.; A Al-Moyed, K.A.; Al-Ankoshy, A.A.M. “Neonatal bacterial conjunctivitis in tertiary hospitals in Sana'a city, Yemen,” Universal Journal of Pharmaceutical Research, 1, 6, pp: 36-42. Jan. 2022. [CrossRef]
- L. M. De La Maza, M. T. L. M. De La Maza, M. T. Pezzlo, C. E. Bittencourt, and E. M. Peterson, Color Atlas of Medical Bacteriology. Third Edition. John Wiley and Sons, 2020.
- Adegbehingbe and, A. Onipede, “Conjunctivitis as seen in Ile-Ife,” Nigerian Journal of Ophthalmology, 13, 1, Oct. 2005. [CrossRef]
- Silvester, A.; Neal, T.; Czanner, G.; Briggs, M.; Harding, S.; Kaye, S. “Adult bacterial conjunctivitis: resistance patterns over 12 years in patients attending a large primary eye care centre in the UK,” BMJ Open Ophthalmology, 2016;1:e000006. [CrossRef]
- Faraz, and M. A. Farhan, “Microbial etiology of neonatal conjunctivitis in a general hospital in Saudi Arabia,” Al-Shifa J Ophthalmol, 15, 1: 30-34, Jan–Mar. 2019.
- A. S. Al-Atrushi, and A. Al-Brefkani, “Ophthalmia neonatorum in Duhok, north of Iraq: bacterial causative agents and their antibiotic sensitivity pattern,” Isra Med J, 4, 4, pp; 09-213, Dec 2012.
- Nsanze, H.; Dawodu, A.; Usmani, A.; Sabarinathan, K.; Varady, E. “Ophthalmia neonatorum in the United Arab Emirates,” Annals of Tropical Paediatrics, 16, 1, pp; 27-32, Mar, 1996.
- Afjeiee, S.A.; Tabatabaei, S.R.; Fallah, F.; Fard, A.T.; Shiva, F.; Adabian, S.; Karimi, A.; Rahbar, M. , “A microbiological study of neonatal conjunctivitis in two hospitals in Tehran, Iran,” Asian Pacific Journal of Tropical Disease, 3, 6: 429–433, Dec. 2013. [CrossRef]
- K. Sehgal, L. K. Sehgal, L. Kant, B. K. Jain, and K. Lal, “Prevalence of eye diseases in a semi-urban area,” Indian J Public Health, 28, 4: 189-93. Oct-Dec. 1984. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. ; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: global and regional exposures and health consequences,” The Lancet, 371, 9608: 243–260, Jan. 2008. [CrossRef]
- G. N. Rao, S. G. N. Rao, S. Sabnam, S. Pal, H. Rizwan, B. Thakur, and A. Pal, “Prevalence of ocular morbidity among children aged 17 years or younger in the eastern India,” Clinical Ophthalmology, 12: 1645–1652, Sep. 2018. [CrossRef]
- Petrillo, F.; Pignataro, D.; Lavano, M.A.; Santella, B.; Folliero, V.; Zannella, C.; Astarita, C.; Gagliano, C.; Franci, G.; Avitabile, T.; et al. “Current evidence on the ocular surface microbiota and related diseases,” Microorganisms, 8, 7; 1033, Jul. 2020. [CrossRef]
- Kumar, R.; Mehra, M.; Dabas, P.; Raha, R. A study of ocular infections amongst primary school children in Delhi,” J Commun Dis, 36, 2; 121–126, 2004.
- A, Subramanian, and S, Yessaian, “Screening and antibiogram pattern of bacterial ophthalmic infections,” Int J Pharm Pharm Sci, vol 7, 1; 412-415, 2014.
- Wen, X.; Miao, L.; Deng, Y.; Bible, P.W.; Hu, X.; Zou, Y.; Liu, Y.; Guo, S.; Liang, J.; Chen, T.; et al. “The Influence of age and sex on ocular surface microbiota in healthy adults,” Investigative Opthalmology and Visual Science, 58, 14; 6030, Dec. 2017. [CrossRef]
- S. J. Lichtenstein and M. Rinehart, “Efficacy and safety of 0.5% levofloxacin ophthalmic solution for the treatment of bacterial conjunctivitis in pediatric patients,” Journal of American Association for Pediatric Ophthalmology and Strabismus, 7, 5: 317–324, Oct. 2003. [CrossRef]
- K. M. Cavuoto, R. K. M. Cavuoto, R. Mendez, D. Miller, A. Galor, and S. Banerjee, “Effect of clinical parameters on the ocular surface microbiome in children and adults,” Clinical Ophthalmology, 12: 1189–1197, Jul. 2018. [CrossRef]
- M. F. Hashmi, “Conjunctivitis,” StatPearls - NCBI Bookshelf, Dec. 06, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541034/.
- K. Cavuoto, D. K. Cavuoto, D. Zutshi, C. L. Karp, D. Miller, and W. Feuer, “Update on bacterial conjunctivitis in South Florida,” Ophthalmology, 115, 1: 51–56, Jan. 2008. [CrossRef]
- Alhazmi, A.; Abuallut, I.; Alwadani, I.; Haddad, M.; Ageeli, B.; Majrabi, H.; Muslihi, I.; AlAli, L.; Homadi, H.; Madkhli, E.; et al. “Neonatal Healthcare-Associated Conjunctivitis: A Descriptive Study from Saudi Arabia,” Medicina, 58, 10, p. 1448, Oct. 2022. [CrossRef]
- Ogunfowora, O.; Ajewole, J.; Ajibode, H. “Conjunctival bacterial infection among hospitalized neonates,” Annals of Health Research, 6, 2: 230–238, May 2020. [CrossRef]
- R. O’Callaghan, “The pathogenesis of Staphylococcus aureus eye infections,” Pathogens, 7, 1, p. 9, Jan. 2018. [CrossRef]
- Alhlale, M.F.; Humaid, A.; Saleh, A.H.; Alsweedi, K.S.; Edrees, W.H. “Effect of most common antibiotics against bacteria isolated from surgical wounds in Aden Governorate hospitals, Yemen,” Universal J Pharm Res, 5, 1: 21–24, Mar. 08, 2020. [CrossRef]
- Al-Khawlany, R.S.; Edrees, W.H.; AL-Jaufy, A.Y.; Nasher, M.A.; Al-Shehari, W.A.; Reem, A.; Almezgagi, M.M. “Prevalence of methicillin-resistant Staphylococcus aureus and antibacterial susceptibility among patients with skin and soft tissue infection at Ibb City, Yemen,” PSM Microbiol, 6, 1: 1–11, Mar. 31, 2021. Available online: https://psmjournals.org/index.php/microbiol/article/view/535.
- Edrees, W.H. Antibacterial susceptibility and Sider honey activity against isolated bacteria from wound patients attending at Al-Gmohori hospital in Hajja City, Yemen,” Al-Razi Univ J Med Sci; 5, 2: 1–8, Juan, 30, 2021. [Google Scholar]
- N. Buznach, R. N. Buznach, R. Dagan, and D. Greenberg, “Clinical and bacterial characteristics of acute bacterial conjunctivitis in children in the antibiotic resistance era,” The Pediatric Infectious Disease Journal, 24, 9: 823–828, Sep. 2005. [CrossRef]
- H. Tao, J. H. Tao, J. Wang, L. Li, H.-Z. Zhang, M.-P. Chen, and L. Li, “Incidence and antimicrobial sensitivity profiles of normal conjunctiva bacterial flora in the central area of China: A Hospital-based study,” Frontiers in Physiology, 8, 17 May 2017. [CrossRef]
- Wahl, B.; O’Brien, K.L.; Greenbaum, A.; Majumder, A.; Liu, L.; Chu, Y.; Lukšić, I.; Nair, H.; McAllister, D.A.; Campbell, H. “Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000–15,” The Lancet Global Health, 6, 7: e744–e757, Jul. 2018. [CrossRef]
- Sugita, G.; Hotomi, M.; Sugita, R.; Kono, M.; Togawa, A.; Yamauchi, K.; Funaki, T.; Yamanaka, N. “Genetic characteristics of Haemophilus influenzae and Streptococcus pneumoniae isolated from children with conjunctivitis-otitis media syndrome,” Journal of Infection and Chemotherapy, 20, 8: 493–497, Aug. 2014. [CrossRef]
- T. Tesfaye, G. T. Tesfaye, G. Beyene, Y. Gelaw, S. Bekele, and M. Saravanan, “Bacterial profile and antimicrobial susceptibility pattern of external ocular infections in Jimma University Specialized Hospital, Southwest Ethiopia,” American Journal of Infectious Diseases and Microbiology, 1, 1: 13–20, Jan. 2013.
- D. Khosravi, M. D. Khosravi, M. Mehdinejad, and M. Heidari, “Bacteriological findings in patients with ocular infection and antibiotic susceptibility patterns of isolated pathogens,” Singap Med J, 28, 8: 741–743, 2007.
- Ly, C.N.; Pham, J.N.; Badenoch, P.R.; Bell, S.M.; Hawkins, G.; Rafferty, D.L.; A McClellan, K. “Bacteria commonly isolated from keratitis specimens retain antibiotic susceptibility to fluoroquinolones and gentamicin plus cephalothin,” Clinical and Experimental Ophthalmology, 34, 1: 44–50, Jan. 2006.
- S. Jebur, A. H. S. Jebur, A. H. Al-Hamadani, and J. Sh, “Evaluation of genetic study and bacterial culture for diagnosis of Pseudomonal eye infections,” Int J Curr Microbiol App Sci, 4, 3: 348–56, 2015.
- R. Henry, H. W. R. Henry, H. W. Flynn, D. Miller, R. K. Forster, and E. C. Alfonso, “Infectious keratitis progressing to endophthalmitis,” Ophthalmology, 119, 12: 2443–2449, Dec. 2012. [CrossRef]
- M. Teweldemedhin, H. M. Teweldemedhin, H. Gebreyesus, A. H. Atsbaha, S. W. Asgedom, and M. Saravanan, “Bacterial profile of ocular infections: a systematic review,” BMC Ophthalmology, Nov. 25, 2017. [CrossRef]
- Al-Haik, W.M.; Al-Haddad, A.M.; Al-Kaf, A.G.; Edrees, W.H. Antimicrobial activities for hadhrami honey on growth of some pathogenic bacteria,” Universal J Pharm Res, 2, 6: 7–12, Jan. 15, 2018. [CrossRef]
- . Alhlale, F.M. The inhibitory effect of Euphorbia hirta extracts against some wound bacteria isolated from Yemeni patients,” COPS, 3, 2: 780–786, Jan. 23, 2019.
- W. H, Edrees, and S. M. Al-Awar. Bacterial contamination of mobile phones of medical laboratory workers at Sana’a city, Yemen and their antimicrobial susceptibility. JPPRes. 2020, 8, 6: 591–599. [Google Scholar]
- Zhang, Y.; Liu, Z.-R.; Chen, H.; Fan, Y.-C.; Duo, J.; Zheng, H.; Wang, G.-J.; Li, Y.-C.; Jiachu, D.-B.; Zewang, G.-M. Comparison on conjunctival sac bacterial flora of the seniors with dry eye in Ganzi autonomous prefecture,” Int J Ophthalmol, 6, 4: 452–457. 2013.
- Moloney, T.P.; Park, J. Microbiological isolates and antibiotic sensitivities in culture-proven endophthalmitis: a 15-year review,” British Journal of Ophthalmology, 98, 11: 1492–1497, Jun. 2014. [CrossRef]
- Flores-Páez, L.A.; Zenteno, J.C.; Alcántar-Curiel, M.D.; Vargas-Mendoza, C.F.; Rodríguez-Martínez, S.; Cancino-Diaz, M.E.; Jan-Roblero, J.; Cancino-Diaz, J.C. Molecular and phenotypic characterization of Staphylococcus epidermidis isolates from healthy conjunctiva and a comparative analysis with isolates from Ocular Infection,” PLOS ONE, 10, 8; e0135964, Aug. 2015. [CrossRef]
- Mj. Bharathi, R. Mj. Bharathi, R. Ramakrishnan, C. Shivakumar, R. Meenakshi, and D. Lionalraj, “Etiology and antibacterial susceptibility pattern of community-acquired bacterial ocular infections in a tertiary eye care hospital in south India,” Indian Journal of Ophthalmology, 58, 6; 497, 2010. [CrossRef]
- J. Costumbrado, “Gonococcal Conjunctivitis,” StatPearls - NCBI Bookshelf, Sep. 12, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459289/#:~:text=Gonococcal%20conjunctivitis%20.
- Hu, Y.L.; Lee, P.I.; Hsueh, P.R.; Lu, C.Y.; Chang, L.Y.; Huang, L.M.; Chen, J.M. Predominant role of Haemophilus influenzae in the association of conjunctivitis, acute otitis media and acute bacterial paranasal sinusitis in children,” Scientific Reports, 11, 1, Jan. 2021.
- R. P. Rietveld, G. R. P. Rietveld, G. ter Riet, P. J. E. Bindels, J. H. Sloos, and H. C. P. M. van Weert, “Predicting bacterial cause in infectious conjunctivitis: cohort study on informativeness of combinations of signs and symptoms,” BMJ, 329, 7459: 206–210, Jun. 2004.
Figure 1.
Map of Yemen indicating the study area in Hadhramout governorate.
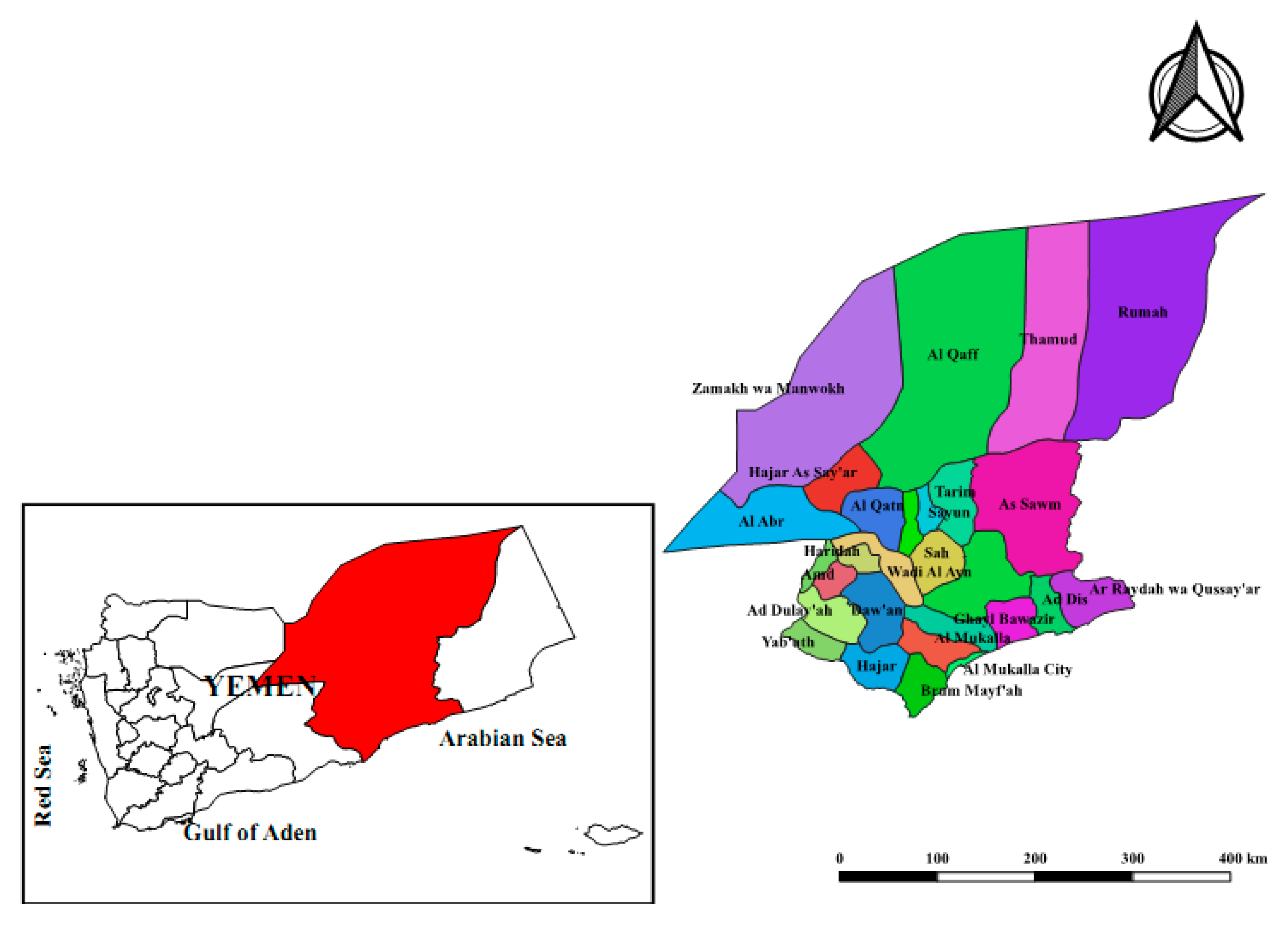
Figure 2.
Prevalence rate of bacterial conjunctivitis.
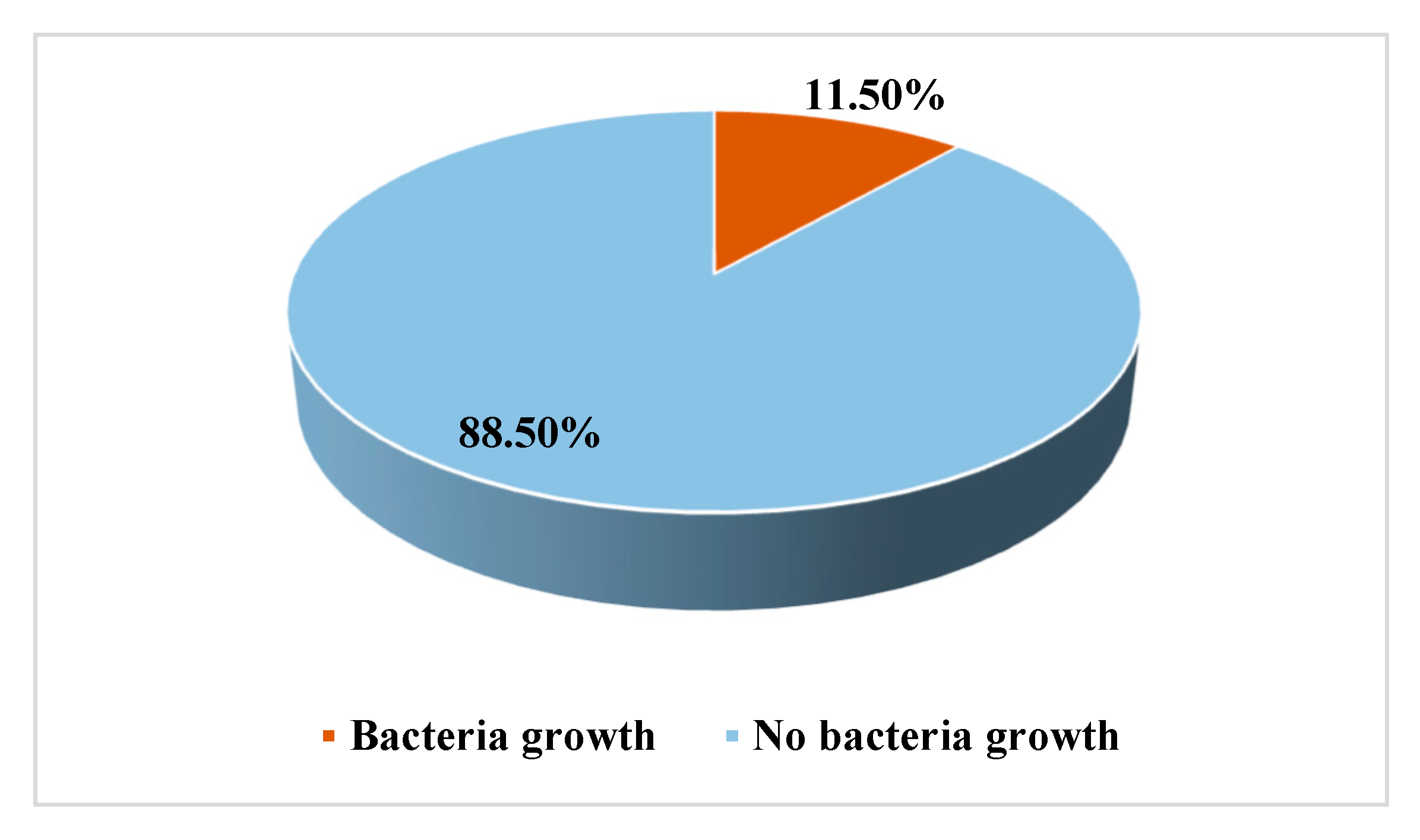
Figure 3.
Frequency of bacterial species among infected patients with conjunctivitis.
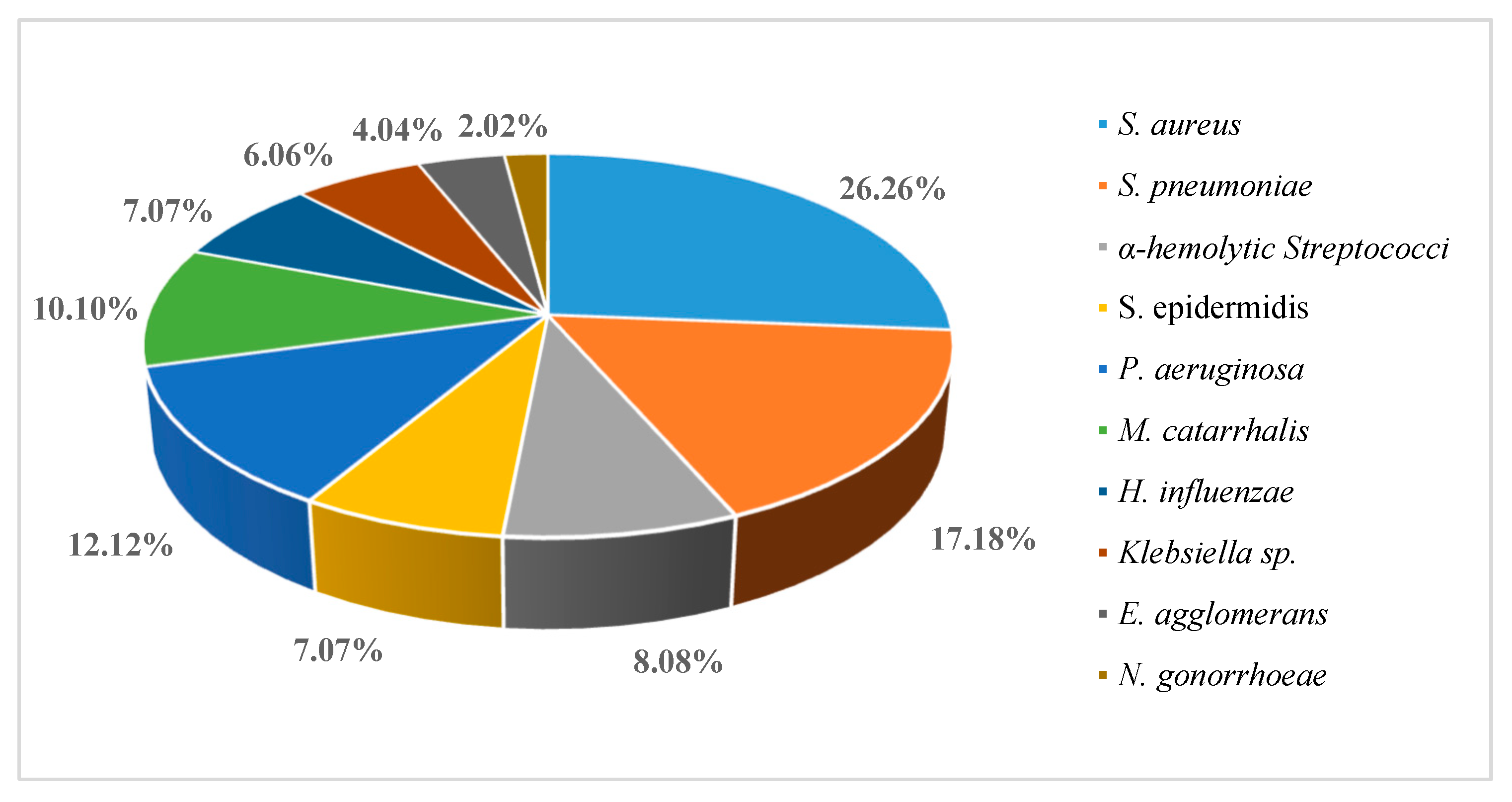

Table 1.
Frequency of bacterial conjunctivitis according to gender.
| Gender | Examined | Infected | Non-infected | ||
|---|---|---|---|---|---|
| No. (%) | No | Rate (%) | No | Rate (%) | |
| Male | 896 (52.03) | 72 | 8.04 | 824 | 91.96 |
| Female | 826 (47.97) | 126 | 15.25 | 700 | 84.75 |
| Total | 1722 | 198 | 11.50 | 1524 | 88.5 |
Table 2.
Frequency of bacterial conjunctivitis concerning age group and gender.
| Age (years) | Patients (n=198) | Male (n=72) | Female (n=126) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No | (%) | No | (%) | No | (%) | ||||
| <1 | 4 | 2.02 | 0 | 0 | 4 | 3.17 | |||
| 1-10 | 42 | 21.21 | 20 | 27.78 | 22 | 17.46 | |||
| 11-20 | 26 | 13.13 | 10 | 13.89 | 16 | 12.70 | |||
| 21-30 | 36 | 18.19 | 14 | 19.44 | 22 | 17.46 | |||
| 31-40 | 58 | 29.29 | 18 | 25.0 | 40 | 31.75 | |||
| 41-50 | 8 | 4.04 | 0 | 0.0 | 8 | 6.35 | |||
| >50 | 24 | 12.12 | 10 | 13.89 | 14 | 11.11 | |||
Table 3.
Frequency of bacterial conjunctivitis concerning signs and symptoms.
| Variables | Cases (n=198) | Percentage % |
|---|---|---|
| Red eye | 198 | 100 |
| Tearing | 186 | 93.93 |
| Itching | 180 | 90.9 |
| Pain | 174 | 87.87 |
| Purulent eye | 112 | 56.56 |
| Eye discharge | 76 | 38.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



