
Submitted:
16 November 2023
Posted:
16 November 2023
You are already at the latest version
Abstract
The increase in incidence of superficial fungal infections combined with the emergence of antifungal resistance represents both a global health challenge and a considerable economic burden. Recently, dermatophytes, the main culprit causing superficial fungal infections, have started to exhibit antifungal resistance. This can be observed in some of the most common species such as Trichophyton rubrum and Trichophyton mentagrophytes. Importantly, the new subspecies, known as Trichophyton indotineae, has been reported to show high resistance to terbinafine, a first-line treatment for dermatophyte infections. Compounding these issues is the realization that diagnosing the causative infectious agents requires using molecular analysis that goes beyond the conventional macroscopic and microscopic methods. These findings emphasize the importance of conducting antifungal susceptibility testing to select the appropriate antifungal necessary for successful treatment. Implementing these changes may improve clinical practices that combat resistant dermatophyte infections.
Keywords:
Incidence
; Terbinafine
; Dermatophytes
; Trichophyton
; T. rubrum
; T. mentagrophytes
; T. indotineae
; Superficial Fungal Infection
1. Introduction
Superficial fungal infections (SFIs) affect approximately 20 to 25 percent of the global population [1]. They can result in a myriad of dermatologic clinical presentations depending on both the organism involved and the area of the body affected [1]. Factors such as age, gender, and geographical location play an important role in the prevalence of these infections [2]. In a 2004 study in partnership with the American Academy of Dermatology, the prevalence of SFIs was reported to be 29.4 million cases. Between 1995 and 2004 there have been approximately 51 million patient visits for these infections [3,4]. Furthermore, between the years of 2005 and 2014, dermatophyte infections were responsible for 4,981,444 outpatient visits in the United States as reported by the Centers for Disease Control and Prevention (CDC). Moreover, the direct medical cost caused by these infections was approximately $845 million dollars in 2019. The worldwide increased incidence of fungal infections and growing trend of resistant organisms have attracted global concern [5,6]. While the exact reason behind this trend is still under investigation, many factors have been reported as potential contributors, such as genetics, environmental factors, and antifungal resistance [5,6].
2. Epidemiology of Dermatophyte Infections
Dermatophytes are the most prevalent pathogenic fungi in the United States and amongst the most common causes of skin diseases worldwide [7]. They belong to three genera: Trichophyton, Epidermophyton, and Microsporum [8]. There are over 40 species of dermatophytes known to infect humans, primarily causing SFIs [9]. As a keratinophilic fungus (i.e., exhibiting affinity to keratin), dermatophytes infect the keratin structures of the skin, hair, and nails, resulting in an inflammatory host response and clinical conditions known as tinea [10]. These dermatophytes can also colonize human hosts without causing disease [9]. While the prevalence of dermatophyte species varies around different regions of the world, Trichophyton rubrum is responsible for the majority of dermatophyte-associated infections reported [11,12].
As dermatophytes thrive in hot, humid environments, many tropical and developing countries are facing an increase in dermatophyte infections [5]. Specifically, India has encountered an enormous challenge due to an alarming increase in the number of chronic and recurrent dermatophyte infections. The tropical and subtropical climate of the country is particularly favorable for dermatophytes [11]. Furthermore, overcrowding, shared living spaces, and urbanization are all contributing factors to the increasing prevalence of dermatophytosis [12]. In addition to the rapidly rising rate of infection, treatment efficacy has been sub-optimal due to a lack of antifungal stewardship in clinical practice [13]. Importantly, it is essential to consider non-dermatophyte molds as causative organisms as well, especially in treatment-resistant conditions. These molds are commonly found in African and Asian countries, as well as the Caribbean islands, Central America, South America, and parts of the United States [14]. T. mentagrophytes has been reported to be the most common cause of tinea infection in India, followed by T. rubrum and T. interdigitale [12]. While in North America and Europe, T. rubrum is the most common dermatophyte pathogen implicated in tinea, closely followed by T. interdigitale [15].
T. rubrum has been reported to be the main cause for chronic dermatophytosis infection [16]. A reason for this could be the uncontrolled use of antifungal medications, which can result in a selective pressure allowing a resistant strain to prevail within a population. In one study, T. rubrum was shown to develop resistance to fluconazole and itraconazole upon prolonged drug exposure. Analysis of minimum inhibitory concentration (MIC) values confirmed the inclination of T. rubrum to acquire resistance against fluconazole when compared to itraconazole. This study also reported patterns of cross-resistance between these two azole antifungals. The underlying mechanisms that can contribute to the development of T. rubrum resistance include increased drug efflux, decreased drug uptake, structural target site modifications, and the production of biofilms [17].
T. tonsurans, on the other hand, was initially native to Southeast Asia and Australia, but quickly expanded to the rest of the world through colonization, migration, and sports-related travel. T. tonsurans can live on household items and easily transmit infection through shared objects [18]. Interestingly, the prevalence of T. tonsurans is now increasing worldwide. In the United States, T. tonsurans is the primary cause of tinea capitis [19]. Additionally, in Germany, there is presently an increasing prevalence of tinea capitis caused by T. tonsurans and fellow anthropophilic pathogens T. violaceum and T. soudanense [20]. One possible explanation for this is the inadequate treatment of infections such as tinea capitis. For example, using griseofulvin, which is more effective at inhibiting Microsporum spp. than Trichophyton spp., in management of such cases may result in treatment failure, chronicity, and spread of infection [21].
3. Clinical Perspectives of Tinea
From a clinical perspective, dermatophyte infection, known as tinea, is further classified based on the anatomical region of the body affected (Table 1) [6]. Additionally, tinea infections can be transmitted from both humans and pets [22]. T. tonsurans and Microsporum canis are mainly known to cause tinea capitis infections [9]. Furthermore, tinea corporis (ringworm) is most commonly caused by T. rubrum, T. mentagrophytes, and T. tonsurans [23]. Tinea corporis can also be caused by contact with infected pets, though, the most common causative organism in this scenario is M. canis [22]. T. rubrum is the most common cause of tinea cruris (jock itch) around the globe, though T. mentagrophytes infections have been increasing in certain areas [24,25,26]. Trichophyton organisms have been found to affect male and female children equally. However, M. canis more commonly affects males [22]
Similarly, onychomycosis is commonly caused by dermatophytes (60-70% of the cases) and less commonly by other non-dermatophytes (mold and yeast). Several studies have shown that the majority of onychomycosis cases are caused by T. rubrum followed by T. mentagrophytes [27,28]. Interestingly, in a study conducted in Iran that included 1,284 microscopically positive onychomycosis cases, the main causative organism was Candida albicans. This was followed by Trichophyton interdigital and Aspergillus flavus. This may suggest a regional factor that can affect the prevalence of this type of infection [29].
The socioeconomic status of individual countries was reported to have an impact on the type of dermatophyte infection encountered in clinical practice. For example, tinea capitis is more prevalent in developing countries, while the prevalence of tinea pedis and onychomycosis is higher in developed countries [30]. Tinea pedis is a common fungal infection seen worldwide, with the most prevalent dermatophytes isolated in these cases being T. rubrum, T. mentagrophytes, and Epidermophyton floccosum [16,33,34,35]. This infection has been growing over recent years, yet the underlying pathogenesis is not definitively known [31,32]. However, tinea pedis was shown to be more prevalent in the adult-aged population, especially in males [33,34]. While tinea pedis and onychomycosis are prevalent around the globe, these infections are less common in India and rural Africa [35].
In the United States and the United Kingdom, T. tonsurans is the most common causative organism of tinea capitis infection [36,37]. Additionally, T. tonsurans can cause a type of tinea corporis infection known as tinea gladiatorum, which is common in athletes participating in direct contact sports, such as wrestlers. The average prevalence of tinea gladiatorum among wrestlers in the United States, Iran, and Turkey is 34.29% [18].
4. Standard Treatment of Tinea Infections and Current Limitations
The standard treatment of tinea infections is largely topical with azoles or allylamines. Tinea capitis and onychomycosis are more difficult to treat and typically require systemic oral therapy. Systemic therapy may also be utilized in chronic, refractory, or severe tinea infections (Table 2).
Medications that are commonly used to treat infections caused by T. rubrum include terbinafine, itraconazole, amorolfine, and ciclopirox [38]. Terbinafine, available as both a topical and oral medication, has long been a standard drug of choice for the treatment of tinea infections [39]. The topical form is available as terbinafine 1% cream and is used as the first line treatment for most tinea corporis, tinea cruris, and tinea pedis infections [6]. On the other hand, oral therapy is mainly used for more resistant conditions such as tinea capitis and onychomycosis, or for areas of extensive skin infection. This is especially true for patients who fail topical therapy or are immunocompromised [40]. In adults, oral terbinafine 250-mg once daily is the recommended first line treatment for onychomycosis. Itraconazole and fluconazole, available as oral medications, are other alternatives used as second line agents for conditions that require systemic treatment [6].
In a Cochrane review conducted in 2017, comparing a terbinafine treatment group to an azole treatment group, terbinafine was shown to be more effective at treating onychomycosis compared to azoles. Additionally, both groups had similar adverse reactions of headache, nausea, and viral infection [41]. For terbinafine, the side effects that are commonly observed include GI disturbance, headache, and taste alteration [42]. Hepatotoxicity, while rare, is a potentially life-threatening complication of both terbinafine and itraconazole [42,43]. Beside the above complications, drug-drug interactions may influence serum itraconazole levels and must be acknowledged before prescribing the medication [44].
The FDA has only approved oral terbinafine and itraconazole for the treatment of onychomycosis. However, fluconazole is also used as an off-label alternative treatment for onychomycosis. Pulse dosing regimens and booster therapy may also be utilized in the treatment approach, particularly with itraconazole. On the other hand, for topical treatments, only ciclopirox 8% nail lacquer, efinaconazole 10% solution, and tavaborole 5% solution have been approved by the FDA for management of onychomycosis [45].
5. Treatment Failure and Diagnostic Challenges
Numerous factors may contribute to treatment failure of SFIs including misdiagnosis, inappropriate use of antifungals, and the development of antifungal resistance. Recurrent chronic dermatophytosis may result from intra-familial infection, prior history of inappropriate corticosteroid use, low treatment compliance, or premature treatment termination. Poor hygiene practices such as infrequent bathing, changing of undergarments, and washing of clothing, as well as sharing items like footwear, towels, and bedsheets, have also been noted as potential contributing factors to persistent infection. Dermatophytes can easily spread in the home environment, and it is important to recognize that asymptomatic carriers may transmit infection as well [12,46]. One study by Ghannoum et al. investigated the transmission of dermatophyte infection among infected households utilizing molecular typing and found that 44% of the investigated households had intra-familial transmission of infection [46].
Many dermatologic conditions may mimic tinea infections, thus, adequate diagnosis of dermatologic presentations is crucial for appropriate treatment, especially when considering systemic therapy [40]. For example, non-dermatophyte infections of the skin folds, such as cutaneous candidiasis, may mimic those of dermatophytes; however, they both have different treatments. Topical treatment with clotrimazole or miconazole for these infections is preferred over terbinafine [47,48]. Moreover, the actual dermatologic condition could be something else other than infection. This can be observed with some types of tineas, such as tinea corporis, which may present similar to other conditions including atopic dermatitis, discoid eczema, annular psoriasis, pityriasis rosea, subacute cutaneous lupus erythematosus, and erythema annulare centrifugum [49,50]. In this scenario, tinea infections may be treated inappropriately with topical corticosteroids or immunosuppressive drugs. This event is referred to as tinea incognito [40]. Corticosteroids can initially suppress the inflammation of tinea infections; however, this is only temporary and most often leads to further inflammation and flare of disease [12].
In recurrent infections, it is important for providers to consider potential dermatophyte reservoirs elsewhere on the body and perform a full skin examination, as a single infection can easily be spread among one host. For example, onychomycosis can further spread to the foot, resulting in tinea pedis, while also spreading to the hand, trunk, and groin. Additionally, animals and household pets may also serve as dermatophytes hosts and should be considered in the treatment approach, especially when considering infection by M. canis [40].
Onychomycosis can also be confused with other conditions such as psoriasis, lichen planus, subungual melanoma, and bacterial infections [51]. Thus, generally, utilization of the available laboratory test to properly identify dermatophyte infections is advisable.

Table 2.
Clinical Viewpoints: Systemic and Local Therapies for Tinea Infections.
| Tinea Infection | Systemic Therapy | Local Therapy |
|---|---|---|
| Tinea Capitis [22] |
Terbinafine or Griseofulvin. If kerion is present, add steroids. | Not recommended. Itraconazole or Fluconazole may be used in some cases. |
| Tinea Corporis [52,53] |
Indicated for severe infection caused by T. rubrum. Terbinafine, Itraconazole, Fluconazole, or Griseofulvin. Terbinafine is indicated for Majocchi Granuloma. | Azoles or Allylamines. |
| Tinea Cruris [25,54] |
Indicated for chronic or recurrent infection. Terbinafine, Itraconazole, or Fluconazole. | Azoles or Allylamines. |
| Tinea Faciei [55,56] |
Indicated for severe or refractory infection or involvement of vellus hair. |
Azoles or Allylamines. |
| Tinea Barbae [57] |
Terbinafine, Itraconazole, Fluconazole, or Ketoconazole. |
Azoles or Allylamines as adjunct therapy. |
| Tinea Manuum [26,58,59] |
Indicated for co-infection of the nail, two feet-one hand syndrome, and chronic or recurrent infection. Terbinafine or Itraconazole may be effective. |
Azoles or Allylamines. |
| Tinea Pedis [6,60,61,62,63] |
Indicated for treatment-resistant infection. Terbinafine, Itraconazole, Fluconazole, Ketoconazole, or Griseofulvin. |
Indicated for uncomplicated or mild interdigital infection. Azoles or Allylamines. Luliconazole or Naftifine may be used for inter- digital infection. Initial treatment with topical corticosteroids may be beneficial. |
| Onychomycosis (Tinea Unguium) [64,65,81,82,83,84] |
Indicated for moderate to severe infection. Terbinafine or Itraconazole. Avoid Griseofulvin (lower efficacy) and Ketoconazole (hepatotoxicity). |
Indicated for mild to moderate infection. Efinaconazole, Ciclopirox, or Amorolfine. |
6. Emergence of Drug Resistant Organisms
A factor that contributes to the observed increase in the incidence of dermatophyte infections is the development of antifungal resistance. Recently, there has been an increasing emergence of antifungal-resistant dermatophyte infections across the globe [66]. This resistance was initially noted in India but has also now been reported in parts of Europe [67]. Additionally, similar observations from other countries such as Iran, Japan, and China have been also reported [12,68,69], as well as recently in the United States [70,71]. The predominant causative dermatophyte for these infections has been reported to be T. mentagrophytes genotype VIII, recently designated T. indotineae.
Resistance to terbinafine, one of the most utilized antifungals, has been reported throughout the literature over the past decade. Terbinafine, a first-line treatment for dermatophytosis, acts by inhibiting the enzyme squalene epoxidase. This enzyme is responsible for the synthesis of ergosterol, which is a necessary component of the fungal cell membrane (Figure 1). In refractory dermatophytosis, terbinafine resistance has been attributed to a point mutation in the squalene epoxidase gene [15]. The F397L and L393F point mutations have been detected in terbinafine-resistant T. rubrum and T. mentagrophytes strains [72]. Similarly, in Delhi, India, a case series evaluating tinea cruris and tinea corporis patients analyzed twenty T. interdigitale strains and reported elevated MIC values for terbinafine. All strains were also reported to have a squalene epoxidase point mutation at either F397L or L393F [66]. These mutations have additionally been reported in another study conducted in Denmark, in which isolates obtained from 14 cases demonstrated resistance to terbinafine. The T. rubrum and T. interdigitale isolates reported in this study also harbored additional squalene epoxidase point mutations such as L393S, F415S, H440Y F484Y and I121M V237I [73].
The Ser395Pro (TCT → CCT) point mutation and amino acid substitution are also common in terbinafine-resistant dermatophytes [73]. In Lausanne, Switzerland over 2,000 Trichophyton strains were evaluated for terbinafine resistance. One percent of these strains demonstrated decreased sensitivity to terbinafine. These isolates were found to carry squalene epoxidase point mutations with a single amino acid substitution at four locations: Leu393, Phe397, Phe415 and His440 [75]. These mutations have also been detected in T. Indotineae isolates as reported by Singh et al. [76]. Additional mutations that have been associated with T. indotineae include Ala448Thr amino acid substitution in erg1. The two tested isolates in that study exhibited an intermittent drug response to terbinafine [77].
7. The Impact of Increasing Trends of Fungal Infections and Growing Antifungal Resistance
The rising number of fungal infections and increasing antifungal resistance are becoming a major global health challenge and an economic burden. Every year, fungal infections result in over 1.5 million deaths worldwide. Mortality is higher in those who are immunocompromised, which is concerning due to the expanding immunocompromised patient population [78].
As for economic costs, fungal infections have become a significant global expense. In 2018, the United States spent approximately $6.7 billion in costs associated with fungal infections [78]. Fungal infections caused by dermatophytes alone account for at least $500 million in healthcare costs [9]. An important aspect likely contributing to the high costs associated with fungal infections is a lack of efficacious treatment. One study by Panackal et al. performed a cross-sectional analysis of ambulatory visits within the United States and reported that polyenes, while ineffective at treating tinea infections, were prescribed by physicians in significant amounts. This indicates a potential need for further provider education on the treatment of dermatophytosis [3].
Dermatophytosis has previously been associated with lower socioeconomic status. Racial differences have also been reported, with Black patients having a higher incidence of some tinea infections [3]. As infections continue to rise, the racial and economic disparities associated with dermatophytosis will only increase. Multiple studies have reported the disparity of tinea capitis disproportionately affecting Black adolescents [3,79,80]. One of these studies additionally reported that children in lower socioeconomic strata were also disproportionately affected by tinea capitis [3].
8. Management Prospective and Alternative Treatments
To address management of SFIs, there is a need for proper identification of the organism causing the infection. Furthermore, development of rapid laboratory assays that can detect the terbinafine resistant mutations can aid in drug selection and reduce the incidence of treatment failure.
Several treatment options have been studied over the past years including newer azoles, such as efinaconazole, luliconazole, and tavaborole, a class of drugs known as oxaborole antifungals. Additionally, other alternative treatments, such as laser therapy, are currently being tested for the treatment of SFIs.
Efinaconazole is a triazole used in the treatment of onychomycosis as a topical 10% solution [81,82,83,84]. Conversely, luliconazole is an imidazole that is available as a 1% topical cream [85]. Efinaconazole has been shown to be effective in treating onychomycosis and may be more effective than other comparable antifungals due to its activity against a wide variety of superficial fungal pathogens [84,86]. It is applied once daily to the affected toenail(s) for 48 weeks. In vitro and in vivo studies have shown efinaconazole to be effective against T. rubrum and T. mentagrophytes isolates with MIC values of 0.06 μg/mL or less against ≥ 90% of the tested isolates [86].
Luliconazole has also demonstrated potent activity against dermatophytes. In a study by Wiederhold et al., luliconazole had a geometric mean MIC of 0.00022 μg/mL against 320 clinical isolates, compared to 0.0194 to 0.3107 μg/mL observed with amorolfine, ciclopirox, and terbinafine [87]. Furthermore, it demonstrated good activity in the treatment of dermatophytosis compared to terbinafine [88].
Tavaborole is another promising topical agent that can be used for the treatment of onychomycosis [89]. Tavaborole has shown activity in eliminating the fungal infection in clinical trials [90,91,92,93,94]. In two phase 3 clinical trials, tavaborole achieved a 6-9% complete cure rate [95]. Additionally, in a phase 4 trial, following 52 weeks of treatment, 14.9% of the patients achieved a complete/almost complete cure [94].
Alternative treatments for onychomycosis have included diode, erbium glass, carbon dioxide, and Neodymium-doped Yttrium Aluminum Garnet (Nd:YAG) laser treatments [96]. Laser therapy with a Nd:YAG 1064nM laser may be a promising treatment modality in diabetic patients [97]. However, laser therapy overall has not been shown to be as effective as traditional topical or oral treatments [98]. While they have fungicidal effects, lasers have lower cure rates and require a long duration of treatment with multiple sessions. Additionally, laser therapy may be painful for some patients and is a costly financial investment. Ultimately, laser therapy is not recommended as a first line treatment [45]. Looking forward it is necessary to recognize the importance of both antifungal stewardship and susceptibility testing to improve patient outcomes and combat growing antifungal resistance.
9. Conclusion
It is evident that an increasing number of antifungal-resistant dermatophyte infections are posing a major global health and economic challenge, in combination with the growing number of non-dermatophyte fungal infections. Moving forward, these growing trends of resistance must be adequately addressed through innovative research with the development of new pharmacologic treatments or alternative therapies. In the clinical setting, it is important for providers to be aware of the various dermatophyte organisms that commonly cause tinea infections and to be aware of the strains that are becoming resistant to treatment. Adequate diagnosis and treatment of tinea infections will be a critical factor in reducing the number of antifungal-resistant dermatophyte strains.
Author Contributions
Conceptualization, C.K. and A.G.; writing—original draft preparation, C.K. and A.G.; writing—review and editing, T.M. and M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Havlickova, B.; Czaika, V.A.; Friedrich, M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008, 51 (Suppl. S4), 2–15. [Google Scholar] [CrossRef]
- Weitzman, I.; Summerbell, R.C. The dermatophytes. Clin Microbiol Rev 1995, 8, 240–259. [Google Scholar] [CrossRef]
- Panackal, A.A.; Halpern, E.F.; Watson, A.J. Cutaneous fungal infections in the United States: Analysis of the National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Medical Care Survey (NHAMCS), 1995-2004. Int J Dermatol 2009, 48, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Bickers, D.R.; Lim, H.W.; Margolis, D.; Weinstock, M.A.; Goodman, C.; Faulkner, E.; Gould, C.; Gemmen, E.; Dall, T.; American Academy of Dermatology, A.; et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J Am Acad Dermatol 2006, 55, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Vena, G.A.; Chieco, P.; Posa, F.; Garofalo, A.; Bosco, A.; Cassano, N. Epidemiology of dermatophytoses: Retrospective analysis from 2005 to 2010 and comparison with previous data from 1975. New Microbiol 2012, 35, 207–213. [Google Scholar] [PubMed]
- Ely, J.W.; Rosenfeld, S.; Seabury Stone, M. Diagnosis and management of tinea infections. Am Fam Physician 2014, 90, 702–710. [Google Scholar]
- Kemna, M.E.; Elewski, B.E. A U.S. epidemiologic survey of superficial fungal diseases. J Am Acad Dermatol 1996, 35, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Abd Elmegeed, A.S.; Ouf, S.A.; Moussa, T.A.; Eltahlawi, S.M. Dermatophytes and other associated fungi in patients attending to some hospitals in Egypt. Braz J Microbiol 2015, 46, 799–805. [Google Scholar] [CrossRef]
- White, T.C.; Findley, K.; Dawson, T.L., Jr.; Scheynius, A.; Boekhout, T.; Cuomo, C.A.; Xu, J.; Saunders, C.W. Fungi on the skin: Dermatophytes and Malassezia. Cold Spring Harb Perspect Med 2014, 4. [Google Scholar] [CrossRef]
- Brasch, J. Current knowledge of host response in human tinea. Mycoses 2009, 52, 304–312. [Google Scholar] [CrossRef]
- Dogra, S.; Uprety, S. The menace of chronic and recurrent dermatophytosis in India: Is the problem deeper than we perceive? Indian Dermatol Online J 2016, 7, 73–76. [Google Scholar] [CrossRef]
- Pathania, S.; Rudramurthy, S.M.; Narang, T.; Saikia, U.N.; Dogra, S. A prospective study of the epidemiological and clinical patterns of recurrent dermatophytosis at a tertiary care hospital in India. Indian J Dermatol Venereol Leprol 2018, 84, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Verma, P.; Chandra, U.; Tiwary, N.K. Risk factors for chronic and chronic-relapsing tinea corporis, tinea cruris and tinea faciei: Results of a case-control study. Indian J Dermatol Venereol Leprol 2019, 85, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Canavan, T.N.; Elewski, B.E. Identifying Signs of Tinea Pedis: A Key to Understanding Clinical Variables. J Drugs Dermatol 2015, 14, s42–s47. [Google Scholar] [PubMed]
- Appelt, L.; Nenoff, P.; Uhrlass, S.; Kruger, C.; Kuhn, P.; Eichhorn, K.; Buder, S.; Beissert, S.; Abraham, S.; Aschoff, R.; et al. [Terbinafine-resistant dermatophytoses and onychomycosis due to Trichophyton rubrum]. Hautarzt 2021, 72, 868–877. [Google Scholar] [CrossRef] [PubMed]
- de Sousa Mda, G.; Santana, G.B.; Criado, P.R.; Benard, G. Chronic widespread dermatophytosis due to Trichophyton rubrum: A syndrome associated with a Trichophyton-specific functional defect of phagocytes. Front Microbiol 2015, 6, 801. [Google Scholar] [CrossRef] [PubMed]
- Hryncewicz-Gwozdz, A.; Kalinowska, K.; Plomer-Niezgoda, E.; Bielecki, J.; Jagielski, T. Increase in resistance to fluconazole and itraconazole in Trichophyton rubrum clinical isolates by sequential passages in vitro under drug pressure. Mycopathologia 2013, 176, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Muller, V.L.; Kappa-Markovi, K.; Hyun, J.; Georgas, D.; Silberfarb, G.; Paasch, U.; Uhrlass, S.; Nenoff, P.; Schaller, J. Tinea capitis et barbae caused by Trichophyton tonsurans: A retrospective cohort study of an infection chain after shavings in barber shops. Mycoses 2021, 64, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Ghannoum, M.; Isham, N.; Hajjeh, R.; Cano, M.; Al-Hasawi, F.; Yearick, D.; Warner, J.; Long, L.; Jessup, C.; Elewski, B. Tinea capitis in Cleveland: Survey of elementary school students. J Am Acad Dermatol 2003, 48, 189–193. [Google Scholar] [CrossRef]
- Pilz, J.F.; Koberle, M.; Kain, A.; Seidl, P.; Zink, A.; Biedermann, T.; Pilz, A.C. Increasing incidence of Trichophyton tonsurans in Munich-A single-centre observation. Mycoses 2023, 66, 441–447. [Google Scholar] [CrossRef]
- Alkeswani, A.; Cantrell, W.; Elewski, B. Treatment of Tinea Capitis. Skin Appendage Disorders 2019, 5, 201–210. [Google Scholar] [CrossRef]
- Al Aboud, AM.; Crane, JS. Tinea Capitis. In StatPearls; Treasure Island (FL) ineligible companies. Disclosure: Ahmad Al Aboud declares no relevant financial relationships with ineligible companies., 2023.
- Takenaka, M.; Murota, H.; Nishimoto, K. Epidemiological survey of 42 403 dermatophytosis cases examined at Nagasaki University Hospital from 1966 to 2015. J Dermatol 2020, 47, 615–621. [Google Scholar] [CrossRef]
- Gupta, A.K.; Chaudhry, M.; Elewski, B. Tinea corporis, tinea cruris, tinea nigra, and piedra. Dermatol Clin 2003, 21, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Kim, S.L.; Jang, Y.H.; Lee, S.J.; Kim, D.W.; Bang, Y.J.; Jun, J.B. Increasing Prevalence of Trichophyton rubrum Identified through an Analysis of 115,846 Cases over the Last 37 Years. J Korean Med Sci 2015, 30, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, A.K.; Mahajan, R. Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review. Indian Dermatol Online J 2016, 7, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Gupta, G.; Jain, H.C.; Lynde, C.W.; Foley, K.A.; Daigle, D.; Cooper, E.A.; Summerbell, R.C. The prevalence of unsuspected onychomycosis and its causative organisms in a multicentre Canadian sample of 30 000 patients visiting physicians’ offices. J Eur Acad Dermatol Venereol 2016, 30, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Ebihara, M.; Makimura, K.; Sato, K.; Abe, S.; Tsuboi, R. Molecular detection of dermatophytes and nondermatophytes in onychomycosis by nested polymerase chain reaction based on 28S ribosomal RNA gene sequences. Br J Dermatol 2009, 161, 1038–1044. [Google Scholar] [CrossRef]
- Chadeganipour, M.; Mohammadi, R. Causative Agents of Onychomycosis: A 7-Year Study. J Clin Lab Anal 2016, 30, 1013–1020. [Google Scholar] [CrossRef]
- Seebacher, C.; Bouchara, J.P.; Mignon, B. Updates on the epidemiology of dermatophyte infections. Mycopathologia 2008, 166, 335–352. [Google Scholar] [CrossRef]
- Shemer, A.; Grunwald, M.H.; Davidovici, B.; Nathansohn, N.; Amichai, B. A novel two-step kit for topical treatment of tinea pedis--an open study. J Eur Acad Dermatol Venereol 2010, 24, 1099–1101. [Google Scholar] [CrossRef]
- Ozturk, P.; Arican, O.; Kurutas, E.B.; Karakas, T.; Gungor, M. Local oxidative stress in interdigital tinea pedis. J Dermatol 2013, 40, 114–117. [Google Scholar] [CrossRef]
- Hawkins, D.M.; Smidt, A.C. Superficial fungal infections in children. Pediatr Clin North Am 2014, 61, 443–455. [Google Scholar] [CrossRef]
- Kaushik, N.; Pujalte, G.G.; Reese, S.T. Superficial Fungal Infections. Prim Care 2015, 42, 501–516. [Google Scholar] [CrossRef] [PubMed]
- Ameen, M. Epidemiology of superficial fungal infections. Clin Dermatol 2010, 28, 197–201. [Google Scholar] [CrossRef]
- Mirmirani, P.; Tucker, L.Y. Epidemiologic trends in pediatric tinea capitis: A population-based study from Kaiser Permanente Northern California. J Am Acad Dermatol 2013, 69, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Fuller, L.C.; Child, F.C.; Midgley, G.; Higgins, E.M. Scalp ringworm in south-east London and an analysis of a cohort of patients from a paediatric dermatology department. Br J Dermatol 2003, 148, 985–988. [Google Scholar] [CrossRef]
- Emilia Ghelardi; Anna Bulgheroni; Federico Mailland, M.; Francesco Celandroni; Gueye, S.A. In vitro evaluation of the potential of ciclopirox to induce resistance in Trichophyton rubrum, in comparison to terbinafine, amorolfine, and itraconazole. Journal of American Academy of Dermatology 2013, 68. [CrossRef]
- Ryder, N.S.; Wagner, S.; Leitner, I. In vitro activities of terbinafine against cutaneous isolates of Candida albicans and other pathogenic yeasts. Antimicrob Agents Chemother 1998, 42, 1057–1061. [Google Scholar] [CrossRef] [PubMed]
- Kovitwanichkanont, T.; Chong, A.H. Superficial fungal infections. Aust J Gen Pract 2019, 48, 706–711. [Google Scholar] [CrossRef]
- Kreijkamp-Kaspers, S.; Hawke, K.; Guo, L.; Kerin, G.; Bell-Syer, S.E.; Magin, P.; Bell-Syer, S.V.; van Driel, M.L. Oral antifungal medication for toenail onychomycosis. Cochrane Database Syst Rev 2017, 7, CD010031. [Google Scholar] [CrossRef]
- Ferguson, J.E.; Prouty, M. Terbinafine used safely in autoimmune hepatitis for treatment of tinea corporis. BMJ Case Rep 2021, 14. [Google Scholar] [CrossRef]
- Itraconazole. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; Bethesda (MD), 2012.
- Puttick, M.P.; Phillips, P. Itraconazole: Precautions regarding drug interactions and bioavailability. Can J Infect Dis 1994, 5, 179–183. [Google Scholar] [CrossRef]
- Lipner, S.R.; Scher, R.K. Onychomycosis: Treatment and prevention of recurrence. J Am Acad Dermatol 2019, 80, 853–867. [Google Scholar] [CrossRef]
- Ghannoum, M.A.; Mukherjee, P.K.; Warshaw, E.M.; Evans, S.; Korman, N.J.; Tavakkol, A. Molecular analysis of dermatophytes suggests spread of infection among household members. Cutis 2013, 91, 237–245. [Google Scholar] [PubMed]
- Rex, J.H.; Walsh, T.J.; Sobel, J.D.; Filler, S.G.; Pappas, P.G.; Dismukes, W.E.; Edwards, J.E. Practice guidelines for the treatment of candidiasis. Infectious Diseases Society of America. Clin Infect Dis 2000, 30, 662–678. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis 2016, 62, e1-50. [Google Scholar] [CrossRef] [PubMed]
- Weyers, W.; Diaz-Cascajo, C.; Weyers, I. Erythema annulare centrifugum: Results of a clinicopathologic study of 73 patients. Am J Dermatopathol 2003, 25, 451–462. [Google Scholar] [CrossRef]
- Al Hasan, M.; Fitzgerald, S.M.; Saoudian, M.; Krishnaswamy, G. Dermatology for the practicing allergist: Tinea pedis and its complications. Clin Mol Allergy 2004, 2, 5. [Google Scholar] [CrossRef]
- Elewski, B.E. Onychomycosis: Pathogenesis, diagnosis, and management. Clin Microbiol Rev 1998, 11, 415–429. [Google Scholar] [CrossRef]
- Hay, R.J.; Ashbee, H.R. Mycology. In Rook’s Textbook of Dermatology; 2010; pp. 1–93.
- Yee, G.; Al Aboud, AM. Tinea Corporis. In StatPearls; Treasure Island (FL) ineligible companies. Disclosure: Garrett Yee declares no relevant financial relationships with ineligible companies., 2023. 2023.
- Pippin, M.M.; Madden, M.L.; Das, M. Tinea Cruris. In StatPearls; Treasure Island (FL) ineligible companies. Disclosure: Michael Madden declares no relevant financial relationships with ineligible companies. Disclosure: Moushumi Das declares no relevant financial relationships with ineligible companies., 2023.
- Pei, Y.; Zhang, L.L.; Liu, Z.H. Tinea Faciei. J Pediatr 2022, 250, 108–109. [Google Scholar] [CrossRef]
- Julapalli, M.R.; Levy, M.L. CHAPTER 67—VIRAL AND FUNGAL SKIN INFECTIONS. In Feigin and Cherry’s Textbook of Pediatric Infectious Diseases (Sixth Edition), Feigin, R.D., Cherry, J.D., Demmler-Harrison, G.J., Kaplan, S.L., Eds.; W.B. Saunders: Philadelphia, 2009; pp. 794–809.
- Kuruvella, T.; Pandey, S. Tinea Barbae. In StatPearls; Treasure Island (FL) ineligible companies. Disclosure: Shivlal Pandey declares no relevant financial relationships with ineligible companies., 2023.
- Chamorro, M.J.; House, S.A. Tinea Manuum. In StatPearls; Treasure Island (FL) ineligible companies. Disclosure: Steven House declares no relevant financial relationships with ineligible companies., 2023.
- Schuller, J.; Remme, J.J.; Rampen, F.H.; Van Neer, F.C. Itraconazole in the treatment of tinea pedis and tinea manuum: Comparison of two treatment schedules. Mycoses 1998, 41, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Rand, S. Overview: The treatment of dermatophytosis. J Am Acad Dermatol 2000, 43, S104–112. [Google Scholar] [CrossRef]
- Korting, H.C.; Schollmann, C. The significance of itraconazole for treatment of fungal infections of skin, nails and mucous membranes. J Dtsch Dermatol Ges 2009, 7, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Drake, L.A.; Dinehart, S.M.; Farmer, E.R.; Goltz, R.W.; Graham, G.F.; Hardinsky, M.K.; Lewis, C.W.; Pariser, D.M.; Skouge, J.W.; Webster, S.B.; et al. Guidelines of care for superficial mycotic infections of the skin: Tinea corporis, tinea cruris, tinea faciei, tinea manuum, and tinea pedis. Guidelines/Outcomes Committee. American Academy of Dermatology. J Am Acad Dermatol 1996, 34, 282–286. [Google Scholar] [CrossRef]
- Zeichner, J.A. New Topical Therapeutic Options in the Management of Superficial Fungal Infections. J Drugs Dermatol 2015, 14, s35–s41. [Google Scholar]
- Gupta, A.K.; Cooper, E.A. Update in antifungal therapy of dermatophytosis. Mycopathologia 2008, 166, 353–367. [Google Scholar] [CrossRef]
- Leelavathi, M.; Noorlaily, M. Onychomycosis nailed. Malays Fam Physician 2014, 9, 2–7. [Google Scholar]
- Singh, A.; Masih, A.; Khurana, A.; Singh, P.K.; Gupta, M.; Hagen, F.; Meis, J.F.; Chowdhary, A. High terbinafine resistance in Trichophyton interdigitale isolates in Delhi, India harbouring mutations in the squalene epoxidase gene. Mycoses 2018, 61, 477–484. [Google Scholar] [CrossRef]
- Gamage, H.; Sivanesan, P.; Hipler, U.C.; Elsner, P.; Wiegand, C. Superficial fungal infections in the department of dermatology, University Hospital Jena: A 7-year retrospective study on 4556 samples from 2007 to 2013. Mycoses 2020, 63, 558–565. [Google Scholar] [CrossRef]
- Hiruma, J.; Noguchi, H.; Hase, M.; Tokuhisa, Y.; Shimizu, T.; Ogawa, T.; Hiruma, M.; Harada, K.; Kano, R. Epidemiological study of terbinafine-resistant dermatophytes isolated from Japanese patients. J Dermatol 2021, 48, 564–567. [Google Scholar] [CrossRef]
- Jia, S.; Long, X.; Hu, W.; Zhu, J.; Jiang, Y.; Ahmed, S.; de Hoog, G.S.; Liu, W.; Jiang, Y. The epidemic of the multiresistant dermatophyte Trichophyton indotineae has reached China. Front Immunol 2022, 13, 1113065. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.S.; Chaturvedi, S.; Zhu, Y.; Todd, G.C.; Yin, L.; Lopez, A.; Travis, L.; Smith, D.J.; Chiller, T.; Lockhart, S.R.; et al. Notes from the Field: First Reported U.S. Cases of Tinea Caused by Trichophyton indotineae—New York City, December 2021-March 2023. MMWR Morb Mortal Wkly Rep 2023, 72, 536–537. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Ghannoum, M.; Elewski, B.E. Treatment-resistant tinea corporis, a potential public health issue. Br J Dermatol 2021, 184, 164–165. [Google Scholar] [CrossRef]
- Shen, J.J.; Arendrup, M.C.; Verma, S.; Saunte, D.M.L. The Emerging Terbinafine-Resistant Trichophyton Epidemic: What Is the Role of Antifungal Susceptibility Testing? Dermatology 2022, 238, 60–79. [Google Scholar] [CrossRef] [PubMed]
- Saunte, D.M.L.; Hare, R.K.; Jorgensen, K.M.; Jorgensen, R.; Deleuran, M.; Zachariae, C.O.; Thomsen, S.F.; Bjornskov-Halkier, L.; Kofoed, K.; Arendrup, M.C. Emerging Terbinafine Resistance in Trichophyton: Clinical Characteristics, Squalene Epoxidase Gene Mutations, and a Reliable EUCAST Method for Detection. Antimicrob Agents Chemother 2019, 63. [Google Scholar] [CrossRef] [PubMed]
- Ghannoum, M.A.; Rice, L.B. Antifungal agents: Mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Clin Microbiol Rev 1999, 12, 501–517. [Google Scholar] [CrossRef]
- Yamada, T.; Maeda, M.; Alshahni, M.M.; Tanaka, R.; Yaguchi, T.; Bontems, O.; Salamin, K.; Fratti, M.; Monod, M. Terbinafine Resistance of Trichophyton Clinical Isolates Caused by Specific Point Mutations in the Squalene Epoxidase Gene. Antimicrob Agents Chemother 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Singh, P.; Dingemans, G.; Meis, J.F.; Chowdhary, A. Evaluation of DermaGenius((R)) resistance real-time polymerase chain reaction for rapid detection of terbinafine-resistant Trichophyton species. Mycoses 2021, 64, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Das, S.; Tigga, R.; Pandey, R.; Bhattacharya, S.N.; Taneja, B. Whole genome sequences of two Trichophyton indotineae clinical isolates from India emerging as threats during therapeutic treatment of dermatophytosis. 3 Biotech 2021, 11, 402. [Google Scholar] [CrossRef]
- Rayens, E.; Norris, K.A. Prevalence and Healthcare Burden of Fungal Infections in the United States, 2018. Open Forum Infect Dis 2022, 9, ofab593. [Google Scholar] [CrossRef]
- Tack, D.A.; Fleishcer, A., Jr.; McMichael, A.; Feldman, S. The epidemic of tinea capitis disproportionately affects school-aged African Americans. Pediatr Dermatol 1999, 16, 75. [Google Scholar] [CrossRef]
- Coloe, J.R.; Diab, M.; Moennich, J.; Diab, D.; Pawaskar, M.; Balkrishnan, R.; Bechtel, M.A. Tinea capitis among children in the Columbus area, Ohio, USA. Mycoses 2010, 53, 158–162. [Google Scholar] [CrossRef]
- Gupta, A.K.; Simpson, F.C. Efinaconazole: A new topical treatment for onychomycosis. Skin Therapy Lett 2014, 19, 1–4. [Google Scholar]
- Rodriguez, D.A. Efinaconazole Topical Solution, 10%, for the Treatment of Mild and Moderate Toenail Onychomycosis. J Clin Aesthet Dermatol 2015, 8, 24–29. [Google Scholar]
- Poulakos, M.; Grace, Y.; Machin, J.D.; Dorval, E. Efinaconazole and Tavaborole. J Pharm Pract 2017, 30, 245–255. [Google Scholar] [CrossRef]
- Gamal, A.; Elshaer, M.; Long, L.; McCormick, T.S.; Elewski, B.; Ghannoum, M.A. Antifungal Activity of Efinaconazole Compared to Fluconazole, Itraconazole, and Terbinafine against Terbinafine- and Itraconazole-Resistant and -Susceptible Clinical Isolates of Dermatophytes, Candida, and Mold. J Am Podiatr Med Assoc 2023, 1–30. [Google Scholar] [CrossRef]
- FDA. LUZU (luliconazole) Cream, 1%. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/204153s000lbl.pdf (accessed on October 5th).
- FDA. JUBLIA® (efinaconazole) topical solution, 10%. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/203567s000lbl.pdf (accessed on November 7).
- Wiederhold, N.P.; Fothergill, A.W.; McCarthy, D.I.; Tavakkol, A. Luliconazole demonstrates potent in vitro activity against dermatophytes recovered from patients with onychomycosis. Antimicrob Agents Chemother 2014, 58, 3553–3555. [Google Scholar] [CrossRef]
- Jerajani, H.; Janaki, C.; Kumar, S.; Phiske, M. Comparative assessment of the efficacy and safety of sertaconazole (2%) cream versus terbinafine cream (1%) versus luliconazole (1%) cream in patients with dermatophytoses: A pilot study. Indian J Dermatol 2013, 58, 34–38. [Google Scholar] [CrossRef]
- FDA. KERYDIN® (tavaborole) topical solution, 5%. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/204427s006lbl.pdf.
- Sharma, N.; Sharma, D. An upcoming drug for onychomycosis: Tavaborole. J Pharmacol Pharmacother 2015, 6, 236–239. [Google Scholar] [CrossRef]
- Ciaravino, V.; Coronado, D.; Lanphear, C.; Shaikh, I.; Ruddock, W.; Chanda, S. Tavaborole, a novel boron-containing small molecule for the topical treatment of onychomycosis, is noncarcinogenic in 2-year carcinogenicity studies. Int J Toxicol 2014, 33, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Scher, R.K.; Nakamura, N.; Tavakkol, A. Luliconazole: A review of a new antifungal agent for the topical treatment of onychomycosis. Mycoses 2014, 57, 389–393. [Google Scholar] [CrossRef]
- Watanabe, S.; Kishida, H.; Okubo, A. Efficacy and safety of luliconazole 5% nail solution for the treatment of onychomycosis: A multicenter, double-blind, randomized phase III study. J Dermatol 2017, 44, 753–759. [Google Scholar] [CrossRef]
- Rich, P.; Spellman, M.; Purohit, V.; Zang, C.; Crook, T.J. Tavaborole 5% Topical Solution for the Treatment of Toenail Onychomycosis in Pediatric Patients: Results from a Phase 4 Open-Label Study. J Drugs Dermatol 2019, 18, 190–195. [Google Scholar]
- Elewski, B.E.; Aly, R.; Baldwin, S.L.; Gonzalez Soto, R.F.; Rich, P.; Weisfeld, M.; Wiltz, H.; Zane, L.T.; Pollak, R. Efficacy and safety of tavaborole topical solution, 5%, a novel boron-based antifungal agent, for the treatment of toenail onychomycosis: Results from 2 randomized phase-III studies. J Am Acad Dermatol 2015, 73, 62–69. [Google Scholar] [CrossRef]
- Francuzik, W.; Fritz, K.; Salavastru, C. Laser therapies for onychomycosis—Critical evaluation of methods and effectiveness. J Eur Acad Dermatol Venereol 2016, 30, 936–942. [Google Scholar] [CrossRef]
- Nijenhuis-Rosien, L.; Kleefstra, N.; Wolfhagen, M.J.; Groenier, K.H.; Bilo, H.J.; Landman, G.W. Laser therapy for onychomycosis in patients with diabetes at risk for foot complications: Study protocol for a randomized, double-blind, controlled trial (LASER-1). Trials 2015, 16, 108. [Google Scholar] [CrossRef]
- Gupta, A.K.; Versteeg, S.G. A critical review of improvement rates for laser therapy used to treat toenail onychomycosis. J Eur Acad Dermatol Venereol 2017, 31, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Ergosterol Biosynthetic Pathway: Antifungal Sites of Action [74].
Figure 1.
Ergosterol Biosynthetic Pathway: Antifungal Sites of Action [74].
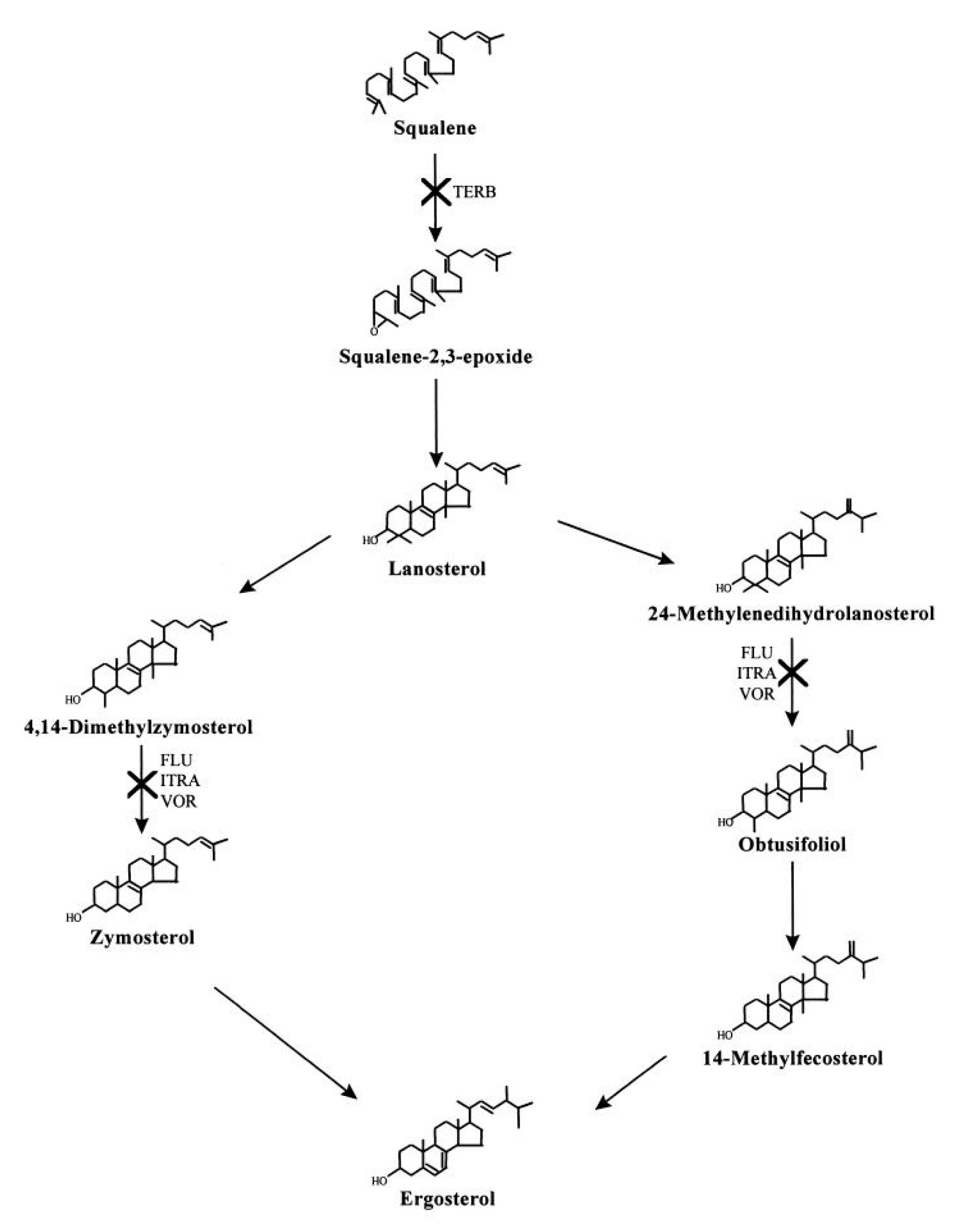
Table 1.
Clinical Classification of Tinea Infections [5].
Table 1.
Clinical Classification of Tinea Infections [5].
| Tinea Infection | Body Area Affected |
|---|---|
| Tinea Capitis | Head and scalp |
| Tinea Corporis | Trunk and extremities |
| Tinea Cruris | Groin, pubic region, intertriginous anogenital region |
| Tinea Faciei | Face |
| Tinea Barbae | Beard and mustache area |
| Tinea Manuum | Hands |
| Tinea Pedis | Feet |
| Onychomycosis (Tinea Unguium) | Nails |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



