
Submitted:
06 March 2025
Posted:
07 March 2025
You are already at the latest version
Abstract
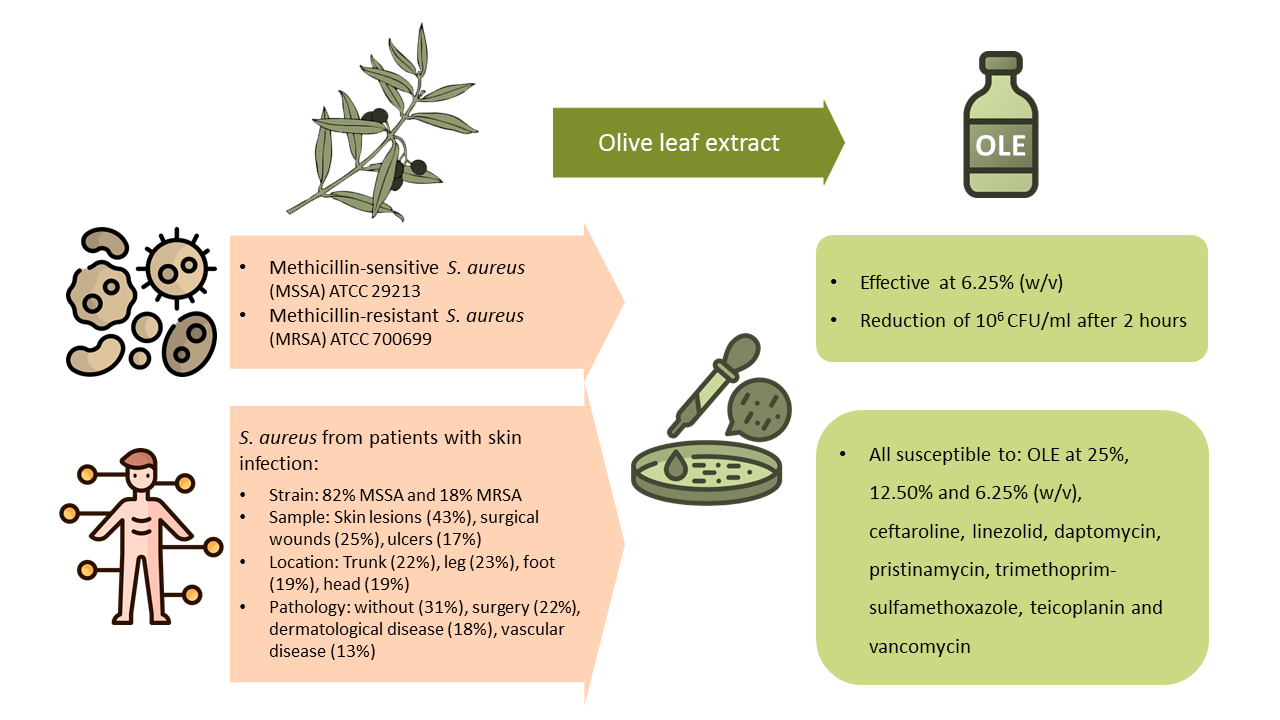
Staphylococcus aureus is one of the most prevalent bacteria in skin and soft tissue infections (SSTIs). Multidrug-resistant strains emergence, particularly methicillin-resistant S. aureus (MRSA), highlights the need for alternative treatments. This study investigates the antimi-crobial properties of olive leaf extract (OLE) and defines the profile of patient with SSTI who may benefit from it. OLE was tested in two reference strains, methicillin-sensitive S. aureus (MSSA) ATCC 29213 and MRSA ATCC 700699, and in 126 clinical isolates from patients with SSTIs. The minimum bactericidal concentration (MBC) ranged from 3.12% to 6.25% w/v for MSSA and 1.56% to 3.12% for MRSA. The lethal curve showed a reduction of 6 log10CFU/ml after two hours of incubation. Most of the 126 clinical samples (103 MSSA and 23 MRSA) came from skin lesions, surgical wounds, and ulcers. Over 90% of MSSA strains were resistant to less than five antibiotics, while 82% of MRSA to more than six. Penicillins demonstrated the lowest susceptibility rate (19.8%), whereas linezolid, daptomycin, pristinamycin, trimethoprim-sulfamethoxazole, teicoplanin, vancomycin, and OLE (25%, 12.50%, and 6.25% w/v) exhibited 100% susceptibility. The findings sug-gest that OLE could serve as a promising alternative treatment for skin infections, partic-ularly in the context of increasing antibiotic resistance.
Keywords:
Olive leaf extract
; Staphylococcus aureus
; MRSA
; Skin and soft tissue infection
1. Introduction
Staphylococcus aureus is naturally present on skin, nares and mucous membranes of healthy population, however it is responsible for more than one million deaths worldwide, being the leading bacterial cause of death in 135 countries [1]. Its great ability to adapt to the stressors present in the skin leads the bacterium to cause persistent and recurrent infections [2], and has been proven to be a disease promoter in inflammatory skin dermatoses as prevalent as atopic dermatitis and psoriasis [3,4]. Thus, it is one of the most frequently identified bacteria in skin and soft tissue infections (SSTIs) [5]. SSTIs range from mild infections, such as pyoderma, which are usually treated with oral antibiotics, to serious, life-threatening infections, such as necrotising fasciitis, which require intravenous treatment [6]. In SSTIs, S. aureus is responsible for more than thirty thousand infection-related deaths worldwide [1].
In this sense, the intensive use of antibiotics in recent decades has led to an increase in multidrug-resistant strains. In 2003, methicillin-resistant S. aureus (MRSA) was the major pathogen in SSTIs in patients from emergency department in the California region [7], as well as MRSA USA 300 clone was the main source of community-onset S. aureus SSTIs in Atlanta [8]. In 2019, in Europe more than 500,000 deaths were associated with bacterial antimicrobial resistance (AMR), with MRSA accounting for approximately 10% [9]. Nowadays, MRSA is responsible for more than 100,000 deaths worldwide and is one of the three antibiotic-resistant bacteria that cause the greatest burden of disease [5,10]. Hence, the rapid increase of antimicrobial-resistant bacteria leads to the challenge of obtaining new antibiotics and therapeutics, making it necessary to find alternative and efficient methods to treat skin infections. Otherwise, infection with antibiotic-resistant strains would be the main cause of death by 2050, including billions of dollars in costs to the population [11].
Traditionally, olive tree has been broadly used in medicine [12]. In particular, olive leaf extract (OLE) has been reported to have multiple uses as an hypotensive [13,14], antioxidant [15] and hypoglycaemic [16], and its polyphenols have also been associated with the reduction of proliferation of pancreatic cancer cells and the induction of apoptosis [17]. More specifically, OLE has shown antimicrobial in vitro activity against a diverse range of Gram-positive, Gram-negative bacteria and fungi (Candida albicans, Escherichia coli, dermatophytes, Helicobacter pylori, methicillin-sensitive S. aureus (MSSA), MRSA, anaerobic periodontal pathogens) [18,19,20,21]. Its antimicrobial properties have been attributed to polyphenols, particularly hydroxytyrosol and oleuropein [22,23]. OLE has been applied as an antimicrobial in food industry to control S. aureus growth during storage of Kasar cheese [24], to preserve seafood [25], to inhibit foodborne pathogens (Listeria monocytogenes, E. coli and Salmonella enteritidis) and avoid their biofilm formation [26].
Apart from that, olive tree products have been applied to the skin as anti-ageing, photo protective, anti-inflammatory and antioxidant agents, as well as for skin wound regeneration [27,28]. In mice, oral administration of OLE and oleuropein prevented the UVB-induced skin damage [29] and intradermal injections of oleuropein accelerated skin wound healing [30]. In rats, the combination of OLE with shea butter has been proven to be effective to treat non-diabetic and diabetic wounds when infected with MRSA [31]. In humans, topical application of olive oil improved the healing of diabetic foot ulcers [32]. Furthermore, it has also been tested in clinical trials for the treatment of papillomavirus and herpes simplex [33,34], achieving faster healing for both viruses infections.
Here, the present work faces two different main objectives. Firstly, to test a new olive leaf extract against S. aureus and its resistance form MRSA in order to combat skin and soft tissue infections, using both standard and clinical strains. Secondly, to epidemiologically describe the S. aureus strains isolated from SSTIs in the Microbiology Department of the Miguel Servet University Hospital over a three-month period, to characterise the number and type of resistances found in the clinical samples where OLE was tested. Hence, define the most common type of patients and samples that could benefit from the potential use of OLE as a treatment.
2. Results
2.1. Epidemiological Description of Clinical Samples
A total of 126 clinical samples were collected and analysed (Table S1). The clinical characteristics are summarized in Table 1.
The analysis of all samples revealed that the median patient age was 56 years (IQR: 27.5-73.8). Seventy-four samples were from male patients and 52 from female patients. Gender showed no association to samples regarding type of sample, location, associated pathology, age and number of antibiotic resistances. The majority of samples came from patients with skin infection without any previous dermatological disease (31%), followed by surgical procedure samples (22.2%). They were collected predominantly from skin lesions (42.9%) and were located on the trunk (22.2%), leg (23.0%), foot (19.0%) and head (19.0%) (Table 1). Thirty-three percent of samples from patients with surgical procedure (9/27) were associated with breast cancer (Table S1). Similarly, impetigo was the most prevalent condition among samples from patients with dermatological disease, occurring for 15 out of 23 cases (65.22%). Patients with skin infection who also had a dermatological disease were significantly younger (median age: 12.0 years, IQR: 6.5-18.0) compared to those with other associated pathologies (median age range: 47.0-79.0 years) (p value <0.05) (Table 1, Figure 1A). Similarly, samples from skin lesions were also obtained from younger patients (median age: 31.0 years, IQR: 12.3-54.5), compared to samples from surgical wounds (median age: 62.0 years, IQR: 47.8-72.5) or other ulcers (median age: 73.0 years, IQR: 64.5-86.8) (p value = 0.011 and <0.001, respectively) (Table 1, Figure 1B).
2.2. Antibiotic Resistance Patterns
Of the 126 samples, 103 (82%) were identified as MSSA and 23 (18%) as MRSA, 63 (61%) and 11 (48%) from male patients respectively. Over 90% of MSSA strains showed less than five antibiotic resistances, whereas 82% of MRSA strains were resistant to more than six antibiotics (Table 1). As expected, the number of antibiotic resistances was statistically higher in MRSA than in MSSA (Figure 1C). In addition, a positive correlation was found between patient age and the number of antibiotic resistances in MRSA strains, the older the patient, the higher the number of antibiotic resistances (Figure 2). With regard to the overall quantity of antibiotic resistances, strains isolated from pressure ulcers showed higher resistance levels compared to those from skin lesions (p value= 0.034) and surgical wounds (p value = 0.039) (Table 1, Figure 1D). It is noteworthy that all the strains from abscesses, surgical wounds, skin lesions, and other ulcers exhibited less than five antibiotic resistances, whereas 60% of pressure ulcer isolates had more than 11 antibiotic resistances (median value: 11.0, IQR: 6.0-13.0) (p value <0.001) (Table 1, Figure 3). Furthermore, a higher prevalence of MRSA was noted in these isolates compared to the rest (p value <0.05) (Figure 4).
2.2.1. Susceptibility Tests on ATCC (American Type Culture Collection) Samples
The susceptibility test on agar plate showed an inhibition of growth in S. aureus at 25, 12.5 and 6.25%w/v, whereas in MRSA OLE was effective at 25, 12.5, 6.25 and 3.125% (w/v). The results of the broth method dilution demonstrated that the OLE MBC for MSSA ranged from 3.125 to 6.25% and for MRSA from 1.56 to 3.125% (w/v), depending on the extraction batch and time since extraction. At least three different extraction batches were analysed. Notwithstanding the observed variation, all samples were effective at a concentration of 6.25% of OLE.
Regarding the lethal curve, the concentration of OLE employed was the maximum feasible (12.5% w/v), aiming for rapid bactericidal activity. After two hours, a reduction of 6 log10CFU/ml was achieved in both MSSA ATCC 29213 and MRSA ATCC 700699 strains treated with OLE against control group (p value <0.005) (Table 2, Figure 5). No bacterial growth (neither MSSA nor MRSA) was observed after 24 hours of OLE treatment, whereas both strains reached a bacterial load of 10⁹ CFU/ml when water was used as control treatment (Table 1, Figure 5).
2.2.2. Susceptibility Tests on ATCC Samples
All clinical isolates described were susceptible to OLE at concentrations of 25, 12.5 and 6.25% (w/v), with seven strains susceptible at 3.125% w/v (Table S1). All the strains were susceptible to seven antibiotics, namely ceftaroline, linezolid, daptomycin, pristinamycin, trimethoprim-sulfamethoxazole, teicoplanin and vancomycin. Conversely, penicillin and ampicillin exhibited the highest resistance frequency (Table 3, Figure 6); in fact, all MRSA strains were resistant to any penicillin (Table 3). Resistant to all aminoglycosides, all penicillins, cefdinir, ciprofloxacin, levofloxacin, erythromycin, quinupristin-dalfopristin, minocycline, fosfomycin, mupirocin and rifampicin was significantly higher in MRSA strains compared to MSSA (p <0.05) (Table 3). Fluoroquinolone-resistant strains were also resistant to moxifloxacin (Table S1).
The interpretation of fusidic acid susceptibility was limited due to testing panel concentrations (2 mg/l) that did not align with EUCAST breakpoints (1 mg/l and 0.5 mg/l for topical use) (The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 14.0, 2024. http://www.eucast.org). Subsequently, an additional antimicrobial disk susceptibility test was conducted based on clinical characteristics and physician requests at the Microbiology department. Apart from that, up to 60% of MRSA analysed isolates were resistant to fusidic acid (Table 3).
When looking for more than one antibiotic resistance in each sample, 8 out of 126 strains were resistant to oxacillin and gentamicin. Additionally, six (three MSSA, three MRSA) out of 28 strains analysed were resistant to both fusidic acid and mupirocin. Similarly, three MRSA out of 28 strains tested were resistant to both fusidic acid and gentamicin. Furthermore, two of these MRSA were resistant to the four antibiotics fusidic acid, gentamicin, mupirocin and oxacillin (Table S1).
2.2.3. Antibiotic Families and Efficacy
In terms of antibiotic susceptibility by antibiotic family, penicillins had the lowest susceptibility rate (19.8%) (Figure 6), while oxazolidinones (linezolid), lipopeptides (daptomycin), pristinamycin, folate pathway inhibitors (trimethoprim-sulfamethoxazole), glycopeptides and lipoglycopeptides (teicoplanin and vancomycin), and OLE showed 100% efficacy (Figure 6).
3. Discussion
The present study demonstrated the antibiotic effect of OLE against multidrug-resistant strains of S. aureus, including the determination of their MBC and lethality curve, based on both reference and hospital clinical samples. Additionally, it provides and epidemiological description of the clinical samples analysed, hence, defining the profile of patient that could benefit from the treatment with OLE.
In our research, susceptibility test on agar plate and MBC values were slightly lower in the MRSA ATCC strain when compared to the MSSA ATCC strain. This variation can be attributed to the faster in vitro growth rate of MSSA, which is characterised by its metabolic efficiency and adaptability. It has been reported that MSSA strains generally exhibit faster replication rates under laboratory conditions, whereas MRSA mechanisms of resistance frequently incur a metabolic cost [35,36]. Furthermore, the genetic diversity among MRSA strains can also contribute to variability in growth rates, as demonstrated by Stevens et al., who showed differences in growth speed and antibiotic tolerance in a MRSA strain [37].
Regarding other studies on OLE, Sujana et al. reported a minimum inhibitory concentration (MIC) of 0.62% for S. aureus with a minimum oleuropein content of 4.4 mg/ml [20]. In our case, the amount of oleuropein was 8.3 mg/ml (Table S2) and the MBC were slightly higher, being 6.25% for MSSA and 3.125% for MRSA. This difference may be attributed to the extraction method, since Sudjana et al. employed fresh leaves whereas we used powdered dried leaves. Markin et al. reported a MBC of 0.6% w/v for S. aureus from powdered leaves, but they stored their extract for up to eight weeks [19], while our OLE was used after being frozen at -80°C for six months (data not shown). Apart from that, the majority of studies report the antimicrobial effect of OLE after a 24-hour incubation period [20,21,26]. In our research, the OLE was able to reduce the number of viable bacteria to nearly zero after two hours of incubation, consistent with the findings of Markin et al. [19], but we also tested a MRSA ATCC strain.
Most authors assign the antimicrobial activity of OLE to polyphenols, such as oleuropein and its derivatives [22,23,38,39]. The amount of oleuropein is commonly used as a standard of OLE characterization [20]. On the other hand, oleanolic acid has been shown to cause cell membrane damage in L. monocytogenes, Enterococcus faecium, and Enterococcus faecalis [40]. Olive leaf extract has also been reported to suppress flagella production in L. monocytogenes [26] and polyphenols from olive mill wastes showed inhibition of E. coli biofilm formation [41]. Although the mode of action of OLE is not fully understood, its antimicrobial efficacy is believed to stem from the synergistic effects of its constituent compounds [23]. Liu et al. reported greater inhibition of bacterial growth when using the olive leaf extract compared to oleuropein and verbascoside separately [26]. Furthermore, Lim et al., (2016) showed enhanced ampicillin efficacy when combined with OLE, highlighting its potential to mitigate antibiotic resistance development through a multi-compound mechanism [43]. In our study, the efficacy of OLE was evaluated against a range of clinical strains of S. aureus, including those exhibiting diverse antibiotic resistance profiles. Even the most resistant MRSA strains were susceptible to OLE at three different concentrations (Table S1).
Regarding skin and soft tissue infections, in our study 31% of the samples derived from a skin infection without any underlying dermatological disease, such as burns, wound infections, trauma, etc. (Table 1). Similarly to other researchers that identified impetigo as the most predominant infection [44], in our case it accounts for the 65% of samples collected from patients with a dermatological disease (Table S1). The frequency of MRSA found in skin and soft tissue infections varied between studies. In our research there were 18.3% MRSA (Table 1); lower than the 54.1% reported in Pakistan [44], and also slightly lower than the Spanish prevalence of 20-30% reported by Murray et al. [9]. However, a higher proportion of MRSA (66.6%) was found in pressure ulcer samples (Figure 3), similar to the 59% reported by Manzur et al. [45].
The most common treatment for S. aureus infection involves oral antibiotic therapy or parenteral treatment for severe cases [5,46] as well as for MRSA infection, including a wide range of adverse reactions [47]. On the other hand, the most commonly used topical antibiotics are fusidic acid or mupirocin [48]. Frazee et al. (2005) proposed the use of trimethoprim/sulfamethoxazole, clindamycin or vancomycin for the treatment of skin and soft tissue infections in communities with high MRSA prevalence [7]. In contrast, Habib and Qadir (2022) recommended rifampicin, minocycline, amikacin, and clindamycin for MRSA, reserving linezolid, teicoplanin and vancomycin for severe cases [44]. We reported only seven antibiotics, apart from OLE, demonstrating susceptibility across all strains (ceftaroline, linezolid, daptomycin, pristinamycin, trimethoprim-sulfamethoxazole, teicoplanin and vancomycin) (Table 3). In comparison to previous studies [7,44,49,50], the data presented here showed higher rates of antibiotic resistance, especially to fluoroquinolones, clindamycin, gentamicin, fusidic acid and mupirocin. In our research, MSSA showed a higher resistance rates for clindamycin (27.2%), fusidic acid (22.2%) and mupirocin (12.6%) in comparison to the 8.8%, 10.9% and 1.4% respectively reported by Zhanel et al. (2021). Similarly, the MRSA resistance rates for levofloxacin (78.9%), ciprofloxacin (73.9%), clindamycin (47.8%), fusidic acid (60%) and mupirocin (39.1%) were higher than the 43.2% reported by Frazee et al. (2005) for levofloxacin or the 67.1%, 9.5%, 10.6% and 14.1% reported by Zhanel et al. (2021) for ciprofloxacin, clindamycin, fusidic acid, and mupirocin respectively [7,50] (Table 3). Although the susceptibility rate to fusidic acid in our research may be overestimated, as only 28 strains were analysed due to the limitations of the technique.
Looking in detail at topical antibiotic resistance, up to 22% of samples analysed were resistant to both fusidic acid and mupirocin simultaneously, which could lead to failure of topical treatment and progression to more severe disease. Additionally, two strains analysed were found to be resistant to fusidic acid, gentamicin, mupirocin and oxacillin, whereas all these strains reported were susceptible to OLE (Table S1).
Besides, OLE and its derivatives have already been successfully applied on the skin as a protective and antioxidant factor, to reduce skin damage, and as a healer of diabetic foot ulcers [27,28,29,30]. Moreover, it has even been employed in the treatment of papillomavirus and herpes simplex virus infections [33,34]. For these reasons, OLE may be used not only to treat but also to prevent skin infections caused by S. aureus. For example, 33% of our samples from surgical procedures were from breast cancer wounds. Given that OLE is known to help with skin regeneration [27], it could be used after surgery to prevent the infection and improve wound healing. In a similar way, it could benefit patients with atopic dermatitis by helping to control the disease by reducing the amount of S. aureus in their microbiome while promoting skin barrier repair [3]. In addition, the application of OLE could be useful in patients with comorbidities, where parenteral administration of antibiotics is ineffective due to the difficulty of reaching the local niche of the bacteria. It could also be applied in patients with antibiotic restrictions, such as children or pregnant women. In our research, the median age of patients with a skin infection and dermatological disease was 12 years old (Table 1), of which 65% were impetigo cases. These patients could benefit from treatment with OLE, thus reducing the spread of this highly contagious paediatric condition.
The potential of OLE as a topical antimicrobial is highlighted by the present work. We propose a localized treatment with OLE as single agent or in combination with other antibiotics to prevent the dispersion of bacteria, given that OLE is already sold as a natural supplement to reduce high blood pressure and decrease cholesterol levels among others, making it easy to implement in the clinic. For instance, it could be useful in countries with high MRSA prevalence [9], taking advantage of the lack of side effects and cost-effective treatment. However, further research is needed to know more about its mechanism of action, stability, skin penetration level and efficacy, alone or in combination with other antimicrobials, in clinical trials involving patients with skin and soft tissue infections.
To our knowledge, this is the best time that OLE is proposed as a topical bactericide to fight against dermatological infections. Furthermore, this is the first report demonstrating that its antimicrobial action, after 2 hours incubation, leads to a complete bacterial eradication of MSSA and MRSA. Additionally, it has been tested on different strains of S. aureus, with varying levels of antibiotic resistances. Moreover, a clinical description of all the S. aureus strains isolated from patients with skin and soft tissue infections in our department was conducted, identifying the most common antibiotic resistance patterns and defining the patient profile that could benefit from the potential use of OLE as a treatment.
4. Materials and Methods
4.1. OLE Extraction
Olive leaf extract was prepared as follows: dried olive leaves of Olea Europaea, stored in an opaque container under nitrogen atmosphere, were weighed on a precision balance and diluted in bidistilled and sterile water at room temperature to a concentration of 25% weight/volume (250 mg/ml). Once the dilution was prepared, it was homogenised with two zirconium/silica beads in a Mini Beadbeater 16 cell disruptor (BioSpec®) at 3450 rpm for 2 minutes. The extract was then subjected to an ultrasound bath for 3 minutes at 37°C. The supernatant was separated from the leaf debris by centrifugation at 5000 rpm for 2 minutes. The aqueous phases of all the fractions were pooled and centrifuged again. Finally, the olive leaf extract was filtered through a 0.22 µm filter and stored in sterile Eppendorf tubes. Once the extract was obtained, the aliquots were kept frozen at -80°C until use.
4.2. OLE phenolic Profile
OLE extract was homogenised with 70% ethanol in Milli-Q water (1,600 rpm, 2 min) using an Ultra-Turrax T25-Basic mixer. Then, the mixture was centrifuged (12,500 rpm, 4°C, 15 min) and the supernatant was filtered through a 0.45 μm membrane. The resulting extracts were stored at -18°C in the dark until further analysis. Identification and quantification of the individual phenolic compounds were carried out by UPLC-MS/MS on an AcQuity Ultra-Performance™ liquid chromatography/tandem mass spectrometry system (Waters, Milford, MA, USA) similarly to that described by Martínez-Beamonte [51]. Calibration curves with an R2 value of 0.99 or higher were generated using commercial standards (Sigma-Aldrich, Madrid, Spain) to ensure accurate quantification. The phenolic profile of OLE is presented in Table S2.
4.3. Bacteria
4.3.1. Reference S. aureus Strains
The reference strains used were MSSA American Type Culture Collection (ATCC) 29213 and MRSA ATCC 700699 and cultured on Columbia blood agar (CBA) (Thermo Scientific™) under aerobic conditions at 35°C for 18-24 hours to obtain fresh isolated colonies. These strains were used to test the bacterial susceptibility to OLE on agar plate, to calculate the minimum bactericidal concentration (MBC), and the lethal curve.
4.3.2. S. aureus Strains from Clinical Samples
This study included all samples from patients with skin and soft tissue infections that were received between May 29th and August 29th 2024 at the Microbiology Department of Miguel Servet University Hospital (the catchment area covers approximately 400,000 people), in which S. aureus was isolated. Identification was performed by Matrix-Assisted Laser Desorption/Ionization Time-of-Flight (MALDI-TOF) (Bruker Daltronik GmbH®). These isolated strains were used to test the bacterial susceptibility to OLE on agar plate, and to stablish its antibiotic susceptibility profile.
Data related to antibiotic susceptibility, sample type, location of infection, associated pathology (when possible) and patient age and gender was collected for each sample. Type of sample was classified according to standard laboratory practice as abscess, skin lesion, surgical wound, ulcer and pressure ulcer. Location was categorized as well as: generalized all body, head, hand, arm, trunk, leg, foot and toenail. The associated pathology was divided into six groups as follows: a) immunosuppression (samples associated with angiosarcoma, basal cell carcinoma and squamous cell cancer); b) surgical procedure (samples from catheter, surgery, amputation and prostheses); c) skin infection without dermatological factors (burns, insect stings, omphalitis, knife cuts, trauma and any skin and wound infection); d) skin infection with dermatological disease (epidermolysis bullosa, herpes zoster, impetigo, psoriasis and scalded skin syndrome); e) vascular disease (elephantiasis, lymphedema, lymphocele and vascular ulcer); f) pressure ulcer (immobilization); and g) diabetic foot.
4.4. OLE Bacterial Susceptibility Test on Agar Plate
The inoculum was prepared by direct saline suspension of fresh isolated colonies and adjusting the turbidity to 0.5 McFarland in a MicroScan turbidity meter (Beckman Coulter®), thus containing approximately 1-2x108 CFU/ml (colony-forming units). A sterile cotton swab was placed in the bacterial suspension and streaked in three directions over the surface of the Müller-Hinton agar (MHA) (Oxoid™) to obtain uniform growth. Then, 10 µl of the OLE was added on the surface, as well as sterile water as negative control. The concentrations of OLE tested were 25% w/v, 12.5% w/v, 6.25% w/v and 3.125% w/v. Plates were incubated at 35°C for 24 hours [52]. The categorisation of strains as either susceptible or resistant was determined by the presence or absence of growth. For the clinical samples, at least two different aliquots of OLE were tested.
4.5. Minimum Bactericidal Concentration (MBC)
The MBC of OLE was determined for the two reference strains by broth microdilution method according to the Clinical Laboratory Standards Institute guidelines [53] with little variation. An inoculum of 0.5 McFarland was prepared as described above. The inoculum was diluted in Cation Adjusted Müller-Hinton Broth (CAMHB) (Becton Dickinson®) to achieve a concentration of 1x106 CFU/ml. 50 µl of the inoculum was then incubated with 50 µl of serial dilutions of OLE to a final concentration of approximately 5x105 CFU/ml per tube. The final concentrations of OLE tested were 12.5, 6.25, 3.12, 1.56 and 0.78% (w/v). The tubes were incubated for 18-20 hours at 35°C. After that, the 100 µl were spread on CBA plates and incubated again 24 hours. The MBC was the dilution at which no growth was observed in each strain. Three different batches of OLE were tested.
4.6. Lethal Curve
The protocol was similar to that described for the MBC. In this case, 50 µl of the inoculum were mixed with either 50 µl of 25% w/v OLE or 50 µl of sterile water (negative control) and incubated at 35°C for 2, 4, 8 and 24 hours. Subsequently, the entire contents of the tubes were spread on CBA plates and the colonies were counted after 24-hour incubation period. Regarding the inoculum, 10 µl of a 1/10000 dilution of the inoculum was spread over the surface of a blood agar plate, the presence of approximately 100 colonies indicated an initial inoculum density of 1x108 CFU/ml, thus 5x105CFU/ml in each assay. Additionally, the negative control for each time point was also diluted and 10 µl used for the colony counting. A minimum of six replicates, comprising two different extract batches, were conducted for each strain.
4.7. Antibiotic Susceptibility
Antibiotic susceptibility testing was done by Microscan Walkway™ semi-automatic system (Beckman Coulter®), Pos MIC panel type 33 with the following antibiotics and dilutions (µg/ml) ranges according to the manufacturer (https://www.beckmancoulter.com/es/products/microbiology/conventional-panels#/): amikacin (8-32), amoxicillin/clavulanic acid (4/2-8/4), ampicillin (0.25, 4-8), ceftaroline (0.5-1), chloramphenicol (8-16), ciprofloxacin (1-2), clindamycin (0.25-2), daptomycin (1-4), erythromycin (0.5-4), fosfomycin (32-64), fusidic acid (2), gentamicin (1-8), imipenem (4-8), levofloxacin (1-4), linezolid (1-4), minocycline (1-8), moxifloxacin (0.5-1), mupirocin (256), nitrofurantoin (32-64), norfloxacin (4-8), oxacillin (0.25-2), penicillin (0.12-0.25, 8), pristinamycin (1-2), rifampin (0.5-2), synercid (quinupristin-dalfopristin) (1-4), teicoplanin (1-16), tetracycline (1-8), tobramycin (1-8), trimethoprim/sulfamethoxazole (2/38-4/76) and vancomycin (0.25-16). For some samples only disk diffusion susceptibility test was done, using disks of: fusidic acid (10 µg), cefoxitin (30 µg), ciprofloxacin (5 µg), clindamycin (2 µg), erythromycin (15 µg), gentamicin (10 µg), linezolid (10 µg), mupirocin (200 µg), rifampicin (5 µg), tetracycline (30 µg), oxacillin (1 µg) and trimethoprim-sulfamethoxazole (25 µg). According to EUCAST [54] the antimicrobial susceptibility was categorized as S (susceptible), I (susceptible, increased exposure) and R (resistant) for each antibiotic tested.
4.8. Statistical Analysis
The Values were expressed as mean and standard deviation (SD) or median value (P25-P75). Normality was tested by Shapiro-Wilk. Differences between the experimental groups in terms of number of colony-forming units were assessed using Students’ t- or Mann-Whitney U test depending on the normality. Differences in clinical samples regarding sample type, pathology and location with number of antibiotic resistances and age were analysed using Kruskal-Wallis test. The association between age and number of antibiotic resistances was evaluated with Pearson correlation coefficient. Two-tailed p value was considered statistically significant when p < 0.05. All analyses and graphs were carried out with the free based R software Jamovi 2.2.5 [55], MS Excel 2016 (Microsoft, WA, USA), MS PowerPoint 2016 (Microsoft, WA, USA) and MS Word 2016 (Microsoft, WA, USA). Images from visual abstract were downloaded from freepik (https://www.freepik.es/) and pixabay (https://pixabay.com/es/).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: clinical strains characterization. Table S2: phenolic profile of OLE.
Author Contributions
Conceptualization, L.C., A.R., R.M.B. and Y.G.; methodology, L.C, R.M.B., A.R., and Y.G.; software, L.C., and M.L.M.; validation, L.C.; formal analysis, L.C., M.L.M., and A.M.M.; investigation, L.C., A.T.B., A.I.L.C., J.M.G.L., B.F., N.d.V., M.A., O.M.B., I.O.S. and R.M.B.; resources, L.C., A.I.L.C., J.M.G.L.,B.F., R.M.B., J.O., A.R. and Y.G.; data curation, L.C.; writing – original draft preparation, L.C.; writing – review & editing, M.L.M., A.M.M., A.T.B., A.I.L.C., J.M.G.L., B.F., N.d.V., M.A., O.M.B., I.O.S., R.M.B., J.O., A.R., and Y.G.; supervision, A.M.M., A.R., and Y.G.; visualization, L.C.; project administration, A.R. and Y.G.; funding acquisition, J.O., A.R. and Y.G. All authors have read and agreed to the published version of the manuscript.
Funding
Laura Clusa holds a postdoctoral contract from Plan de Recuperación, Transformación y Resiliencia (Instituto de Salud Carlos III, Ministerio de Ciencia, Innovación y Universidades) from Unión Europea-NextGeneration EU, grant number Sara Borrell CD22/00152. This research was funded by The Ministerio de Ciencia e Innovación-Fondo Europeo de Desarrollo Regional grant number PID2022-136414OB-I00, by Spanish Ministry of Science and Innovation with funds from the European Union NextGeneration EU, from the Recovery, Transformation and Resilience Plan grant number PRTR-C17.I1, by Interreg Sudoe Program grant number NEWPOWER, S1/1.1/E01116, by CIBER Fisiopatología de la Obesidad y la Nutrición as an initiative of FEDER-ICCIII grant number CIBEROBN, CB06/03/1012, by Fondo Social Europeo-Gobierno de Aragón grant number research groups: B10_23R, B16_23R and B59_23D.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Autonomous Community of Aragon (protocol code C.I. PI24/316, approval date 10/07/2024 and updated on 25/09/2024 and 18/12/2024).
Informed Consent Statement
Patient consent was waived due to the use of historical samples.
Data Availability Statement
Acknowledgments
We are kindly grateful to the Microbiology Department at Miguel Servet University Hospital for providing the clinical samples, and especially to the technicians Carmen Guerrero and Rebeca Fernández for performing the routine antibiotic susceptibility tests on the clinical samples.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| SSTIs | Skin and soft tissue infections |
| MSSA | Methicillin-sensitive Staphylococcus aureus |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| OLE | Olive leaf extract |
| MBC | Minimum bactericidal concentration |
| CFU | Colony-forming units |
| AMR | Antimicrobial resistance |
| UVB | Ultraviolet B |
| IQR | Interquartile range |
| DF | Diabetic foot |
| IS | Immunosuppression |
| PU | Pressure ulcer |
| SIWDD | Skin infection with dermatological disease |
| SIWODF | Skin infection without dermatological factors |
| SP | Surgical procedure |
| VD | Vascular disease |
| ATCC | American Type Culture Collection |
| EUCAST | European Committee on Antimicrobial Susceptibility Testing |
| MIC | Minimum inhibitory concentration |
| CBA | Columbia blood agar |
| MALDI-TOF | Matrix-Assisted Laser Desorption/Ionization Time-of-Flight |
| MHA | Müller-Hinton agar |
| CAMHB | Cation Adjusted Müller-Hinton Broth |
| SD | Standard deviation |
| UPLC-MS/MS | Ultra-Performance liquid chromatography/tandem mass spectrometry system |
References
- Ikuta, K.S.; Swetschinski, L.R.; Robles Aguilar, G.; Sharara, F.; Mestrovic, T.; Gray, A.P.; Davis Weaver, N.; Wool, E.E.; Han, C.; Gershberg Hayoon, A.; et al. Global Mortality Associated with 33 Bacterial Pathogens in 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. The Lancet 2022, 400, 2221–2248. [CrossRef]
- Gehrke, A.-K.E.; Giai, C.; Gómez, M.I. Staphylococcus Aureus Adaptation to the Skin in Health and Persistent/Recurrent Infections. Antibiotics 2023, 12, 1520. [CrossRef]
- Schachner, L.A.; Andriessen, A.; Gonzalez, M.E.; Lal, K.; Hebert, A.A.; Eichenfield, L.F.; Lio, P. A Consensus on Staphylococcus Aureus Exacerbated Atopic Dermatitis and the Need for a Novel Treatment. J Drugs Dermatol. 2024, 23, 825–832. [CrossRef]
- Tomi, N.S.; Kränke, B.; Aberer, E. Staphylococcal Toxins in Patients with Psoriasis, Atopic Dermatitis, and Erythroderma, and in Healthy Control Subjects. Journal of the American Academy of Dermatology 2005, 53, 67–72. [CrossRef]
- Linz, M.S.; Mattappallil, A.; Finkel, D.; Parker, D. Clinical Impact of Staphylococcus Aureus Skin and Soft Tissue Infections. Antibiotics 2023, 12, 557. [CrossRef]
- Ki, V.; Rotstein, C. Bacterial Skin and Soft Tissue Infections in Adults: A Review of Their Epidemiology, Pathogenesis, Diagnosis, Treatment and Site Of Care. Canadian Journal of Infectious Diseases and Medical Microbiology 2008, 19, 173–184. [CrossRef]
- Frazee, B.W.; Lynn, J.; Charlebois, E.D.; Lambert, L.; Lowery, D.; Perdreau-Remington, F. High Prevalence of Methicillin-Resistant Staphylococcus Aureus in Emergency Department Skin and Soft Tissue Infections. Annals of Emergency Medicine 2005, 45, 311–320. [CrossRef]
- King, M.D.; Humphrey, B.J.; Wang, Y.F.; Kourbatova, E.V.; Ray, S.M.; Blumberg, H.M. Emergence of Community-Acquired Methicillin-Resistant Staphylococcus Aureus USA 300 Clone as the Predominant Cause of Skin and Soft-Tissue Infections. Ann Intern Med 2006, 144, 309–317.
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. The Lancet 2022, 399, 629–655. [CrossRef]
- European Centre for Disease Prevention and Control Antimicrobial Resistance in the EU-EEA (EARS-Net) Annual Epidemiological Report for 2021; ECDC: Stockholm, 2022; p. 20;.
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. IDR 2019, Volume 12, 3903–3910. [CrossRef]
- Hashmi, M.A.; Khan, A.; Hanif, M.; Farooq, U.; Perveen, S. Traditional Uses, Phytochemistry, and Pharmacology of Olea Europaea (Olive). Evidence-Based Complementary and Alternative Medicine 2015, 2015, 1–29. [CrossRef]
- Cabrera-Vique, C.; Navarro-Alarcón, M.; Rodríguez Martínez, C.; Fonollá-Joya, J. Efecto hipotensor de un extracto de componentes bioactivos de hojas de olivo: estudio clínico preliminar. Nutrición Hospitalaria 2015, 242–249. [CrossRef]
- Ismail, M.A.; Norhayati, M.N.; Mohamad, N. Olive Leaf Extract Effect on Cardiometabolic Profile among Adults with Prehypertension and Hypertension: A Systematic Review and Meta-Analysis. PeerJ 2021, 9, e11173. [CrossRef]
- Lins, P.G.; Marina Piccoli Pugine, S.; Scatolini, A.M.; De Melo, M.P. In Vitro Antioxidant Activity of Olive Leaf Extract (Olea Europaea L.) and Its Protective Effect on Oxidative Damage in Human Erythrocytes. Heliyon 2018, 4, e00805. [CrossRef]
- Wainstein, J.; Ganz, T.; Boaz, M.; Bar Dayan, Y.; Dolev, E.; Kerem, Z.; Madar, Z. Olive Leaf Extract as a Hypoglycemic Agent in Both Human Diabetic Subjects and in Rats. Journal of Medicinal Food 2012, 15, 605–610. [CrossRef]
- Goldsmith, C.D.; Bond, D.R.; Jankowski, H.; Weidenhofer, J.; Stathopoulos, C.E.; Roach, P.D.; Scarlett, C.J. The Olive Biophenols Oleuropein and Hydroxytyrosol Selectively Reduce Proliferation, Influence the Cell Cycle, and Induce Apoptosis in Pancreatic Cancer Cells. IJMS 2018, 19, 1937. [CrossRef]
- Karygianni, L.; Cecere, M.; Skaltsounis, A.L.; Argyropoulou, A.; Hellwig, E.; Aligiannis, N.; Wittmer, A.; Al-Ahmad, A. High-Level Antimicrobial Efficacy of Representative Mediterranean Natural Plant Extracts against Oral Microorganisms. BioMed Research International 2014, 2014, 1–8. [CrossRef]
- Markin, D.; Duek, L.; Berdicevsky, I. In Vitro Antimicrobial Activity of Olive Leaves. Antimikrobielle Wirksamkeit von Olivenblättern in Vitro. Mycoses 2003, 46, 132–136. [CrossRef]
- Sudjana, A.N.; D’Orazio, C.; Ryan, V.; Rasool, N.; Ng, J.; Islam, N.; Riley, T.V.; Hammer, K.A. Antimicrobial Activity of Commercial Olea Europaea (Olive) Leaf Extract. International Journal of Antimicrobial Agents 2009, 33, 461–463. [CrossRef]
- Zorić, N.; Kopjar, N.; Bobnjarić, I.; Horvat, I.; Tomić, S.; Kosalec, I. Antifungal Activity of Oleuropein against Candida Albicans—The In Vitro Study. Molecules 2016, 21, 1631. [CrossRef]
- Borjan, D.; Leitgeb, M.; Knez, Ž.; Hrnčič, M.K. Microbiological and Antioxidant Activity of Phenolic Compounds in Olive Leaf Extract. Molecules 2020, 25, 5946. [CrossRef]
- Pereira, A.P.; Ferreira, I.C.; Marcelino, F.; Valentão, P.; Andrade, P.B.; Seabra, R.; Estevinho, L.; Bento, A.; Pereira, J.A. Phenolic Compounds and Antimicrobial Activity of Olive (Olea Europaea L. Cv. Cobrançosa) Leaves. Molecules 2007, 12, 1153–1162. [CrossRef]
- Ayana, B.; Turhan, K.N. Use of Antimicrobial Methylcellulose Films to Control Staphylococcus Aureus during Storage of Kasar Cheese. Packag Technol Sci 2009, 22, 461–469. [CrossRef]
- Ahmed, A.M.; Rabii, N.S.; Garbaj, A.M.; Abolghait, S.K. Antibacterial Effect of Olive (Olea Europaea L.) Leaves Extract in Raw Peeled Undeveined Shrimp (Penaeus Semisulcatus). International Journal of Veterinary Science and Medicine 2014, 2, 53–56. [CrossRef]
- Liu, Y.; McKeever, L.C.; Malik, N.S.A. Assessment of the Antimicrobial Activity of Olive Leaf Extract Against Foodborne Bacterial Pathogens. Front. Microbiol. 2017, 8. [CrossRef]
- Melguizo-Rodríguez, L.; González-Acedo, A.; Illescas-Montes, R.; García-Recio, E.; Ramos-Torrecillas, J.; Costela-Ruiz, V.J.; García-Martínez, O. Biological Effects of the Olive Tree and Its Derivatives on the Skin. Food Funct. 2022, 13, 11410–11424. [CrossRef]
- Torrecillas-Baena, B.; Camacho-Cardenosa, M.; Carmona-Luque, M.D.; Dorado, G.; Berenguer-Pérez, M.; Quesada-Gómez, J.M.; Gálvez-Moreno, M.Á.; Casado-Díaz, A. Comparative Study of the Efficacy of EHO-85, a Hydrogel Containing Olive Tree (Olea Europaea) Leaf Extract, in Skin Wound Healing. IJMS 2023, 24, 13328. [CrossRef]
- Sumiyoshi, M.; Kimura, Y. Effects of Olive Leaf Extract and Its Main Component Oleuroepin on Acute Ultraviolet B Irradiation-induced Skin Changes in C57BL/6J Mice. Phytotherapy Research 2010, 24, 995–1003. [CrossRef]
- Mehraein, F.; Sarbishegi, M.; Aslani, A. Evaluation of Effect of Oleuropein on Skin Wound Healing in Aged Male Balb/c Mice. Cell Journal 2014, 16, 25–30.
- Elnahas, R.A.; Elwakil, B.H.; Elshewemi, S.S.; Olama, Z.A. Egyptian Olea Europaea Leaves Bioactive Extract: Antibacterial and Wound Healing Activity in Normal and Diabetic Rats. Journal of Traditional and Complementary Medicine 2021, 11, 427–434. [CrossRef]
- Zamanifard, M.; Nasiri, M.; Yarahmadi, F.; Zonoori, S.; Razani, O.; Salajegheh, Z.; Imanipour, M.; Mohammadi, S.M.; Jomehzadeh, N.; Asadi, M. Healing of Diabetic Foot Ulcer with Topical and Oral Administrations of Herbal Products: A Systematic Review and Meta-analysis of Randomized Controlled Trials. International Wound Journal 2024, 21, e14760. [CrossRef]
- Mehrabi Rad, F.; Changaee, F.; Toulabi, T.; Yari, F.; Rashidipour, M.; Mohammadi, R.; Yarahmadi, S.; Almasian, M. The Efficacy of Combined Olive Leaf and Curcumin Extract on Healing Human Papillomavirus: A Randomized Clinical Trial. Evidence-Based Complementary and Alternative Medicine 2023, 2023, 2001770. [CrossRef]
- Toulabi, T.; Delfan, B.; Rashidipour, M.; Yarahmadi, S.; Ravanshad, F.; Javanbakht, A.; Almasian, M. The Efficacy of Olive Leaf Extract on Healing Herpes Simplex Virus Labialis: A Randomized Double-Blind Study. EXPLORE 2022, 18, 287–292. [CrossRef]
- Hiramatsu, K.; Ito, T.; Tsubakishita, S.; Sasaki, T.; Takeuchi, F.; Morimoto, Y.; Katayama, Y.; Matsuo, M.; Kuwahara-Arai, K.; Hishinuma, T.; et al. Genomic Basis for Methicillin Resistance in Staphylococcus Aureus. Infect Chemother 2013, 45, 117. [CrossRef]
- Laurent, F. Fitness and Competitive Growth Advantage of New Gentamicin-Susceptible MRSA Clones Spreading in French Hospitals. Journal of Antimicrobial Chemotherapy 2001, 47, 277–283. [CrossRef]
- Stevens, C.E.; Deventer, A.T.; Johnston, P.R.; Lowe, P.T.; Boraston, A.B.; Hobbs, J.K. Staphylococcus Aureus COL: An Atypical Model Strain of MRSA That Exhibits Slow Growth and Antibiotic Tolerance 2024.
- Li, X.; Liu, Y.; Jia, Q.; LaMacchia, V.; O’Donoghue, K.; Huang, Z. A Systems Biology Approach to Investigate the Antimicrobial Activity of Oleuropein. Journal of Industrial Microbiology and Biotechnology 2016, 43, 1705–1717. [CrossRef]
- Silvan, J.M.; Guerrero-Hurtado, E.; Gutierrez-Docio, A.; Prodanov, M.; Martinez-Rodriguez, A.J. Olive Leaf as a Source of Antibacterial Compounds Active against Antibiotic-Resistant Strains of Campylobacter Jejuni and Campylobacter Coli. Antibiotics 2023, 12, 26. [CrossRef]
- Kim, S.; Lee, H.; Lee, S.; Yoon, Y.; Choi, K.-H. Antimicrobial Action of Oleanolic Acid on Listeria Monocytogenes, Enterococcus Faecium, and Enterococcus Faecalis. PLoS ONE 2015, 10, e0118800. [CrossRef]
- Carraro, L.; Fasolato, L.; Montemurro, F.; Martino, M.E.; Balzan, S.; Servili, M.; Novelli, E.; Cardazzo, B. Polyphenols from Olive Mill Waste Affect Biofilm Formation and Motility in Escherichia Coli K-12. Microbial Biotechnology 2014, 7, 265–275. [CrossRef]
- Lim, A.; Subhan, N.; Jazayeri, J.A.; John, G.; Vanniasinkam, T.; Obied, H.K. Plant Phenols as Antibiotic Boosters: In Vitro Interaction of Olive Leaf Phenols with Ampicillin. Phytotherapy Research 2016, 30, 503–509. [CrossRef]
- Cela, E.M.; Urquiza, D.; Gómez, M.I.; Gonzalez, C.D. New Weapons to Fight against Staphylococcus Aureus Skin Infections. Antibiotics 2023, 12, 1477. [CrossRef]
- Habib, A.; Qadir, A. Frequency and Antibiotic Susceptibility Pattern of Community-Associated Methicillin-Resistant Staphylococcus Aureus (CA-MRSA) in Uncomplicated Skin and Soft Tissue Infections. J Coll Physicians Surg Pak 2022, 32, 1398–1403. [CrossRef]
- Manzur, A.; Gavalda, L.; Ruiz De Gopegui, E.; Mariscal, D.; Dominguez, M.A.; Perez, J.L.; Segura, F.; Pujol, M. Prevalence of Methicillin-Resistant Staphylococcus Aureus and Factors Associated with Colonization among Residents in Community Long-Term-Care Facilities in Spain. Clinical Microbiology and Infection 2008, 14, 867–872. [CrossRef]
- Tognetti, L.; Martinelli, C.; Berti, S.; Hercogova, J.; Lotti, T.; Leoncini, F.; Moretti, S. Bacterial Skin and Soft Tissue Infections: Review of the Epidemiology, Microbiology, Aetiopathogenesis and Treatment: A Collaboration between Dermatologists and Infectivologists. Acad Dermatol Venereol 2012, 26, 931–941. [CrossRef]
- Kaushik, A.; Kest, H.; Sood, M.; Steussy, B.; Thieman, C.; Gupta, S. Biofilm Producing Methicillin-Resistant Staphylococcus Aureus (MRSA) Infections in Humans: Clinical Implications and Management. Pathogens 2024, 13, 76. [CrossRef]
- Porras-Luque, J.I. Antimicrobianos tópicos en Dermatología. Actas Dermo-Sifiliográficas 2007, 98, 29–39. [CrossRef]
- Zabielinski, M.; McLeod, M.P.; Aber, C.; Izakovic, J.; Schachner, L.A. Trends and Antibiotic Susceptibility Patterns of Methicillin-Resistant and Methicillin-Sensitive Staphylococcus Aureus in an Outpatient Dermatology Facility. JAMA Dermatol 2013, 149, 427. [CrossRef]
- Zhanel, G.G.; Adam, H.J.; Baxter, M.; Lagace-Wiens, P.R.S.; Karlowsky, J.A. In Vitro Activity and Resistance Rates of Topical Antimicrobials Fusidic Acid, Mupirocin and Ozenoxacin against Skin and Soft Tissue Infection Pathogens Obtained across Canada (CANWARD 2007–18). Journal of Antimicrobial Chemotherapy 2021, 76, 1808–1814. [CrossRef]
- Martínez-Beamonte, R.; Barranquero, C.; Gascón, S.; Mariño, J.; Arnal, C.; Estopañán, G.; Rodriguez-Yoldi, M.J.; Surra, J.C.; Martín-Belloso, O.; Odriozola-Serrano, I.; et al. Effect of Virgin Olive Oil as Spreadable Preparation on Atherosclerosis Compared to Dairy Butter in Apoe-Deficient Mice. J Physiol Biochem 2024, 80, 671–683. [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI) Performance Standards for Antimicrobial Disk Susceptibility Test; Approved Standards- Twelfth Edition; Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087 USA, 2015; ISBN 978-1-56238-985-7.
- Clinical and Laboratory Standards Institute (CLSI) Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard - Ninth Edition; Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2012; ISBN 978-1-56238-783-9.
- Eucast: S, I and R Definitions Available online: https://www.eucast.org/newsiandr (accessed on 23 September 2024).
- The Jamovi Project 2022.
Figure 1 .
Box plots. A) Age per associated pathology, B) Age per type of sample, C) Number of antibiotic resistances per strain (MSSA and MRSA), and D) Number of antibiotic resistance strains per type of sample. Statistically differences among groups are shown (*p value< 0.05, **p value < 0.01 and *** p value < 0.001). DF: diabetic foot, IS: immunosuppression, PU: pressure ulcer, immobilization, SIWDD: skin infection with dermatological disease, SIWODF: skin infection without dermatological factors, SP: surgical procedure and VD: vascular disease.
Figure 1 .
Box plots. A) Age per associated pathology, B) Age per type of sample, C) Number of antibiotic resistances per strain (MSSA and MRSA), and D) Number of antibiotic resistance strains per type of sample. Statistically differences among groups are shown (*p value< 0.05, **p value < 0.01 and *** p value < 0.001). DF: diabetic foot, IS: immunosuppression, PU: pressure ulcer, immobilization, SIWDD: skin infection with dermatological disease, SIWODF: skin infection without dermatological factors, SP: surgical procedure and VD: vascular disease.
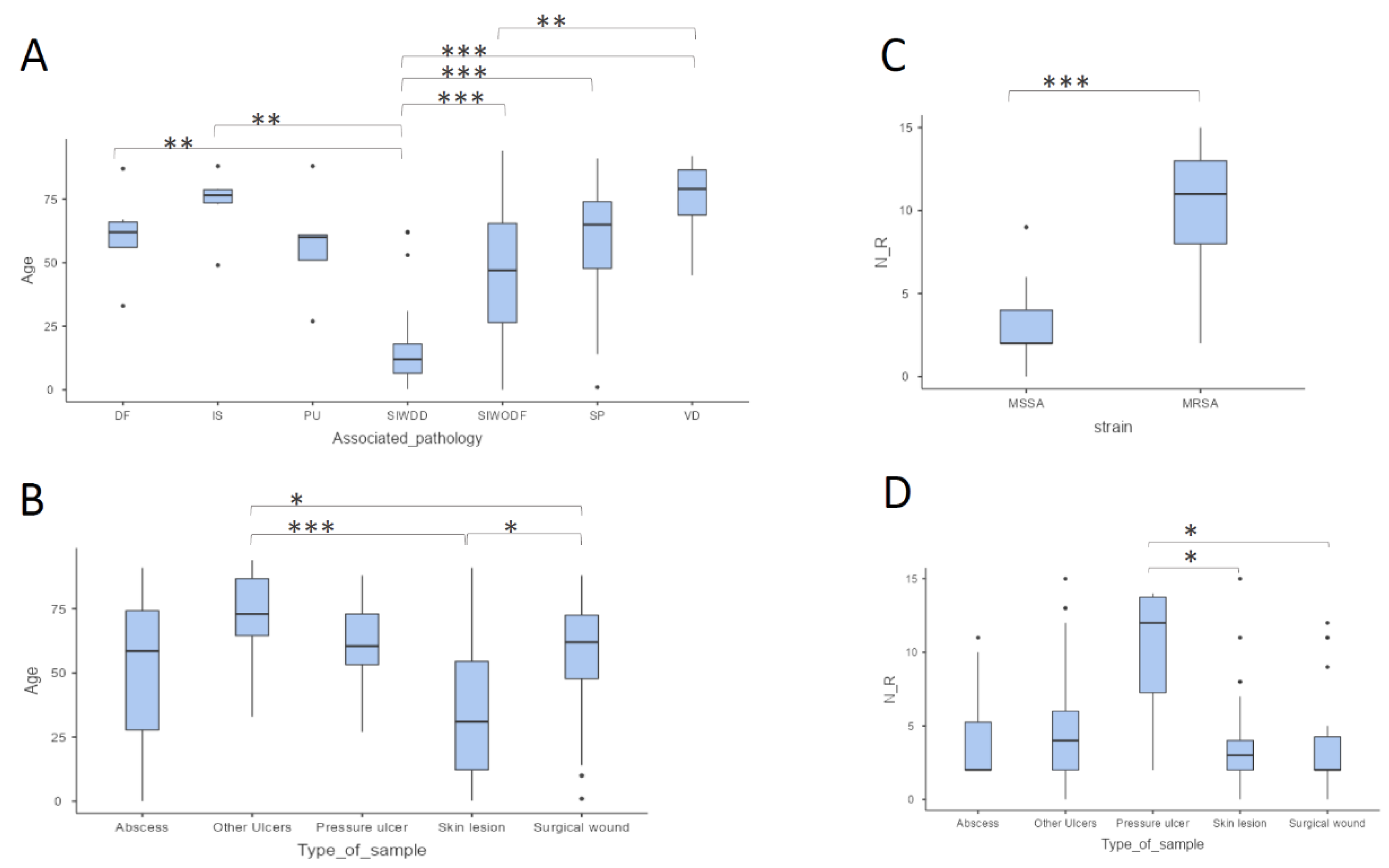
Figure 2.
Scatter plot of age (years) versus number of antibiotic resistances (N_R) in MRSA isolates.
Figure 2.
Scatter plot of age (years) versus number of antibiotic resistances (N_R) in MRSA isolates.
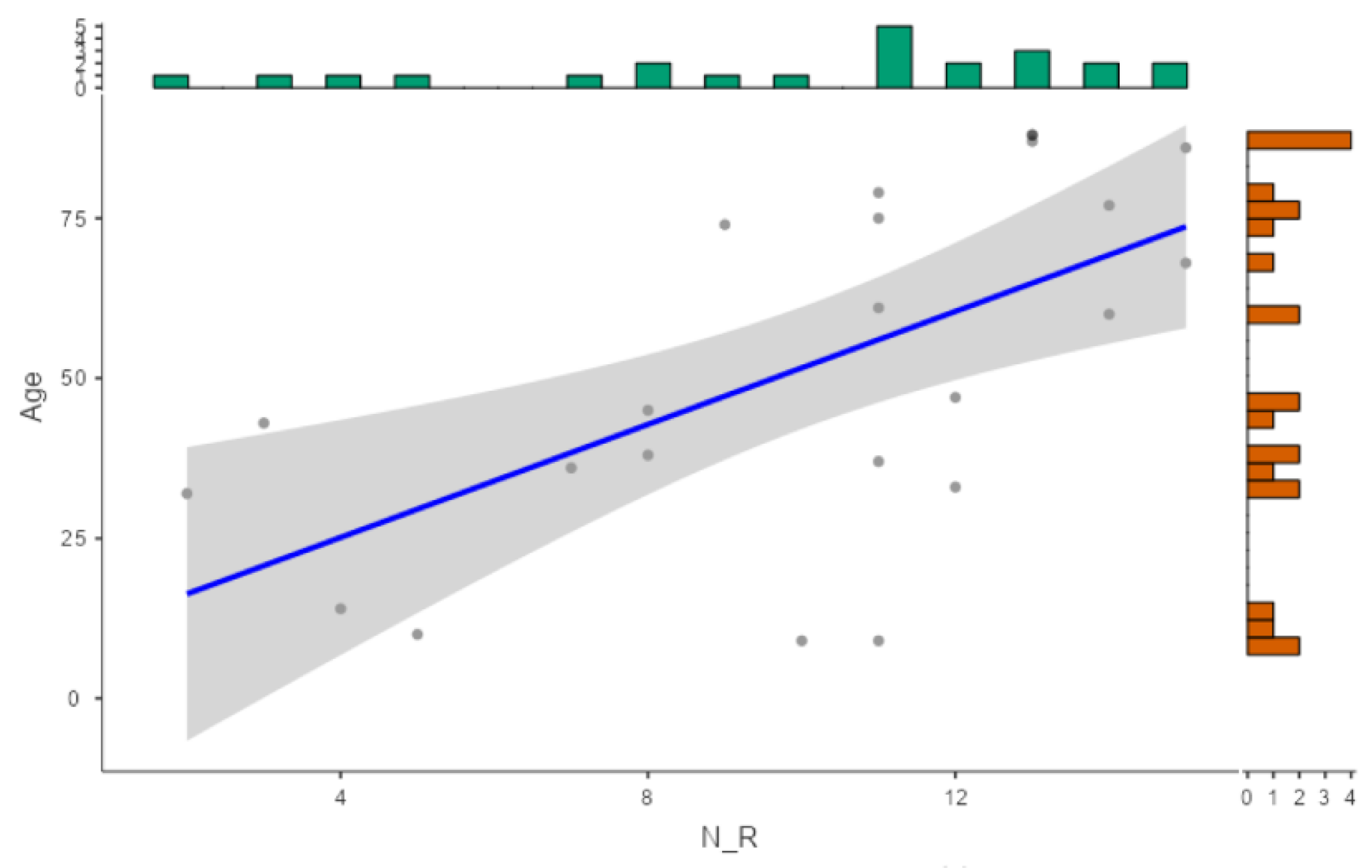
Figure 3.
Relative frequency of strains by number of antibiotic resistances classified and type of pathology. DF: diabetic foot, PU: pressure ulcer, IS: immunosuppression, SIWODF: skin infection without dermatological factors, SIWDD: skin infection with dermatology disease, SP: surgical procedure, VD: vascular disease.
Figure 3.
Relative frequency of strains by number of antibiotic resistances classified and type of pathology. DF: diabetic foot, PU: pressure ulcer, IS: immunosuppression, SIWODF: skin infection without dermatological factors, SIWDD: skin infection with dermatology disease, SP: surgical procedure, VD: vascular disease.

Figure 4.
Relative frequency of MSSA and MRSA strains classified by type of sample.
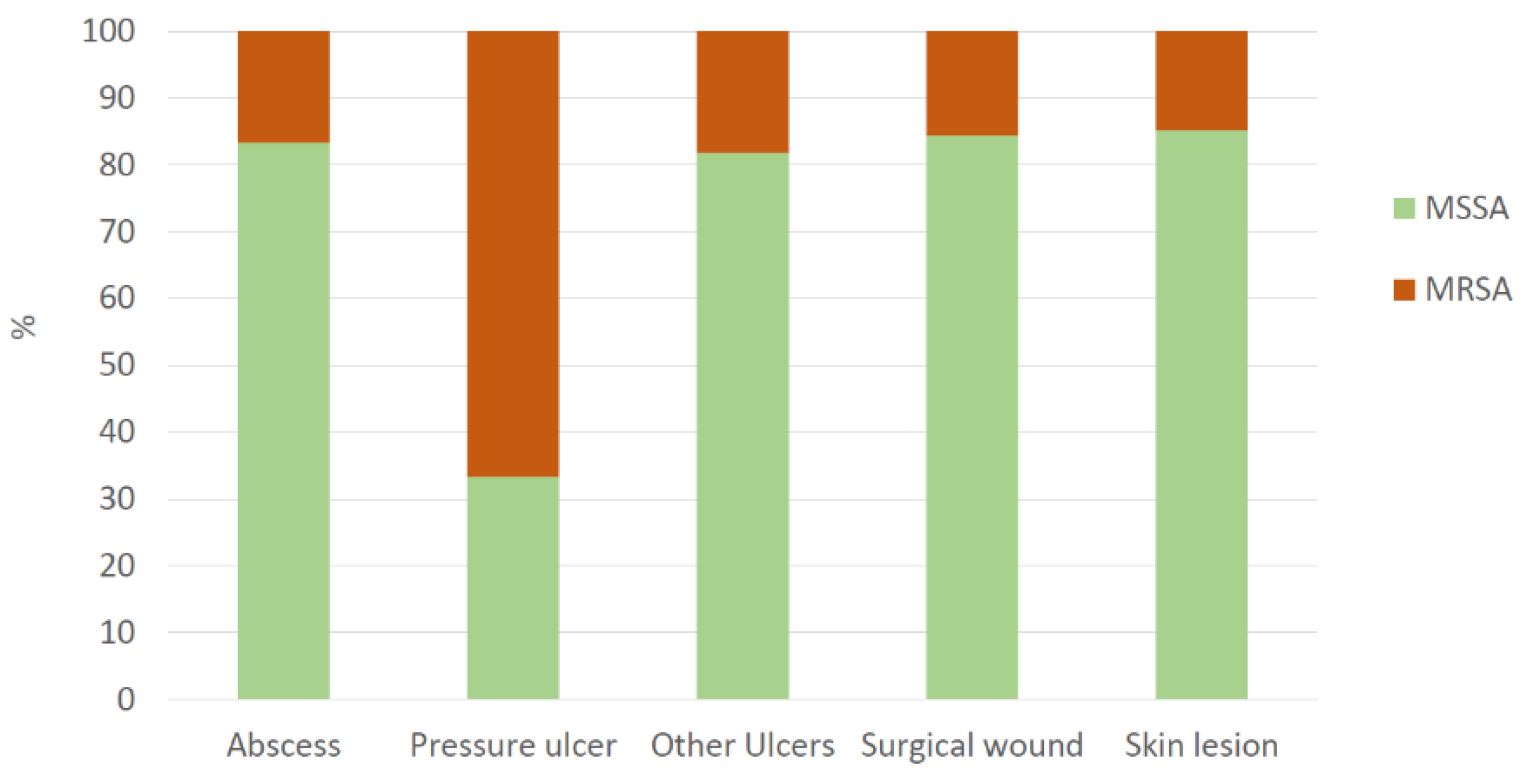
Figure 5.
Log10CFU/ml after 0, 2, 4, 8 and 24 hours treated with 12.5% w/v OLE (triangle) or distilled water (circle) for A) MSSA ATCC 29213 and (B) MRSA ATCC 700699.
Figure 5.
Log10CFU/ml after 0, 2, 4, 8 and 24 hours treated with 12.5% w/v OLE (triangle) or distilled water (circle) for A) MSSA ATCC 29213 and (B) MRSA ATCC 700699.
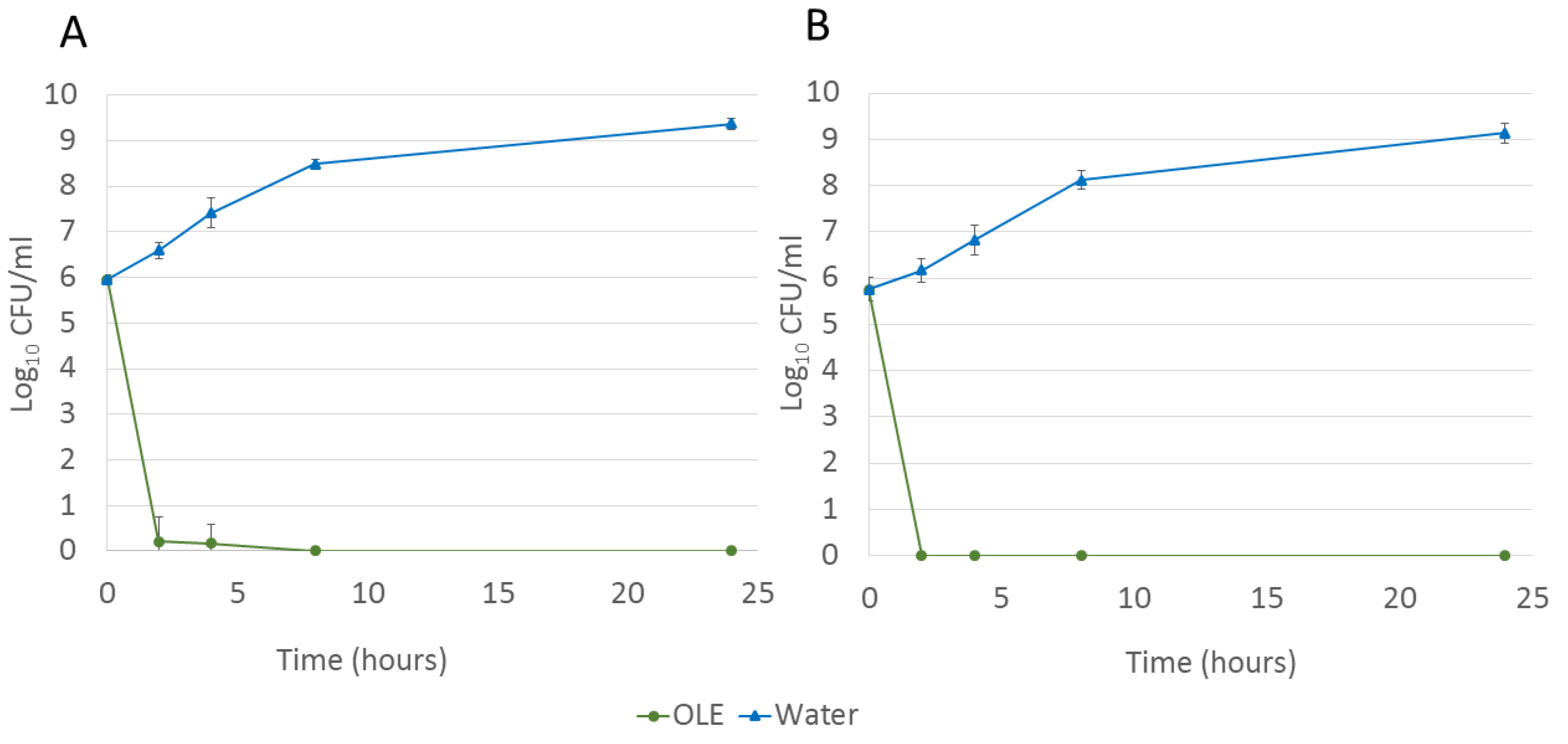
Figure 6.
Antibiotic susceptibility relative frequency. Olive leaf extract (OLE), 25 to 6.25% w/v, is shown in green.
Figure 6.
Antibiotic susceptibility relative frequency. Olive leaf extract (OLE), 25 to 6.25% w/v, is shown in green.
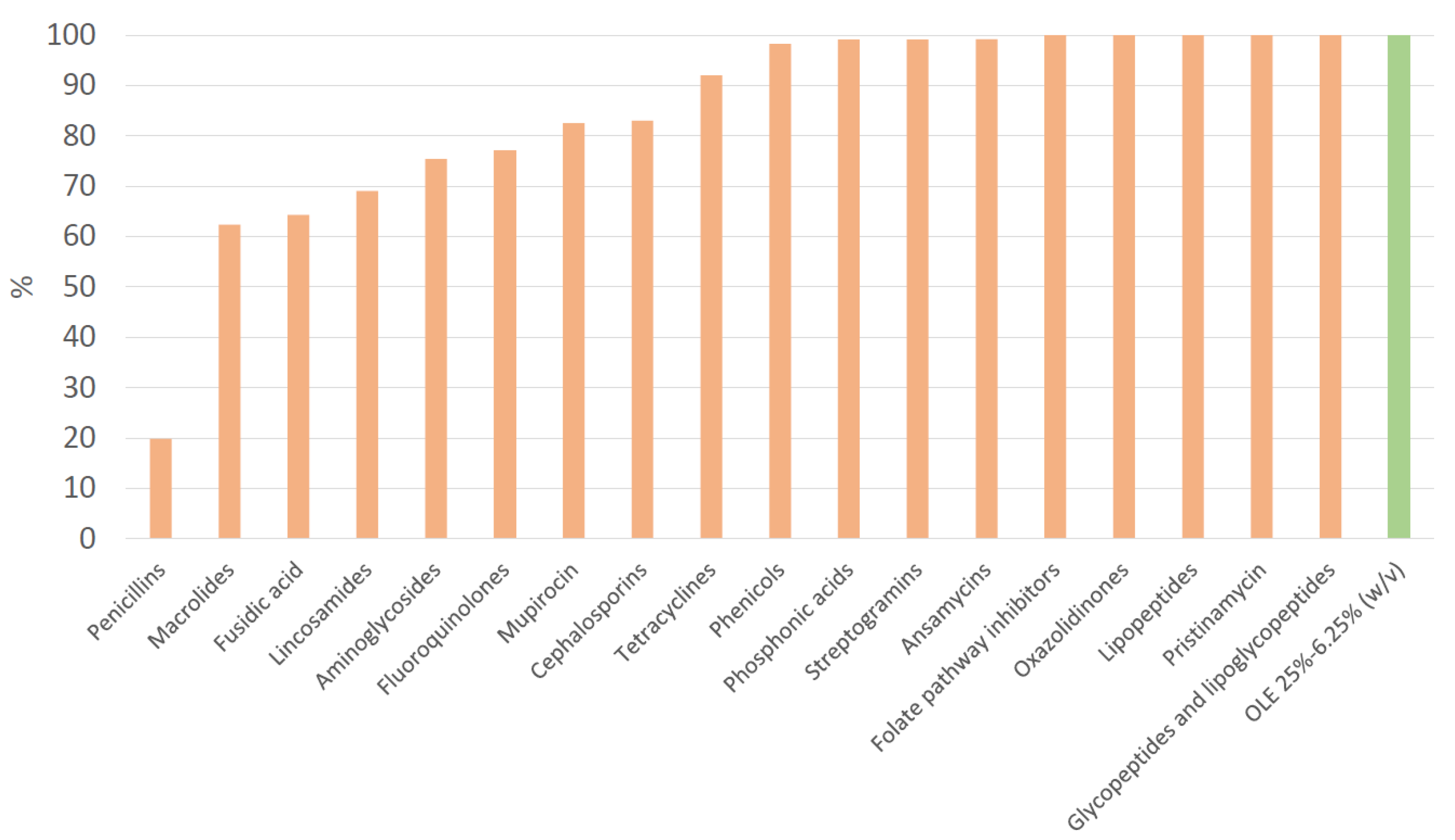

Table 1.
Descriptive characteristics of MSSA, MRSA, overall samples, age and quantity of antibiotic resistances: age range, number of antibiotic resistances, sample type, location and associated pathology.
Table 1.
Descriptive characteristics of MSSA, MRSA, overall samples, age and quantity of antibiotic resistances: age range, number of antibiotic resistances, sample type, location and associated pathology.
| MSSA N (%) | MRSA N (%) | Overall samples N (%) | Age (median (P25-P75)) |
Quantity of antibiotic resistances (median (P25-P75)) |
|
|---|---|---|---|---|---|
| 103 (81.7) | 23 (18.3) | 126 | 56.0 (27.5-73.8) | 3.0 (2.0-5.0) | |
| Gender | |||||
| Men | 63 (61.2) | 11 (47.8) | 74 (58.7) | 59.5 (25.3-72.8) | 3.5 (2.0-5.0) |
| Women | 40 (38.8) | 12 (52.2) | 52 (41.3) | 50.0 (28.5-74.8) | 3.0 (2.0-5.0) |
| Age (years) | |||||
| 0-18 | 22 (21.4) | 4 (17.4) | 26 (20.6) | 8.0 (5.0-12.8) | 3.5 (2.0-4.0) |
| 19-65 | 44 (42.7) | 10 (43.5) | 54 (42.9) | 50.0 (36.3-58.8) | 3.5 (2.0-5.0) |
| >65 | 37 (35.9) | 9 (39.1) | 46 (36.5) | 78.5 (72.3-85.3) | 2.0 (2.0-4.75) |
| Number of antibiotic resistances | |||||
| 0-5 | 97 (94.2) | 4 (17.4) | 101 (80.2) | 56.0 (20.0-72.0) | 2.0 (2.0-4.0) |
| 6-10 | 6 (5.8) | 5 (21.7) | 11 (8.7) | 45.0 (35.0-59.0) | 7.0 (6.0-8.5) |
| 11-15 | 0 (0) | 14 (60.9) | 14 (11.1) | 71.5 (50.3-84.3) | 12.5 (11.0-13.8) |
| Type of sample | |||||
| Abscess | 10 (9.7) | 2 (8.7) | 12 (9.5) | 58.5 (27.8-74.3) | 2.0 (2.0-5.25) |
| Pressure ulcer | 2 (1.9) | 4 (17.4) | 6 (4.8) | 60.5 (53.3-73.0) | 12.0 (7.25-13.8) |
| Other Ulcers | 18 (17.5) | 4 (17.4) | 22 (17.5) | 73.0 (64.5-86.8) | 4.0 (2.0-6.0) |
| Surgical wound | 27 (26.2) | 5 (21.7) | 32 (25.4) | 62.0 (47.8-72.5) | 2.0 (2.0-4.25) |
| Skin lesion | 46 (44.7) | 8 (34.8) | 54 (42.9) | 31.0 (12.3-54.5) | 3.0 (2.0-4.0) |
| Location | |||||
| Generalized (all body) | 2 (1.9) | 0 (0) | 2 (1.6) | 3.5 (3.25-3.75) | 4.5 (4.25-4.75) |
| Arm | 8 (7.8) | 2 (8.7) | 10 (7.9) | 59.0 (40.3-69.5) | 3.50 (2.0-5.0) |
| Hand | 3 (2.9) | 2 (8.7 | 5 (4.0) | 50.0 (22.0-68.0) | 5.0 (4.0-5.0) |
| Head | 21 (20.4) | 3 (13.0) | 24 (19.0) | 50.5 (18.8-73.3) | 4.0 (2.0-4.0) |
| Trunk | 21 (20.4) | 7 (30.4) | 28 (22.2) | 58.0 (30.0-68.0) | 2.5 (2.0-6.25) |
| Leg | 26 (25.2) | 3 (13.0) | 29 (23.0) | 64.0 (24.0-82.0) | 2.0 (2.0-4.0) |
| Foot | 20 (19.4) | 4 (17.4) | 24 (19.0) | 62.5 (50.0-80.5) | 3.0 (2.0-6.0) |
| Toenail | 2 (1.9) | 2 (8.7) | 4 (3.2) | 34.0 (28.0-39.5) | 2.0 (1.5-3.25) |
| Associated pathology | |||||
| Diabetic foot | 7 (6.8) | 2 (8.7) | 9 (7.1) | 62.0 (56.0-66.0) | 4.0 (2.0-6.0) |
| Immunosuppression | 4 (3.9) | 2 (8.7) | 6 (4.8) | 76.5 (73.5-78.8) | 3.5 (2.25-9.25) |
| Immobilization (Pressure ulcer) | 2 (1.9) | 3 (13.0) | 5 (4.0) | 60.0 (51.0-61.0) | 11 (6.0-13.0) |
| Skin infection w/o dermatological factors | 31 (30.1) | 8 (34.8) | 39 (31.0) | 47.0 (26.5-65.5) | 2.0 (2.0 -4.0) |
| Skin infection with dermatological disease | 22 (21.4) | 1 (4.3) | 23 (18.3) | 12.0 (6.50-18.0) | 4.0 (2.0-4.0) |
| Surgical procedure | 25 (24.3) | 3 (13.0) | 28 (22.2) | 65.0 (47.8-74.0) | 2.0 (2.0-4.0) |
| Vascular disease | 12 (11.7) | 4 (17.4) | 16 (12.7) | 79.0 (68.8-86.5) | 4 (2.75-6.5) |
Note. Data are expressed as absolute (N) and relative (%) frequencies for categorical variables, and as median and interquartile range (M (p25 – p75)) for continuous ones. MSSA: methicillin-sensitive Staphylococcus aureus, MRSA: methicillin-resistant Staphylococcus aureus, w/o: without.
Table 2.
MSSA ATCC 29213 and MRSA ATCC 700699 concentration after 0, 2, 4, 8 and 24 hours treated either with 12.5% w/v OLE or with distilled water (control).
Table 2.
MSSA ATCC 29213 and MRSA ATCC 700699 concentration after 0, 2, 4, 8 and 24 hours treated either with 12.5% w/v OLE or with distilled water (control).
| MSSA | MRSA | |||
| Control | OLE | Control | OLE | |
| 0 (hours) | 5.95 ± 0.11 | 5.95 ± 0.11 | 5.76 ± 0.25 | 5.76 ± 0.25 |
| 2 (hours) | 6.60 ± 0.18 | 0.22 ± 0.53 | 6.17 ± 0.26 | 0.00 ± 0.00 |
| 4 (hours) | 7.42 ± 0.33 | 0.17 ± 0.41 | 6.83 ± 0.33 | 0.00 ± 0.00 |
| 8 (hours) | 8.49 ± 0.10 | 0.00 ± 0.00 | 8.12 ± 0.20 | 0.00 ± 0.00 |
| 24 (hours) | 9.37 ± 0.13 | 0.00 ± 0.00 | 9.14 ± 0.22 | 0.00 ± 0.00 |
Note. Data reports Means and standard deviations (SD) of Log10CFU/ml. OLE: Olive leaf extract, MSSA: methicillin-sensitive Staphylococcus aureus, MRSA: methicillin-resistant Staphylococcus aureus.
Table 3.
Antibiotic susceptibility characterisation for overall analysed and resistant isolates, including MSSA and MRSA.
Table 3.
Antibiotic susceptibility characterisation for overall analysed and resistant isolates, including MSSA and MRSA.
| Antibiotic class | Antibiotic | Overall N | Resistant N (%) | MSSA N (%) | MRSA N (%) | p value |
|---|---|---|---|---|---|---|
| Fucidane | Fusidic acid | 28 | 10 (35.7) | 4 (22.2) | 6 (60.0) | |
| Aminoglycosides | 126 | 31 (24.6) | 17 (16.5) | 14 (60.9) | <0.001 | |
| Amikacin | 119 | 16 (13.4) | 3 (3.0) | 13 (68.4) | <0.001 | |
| Gentamicin | 126 | 13 (10.3) | 5 (4.9) | 8 (34.8) | <0.001 | |
| Tobramycin | 119 | 29 (24.4) | 17 (17.0) | 12 (63.2) | <0.001 | |
| Penicillins | 126 | 101 (80.2) | 78 (75.7) | 23 (100.0) | 0.008 | |
| Ampicillin | 119 | 97 (81.5) | 78 (78.0) | 19 (100) | 0.024 | |
| Amoxicillin/clavulanic acid | 119 | 19 (16.0) | 0 (0) | 19 (100) | <0.001 | |
| Oxacillin | 126 | 23 (18.3) | 0 (0) | 23 (100) | <0.001 | |
| Penicillin | 119 | 97 (81.5) | 78 (78) | 19 (100) | 0.024 | |
| Cephalosporins | 119 | 19 (16.0) | 0 (0.0) | 19 (100.0) | <0.001 | |
| Cefdinir | 119 | 19 (16.0) | 0 (0) | 19 (100) | <0.001 | |
| Ceftaroline* | 119 | 0 (0.0) | 0 (0) | 0 (0.0) | ||
| Fluoroquinolones | 126 | 29 (23.0) | 12 (11.7) | 17 (73.9) | <0.001 | |
| Ciprofloxacin | 126 | 28 (22.2) | 11 (10.7) | 17 (73.9) | <0.001 | |
| Levofloxacin | 119 | 24 (20.2) | 9 (9.0) | 15 (78.9) | <0.001 | |
| Moxifloxacin | 22 | 22 (100.0) | 7 (100) | 15 (100) | ||
| Lincosamides | Clindamycin | 126 | 39 (31.0) | 28 (27.2) | 11 (47.8) | |
| Macrolides | Erythromycin | 125 | 47 (37.6) | 31 (30.1) | 16 (72.7) | <0.001 |
| Streptogramins | Quinupristin-dalfopristin | 119 | 1 (0.8) | 0 (0.0) | 1 (5.3) | 0.021 |
| Oxazolidinones | Linezolid* | 126 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Tetracyclines | 126 | 10 (7.9) | 6 (5.8) | 4 (17.4) | ||
| Minocycline | 118 | 1 (0.8) | 0 (0.0) | 1 (5.3) | 0.022 | |
| Tetracycline | 126 | 10 (7.9) | 6 (5.8) | 4 (17.4) | ||
| Phenicols | Chloramphenicol | 119 | 2 (1.7) | 1 (1.0) | 1 (5.3) | |
| Lipopeptides | Daptomycin* | 119 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Phosphonic acids | Fosfomycin | 118 | 1 (0.8) | 0 (0.0) | 1 (5.3) | 0.022 |
| Mupirocin | 126 | 22 (17.5) | 13 (12.6) | 9 (39.1) | 0.002 | |
| Pristinamycin* | 119 | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Ansamycins | Rifampicin | 126 | 1 (0.8) | 0 (0.0) | 1 (4.3) | 0.034 |
| Folate pathway inhibitors | Trimethoprim-sulfamethoxazole* | 126 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Glycopeptides and lipoglycopeptides | Teicoplanin* | 119 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Vancomycin* | 119 | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Olive leaf extract | OLE 25%* | 126 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| OLE 12.5%* | 126 | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| OLE 6.25%* | 126 | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| OLE 3.125% | 126 | 119 (94.5) | 99 (96.1) | 20 (87.0) |
Note. Data are expressed as absolute (N) and relative (%) frequencies for categorical variables. P values on Chi2 test for significant differences on proportion of antibiotic resistance strains between MSSA and MRSA are shown for each antibiotic. * Antibiotics to which all strains tested were susceptible. MSSA: methicillin-sensitive Staphylococcus aureus, MRSA: methicillin-resistant Staphylococcus aureus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



