
Submitted:
05 September 2023
Posted:
06 September 2023
Read the latest preprint version here
Abstract
Traumatic brain injury (TBI) is among the leading causes of mortality and long-term impairment globally. TBI has a dynamic pathology encompassing a variety of metabolic and molecular events that occur in two phases, primary and secondary. An external forceful blow to the brain initiates the primary phase, which is followed by a secondary phase that involves the release of calcium ions (Ca2+) and the initiation of a cascade of inflammatory processes, including mitochondrial dysfunction, rise in oxidative stress, activation of glial cells, and damage to the blood-brain barrier (BBB), resulting in paracellular leakage. There is currently no FDA-approved drug for TBI, but existing approaches rely on delivering small and macromolecular treatments, which are severely constrained by the BBB, poor retention, off-target toxicity, and complex pathology of TBI. Therefore, there is a demand for innovative and alternative therapeutics with effective delivery tactics for diagnosis and treatment of TBI. Tissue engineering and use of biomaterials is one such alternative approach. With this approach, neuronal stem cell therapy is combined with synthetically generated tissue materials such as hydrogels, self-assembling peptides, and electrospun nanofibers, which may induce neurite outgrowth, differentiation of human neural stem cells, and nerve gap bridging in TBI. This review examines tissue engineering and the use of biomaterials as potential treatments for TBI, including their synthesis, mechanisms of action, and limitations. The review also discusses challenges facing tissue engineering and biomaterial technology including survival rate of transplanted stem cells and the development of biodegradable, biocompatible, and mechanically flexible biomaterials. A better understanding of the mechanisms and drawbacks of these novel therapeutic approaches will help guide the design of future TBI therapies.
Keywords:
Traumatic brain injury
; TBI
; Biomaterials
; hydrogels
; self-assembling peptides
; electrospinning
1. Introduction
Globally, traumatic Brain Injury (TBI) is one of the prime causes of mortality and long-term physical and cognitive disabilities. The global incidence of TBI is estimated at a rate of 939 per 10,000 individuals, and these are most often caused by falls, motor vehicle accidents, wars, and sports [1,2,3,4,5]. TBI is more frequent in low- and middle-income countries, severely affecting young people and adolescents [1,2,3,4,6].The effects of TBI can have a considerable impact on a patient's quality of life, with its consequences persisting for a prolonged period of time after the injury. TBI survivors often face significant socioeconomic consequences, such as job loss and divorce, further contributing to the economic burden of TBI [7,8]. Furthermore, epilepsy, sleep difficulties, neurodegenerative illnesses, neuroendocrine dysregulation, and psychological issues are all subsequent pathological symptoms caused by a single TBI or repeated insults to the brain [9,10,11,12,13]. In a study of American army soldiers who reported symptoms post-TBI, more than 17% of participants had positive diagnosis for post-traumatic stress syndrome [14]. Notably, TBI may precipitate Alzheimer's disease, Parkinson's disease, or total cognitive impairment [15,16].
TBI severity is determined by the primary injury, which is the most important prognostic factor [17]. Depending on the degree of neurological damage, TBI is classified as mild, moderate, or severe. At least 75% of all TBIs recorded in the United States are categorized as minor or mild concussions, covering the spectrum of mild TBI (mTBI) [18]. While mTBI patients usually recover on their own, within days to months, it is important to note that a significant percentage of patients, ranging from 30% to 53%, may continue to experience disabling symptoms for at least a year following brain injury [19,20]. The complex pathology of TBI develops at the time of mechanical impact and initial injury to the brain, constituting the primary phase, and continues to evolve over time through the secondary phase. The primary phase is triggered immediately by an external mechanical insult such as acceleration, deceleration, or rotational forces, while the secondary phase may occur minutes or days after the primary injury [21,22]. Primary injury usually manifests as elevated intracranial pressure, nerve damage, vascular damage, tissue swelling, and hypoxic damage [23]. Secondary brain injury follows and is triggered through a variety of molecular and cellular events that include oxidative stress, neuronal excitotoxicity, mitochondrial dysfunction, inflammation, edema, and neuronal cell death, all leading to further cerebral damage [21,22]. Table 1 provides a synopsis of the main highlights concerning TBI.

Table 1.
Main highlights concerning Traumatic Brain Injury (TBI).
| Key highlights of TBI |
|
In response to a physical force, the white matter of the brain deforms, leading to diffuse axonal damage and release of calcium ions (Ca2+) from intracellular stores [24,25]. After excessive release of excitatory neurotransmitters such as glutamate, post-synaptic terminals become depolarized due to an influx of Ca2+, thereby resulting in hypermetabolism, which eventually leads to metabolic depression lasting several days [26,27]. High Ca2+ levels lead to disruption of several intracellular functions including the generation of a state of cellular hypoxia. Under hypoxia, the brain is compelled to switch to glycolytic metabolism, which leads to the accumulation of lactic acid [20]. Mitochondria play a crucial role in TBI pathology. Increased Ca2+ concentration induces excess mitochondrial Ca2+ absorption, leading to mitochondrial membrane permeabilization, mitochondrial dysfunction, and an enhanced state of oxidative stress illustrated by generation of reactive oxygen species (ROS) [28]. Oxidative stress contributes to exacerbation of other TBI-associated pathologic pathways, such as cytoskeletal damage, via calpain activation, and neuroinflammation, via glial cell activation [29,30]. After a brain injury, oxidative stress changes the crucial architecture of tight junction proteins at the blood-brain barrier (BBB), which is one of the most vital components of a healthy brain, acting as a barrier between the central nervous system (CNS) and the rest of the body [31]. Breaching of the BBB in TBI results in increased paracellular leakage [32]. The harsh microenvironment near the lesion site mainly drives the transformation of activated native neural stem cells (NSCs) into astrocytes. This process also results in the formation of glial fibrosis that seals the cavities [33]. Consequently, this tissue obstructs the transfer of electrical signals in functioning nerve cells at the affected site [34], and acts as a major physical barrier of axonal regeneration which impedes recovery [35]. Astrocytes further promote BBB rupture after TBI by activating paracellular channels, physically disrupting astrocyte-endothelial junctions, and digesting BBB matrix proteins [36,37]. TBI-induced disruption of the BBB significantly contributes to TBI pathology, but may be exploited to pass therapeutics through the damaged BBB.
Despite gradual advances in TBI treatment, long-term damage following TBI remains a substantial healthcare concern. As of now, the Food and Drug Administration (FDA) has not approved any drugs to treat TBI. The current standard of care for patients with moderate to severe TBI includes ventilation and oxygenation interventions, fluid management, hypothermic stimulation, intracranial pressure (ICP) control, cerebral perfusion pressure (CPP), blood pressure (BP) management, nutrition and glucose level management, and surgery [38]. Many of the available diagnostic and treatment options are limited by the exceedingly complicated pathology that follows a brain injury. Importantly, the BBB, which primarily governs material access into the brain, inhibits the entry of micro and macromolecular therapies [39]. As a result, TBI therapy by systemic or local delivery of medications are mostly ineffective [40,41,42]. Hence, current therapeutic approaches are often constrained by two major obstacles: 1) ineffective delivery and retention, restricting therapeutic thresholds, and 2) off-target toxicity induced by treatments that target receptors of biochemical derangements rather than the biochemical derangements themselves, resulting in loss of function in off-target cells [43].
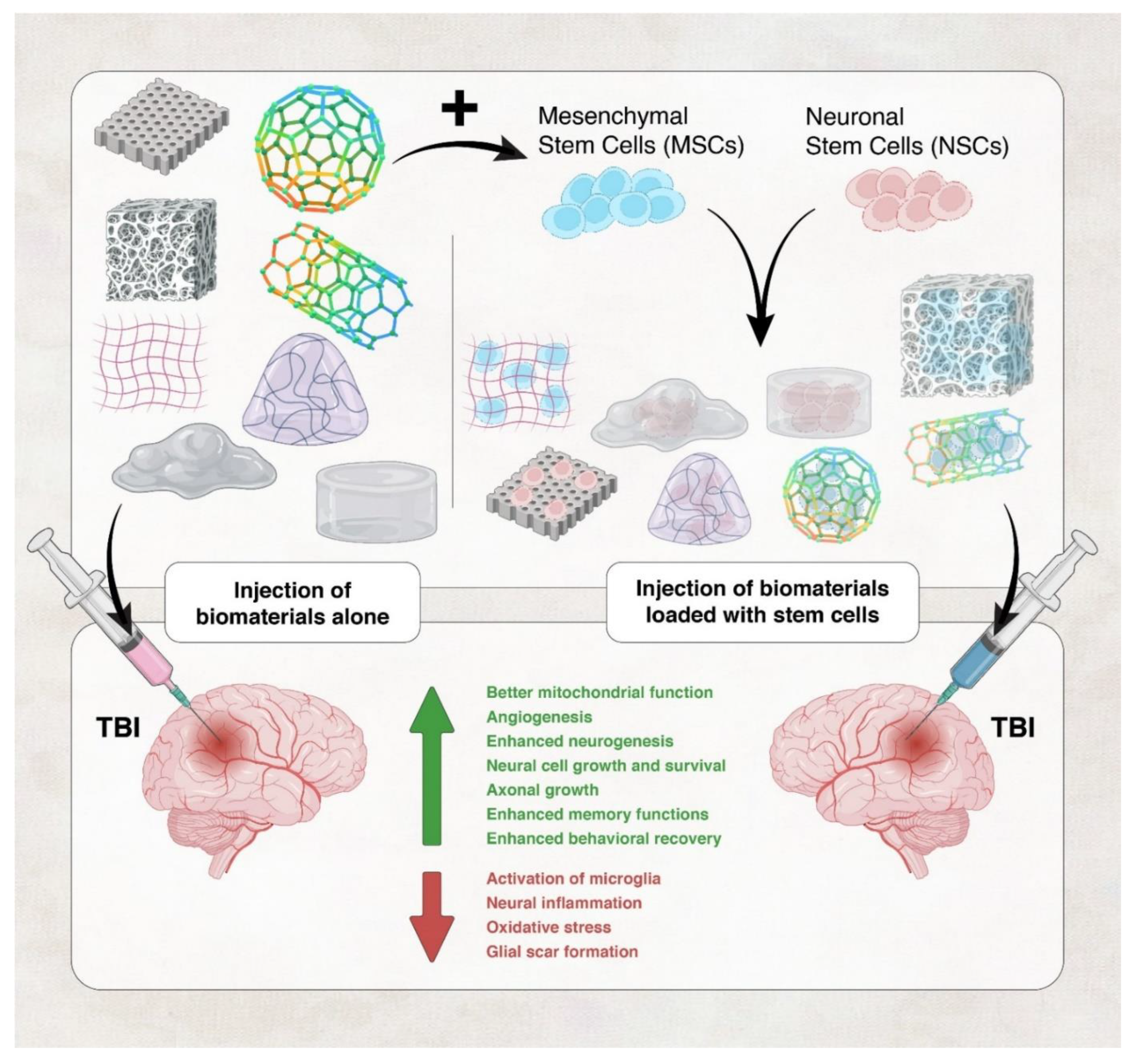
Recently, novel strategies have been developed to repair brain tissue damage. One approach that has gained major attention as a potential TBI treatment is tissue engineering, which relies on the use of biomaterials alone or biomaterials in combination with stem cells (Figure 1). In this regard, low survival rate of transplanted stem cells is the most significant impediment to successful stem cell-based therapy [44], and biomaterials can enhance survival of transplanted stem cells. Today, tissue engineering combines cells, bioactive chemicals, and biocompatible three-dimensional biomaterials to repair injured tissues, while preserving, as much as possible, of the anatomy of the injured tissues. Enhancement of neurite outgrowth, differentiation of human neural stem cells, and nerve gap bridging, of the damaged neurons or the transplanted stem cells, have all been successfully accomplished in TBI using both natural and synthetic biomaterials [45,46,47,48].
Figure 1.
Use of Hydrogels and self-assembling peptides in TBI. These biomaterials can be used alone (left panel) or in combination with stem cells (left panel) to exert their therapeutic effects in TBI.
Figure 1.
Use of Hydrogels and self-assembling peptides in TBI. These biomaterials can be used alone (left panel) or in combination with stem cells (left panel) to exert their therapeutic effects in TBI.
2. Tissue Engineering and Biomaterials in TBI
Compared to other organ systems, therapeutic strategies such as providing increased oxygen supply to damaged tissue and regulating temperature, have been less effective and more difficult to apply to injured tissues of the brain [49]; a possible consequence of the complexity of the CNS or the inhospitable environment around the site of injury. Treatment of TBI currently relies mainly on surgical methods with pharmacological treatments are still under exploration [50]. Limited drug diffusion into the brain across the BBB is still a major hurdle in TBI treatment; hence, the efficiency of current treatment options is restricted, warranting the use of other medical strategies for TBI therapy. Tissue engineering and the use of biomaterials, to assist exogenous cell transplantation or stimulate endogenous cell repair, are good candidate strategies in this regard (Figure 1) [49].
When used to transplant exogenous cells, tissue engineering can involve the assembly of scaffolds, cells, and biologically active molecules into functional tissues, capable of regenerating a patient’s own damaged tissues or whole organ. This may reduce the risk of immune rejection. Artificial skin and cartilage are well known examples of engineered tissues approved by the FDA [51]. In TBI, biomedically active biomaterials can be used as delivery agents for factors that assist in tissue regeneration, such as extracellular matrix (ECM) proteins and growth factors, in addition to promoting recovery and repair by themselves [52].
2.1. Mechanisms of repair by tissue engineering and biomaterials in TBI
Biomaterials are used in tissue engineering to enhance recovery from TBI either alone or in combination with stem cells. Biomaterials were shown to help transplanted neuronal stem cells survive post-implantation by providing a microenvironment favorable for their growth. For example, in addition to promoting recovery and repair by themselves, using biomaterials to deliver neurotrophic growth factors or extracellular matrix (ECM) proteins can properly guide the differentiation of stem cells and assist in tissue regeneration [52]. Importantly, functionalized biomaterials can offer a diverse array of therapeutic effects to address the multifaceted nature of TBI. Among their remarkable capabilities are the promotion of neurogenesis [53,54], inhibition of apoptosis [55,56], elicitation of anti-inflammatory effects [57], providing antioxidant properties[58], and facilitation of angiogenesis [59].
Neuroinflammation in particular has a dual role following TBI. It can have both beneficial effects, such as facilitating cell debris removal, and detrimental effects, including neuronal death and neurodegeneration. Hence, anti-inflammatory therapy represents a viable approach for treating TBI [60]. Li et al. showed that employing an injectable enzymatically-digested gelatin hydrogel, loaded with mouse MSCs differentiated into the neuronal lineage, significantly reduced the damaged area, mitigated inflammation, and lessened neuronal apoptosis in vivo in a moused model of intermediate TBI [61]. Similarly, an injectable self-assembling nanofibrous peptide hydrogel effectively lowered acute brain injury by reducing the number of apoptotic cells, suppressing inflammation, and supporting cell survival [62]. Liu et al. demonstrated that the addition of hyaluronic acid (HA) to chitosan-based hydrogels (CH) reduced the expression of inflammatory markers and cell apoptosis, suggesting that the CH hydrogel effectively inhibited cell death at the injury site [55]. Hypoxia at the site of a traumatic brain injury can set off a chain of detrimental events, such as triggering glutamate excitotoxicity and the influx of Ca2+, which subsequently leads to the generation of free radicals and oxidative stress [63]. Consequently, the introduction of a biomaterial possessing antioxidant properties can be particularly advantageous. An injectable scaffold, HGA, created by combining HA–tyramine (HT) polymer with the antioxidant molecule gallic acid significantly improved the neurological functions of mice with TBI. HGA effects were attributed to its ability to suppress oxidative stress through the activation of the Nrf2/HO-1 pathway [64]. Such biomaterials have the potential to counteract TBI-induced hypoxia, by suppressing oxidative stress.
Injectable hydrogels have the ability to encapsulate different types of molecules, medications, or cytokines, and even cells. They can absorb and then release various growth factors to enhance the microenvironment in a lesion area, stimulating new nerve cell formation and improving neurological function following TBI. Thus, biomaterials can enhance drug accessibility as they were shown to exhibit a controlled-release mechanism of stem cells, growth factors, anti-inflammatory drugs, etc. [65]. Furthermore, using biomaterials to deliver growth factors introduces the possibility of achieving localized delivery [66]. In other words, optimal doses of growth factors can be introduced at the desired sites to allow maximized brain tissue regeneration. Ultimately, the engineering and design of biomaterial-based tissue-like constructs to deliver therapy or growth factors results in a structure that more accurately replaces the lost endogenous tissue environment by creating a suitable environment for neural cell survival, tissue regeneration, and host tissue integration and synapse formation [66,67]. Ma et al. created a hydrogel composed of sodium alginate, collagen, and stromal cell-derived factor-1 (SA/Col/SDF-1) and loaded them with human bone marrow MSCs (hBMSCs). The combination was able to enhance recovery of neurological function after TBI by promoting neurogenesis in the hippocampus, indicated by an increase in EdU+/NeuN+ cells and the expression of neurotrophic factors [68]. Shi et al. involved introducing human umbilical cord-derived MSCs (hUC-MSCs) and activated astrocytes into a self-assembled peptide hydrogel scaffold called RADA16-BDNF (R-B-SPH scaffold). This scaffold stimulated the regeneration of neurons and the reconstruction of neural networks following TBI [69].
Neural stem cells and MSCs are the preferred cell source for neural regeneration in an in cell-based therapy of TBI. Neural stem cells have the capacity of self-renewal and the ability to develop into neurons, astrocytes, and oligodendrocytes [70]. Therefore, they can replace the function of cells lost due to brain injury, making the transplantation of stem cells a promising way to restore the damaged CNS [71]. Neural stem cells and MSCs are used in cell-based therapy of TBI by implanting them directly at the site of injury [70]. Growth factors are needed to stimulate neurogenesis of the transplanted cells [52]. In addition, a suitable biomaterial offering a three-dimensional (3D) matrix or scaffold will be required to support implantation and growth of the transplanted cells and for the endogenous repair of damaged neural tissue; this is particularly crucial in brain tissue reconstruction. This scaffold can fill in structural gaps, knit back the injured brain together, provide a substrate for neurite outgrowth, and act as a pathway for endogenous cells to migrate and axons to elongate [7]. In addition, the harsh microenvironment around the CNS injury site favors differentiation of endogenous neural stem cells into astrocytes rather than neurons, contributing to the formation of the glial scar which impedes recovery [35]. A conductive supramolecular hydrogel biomaterial was shown to provide an optimal niche for neurogenesis of endogenous neural stem cells, thereby reducing glial scar formation and promoting repair of spinal cord injury [72]. Therefore, biomaterials and stem cells are also used to replace or augment the endogenous normal function of tissues, thus providing an efficient means for therapeutic intervention in TBI [52].
Collectively, many studies have indicated that combination treatments of cells, biomaterials, and bioactive molecules, are more effective than treatments involving a single component. Combination of biomaterial-enriched micro-environments, neural stem cells, and growth factors can be combined to increase functional recovery following TBI. These combination treatments are able to bypass the BBB in TBI, thus achieving local delivery to the brain, and enhancing cell survival following cell transplantation. Wang et al. designed a hybrid hydrogel combining a self-assembling peptide and myoglobin protein, which effectively delivers oxygen to tissues. This hydrogel facilitated the delivery of both cortical neural stem cells and oxygen to mouse brain injury sites, supporting stem cell engraftment, survival, and integration for up to 28 days. The hybrid hydrogel outperformed a myoglobin-free version of the hydrogel in promoting engraftment, survival, and maturation of neuronal stem cells into neurons, while also encouraging blood vessel growth in the endogenous tissue. This study suggested that oxygen release from the hydrogel is linked to functional stem cell integration, offering a general strategy for developing improved tissue-mimicking biomaterials [73]. Biomaterials can contribute to the creation of an enriched environment by acting as a delivery agent for the cells, as well as other therapeutic molecules, and ensuring cell retention at the site of integration. Although this method holds promise in replacing lost neurons and rebuilding damaged neural pathways, it is not free of shortcomings. Challenges of cell transplantation include limited survival due to the lack of a supporting microenvironment and difficulties related to the delivery of cell-based therapy [74]. Biomaterials and scaffolds can be used to combat these challenges.
2.2. Biomaterials used in TBI therapy
Biomedically active scaffolds can aid in assembly from single cells into tissues [51], providing a suitable environment for cellular regrowth and repair. Several studies have shown that using a scaffold supports better regeneration of transplanted stem cells than transplanting a cell suspension alone [75,76,77,78]. In this regard, scaffolds derived from biological sources have shown to be more effective in terms of cell survival and behavioral recovery than scaffolds without biological materials [79]. Some biological scaffolds that can be used in these applications include collagen, gelatin, fibrin, and hyaluronic acid, while options for using synthetic scaffolds exist and include linear aliphatic polyesters, poly-anhydrides, and poly-orthoesters. [66]. Natural or biological biomaterials are well known for their high bioactivity, good biocompatibility and degradation properties, and their resemblance to the extracellular matrix (ECM) [80]. While advantages of using synthetic hydrogels include the ability to predict their mechanical and physical properties and behaviors, since they are manufactured under controlled conditions. Moreover, they are easily sterilized and are less likely to produce an immune response. This level of control offers a notable advantage when compared to natural biomaterials [81]. However, synthetic biomaterials suffer from low biocompatibility and a lower ability to induce tissue regeneration [66,80]. Table 2 summarizes the main differences between biomaterials of natural or synthetic sources.
Table 2.
Main differences between biomaterials of natural or synthetic sources.
| Aspect | Synthetic | Natural |
|---|---|---|
| Source | Artificially synthesized | Biological sources |
| Biodegradability | Variable, controllable | Naturally degradable |
| Immunogenicity | Generally low | Potential immune response |
| Mechanical Properties | Customizable for specific needs | Variable |
| Biocompatibility | Reduced, can be optimized | Good biocompatibility |
| Growth Factors | Controlled release | Potential endogenous release |
| Examples | poly-anhydrides, and poly-orthoesters. | Collagen, chitosan, hyaluronic acid |
Recent advancements in biotechnology, particularly 3D bioprinting, have enabled precise control over the internal microstructures of scaffolds, including the manipulation of pore size and microchannels. This level of control allows for the creation of complex scaffold architectures that closely resemble the intricate structures found in native tissue [82]. Scaffolds that contain crucial ECM components can mimic the natural microenvironment required for tissue regeneration, facilitating endogenous tissue repair processes [83]. Biomaterial properties such as surface chemistry, topography, and matrix stiffness can significantly influence cellular functionality and behavior like cell differentiation, proliferation, and adhesion [84]. Therefore, it is essential to consider specific material parameters that impact cell behavior, by effectively interacting with cells to promote tissue regeneration, when developing synthetic biomaterials for the regeneration of functional tissues. These parameters include the physical and mechanical features of the material, its chemical composition, coating of biomaterials with native ECM macromolecules, functionalization of biomaterials with adhesion proteins, reduction of inflammatory responses typically associated with biomaterial implantation, loading of biomaterials with growth factors and incorporation of pharmaceuticals [85]. As such, altering or choosing a biomaterial with specific physical/chemical properties allows the alteration of cellular behaviors. For example, cell proliferation is supported by positively charged biomaterials, while cell differentiation can be promoted by a negatively charged biomaterial [86]. The ability to modify the characteristics of biomaterials allows for high flexibility in their application.
2.3. Materials used to make biomaterials for TBI therapy
A variety of scaffolds exist for potential application in neural tissue engineering in the brain. These include hydrogels, self-assembling peptides, and electrospun nanofiber scaffolds. Each of these scaffolds is made using a different set of methods, hence each has unique morphologies. For brain tissue engineering and TBI recovery, the scaffold surface must be tuned to sustain neurogenesis of endogenous or implanted cells and enable guided axonal growth. Because of the trade-offs between bulk and surface qualities, the scaffold may need to be optimized using techniques like adding biomolecules and applying surface treatments for better biorecognition [87,88]. Table 3 presents findings from studies that have tested the ability of biomaterials to support neuronal growth and aid in the regeneration of damaged brain tissues following TBI in experimental models of TBI. In general, these studies have yielded promising results, with various scaffolds showing potential to improve outcomes in models of TBI.
TBI creates tissue discontinuity along with disruptions in the organized structure of the nerve tracts, have detrimental effects on brain function. Restoring the neural network is vital for optimal brain function, and this can only be achieved by restoring continuity of functional tissue at the cavity/injury site. Thus, TBI creates irregularly shaped cavities, requiring a scaffold that conforms to the shape of the injury while maintaining a suitable environment for cellular integration and repair, and the challenge faced in the restoration process lies in ensuring that a scaffold closely resembles the native tissue both in terms of biological composition and architectural characteristics [89,90,91]. Scaffolds for the use in TBI may be tailored in an injury/tissue-specific manner by altering the 3D architecture of the scaffold, porous spaces within the scaffold, and its physiochemical characteristics such as stiffness and cell-binding ability. The hydrogel scaffold approach has shown the most promise so far because it does not exhibit mechanical/spatial restrictions compared to synthetic polymer scaffolds which must be molded into a specific shape before implantation. Solid systems like nanofibers lack the fluidity present in hydrogels, and therefore cannot fill irregularly shaped lesions, as effectively. Another disadvantage is that using a solid scaffold system may lead to further injury, requiring tissue removal to accommodate the 3D scaffold architecture [92,93,94,95,96]. Considering the number of factors that influence scaffold efficiency, the perfect scaffold for CNS tissue repair has not been developed yet, and research is still being conducted to optimize existing scaffold compatibility and maximize the differentiation of transplanted or endogenous neural stem cells. The following sections collect studies that have used biomaterials for TBI therapy.
Hydrogels
Hydrogels form by cross-linking hydrophilic polymers, a process affected by physical factors (i.e. light and temperature) and chemical factors (i.e. pH and ionic concentration) [97,98]. For materials to be considered as hydrogels, 10-20% of their total weight must consist of water [99], granting them flexibility [100]. Thier highly hydrophilic nature allows them to transport various soluble molecules, making them valuable in biomedical contexts [101]. Notably, hydrogels mirror essential physical traits of native tissues; encompassing high water content, comparable elasticity ranges, and effective mass transfer mechanisms [102]. A primary advantage of hydrogels is their capability to modify their mechanical properties to mimic those of soft tissues, such as the brain. This feature facilitates the transmission of mechanical signals to cells, similar to what occurs in natural tissues [103]. This is especially important for TBI recovery where the presence of the glial scar impedes neuronal signal transmission, neurogenesis, and functional recovery. The presence of a conductive hydrogel may mitigate these defects [35,72].
Covalently cross-linked hydrogels and self-assembled hydrogels are two main types of hydrogels differing in their synthesis mechanisms [104,105]. Polymeric covalently cross-linked hydrogels are considered more stable to changes in environmental factors such as temperature and pH, because of their covalently linked monomers [106]. In addition, they are mostly less deformable but stiffer, requiring a surgery for their implant inside the human body [107,108]. They can be made of synthetic materials or natural sources such as hyaluronic acid, fibroin, chitosan, collagen, and alginate [109,110,111,112,113,114]. The main benefit of these natural molecules is that they are biodegradable, easy to acquire, highly biocompatible and contain particular cell adhesion molecules [115]. Polysaccharides and glycosaminoglycans, some of which are components of the ECM, such as hyaluronic acid (HA), make up the majority of biologically generated hydrogels [116,117,118]. Collagen and HA are the most often used natural polymers to make hydrogels used in brain tissue engineering [119,120]. Nevertheless, these hydrogel scaffold of natural compounds lack homogeneity, due to variations between batches [116].
On the other hand, synthetic hydrogels are often chemically stable, but have poor cell adhesion properties because they are biologically inert. However, they can be modified and functionalized for use in neural tissue engineering. Nowadays, polyethylene glycol (PEG) is a main component of synthetic hydrogels that are applied for CNS therapy [121,122,123]. For the repair of brain injuries, a number of synthetic hydrogels have been employed, including poly(N-2-(hydroxypropyl)methacrylamide) (pHPMA) [124,125], poly(hydroxyethylmethacrylate) (pHEMA), and PEG [126]. pHPMA and pHEMA hydrogels must be implanted premade, requiring invasive surgery [127]. Several of these hydrogels have produced encouraging outcomes. For example, a macroporous pHPMA was created by heterophase separation, employing radical polymerization in a pore-forming solvent with a divinyl crosslinking agent to bridge a brain lesion. This scaffold also allowed for cell penetration, angiogenesis, axon growth, and ECM production [124,125,126].
Biodegradable scaffolds can be synthesized from natural or synthetic materials. The natural materials that are often used include collagen, fibronin protein, chitosan, and HA [105,128,129,130]. On the other hand, poly Ɛ-caprolactone (PCL), poly L-lactic acid (PLA) and polyurethane are all examples of materials used to synthesize synthetic biodegradable scaffolds [131,132,133]. Yet, PCL is hydrophobic, resulting in lack of cell interaction, poor cell adhesion and proliferation. As a solution for this problem, copolymer biodegradable scaffolds have been established by combining two or more chemical species into the polymer, converting the scaffold from hydrophobic to hydrophilic. The main two examples of copolymers are poly D, L-lactide-co-glycolic acid (PLGA), and poly Ɛ-caprolactone-co-ethyl ethylene phosphate (PCLEEP) [134,135].
Another frequently employed category of hydrogels is referred to as “smart” or stimuli responsive hydrogels. Smart hydrogels have a high degree of sensitivity even to minor changes in their external surroundings such as temperature and pH. This adaptability enables them to promptly adjust their physical properties, including mechanical strength and swelling capacity, in response to these changes [7,8]. Stimuli-responsive hydrogels have a variety of subtypes, which include, but are not confined to, thermoresponsive, photoresponsive, electroresponsive, and bioresponsive.smart hydrogels Yao et al. developed a temperature-sensitive chitosan–cellulose hyaluronic acid/β-glycerophosphate (CS-HEC-HA/GP) hydrogel, transitioning from a liquid state below 25°C to a hydrogel form at 37°C. Furthermore, this CS-HEC-HA/GP hydrogel, when laden with human hUC-MSCs, improved the survival rate and retention of the enclosed hUC-MSCs. Additionally, it is able to stimulate neurogenesis, suppress cell apoptosis, leading to expedited brain structure reformation and neurological function restoration in TBI rats [56].
Self-assembling peptides
Self-assembled scaffolds are characterized by soft and deformable structures due to the internal noncovalent forces that link their monomers. They can be injected into damaged tissues or organs [136,137]. Self-assembling peptides (SAPs), composed of repeating units of amino acids and characterized by the formation of double-β-sheet structures in water [138], are a main type of self-assembled biomaterials. Self-assembling peptide nanofiber scaffolds (SAPNS) are created from different oligopeptides or amphiphilic compounds that naturally aggregate to form nanofibers. These in-turn form a fibrillar network under physiological ionic conditions [139]. SAPNS are known to have tissue-like water content, high porosity, and increased cell signaling from bioactive peptides that are presented in high density at the damaged site [139]. SAPs can be modified by adding laminin moieties, which are important proteins present in the ECM of brain tissue [71]
Guo et al. investigated the application of SAPNS by implanting their scaffolds into the brains of rats that had experienced acute brain injury. The results demonstrated a notable enhancement in neurological functions and accelerated tissue regeneration when compared to the control group. Furthermore, SAPNS virtually abolished cavitation in brain lesions, with lower levels of macrophages and astrocytes at the lesion site than in controls with secondary tissue loss [140]. SAPNS are also permissive to axonal growth, such that neural tracts can be partially restored and functional recovery is accomplished after brain injury [141,142,143]. Relatedly, a self-assembling peptide, comprising a 14-amino-acid portion of ependymin, a neuroprotective extracellular glycoprotein that is capable of forming nanofibrous matrices, demonstrated its ability to promote neuronal survival both in vitro and in vivo. This peptide was tested in an acute fluid-percussion injury model of TBI in rats, yielding favorable outcomes[144].
RADA16-I, one of the most studied SAPNS, is made up of repeating sequences of alanine, lysine, and glutamate in the form of RADA. Its nanofibers have a diameter of approximately 10 nm and are highly hydrated. RADA16-I has been extensively researched for tissue culture applications and is available in liquid and powder forms [145,146]. More importantly, it has also been shown to promote regeneration in experimental spinal cord and brain injuries[147]. In a study done by Cheng et al., the self-assembling peptides RADA16 were combined with a laminin-derived IKVAV motif to create a nanofibrous hydrogel that had mechanical properties similar to brain tissue. This IKVAV sequence directed the neural stem cells towards neuronal differentiation in laboratory tests, and in animal studies, the peptide hydrogel increased the survival of stem cells and decreased the formation of glial astrocytes. As a result, there was an improvement in brain tissue regeneration after six weeks [71]. In another study, Ohno et al. developed an amphiphilic peptide [(RADA)3-(RADG)] (mRADA)-tagged N-cadherin extracellular domain (Ncad-mRADA), which can be retained in mRADA hydrogels and injected into deep brain tissue to aid neuroblast migration. Administering Ncad-mRADA in neonatal cortical brain injuries effectively enhanced neuronal regeneration and functional recovery [148].
Another recent study demonstrated that transplantation of hMgSCs seeded in R-GSIK scaffold improved functional recovery following TBI. The presence of R-GSIK scaffold significantly increased the number of hMgSCs in the brain compared to control groups. Furthermore, hMgSCs seeded in R-GSIK effectively reduced injury volume, reactive gliosis and apoptosis. Notably, hMgSCs seeded in R-GSIK exhibited a significant inhibition of Toll-like receptor 4 expression, as well as downstream signaling molecules including interleukin-1β and tumor necrosis factor. These findings suggest that the SAPN hMgSCs with R-GSIK may enhance brain injury healing by enhancing implantation of neuronal stem cells and suppressing inflammation [149].
Electrospun nanofibers
A viscoelastic polymer solution is uni-axially stretched to create a nanofibrous mesh as part of the electrospinning scaffolding process [150]. The structural resemblance of the electrospun nanofibers to the hierarchical fibrillar arrangement of collagen, laminin, and other fibrils of the ECM is the basis of interest in nanofibrous scaffolds for tissue engineering [151,152,153,154]. Nanofibers mimic other features of the cellular ECM, including a large surface area-to-volume ratio, high porosity and similar mechanical properties [153]. The high porosity and large specific surface area exhibited by electrospun fiber scaffolds offer remarkable benefits in terms of enhancing drug-loading efficiency and the response speed of stimuli-triggered drug delivery [155]. In addition, it presents a promising avenue for the development of controlled drug delivery systems. An important illustration is the utilization of two types of PLGA fiber mats loaded with nimodipine (a neuroprotective drug). These fiber mats demonstrated prolonged and controlled release of the drug for a period of 4–8 days and reduced oxidative stress-induced death of neuronal, Schwan, and astrocyte cells in vitro [156].
Compared with other biomaterials, electrospun nanofiber present distinct advantages which include simple preparation, high loading capability and adjustable mechanical properties [157,158]. Additionally, electroactive scaffolds have been recently under intensive investigation as they may help in the communication between brain neurons. For example, in situ polymerization was used to cover PCL and poly-l-lactide nanofibrous scaffolds with polypyrrole (Ppy) to create conductive sheaths [159]. In addition, biomolecules like collagen can be attached to the surface of nanofibrous scaffolds to improve their properties, including enhancement of cell survival and attachment [160]. In fact, various biocompatible materials, both natural and synthetic, have been employed in the fabrication of electrospun nanofibers for brain tissue repair, including collagen, chitosan, silk, fibronectin, fibrinogen, PLA, PCL, PLGA, Ppy, as well as their composites formed by combining them with each other or other materials [161]. The effects of an L-lactide-caprolactone copolymer nanofiber net dressing were examined in a study by Sulejczak et al., revealing its ability to delay and alleviate damaging processes such as neurodegeneration, systemic inflammatory cell infiltration, and excessive formation of glial scars [162]. The anti-inflammatory properties of electrospun nanofiber scaffolds are particularly noteworthy. A recent study performed covalent bonding of galactose onto the surface of PCL nanofiber scaffolds, generating a a polymer referred to as poly(L-lysine)-lactic acid (PLL-LBA). It was observed that, when implanted into a mouse model of TBI, this scaffold led to increased survival of neurons 21 days post-implantation, emphasizing its potential therapeutic impact. Furthermore, this scaffold demonstrated the capability of galactose to sustain an attenuated inflammatory response when compared to control PCL nanofibers devoid of galactose [163].
2.4. Complications with the Use of Biomaterials and Tissue Engineering
Tissue engineering and the use of biomaterials are novel approaches in the treatment of TBI. Despite offering a fair chance of addressing critical medical problems that lack effective treatments, like TBI, they still suffer from significant limitations. They have been linked with substantial side effects as they may require surgical operation to the brain. In addition, tissue engineering techniques, particularly cell- and gene-based therapy, involve manipulation of living cells and their interactions with substrates and biomolecules, potentially resulting in contamination and process failures. There may also be catastrophic repercussions of cell-substrate interactions that are yet-to-be-discovered [164].
In the field of CNS regeneration, developing biomaterials that are biodegradable, biocompatible, and mechanically flexible is still a major challenge. The design and use of these materials will require precise control over their delivery in order for them to exert a therapeutic function in the right place at the right time. Furthermore, creating materials that exhibit the same or similar delicate balance of structure and biological properties as the natural tissues is another hurdle. Other challenges, including the necessity to improve mechanical strength, durability, and stability during application, as well as the balance between fluidity and mechanical strength, limit biomaterials use. To add, creating biomaterials presents a fundamental technical challenge in preserving the free flow of nutrients, oxygen, and medicinal substances produced by enclosed cells, while preventing swelling and eventual rupture of the cells [165].
Biomaterials from natural sources have flaws as well. Batch inconsistency is one of which, resulting in difficulty of controlling the homogeneity of the resultant scaffolds. Additionally, there are more risks related to cryo-preservatives, process additives, and other residues, as well as patient-specific reactions such allergy to antibiotics or other drugs. Furthermore, the original natural sources may contain pathogens that cause immunological reactions [166]. Incompatible materials can cause unanticipated inflammatory responses against the foreign bodies, leading to implanted tissue necrosis and/or rejection. Another complication is the degradation process. In vivo, synthetic polymers lack intrinsic biological properties, and their breakdown products may have negative effects or impact the local microenvironment [167]. If degradation products are created, they should be eliminated from the body through the metabolic path at a rate that keeps their concentration in the body at a manageable level [168]. Some biomaterials dissociate in a slow and unpredictable fashion [169]. The rate of biodegradation within an organism is determined by the polymer properties and the location in the body where it will be exposed. Composition and molecular structure, polydispersity, crystallinity, surface area, and hydrophilic or hydrophobic properties all impact chemical degradation. Chemical degradation affects major polymer chains by causing random breakage of covalent bonds, depolymerization or crosslinking of linear polymers, interference with regular order and crystallinity, and reduction of mechanical characteristics [170,171,172]. If the biomaterial remains in place for longer than intended, the residual material may inhibit rather than promote tissue regeneration. This suggests that biomaterial absorption kinetics will have a significant impact on tissue engineering success rates [51]. Moreover, while biomaterials are generally not considered to be carcinogenic, there are instances where their interaction with living tissue can trigger biological responses that may contribute to the development of cancer [173]. This highlights the need for further research on the long-term side effects of biomaterials. Table 4 provides a concise overview of the advantages and disadvantages associated with the use of biomaterials in tissue engineering.
Table 3.
Studies testing the therapeutic potential of biomaterials in TBI.
| Study | Biomaterial | Species | Outcome | Reference |
| Liu et al. (2023) | Collagen/chitosan/BMExos scaffold | Rat |
|
[174] |
| Li et al. (2021) | Gelatin hydrogel | In vitro & mice |
|
[61] |
| Tang et al. (2020) | aPLGA-LysoGM1 scaffold | In vitro & rat model |
|
[175] |
| Zheng et al. (2020) | gelatin methacrylate hydrogel with polydopamine nanoparticles and hAMSCS | Rat |
|
[54] |
| Mahumane et al. (2020) | N-acetylcysteine (NAC)-loaded poly(lactic-co-glycolic acid) (PLGA) electrospun nanofiber | In vitro & ex vivo (Rat pheochromocytoma (PC12) and human glioblastoma multiform (A172) cell lines) |
|
[176] |
| Zhou et al. (2018) | Poly(lactic-co-glycolic acid) (PLGA) scaffold | In vitro & in vivo Mesenchymal stem cells (MSCs) and neurons |
|
[177] |
| Álvarez et al. (2014) | poly-l/dl lactic acid (PLA70/30) nanofibers | Mice |
|
[178] |
| Sulejczak et al. (2014) | Electrospun nanofiber/ L-lactide-caprolactone copolymer nanofiber net | Rat |
|
[162] |
| Zhang et al. (2018) | Vepoloxamer | Rats |
|
[179] |
| Macks et al. (2022) | poly(ethylene) glycol-bis-(acryloyloxy acetate) (PEG-bis-AA) with dexamethasone (DX)-conjugated hyaluronic acid (HA-DXM) | Rats |
|
[180] |
| Latchoumane et al. (2021) | Engineered Chondroitin sulfate (eCS) | Rats |
|
[78] |
| Liu et al. (2022) | secretome/collagen/heparan sulfate scaffold | Rats |
|
[181] |
| Sahab Negah et al. (2019) | Self- assembling peptide hMgSCs + R-GSIK | Rats |
|
[149] |
| Liu et al. (2023) | Bone marrow mesenchymal stem cell-derived exosomes (BME) + hyaluronan-collagen hydrogel (DHC-BME) | Rats |
|
[182] |
| Tanikawa et al. (2023) | Electrically charged hydrogels (C1A1) + VEGF | Mice |
|
[183] |
| Hu et al. (2023) | Self-healing hydrogel (HA-PBA/Gel-Dopa) | Mice |
|
[184] |
| Moisenovich et al. (2019) | Silk fibroin scaffold | Rats |
|
[185] |
| Chen et al (2022) | hydrogen sulfide(H2S)-releasing silk fibroin (SF) hydrogel (H2S@SF) | Mice |
|
[186] |
| Jiang et al (2021) | Collagen/Silk Fibroin (SF) scaffold | Canine |
|
[187] |
| Qian et al (2021) | TM/PC hydrogel (Tri-glycerol monostearate, propylene sulfide and curcumin) |
Mice |
|
[188] |
| Zhang et al. (2022) | HT/HGA hydrogel (hyaluronic acid-tyramine + antioxidant gallic acid-grafted hyaluronic acid) | Mice |
|
[64] |
| Chen et al (2023) | gelatin methacrylate and sodium alginate hydrogel (GelMA/Alg) | Rat |
|
[189] |
| Ma et al (2020) | self-assembling peptide-based hydrogel | Rat |
|
[190] |
Table 4.
Advantages and limitations of the use of biomaterials in tissue engineering.
| Biomaterial | Characteristic | Advantages | Disadvantages | Reference |
| Natural Hydrogels | cross-linked macromolecular networks | - no mechanical/spatial restrictions compared to synthetic polymer scaffolds - mesh size and porosity of hydrogels can be modified -Biocompatible -Injectable -Porous |
-heterogeneity between batches -May carry natural pathogen -difficulty in precise modification of the material |
[54,64] |
| Synthetic hydrogels | Can be modified according to need | -Biologically inert -Chemically stable -Easier to control important perimeters |
- Premade, require invasive implantation surgery -Cause more inflammatory response than natural hydrogels |
[191,192,193] |
| Self-assembling peptides SAPNS | composed of repeating units of amino acids and characterized by the formation of double-β- sheet structures | -high porosity -increased cell signaling from bioactive peptides that are presented in high density at the damaged site -Highly biocompatible -Allow minimally invasive treatments |
-Lack of understanding on their degradability -Lack of data on long-term electroactivity of the scaffold |
[140,194,195] |
| Electrospun nanofibers | A nonwoven mat of micro- and nanofibers is created when fluid filament is stretched in a powerful electric field. | - Aligned nanofibers can resemble the topographical characteristics of the extracellular matrix in the brain. - Due to large surface-to-volume ratio electrospun fibers improve cell adhesion, mass transfer characteristics, and drug loading. |
-pH difference, local enzymes may degrade the fibers | [196,197] |
3. Conclusion
Although TBI remains a leading cause of mortality and disability worldwide, it is still without a definitive treatment. The use of tissue engineering biomaterials in TBI is emerging as a promising treatment approach of TBI. These innovative therapies, involve the repair of damaged brain tissue using hydrogels, self-assembling peptides, and electrospun nanofibers. The biomaterials can be used alone or in combination with stem cells, neurotrophic and growth factors, matrix metalloproteinases, antioxidants, oxygen delivery moieties, angiogenic factors, and other functional moieties. These biomaterials have shown great potential in reducing oxidative stress, neuroinflammation, apoptosis, formation of astrocytes and glial scars, and rupture of the BBB, and promoting neurite outgrowth, neural stem cell neurogenesis and differentiation, neovascularization, synapse formation, and nerve gap bridging in models of TBI. Nevertheless, these biomaterials have not been used for treating TBI in a clinical setting. While animal models have demonstrated the effectiveness of these tissue engineering strategies in treating TBI, there is still insufficient data on their efficacy in human subjects Challenges persist, including ensuring the survival of transplanted neuronal stem cells in harsh the cellular environment of TBI and the development of biodegradable, biocompatible, and mechanically adaptable biomaterials.. Functionalization and the use of multi-functional supramolecular scaffolds of these biomaterials is steadily overcoming these limitations. As of now, tissue engineering with biomaterials offers a valuable opportunity to explore new therapeutic avenues for TBI beyond traditional drug-based treatments and delivery methods.
Funding
This research is funded by a grant from Morehouse School of Medicine to Firas Kobeissy and a grant from Qatar University to Abdullah A. Shaito.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dewan, M.C., et al., Estimating the global incidence of traumatic brain injury. Journal of neurosurgery, 2018. 130(4): p. 1080-1097. [CrossRef]
- Peeters, W., et al., Epidemiology of traumatic brain injury in Europe. Acta neurochirurgica, 2015. 157(10): p. 1683-1696. [CrossRef]
- Phillips, S. and D. Woessner, Sports-related traumatic brain injury. Primary Care: Clinics in Office Practice, 2015. 42(2): p. 243-248.
- Wojcik, B.E., et al., Traumatic brain injury hospitalizations of US army soldiers deployed to Afghanistan and Iraq. American journal of preventive medicine, 2010. 38(1): p. S108-S116. [CrossRef]
- Theadom, A., et al., Incidence of sports-related traumatic brain injury of all severities: a systematic review. 2020. 54(2): p. 192-199. [CrossRef]
- Harrison, J.E., J.G. Berry, and L.M. Jamieson, Head and traumatic brain injuries among Australian youth and young adults, July 2000–June 2006. Brain injury, 2012. 26(7-8): p. 996-1004. [CrossRef]
- Peplow, P.V., B. Martinez, and T.A.J.N.D.B.T.T.R.t.C.P. Gennarelli, Prevalence, needs, strategies, and risk factors for neurodegenerative diseases. 2022: p. 3-8. [CrossRef]
- Norup, A., et al., Socioeconomic consequences of traumatic brain injury: a danish nationwide register-based study. Journal of neurotrauma, 2020. 37(24): p. 2694-2702. [CrossRef]
- Howlett, J.R., L.D. Nelson, and M.B. Stein, Mental Health Consequences of Traumatic Brain Injury. Biol Psychiatry, 2022. 91(5): p. 413-420. [CrossRef]
- DeKosky, S.T., et al., Acute and chronic traumatic encephalopathies: pathogenesis and biomarkers. Nature Reviews Neurology, 2013. 9(4): p. 192-200. [CrossRef]
- Crane, P.K., et al., Association of Traumatic Brain Injury With Late-Life Neurodegenerative Conditions and Neuropathologic Findings. JAMA Neurol, 2016. 73(9): p. 1062-9. [CrossRef]
- Vespa, P.M., Hormonal dysfunction in neurocritical patients. Current opinion in critical care, 2013. 19(2): p. 107-112. [CrossRef]
- Foreman, B., et al., Seizures and Cognitive Outcome After Traumatic Brain Injury: A Post Hoc Analysis. Neurocrit Care, 2022. 36(1): p. 130-138. [CrossRef]
- Monsour, M., D. Ebedes, and C.V. Borlongan, A review of the pathology and treatment of TBI and PTSD. Exp Neurol, 2022. 351: p. 114009. [CrossRef]
- Alouani, A.T. and T. Elfouly, Traumatic Brain Injury (TBI) Detection: Past, Present, and Future. Biomedicines, 2022. 10(10). [CrossRef]
- Brett, B.L., et al., Traumatic Brain Injury and Risk of Neurodegenerative Disorder. Biol Psychiatry, 2022. 91(5): p. 498-507. [CrossRef]
- Haidar, M.A., et al., Mitoquinone Helps Combat the Neurological, Cognitive, and Molecular Consequences of Open Head Traumatic Brain Injury at Chronic Time Point. Biomedicines, 2022. 10(2): p. 250. [CrossRef]
- Control, C.f.D. and Prevention, national center for injury prevention and control: report to congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Atlanta, GA: Centers for Disease Control and Prevention, 2003.
- Dikmen, S., et al., Rates of symptom reporting following traumatic brain injury. J Int Neuropsychol Soc, 2010. 16(3): p. 401-11. [CrossRef]
- Dixon, K.J., Pathophysiology of Traumatic Brain Injury. Phys Med Rehabil Clin N Am, 2017. 28(2): p. 215-225. [CrossRef]
- McKee, A.C. and D.H. Daneshvar, The neuropathology of traumatic brain injury. Handbook of clinical neurology, 2015. 127: p. 45-66. [CrossRef]
- Kaur, P. and S. Sharma, Recent advances in pathophysiology of traumatic brain injury. Current neuropharmacology, 2018. 16(8): p. 1224-1238. [CrossRef]
- Dong, G.-C., et al., A potent inhibition of oxidative stress induced gene expression in neural cells by sustained ferulic acid release from chitosan based hydrogel. 2015. 49: p. 691-699. [CrossRef]
- Stirling, D.P., et al., Axoplasmic reticulum Ca2+ release causes secondary degeneration of spinal axons. Annals of neurology, 2014. 75(2): p. 220-229. [CrossRef]
- Mu, J., et al., Calcium signaling is implicated in the diffuse axonal injury of brain stem. 2015. 8(5): p. 4388.
- Arciniegas, D.B. and J.M. Silver, Pharmacotherapy of posttraumatic cognitive impairments. Behavioural neurology, 2006. 17(1): p. 25-42. [CrossRef]
- Weil, Z.M., K.R. Gaier, and K. Karelina, Injury timing alters metabolic, inflammatory and functional outcomes following repeated mild traumatic brain injury. Neurobiology of disease, 2014. 70: p. 108-116. [CrossRef]
- Fehily, B. and M. Fitzgerald, Repeated mild traumatic brain injury: potential mechanisms of damage. Cell transplantation, 2017. 26(7): p. 1131-1155.
- Mustafa, A.G., et al., Pharmacological inhibition of lipid peroxidation attenuates calpain-mediated cytoskeletal degradation after traumatic brain injury. Journal of neurochemistry, 2011. 117(3): p. 579-588. [CrossRef]
- Abdul-Muneer, P., N. Chandra, and J. Haorah, Interactions of oxidative stress and neurovascular inflammation in the pathogenesis of traumatic brain injury. Molecular neurobiology, 2015. 51(3): p. 966-979. [CrossRef]
- Alves, J.L., Blood–brain barrier and traumatic brain injury. Journal of neuroscience research, 2014. 92(2): p. 141-147. [CrossRef]
- Shlosberg, D., et al., Blood–brain barrier breakdown as a therapeutic target in traumatic brain injury. Nature Reviews Neurology, 2010. 6(7): p. 393-403. [CrossRef]
- Llorens-Bobadilla, E., et al., A latent lineage potential in resident neural stem cells enables spinal cord repair. 2020. 370(6512): p. eabb8795. [CrossRef]
- Zhou, L., et al., Soft conducting polymer hydrogels cross-linked and doped by tannic acid for spinal cord injury repair. 2018. 12(11): p. 10957-10967. [CrossRef]
- Ng, S.Y. and A.Y.W. Lee, Traumatic Brain Injuries: Pathophysiology and Potential Therapeutic Targets. Front Cell Neurosci, 2019. 13: p. 528. [CrossRef]
- Perez, E.J., et al., Enhanced astrocytic d-serine underlies synaptic damage after traumatic brain injury. J Clin Invest, 2017. 127(8): p. 3114-3125. [CrossRef]
- Chen, Y. and R.A. Swanson, Astrocytes and brain injury. Journal of Cerebral Blood Flow & Metabolism, 2003. 23(2): p. 137-149.
- Al-Haj, N., et al., Phytochemicals as Micronutrients: What Is their Therapeutic Promise in the Management of Traumatic Brain Injury?, in Role of Micronutrients in Brain Health. 2022, Springer. p. 245-276.
- Xiong, B., et al., Strategies for structural modification of small molecules to improve blood–brain barrier penetration: A recent perspective. Journal of Medicinal Chemistry, 2021. 64(18): p. 13152-13173. [CrossRef]
- Silva, G.A., Nanotechnology approaches for the regeneration and neuroprotection of the central nervous system. Surgical Neurology, 2005. 63(4): p. 301-306. [CrossRef]
- Han, L. and C. Jiang, Evolution of blood-brain barrier in brain diseases and related systemic nanoscale brain-targeting drug delivery strategies. Acta Pharm Sin B, 2021. 11(8): p. 2306-2325. [CrossRef]
- Cash, A. and M.H. Theus, Mechanisms of Blood-Brain Barrier Dysfunction in Traumatic Brain Injury. Int J Mol Sci, 2020. 21(9). [CrossRef]
- Kochanek, P.M., et al., Operation brain trauma therapy: 2016 update. Military medicine, 2018. 183(suppl_1): p. 303-312.
- Francis, N.L., et al., Self-assembling peptide nanofiber scaffolds for 3-D reprogramming and transplantation of human pluripotent stem cell-derived neurons. ACS biomaterials science & engineering, 2016. 2(6): p. 1030-1038. [CrossRef]
- Gonzalez-Perez, F., et al., Stabilization, rolling, and addition of other extracellular matrix proteins to collagen hydrogels improve regeneration in chitosan guides for long peripheral nerve gaps in rats. Neurosurgery, 2017. 80(3): p. 465-474. [CrossRef]
- Yang, R., et al., PTMAc-PEG-PTMAc hydrogel modified by RGDC and hyaluronic acid promotes neural stem cells' survival and differentiation in vitro. RSC advances, 2017. 7(65): p. 41098-41104. [CrossRef]
- Zhou, X., et al., Enhancement of neurite adhesion, alignment and elongation on conductive polypyrrole-poly (lactide acid) fibers with cell-derived extracellular matrix. Colloids and Surfaces B: Biointerfaces, 2017. 149: p. 217-225.
- Xue, C., et al., Electrospun silk fibroin-based neural scaffold for bridging a long sciatic nerve gap in dogs. Journal of tissue engineering and regenerative medicine, 2018. 12(2): p. e1143-e1153. [CrossRef]
- Pardridge, W.M., Drug transport across the blood-brain barrier. J Cereb Blood Flow Metab, 2012. 32(11): p. 1959-72. [CrossRef]
- Skolnick, B.E., et al., A Clinical Trial of Progesterone for Severe Traumatic Brain Injury. New England Journal of Medicine, 2014. 371(26): p. 2467-2476. [CrossRef]
- Ikada, Y., Challenges in tissue engineering. Journal of the Royal Society Interface, 2006. 3(10): p. 589-601.
- Babensee, J.E., L.V. McIntire, and A.G. Mikos, Growth factor delivery for tissue engineering. Pharmaceutical research, 2000. 17(5): p. 497-504. [CrossRef]
- Yao, M., et al., A dual-enzymatically cross-linked injectable gelatin hydrogel loaded with BMSC improves neurological function recovery of traumatic brain injury in rats. 2019. 7(10): p. 4088-4098. [CrossRef]
- Zheng, Y., et al., Neuro-regenerative imidazole-functionalized GelMA hydrogel loaded with hAMSC and SDF-1α promote stem cell differentiation and repair focal brain injury. Bioact Mater, 2021. 6(3): p. 627-637. [CrossRef]
- Liu, Y., et al., Semi-interpenetrating polymer network of hyaluronan and chitosan self-healing hydrogels for central nervous system repair. 2020. 12(36): p. 40108-40120. [CrossRef]
- Yao, M., et al., Chitosan-based thermosensitive composite hydrogel enhances the therapeutic efficacy of human umbilical cord MSC in TBI rat model. 2019. 14: p. 100192. [CrossRef]
- Jeong, D.U., et al., Hydrogel-mediated local delivery of dexamethasone reduces neuroinflammation after traumatic brain injury. Biomed Mater, 2021. 16(3). [CrossRef]
- Kuan, C.-Y., et al., The preparation of oxidized methylcellulose crosslinked by adipic acid dihydrazide loaded with vitamin C for traumatic brain injury. 2019. 7(29): p. 4499-4508. [CrossRef]
- Lu, J., et al., Synergistic effects of dual-presenting VEGF-and BDNF-mimetic peptide epitopes from self-assembling peptide hydrogels on peripheral nerve regeneration. 2019. 11(42): p. 19943-19958. [CrossRef]
- Zheng, R.Z., et al., Neuroinflammation Following Traumatic Brain Injury: Take It Seriously or Not. Front Immunol, 2022. 13: p. 855701. [CrossRef]
- Li, J., et al., Dual-enzymatically cross-linked gelatin hydrogel promotes neural differentiation and neurotrophin secretion of bone marrow-derived mesenchymal stem cells for treatment of moderate traumatic brain injury. Int J Biol Macromol, 2021. 187: p. 200-213. [CrossRef]
- Zhang, N., L. He, and W. Wu, Self-assembling peptide nanofibrous hydrogel as a promising strategy in nerve repair after traumatic injury in the nervous system. Neural Regen Res, 2016. 11(5): p. 717-8. [CrossRef]
- Carvajal, F.J. and W. Cerpa, Regulation of Phosphorylated State of NMDA Receptor by STEP(61) Phosphatase after Mild-Traumatic Brain Injury: Role of Oxidative Stress. Antioxidants (Basel), 2021. 10(10). [CrossRef]
- Zhang, D., et al., In situ forming and biocompatible hyaluronic acid hydrogel with reactive oxygen species-scavenging activity to improve traumatic brain injury repair by suppressing oxidative stress and neuroinflammation. Mater Today Bio, 2022. 15: p. 100278. [CrossRef]
- Tan, H.X., et al., The use of bioactive matrices in regenerative therapies for traumatic brain injury. 2020. 102: p. 1-12. [CrossRef]
- Zhen Xu, S.L., Min Liang, Haoyi Yang, Chunqi Chang, Biomaterials Based Growth Factor Delivery for Brain Regeneration After Injury. Smart Materials in Medicine, 2022. 3: p. 352-360. [CrossRef]
- Mukherjee, N., A. Adak, and S.J.S.M. Ghosh, Recent trends in the development of peptide and protein-based hydrogel therapeutics for the healing of CNS injury. 2020. 16(44): p. 10046-10064. [CrossRef]
- Ma, S., et al., Sodium alginate/collagen/stromal cell-derived factor-1 neural scaffold loaded with BMSCs promotes neurological function recovery after traumatic brain injury. Acta Biomater, 2021. 131: p. 185-197. [CrossRef]
- Shi, W., et al., Transplantation of RADA16-BDNF peptide scaffold with human umbilical cord mesenchymal stem cells forced with CXCR4 and activated astrocytes for repair of traumatic brain injury. Acta Biomater, 2016. 45: p. 247-261. [CrossRef]
- Tabet, M., et al., Evaluation of Evidence: Stem Cells as a Treatment Option for Traumatic Brain Injury, in eLS. p. 1-12. [CrossRef]
- Cheng, T.-Y., et al., Neural stem cells encapsulated in a functionalized self-assembling peptide hydrogel for brain tissue engineering. Biomaterials, 2013. 34(8): p. 2005-2016. [CrossRef]
- Yang, B., et al., A conductive supramolecular hydrogel creates ideal endogenous niches to promote spinal cord injury repair. Bioact Mater, 2022. 15: p. 103-119. [CrossRef]
- Wang, Y., et al., Hydrogel oxygen reservoirs increase functional integration of neural stem cell grafts by meeting metabolic demands. 2023. 14(1): p. 457. [CrossRef]
- Keimpema, E., et al., Early transient presence of implanted bone marrow stem cells reduces lesion size after cerebral ischaemia in adult rats. Neuropathol Appl Neurobiol, 2009. 35(1): p. 89-102. [CrossRef]
- Clarkson, E.D., et al., Strands of embryonic mesencephalic tissue show greater dopamine neuron survival and better behavioral improvement than cell suspensions after transplantation in parkinsonian rats. Brain Res, 1998. 806(1): p. 60-8. [CrossRef]
- Sautter, J., et al., Implants of polymer-encapsulated genetically modified cells releasing glial cell line-derived neurotrophic factor improve survival, growth, and function of fetal dopaminergic grafts. Experimental neurology, 1998. 149(1): p. 230-236. [CrossRef]
- Yan, F., et al., Collagen-chitosan scaffold impregnated with bone marrow mesenchymal stem cells for treatment of traumatic brain injury. 2019. 14(10): p. 1780. [CrossRef]
- Latchoumane, C.V., et al., Engineered glycomaterial implants orchestrate large-scale functional repair of brain tissue chronically after severe traumatic brain injury. Sci Adv, 2021. 7(10). [CrossRef]
- Donaghue, I.E., et al., Cell and Biomolecule Delivery for Tissue Repair and Regeneration in the Central Nervous System. Journal of Controlled Release, 2014. [CrossRef]
- Chen, F.-M. and X.J.P.i.p.s. Liu, Advancing biomaterials of human origin for tissue engineering. 2016. 53: p. 86-168.
- Davim, J.P., Biomedical composites: materials, manufacturing and engineering. Vol. 2. 2013: Walter de Gruyter.
- Feng, C., et al., 3D Printing of Lotus Root-Like Biomimetic Materials for Cell Delivery and Tissue Regeneration. Adv Sci (Weinh), 2017. 4(12): p. 1700401. [CrossRef]
- Kyburz, K.A. and K.S. Anseth, Synthetic mimics of the extracellular matrix: how simple is complex enough? Ann Biomed Eng, 2015. 43(3): p. 489-500. [CrossRef]
- Ventre, M. and P.A. Netti, Engineering Cell Instructive Materials To Control Cell Fate and Functions through Material Cues and Surface Patterning. ACS Appl Mater Interfaces, 2016. 8(24): p. 14896-908. [CrossRef]
- Wu, R.-X., et al., Biomaterials for endogenous regenerative medicine: coaxing stem cell homing and beyond. 2018. 11: p. 144-165. [CrossRef]
- Yu-Shuan Chen, H.-J.H., Tzyy-Wen Chiou, The Role of Biomaterials in Implantation for Central Nervous System Injury. Cell Transplant, 2018. 27(3): p. 407-422. [CrossRef]
- Pettikiriarachchi, J.T.S., et al., Biomaterials for Brain Tissue Engineering. Australian Journal of Chemistry, 2010. 63(8): p. 1143-1154. [CrossRef]
- Zhang, K., et al., Structurally dynamic hydrogels for biomedical applications: pursuing a fine balance between macroscopic stability and microscopic dynamics. 2021. 121(18): p. 11149-11193. [CrossRef]
- He, J., et al., Scaffolds for central nervous system tissue engineering. 2012. 6: p. 1-25. [CrossRef]
- Su, Z., et al., In vivo conversion of astrocytes to neurons in the injured adult spinal cord. 2014. 5(1): p. 3338. [CrossRef]
- Tamariz, E. and A.J.F.i.n. Varela-Echavarría, The discovery of the growth cone and its influence on the study of axon guidance. 2015. 9: p. 51.
- Musah, S., et al., Glycosaminoglycan-binding hydrogels enable mechanical control of human pluripotent stem cell self-renewal. ACS Nano, 2012. 6(11): p. 10168-77. [CrossRef]
- Li, X., et al., Applications and Mechanisms of Stimuli-Responsive Hydrogels in Traumatic Brain Injury. Gels, 2022. 8(8). [CrossRef]
- Jurga, M., et al., The performance of laminin-containing cryogel scaffolds in neural tissue regeneration. 2011. 32(13): p. 3423-3434. [CrossRef]
- Cholas, R.H., H.-P. Hsu, and M.J.B. Spector, The reparative response to cross-linked collagen-based scaffolds in a rat spinal cord gap model. 2012. 33(7): p. 2050-2059. [CrossRef]
- Martínez-Ramos, C., et al., Neural tissue regeneration in experimental brain injury model with channeled scaffolds of acrylate copolymers. 2015. 598: p. 96-101. [CrossRef]
- Kretlow, J.D., L. Klouda, and A.G.J.A.d.d.r. Mikos, Injectable matrices and scaffolds for drug delivery in tissue engineering. 2007. 59(4-5): p. 263-273. [CrossRef]
- Li, J. and D.J.J.N.R.M. Mooney, Designing hydrogels for controlled drug delivery. 2016. 1(12): p. 1-17. [CrossRef]
- Peppas, N.A. and A.S. Hoffman, Hydrogels, in Biomaterials science. 2020, Elsevier. p. 153-166.
- Gradinaru, V., et al., Hydrogel-tissue chemistry: principles and applications. 2018. 47: p. 355-376. [CrossRef]
- El-Sherbiny, I.M., M.H.J.G.C.S. Yacoub, and Practice, Hydrogel scaffolds for tissue engineering: Progress and challenges. 2013. 2013(3): p. 38. [CrossRef]
- Martin, N. and G.J.J.o.t.m.b.o.b.m. Youssef, Dynamic properties of hydrogels and fiber-reinforced hydrogels. 2018. 85: p. 194-200.
- Che, L., et al., A 3D printable and bioactive hydrogel scaffold to treat traumatic brain injury. 2019. 29(39): p. 1904450. [CrossRef]
- Saracino, G.A., et al., Nanomaterials design and tests for neural tissue engineering. Chem Soc Rev, 2013. 42(1): p. 225-62. [CrossRef]
- Collins, M.N. and C. Birkinshaw, Hyaluronic acid based scaffolds for tissue engineering--a review. Carbohydr Polym, 2013. 92(2): p. 1262-79. [CrossRef]
- Stratton, S., et al., Bioactive polymeric scaffolds for tissue engineering. Bioact Mater, 2016. 1(2): p. 93-108. [CrossRef]
- Patenaude, M., N.M. Smeets, and T. Hoare, Designing injectable, covalently cross-linked hydrogels for biomedical applications. Macromol Rapid Commun, 2014. 35(6): p. 598-617. [CrossRef]
- Bakarich, S.E., et al., Recovery from applied strain in interpenetrating polymer network hydrogels with ionic and covalent cross-links. Soft Matter, 2012. 8(39): p. 9985-9988. [CrossRef]
- Führmann, T., et al., Click-crosslinked injectable hyaluronic acid hydrogel is safe and biocompatible in the intrathecal space for ultimate use in regenerative strategies of the injured spinal cord. Methods, 2015. 84: p. 60-9. [CrossRef]
- Koh, L.-D., et al., Structures, mechanical properties and applications of silk fibroin materials. Progress in Polymer Science, 2015. 46: p. 86-110. [CrossRef]
- Alvarez, G.S., et al., Antibiotic-loaded silica nanoparticle–collagen composite hydrogels with prolonged antimicrobial activity for wound infection prevention. Journal of Materials Chemistry B, 2014. 2(29): p. 4660-4670. [CrossRef]
- Desai, R.M., et al., Versatile click alginate hydrogels crosslinked via tetrazine–norbornene chemistry. Biomaterials, 2015. 50: p. 30-37. [CrossRef]
- Zamproni, L.N., et al., Neurorepair and regeneration of the brain: a decade of bioscaffolds and engineered microtissue. 2021. 9: p. 649891.
- Nih, L.R., et al., Dual-function injectable angiogenic biomaterial for the repair of brain tissue following stroke. 2018. 17(7): p. 642-651. [CrossRef]
- Thiele, J., et al., 25th anniversary article: Designer hydrogels for cell cultures: a materials selection guide. Adv Mater, 2014. 26(1): p. 125-47. [CrossRef]
- Namba, R., et al., Development of porous PEG hydrogels that enable efficient, uniform cell-seeding and permit early neural process extension. Acta Biomaterialia, 2009. 5(6): p. 1884-1897. [CrossRef]
- Trombino, S., et al., Strategies for Hyaluronic Acid-Based Hydrogel Design in Drug Delivery. Pharmaceutics, 2019. 11(8). [CrossRef]
- Cook, D.J., et al., Hydrogel-delivered brain-derived neurotrophic factor promotes tissue repair and recovery after stroke. 2017. 37(3): p. 1030-1045.
- Jensen, G., J.L. Holloway, and S.E. Stabenfeldt, Hyaluronic Acid Biomaterials for Central Nervous System Regenerative Medicine. Cells, 2020. 9(9). [CrossRef]
- Ucar, B. and C. Humpel, Collagen for brain repair: therapeutic perspectives. Neural Regen Res, 2018. 13(4): p. 595-598. [CrossRef]
- Peppas, N.A., H.J. Moynihan, and L.M. Lucht, The structure of highly crosslinked poly(2-hydroxyethyl methacrylate) hydrogels. J Biomed Mater Res, 1985. 19(4): p. 397-411. [CrossRef]
- Ahmad, M.B. and M.B. Huglin, DSC studies on states of water in crosslinked poly (methyl methacrylate-co-n-vinyl-2-pyrrolidone) hydrogels. Polymer international, 1994. 33(3): p. 273-277. [CrossRef]
- Almany, L. and D. Seliktar, Biosynthetic hydrogel scaffolds made from fibrinogen and polyethylene glycol for 3D cell cultures. Biomaterials, 2005. 26(15): p. 2467-77. [CrossRef]
- Woerly, S., et al., Development of a sialic acid-containing hydrogel of poly [N-(2-hydroxypropyl) methacrylamide]: characterization and implantation study. Biomacromolecules, 2008. 9(9): p. 2329-2337. [CrossRef]
- Woerly, S., et al., Neural tissue formation within porous hydrogels implanted in brain and spinal cord lesions: ultrastructural, immunohistochemical, and diffusion studies. Tissue engineering, 1999. 5(5): p. 467-488. [CrossRef]
- Lesný, P., et al., Polymer hydrogels usable for nervous tissue repair. Journal of chemical neuroanatomy, 2002. 23(4): p. 243-247.
- Zhong, Y. and R.V. Bellamkonda, Biomaterials for the central nervous system. Journal of the Royal Society Interface, 2008. 5(26): p. 957-975. [CrossRef]
- Phipps, M.C., et al., Increasing the pore sizes of bone-mimetic electrospun scaffolds comprised of polycaprolactone, collagen I and hydroxyapatite to enhance cell infiltration. Biomaterials, 2012. 33(2): p. 524-34. [CrossRef]
- Paşcu, E.I., J. Stokes, and G.B. McGuinness, Electrospun composites of PHBV, silk fibroin and nano-hydroxyapatite for bone tissue engineering. Mater Sci Eng C Mater Biol Appl, 2013. 33(8): p. 4905-16. [CrossRef]
- Croisier, F. and C. Jérôme, Chitosan-based biomaterials for tissue engineering. European polymer journal, 2013. 49(4): p. 780-792. [CrossRef]
- Farrugia, B.L., et al., Dermal fibroblast infiltration of poly(ε-caprolactone) scaffolds fabricated by melt electrospinning in a direct writing mode. Biofabrication, 2013. 5(2): p. 025001. [CrossRef]
- Izal, I., et al., Culture of human bone marrow-derived mesenchymal stem cells on of poly(L-lactic acid) scaffolds: potential application for the tissue engineering of cartilage. Knee Surg Sports Traumatol Arthrosc, 2013. 21(8): p. 1737-50. [CrossRef]
- Grad, S., et al., The use of biodegradable polyurethane scaffolds for cartilage tissue engineering: potential and limitations. Biomaterials, 2003. 24(28): p. 5163-71. [CrossRef]
- Bini, T., et al., Electrospun poly (L-lactide-co-glycolide) biodegradable polymer nanofibre tubes for peripheral nerve regeneration. Nanotechnology, 2004. 15(11): p. 1459. [CrossRef]
- Chew, S.Y., et al., Aligned Protein-Polymer Composite Fibers Enhance Nerve Regeneration: A Potential Tissue-Engineering Platform. Adv Funct Mater, 2007. 17(8): p. 1288-1296. [CrossRef]
- Kartha, K.K., et al., Attogram sensing of trinitrotoluene with a self-assembled molecular gelator. J Am Chem Soc, 2012. 134(10): p. 4834-41. [CrossRef]
- Hosseinkhani, H., P.D. Hong, and D.S. Yu, Self-assembled proteins and peptides for regenerative medicine. Chem Rev, 2013. 113(7): p. 4837-61. [CrossRef]
- Chassenieux, C. and C. Tsitsilianis, Recent trends in pH/thermo-responsive self-assembling hydrogels: from polyions to peptide-based polymeric gelators. Soft Matter, 2016. 12(5): p. 1344-59. [CrossRef]
- Collier, J.H., Modular self-assembling biomaterials for directing cellular responses. Soft Matter, 2008. 4(12): p. 2310-2315. [CrossRef]
- Guo, J., et al., Self-assembling peptide nanofiber scaffold promotes the reconstruction of acutely injured brain. Nanomedicine: Nanotechnology, Biology and Medicine, 2009. 5(3): p. 345-351. [CrossRef]
- Ellis-Behnke, R., K.-F. So, and S. Zhang, Molecular repair of the brain using self-assembling peptides. Chimica oggi, 2006. 24(4): p. 42-45.
- Ellis-Behnke, R., et al., Using nanotechnology to design potential therapies for CNS regeneration. Current pharmaceutical design, 2007. 13(24): p. 2519-2528. [CrossRef]
- Zhang, N., et al., A self-assembly peptide nanofibrous scaffold reduces inflammatory response and promotes functional recovery in a mouse model of intracerebral hemorrhage. Nanomedicine, 2016. 12(5): p. 1205-17. [CrossRef]
- Sarkar, B., et al., In vivo neuroprotective effect of a self-assembled peptide hydrogel. 2021. 408: p. 127295. [CrossRef]
- Zhang, S., et al., Self-complementary oligopeptide matrices support mammalian cell attachment. 1995. 16(18): p. 1385-1393. [CrossRef]
- Leung, G.K.K., Y.C. Wang, and W.J.M.i.E. Wu, Peptide nanofiber scaffold for brain tissue reconstruction. 2012. 508: p. 177-190.
- Ellis-Behnke, R.G., et al., Nano neuro knitting: peptide nanofiber scaffold for brain repair and axon regeneration with functional return of vision. 2006. 103(13): p. 5054-5059. [CrossRef]
- Ohno, Y., et al., Amphiphilic peptide-tagged N-cadherin forms radial glial-like fibers that enhance neuronal migration in injured brain and promote sensorimotor recovery. Biomaterials, 2023. 294: p. 122003. [CrossRef]
- Sahab Negah, S., et al., Transplantation of human meningioma stem cells loaded on a self-assembling peptide nanoscaffold containing IKVAV improves traumatic brain injury in rats. Acta Biomater, 2019. 92: p. 132-144. [CrossRef]
- Teo, W., A Review on Electrospinning Design and Nanofibre Assemblies. Nanotechnology, 2006. 17: p. R89-R106. [CrossRef]
- Venugopal, J., et al., Interaction of cells and nanofiber scaffolds in tissue engineering. Journal of Biomedical Materials Research Part B: Applied Biomaterials, 2008. 84(1): p. 34-48.
- Smith, L. and P. Ma, Nano-fibrous scaffolds for tissue engineering. Colloids and surfaces B: biointerfaces, 2004. 39(3): p. 125-131. [CrossRef]
- Kumbar, S., et al., Electrospun nanofiber scaffolds: engineering soft tissues. Biomedical materials, 2008. 3(3): p. 034002. [CrossRef]
- Alhosseini, S.N., et al., Synthesis and characterization of electrospun polyvinyl alcohol nanofibrous scaffolds modified by blending with chitosan for neural tissue engineering. Int J Nanomedicine, 2012. 7: p. 25-34. [CrossRef]
- Yang, G., et al., From nano to micro to macro: Electrospun hierarchically structured polymeric fibers for biomedical applications. 2018. 81: p. 80-113. [CrossRef]
- Zech, J., et al., Electrospun Nimodipine-loaded fibers for nerve regeneration: Development and in vitro performance. 2020. 151: p. 116-126. [CrossRef]
- Bhattarai, R.S., et al., Biomedical applications of electrospun nanofibers: Drug and nanoparticle delivery. 2018. 11(1): p. 5. [CrossRef]
- Feng, X., et al., Electrospun polymer micro/nanofibers as pharmaceutical repositories for healthcare. 2019. 302: p. 19-41. [CrossRef]
- Gommans, H., et al., Electro-Optical Study of Subphthalocyanine in a Bilayer Organic Solar Cell. Advanced functional materials, 2007. 17(15): p. 2653-2658. [CrossRef]
- Li, W., et al., Electrospun nanofibers immobilized with collagen for neural stem cells culture. Journal of Materials Science: Materials in Medicine, 2008. 19(2): p. 847-854. [CrossRef]
- Qian, J., et al., Functionalization strategies of electrospun nanofibrous scaffolds for nerve tissue engineering. 2021. 2: p. 260-279. [CrossRef]
- Sulejczak, D., et al., Electrospun nanofiber mat as a protector against the consequences of brain injury. Folia Neuropathol, 2014. 52(1): p. 56-69. [CrossRef]
- Maclean, F.L., et al., Galactose-functionalised PCL nanofibre scaffolds to attenuate inflammatory action of astrocytes in vitro and in vivo. J Mater Chem B, 2017. 5(22): p. 4073-4083. [CrossRef]
- Williams, D., Benefit and risk in tissue engineering. Materials Today, 2004. 7(5): p. 24-29. [CrossRef]
- Zimmermann, H., et al., Towards a medically approved technology for alginate-based microcapsules allowing long-term immunoisolated transplantation. Journal of materials science: Materials in Medicine, 2005. 16(6): p. 491-501. [CrossRef]
- Shapiro, J.M. and M.L. Oyen, Hydrogel composite materials for tissue engineering scaffolds. Jom, 2013. 65(4): p. 505-516. [CrossRef]
- Gunatillake, P.A., R. Adhikari, and N. Gadegaard, Biodegradable synthetic polymers for tissue engineering. Eur Cell Mater, 2003. 5(1): p. 1-16.
- Bergsma, J.E., et al., In vivo degradation and biocompatibility study of in vitro pre-degraded as-polymerized polylactide particles. Biomaterials, 1995. 16(4): p. 267-274. [CrossRef]
- Boontheekul, T., H.-J. Kong, and D.J. Mooney, Controlling alginate gel degradation utilizing partial oxidation and bimodal molecular weight distribution. Biomaterials, 2005. 26(15): p. 2455-2465. [CrossRef]
- Saha, S.K. and H. Tsuji, Effects of molecular weight and small amounts of d-lactide units on hydrolytic degradation of poly (l-lactic acid) s. Polymer degradation and stability, 2006. 91(8): p. 1665-1673. [CrossRef]
- Makadia, H.K. and S.J. Siegel, Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers, 2011. 3(3): p. 1377-1397. [CrossRef]
- Tsuji, H., A. Mizuno, and Y. Ikada, Properties and morphology of poly (L-lactide). III. Effects of initial crystallinity on long-term in vitro hydrolysis of high molecular weight poly (L-lactide) film in phosphate-buffered solution. Journal of Applied Polymer Science, 2000. 77(7): p. 1452-1464.
- Suzui, M., et al., Multiwalled carbon nanotubes intratracheally instilled into the rat lung induce development of pleural malignant mesothelioma and lung tumors. Cancer Sci, 2016. 107(7): p. 924-35. [CrossRef]
- Liu, X., et al., Integrated printed BDNF-stimulated HUCMSCs-derived exosomes/collagen/chitosan biological scaffolds with 3D printing technology promoted the remodelling of neural networks after traumatic brain injury. Regen Biomater, 2023. 10: p. rbac085. [CrossRef]
- Tang, W., et al., Aligned Biofunctional Electrospun PLGA-LysoGM1 Scaffold for Traumatic Brain Injury Repair. ACS Biomater Sci Eng, 2020. 6(4): p. 2209-2218. [CrossRef]
- Mahumane, G.D., et al., Repositioning N-Acetylcysteine (NAC): NAC-Loaded Electrospun Drug Delivery Scaffolding for Potential Neural Tissue Engineering Application. Pharmaceutics, 2020. 12(10). [CrossRef]
- Zhou, L., et al., Combining PLGA Scaffold and MSCs for Brain Tissue Engineering: A Potential Tool for Treatment of Brain Injury. Stem Cells Int, 2018. 2018: p. 5024175. [CrossRef]
- Álvarez, Z., et al., Neurogenesis and vascularization of the damaged brain using a lactate-releasing biomimetic scaffold. Biomaterials, 2014. 35(17): p. 4769-81. [CrossRef]
- Zhang, Y., et al., Treatment of Traumatic Brain Injury with Vepoloxamer (Purified Poloxamer 188). J Neurotrauma, 2018. 35(4): p. 661-670. [CrossRef]
- Macks, C., et al., Dexamethasone-Loaded Hydrogels Improve Motor and Cognitive Functions in a Rat Mild Traumatic Brain Injury Model. Int J Mol Sci, 2022. 23(19). [CrossRef]
- Liu, X.Y., et al., 3D printing of injury-preconditioned secretome/collagen/heparan sulfate scaffolds for neurological recovery after traumatic brain injury in rats. Stem Cell Res Ther, 2022. 13(1): p. 525. [CrossRef]
- Liu, X., et al., Hyaluronan-based hydrogel integrating exosomes for traumatic brain injury repair by promoting angiogenesis and neurogenesis. Carbohydr Polym, 2023. 306: p. 120578. [CrossRef]
- Tanikawa, S., et al., Engineering of an electrically charged hydrogel implanted into a traumatic brain injury model for stepwise neuronal tissue reconstruction. Sci Rep, 2023. 13(1): p. 2233. [CrossRef]
- Hu, Y., et al., An ECM-Mimicking, Injectable, Viscoelastic Hydrogel for Treatment of Brain Lesions. Adv Healthc Mater, 2023. 12(1): p. e2201594. [CrossRef]
- Moisenovich, M.M., et al., Effect of Silk Fibroin on Neuroregeneration After Traumatic Brain Injury. Neurochem Res, 2019. 44(10): p. 2261-2272. [CrossRef]
- Chen, X., et al., Surface-fill H2S-releasing silk fibroin hydrogel for brain repair through the repression of neuronal pyroptosis. 2022. 154: p. 259-274. [CrossRef]
- Jiang, J., et al., Implantation of regenerative complexes in traumatic brain injury canine models enhances the reconstruction of neural networks and motor function recovery. Theranostics, 2021. 11(2): p. 768-788. [CrossRef]
- Qian, F., et al., In Situ implantable, post-trauma microenvironment-responsive, ROS Depletion Hydrogels for the treatment of Traumatic brain injury. Biomaterials, 2021. 270: p. 120675. [CrossRef]
- Chen, T., et al., Loading neural stem cells on hydrogel scaffold improves cell retention rate and promotes functional recovery in traumatic brain injury. Mater Today Bio, 2023. 19: p. 100606. [CrossRef]
- Ma, X., et al., Angiogenic peptide hydrogels for treatment of traumatic brain injury. Bioact Mater, 2020. 5(1): p. 124-132. [CrossRef]
- Hackelbusch, S., et al., Hybrid microgels with thermo-tunable elasticity for controllable cell confinement. Advanced Healthcare Materials, 2015. 4(12): p. 1841-1848. [CrossRef]
- Bjugstad, K., et al., Biocompatibility of poly (ethylene glycol)-based hydrogels in the brain: An analysis of the glial response across space and time. Journal of Biomedical Materials Research Part A, 2010. 95(1): p. 79-91. [CrossRef]
- Tamariz, E., et al., Delivery of chemotropic proteins and improvement of dopaminergic neuron outgrowth through a thixotropic hybrid nano-gel. Journal of Materials Science: Materials in Medicine, 2011. 22(9): p. 2097-2109. [CrossRef]
- Carvalho, A., et al., Magnetic dehydrodipeptide-based self-assembled hydrogels for theragnostic applications. Nanomaterials, 2019. 9(4): p. 541. [CrossRef]
- Koss, K. and L. Unsworth, Neural tissue engineering: Bioresponsive nanoscaffolds using engineered self-assembling peptides. Acta biomaterialia, 2016. 44: p. 2-15. [CrossRef]
- Cui, W., Y. Zhou, and J. Chang, Electrospun nanofibrous materials for tissue engineering and drug delivery. Science and Technology of Advanced Materials, 2010. 11(1): p. 014108. [CrossRef]
- Sulejczak, D., et al., Original articleElectrospun nanofiber mat as a protector against the consequences of brain injury. Folia Neuropathologica, 2014. 52(1): p. 56-69. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



