
Submitted:
28 August 2023
Posted:
29 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The BNT162b2 vaccine is globally used for preventing morbidity and mortality related to COVID-19. Cancer patients have had priority for receiving the vaccine due to their diminished immunity. This study reports the response of administering the 3rd and 4th vaccine doses to can-cer patients receiving active anti-neoplastic treatment. 142 patients have received two doses of the mRNA-based BNT162b2 COVID-19 vaccine, while 76 and 25 patients have received three and four doses, respectively. The efficacy of the humoral response following two vaccine doses was diminished in cancer patients, especially in the group of patients receiving chemotherapy. In a multivariate analysis, patients after three and four BNT162b2 vaccine doses were more likely to have antibody titers in the upper tertile compared to patients after two doses of the vaccine (odds ratio (OR) 7.62 (95% CI 1.38-42.12), p=0.02 and 17.15 (95% CI 5.01-58.7), p<0.01, respective-ly). Unlike the response after two doses, the 3rd and 4th BNT162b2 vaccine booster doses, had an increased efficacy of 95-100% in cancer patients while on active treatment. This result could be explained by different mechanisms including the development of memory B cells.
Keywords:
SARS-CoV-2
; BNT162b2 vaccine
; cancer patients
; anti-neoplastic treatment
; chemotherapy
; antibodies
; immunogenicity.
1. Introduction
After the global outbreak of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the high number of deaths caused by the coronavirus disease (COVID-19) [1,2,3], a pandemic was declared on 11 March 2020 by the World Health Organization (WHO) [4]. Immune-compromised individuals have been more susceptible to the disease [5,6]. Cancer patients are at higher risk for SARS-CoV-2 infection and have a higher mortality rate than the general population [7,8,9]. This is probably related to the low activity state of their immune system, due to their cancer disease and the immunosuppressive treatments they receive [10,11]. The United States Food and Drug Administration, (FDA), have urgently approved the (SARS-CoV-2) vaccines, including the BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna Biotech), to reduce the spread of infection and its severity [12,13].
While several trials have shown a relatively reduced immunogenicity for BNT162b2 vaccine in patients with solid tumors receiving anti-neoplastic treatment [14,15,16], a recent prospective trial has shown that most patients develop an adequate antibody response to vaccination with the mRNA-1273 COVID-19 vaccine [17]. Most of these trials have tested the effect after one or 2 doses of the BNT162b2 vaccine [18].
In Israel, the BNT162b2 vaccine has been widely used [19,20], and cancer patients have had priority for receiving the vaccine [21]. We previously reported that after two doses of BNT162b2 vaccine, a reduced immunogenicity was observed in this group of patients especially in those receiving chemotherapy [22].
The aim of the present study was to assess the response of cancer patients undergoing anti neoplastic treatments, to the mRNA SARS-CoV-2 vaccine additional 3rd and 4th doses.
The current study reports that administrating anti COVID-19 vaccine, 3rd and 4th doses, to a group of cancer patients while on anti-neoplastic treatments has a high efficacy, resulting in 95-100% response rate demonstrated by all participants developing antibodies to COVID-19, following the 4th dose.
2. Materials and Methods
2.1. Study Design and Participants
The Institutional Review Boards of the Edith Wolfson Medical Center (WMC) and Bnai Zion Medical Center (BZMC) approved the study protocol. A written informed consent was signed by all participants who were recruited at both medical centers between January 2021 and February 2022. Inclusion criteria were ≥18 years old oncology patients, bearing solid tumors who were receiving active antineoplastic treatment when the second, third and fourth dose of the BNT162b2 vaccine (Pfizer-BioNTech, Kalamazoo, MI, USA) was administered. The third and fourth vaccine doses were administered six and three months (respectively) from the previous vaccine, while the second dose was delivered three weeks following the first vaccine dose. Participants who acquired COVID-19 or had a serological response indicating a past infection, were excluded.
Participants filled a survey recording demographic parameters such as age, gender, previous cancer disease, history of exposure to COVID-19 and vaccination dates. Medical charts were used to obtain clinical data such as cancer types, and treatment regimen protocols (Table 1). Patients included in the study had gastrointestinal cancers (colon, gastric, esophagus, ampullary, pancreas and cholangiocarcinoma), breast, lung, urinary cancers (bladder, kidney, and prostate), gynecological cancers (ovarian and uterine), melanoma and other cancers. Patients undergoing treatment were analyzed based on the treatment type, chemotherapy and non-chemotherapy-containing regimens such as immunotherapy and biological drugs. Chemotherapy drugs used for treatment included: gemcitabine, eribulin, paclitaxel, carboplatin, oxaliplatin, cisplatin, irinotecan, fluorouracil, etoposide, pemetrexed, vincristine, doxorubicin, and cyclophosphamide. Immunotherapy drugs included pembrolizumab, nivolumab, ipilimumab, durvalumab, avelumab, atezolizumab, and cemiplimab. Biological drugs included trastuzumab, pertuzumab, panitumumab, ribociclib, axitinib, regorafenib, olaparib, and Lenvatinib.
2.2. Determination of Anti-SARS-CoV-2 Antibodies Level
COVID-19 vaccine triggers the immune system against the S-protein, which is detected through laboratory analysis. Anti-SARS-CoV-2 antibodies level was determined as previously described [22]. Briefly, at least 7 days after the administration of the second, third or fourth vaccine dose, peripheral venous blood samples were obtained from the participants. Serum was separated and held at 4 ºC prior to testing. IgG testing was performed at the WMC Immunology Laboratory using the SARS-CoV-2 IgG II Quant assay on an ARCHITECT analyzer (Abbott). This high-throughput chemiluminescent microparticle immunoassay is able to quantify IgG antibodies that bind to the receptor binding domain of the S1 subunit of the SARS-CoV-2 spike protein. Antibodies titers serve as a way of protection against COVID-19 after vaccination, and are indicators for vaccine efficacy through their neutralizing activity The assay threshold was 6.5 arbitrary units (AU) per mL and its maximal quantitation reached 40,000 AU. IgG levels < 50 AU/mL were considered negative, values between 50 AU/mL and 150 AU/mL were considered borderline, values > 150 AU/mL were included as positive results. For the purpose of the analysis, participants with borderline response were considered negative.
The serum samples from patients collected after three and four vaccine doses were also assessed for the presence of antibodies against the SARS-CoV-2 nucleocapside (anti-N) using the SARS-CoV-2 IgG on an ARCHITECT analyzer. The assay was used to identify participants with an adaptive immune response to SARS-CoV-2, indicating recent or prior infection. Participants with COVID-19 Anti N IgG (S/C index) above 1.4 were considered positive according to the manufacturer's instructions, and excluded from the study.
2.3. Statistical Analysis
Categorical variables were summarized as frequency and percentage. Continuous variables were evaluated for normal distribution using histogram and box plot and reported as Mean and Standard Deviation (SD) for normally distributed variables or as Median and Interquartile Range (IQR) for skewed variables. Continuous variables were compared using Independent Samples t Test or the Mann–Whitney test. Crude and Adjusted Odds Ratio were evaluated using logistic regression. Age, gender, days from last COVID-19 vaccine and chemotherapy were included in the multivariate analysis. All statistical tests were two tailed. p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, version 27, IBM Corp., Armonk, NY, USA, 2020)
3. Results
3.1. Study Population
Two hundred and forty-three cancer patients with active anti-neoplastic treatment were included in the study. One hundred and forty-two patients have received two doses of BNT162b2 vaccine, 76 patients, have received three doses and 25 patients four doses of the anti-SARS-CoV-2 vaccine. The patients’ demographic characteristics, cancer types and treatments are summarized in Table 1. The median age was 67 years (IQR 56.75-75), 66.5 years (IQR 57-74.75) and 72 years (IQR 67.5-79) in the second, third and fourth vaccine dose cohorts respectively. Men were representing 54.9%, 56.6% and 60% of the patients in the second, third and fourth vaccine dose cohorts. The highest incidence cancer types were gastrointestinal, breast and lung malignancies. The treatment regimens were administered by chemotherapy agents or non-chemotherapy such as immunotherapy and biological agents.

Table 1.
Demographic and clinical characteristics of participants receiving BNT162b2 vaccine dose.
| After 2nd dose | After 3rd dose | After 4th dose | |
|---|---|---|---|
| Frequency (n) | 142 | 76 | 25 |
| Age, median years (IQR) | 67 (56.75-75) | 66.5 (57-74.75) | 72 (67.5-79) |
| Male, (%) | 78 (54.9) | 43 (56.6) | 15 (60) |
| Time from last BNT162b2 dose, median days (IQR) | 35 (24.5-46.25) | 147 (130.5-160.8) | 18 (12-25) |
| Type of Cancer, n (%) | |||
| Gastrointestinal | 49 (34.5) | 42 (55.3) | 10 (40) |
| Breast | 30 (21.1) | 12 (15.8) | 3 (12) |
| Lung | 28 (19.7) | 10 (22.7) | 6 (24) |
| Urinary | 13 (9.2) | 3 (3.9) | 2 (8) |
| Melanoma | 7 (4.9) | 4 (5.3) | 3 (12) |
| Gynecological | 9 (6.3) | 2 (2.6) | 0 |
| Other types | 6 (4.2) | 3 (3.94) | 1 (4) |
| Treatment, n (%) | |||
| Chemotherapy | 73 (51.4) | 56 (73.7) | 13 (52) |
| Non Chemotherapy | 69 (48.6) | 20 (26.3) | 12 (48) |
3.2. Antibody Levels and Seropositivity Response to BNT162b2 Vaccine
The median SARS-CoV-2 IgG levels were significantly different (p< 0.001) among the groups: median IgG levels following the second vaccine dose were 2232 AU/mL (IQR 445-8023); 4025 AU/mL (IQR 1676-7884) and 24465 AU/ml (IQR 1245-40000) after the third and fourth BNT162b2 doses, respectively (Table 2 and Figure 1a). When the humoral response was stratified according to the treatment received, only after the second vaccine there were significant differences in seropositivity (Figure.1b) and antibody levels (Figure 1a and Table 2) between participants who received chemotherapy and those who did not (p<0.001).
Analyzing the IgG response between patients actively recieving chemotherapy vs. non chemotherapy demonstrated no significant difference in antibodies levels (Table 2, and Figure 1a (p=0.443 and p=0.81 respectively) and in seropositivity (Figure 1b) after the third and fourth vaccine doses.
No significant adverse-effects of the vaccines were reported among the participant cancer patients (data not shown).
Figure 2 compares the effect of different variables between patients after two, three or four vaccine doses.
After adjusting for gender, age, and days from sample collection since the last COVID-19 vaccine and chemotherapy treatment, patients after third and fourth mRNA BNT162b2 vaccine doses had a significantly higher probability to have antibody titers in the upper tertile compared to patients after two doses of the vaccine (odds ratio (OR) 7.62 (95% CI 1.38-42.12), p=0.02 and 17.15 (95% CI 5.01-58.7), p<0.01, respectively). The titer of antibodies and their binding assay to specific SARS-CoV-2 depends on the individual and usually high titer correlated with long persistence.
There was no significant difference in gender among the participants. The age, however was different, patients who received four doses of the vaccine were older than those receiving two or three doses. Nevertheless, their serologic response was not impaired (Table 2).
Although the time since the last vaccine dose was significantly longer in patients after three doses of vaccine, their serologic response was still positive.
4. Discussion
COVID-19 outbreak has caused an unprecedented challenge for the medical system worldwide [23,24,25]. High morbidity rates among individuals with chronic conditions and senior individuals have been recorded [26,27]. Patients with conditions such as immune-suppression were at higher risk for getting infected by the SARS virus, complications and mortality [28]. Cancer patients have a higher risk and susceptibility to infectious diseases (especially respiratory system) due to a compromised immune system as a result of the chronic disease and the immune-suppressive treatments they receive [29]. Many studies have highlighted the importance of the vaccine for this group of patients [30,31]. Following the first two vaccine doses the majority of cancer patients surveyed, have been found to carry antibodies against COVID-19 with diminished level in patients receiving chemotherapy [32,33].
We have previously analyzed the humoral response following vaccination with the second dose of BNT162b2 in patients with solid malignancies who were receiving anti-cancer therapy at the time of vaccination. It was compared to a matched group of participants who had not been diagnosed with cancer. The humoral response of cancer patients on active anti-neoplastic treatment was significantly reduced including seronegative results and lower antibody levels compared with that of non-cancer individuals [22,34].
The present study analyzes the humoral response of cancer patients with solid malignancies following the third and fourth doses of BNT162b2 vaccine.
Interestingly, 74 of 76 cancer patients were seropositive (97.4%) following the third dose of anti-COVID-19 vaccine compared to 85.7% of cancer patients tested after the second vaccine dose in previous study [22]. Similar results were also reported for solid-organ transplant recipients, where 44% of the recipients who had been seronegative after 2 doses of BNT162b2 vaccine became seropositive following the administration of a third vaccine dose [35]. Moderna mRNA-1273 vaccine also responded in a higher antibody titer in kidney transplant recipients who were borderline responsive after two doses [36].
Additionally, the recent study has shown no significant difference between the anti-cancer protocols i.e., all participants who received the fourth BNT162b2 dose were seropositive regardless of their treatment regimen, chemotherapy vs non-chemotherapy. This may indicate that the patients' immune system could still respond well to the immunization. The path/process of producing IgG could be unharmed and work independently as a result of the immunization program without being affected by the active anti-cancer treatment.
Some explanations regarding these results can be postulated: first, cancer patients have a diminished immune response to vaccinations due to their underlying malignancy and anti-cancer treatment [37,38]. As a result, their humoral immunity can be boosted by additional doses of BNT162b2 vaccine that can lead to a more robust immune response reflected by higher antibody levels [39,40,41,42,43].
Second, varied timing of the antibody sampling may represent different levels of antibody response. A previous study was conducted 7 days after 2nd vaccination was administered [22] while in the present study, the blood collection was done at a median of 140 days (IQR 130.5-160.8) and 18 days (IQR 12-25) following the third and fourth vaccine dose respectively. The finding of such high seropositive percentage of patients bearing antibodies to SARS-CoV-2, over 4 months following the third vaccine administration could point to the long duration of the response to this dose. Antibody levels may have been low immediately after the second dose, but increase progressively over time. Shroff et al. [44] evaluated the immune response after third dose of BNT162b2 vaccine in a phase 1 trial of 20 cancer cohort patients on active anti-cancer therapy. Supporting the timely gradual development of antibodies, their report included two participants who initially were found to be seronegative by one week after the second vaccination, however their follow-up monitoring detected antibodies before the third dose. Similar results were reported by Shmueli et al. [45]. This suggests that, for at least a subset of the non-responding cancer cohort, antibody responses might be delayed however not completely absent.
Six months following BNT162b2 vaccination, immunity in immunocompetent individuals has reportedly started to decline [46,47,48,49]. A BNT162b2 booster dose can increase the antibody neutralization level by an average of 5 to 7 times, compared with that after a second dose [50,51,52]. Another study with 20 cancer patients, having solid tumours actively treated, who were seronegative after the second of BNT162b2 dose, showed 95% seropositivity after the administratin of the third BNT162b2 vaccine [53].
In addition to humoral and T cell mediated immunity, memory B cells play a major role in seropositivity to COVID-19 vaccinations and are predictive of anamnestic responses after booster vaccination. Vietri et al. assumed that SARS-CoV-2-specific memory lymphocytes induced by the first vaccination trigger a faster and more effective antibody response following a booster vaccine [54,55,56,57,58,59]. Moreover, Shroff [44] detected spike receptor-binding domain and other S1-specific memory B cell subsets as potential predictors of anamnestic responses to additional immunizations in most patients with cancer.
BNT162b2 third vaccine dose was reported to elevate immunogenicity in bone marrow transplantation patients [60,61].
Healthcare workers vaccinated with two doses of mRNA 1273 in Belgium were observed to have a higher titer compared with the individuals vaccinated with BNT162b2 [62]. Moderna mRNA COVID-19 vaccine was found in real-world data to be more effective than Pfizer-BioNTech (95% vs 88% respectively) in protecting immunocompromised individuals from hospitalization in the U.S.A following two doses [63]. A plausible reason was attributed to the higher concentration of the vaccine and the fact that the first two doses were administered 28 days apart, while the BNT162b2 vaccine was subcutaneously injected 21 days after the first vaccine. Oosting et al. [17] evaluated in the Netherlands, the immunogenicity response of patients with solid tumors undergoing different treatment regimens to mRNA-1273 (Moderna Biotech). Their finding indicated that the SARS-CoV-2 binding was of similar magnitude among all cancer patients after two doses, regardless of the treatment they received (chemotherapy, immunotherapy or combined chemoimmunotherapy). Moderna's mRNA-1273 vaccine durability of high response level, was measured at 4 months following the second dose was longer than the Pfizer's BNT162b2 mRNA vaccine which was waning down at 4-6 months' time. In addition, a study of chronic lymphocytic leukemia and other non-Hodgkin lymphomas showed better antibody responses with the Moderna vaccine than with Pizer-BioNTech vaccine [64].
Hemodialysis immunosuppressed patients responded to fourth vaccine (mRNA-1273) following three BNT162b vaccine doses, showing a strong augmentation of the humoral immunity against SARS-CoV-2 variants compared with pre vaccination level. These dialysis patients also had an increase in T-cell responses as a result of the fourth vaccine [65].
Alexopopoulos et al. [66] have reviewed effective clinical uses of interpreting results of testing for antibody against SARS-CoV-2. Following BNT162B2 vaccine administration the humoral response can be detected by analyzing SARS-CoV-2 IgG of anti-spike IgG within two weeks. It is of utmost importance to be able to understand patients' competence to develop antibodies, considering the role of COVID-19 vaccination is to serve as prophylactic protection against a SARS infection
Alexopopoulos et al. suggests that antibody testing may evaluate the effect of immunosuppressive medications. According to the publication uptake of third dose of vaccination, may protect better than the first and second doses against several variants such as omicron. Omicron mutants (BA.1), evolved and spread during the 4th COVID wave, vary from the original SARS-CoV-2 strains. Therefore, the vaccination through 1st and 2nd doses which took place six months earlier, provided lower protection to this strain [66].
It was reported that among cancer patients who received anti-CD 20 monoclonal antibody, the seroconversion rate following anti COVID vaccination was low up to six month following treatment. However, on later time points such as a year and the seroconversion ability returned [66].
Immune Checkpoint Inhibitors treatment for patients bearing solid tumors was evaluated in relation to seroconversion by Terpos et al. [67]. It was demonstrated that the third dose following anti-COVID-19 vaccination boosted the antibody response in comparison with 1st and 2nd doses. That report supports the present study which showed that after the third vaccine dose, the seropositivity was very high in addition to enhanced humoral response following 3rd dose in patients with solid-tumors.
Most cancer patients with hematological malignancies have low seroconversion rates (84.7%) vs. solid tumor patients (90.3%) after 2 doses. However, seroconversion of Acute Myeloid Leukemia patients was 94.7% [66].
Patients diagnosed with hematological malignancies while on active treatment (including anti-CD20 therapy) were reported to have 76.3% of cases develop humoral immunity. It was reported that among cancer patients who received anti-CD 20 monoclonal antibody, the seroconversion rate following anti COVID vaccination was low for the six months following treatment. However, on a later date (one to two years) the calculated seroconverion rate increased, suggesting that Anti-CD 20 therapy has caused reduced humoral response [66].
Bergamaschi et al., [68] reported that in cancer patients who were immunocompromised due to therapy and had undergone bone-marrow transplantation, response to the 1st and 2nd doses of BNT162b2 mRNA vaccination yielded low-titer of anti-S (SARS-CoV-2 Spike) antibodies to the Wuhan strain in comparison to healthy control cohort. The patients weakened immune system could be impaired during immunosuppressive therapy. In that study, cytokines and chemokines serum levels were also evaluated, as markers of inflammation. Elicited IFN-γ, IP-10/CXCL10 showed the highest presence as a consequence of vaccination, which correlated to antibody titer, nevertheless diminished vis-a vis the control cohort. The analysis demonstrated that cytokines associated with inflammation were upregulated during vaccination. The authors concluded that the BNT162b2 mRNA vaccine induced cytokine changes that could serve as predictors for antibody titer development.
Rosati et al. [69], assessed Multiple Myeloma (MM) and Waldenstrom macroglobulinemia (WM) patient cohorts administered with BNT162b2 mRNA vaccination. The observed increase in neutralizing anti-spike antibody response following the 3rd vaccine, points to its benefit for MM and WM patients on active treatment. Of note, active treatment regimen interfering with antibody development (such as anti-CD-20, anti-CD38, anti-BCMA) revealed relative low response rate in WM and MM patient cohorts showing reduced quantity of SARS-CoV-2 antibodies which could be attributed to impairment in the development of vaccine induced neutralizing antibodies. Nonetheless, patients off-therapy showed increased response rates 30 days after the 3rd vaccine dose.
A review of 60 studies evaluating COVID-19 vaccine efficacy in patients with either solid tumors or hematological malignances was conducted by Liatsou et al., [70]. The findings regarding humoral response showed that after the third vaccine dose the effect size of the seroconversion rate for patients on active therapy, was estimated at 0.63 (95%CI: 0.54-0.72) for hematological cancers and 0.88 (95% CI: 0.75-0.97) for solid tumors. Patients' cohort with hematological malignancies were more affected in terms of anti-SARS-CoV-2 production due to type of cancer and treatment with monoclonal antibodies.
In conclusion oncology patients with hematological malignancies should be protected by vaccination to augment their immune response and any other available anti-viral drugs as prophylaxis measure.
The neutralizing antibodies level following vaccination against the SARS-CoV-2 in cancer patients treated with targeted therapies were assessed by Zagouri et al. [71]. The solid tumors bearing patients were diagnosed with breast, ovarian or prostate malignancy. The targeted therapies administered to the breast cancer patients were cyclin D kinase 4/6 inhibitors and hormonal therapy, for ovarian cancer patients, poly (ADP-ribose) polymerase inhibitors, and for prostate cancer patients an androgen receptor targeted agent. The third BNT162b2 mRNA vaccine has boosted the neutralizing antibodies levels one month after vaccination, in all cancer treated patient groups, however they were lower in comparison to healthy individuals control group. Nevertheless, these results suggest that neoplasms harboring patients receiving targeted therapies should be offered protective third vaccine dose against COVID-19.
Limitations of the study include small cohorts and non-uniform time of sampling the participants. Future research directions may incorporate expanded cohort size and explore additional mechanisms involved in immunity to SARS-CoV-2 following vaccination. It is important to note that by the time the third and fourth anti-COVID-19 vaccine were introduced, different virus variants of concern were spreading the infection in Israel and worldwide. Therefore, the production of the vaccine by the pharmaceutical companies such as Pfizer have been adapted and updated accordingly, to be specific to delta / omicron strains. Furthermore, studying the response to Moderna third and fourth anti-COVID-19 vaccine doses could be beneficial as apparently these mRNA vaccines were providing better protection to cancer patients.
5. Conclusions
In contrast to the 2nd dose of anti-COVID-19 vaccine, the 3rd and 4th doses administered to cancer patients, while on anti-neoplastic treatments, had a high humoral response in chemotherapy as well as in non-chemotherapy treated patients.
Distinct pathways contribute to vaccine immunity with different measurable tests such as humoral immunity and T cell activity. While these tests provide valuable information they are not the only indicators of immunity with and the vast majority of cancer patients have some level of protection against COVID-9 even if antibody or T-cell levels are not as high as expected. The titer of antibodies and their binding assay to specific SARS-CoV-2 depends on the individual and usually high titer correlated with long persistence.
Author Contributions
Conceptualization, A.A. and R.B.; methodology, I.S. and O.S.; software, T.Z.-B.; validation, I.S.; formal analysis, T.Z.-B. and I.S.; investigation, I.S.; resources, AA and RB.; data curation, IS.; writing—original draft preparation, I.S.; writing—review and editing, A.A.; visualization, I.S. and T.Z.-B.; supervision, R.B. project administration, A.A and R.B..; funding acquisition, A.A. and R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Boards of Edith Wolfson Medical Center and Bnai Zion Medical Center (protocols code 0010-21 WOMC and 0009-21-BNZ respectively).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors
Acknowledgments
The authors thank the participants, the clinical study coordinators and the nursing staff members at the Oncology Institutes in the Wolfson and Bnai-Zion Medical Centers.
Conflicts of Interest
The authors declare no conflict of interest
References
- WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data (accessed on 19 May 2023).
- Ciotti, M.; Ciccozz,i M.;Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57(6), 365-388. [CrossRef]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: a timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. http://doi.org/10.1038/s41577-021-00522-1.
- World Health Organization. WHO Director-General’s Opening Remarks at the Medica Briefing COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-themedia-briefing-on-covid-19-11-march-2020 (accessed on 19 May 2023).
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791.
- Stainer, A.; Amati, F.; Suigo, G.; Simonetta, E.; Gramegna, A.; Voza, A.; Aliberti S. COVID-19 in Immunocompromised Patients: A Systematic Review. Semin. Respir. Crit. Care Med. 2021, 42(6), 839-858. [CrossRef]
- Sengar, M.; Chinnaswamy, G.; Ranganathan, P.; et al. Outcomes of COVID-19 and risk factors in patients with cancer. Nat. Cancer. 2022, 3, 547–551. [CrossRef]
- Russell, B.; Moss, C.L.; Shah, V.; et al. Risk of COVID-19 death in cancer patients: an analysis from Guy’s Cancer Centre and King’s College Hospital in London. Br. J. Cancer. 2021, 125, 939–947.
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Bhushan-Singh, C.; Aneja, R. SARS-CoV-2 Infection in Cancer Patients: Effects on Disease Outcomes and Patient Prognosis. Cancers (Basel). 2020, 12(11), 3266. [CrossRef]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer MH. Systemic immunity in cancer. Nat. Rev. Cancer. 2021, 21(6), 345-359. [CrossRef]
- Norris, J. Tumors Disrupt the Immune System Throughout the Body. University of California San Francisco 2020, Tumors Disrupt the Immune System Throughout the Body | UC San Francisco (ucsf.edu) (accessed on 19 May 2023).
- Teo S.P. Review of COVID-19 mRNA Vaccines: BNT162b2 and mRNA-1273. J. Pharm. Pract. 2022, 35(6), 947-951. [CrossRef]
- The Food and Drug Administration. Available online: Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals | FDA (accessed on 21 May 2023).
- Rahav, G.; Lustig, Y.; Lavee, J.; Benjamini, O.; Magen H.; Hod, T.; Shem-Tov, N.; Shacham Shmueli, E.; Merkel, D.; Ben-Ari, Z.; et al. BNT162b2 mRNA COVID-19 vaccination in immunocompromised patients: A prospective cohort study. eClinicalMedicine 2021, 41, 101158. https://doi.org/.
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel A., Ben-Zvi H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7(8), 1-8. [CrossRef]
- Uaprasert, N.; Pitakkitnukun, P.; Tangcheewinsirikul, N.; Chiasakul, T.; Rojnuckarin, P. Immunogenicity and risks associated with impaired immune responses following SARS-CoV-2 vaccination and booster in hematologic malignancy patients: an updated meta-analysis. Blood Cancer J. 2022, 12, 173. [CrossRef]
- Oosting, S.F.; van der Veldt, A.A.M.; GeurtsvanKessel, C.H.; Fehrmann, R.S.N.; van Binnendijk, R.S.; Dingemans, A.C.; Smit, E.F.; Hiltermann, T.J.N.; den Hartog, G.; Jalving, M.; Westphal, T.T.; Bhattacharya, A.; van der Heiden, M.; Rimmelzwaan, G.F.; Kvistborg, P.; Blank, C.U.; Koopmans, M.P.G.; Huckriede, A.L.W.; van Els, C.A.C.M.; Rots, N.Y.; van Baarle, D.; Haanen, J.B.A.G.; de Vries, E.G.E. mRNA-1273 COVID-19 vaccination in patients receiving chemotherapy, immunotherapy, or chemoimmunotherapy for solid tumours: a prospective, multicentre, non-inferiority trial. Lancet Oncol. 2021, 22(12), 1681-1691. [CrossRef]
- Stampfer, S.D., Goldwater, MS., Jew, S.; et al. Response to mRNA vaccination for COVID-19 among patients with multiple myeloma. Leukemia 2021, 35, 3534–3541. [CrossRef]
- Dagan, N.; Barda, N.; Epten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Eng. J. Med. 2021, 384, 1412–1423. [CrossRef]
- Leshem, E.; Wilder-Smith, A. COVID-19 vaccine impact in Israel and a way out of the pandemic. Lancet 2021, 397(10287), 1783-1785. [CrossRef]
- Jeffay, N. COVID vaccine effective for 90% of cancer patients, Israeli study finds. The Times of Israel. 2021. Available on line COVID vaccine effective for 90% of cancer patients, Israeli study finds | The Times of Israel (accessed on 23 May 2023).
- Agbarya, A.; Sarel, I.; Ziv-Baran, T.; Agranat, S.; Schwartz, O.; Shai, A.; Nordheimer, S.; Fenig, S.; Shechtman, Y.; Kozlener, E.; Taha, T.; Nasrallah, H.; Parikh, R.; Elkoshi, N.; Levy, C.; Khoury, R.; Brenner, R. Efficacy of the mRNA-Based BNT162b2 COVID-19 Vaccine in Patients with Solid Malignancies Treated with Anti-Neoplastic Drugs. Cancers, 2021, 13(16), 4191. [CrossRef]
- Isasi, F.; Naylor, M.D., Skorton, D.; Grabowski, D.C.; Hernández, S.; Montomery Rice, V. Patients, Families, and Communities COVID-19 Impact Assessment: Lessons Learned and Compelling Needs. NAM Perspect. 2021, 2021: 1.31478/202111c. [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Chen, G. Long COVID and its management. Int. J. Biol. Sci. 2022, 18(12), 4768-4780. [CrossRef]
- World Health Organization. Chapter 2. Current context: the COVID-19 pandemic and continuing challenges to global health. Available online: https://www.who.int/about/funding/invest-in-who/investment-case-2.0/challenges: (accessed on 24 May 2023).
- Fekadu, G.; Bekele, F.; Tolossa, T.; Fetensa, G.; Turi, E.; Getachew, M.; et al. Impact of COVID-19 pandemic on chronic diseases care follow-up and current perspectives in low resource settings: a narrative review. Int. J. Physiol. Pathophysiol. Pharmacol. 2021, 13(3), 86-93.
- Kang S.J.; Jung, S.I. Age related Morbidity and mortalities among Patients with COVID-19. Infect Chemother. 2020, 52(2), 154-164. [CrossRef]
- Tassone, D.; Thompson, A.; Connell, W.; Lee, T.; Ungaro, R.; An, P.; Ding, Y.; Ding, N.S. Immunosuppression as a risk factor for COVID-19: a meta-analysis. Intern. Med. J. 2021 51(2), 199-205. [CrossRef]
- Seo, S.K.; Liu C.; Dadwal, S.S. Infectious Disease Complications in Cancer Patients. Crit Care Clin. 2021, 37(1), 69-84. [CrossRef]
- Kim, A.H.J.; Sparks, J.A. Immunosuppression and SARS-CoV-2 breakthrough infections. Lancet Rheumatology. 2022, COMMENT 4 (6), E379-E380. https://doi.org/.
- Trapani, D.; Curlgliano, G. COVID-19 vaccines in patients with cancer. Lancet Oncol. 2021, 22(6), 738-739. https://doi.org/.
- Monin, L.; Laing, A.G.; Munoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: interim analysis of a prospective observational study Lancet Oncol. 2021, 22(6), 765-778. https://doi.org/.
- Guven, D.C.; Sahin, T.K.; Klickap, S.; Uckun, F.M. Antibody Responses to COVID-19 Vaccination in Cancer: A Systematic Review. Front. Oncol. 2021, 11, 2021. [CrossRef]
- Fendler, A.; de Vries, E.G.E; GeurtsvanKessel, C.H.; Haanen, J.B.; Wörmann, B.; Turajlic, S.; von Lilienfeld-Toal, M. COVID-19 vaccines in patients with cancer: immunogenicity, efficacy and safety. Nat. Rev. Clin. Oncol. 2022, 19, 385–401. [CrossRef]
- Kamar, N.; Abravenel, F.; Narion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385(7),661-662. [CrossRef]
- Benotmane, I.; Gautier, G.; Perrin, P.; et al. Antibody Response After a Third dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA 2021, 326(11), 1063-1065. [CrossRef]
- Rüthrich, M.M.; Giesen, N.; Mellinghoff, S.C.; Rieger, C.T.; von Lilienfeld-Toal, N.Cellular Immune Response after Vaccination in Patients with Cancer-Review on Past and Present Experiences. Vaccines 2022, 10(2), 182. [CrossRef]
- Negahdaripour, M.; Shafiekhani, M.; Iman Moezzi, S.M.; Amiri, S.; Rasekh, S.; Bagheri, A.; Mosaddeghi, M.; Vazin, A. Administration of COVID-19 vaccines in immunocompromised patients. Int. Immunopharmacol. 2021, 10802. [CrossRef]
- Cohen, I.; Campisi-Pfinto, S.; Rozenberg, O.; Colodner, R.; Bar-Sela, G. The Humoral Response of Patients With Cancer to Breakthrough COVID-19 Infection or the Fourth BNT162b2 Vaccine dose. Oncologist 2023, 28(4), e225-e227. [CrossRef]
- Magen, O.; Waxman, J.G.; Makov-Assif, M.; Vered, R.; Dicker, D.; Hernán M.A.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Dagan, N. Fourth Dose of BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2022, 386(17), 1603-1614. [CrossRef]
- Curlin M.E.; Bates, T.A.; Guzman, G.; Schoen, D.; McBride, S.K.; Carpenter, S.D.; Tafesse F.G. Omicron neutralizing antibody response following booster vaccination compared with breakthrough infection. medRxiv. 2022, 2022.04.11.22273694. [CrossRef]
- Lasagna A, Bergami F, Lilleri D, Percivalle E, Quaccini M, Alessio N, Comolli G, Sarasini A, Sammartino JC, Ferrari A, Arena F, Secondino S, Cicognini D, Schiavo R, Lo Cascio G, Cavanna L, Baldanti F, Pedrazzoli P, Cassaniti I. Immunogenicity and safety after the third dose of BNT162b2 anti-SARS-CoV-2 vaccine in patients with solid tumors on active treatment: a prospective cohort study. ESMO Open 2022, 7(2),100458. [CrossRef]
- Di Noia, V.; Pimpinelli, F.; Renna, D.; Campo, F.; Cosimati, A.; Torchia, A.; Marcozzi, B.; Massacci, A.; Pallocca, M.; Pellini, R.; Morrone, A.; Cognetti, F. Duration of humoral response to the third dose of BNT162b2 vaccine in patients with solid cancer: Is fourth dose urgently needed? Eur. J. Cancer. 2022, 176, 164–167. [CrossRef]
- Shroff, R.T.; Chalasani, P.; Wei, R.; Pennington, D.; Quirk, G.; Schoenle, M.V.; et al. Immune responses to two and three doses of the BNT162b mRNA vaccine in adults with solid tumors. Nat. Med. 2021, 27(11):2002-2011. [CrossRef]
- Shacham Shmueli, E.; Lawrence, Y.R.; Rahav, G.; Itay, A.; Lustig, Y.; Halpern, N.; Boursi, B.; Margalit, O. Serological response to a third booster dose of BNT162b2 COVID-19 vaccine among seronegative cancer patients. Cancer Rep. (Hoboken) 2022, 5(8), e1645. [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; Rubin, C.; Freedman, L.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [CrossRef]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Gavariatopoulou, M.; Gumeni, S.; Malandrakis, P.; et al. Robust Neutralizing Antibody Responses 6 Months post Vaccination with BNT162b2: A Prospective study in 308 Health Individuals. Life 2021, 11(10), 1077. [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-on, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [CrossRef]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; Sundar, R.; Soon, Y.Y. Efficacy of covid-19 vaccines in immunocompromised patients: systematic review and meta-analysis. BMJ. 2022, 376:e068632. [CrossRef]
- Campos, G.R.F., Almeida, N.B.F., Filgueiras, P.S. et al. Booster dose of BNT162b2 after two doses of CoronaVac improves neutralization of SARS-CoV-2 Omicron variant. Commun. Med. 2022, 2, 76. [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; Huppert, A. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, NEJMoa2114255. [CrossRef]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E.; Kitchin, N.; Abslon, J.; Gurtman, A.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, NEHMc2113468. [CrossRef]
- Ligumsky, H.; Dor, H.; Etan, T.; Golomb, I.; Nikolaevski-Berlin, A.; Greenberg, I.; et al. Immunogenicity and safety of BNT162b2 mRNA vaccine booster in actively treated patients with cancer. The Lancet Oncology 2021, 23(2), 193-195. https://doi.org/.
- Vietri, M.T.; Albanese, L.; Passariello, L.; D'Elia, G.; Caliendo, G.; Molinari, A.M.; Angelillo, I.F. Evaluation of neutralizing antibodies after vaccine BNT162b2: Preliminary data. J. Clin. Virol. 2022, 146,105057. [CrossRef]
- Vietri, M.T.; DeElia, G.; Caliendo, G.; Passariello, L.; Albanese, L.; Molinari, A.M.; Angelillo I.F. Antibody levels after BNT162b2 vaccine booster and SARS-CoV-2 Omicron infection. Vaccine 2022, 40(39), 5726-5731. [CrossRef]
- Gray-Gaillard, S.L.; Solis, S.; Monteiro, C.; Chen, H.M.; Ciabattoni, G.; Samanovic, M.I.; Cornelius, A.R.; Williams, T.; Geesey, E.; Rodriguez, M.; Ortigoza, M.B.; Ivanova, E.N.; Koralov, S.B.; Mulligan, M.J.; Herati, R.S. Molecularly distinct memory CD4+ T cells are induced by SARS-CoV-2 infection and mRNA vaccination. bioRxiv. 2022, 2022.11.15.516351. [CrossRef]
- Fiorino, F.; Ciabattini, A.; Sicuranza, A.; Pastore, G.; Santoni, A.; Simoncelli, M.; Polvere, J.; Galimberti, S.; Baratè, C.; Sammartano, V.; Montagnani, F.; Bocchia, M.; Medaglini, D. The third dose of mRNA SARS-CoV-2 vaccines enhances the spike-specific antibody and memory B cell response in myelofibrosis patients. Front. Immunol. 2022, 13, 1017863. [CrossRef]
- Vallejo, A.; Vizcarra, P.; Martin-Hondarza, A.; Gómez-Maldonado, S.; Haemmerle, J.; Velasco, H.; Casado. J.L. Impact of SARS-CoV-2-specific memory B cells on the immune response after mRNA-based Comirnaty vaccine in seronegative health care workers. Front. Microbiol. 2022, 13, 1002748. [CrossRef]
- Ciabattini, A.; Pastore, G.; Fiorino, F.; Polvere, J.; Lucchesi, S.; Pettini, E.; et al. Evidence of SARS-CoV-Specific Memory B Cells Six months after vaccination With the BNT162b2 mRNA Vaccine. Front. Immunol. 2021, 12. [CrossRef]
- Henig, I.; Isenberg, J.; Yehudai-Ofir, D.; Leiba, R.; Ringelstein-Harlev, S.; Ram, R.; Avni, B.; Amit, O.; Grisariu, S.; Azoulay,T.; Slouzkey, I.; Zuckerman, T. Third BNT162b2 mRNA SARS-CoV-2 Vaccine Dose Significantly Enhances Immunogenicity in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation. Vaccines (Basel). 2023, 11(4), 775. [CrossRef]
- Watanabe, M.; Yakushijin, K.; Funakoshi, Y.; Ohji,G.; Ichikawa, H.; Sakai, H.; et al.. A Third Dose COVID-19 Vaccination in Allogeneic Hematopoietic Stem Cell Transplantation Patients. Vaccines (Basel). 2022, 10(11),1830. [CrossRef]
- Steensels, D.; Pierlet N.; Penders, J.; et al. Comparison of SARS-CoV-2 Antibody Response Following Vaccination With BNT162b2 and mRNA-1273. JAMA 2021, 326(15); 1533-1535. [CrossRef]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky K.E.; Ferolito B.R.; Figueroa Muñiz M.J.; et al. Comparative Effective ness of BNT162b2 and mRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2022, 386, 105–115. [CrossRef]
- Moderna’s COVID-19 Vaccine May Be More Effective for Cancer Patients - Cancer Therapy Advisor (Accessed 9 June 2023).
- Becker, M.; Cossmann, A.; Lürken, K.; Junker, D.; Gruber, J.; Juengling, J.; et al.. Longitudinal cellular and humoral immune responses after triple BNT162b2 and fourth full-dose mRNA-1273 vaccination in haemodialysis patients. Front Immunol. 2022, 13,1004045. [CrossRef]
- Alexopoulos, H.; Trougakos,I.P.; Dimopoulos, M.A.; Terpos, E. Clinical usefulness of testing for severe acute respiratory syndrome coronavirus 2 antibodies. Eur. J. Intern Med. 2023, 107, 7–16. [CrossRef]
- Terpos, E.; Liontos, M.; Fiste, O.; Zagouri, F.; Briasoulis, A.; Sklirou, A.D.; Markellos, C.; Skafida, E.; Papatheodoridi, A.; Andrikopoulou, A.; Koutsoukos, K.; Kaparelou, M.; Iconomidou, V.A.; Trougakos, I.P.; Dimopoulos, M.A. SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition. Cancers (Basel). 2022, 14(11), 2796. [CrossRef]
- Bergamaschi, C.; Pagoni, M.; Rosati, M.; Angel, M.; Tzannou, I.; Vlachou, M.; Darmani, I.; Ullah, A.; Bear, J.; Devasundaram, S.; Burns, R.; Baltadakis, I.; Gigantes, S.; Dimopoulos, M.A.; Pavlakis, G.N.; Terpos, E.; Felber, BK. Reduced Antibodies and Innate Cytokine Changes in SARS-CoV-2 BNT162b2 mRNA Vaccinated Transplant Patients With Hematological Malignancies. Front. Immunol. 2022,13,899972. [CrossRef]
- Rosati, M.; Terpos, E.; Bear, J.; Burns, R.; Devasundaram, S.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Kastritis, E.; Dimopoulos, M.-A.; Pavlakis, G.N.; et al. Low Spike Antibody Levels and Impaired BA.4/5 Neutralization in Patients with Multiple Myeloma or Waldenstrom’s Macroglobulinemia after BNT162b2 Booster Vaccination. Cancers 2022, 14, 5816. [CrossRef]
- Liatsou, E.; Ntanasis-Stathopoulos, I.; Lykos, S.; Ntanasis-Stathopoulos, A.; Gavriatopoulou, M.; Psaltopoulou, T.; Sergentanis, T.N.; Terpos, E. Adult Patients with Cancer Have Impaired Humoral Responses to Complete and Booster COVID-19 Vaccination, Especially Those with Hematologic Cancer on Active Treatment: A Systematic Review and Meta-Analysis. Cancers (Basel). 2023, 15(8), 2266. [CrossRef]
- Zagouri, F.; Papatheodoridi, A.; Liontos, M.; Briasoulis, A.; Sklirou, A.D.; Skafida, E.; Fiste, O.; Markellos, C.; Andrikopoulou, A.; Koutsoukos, K.; Kaparelou, M.; Gkogkou, E.; Trougakos, I.P.; Dimopoulos, M.A.; Terpos, E. Assessment of Postvaccination Neutralizing Antibodies Response against SARS-CoV-2 in Cancer Patients under Treatment with Targeted Agents. Vaccines (Basel). 2022;10(9):1474. [CrossRef]
Figure 1.
(a). Box plots of the distribution of anti-SARS-CoV-2 antibody levels (AU/mL), showing IgG a titer following two, three and four BNT162b2 vaccine doses in cancer patients actively receiving chemotherapy or non-chemotherapy treatment. The median and quartiles are presented as horizontal lines within the box plot. After two vaccine doses, the lower IgG values are more frequent in the chemotherapy-treated group. The data points outside the boxes represent outliers. (b). Vaccine Response: Percent of seropositive cancer patients actively treated with chemotherapy or non-chemotherapy drugs, following two, three and four BNT162b2 vaccine doses.
Figure 1.
(a). Box plots of the distribution of anti-SARS-CoV-2 antibody levels (AU/mL), showing IgG a titer following two, three and four BNT162b2 vaccine doses in cancer patients actively receiving chemotherapy or non-chemotherapy treatment. The median and quartiles are presented as horizontal lines within the box plot. After two vaccine doses, the lower IgG values are more frequent in the chemotherapy-treated group. The data points outside the boxes represent outliers. (b). Vaccine Response: Percent of seropositive cancer patients actively treated with chemotherapy or non-chemotherapy drugs, following two, three and four BNT162b2 vaccine doses.

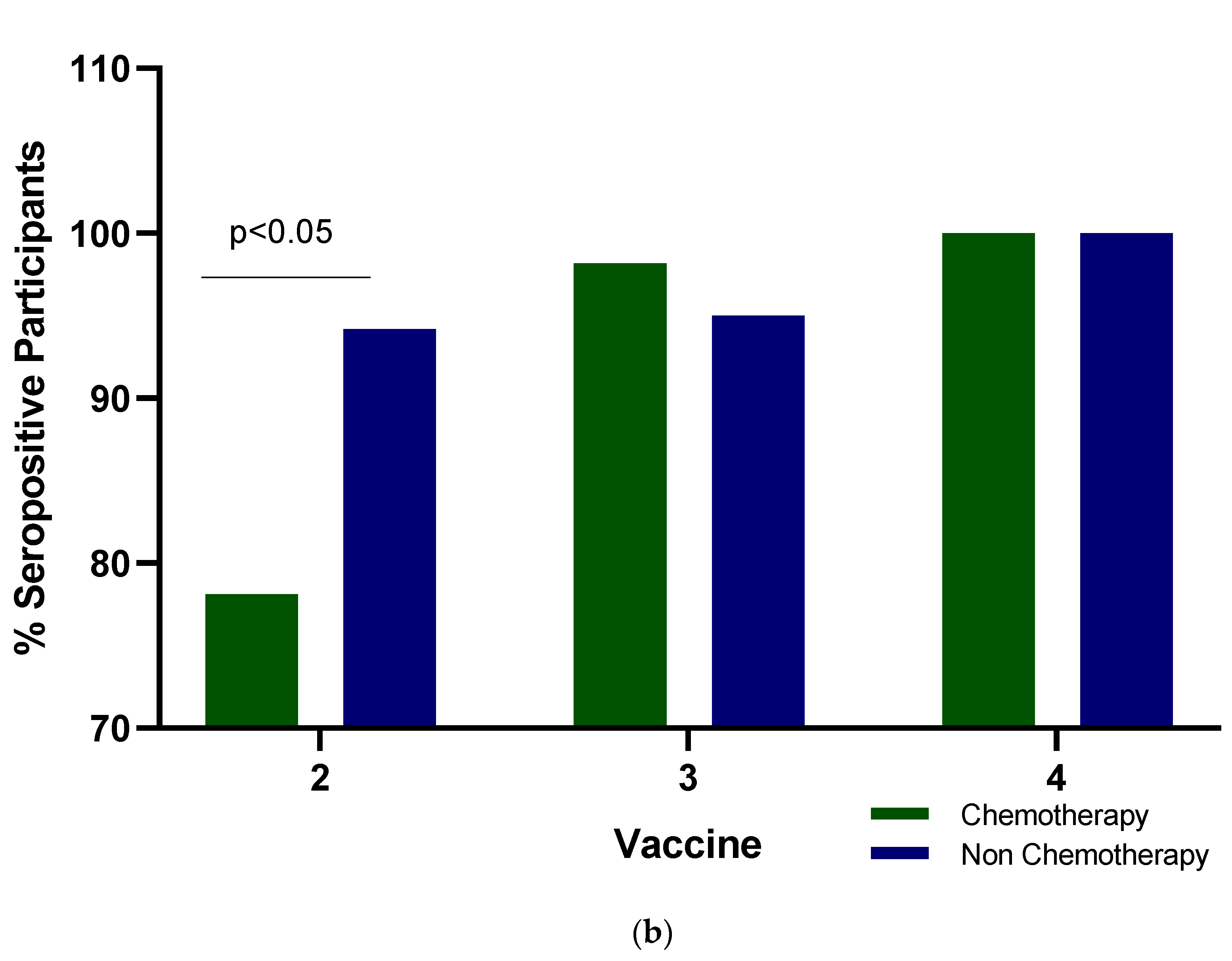
Figure 2.
Forest plot of odds ratios. Abbreviations: OR, odds ratio; CI, confidence interval.
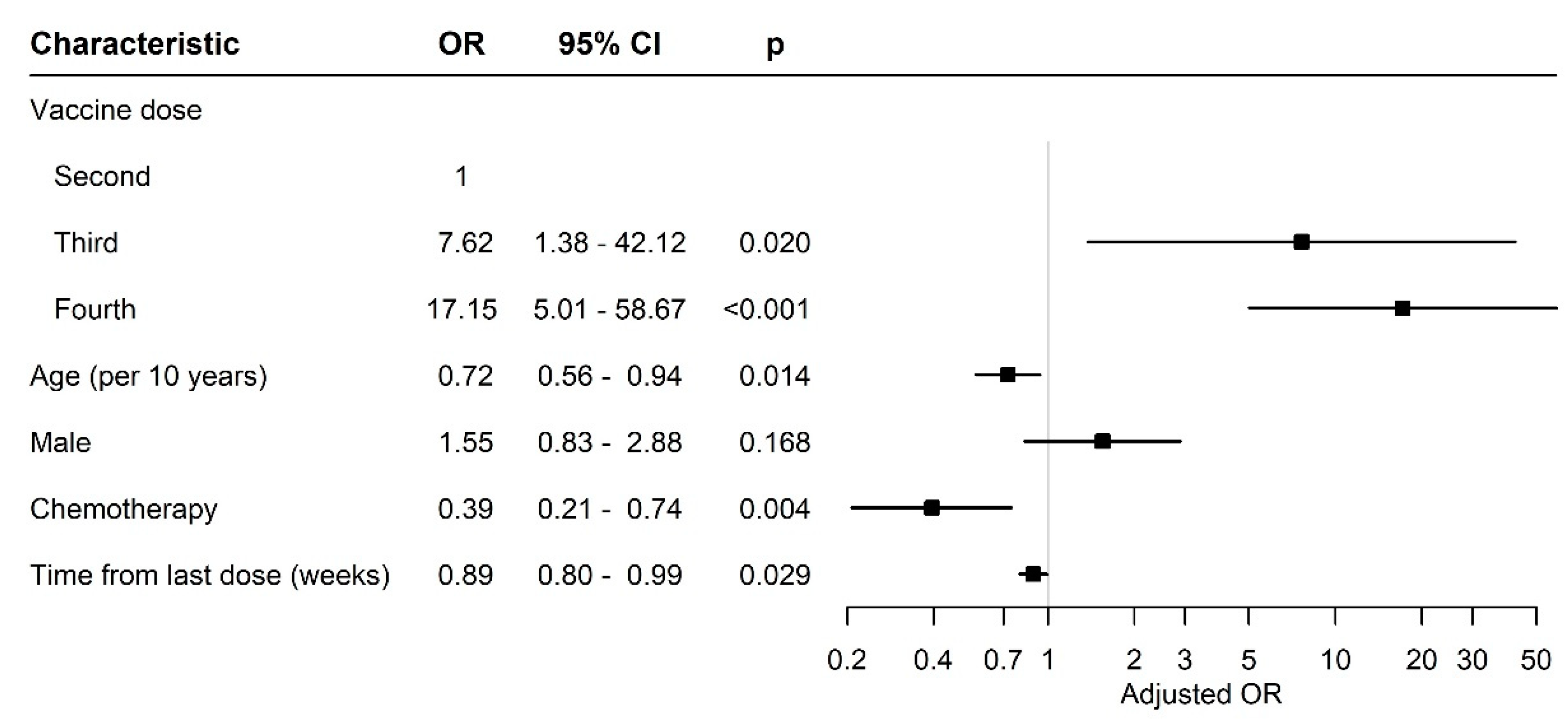
Table 2.
Antibody response rate and titers after a second, third and fourth dose of the BNT162b2 mRNA vaccine in cancer patients.
Table 2.
Antibody response rate and titers after a second, third and fourth dose of the BNT162b2 mRNA vaccine in cancer patients.
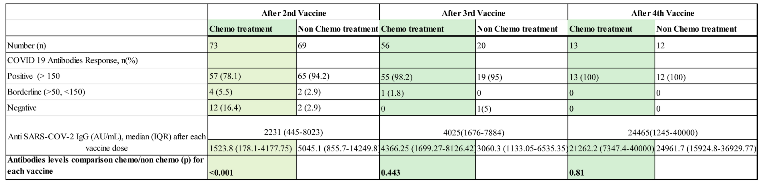 |
1 Chemo denotes chemotherapy treatment. 2 Non-Chemo denotes non-chemotherapy treatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



