Submitted:
22 August 2023
Posted:
23 August 2023
You are already at the latest version
Abstract
Abstract: Autism spectrum disorders (ASDs) are complex, lifelong, neurodevelopmental conditions of largely unknown cause. The global prevalence of autism has increased twentyfold to thirtyfold since the earliest epidemiologic studies were conducted in the late 1960s and early 1970s. Recent reports agree on the association of ASD with the alteration of the microbiome (dysbiosis), which raises the possible role of external factors. Our study aimed at identifying antibiotic classes that might be associated with the development of ASD-related dysbiosis either promoting or inhibiting the process. Statistical comparison was made between the average yearly consumption of different antibiotic classes (1997-2020) and the number of individuals living with ASD estimated for 2023/100000 population in 30 European countries and the results were statistically analyzed. Tetracycline (J01A) showed significant positive (promoting) association with the prevalence of ASD (Pearson r: 0.373, p: 0.043. OR: 1.312, CI95%: 0.995-1.791, p: 0.065) and narrow-spectrum, beta-lactamase resistant penicillin (J01CF) (Pearson r: 0.524, p: 0.003, OR: 3.240, CI95%: 1.710-8.853, p: 0.004, Kruskal-Wallis p: 0.032). Mild, negative (inhibitory) association was observed with broad-spectrum, beta-lactamase sensitive penicillin (J01CA) (Pearson r: -0.278, p: 0.157, OR: 0.808, CI95%: 0649-0957, p: 0.028) and narrow-spectrum, beta-lactamase-sensitive penicillin (J01CE) (Pearson p: -0.032, r: 0.865, OR: 0.725, CI95%: 0.543-0.885, p: 0,009). Our findings strongly support the animal experiments when penicillin-exposed newborn mice developed "autism-like" behavior.
Keywords:
Autism spectrum disorders (ASD)
; antibiotics
; penicillin
; tetracycline
; microbiome
; gut-brain axis (GBA)
1. Introduction
Autism spectrum disorder (ASD), which was first described by Karner (1942) is a neurodevelopmental disease, which is characterized by deficits in social communication and the presence of restricted interests and repetitive behaviors [1]. Its recent, pandemic-like spread is alarming and it became a public health issue. According to the Centers for Disease Control and Prevention (CDC) report in 2018, the ASD prevalence among children by 8 years has been estimated as 16.8/ 1000 (1:56) with more boys (26.6/ 1000 boys) than girls (6.6/ 1000 girls), which means a 150% increase from 2000 to 2014 [2]. The World’s prevalence of ASD has increased several folds since the first epidemiological observations in the past ~50 years and has reached the level of 1-2% of all children by 2000. The reasons for the increase could not be clearly stated, but researchers agree that better diagnostic criteria and some external factors might play a role [2].
People did not know much about autism before the excellent film of Rain man, but the pandemic of autism is rapidly spreading and by now, 1 in 56 children have a chance to develop autism and we are still not capable to show up any appropriate reason for this ailment, despite the fact, that several associations of different conditions were suspected as a causative agent [3,4]. Genetic mechanisms account for approximately 10–20% of ASD cases [5,6]. It was observed, that vancomycin treatment ameliorated the symptoms of ASD, suspecting the role of some clostridial bacteria [7,8,9]. The abundance of Clostridium bolte in autism prompted speculation about the use of developing a vaccine against this pathogen [10]. Desulfivibrio was suspected as an etiological agent in autism also [11]. Several publications support the role of intestinal bacteria [12,13]. The role of transvaginal ultrasonography [14], and conjugate vaccines [15] accumulation of insulin-like growth factors [16]. Other reasons leading to autism were also discussed in the literature [17]. A few of the latest proposal includes the role of electromagnetic frequency and radiofrequency radiation exposures (EMF/RFR) [18]. Tylenol/Augmentin and pesticide combined are suspected also [19]. Moreover, new evidence suggests that the peripheral immune system plays an important role in normal neuronal function [20,21,22].
ASD comprises a group of developmental disorders, starting in early childhood and characterized by pervasive behavioral deficits and social interaction [23]. The International Classification of Diseases and the Diagnostic Statistical Manual that the ASD group includes childhood autism, atypical autism, Asperger’s syndrome, disintegrative disorders, and Rett syndrome. ASD is considered genetically and phenotypically as a heterogenous group of symptoms with various severity, symptomatology, and outcome [24]. All manifestations are considered serious, devastating manifestations regarding the outcome, and co-morbidity, which bears down the affected families, society, and the health care systems alike. The overlap between autism and childhood obesity indicates that autistic patients are obese as well. Recent publications in increasing numbers indicate the role of microbiome alteration (dysbiosis) in autism. Experiments proved that fecal samples from autistic children when injected into germ-free mice, produce similar symptoms [25,26].
In ASD cases the balance between the pro-inflammatory bacteria (clostridia and desulfivibrio) and the anti-inflammatory bacteria (bifidobacteria) destabilized even before the symptoms of ASD occurred. This imbalance results in the so-called “leaky gut” syndrome and through the more porous epithelial membrane, toxins, produced by the microbes, are easily can enter the circulation, which may affect the brain and the development of ASD [27,28]. The alteration of the intestinal microbial taxa in ASD cases is repeatedly reported as the reduction of Firmicutes and an increase in the number of Bacteroidetes [29].
Other investigators observed the relative abundance of other bacteria, like Clostridia, Caloramator, Alistipes, Sarcina, Akkermansia, Lactobacillus, Enterobacteriaceae, and Sutterellaceae [30,31,32,33,34], and the reduction in the abundance of Bifidobacteria, Desulfovibrio, Coprococcus, Veillonellaceae and Prevotellaare species [8]. The pathogenetic process of ASD might be associated with the overgrowth or the reduction of different species, like Clostridium, which develops particularly with the use of antibiotics [11,35,36,37,38,39].
The presence of an altered microbiome (dysbiosis) in ASD is well documented and its possible role in the development of ASD has been reported also (see above references). It was hypothesized that antibiotic exposure to the microbiome might produce “ASD-promoting” dysbiosis in the mother, or the early modification of the gut microbiome in infancy might facilitate the development of ASD through the action of different mediator molecules involving the gut-brain axis (GBA) [40].
In mice, in utero exposure to the anticonvulsant valproic acid (VPA), leads to developmental and behavioral deficits in offspring that are similar to ASD [41].
Recent studies indicated two specific microbiota-derived host metabolites, p-cresol sulfate, and 4-ethyl phenyl sulfate, have been associated with ASD in both patients and animal models. These metabolites originate from bacterially produced p-cresol and 4-ethylphenol, respectively, which are produced through aromatic amino acid fermentation by a range of commensal bacteria, most notable bacteria from the Clostridioides genus, which are among the dysregulated bacteria frequently detected in ASD patients [42].
Epidemiological studies have revealed that early-life antibiotic exposure can increase the risk of neurodevelopmental disorders later in life [43,44].
Hypothesis
It is of consideration that different classes of antibiotics might induce different dysbiosis; hence, different molecular products of the altered microbiome leaking in the circulation might augment or inhibit the development of ASD. We have aimed to identify antibiotic classes, which might promote or inhibit the development of ASD-related dysbiosis and hence the prevalence of ASD.
2. Materials and methods
To evaluate the above hypothesis, antibiotic consumption databases were compared to the autism (ASD) prevalence in countries of people living with autism/ 100000 population in 30 European countries estimated for 2023 (https://wisevoter.com/country-rankings/autism-rates-by-country/).
Average, yearly antibiotic consumption had been calculated from the publicly available antibiotic databases of 30 European countries (ECDC yearly reports) for 1997-2020 https://www.ecdc.europa.eu/en/antimicrobial-consumption/database/quality-indicators. Based on the Anatomical Therapeutic Chemical classification system (ATC), the average yearly consumption of the total systemic antibiotics (J01) has been calculated and expressed in Defined Daily Dose/1000 Inhabitants/ Day (DID). The consumption of major antibiotic classes covering the 94% antibiotic use in the community at ATC levels two and three were calculated as a relative share of the total amount of systemic antibiotics (J01) and expressed in percentage (%). Antibiotic classes included: tetracycline (J01A), penicillin (J01C), broad-spectrum, beta-lactamase sensitive penicillin (J01CA), narrow spectrum, beta-lactamase sensitive penicillin (J01CE), narrow spectrum, beta-lactamase resistant penicillin (J01CF), broad-spectrum, beta-lactamase resistant combination penicillin (J01CR), cephalosporin (J01D), macrolide and lincosamides, streptogramins (J01F), and quinolone (J01M) expressed in percentage of the total amount.
Statistics
Pearson calculation was applied to estimate the correlation between antibiotic consumption and the prevalence of ASD. A significant correlation (positive/negative) was considered when p values were ≤ 0.05. A non-significant correlation was estimated when the p values fall between 0.051-0.09. Positive (supportive) and negative (inhibitor) significant correlations were considered and evaluated. Logistic regression analysis was performed to determine the odds ratio (OR, CI 95%) for each antibiotic class. A significant result was estimated when p values were equal to or less than 0.05 (≤ 0.05). A non-significant positive/negative) correlation has been considered when the p-value falls between 0.05 and 0.09 (p: 0.05 ≤ 0.09). The Kruskal–Wallis test was performed to determine statistically significant differences among the groups formed by country ranking. A significant difference was considered when p values were equal to or less than 0.05 (≤ 0.05), and a nonsignificant difference was considered when p values were between 0.051–0.09. Statistical results were recorded and featured in Table 1. Scatter diagrams were plotted to demonstrate the association (positive/negative) between the prevalence of autism and the average consumption of narrow spectrum, beta-lactamase resistant penicillin (J01CF) and tetracycline (J01A), (Figure 1 and Figure 2).
3. Results
Tetracycline (J01A) consumption showed a significant positive (promoting) association with the prevalence of ASD (Pearson r: 0.373, p: 0.043. OR: 1.312, CI95%: 0.995-1.791, p: 0.065) and narrow-spectrum, beta-lactamase resistant penicillin (J01CF) (Pearson r: 0.524, p: 0.003, OR: 3.240, CI95%: 1.710-8.853, p: 0.004, Kruskal-Wallis p: 0.032). Mild, negative (inhibitory) association was observed with broad-spectrum, beta-lactamase sensitive penicillin (J01CA) (Pearson r: -0.278, p: 0.157, OR: 0.808, CI95%: 0649-0957, p: 0.028) and narrow-spectrum, beta-lactamase-sensitive penicillin (J01CE) (Pearson p: -0.032, r: 0.865, OR: 0.725, CI95%: 0.543-0.885, p: 0,009).
4. Discussion
Early life is a critical period for neurodevelopment. In recent decades, there has been a rise in the incidence of childhood neurodevelopmental disorders including ASD, attention-deficit/hyperactivity disorder (ADHD), and learning disabilities worldwide. It has been observed that the incidence of ASD increased significantly over time, especially among toddlers and preschool children but also in older age groups [45]. Recent publications (cited above) agree on the principal role of certain gut bacteria in the development of autism, particularly of clostridia species. This theory was supported by the fact that vancomycin ameliorated the symptoms of autism, but it returned after the cessation of antibiotic treatment, probably indicating that after temporally suppressing the clostridial species, the appropriate balance of the gut flora was not restored [46]. Similarly, the fecal microbiome transfer has greatly ameliorated the symptoms of ASD [47,48,49]. The initial development and maturation of the neonatal microbiome are largely determined by maternal–offspring exchanges of microbiota, which indicates that dysbiotic maternal microbiome might populate the newborn intestine also [50].
The importance of biochemical changes observed early in the newborn, such as the depressed level of insulin-like growth factor-1 (IGF-1) in the process of the neurodevelopmental period, are considered important by several researchers in the development of ASD. This observation leads to early diagnosis and probable intervention in the prevention of developing dysconnectivity. According to Steinmann [51], the process of developing ASD could be preventable even before irreversible psychosocial changes develop.
It might be concluded that biochemical changes observed in ASD, are probably triggered by the altered microbiome induced by antibiotics. Reports on the association between autism and antibiotics are controversial. Some observations indicate a certain association between prenatal exposure to antibiotics and autism [52], while others found some beneficial effects of perinatal antibiotic use [53]. Controversy might arise from the fact that different antibiotic classes induce different dysbiosis, which either promotes or inhibits the development of ASD-related dysbiosis.
In animal experiments, when newborn mice were exposed to low-dose penicillin, profound changes in the intestinal microbiota were observed, which might be implicated in the perturbance of neurodevelopmental and neuropsychiatric pathways. Significant effects were observed on different areas of the brain (frontal cortex, amygdala gene, etc.). Linkage was observed between the specific microbial taxa and the early-life expression of particularly affected genes [54].
The results derived from animal models [55] strongly support our observations as we have detected the possible association between the consumption of the narrow-spectrum, beta-lactamase-resistant penicillin (J01CF) and the prevalence of autism, which might induce developmental difficulties in the brain, resulting in ASD. Group B Streptococcus (GBS) remains the most common cause of neonatal early-onset sepsis among term infants and a major cause of late-onset sepsis among both term and preterm infants and penicillin is frequently used for prophylaxis [56].
Our comparative analyses indicated a significant, positive correlation between the consumption of tetracycline/penicillin and the prevalence of ASD. It was observed that the highest rate of ASD and the highest tetracycline (J01A) consumption together with the second highest consumption of narrow-spectrum, beta-lactamase resistant penicillin (J01CF) is reported from the UK. Similarly, Sweden records the highest consumption of narrow-spectrum, beta-lactamase-resistant penicillin (J01CF) and fifth place on the tetracycline consumption rank order and second place on the ASD prevalence list. (Table 1). As far as pregnant women, newborn babies, and infants are not taking any tetracycline compound because it is contraindicated, it could be suspected, that tetracycline might arrive from environmental antibiotic pollution, or the women were exposed to tetracycline before being pregnant, which triggered the ASD-related dysbiosis. As a medication, more than 70 % of tetracycline antibiotics are excreted and released in active form into the environment via urine and feces from humans and animals. Tetracycline has become a serious threat to the environment because of its overuse by humans and veterinarians and its weak ability to degrade. Tetracycline is capable of accumulating along the food chain and influencing microbial communities [57]. It might be concluded that higher consumption could result in higher environmental pollution also.
Clinical and experimental data indicate that the risk of developing ASD is associated with the presence of inflammatory changes during pregnancy and the modification of the microbiome that defined gut commensal bacteria with a propensity to induce Th17 cells may increase the risk for neurodevelopmental disorders in the offspring of pregnant mothers undergoing immune system activation due to infections or auto-inflammatory syndromes [58,59,60,61,62].
Animal models (mice) indicated that applying a low dose of Penicillin V induced a more robust behavioral abnormalities response than the cocktail of broad-spectrum antibiotics [63].
The above findings strongly support our observations regarding the possible role of narrow-spectrum penicillin (J01CF) as a possible putative factor in the development of ASD.
4.1. Limitations of our study
Our results could not be interpreted at the individual level, only statistical correlations and concordance could be established, but a firm, statistical correlation between tetracycline and penicillin consumption and ASD was estimated. This might indicate a possible association between maternal consumption of tetracycline/penicillin (dysbiosis) and autism, shown in the scatter diagrams also.
4.2. Strength of our study
The results of our comparative analysis is in full accord with previous animal experiments indicating the role of even low-dose penicillin applied intrauterine, or newborn mice, in the development of autism-like behavior.
Author Contributions
GT: Writing - original draft, conceptualization, MN: Resources, GM: Formal analysis, and LB: Supervision, Funding: This research received no external funding, Institutional Review Board Statement: Not applicable for studies not involving humans or animals, Informed Consent Statement: Not applicable, Data Availability Statement: Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ziats CA, Patterson WG, Friez M. Syndromic Autism Revisited: Review of the Literature and Lessons Learned. Pediatr Neurol. 2021, 114:21-25. [CrossRef]
- Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z,. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveill Summ. 2018, 67:1-23. [CrossRef]
- Rapin I, Tuchman RF. Autism: definition, neurobiology, screening, diagnosis. Pediatr Clin North Am. 2008, 55:1129-46, . [CrossRef]
- Kočovská E, Fernell E, Billstedt E, Minnis H, Gillberg C. Vitamin D and autism: clinical review. Res Dev Disabil. 2012, 33:1541-50. [CrossRef]
- Rylaarsdam L, Guemez-Gamboa A. Genetic Causes and Modifiers of Autism Spectrum Disorder. Front Cell Neurosci. 2019, 20;13:385. [CrossRef]
- Abrahams BS, Geschwind DH. Advances in autism genetics: on the threshold of a new neurobiology. Nat Rev Genet. 2008, 9:341-55. [CrossRef]
- Finegold SM, Downes J, Summanen PH. Microbiology of regressive autism. Anaerobe.2012, 18:260-2. [CrossRef]
- Finegold SM. (2011) State of the art; microbiology in health and disease. Intestinal bacterial flora in autism. Anaerobe. 2011, 17:367-8. [CrossRef]
- Finegold SM. Therapy and epidemiology of autism--clostridial spores as key elements. Med Hypotheses, 2008, 70:508-11. [CrossRef]
- Pequegnat B, Sagermann M, Valliani M, Toh M, Chow H, Allen-Vercoe E, et al. A vaccine and diagnostic target for Clostridium bolteae, an autism-associated bacterium. Vaccine. 2013, 31:2787-90. [CrossRef]
- Finegold SM. Desulfovibrio species are potentially important in regressive autism. Med Hypotheses, 2011, 77:270-4. [CrossRef]
- Heberling CA, Dhurjati PS, Sasser M. Hypothesis for a systems connectivity model of Autism Spectrum Disorder pathogenesis: links to gut bacteria, oxidative stress, and intestinal permeability. Med Hypotheses. 2013 80:264-70. doi:10.1016/j.mehy.2012.11.044.
- Zafeiriou DI, Ververi A, Vargiami E. Childhood autism and associated comorbidities. Brain Dev. 2007, 29:257-72. [CrossRef]
- Webb SJ, Mourad PD. Prenatal Ultrasonography and the Incidence of Autism Spectrum Disorder. JAMA Pediatr. 2018, 172:319-320. [CrossRef]
- Richmond BJ. Hypothesis: conjugate vaccines may predispose children to autism spectrum disorders. Med Hypotheses. 2011, 77:940-7. [CrossRef]
- Steinman G, Mankuta D. Insulin-like growth factor and the etiology of autism. Med Hypotheses. 2013, 80:475-80. [CrossRef]
- Odent M. (2010) Autism and anorexia nervosa: Two facets of the same disease? Med Hypotheses. 75(1):79-81. [CrossRef]
- Herbert MR, Sage C. Autism and EMF? Plausibility of a pathophysiological link part II. Pathophysiology. 2013, 20:211-34. [CrossRef]
- Good P. Evidence the U.S. autism epidemic initiated by acetaminophen (Tylenol) is aggravated by oral antibiotic amoxicillin/clavulanate (Augmentin) and now exponentially by herbicide glyphosate (Roundup). Clin Nutr ESPEN. 2018, 23:171-183. [CrossRef]
- Marchezan J. Editorial: Autism Spectrum Disorder and Autoimmune Diseases: A Pathway in Common? J Am Acad Child Adolesc Psychiatry. 2019, 58:481-483. [CrossRef]
- Gottfried C, Bambini-Junior V, Francis F, Riesgo R, Savino W. The Impact of Neuroimmune Alterations in Autism Spectrum Disorder. Front Psychiatry, 2015, 6:121. [CrossRef]
- Mead J, Ashwood P. Evidence supporting an altered immune response in ASD. Immunol Lett. 2015, 163:49-55. [CrossRef]
- Wing L. The autistic spectrum. Lancet. 1997, 350:1761-6. [CrossRef]
- Caronna EB, Milunsky JM, Tager-Flusberg H. Autism spectrum disorders: clinical and research frontiers. Arch Dis Child. 2008, 93:518-23. [CrossRef]
- Phillips KL, Schieve LA, Visser S, Boulet S, Sharma AJ, Kogan MD, et al Prevalence and impact of unhealthy weight in a national sample of US adolescents with autism and other learning and behavioral disabilities. Matern Child Health J. 2014, 18:1964-75. [CrossRef]
- Sharon G, Cruz NJ, Kang DW, Gandal MJ, Wang B, Kim YM, et al Human Gut Microbiota from Autism Spectrum Disorder Promote Behavioral Symptoms in Mice. Cell. 2019, 30:1600-1618.e17. [CrossRef]
- Nagaraju K, Sudeep KS, Kurhekar MP. A cellular automaton model to find the risk of developing autism through gut-mediated effects. Comput Biol Med. 2019, 110:207-217. [CrossRef]
- Weston B, Fogal B, Cook D, Dhurjati P. An agent-based modeling framework for evaluating hypotheses on risks for developing autism: effects of the gut microbial environment. Med Hypotheses. 2015, 84:395-401. [CrossRef]
- Finegold SM, Dowd SE, Gontcharova V, Liu C, Henley KE, Wolcott RD, et al 3rd. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe. 2010, 16:444-53. [CrossRef]
- De Angelis M, Piccolo M, Vannini L, Siragusa S, De Giacomo A, Serrazzanetti DI, et al Fecal microbiota and metabolome of children with autism and pervasive developmental disorder not otherwise specified. PLoS One. 2013, 8:e76993. [CrossRef]
- Finegold SM, Molitoris D, Song Y, Liu C, Vaisanen ML, Bolte E, et al Gastrointestinal microflora studies in late-onset autism. Clin Infect Dis. 2002, 35(Suppl 1):S6-S16. [CrossRef]
- Wang L, Christophersen CT, Sorich MJ, Gerber JP, Angley MT, Conlon MA. Elevated fecal short chain fatty acid and ammonia concentrations in children with autism spectrum disorder. Dig Dis Sci. 2012, 57:2096-102. [CrossRef]
- Parracho HM, Bingham MO, Gibson GR, McCartney AL. Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children. J Med Microbiol. 2005, 54:987-991. [CrossRef]
- Andreo-Martínez P, García-Martínez N, Sánchez-Samper EP, Martínez-González AE. An approach to gut microbiota profile in children with autism spectrum disorder. Environ Microbiol Rep. 2020, 12:115-135. [CrossRef]
- S.M. Bolte ER. Autism and Clostridium tetani. Med Hypotheses. 1998, 51:133-44. [CrossRef]
- Tomova A, Husarova V, Lakatosova S, Bakos J, Vlkova B, Babinska K, et al Gastrointestinal microbiota in children with autism in Slovakia. Physiol Behav. 2015, 138:179-87. [CrossRef]
- De Angelis M, Francavilla R, Piccolo M, De Giacomo A, Gobbetti M. Autism spectrum disorders and intestinal microbiota. Gut Microbes. 2015, 6:207-13. [CrossRef]
- Persico AM, Napolioni V. Urinary p-cresol in autism spectrum disorder. Neurotoxicol Teratol. 2013, 36:82-90. [CrossRef]
- Macfabe DF. Short-chain fatty acid fermentation products of the gut microbiome: implications in autism spectrum disorders. Microb Ecol Health Dis. 2012, 24;23. [CrossRef]
- Cryan JF, O’Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, et al The Microbiota-Gut-Brain Axis. Physiol Rev. 2019, 99:1877-2013. [CrossRef]
- Roullet FI, Wollaston L, Decatanzaro D, Foster JA. Behavioral and molecular changes in the mouse in response to prenatal exposure to the anti-epileptic drug valproic acid. Neuroscience. 2010, 170:514-22. [CrossRef]
- Zheng Y, Bek MK, Prince NZ, Peralta Marzal LN, Garssen J, Perez Pardo P, Kraneveld AD. The Role of Bacterial-Derived Aromatic Amino Acids Metabolites Relevant in Autism Spectrum Disorders: A Comprehensive Review. Front Neurosci. 2021, 15:738220. [CrossRef]
- Atladóttir HÓ, Henriksen TB, Schendel DE, Parner ET. Autism after infection, febrile episodes, and antibiotic use during pregnancy: an exploratory study. Pediatrics. 2012 130(6):e1447-54. [CrossRef]
- Niehus, R., and Lord, C. Early medical history of children with autism spectrum disorders. J. Dev. Behav. Pediatr. 2006, 2(Suppl.), S120–S127. [CrossRef]
- Davidovitch M, Slobodin O, Weisskopf MG, Rotem RS. Age-Specific Time Trends in Incidence Rates of Autism Spectrum Disorder Following Adaptation of DSM-5 and Other ASD-Related Regulatory Changes in Israel. Autism Res. 2020, 13:1893-1901. [CrossRef]
- Sandler RH, Finegold SM, Bolte ER, Buchanan CP, Maxwell AP, Väisänen ML, et al Short-term benefit from oral vancomycin treatment of regressive-onset autism. J Child Neurol. 2000, 15:429-35. [CrossRef]
- Żebrowska P, Łaczmańska I, Łaczmański Ł. Future Directions in Reducing Gastrointestinal Disorders in Children With ASD Using Fecal Microbiota Transplantation. Front Cell Infect Microbiol. 2021, 11:630052. [CrossRef]
- Abuaish S, Al-Otaibi NM, Aabed K, Abujamel TS, Alzahrani SA, Alotaibi SM, et al The Efficacy of Fecal Transplantation and Bifidobacterium Supplementation in Ameliorating Propionic Acid-Induced Behavioral and Biochemical Autistic Features in Juvenile Male Rats. J Mol Neurosci. 2022, 72:372-381. [CrossRef]
- Johnson D, Letchumanan V, Thurairajasingam S, Lee LH. A Revolutionizing Approach to Autism Spectrum Disorder Using the Microbiome. Nutrients. 2020, 12:1983. [CrossRef]
- Mueller NT, Bakacs E, Combellick J, Grigoryan Z, Dominguez-Bello MG. The infant microbiome development: mom matters. Trends Mol Med. 2015, 21:109-17. [CrossRef]
- Steinman G. The putative etiology and prevention of autism. Prog Mol Biol Transl Sci. 2020, 173:1-34. [CrossRef]
- Hamad AF, Alessi-Severini S, Mahmud SM, Brownell M, Kuo IF. Prenatal antibiotics exposure and the risk of autism spectrum disorders: A population-based cohort study. PLoS One. 2019, 14:e0221921. [CrossRef]
- Abelson N, Meiri G, Solomon S, Flusser H, Michaelovski A, Dinstein I, et al Association Between Antenatal Antimicrobial Therapy and Autism Spectrum Disorder-A Nested Case-Control Study. Front Psychiatry. 2021, 12:771232. PMID: 34867555. [CrossRef]
- Volkova A, Ruggles K, Schulfer A, Gao Z, Ginsberg SD, Blaser MJ. Effects of early-life penicillin exposure on the gut microbiome and frontal cortex and amygdala gene expression. Science, 2021, 24:102797. [CrossRef]
- Leclercq S, Mian FM, Stanisz AM, Bindels LB, Cambier E, Ben-Amram H, et al. Low-dose penicillin in early life induces long-term changes in murine gut microbiota, brain cytokines and behavior. Nat Commun. 2017, 8:15062. [CrossRef]
- Dhudasia MB, Flannery DD, Pfeifer MR, Puopolo KM. (2021) Updated Guidance: Prevention and Management of Perinatal Group B Streptococcus Infection. Neoreviews. 2021, (3):e177-e188. [CrossRef]
- Amangelsin Y, Semenova Y, Dadar M, Aljofan M, Bjørklund G. The Impact of Tetracycline Pollution on the Aquatic Environment and Removal Strategies. Antibiotics (Basel). 2023, 12:440. PMID: 36978308; PMCID: PMC10044355. [CrossRef]
- Lee BK, Magnusson C, Gardner RM, Blomström Å, Newschaffer CJ, Burstyn I, et al Maternal hospitalization with infection during pregnancy and risk of autism spectrum disorders. Brain Behav Immun. 2015, 44:100-5. [CrossRef]
- Brown AS, Sourander A, Hinkka-Yli-Salomäki S, McKeague IW, Sundvall J, Surcel HM. Elevated maternal C-reactive protein and autism in a national birth cohort. Mol Psychiatry. 2014, 19:259-64. [CrossRef]
- Atladóttir HO, Thorsen P, Østergaard L, Schendel DE, Lemcke S, Abdallah M, et al Maternal infection requiring hospitalization during pregnancy and autism spectrum disorders. J Autism Dev Disord. 2010, 40:1423-30. [CrossRef]
- Choi GB, Yim YS, Wong H, Kim S, Kim H, Kim SV, et al. The maternal interleukin-17a pathway in mice promotes autism-like phenotypes in offspring. Science, 2016, 26;351(6276):933-9. [CrossRef]
- Kim S, Kim H, Yim YS, Ha S, Atarashi K, Tan TG, et al (2017) Maternal gut bacteria promote neurodevelopmental abnormalities in mouse offspring. Nature, 2017, 28;549(7673):528-532. [CrossRef]
- O’Connor R, Moloney GM, Fulling C, O’Riordan KJ, Fitzgerald P, Bastiaanssen TFS, et al. Maternal antibiotic administration during a critical developmental window has enduring neurobehavioural effects in offspring mice. Behav Brain Res. 2021, 404:113156. [CrossRef]
Figure 1.
Significant, positive association observed between ASD prevalence and the consumption of tetracycline.
Figure 1.
Significant, positive association observed between ASD prevalence and the consumption of tetracycline.
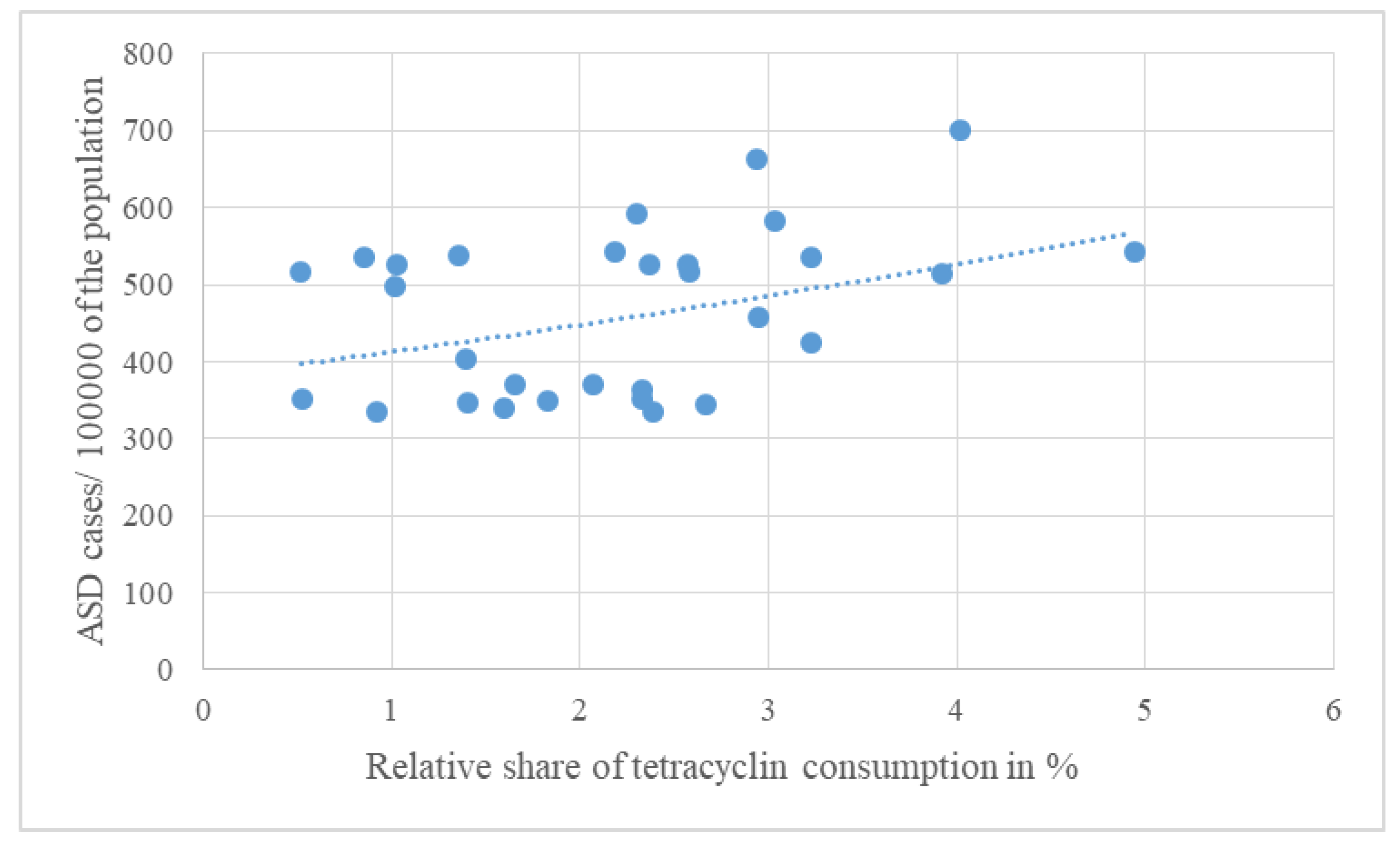
Figure 2.
Significant, positive association observed between ASD prevalence and the consumption of narrow-spectrum, beta-lactamase-resistant penicillin (j01CF).
Figure 2.
Significant, positive association observed between ASD prevalence and the consumption of narrow-spectrum, beta-lactamase-resistant penicillin (j01CF).
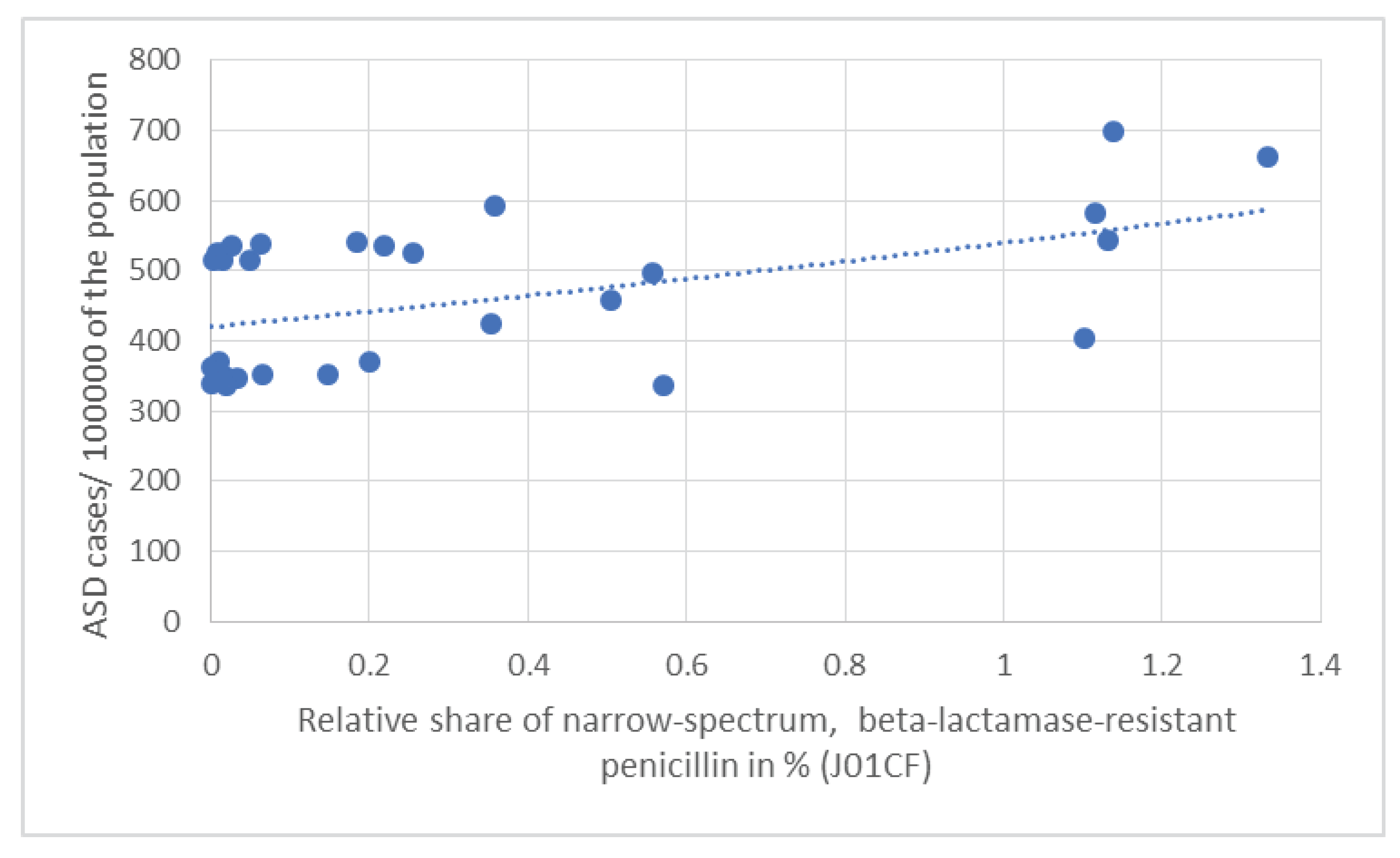

Table 1.
Average antibiotic consumption in 30 European countries between 1997-2020 expressed as the relative share (%) of the total consumption of systemic antibiotics in the community (expressed in DID) and the rank order of ASD prevalence/100000 inhabitants. Significant positive correlations marked with yellow filling color and the negative correlation marked with green filling color. Non-significant correlations marked with blue filling color.
Table 1.
Average antibiotic consumption in 30 European countries between 1997-2020 expressed as the relative share (%) of the total consumption of systemic antibiotics in the community (expressed in DID) and the rank order of ASD prevalence/100000 inhabitants. Significant positive correlations marked with yellow filling color and the negative correlation marked with green filling color. Non-significant correlations marked with blue filling color.
| Average antibiotic consumption 1997-2020 | J01 (DID) | J01A% | J01C% | J01CA% | J01CE% | J01CF% | J01CR% | J01D% | J01F% | J01M% | People living with ASD 2023/100000 population | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Countries | ||||||||||||
| UK | 15.294 | 26.259 | 38.257 | 21.296 | 4.878 | 7.447 | 4.799 | 3.570 | 17.177 | 3.492 | 700.070 | |
| Sweden | 13.370 | 21.960 | 47.771 | 7.831 | 28.579 | 9.970 | 1.361 | 2.094 | 5.460 | 6.171 | 661.850 | |
| Netherlands | 9.218 | 24.995 | 32.046 | 13.734 | 3.873 | 3.884 | 10.545 | 0.966 | 15.003 | 9.069 | 591.540 | |
| Ireland | 18.256 | 16.608 | 45.021 | 15.425 | 5.094 | 6.113 | 18.482 | 8.600 | 18.695 | 4.700 | 583.690 | |
| Iceland | 19.148 | 25.804 | 48.146 | 17.715 | 12.774 | 5.907 | 11.657 | 2.961 | 8.147 | 4.162 | 543.420 | |
| Luxembourg | 22.410 | 9.768 | 35.582 | 13.788 | 0.393 | 0.826 | 20.607 | 18.237 | 17.840 | 10.768 | 541.660 | |
| Malta | 18.465 | 7.344 | 33.929 | 2.908 | 0.498 | 0.336 | 30.176 | 21.847 | 20.422 | 11.373 | 537.950 | |
| Cyprus | 27.338 | 11.800 | 34.582 | 11.405 | 0.369 | 0.095 | 22.803 | 21.666 | 11.435 | 16.911 | 535.350 | |
| Spain | 17.697 | 4.826 | 51.794 | 20.405 | 0.571 | 1.232 | 29.011 | 11.804 | 14.341 | 13.330 | 535.140 | |
| Belgium | 21.427 | 11.051 | 40.720 | 17.716 | 0.425 | 1.195 | 21.366 | 11.140 | 14.958 | 10.295 | 526.130 | |
| Austria | 11.683 | 8.816 | 36.386 | 7.010 | 8.097 | 0.068 | 21.176 | 13.396 | 26.329 | 11.221 | 526.020 | |
| Germany | 12.610 | 20.412 | 27.113 | 16.122 | 8.438 | 0.111 | 2.395 | 15.131 | 18.184 | 9.556 | 525.310 | |
| Italy | 21.524 | 2.407 | 42.241 | 16.303 | 0.060 | 0.070 | 25.832 | 13.171 | 21.957 | 14.277 | 516.090 | |
| Greece | 30.474 | 8.470 | 28.152 | 13.415 | 1.447 | 0.013 | 13.185 | 23.571 | 26.337 | 8.814 | 515.700 | |
| Finland | 16.157 | 24.293 | 28.217 | 14.539 | 9.371 | 0.297 | 4.023 | 12.960 | 9.123 | 4.945 | 514.680 | |
| Portugal | 18.094 | 5.610 | 43.307 | 11.087 | 0.155 | 3.078 | 29.004 | 12.756 | 17.569 | 13.795 | 496.610 | |
| Norway | 15.046 | 19.567 | 40.635 | 12.754 | 24.465 | 3.356 | 0.060 | 0.957 | 10.415 | 3.110 | 457.900 | |
| France | 24.478 | 13.171 | 46.666 | 27.796 | 0.735 | 1.446 | 16.615 | 11.512 | 16.697 | 7.856 | 425.410 | |
| Denmark | 14.068 | 9.937 | 62.425 | 19.420 | 32.521 | 7.840 | 2.687 | 0.213 | 14.437 | 3.234 | 403.840 | |
| Estonia | 10.947 | 18.928 | 33.808 | 22.125 | 2.412 | 0.091 | 9.199 | 8.148 | 17.786 | 7.582 | 369.490 | |
| Lithuania | 16.714 | 9.908 | 52.315 | 30.531 | 13.312 | 1.191 | 7.341 | 7.784 | 10.452 | 5.881 | 369.320 | |
| Latvia | 10.653 | 21.862 | 37.924 | 25.505 | 0.901 | 0.019 | 11.508 | 5.107 | 13.470 | 9.218 | 362.530 | |
| Slovenia | 12.873 | 4.109 | 55.543 | 16.686 | 15.397 | 1.150 | 22.380 | 4.350 | 19.125 | 9.827 | 351.370 | |
| Czech Rep. | 14.685 | 15.887 | 37.719 | 9.227 | 12.782 | 0.443 | 15.131 | 10.555 | 20.620 | 7.014 | 350.850 | |
| Slovakia | 21.098 | 8.660 | 39.241 | 10.579 | 13.366 | 0.081 | 15.253 | 17.082 | 21.955 | 8.731 | 349.180 | |
| Croatia | 17.911 | 7.839 | 42.326 | 13.774 | 5.622 | 0.190 | 22.746 | 17.710 | 14.745 | 8.352 | 346.790 | |
| Poland | 18.773 | 14.228 | 32.952 | 19.459 | 2.243 | 0.117 | 11.144 | 12.332 | 17.823 | 6.797 | 345.130 | |
| Hungary | 14.711 | 10.842 | 35.817 | 9.972 | 4.310 | 0.000 | 21.508 | 14.696 | 20.760 | 12.528 | 340.310 | |
| Romania | 22.897 | 4.044 | 46.840 | 17.745 | 3.035 | 2.494 | 23.925 | 18.697 | 12.517 | 12.901 | 335.890 | |
| Bulgaria | 17.828 | 13.383 | 36.740 | 22.655 | 5.346 | 0.107 | 8.750 | 14.988 | 14.522 | 11.168 | 335.580 | |
| Pearson R | 0.039 | 0.373 | -0.146 | -0.278 | -0.032 | 0.524 | -0.078 | -0.157 | -0.121 | -0.089 | ||
| Pearson p | 0.839 | 0.043 | 0.442 | 0.137 | 0.865 | 0.003 | 0.682 | 0.408 | 0.523 | 0.640 | ||
| OR | 1.077 | 1.312 | 1.131 | 0.808 | 0.725 | 3.240 | 0.892 | 1.073 | 1.063 | 1.296 | ||
| CI95% | 0.922 - 1.259 | 0.995 - 1.791 | 0.934 - 1.395 | 0.649 - 0.957 | 0.543 - 0.885 | 1.710 - 8.852 | 0.747 - 1.029 | 0.859 - 1.354 | 0.868 - 1.308 | 0.954 - 1.811 | ||
| p | 0.348 | 0.065 | 0.221 | 0.028 | 0.009 | 0.004 | 0.154 | 0.534 | 0.554 | 0.107 | ||
| Kruskal-Wallis p | 0.679 | 0.342 | 0.606 | 0.668 | 0.278 | 0.032 | 0.481 | 0.733 | 0.447 | 0.903 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



