
Submitted:
09 August 2023
Posted:
10 August 2023
You are already at the latest version
Abstract
Background: Calcaneal fractures are the most frequent traumatic injuries of the hindfoot and can cause severe disability with social and economic sequelae; since 1980 an increasing number of studies and new technologies have led to an improvement in their management and complications but treatment is still controversial. The purpose of the study to review the secondary scientific literature looking for the optimal management of calcaneal fracture; Methods: through the PubMed MEDLINE database, 4856 articles were identified; only meta-analyses and systematic reviews were included in the study. Results: 59 reviews with more than 10,000 calcaneus fractures were examined and results were divided into various topics; the majority of articles agree on the superiority of surgical versus conservative treatment; minimally invasive access to the sinus tarsi shows better results and fewer complications than traditional extended lateral access; reduction and osteosynthesis with percutaneous and/or minimally invasive techniques seem to provide better outcomes if compared to open treatments. Conclusions: The management of calcaneus fractures requires an individualized planning based on the functional demands of the patient, the type of fracture and associated injuries. New technologies and further studies may still improve the management of these lesions.
Keywords:
calcaneus
; calcaneal fracture
; ORIF
; conservative
; operative
; extensile lateral approach (ELA)
; sinus tarsi approach (STA)
1. Introduction
Among the bones of the foot, the calcaneus is the largest, has an irregular shape and is essential in supporting weight especially in walking and running. Its inner part consists of cancellous bone with non-uniform density while the outer shell consists of thin cortical bone [1,2,3,4,5,6]. Calcaneus fractures usually develop with a traumatic mechanism in compression with forces that cause the collapse especially of the spongy bone [7,8]. In particular, falls from heights or high-energy road accidents, which cause a vertical impact on the heel, represent the most frequent injury mechanisms, and in 70-75% of cases they are intra-articular fractures [9].
Among the fractures of the hindfoot, the calcaneal ones are the most common, representing 61% of fractures of the tarsus and about 2.6% of total body fractures [3,10,11,12].
Temporary and permanent disability are inexorable consequences of calcaneal fractures with socio-economic and psychological repercussions. This is mainly due to the loss of the bone shape in height, width and incongruity of the articular surfaces, which evolves into calcaneal malunion and post-traumatic osteoarthritis, affecting standing, walking and jumping [6]. Sanders type II or III is the most common pattern of fractures involving the posterior subtalar facet; associated injuries are common such as ipsilateral fractures of the talus or fibula, lesionof the lateral ligament complex, dislocation of the fibula tendons, entrapment of the Flexor Hallucis Longus tendon, and other body fractures [13]. For a complete diagnosis, an MRI examination can therefore be useful [14].
Soft tissues conditions are also a problematic issue. The management and surgical strategy to face up the fractures of the calcaneus have been extensively discussed over the past years and the many papers show that this topic is still a challenge.
Therapeutical options include: conservative treatment, closed reduction and external fixation with Kirschner wires or external fixator, Closed Reduction and Internal Fixation with screws or nail, closed reduction with calcaneoplasty, Open Reduction and Internal Fixation (ORIF) with plate, Arthroscopic assisted Reduction and Internal Fixation (ARIF), Arthroscopic Reduction and External Fixation (AREF), subtalar arthrodesis, bone or derivates grafting.
To date the best calcaneal fracture management is still controversial. We aimed to review the secondary scientific literature looking for the optimal management of calcaneal fracture.
2. Materials and Methods
On November 18th, 2022, we performed a literature research in Pubmed/Medline typing the keywords: “calcane* AND fracture”; results were filtered only for metanalysis and systematic reviews without any language nor time restrictions.
Selected articles were reported and grouped based on the main topic, number of reviews, number of articles compared, number of patients, results.
3. Results
In the scientific literature we found out 4.856 articles about calcaneal fracture from 1945 to November 18th 2022, with an increasing number from 1980, (Figure 1).
Including only the metanalysis and systematic reviews the total pool of articles was 105 and all of them were published within 1997 and November 18th 2022.
46 out of the 105 papers were excluded because not focused on calcaneal fracture; thus, only 59 articles reviewed and discussed the calcaneal fracture management: 25 were metanalysis, 24 systematic reviews and 10 both (Figure 2).
The total number of articles analyzed in all the systematic reviews and/or metanalysis was 888 with over 10,000 calcaneal fractures treated.
Many topics have been covered in the reviews. (Table 1).
Direct Access to the Sinus Tarsi (STA) was compared to the Extended Lateral Approach (ELA) in 13 papers, 9 of which supported the superiority of minimally invasive STA versus extended lateral approach, while 4/13 papers declared no statistical difference between them [1,2,3,4,5,6,10,15,16,17,18,19,20].
Surgical approach was compared to conservative treatment in 12 studies, and 10 of these recognized more effectiveness in the surgical approach and only one didn’t show any significant statistical difference between these two strategies [11,12,21,22,23,24,25,26,27,28,29].
Complications and soft tissues were analyzed in 4 articles, and two of these stated that the most frequent complications occurred using the ELA; all articles pointed out that the clinical condition of overlying soft tissues is the most important predictor of complication; one of these four studies found out that there is no statistically significant difference between post-operative wound closure complications throughout different countries; one of the four articles mentioned that “bone graft, diabetes, no drainage, and fracture severity were all associated with an increased risk of wound complications after ORIF” [30,31,32,33].
ARIF was compared to AREF in 2 articles and both demonstrated good results in the outcomes but without statistically significant differences compared to traditional treatment [34,35].
ORIF revealed to be better in the results with respect to arthrodesis in Sanders type II/III fractures in both the dealing articles, while for Sanders type IV there was no statistical significant difference between the two treatments [35,40].
Three-dimensional (3D) printed assisted ELA surgery showed a better rate of excellent and good outcome, shorter operation time, less intraoperative blood loss, fewer intraoperative fluoroscopies, fewer complications (1 review) [36] .
The 2 reviews dealing with cannulated percutaneous screws versus ORIF showed that there is no statistically significant difference between these two treatments in the outcomes but seems that using the screws diminishes the risk of complications, surgical timing and they can afford a better reduction [9,37].
The review regarding fracture-dislocations showed that the time between diagnosis and treatment is the most important predictive factor determining outcomes [38].
Various treatments were compared in 6 papers: “in terms of excellent and good satisfaction ratings, the treatments were ranked as follows: STA (96.2%), ELA (66.8%), PRF (34.9%), and nonoperative (2%); in terms of incision complications, the treatments were ranked as follows: PRF (84.1%), MILA (80.0%), STA (35.8%), and ELA (0.1%)” [13,39,40,41,42,43,44].
One article talked about pedo-barography and showed that it can bea prediction tool for outcome, but it should be more standardized [44].
The results of the review that discussed the circular external fixator suggested its utility in treating this kind of lesion [45].
The degree of fracture exposure in open fractures affected the result especially in the healing time of the wound [46].
Two reviews proved the superiority of bone grafting in terms of AOFAS score with respect to the non-bone graft [15,47].
Percutaneous osteosynthesis was compared to ORIF in 3 reviews, but any statistically significant difference in functional scores and results was found; ORIF seems to be worst in wound complications [48,49,50].
One review told that instability of peroneal tendons is frequently associated with intra-articular fracture of the calcaneus and incidence increases with the severity of the fracture [51].
Timing in weight bearing is addressed in 1 review as a prediction tool: even allowing early weight bearing the outcome doesn’t change [52].
One article investigated various osteosynthesis treatments on cadaver finding any significant difference [53].
One article focused on the better results obtained with percutaneous osteosynthesis [54].
Calcaneus filling with calcium phosphates showed better results compared to autogenous bone graft in terms of pain and loss of fracture reduction [56].
4. Discussion
From the review of the secondary scientific literature we can understand that still to date the optimal calcaneal fracture management can be considered controversial.
Although treatment options are in continuous evolution and supported by research from surgical techniques to biomaterials and from tissue engineering to regenerative surgery, the field of calcaneal fracture is particularly challenging [59].
Papers dealing with operative versus conservative treatment show a superiority of surgery [1,2,3,4,5,6,15,16,17,18,19,20]. Patients surgically treated had less problems with shoe fitting and most of them returned to their preinjury activity and work; however, the AOFAS score did not reveal a statistically significant difference [60]. Anyway, the surgical treatment should be tailored on each patient considering that if surgical treatment can increase the probability of returning to previous activities, on the other hand the risk of complications is greater. However, in the case of an intra-articular displaced fracture of the calcaneus, reduction and osteosynthesis can prevent early subtalar arthrodesis. [20].
The most reported complications are skin problems with eventual infection, residual pain and development of osteoarthritis [6,61,62,63,64,65]. Many studies agree that the most important prognostic predictive factor of surgical treated fractures is the state of the soft tissues. In addition, post-ORIF complication risk is increased with bone graft, diabetes, no drainage and fracture severity [30,31,32,33].
Results concord that STA demonstrated to obtain better results while ELA has experienced a higher number of complications. The benefits highlighted for STA are shorter operation time, lower incidence of complications and overall better safety [10].
ARIF has experienced good results in diagnosis, but any statistically significant difference in outcomes if compared to other treatments. This procedure of increasing diagnostic importance in the future could improve the quality of the obtainable reduction and therefore the healing of the fracture [34,35,62].
3D printing is becoming an increasingly innovative and interesting solution [66,67,68,69]. “3D printing-assisted ELA surgery showed a better rate of excellent and good outcome, shorter operation time, less intraoperative blood loss, fewer intraoperative fluoroscopies and fewer overall complications. Besides, there is still a need for large- sample, high-quality, long-term randomized controlled trials to confirm this conclusion” [37].
ORIF seems to provide better results rather than with subtalar arthrodesis in Sanders type II/III, while for type IV there is no statistical difference. ORIF is the most suitable treatment for less complex calcaneus fractures, while when anatomical reduction is impossible, subtalar arthrodesis has better results in terms of functionality and complications [35]. Primary arthrodesis for the treatment of Sanders type IV fractures has shown good results considering the severity of bone impairment; however, this treatment is rarely chosen as the first approach due to poor residual function; its importance is therefore emphasized in a review when the degree of displacement is high [57,58].
Treatment with cannulated screws did not show a statistically significant difference compared to treatment with ORIF in terms of functional results. The treatment with cannulated screws, however, is told to be superior in terms of surgical timing and quality of reduction [9,38].
Resorbable metal osteosynthesis devices can also be a valid tool in certain cases, but unfortunately none of the reviews on calcaneal fractures have specifically considered them [70].
The instability of the peroneal tendons is often undiagnosed, despite it is frequently associated with increasing degree of calcaneus fracture and can compromise the stability of the hindfoot if not properly treated. “The double-density sign on profile radiography and abnormal talar tilt in the distal talofibular joint are important signs that may indicate fibular tendon dislocation. Timing in surgical intervention is essential for satisfactory clinical outcome. Orthopedic surgeons should be aware of this uncommon injury to avoid misdiagnosis or inappropriate treatment” [52].
In terms of functional results STA can be considered a good option, while in terms of complications arising in the skin, minimally invasive treatments are superior. Residual pain was reported to be not so different while return to preinjury activity and work and shoe fitting was better with surgery. Moreover, secondary subtalar fusion rate was lower with surgery. Anyway, workers' compensation affected outcome andnone of the methods of fixation revealed to be significantly superior [44].
In cases of osteoporotic fractures, angular stability plates appear to demonstrate greater mechanical strength than non-locking devices [45,46].
Comparing various studies it emerges that calcaneus fractures are treated more frequently with ORIF as the degree of complexity of the fracture increases. In case of lower complexity fracture, percutaneous management is the best alternative in terms of complications and anatomical reduction. Many percutaneous fixation methods were reported, like Schanz pins and Kirschner wires, cannulated screws, arthroscopically assisted techniques, but the inconsistency of documentation and the lack of statistical significance don’t allow definitive conclusions. Anyway, percutaneous fixations were associated with a much lower complication rate than those with open procedures, regardless of the technique [49,50,51].
An improvement in the quality of the reduction could be obtained with the use of intraoperative CT but at the expense of time and biological and economic costs.
Pedobarography sems to be a promising tool to predict outcomes but it should be more standardized. Possibly it could be useful in developing customized aids such as insoles, aiming for a more individualized improvement [45].
Using circular external fixator for calcaneal fracture is a good option for high degree displacement if the condition of the overlying tissues makes the fracture not surgically attackable. The results show a good reduction and recovery of function with low rates of complications such as infection. So we could consider external fixation a valid surgical alternative, but further high level studies are needed [46].
The use of bone graft is justified by the lack of spongy tissue that the compressive force determining the fracture causes. In many studies AOFAS scores were higher than with non-bone andsimilar Böhler’s angle, Gissane’s angle, calcaneal width, and calcaneal height were obtained. Moreover, no increased risk of postoperative complications was identifiedand it seems that with bone graft full weight bearing can be granted earlier without compromising outcomes compared to more conservative protocols. The use of bone graft seems to improve outcomes in terms of fracture reduction, lower pain into the fracture site and restoration of function [15,48]. An innovative solution is represented by injectable bone substitutes with regenerative capacity [71,72].
5. Conclusions
The management of calcaneus fractures is still controversial. The traumatic nature of the injury and the importance of this bone in supporting the load in the standing position and stepping, make its treatment and healing important. A correct and precise diagnostic pathway is crucial for an optimal treatment, and should include an accurate and specific history taking, a careful physical examination including soft tissue assessment and a precise classification of the fracture based on targeted radiographic and CT examinations. (Figure 3).
Only after a correct evaluation the most appropriate therapeutic path can be undertaken for that specific patient.
From this review of the secondary literature about calcaneus fracture management emerges that the optimal treatment should be studied and individualized according to the patient, his functional requirements and the type of fracture. New emerging technologies and new studies appear to offer an important therapeutic diagnostic support, but further investigations are necessary to determine its validity.
Author Contributions
Conceptualization, M.L.; methodology, M.L. and F.C..; software, F.C.; validation, all authors; formal analysis, F.C..; investigation, F.C., E.M. S., A.M., M.B., P.C., A.C., F.D.; resources, all authors; data curation, F.C.; writing—original draft preparation, M.L. and F.C.; writing—review and editing, all authors; visualization, all authors; supervision, M.L., M.R., F.A. G., L.R.; project administration, M.L.; funding acquisition, J.H. V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
J.H. Villafañe was supported by the Italian Ministry of Health - ricerca corrente 2023
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhang F, Tian H, Li S, Liu B, Dong T, Zhu Y, Zhang Y: Meta-analysis of two surgical approaches for calcaneal fractures: sinus tarsi versus extensile lateral approach. ANZ journal of surgery 2017, 87, 126–131. [CrossRef]
- Schepers T: The sinus tarsi approach in displaced intra-articular calcaneal fractures: a systematic review. International orthopaedics 2011, 35, 697–703. [CrossRef] [PubMed]
- Peng C, Yuan B, Guo W, Li N, Tian H: Extensile lateral versus sinus tarsi approach for calcaneal fractures: A meta-analysis. Medicine 2021, 100, e26717. [CrossRef]
- Ma D, Huang L, Liu B, Liu Z, Xu X, Liu J, Chu T, Pan L: Efficacy of Sinus Tarsal Approach Compared With Conventional L-Shaped Lateral Approach in the Treatment of Calcaneal Fractures: A Meta-Analysis. Frontiers in surgery 2020, 7, 602053.
- Lv Y, Zhou YF, Li L, Yu Z, Wang Q, Sun YY, Zhou DS: Sinus tarsi approach versus the extended lateral approach for displaced intra-articular calcaneal fractures: a systematic review and meta-analysis. Archives of orthopaedic and trauma surgery 2021, 141, 1659–1667. [CrossRef] [PubMed]
- Seat A, Seat C: Lateral Extensile Approach Versus Minimal Incision Approach for Open Reduction and Internal Fixation of Displaced Intra-articular Calcaneal Fractures: A Meta-analysis. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2020, 59, 356–366. [CrossRef]
- Ieropoli G, Villafane JH, Zompi SC, Morozzo U, D'Ambrosi R, Usuelli FG, Berjano P: Successful treatment of infected wound dehiscence after minimally invasive locking-plate osteosynthesis of tibial pilon and calcaneal fractures by plate preservation, surgical debridement and antibiotics. Foot 2017, 33, 44–47.
- Indino C, Villafane JH, D'Ambrosi R, Manzi L, Maccario C, Berjano P, Usuelli FG: Effectiveness of subtalar arthroereisis with endorthesis for pediatric flexible flat foot: a retrospective cross-sectional study with final follow up at skeletal maturity. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2020, 26, 98–104. [CrossRef]
- Fan B, Zhou X, Wei Z, Ren Y, Lin W, Hao Y, Shi G, Feng S: Cannulated screw fixation and plate fixation for displaced intra-articular calcaneus fracture: A meta-analysis of randomized controlled trials. International journal of surgery 2016, 34, 64–72. [CrossRef]
- Zeng Z, Yuan L, Zheng S, Sun Y, Huang F: Minimally invasive versus extensile lateral approach for sanders type II and III calcaneal fractures: A meta-analysis of randomized controlled trials. International journal of surgery 2018, 50, 146–153. [CrossRef]
- Selim A, Ponugoti N, Chandrashekar S: Systematic Review of Operative vs Nonoperative Treatment of Displaced Intraarticular Calcaneal Fractures. Foot & ankle orthopaedics 2022, 7, 24730114221101609.
- Meena S, Hooda A, Sharma P, Mittal S, Sharma J, Chowdhury B: Operative versus Non operative treatment of displaced intraarticular fracture of calcaneum: a meta-analysis of randomized controlled trials. Acta orthopaedica Belgica 2017, 83, 161–169.
- Zhang C, Ye ZM, Lin P, Miao XD: Lateral Fracture-Dislocation of the Calcaneus: Case Reports and a Systematic Review. Orthopaedic surgery 2021, 13, 682–691. [CrossRef] [PubMed]
- Barini M, Zagaria D, Licandro D, Pansini S, Airoldi C, Leigheb M, Carriero A: Magnetic Resonance Accuracy in the Diagnosis of Anterior Talo-Fibular Ligament Acute Injury: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11.
- Yang Y, Zhao H, Zhou J, Yu G: Treatment of displaced intraarticular calcaneal fractures with or without bone grafts: A systematic review of the literature. Indian journal of orthopaedics 2012, 46, 130–137. [CrossRef] [PubMed]
- Yao H, Liang T, Xu Y, Hou G, Lv L, Zhang J: Sinus tarsi approach versus extensile lateral approach for displaced intra-articular calcaneal fracture: a meta-analysis of current evidence base. Journal of orthopaedic surgery and research 2017, 12, 43. [CrossRef]
- Yu T, Xiong Y, Kang A, Zhou H, He W, Zhu H, Yang Y: Comparison of sinus tarsi approach and extensile lateral approach for calcaneal fractures: A systematic review of overlapping meta-analyses. Journal of orthopaedic surgery 2020, 28, 2309499020915282.
- Nosewicz TL, Dingemans SA, Backes M, Luitse JSK, Goslings JC, Schepers T: A systematic review and meta-analysis of the sinus tarsi and extended lateral approach in the operative treatment of displaced intra-articular calcaneal fractures. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2019, 25, 580–588. [CrossRef]
- Wu MH, Sun WC, Yan FF, Hou ZQ, Feng F, Cai L: [Minimally invasive sinus tarsal approach versus conventional L-shaped lateral approach in treating calcaneal fractures: a Meta-analysis]. Zhongguo gu shang = China journal of orthopaedics and traumatology 2017, 30, 1118–1126.
- Bai L, Hou YL, Lin GH, Zhang X, Liu GQ, Yu B: Sinus tarsi approach (STA) versus extensile lateral approach (ELA) for treatment of closed displaced intra-articular calcaneal fractures (DIACF): A meta-analysis. Orthopaedics & traumatology, surgery & research : OTSR 2018, 104, 239–244.
- Meena S, Gangary SK, Sharma P: Review Article: Operative versus nonoperative treatment for displaced intraarticular calcaneal fracture: a meta-analysis of randomised controlled trials. Journal of orthopaedic surgery 2016, 24, 411–416. [CrossRef] [PubMed]
- Jiang N, Lin QR, Diao XC, Wu L, Yu B: Surgical versus nonsurgical treatment of displaced intra-articular calcaneal fracture: a meta-analysis of current evidence base. International orthopaedics 2012, 36, 1615–1622. [CrossRef] [PubMed]
- Griffin D, Parsons N, Shaw E, Kulikov Y, Hutchinson C, Thorogood M, Lamb SE, Investigators UKHFT: Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. Bmj 2014, 349, g4483. [CrossRef] [PubMed]
- Luo X, Li Q, He S, He S: Operative Versus Nonoperative Treatment for Displaced Intra-Articular Calcaneal Fractures: A Meta-Analysis of Randomized Controlled Trials. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2016, 55, 821–828. [CrossRef] [PubMed]
- Zhang W, Lin F, Chen E, Xue D, Pan Z: Operative Versus Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures: A Meta-Analysis of Randomized Controlled Trials. Journal of orthopaedic trauma 2016, 30, e75–81. [CrossRef] [PubMed]
- Bruce J, Sutherland A: Surgical versus conservative interventions for displaced intra-articular calcaneal fractures. The Cochrane database of systematic reviews 2013, CD008628.
- Randle JA, Kreder HJ, Stephen D, Williams J, Jaglal S, Hu R: Should calcaneal fractures be treated surgically? A meta-analysis. Clinical orthopaedics and related research 2000, 217–227.
- Wei N, Yuwen P, Liu W, Zhu Y, Chang W, Feng C, Chen W: Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures: A meta-analysis of current evidence base. Medicine 2017, 96, e9027. [CrossRef]
- Liu Y, Li Z, Li H, Zhang Y, Wang P: Protective Effect of Surgery Against Early Subtalar Arthrodesis in Displaced Intra-articular Calcaneal Fractures: A Meta-Analysis. Medicine 2015, 94, e1984–e1980. [CrossRef]
- Backes M, Spierings KE, Dingemans SA, Goslings JC, Buckley RE, Schepers T: Evaluation and quantification of geographical differences in wound complication rates following the extended lateral approach in displaced intra-articular calcaneal fractures - A systematic review of the literature. Injury 2017, 48, 2329–2335.
- Zhang W, Chen E, Xue D, Yin H, Pan Z: Risk factors for wound complications of closed calcaneal fractures after surgery: a systematic review and meta-analysis. Scandinavian journal of trauma, resuscitation and emergency medicine 2015, 23, 18. [CrossRef]
- Zhang L, Su P, Li J: Complications in the Management of Displaced Intra-articular Calcaneal Fractures: A Systematic Review and Network Meta-Analysis of 2538 Patients. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2022.
- Halvachizadeh S, Klingebiel FKL, Pfeifer R, Gosteli M, Schuerle S, Cinelli P, Zelle BA, Pape HC: The local soft tissue status and the prediction of local complications following fractures of the ankle region. Injury 2022, 53, 1789–1795. [CrossRef] [PubMed]
- Williams CE, Joo P, Oh I, Miller C, Kwon JY: Arthroscopically Assisted Internal Fixation of Foot and Ankle Fractures: A Systematic Review. Foot & ankle orthopaedics 2021, 6, 2473011420950214.
- Marouby S, Cellier N, Mares O, Kouyoumdjian P, Coulomb R: Percutaneous arthroscopic calcaneal osteosynthesis for displaced intra-articular calcaneal fractures: Systematic review and surgical technique. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2020, 26, 503–508. [CrossRef] [PubMed]
- Almeida JF, Vale C, Gonzalez T, Gomes TM, Oliva XM: Osteosynthesis or primary arthrodesis for displaced intra-articular calcaneus fractures Sanders type IV - A systematic review. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2022, 28, 281–287. [CrossRef] [PubMed]
- Shi G, Liu W, Shen Y, Cai X: 3D printing-assisted extended lateral approach for displaced intra-articular calcaneal fractures: a systematic review and meta-analysis. Journal of orthopaedic surgery and research 2021, 16, 682. [CrossRef]
- Wang Q, Zhang N, Guo W, Wang W, Zhang Q: Cannulated screw fixation versus plate fixation in treating displaced intra-articular calcaneus fractures: a systematic review and meta-analysis. International orthopaedics 2021, 45, 2411–2421. [CrossRef]
- Gougoulias N, Khanna A, McBride DJ, Maffulli N: Management of calcaneal fractures: systematic review of randomized trials. British medical bulletin 2009, 92, 153–167. [CrossRef]
- Bridgman S, Dunn K, McBride D, Richards P: WITHDRAWN: Interventions for treating calcaneal fractures. The Cochrane database of systematic reviews 2008, CD001161.
- Wallin KJ, Cozzetto D, Russell L, Hallare DA, Lee DK: Evidence-based rationale for percutaneous fixation technique of displaced intra-articular calcaneal fractures: a systematic review of clinical outcomes. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2014, 53, 740–743. [CrossRef] [PubMed]
- Veltman ES, Doornberg JN, Stufkens SA, Luitse JS, van den Bekerom MP: Long-term outcomes of 1,730 calcaneal fractures: systematic review of the literature. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2013, 52, 486–490. [CrossRef] [PubMed]
- Pelliccioni AA, Bittar CK, Zabeu JL: Surgical treatment of intraarticular calcaneous fractures of sanders' types II and III. Systematic review. Acta ortopedica brasileira 2012, 20, 39–42. [Google Scholar]
- Shi F, Wu S, Cai W, Zhao Y: Comparison of 5 Treatment Approaches for Displaced Intra-articular Calcaneal Fractures: A Systematic Review and Bayesian Network Meta-Analysis. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2020, 59, 1254–1264. [CrossRef]
- Sanders FRK, Peters JJ, Schallig W, Mittlmeier T, Schepers T: What is the added value of pedobarography for assessing functional outcome of displaced intra-articular calcaneal fractures? A systematic review of existing literature. Clinical biomechanics 2020, 72, 8–15. [CrossRef] [PubMed]
- Muir RL, Forrester R, Sharma H: Fine Wire Circular Fixation for Displaced Intra-Articular Calcaneal Fractures: A Systematic Review. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2019, 58, 755–761. [CrossRef]
- Spierings KE, Min M, Nooijen LE, Swords MP, Schepers T: Managing the open calcaneal fracture: A systematic review. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2019, 25, 707–713. [CrossRef]
- Zheng W, Xie L, Xie H, Chen C, Chen H, Cai L: With versus without bone grafts for operative treatment of displaced intra-articular calcaneal fractures: A meta-analysis. International journal of surgery 2018, 59, 36–47. [CrossRef]
- Wang XJ, Su YX, Li L, Zhang ZH, Wei XC, Wei L: Percutaneous poking reduction and fixation versus open reduction and fixation in the treatment of displaced calcaneal fractures for Chinese patients: A systematic review and meta-analysis. Chinese journal of traumatology = Zhonghua chuang shang za zhi 2016, 19, 362–367.
- Wu J, Zhou F, Yang L, Tan J: Percutaneous Reduction and Fixation with Kirschner Wires versus Open Reduction Internal Fixation for the Management of Calcaneal Fractures: A Meta-Analysis. Scientific reports 2016, 6, 30480. [CrossRef]
- Majeed H, Barrie J, Munro W, McBride D: Minimally invasive reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular calcaneal fractures: A systematic review of the literature. EFORT open reviews 2018, 3, 418–425. [CrossRef] [PubMed]
- Mahmoud K, Mekhaimar MM, Alhammoud A: Prevalence of Peroneal Tendon Instability in Calcaneus Fractures: A Systematic Review and Meta-Analysis. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2018, 57, 572–578. [CrossRef] [PubMed]
- De Boer AS, Van Lieshout EMM, Van Moolenbroek G, Den Hartog D, Verhofstad MHJ: The effect of time to post-operative weightbearing on functional and clinical outcomes in adults with a displaced intra-articular calcaneal fracture; A systematic review and pooled analysis. Injury 2018, 49, 743–752.
- Dingemans SA, Sintenie FW, de Jong VM, Luitse JSK, Schepers T: Fixation Methods for Calcaneus Fractures: A Systematic Review of Biomechanical Studies Using Cadaver Specimens. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2018, 57, 116–122. [CrossRef] [PubMed]
- van Hoeve S, Poeze M: Outcome of Minimally Invasive Open and Percutaneous Techniques for Repair of Calcaneal Fractures: A Systematic Review. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons 2016, 55, 1256–1263. [CrossRef]
- Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P, 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M: The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. The Journal of bone and joint surgery American volume 2008, 90, 1186–1196. [Google Scholar] [CrossRef]
- Schepers T: The primary arthrodesis for severely comminuted intra-articular fractures of the calcaneus: a systematic review. Foot and ankle surgery : official journal of the European Society of Foot and Ankle Surgeons 2012, 18, 84–88. [CrossRef]
- Schepers T: The subtalar distraction bone block arthrodesis following the late complications of calcaneal fractures: a systematic review. Foot 2013, 23, 39–44. [CrossRef]
- Leigheb M: Wrist traumatology in the 2020s. Minerva Orthop 2021, 72, 93–94.
- Leigheb M, Janicka P, Andorno S, Marcuzzi A, Magnani C, Grassi F: Italian translation, cultural adaptation and validation of the "American Orthopaedic Foot and Ankle Society's (AOFAS) ankle-hindfoot scale". Acta bio-medica : Atenei Parmensis 2016, 87, 38–45.
- Leigheb M, Massa M, Bosetti M, Nico P, Tarallo L, Pogliacomi F, Grassi FA: Autologous Platelet Rich Plasma (PRP) in the treatment of elbow epicondylitis and plantar fasciitis: medium to long term clinical outcome. Acta bio-medica : Atenei Parmensis 2020, 91, e2020029.
- Leigheb M, Rusconi M, De Consoli A, Fredo M, Rimondini L, Cochis A, Pogliacomi F, Grassi FA: Arthroscopically-assisted Reduction and Internal Fixation (ARIF) of tibial plateau fractures: clinical and radiographic medium-term follow-up. Acta bio-medica : Atenei Parmensis 2020, 91, 152–159.
- Villafane JH, Valdes K, Pedersini P, Berjano P: Osteoarthritis: a call for research on central pain mechanism and personalized prevention strategies. Clinical rheumatology 2019, 38, 583–584. [CrossRef] [PubMed]
- Caruso I, Leonardini A, Caizzi G, Vicenti G, Caporusso M, Guarini F, Bernardis M, Moretti B, Giorgino F: Diabetic foot: clinical ap-proach. Minerva Orthop 2022, 73, 63–75.
- Buda R, Bruni D, Pantalone A: Current concepts in the treatment of ankle osteoarthritis. Minerva Orthop 2021, 72, 539–540.
- Cochis A, Bonetti L, Sorrentino R, Contessi Negrini N, Grassi F, Leigheb M, Rimondini L, Fare S: 3D Printing of Thermo-Responsive Methylcellulose Hydrogels for Cell-Sheet Engineering. Materials 2018, 11.
- Parchi P: 3D printing in orthopedic surgery. Minerva Orthop 2021, 72, 347–348.
- Aprato A, Giudice C: 3D printing in pediatrics orthopedics. Minerva Orthop 2022, 73, 551–553.
- Bonatti AF, Chiesa I, Micalizzi S, Vozzi G, De Maria C: Bioprinting for bone tissue engineering. Minerva Orthop 2021, 72, 376–394.
- Leigheb M, Veneziano M, Tortia R, Bosetti M, Cochis A, Rimondini L, Grassi FA: Osteosynthesis devices in absorbable Magnesium alloy in comparison to standard ones: a Systematic Review on effectiveness and safety. Acta bio-medica : Atenei Parmensis 2021, 92, e2021025.
- Bosetti M, Borrone A, Leigheb M, Shastri VP, Cannas M: Injectable Graft Substitute Active on Bone Tissue Regeneration. Tissue engineering Part A 2017, 23, 1413–1422. [CrossRef] [PubMed]
- Vicenti G, Ottaviani G, Bizzoca D, Carrozzo M, Simone F, Grosso A, Zavattini G, Elia R, MAuruccia M, SOlarino G et al: The manage-ment of post-traumatic bone defects: a systematic review. Minerva Orthop 2022, 73, 10–19.
- Waldorff EI, Markov MS: Magnetic and electromagnetic field in therapeutic application for bone stimulation. Minerva Orthop 2022, 73, 73–74.
- Mazzotti A, Langone L, Artioli E, Zielli SO, Arceri A, Setti S, Leigheb M, Samaila EM, Faldini C: Applications and Future Perspective of Pulsed Electromagnetic Fields in Foot and Ankle Sport-Related Injuries. Applied Sciences 2023, 13, 5807. [CrossRef]
Figure 1.
Trends and advances in calcaneal fracture research.
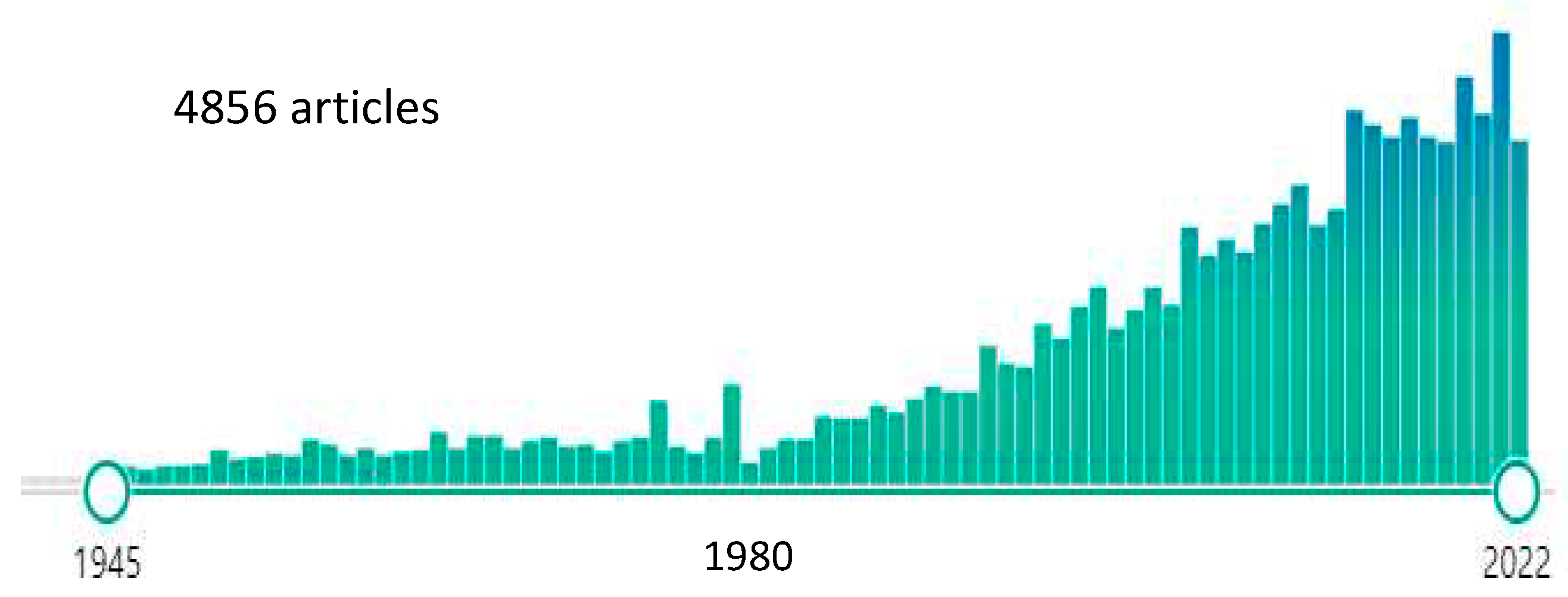
Figure 2.
Flow chart.
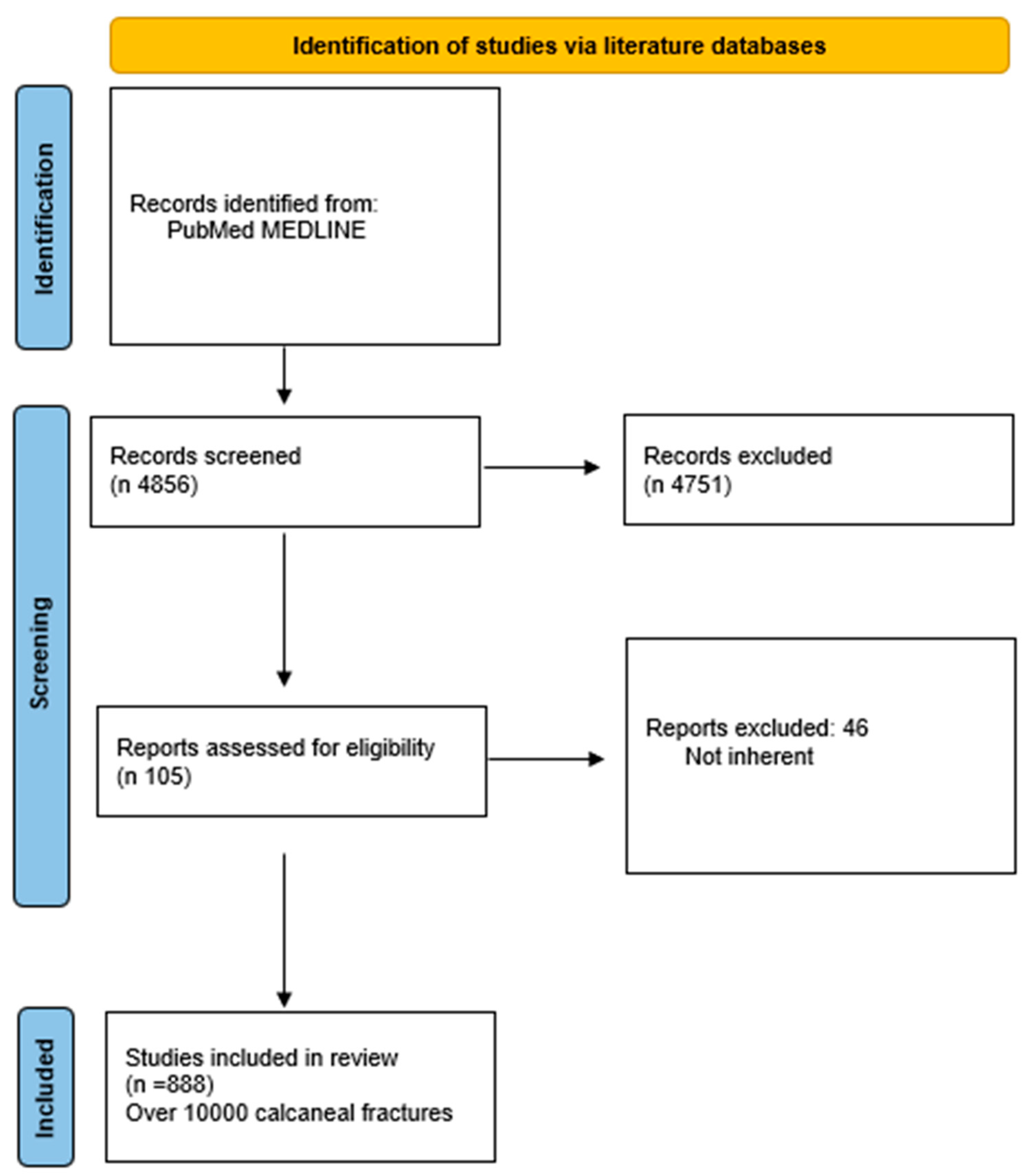
Figure 3.
Optimizing Diagnosis and Treatment of Calcaneus Fractures.
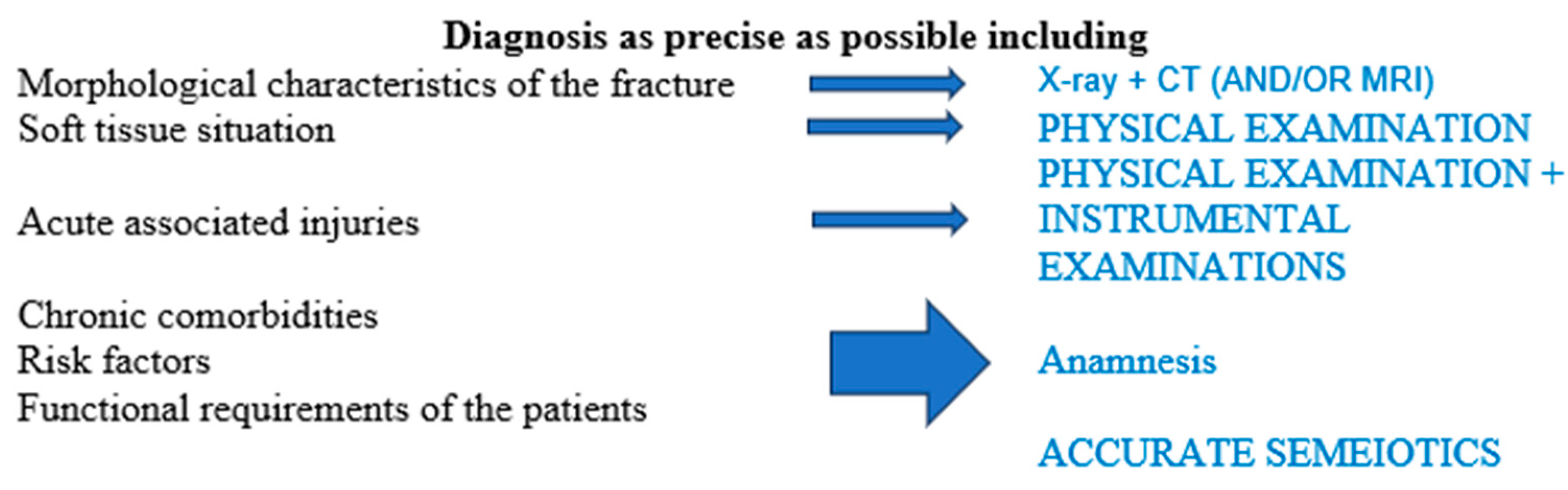

Table 1.
The analyzed articles.
| TOPIC | N Metanalysis or/and systematic reviews |
N Articles compared |
Results |
|---|---|---|---|
| STA VS ELA [1,2,3,4,5,6,10,15,16,17,18,19,20] |
13 | 8 8 7 8 X 12 15 5 27 9 8 7 8 |
STA > ELA 9 STA = ELA 4 |
| Conservative treatment VS Surgical treatment [11,12,21,22,23,24,25,26,27,28,29] |
11 | 8 10 18 8 7 4 7 7 13 8 18 4 |
Conservative treatment < Surgical treatment 11 Conservative treatment = Surgical treatment 1 |
| Complications and soft tissues [30,31,32,33] |
4 | 123 10 26 34 |
ELA experienced the most frequent complications PA better results The state of the overlying tissues is the + important predictor No difference between POWI and POWC over the countries |
| ARIF VS AREF [34,35] |
2 | 32 8 |
ARIF = others treatments ARIF > into diagnosyis |
| ORIF VS Arthrodesys [35,36] |
2 | 14 9 |
ORIF > arthrodesis in Sanders type II/III ORIF = arthrodesis in Sanders type IV |
| 3D printed-assisted [37] |
1 | 9 | “Excellent and good outcome, shorter operation time, less intraoperative blood loss, fewer intraoperative fluoroscopies, fewer complications.” |
| Cannulated screws VS ORIF [9,38] |
2 | 5 7 |
Same functional results Screw > ORIF for complications, quality of reduction, surgical timing |
| Dislocated fractures [13] |
1 | 4 | “Timely surgical intervention is essential for satisfactory clinic outcomes.” |
| Comparison between treatments [13,39,40,41,42,43,44] |
6 | 4 7 25 3 2 17 |
“PRF (87.0%), MILA (52.9%), STA (46.6%), ELA (40.4%), nonoperative (23.1%). In terms of excellent and good satisfaction ratings, the treatments were ranked as follows: STA (96.2%), ELA (66.8%), PRF (34.9%), and nonoperative (2%). In terms of incision complications, the treatments were ranked as follows: PRF (84.1%), MILA (80.0%), STA (35.8%), and ELA (0.1%).” “Results showed no difference in residual pain, but favoured surgical management on ability to return to the same work and to wear the same shoes as before the fracture.” “Displaced calcaneal fractures are treated surgically from 1 level I evidence study, 1 level II, and multiple studies with less than level II evidence, with open reduction and internal fixation as the method of choice. If the fracture is less complex, percutaneous treatment can be a good alternative according to current level 3 and 4 retrospective data.” “The results from the current data appear to be promising; however, the lack of statistical power and inconsistent documentation have made it difficult to determine any superiority. The complication rates were much lower than those with open procedures, regardless of the technique. The percutaneous fixation technique appears to be a favorable option for displaced intra-articular calcaneal fractures. Percutaneous fixation using Kirschner wires presented the best results, however, evidence is insufficient to assert superiority of this treatment in comparison with other surgical techniques. Sanders II/III” |
| Pedobarography for outcomes [45] |
1 | 9 | “As a prediction tool, it should be more standardised. may be useful in developing customized aids such as insoles, aiming for a more individualized improvement.” |
| Circular external fixator [46] |
1 | 11 | “Pin site infections were common (22.6%), serious complications, including deep infection (0.8%), wound infection (1.6%), and complex regional pain syndrome (0.8%), were exceedingly rare.” |
| Open fractures [47] |
1 | 18 | The degree of exposure affects the result, especially on the wound healing time |
| Bone plug [15,48] |
2 | 32 9 |
“Bone grafts achieved better AOFAS scores than the non-bone graft group. The two groups had similar results in Böhler angle, Gissane angle, calcaneal width, and calcaneal height. No increased risk of postoperative complications was identified.” |
| Percutaneous osteosyntesis VS ORIF [49,50,51] |
3 | 15 18 9 |
No differences in functional scores ORIF < in wound complications |
| Peroneal tendons instability [52] |
1 | 9 | “Prevalence of peroneal tendon instability is associated with intraarticular calcaneal fractures and increases with the severity of the fracture.” |
| Timing of load bearing [53] |
1 | 72 | “The adverse sequelae which are assumed to be associated with starting partial weightbearing already within six weeks after internal fixation of calcaneal fractures, is not supported by literature data.” |
| Osteosintesys on cadaver [54] |
1 | 14 | “None of the studies found a significant difference in favor of any of the fixation methods.” |
| Percutaneal osteosyntheses [55] |
1 | 46 | “Best outcomes for the minimal invasive open surgical treatment of calcaneal fractures” |
| Cementation with Calcium Phosphate [56] |
1 | 14 | “Lower prevalence of pain at the fracture site”; loss of fracture reduction |
| Arthrodesys in Sanders type IV [57,58] |
2 | 7 22 |
“Good results considering the severe nature of the injury.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



