
Submitted:
08 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Postoperative adhesive arachnoiditis is an inflammatory response of the spinal leptomeninges that occurs after surgery, resulting in scar formation in the avascular nature of the arachnoid layer. Clinical manifestations of this condition include pain, sensory deficits, motor dysfunction, reflex abnormalities, and bladder/bowel impairments. In MRI scans, the signs of postoperative adhesive arachnoiditis can vary, but some specific indicators can assist surgeons in locating the lesion and planning surgical interventions more accurately. In this report, we reported a 37-year-old man with postoperative adhesive arachnoiditis after two surgeries for Chiari I malformation, demonstrating that the gradually-forming the delta cord sign with sequential syringomyelia. During the intraoperative examination, we identified the presence of the delta cord sign, which was formed by an arachnoid scar that was tethering the dorsal spinal cord to the dura. This discovery allowed us to precisely pinpoint the location of the arachnoid scar, thereby providing valuable guidance to avoid any unnecessary exploration of innocent structures during the procedure. Other localization signs were also reviewed.
Keywords:
adhesive arachnoidit
; postoperative
; Chiari 1 malformation
; syringomyelia
; reoperation
; neuroimaging
1. Introduction
Postoperative adhesive arachnoiditis refers to an inflammatory response of the spinal leptomeninges following surgery. Previous studies have reported a prevalence of up to 20% [1]. The most common symptom is pain (92.9%), followed by motor deficits (35.7%) and sensory deficits (28.6%) [2]. Magnetic resonance imaging (MRI) is widely used for the diagnosis of postoperative adhesive arachnoiditis. MRI findings associated with adhesive arachnoiditis include various features at the adhesive site, such as clumped nerves [3,4], cord tethering [3-6], arachnoid septations [4], and arachnoiditis ossificans [4]. Additionally, non-specific findings may include hydrocephalus, syringomyelia [4,6] and arachnoid cysts [4]. These findings can be categorized as either localization signs or associated signs. Localization signs indicate the location of adhesive arachnoiditis, while associated signs are consequences of adhesive arachnoiditis. In cases where there is a lack of localization signs before surgery, the diagnosis is typically established during surgical exploration [7]. However, surgical exploration in the spine is a time-consuming and invasive procedure. Therefore, precise localization of the adhesive site before the operation can help avoid unnecessary surgical exploration. Recognizing the localization signs of adhesive arachnoiditis is crucial in this regard. This case report aims to present a new localization sign of adhesive arachnoiditis on MRI which was confirmed by intraoperative findings in a young adult patient with postoperative adhesive arachnoiditis after a surgery for Chiari I malformation. Additionally, it reviews the literature on adhesive arachnoiditis and categorizes the imaging findings as localization or associated signs.
2. Case illustration
A 29-year-old man presented with bilateral hand numbness and clumsiness. Neurological examination showed hyperreflexia in all limbs, suggesting cervical myelopathy. MRI revealed a 5mm descent of the tonsil below the foramen magnum, with syrinx formation, leading to a diagnosis of Chiari I malformation. No congenital abnormalities were found. The patient underwent a decompressive surgery involving suboccipital craniectomy, laminectomy of C1 and C2, and duroplasty. The first operation included a 2.5cm high and approximately 3cm wide suboccipital craniectomy. Intra-operatively, arachnoid space was dissected to confirm cerebrospinal fluid (CSF) flow patency. After the surgery, the patient's clumsiness improved, but poor wound healing and cerebral spinal fluid leakage occurred after 3 months, leading to a revision surgery for wound repair.
Over the 8-year follow-up, the patient's MRI studies revealed that the syrinx initially subsided after the 3-month post-operative MRI, but subsequently progressed over the next 5 years (Figure 1). By the 8th year, the patient returned with worsening symptoms, including intermittent neck and back pain, progressive left hemiparesis, and paresthesia over 6 months. Initially, the patient could walk with a cane, but his ambulation gradually deteriorated, and he required a quadricane for walking support. He also experienced numbness, clumsiness, and loss of grasp strength. His modified Japanese Orthopaedic Association (mJOA) scale score was 10, and the Barthel Index was 50. Neurological examination revealed muscle strength of 4 in the right upper and lower extremities and muscle strength of 2 in the left extremities. Atrophy of the intrinsic hand muscles was observed, along with hyperreflexia in all four limbs. However, there were no Hoffman's or Babinski's signs, and no cranial nerve involvement was noted. Cervical myelopathy was suspected, and cervical spine MRI confirmed the progression of the syrinx, extending to the C4 level, with edematous changes in the spinal cord. No brain or thoraco-lumbar abnormalities were found, and there was no epidural mass at the craniocervical junction.
During the review of the patient's cervical MRI series from previous years, a significant finding was identified at the C2 level. A thick arachnoid band was observed, attaching to the spinal cord and the dural sac, causing the cord to take on a triangular shape in the axial view. This characteristic change in cord shape was termed the "delta cord " sign (Figure 2). Over time, there was progression of the syrinx from the C2 level to the C4 level. Taking into account other potential factors that could contribute to recurrent syringomyelia, post-operative adhesive arachnoiditis was suspected.
To address this issue, a third surgery was performed, involving laminoplasty of C3-4 and extensive duroplasty from the suboccipital region to the C4 level. During the surgery, a thick arachnoid band was found tethering the cord at the C2 level, confirming the presence of the "delta cord" sign. After separating the arachnoid band, the syrinx collapsed, and there was no obstruction in the arachnoid space (Figure 3). Following one year of post-operative follow-up, the syrinx collapsed, and there was an improvement of the edematous change in the spinal cord (Figure 4). The patient's functional status also improved, with an increase in the mJOA scale score from 10 to 11 and in the Barthel Index score from 50 to 60.
3. Discussion
Adhesive arachnoiditis, or arachnoid scar, is an inflammatory response of the arachnoid mater after prior spinal surgery, infection, subarachnoid hemorrhage, or foreign body reaction after lumbar epidural injections, oil-based myelographic contrast agents, chemical irritation, or idiopathic [8-10]. Clinical manifestations include pain, sensory deficit, motor dysfunction, reflex abnormality and bladder/bowel impairment [2, 11]. However, the mechanism of postoperative adhesive arachnoidits is still not clear. The inflammation process from cytokines in cerebral spinal fluid inhibited healing process and caused scar formation at the avascular nature of arachnoid layer [8]. Adhesions or scarring within arachnoid channels may cause persistent syrinx or new onset symptoms without clear evidence of obstruction to CSF flow [12]. When the arachnoid scar blocked the CSF flow, the pressure gradient cause the syrinx formation [13]. Difference of microanatomical structure from ventral and dorsal subarachnoid space was well described, and dorsal site have more mesh-like arachnoid trabeculae than ventral site [14]. Theoretically, Koyanagi supposed that the dorsal subarachnoid space with rich arachnoid trabeculae and veins is prone to adhesive changes [10].
Adhesive arachnoiditis has been a significant focus of investigation in the past era when studying failed back surgery syndrome. Studies conducted in 1978 by Benner, Burton, Auld, and Quiles et al. provided evidence of adhesive arachnoiditis through myelography [15-18]. Subsequent research has delved into various imaging findings related to adhesive arachnoiditis. For instance, Matsui et al. revealed cauda equina adhesion on MRI in their study on a group with adhesive arachnoiditis.19 To identify adhesive arachnoiditis in MRI, using T2 MRI with true fast imaging with steady-state precession (TrueFISP) or acquisition sequences has proven to be helpful for localization [10,20]. The MRI signs associated with adhesive arachnoiditis encompass a range of features, such as hydrocephalus, syringomyelia [4,6], arachnoid cyst [4], clumped nerve [4], cord tethering [3-6], arachnoid septations [4], and arachnoiditis ossificans [4]. These signs are categorized as either localizzation signs, indicating the location of adhesive arachnoiditis, or associated signs, which represent the consequences of the condition (Table 1). In the case described in this report, the delta cord sign suggested an adhesive arachnoid scar at the C2 level, which was later confirmed during the operation. The delta cord sign uniquely provides diagnostic information from an axial view over the cord level while offering insights into the natural history of syrinx formation simultaneously.
Typically, the arachnoid space is challenging to visualize on MRI due to its woven and loose tubular texture filled with cerebrospinal fluid [14]. However, pathological changes can cause the arachnoid to become more compact and thicker, making it visible on MRI. In the case under consideration, the arachnoid band connecting the spinal cord to the thecal sac initially caused cord distortion, leading to the formation of a triangular shape (Figure 2 and Figure 3). This separation of CSF flow from cranial to caudal sides resulted in CSF filling the spinal canal and eventual syrinx formation. The impact of localization signs proves valuable for neurosurgeons in making precise surgical plans and avoiding unnecessary exploration of innocent structures. Cord tethering, which is often revealed on sagittal views on MRI, is another localization sign [3-6]. In a Chiari 1 malformation case with postoperative pseudomeningocele and cord distortion, Belen et al. successfully detethered the spinal cord based on the localization sign and repaired the pseudomeningocele [5]. Clumped root is another reported sign in lumbar adhesive arachnoiditis [3,4].
Surgical treatment options for postoperative adhesive arachnoiditis include adhesiolysis, expansile duroplasty, and CSF diversion from the ventricle or syrinx [10,12]. However, the surgical outcomes still unsatisfactory in some cases15-18.. For instance, David et al. reported eight cases of cranio-cervical junction arachnoiditis with syringomyelia diagnosed through MRI. All cases showed clinical improvement after undergoing adhesiolysis and duroplasty during a mean follow-up period of 27 months (ranging from 10 to 60 months). Nevertheless, three cases required additional shunt surgery. Hirai et al. presented a case of adhesive arachnoiditis with a large arachnoid cyst after epidural injection during a cesarean section. The patient received adhesiolysis and arachnoid cyst diversion, and symptoms improved over a period of 3 years [21]. In a study by Koyanagi et al., only 30.8% of secondary adhesive arachnoiditis cases (n=4) and all idiopathic adhesive arachnoiditis cases (n=6) showed clinical improvement after surgical treatment [10]. However, without precise localization, the arachnoid scar may be widespread or not found during exploratory surgery [12]. Killeen et al. presented a case of severe adhesive arachnoiditis developing after obstetric spinal anesthesia. The patient underwent several unsuccessful exploratory laminectomies and external drainage of the syrinx [10]. In the case described in this report, the delta cord sign served as a localization sign, indicating that the arachnoid band with cord tethering was located at the C2 level. The surgical strategy involved exploration at the C2 level to release the arachnoid band with expansile duroplasty. Additionally, the surgical approach was extended to the C4 level, and even lower levels if necessary, to assess the length of the arachnoid band and the flow of CSF intraoperatively. By utilizing the delta cord sign as a guide, the surgical team could focus on the precise location of the arachnoid scar, which helped in planning a targeted and effective surgical intervention. Extending the exploration to adjacent levels allowed for a comprehensive assessment of the condition, ensuring optimal treatment for the patient. This approach aimed to alleviate the symptoms associated with adhesive arachnoiditis and improve the patient's overall clinical outcome.
In this case, the treatment approach involved decompression surgery with duroplasty followed by a revision surgery for CSF leakage. Posterior fossa decompressive (PFD) craniectomy, laminectomy, and duroplasty are standard surgical treatments for symptomatic Chiari I malformation [22]. However, the routine use of duroplasty remains a topic of debate in the medical community. Yilmaz et al. suggested that patients with the cerebellar tonsil positioned below the C1 arch may benefit from duroplasty [23]. On the other hand, a review of 10 studies from 2000 to 2017 conducted by Xu et al. showed that PFD with duroplasty provided better clinical outcomes compared to PFD without duroplasty (mean difference = 0.85, 95% CI (0.73, 0.99), p < 0.05) [24]. However, it was also associated with a higher complication rate (mean difference = 0.34, 95% CI (0.19, 0.60), p < 0.05) [25]. The common complications observed were CSF leakage and arachnoid scar formation. Arachnoid scar were theoretically attributed to the exposure of subarachnoid space to blood and muscle cellular debris during the surgery, as well as the use of dural grafts [25]. In this specific case, the cerebellar tonsil was situated below the C1 level, prompting the surgical team to perform duroplasty to ensure sufficient decompression. However, the subsequent occurrence of CSF leakage and the need for revision surgery resulted in repetitive trauma and a higher likelihood of debris accumulation in the subarachnoid space. It is essential for surgeons to carefully weigh the potential benefits and risks of duroplasty in each individual case, taking into account the patient's specific anatomical characteristics and clinical condition. While duroplasty can improve clinical outcomes, it also poses an increased risk of complications such as CSF leakage and arachnoid scar formation.
Second, we also use fibrin glue to cover the suture site of dural graft and prevent CSF leakage. The use of fibrin glue to cover the suture site of the dural graft and prevent CSF leakage is a common practice in surgical procedures [26-28]. However, it is essential to recognize that fibrin glue acts by mimicking the final step in the coagulation pathway to form a fibrin clot [27]. It may cause hypersensitivity reaction in previous observation [29]. Another possibility is that fibrin glue might have been inadvertently squeezed into the subarachnoid space during wound closure, as it is inserted between muscular and fascial layers. Hayashi et al. reported a case of fibrin glue-induced adhesive arachnoiditis during the treatment of a sacral meningeal cyst. In this case, direct exposure to fibrin glue caused adhesion processes within the subarachnoid space [30]. Exposure to fibrin glue will cause the adhesion process within the subarachnoid space in our case. Third, dural graft material is also a risk factor of adhesive arachnoiditis [25]. We used DuroGen (Integra®) artificial dural graft for duroplasty in the first and revision surgery. As an allogenic substitute, it also bring a chance to stimulate the inflammatory process, especially while it directly contacts the subarachnoid space [31]. At last, surgery itself and blood content are also risk factors of adhesive arachnoiditis [8,9,15-19,32,33]. Avoiding unnecessary or repetitive exploration, removing blood clots while dura closure, water-tight fashion closure and preventing fibrin glue injection into subdural space might be the ways to prevent adhesive arachnoiditis.
4. Conclusions
The delta cord sign revealed the arachnoid scar location and nature history of adhesive arachnoiditis and syrinx formation. This sign will be beneficial to make a better surgical planning and avoid unnecessary exploration of innocent structure..
Author Contributions
JH Lin & YH Chiang developed the conceptualization and writing – review & editing. IT Tu contributed data curation, formal analysis, visualization, writing – original draft. YH Chiang provided project administration.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Taipei Medical University Hospital (protocol code 202305025 on 2023.5.10 of approval).
Informed Consent Statement
Patient consent was waived due to retrospective observation study
Data Availability Statement
All data is available in this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fitt, G.J.; Stevens, J.M. Postoperative arachnoiditis diagnosed by high resolution fast spin-echo MRI of the lumbar spine. Neuroradiology 1995, 37, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Parenti, V.; Huda, F.; Richardson, P.K.; Brown, D.; Aulakh, M.; Taheri, M.R. Lumbar arachnoiditis: Does imaging associate with clinical features? Clin Neurol Neurosurg 2020, 192, 105717. [Google Scholar] [CrossRef] [PubMed]
- Killeen, T.; Kamat, A.; Walsh, D.; Parker, A.; Aliashkevich, A. Severe adhesive arachnoiditis resulting in progressive paraplegia following obstetric spinal anaesthesia: a case report and review. Anaesthesia Anderson, T.L.; Morris, J.M.; Wald, J.T.; Kotsenas, A.L. Imaging Appearance of Advanced Chronic Adhesive Arachnoiditis: A Retrospective Review. AJR Am J Roentgenol 2017, 209, 648–655, 10.2214/ajr.16.16704. 2012, 67, 1386–1394. [Google Scholar] [CrossRef]
- Belen, D.; Er, U.; Gurses, L.; Yigitkanli, K. Delayed pseudomyelomeningocele: a rare complication after foramen magnum decompression for Chiari malformation. Surg Neurol 2009, 71, 357–361. [Google Scholar] [CrossRef]
- Inoue, Y.; Nemoto, Y.; Ohata, K.; Daikokuya, H.; Hakuba, A.; Tashiro, T.; Shakudo, M.; Nagai, K.; Nakayama, K.; Yamada, R. Syringomyelia associated with adhesive spinal arachnoiditis: MRI. Neuroradiology 2001, 43, 325–330. [Google Scholar] [CrossRef]
- Klekamp, J.; Iaconetta, G.; Batzdorf, U.; Samii, M. Syringomyelia associated with foramen magnum arachnoiditis. J Neurosurg 2002, 97, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.H.; Denney, L.C. A comprehensive review of spinal arachnoiditis. Orthop Nurs 2003, 22, 215–219. [Google Scholar] [CrossRef]
- Peng, H.; Conermann, T. Arachnoiditis. In StatPearls; StatPearls Publishing.
- Copyright © 2023, StatPearls Publishing LLC.: Treasure Island (FL), 2023.
- Koyanagi, I.; Chiba, Y.; Uemori, G.; Imamura, H.; Yoshino, M.; Aida, T. Pathophysiology and surgical treatment of spinal adhesive arachnoid pathology: patient series. J Neurosurg Case Lessons 2021, 2, Case21426. [Google Scholar] [CrossRef] [PubMed]
- Shikata, J.; Yamamuro, T.; Iida, H.; Sugimoto, M. Surgical treatment for symptomatic spinal adhesive arachnoiditis. Spine (Phila Pa 1976) 1989, 14, 870–875. [Google Scholar] [CrossRef]
- Silva, A.; Thanabalasundaram, G.; Wilkinson, B.; Tsermoulas, G.; Flint, G. Experience with revision craniovertebral decompression in adult patients with Chiari malformation type 1, with or without syringomyelia. Br J Neurosurg 2022, 36, 750–755. [Google Scholar] [CrossRef]
- Klekamp, J. The pathophysiology of syringomyelia - historical overview and current concept. Acta Neurochir (Wien) 2002, 144, 649–664. [Google Scholar] [CrossRef]
- Parkinson, D. Human spinal arachnoid septa, trabeculae, and "rogue strands". Am J Anat 1991, 192, 498–509. [Google Scholar] [CrossRef]
- Benner, B.; Ehni, G. Spinal arachnoiditis. The postoperative variety in particular. Spine (Phila Pa 1976) 1978, 3, 40–44. [Google Scholar] [CrossRef]
- Burton, C.V. Lumbosacral arachnoiditis. Spine (Phila Pa 1976) 1978, 3, 24–30. [Google Scholar] [CrossRef]
- Auld, A.W. Chronic spinal arachnoiditis. A postoperative syndrome that may signal its onset. Spine (Phila Pa 1976) 1978, 3, 88–91. [Google Scholar] [CrossRef]
- Quiles, M.; Marchisello, P.J.; Tsairis, P. Lumbar adhesive arachnoiditis. Etiologic and pathologic aspects. Spine (Phila Pa 1976) 1978, 3, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Matsui, H.; Tsuji, H.; Kanamori, M.; Kawaguchi, Y.; Yudoh, K.; Futatsuya, R. Laminectomy-induced arachnoradiculitis: a postoperative serial MRI study. Neuroradiology 1995, 37, 660–666. [Google Scholar] [CrossRef]
- Morisako, H.; Takami, T.; Yamagata, T.; Chokyu, I.; Tsuyuguchi, N.; Ohata, K. Focal adhesive arachnoiditis of the spinal cord: Imaging diagnosis and surgical resolution. J Craniovertebr Junction Spine 2010, 1, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Hirai, T.; Kato, T.; Kawabata, S.; Enomoto, M.; Tomizawa, S.; Yoshii, T.; Sakaki, K.; Shinomiya, K.; Okawa, A. Adhesive arachnoiditis with extensive syringomyelia and giant arachnoid cyst after spinal and epidural anesthesia: a case report. Spine (Phila Pa 1976) 2012, 37, E195–198. [Google Scholar] [CrossRef]
- De Vlieger, J.; Dejaegher, J.; Van Calenbergh, F. Posterior fossa decompression for Chiari malformation type I: clinical and radiological presentation, outcome and complications in a retrospective series of 105 procedures. Acta Neurol Belg 2019, 119, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Kanat, A.; Musluman, A.M.; Colak, I.; Terzi, Y.; Kayacı, S.; Aydin, Y. When is duraplasty required in the surgical treatment of Chiari malformation type I based on tonsillar descending grading scale? World Neurosurg 2011, 75, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Chu, L.; He, R.; Ge, C.; Lei, T. Posterior fossa decompression with and without duraplasty for the treatment of Chiari malformation type I-a systematic review and meta-analysis. Neurosurg Rev 2017, 40, 213–221. [Google Scholar] [CrossRef]
- Abla, A.A.; Link, T.; Fusco, D.; Wilson, D.A.; Sonntag, V.K. Comparison of dural grafts in Chiari decompression surgery: Review of the literature. J Craniovertebr Junction Spine 2010, 1, 29–37. [Google Scholar] [CrossRef]
- Shaffrey, C.I.; Spotnitz, W.D.; Shaffrey, M.E.; Jane, J.A. Neurosurgical Applications of Fibrin Glue: Augmentation of Dural Closure in 134 Patients. Neurosurgery 1990, 26, 207–210. [Google Scholar] [CrossRef]
- Green, A.L.; Arnaud, A.; Batiller, J.; Eljamel, S.; Gauld, J.; Jones, P.; Martin, D.; Mehdorn, M.; Ohman, J.; Weyns, F. A multicentre, prospective, randomized, controlled study to evaluate the use of a fibrin sealant as an adjunct to sutured dural repair. Br J Neurosurg 2015, 29, 11–17. [Google Scholar] [CrossRef]
- Atkinson, J.B.; Gomperts, E.D.; Kang, R.; Lee, M.; Arensman, R.M.; Bartlett, R.H.; Rais-Bharami, K.; Breaux, C.W., Jr.; Cornish, J.D.; Haase, G.M.; et al. Prospective, randomized evaluation of the efficacy of fibrin sealant as a topical hemostatic agent at the cannulation site in neonates undergoing extracorporeal membrane oxygenation. Am J Surg 1997, 173, 479–484. [Google Scholar] [CrossRef]
- Beierlein, W.; Scheule, A.M.; Dietrich, W.; Ziemer, G. Forty years of clinical aprotinin use: a review of 124 hypersensitivity reactions. Ann Thorac Surg 2005, 79, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Nagano, J.; Hattori, S. Adhesive arachnoiditis after percutaneous fibrin glue treatment of a sacral meningeal cyst. J Neurosurg Spine 2014, 20, 763–766. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.R.; Aleksic, S.; Ransohoff, J. Inflammatory reaction to synthetic dural substitute. Case report. J Neurosurg 1989, 70, 633–635. [Google Scholar] [CrossRef] [PubMed]
- Kok, A.J.; Verhagen, W.I.; Bartels, R.H.; van Dijk, R.; Prick, M.J. Spinal arachnoiditis following subarachnoid haemorrhage: report of two cases and review of the literature. Acta Neurochir (Wien) 2000, 142, 795–798. [Google Scholar] [CrossRef]
- Tumialán, L.M.; Cawley, C.M.; Barrow, D.L. Arachnoid cyst with associated arachnoiditis developing after subarachnoid hemorrhage. Case report. J Neurosurg 2005, 103, 1088–1091. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The series of cervical MRI (A) Typical Chiari 1 malformation before decompressive surgery (B)Due to transient dysphagia, we arranged C-spine MRI 1 week after decompressive surgery. Mild edematous change over medulla was found, short-term steroid was prescribed . Besides, adequate decompression was achieved and syrinx shrunk. (C) However, CSF leakage was noted 3 month after first operation, we performed dura repair. MRI before the operation showed no infection sign, and syrinx length decreased. (D) After half-year from revision surgery, MRI showed syrinx mild progression and a tethered cord to thecal sac. (E) In the 5th years follow-up, syrinx still progressed and extended to C3 level and edematous change of spinal cord was found. However, no clinical symptoms developed. (F) In the 8th years, progressive left side hemiparesis was found, MRI revealed syrinx extended to C4 level (arrow) and the revision surgery was performed.
Figure 1.
The series of cervical MRI (A) Typical Chiari 1 malformation before decompressive surgery (B)Due to transient dysphagia, we arranged C-spine MRI 1 week after decompressive surgery. Mild edematous change over medulla was found, short-term steroid was prescribed . Besides, adequate decompression was achieved and syrinx shrunk. (C) However, CSF leakage was noted 3 month after first operation, we performed dura repair. MRI before the operation showed no infection sign, and syrinx length decreased. (D) After half-year from revision surgery, MRI showed syrinx mild progression and a tethered cord to thecal sac. (E) In the 5th years follow-up, syrinx still progressed and extended to C3 level and edematous change of spinal cord was found. However, no clinical symptoms developed. (F) In the 8th years, progressive left side hemiparesis was found, MRI revealed syrinx extended to C4 level (arrow) and the revision surgery was performed.
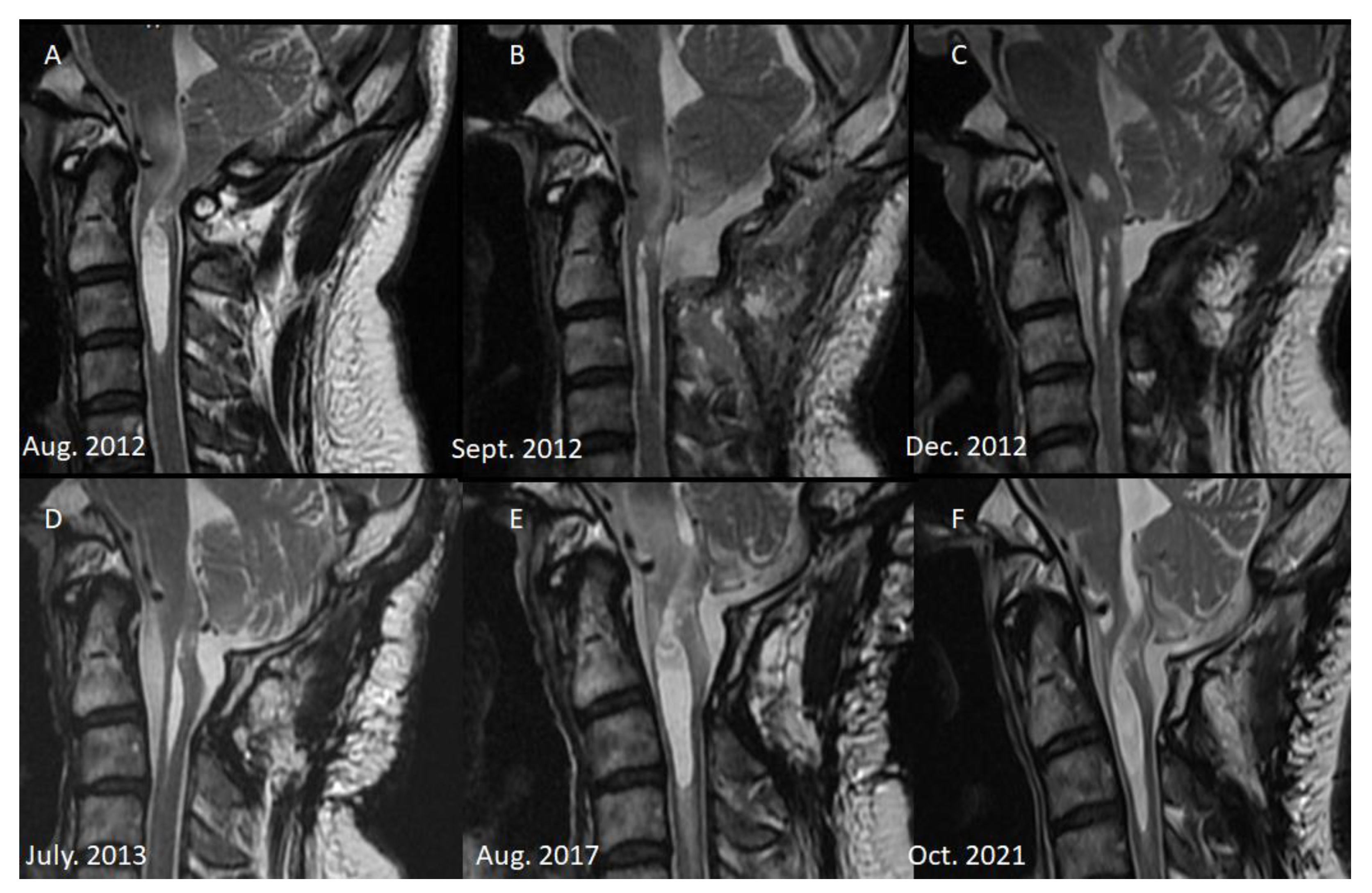
Figure 2.
Axial view of C2 level in different period (A) after 3 month from the first operation. (B) After 1 year, a thick arachnoid band (white arrow) attached posterior aspect of thecal sac, and made cord into a triangular shape: the delta cord sign. Syrinx progression was observed from this year. (C) spinal cord attached the thecal sac, and progressive syrinx and cord edematous change were found.
Figure 2.
Axial view of C2 level in different period (A) after 3 month from the first operation. (B) After 1 year, a thick arachnoid band (white arrow) attached posterior aspect of thecal sac, and made cord into a triangular shape: the delta cord sign. Syrinx progression was observed from this year. (C) spinal cord attached the thecal sac, and progressive syrinx and cord edematous change were found.
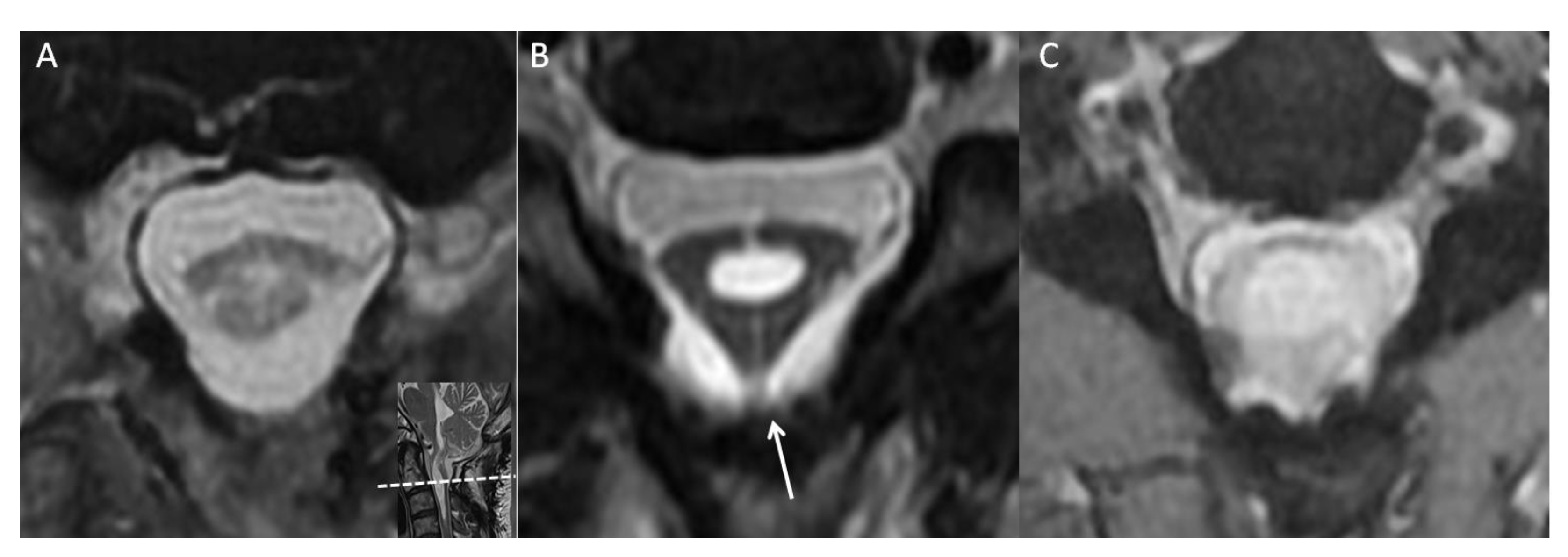
Figure 3.
Operative finding (A)at C2 level, a thick arachnoid band (white arrow) extended to C4 level and obstructed the CSF flow between cranial and caudal site. It was compactible to previous MRI finding of the delta cord sign (we rotated the axial MRI view 180 degree to match the operative finding) (B) after releasing the arachnoid band (arrow heads), the cord collapsed and connected CSF flow from cranial and caudal site was found.
Figure 3.
Operative finding (A)at C2 level, a thick arachnoid band (white arrow) extended to C4 level and obstructed the CSF flow between cranial and caudal site. It was compactible to previous MRI finding of the delta cord sign (we rotated the axial MRI view 180 degree to match the operative finding) (B) after releasing the arachnoid band (arrow heads), the cord collapsed and connected CSF flow from cranial and caudal site was found.
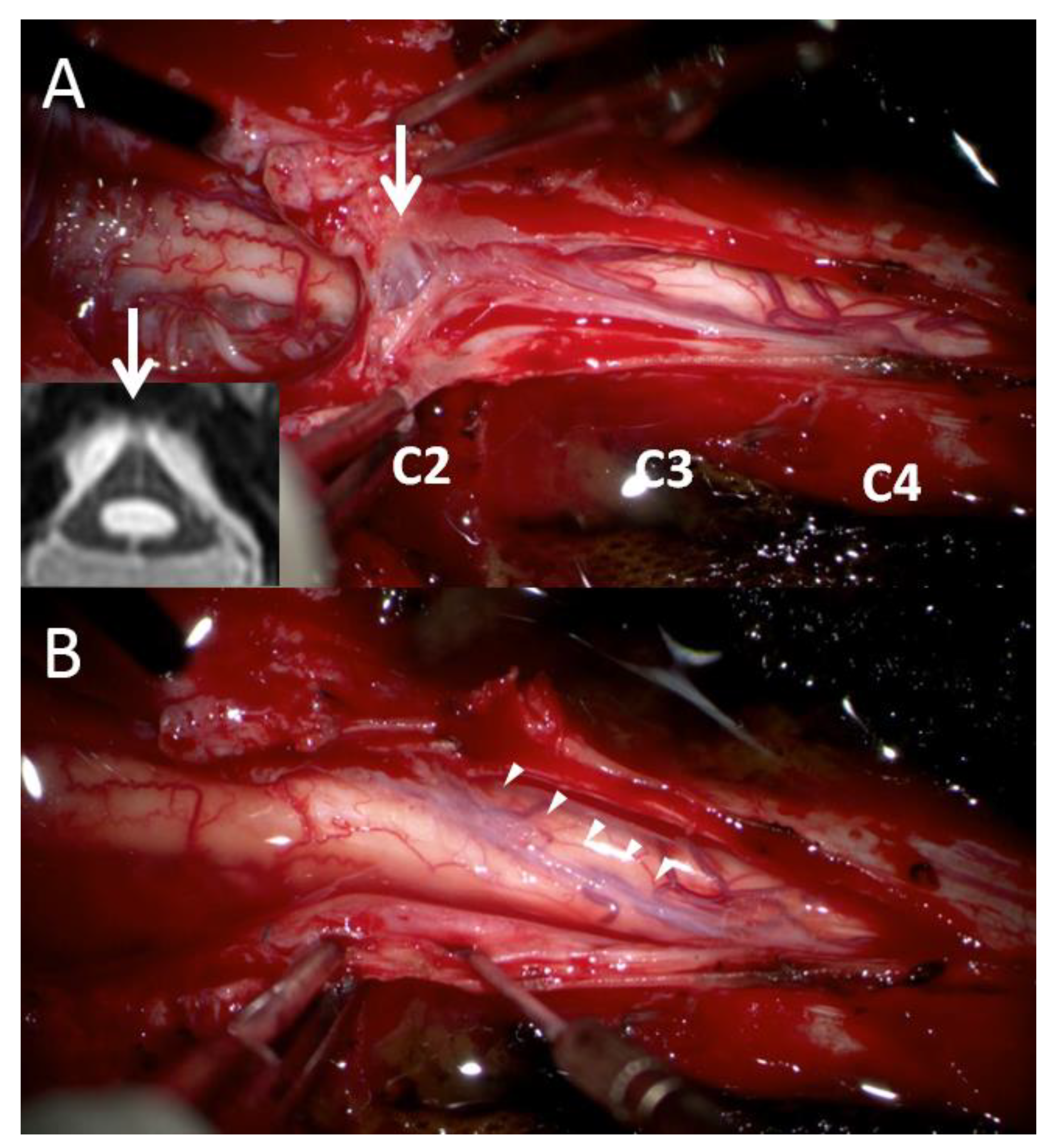
Figure 4.
(A) and (B) the delta cord sign and one year post-operation in MRI. The shape of cord became more oval. (C) Sagittal view of post-operative one year MRI. Decreasing diameter of the syrinx and absence of edematous change were found.
Figure 4.
(A) and (B) the delta cord sign and one year post-operation in MRI. The shape of cord became more oval. (C) Sagittal view of post-operative one year MRI. Decreasing diameter of the syrinx and absence of edematous change were found.
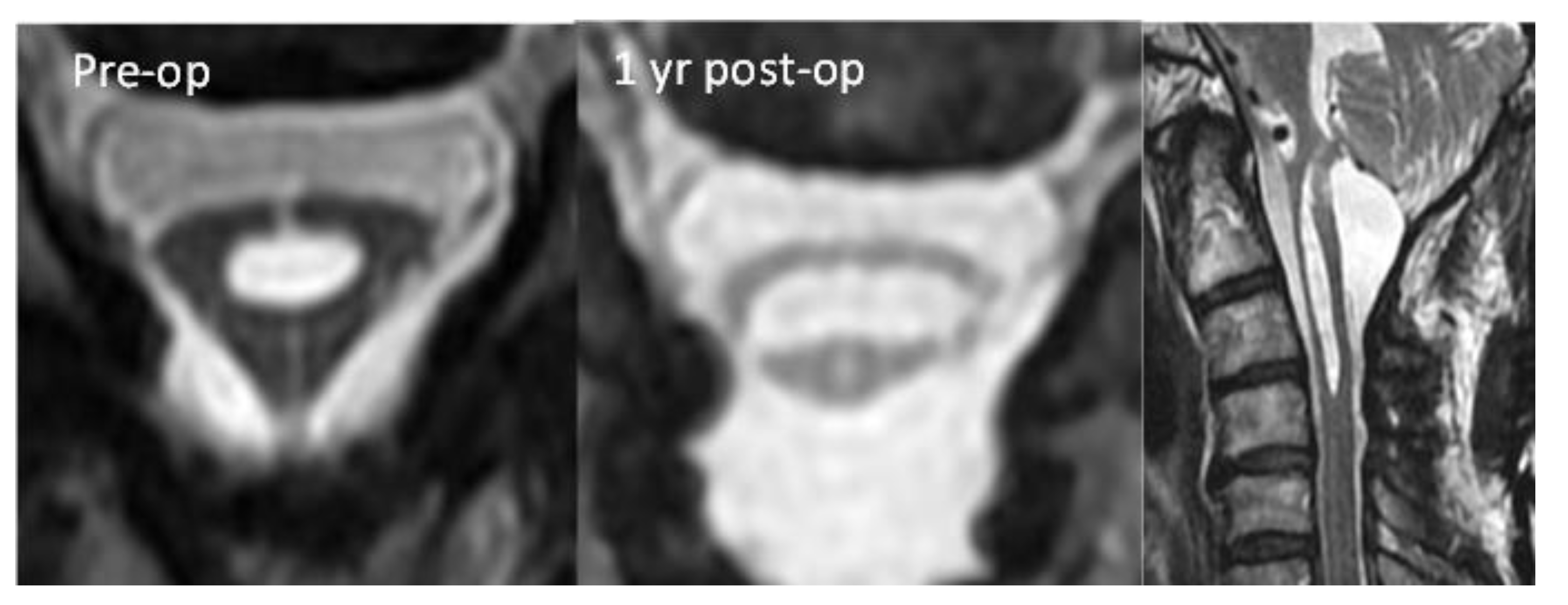

Table 1.
The localization and associated signs of adhesive arachnoiditis.
| CT or MRI finding | Evidence type | Hypothesis of pathophysiology |
|---|---|---|
| Nerve root clumping | localization sign | forming arachnoid scar in accordance with the magnitude of surgery and wound healing [19]. |
| Cauda equina adhesion | ||
| Disrupted cord contour | localization sign | fibrinous bands lead adhesions between the cord of the thecal sac [3]. |
| “ Delta cord” sign | ||
| Syringomyelia/syrinx | associated sign | Blocked CSF flow likely caused by adhesions or pressure gradient at the site of obstruction [4]. |
| Arachnoid septations | associated sign | Arachnoid web formation by chronic inflammation of the arachnoid [4]. |
| Arachnoid cyst | ||
| Pseudomyelomeningocele | associated sign | continuous CSF pressure that forced CSF came in contact with muscular layer [5]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



