
Submitted:
02 August 2023
Posted:
04 August 2023
You are already at the latest version
Abstract
This study aimed to present a systematic meta-analysis examining the association between Helicobacter pylori (H. pylori) infection, hemoglobin A1c levels, and the development of type 1 diabetes mellitus. The initial search identified 451 articles related to the association between H. pylori infection and T1DM. Among them, 14 articles had 2,971 participants meeting the inclusion criteria for advanced meta-analysis. A significant association was observed between H. pylori infection and T1DM, with an odds ratio (OR) of 1.87 (95% confidence interval [CI]: 1.27–2.78, p = 0.002). A subgroup analysis on H. pylori status showed that a longer duration of diabetes diagnosis and higher hemoglobin A1c levels were significantly associated with H. pylori infection (p < 0.001 for both). However, there was no significant association between H. pylori infection and the diagnostic age of diabetes (p = 0.306). These findings contribute to the understanding of the association between H. pylori infection and T1DM, thereby highlighting the potential role of H. pylori in influencing the duration and glycemic control of diabetes.
Keywords:
Helicobacter pylori
; Type 1 diabetes mellitus
; HbA1c
; Child
; Children
; Young patients
; Pediatrics
; Adolescents
; Meta-analysis
1. Introduction
Type 1 diabetes mellitus (T1DM) is a chronic and severe disease characterized by insufficient insulin produced by pancreatic β-cells. It generally believes that T1DM predominantly affects children and young adults. However, it can manifest at any age [1]. Recent studies have shown that the incidence of T1DM had been increasing. For example, several countries in South and Central America (e.g., Colombia, Mexico, Paraguay, Peru, and Venezuela) and East Asia (including China, Japan, Pakistan, and South Korea) reported that the incidence rates of T1DM range from 0.1 to 2.2 cases per 100,000 children per year [2]. Finland and Sardinia had relatively higher rates, with approximately 40 cases per 100,000 children per year, thereby indicating a significant subsequent increase to 60 cases per 100,000 children per year [3,4]. The actual etiology and underlying mechanisms remain largely elusive. Approximately 85%–90% of patients with T1DM exhibit autoantibodies targeting insulin, glutamic acid decarboxylase 65, insulinoma-associated autoantigen 2, zinc transporter 8, and tyrosine phosphatase IA-2β [5, 6]. Those autoimmune destruction of β-cells may lead to the development of T1DM. Therefore, an early and accurate diagnosis is imperative to provide an appropriate management and prevent complications.
Helicobacter pylori is a common gram-negative bacterium and pathogen, infecting over 50% of the global population. Because this bacterium is associated with carcinogenesis, several invasive and noninvasive diagnostic methods have been developed in clinical practice to detect this carcinogen. The invasive procedures include upper gastrointestinal endoscopy with gastric biopsy. Meanwhile, the noninvasive tests include the urea breath test, stool antigen test, and blood antigen test. These diagnostic approaches can help accurately identify H. pylori infection [7]. The prevalence of H. pylori infection ranges from 85% to 95% developing countries and from 30% to 50% in developed countries. Moreover, there has been a remarkable decline in the prevalence of H. pylori infection in European countries since 2000. However, the prevalence of H. pylori infection in Asian countries has remained relatively stable during this period [8,9]. H. pylori infection can have various effects on human health, thereby affecting both gastric and extra-gastric systems. The gastric complications associated with H. pylori infection include gastritis, peptic ulcer disease, functional dyspepsia, reflux disease, and gastric cancer. In addition, H. pylori infection is associated with extra-gastric complications such as cardiopulmonary diseases (coronary artery disease and asthma), hematologic diseases (iron deficiency anemia and immune thrombocytopenic purpura), neurologic diseases (ischemic stroke, Parkinson’s disease, Alzheimer’s disease, Guillain-Barré syndrome and migraines), dermatologic diseases (chronic spontaneous urticaria), and metabolic diseases (metabolic syndrome and insulin resistance). These diverse effects underscore the broad impact of H. pylori infection on human health [10-12].
Several studies have shown a significant association between H. pylori infection and elevated hemoglobin A1c (HbA1c) levels, particularly in individuals with type 2 diabetes [13-18]. Moreover, previous studies have reported higher serological prevalence rates of H. pylori infection among patients with T1DM [19]. Therefore, the current study aimed to conduct a systematic meta-analysis to determine the overall effect size of the association between H. pylori infection, HbA1c levels, and the development of T1DM in pediatric patients.
2. Material and Methods
2.1. Data Collection
All original articles were searched from international databases, including NCBI (PubMed), ISI Web of Science, EMBASE, and Cochrane Library, without language limitations. The search strategy was conducted using the PICOS tool, which uses data on population (children), intervention (diabetes), outcomes (H. pylori infection), and study type (case-control study). The complete list of searched keywords were Diabetes, Diabetes Mellitus (type 1 and 2), Insulin Dependent, IDDM, NIDDM, Noninsulin Dependent, Insulin Sensitivity, Helicobacter pylori, campylobacter pylori, H Pylori, Child, Children, Young patients, Pediatric, and Adolescents.
The articles meeting the following inclusion criteria were evaluated: (1) case-control studies, (2) those with patients aged <20 years, (3) those that used H. pylori as an exposure variable. Case reports, reviews, meta-analyses, cross-sectional studies, and cohort studies were excluded from the analysis.
2.2. Statistical Analysis
Odds ratio (OR) and standard error were used in the meta-analysis. MedCalc was used to calculate the estimated odds ratio with 95% confidence interval. Differences in terms of means and standard deviations were used for subgroup analysis. The random-effect model was used to combine the estimated effects [20]. Statistical heterogeneity among studies was evaluated using I2 statistics [21].
All statistical analyses were performed using the Comprehensive Meta-Analysis (CMA) 4.0 software, and a p-value of <0.05 was considered statistically significant.
3. Results
3.1. Characteristics and Methodologies of the Included Studies
The initial search yielded 451 articles examining the association between H. pylori infection and T1DM. Further examination excluded 437 articles, including 106 duplicate articles, 265 articles with unrelated outcomes, 66 reviews, letters, meta-analysis studies, and case reports. The remaining 14 articles were selected for an advanced meta-analysis (Figure 1). One study was conducted on children without information regarding age, and other studies included patients aged 10–20 years. Table 1 shows the characteristics of the included articles. In total, 2,971 participants were selected in this meta-analysis, and the total number of cases and controls in the study was 1190 and 1781, respectively. In six studies, H. pylori infection was diagnosed using the enzyme-linked immunosorbent assay. The remaining studies used other methods such as the 13C urea breath test, RIBASIA, rapid urease test, enzyme immunoassay (EIA), and stool antigen test. Most studies are case-control studies regarding T1DM and H. pylori infection. To assess publication bias, a funnel plot was constructed using the logarithm and logarithm standard error of the odds ratio (OR) values for H. pylori infection. The funnel plot exhibited a symmetrical distribution, and it was analyzed using the Begg’s rank correlation method. Results showed that the association was not statistically significant (Pr > |z| = 0.656 > 0.05), thereby indicating the absence of publication bias (Figure 2)
3.2. Meta-Analysis Results
In total, 578 (44.74%) and 420 (23.32%) participants in the diabetes and healthy groups had H. pylori infection, respectively. The OR of the association between H. pylori infection and diabetes was 1.87 (95% CI: 1.27–2.78, p = 0.002) (Figure 3).
Data, including diagnostic age, HbA1c levels, and duration of diabetes, were comprehensively collected from patients with diabetes for an advanced subgroup analysis. The participants were divided into the H. pylori positive (HP+) and H. pylori negative (HP-) groups. This division allowed for the analysis of the association between H. pylori infection and these respective subgroups (Table 2).
In the diabetic group, further subgroup analysis was performed with the random effect model. The association between H. pylori infection and the diagnostic age of diabetes was not significant (p = 0.306) (Figure 4). Our results revealed that a longer diabetes diagnosis duration and high HbA1c levels were significantly associated with the H. pylori infection (p < 0.001 and p < 0.001, respectively) (Figure 5 and Figure 6).
4. Discussion
This meta-analysis aimed to investigate the association between H. pylori infection and T1DM. Results showed a significant association between H. pylori infection and the risk of elevated HbA1c levels and diabetic duration in patients with T1DM. These results are in accordance with those of previous studies conducted worldwide, thereby providing further support for the above mentioned association. The seroprevalence of H. pylori in patients diagnosed with T1DM was significantly elevated compared with that in healthy control individuals [22-24]. The prevalence of positive H. pylori cases was slightly higher in patients with diabetes who were aged over 12 years and who had longer disease duration. However, the result did not significantly differ [24]. Another study showed that H. pylori-positive patients with higher HbA1c levels exhibited a significantly longer diabetes duration [24]. H. pylori infection has a substantial negative impact on metabolic control in children and adolescents diagnosed with type 1 diabetes mellitus [25,26]. In patients infected with H. pylori, impaired glycemic control may be attributed to the high production of pro-inflammatory cytokines triggered by gastric infection [27]. Conversely, disturbances in glucose metabolism could facilitate the colonization of H. pylori [28].
A meta-analysis conducted by Feng Wang, including 39 eligible studies from 1997 to 2012, showed a significant association between H. pylori infection and an elevated risk of both T1DM and type 2 diabetes mellitus (T2DM) [29]. Kamyar Mansori performed a meta-analysis on 41 studies with 9,559 individuals from 1990 to 2019. Results showed a significant statistical association between H. pylori infection and the risk of developing diabetes. Subgroup analysis based on the type of diabetes revealed a significant association between H. pylori infection and the risk of T2DM. However, this meta-analysis found a positive association between T1DM and H. pylori infection. However, the result was not statistically significant [14]. Another study revealed that the presence of H. pylori infection was not significantly associated with diabetes in children with T1DM, and there was no difference in terms of glycemic control between patients with T1DM who developed H. pylori infection and those without [30]. The potential association between H. pylori infection and T1DM remains a topic of debate, particularly concerning factors such as glycemic control, gastrointestinal symptoms, infection prevalence, eradication and reinfection rates, and sanitary condition [22]. Our current study performed a meta-analysis of 14 studies with 2,971 individuals from 1997 to 2020. Results showed a positive correlation between H. pylori infection and HbA1c levels as well as diabetic duration in patients with T1DM. This study performed an extensive and up-to-date literature search, which identified a significant number of studies. These studies provided sufficient data to pool information from nearly 2,971 pediatric subjects, thereby indicating relatively large sample sizes. Importantly, no individual study had a substantial influence on the overall results.
An alternative inference can be made based on our findings regarding the impact of diabetes mellitus on the incidence of H. pylori infection. Hence, this infection might be a complication rather than a cause of DM. This result could be attributed to reduced gastric motility and peristaltic activity in individuals with diabetes, which could facilitate the colonization of H. pylori [28]. Furthermore, chemical changes in the gastric mucosa, such as non-enzymatic glycosylation of mucins and elevated sialic acid levels, may act as receptors on cell surfaces, thereby facilitating the adhesion of H. pylori to gastric mucosa cells. [31-33]. In addition, impaired non-specific immunity further contributes to the risk of H. pylori infection in patients with diabetes [31]. Further, several mechanisms that can explain the association between H. pylori infection and the risk of diabetes have been proposed. One mechanism involves inflammatory cytokines, which can induce the phosphorylation of serine residues on the insulin receptor substrate. This phosphorylation may impair the interaction between the substrate and the insulin receptors, leading to impaired insulin function [34]. Furthermore, H. pylori infection induces inflammation, which affects pancreatic β-cells, leading to a decrease in insulin secretion. In particular, cag+ strains of H. pylori can further reduce insulin secretion by affecting the production of somatostatin [14,35]. Another mechanism involves lipopolysaccharides (LPS) produced by gram-negative bacteria such as H. pylori. These LPS can activate Toll-like receptors, resulting in insulin resistance [36]. Moreover, H. pylori infection is associated with elevated leptin and ghrelin levels, which can contribute to obesity and increase the risk of developing diabetes [37]. These events collectively contribute to poor blood sugar control and the development of diabetes mellitus.
Differences in the prevalence of infection can be attributed to several factors, including the inclusion of study populations with various age and sample size. Age is an important factor as it influences H. pylori exposure over time, and similar age groups should be compared when examining the prevalence of infection. Furthermore, the diagnostic methods used for assessing H. pylori infection varied. These included the urea breath test, measurement of anti-H. pylori IgA, IgG, and IgM antibodies, detection of H. pylori antigen in stool samples, and measurement of anti-CagA IgG antibodies. These methods contribute to the divergent findings on this topic. In the current study, the assessment of fecal H. pylori antigens was performed, which may offer a greater relevance for identifying active gastrointestinal infection in specific patients with diabetes [38]. Notably, serologic methods cannot differentiate between recent and previous infections. Therefore, future studies should include multiple tests to provide more comprehensive and reliable results. The current study had several limitations. First, there was no information regarding the history of drug or non-drug treatments in patients with H. pylori infection. Such treatments can affect the presence of H. pylori infection and the development of metabolic syndrome and insulin resistance. Future studies should consider evaluating the impact of different treatments on these outcomes in individuals with H. pylori infection. Second, gastrointestinal co-morbidities, such as coeliac disease, were not considered; hence, these should be addressed in future studies. Third, the current study focused on patients with T1DM patients, which limited the ability to compare the association between H. pylori infection and HbA1c levels between patients with T1DM and those with T2DM. Therefore, future studies should include patients with T2DM to facilitate a more comprehensive analysis and provide valuable insights on the differences and similarities in the association between H. pylori infection and HbA1c levels across different types of diabetes. However, our study does not have access to a dataset from Asian populations, thereby limiting the generalizability of our findings to this specific demographic. To further investigate the association between H. pylori infection and HbA1c levels in patients with diabetes mellitus, future research should include datasets from Asian populations. This could provide a more comprehensive understanding of the association and help determine any regional variations or specific considerations that must be considered in clinical practice and the management of patients with diabetes worldwide. Notably, in this meta-analysis, all studies had a case-control design. Case-control studies can provide valuable insights about associations. However, they have inherent limitations, such as recall, and selection biases. Therefore, the design and implementation of cohort studies could be essential for a more comprehensive and detailed assessment of the association between H. pylori infection and diabetes. By incorporating cohort study designs, researchers can establish temporal associations, follow-up participants over time, and gather longitudinal data, which can enhance our understanding of the causal association between H. pylori infection and diabetes. Further, they can examine potential confounding factors and provide more robust evidence. In addition, it is important to acknowledge that personal judgments may have influenced various stages of the meta-analysis, including the search for articles, data extraction, and the assessment of included articles. To minimize bias, rigorous, and systematic methods, such as predefined search criteria, independent data extractions, and quality assessment, were used. To further advance our understanding of the association between H. pylori infection and diabetes, future research should prioritize the inclusion of well-designed cohort studies. These studies should adhere to transparent and rigorous methodologies to minimize biases and increase the validity and generalizability of the findings. Moreover, data on important variables including weight loss, socioeconomic status, and household size were not collected. Nevertheless, future studies should include such details as they can contribute to a more comprehensive understanding of the topic.
5. Conclusions
The subgroup analysis revealed a significant positive association between H. pylori infection and HbA1c levels as well as the duration of diabetes diagnosis. Therefore, chronic conditions characterized by dysregulated glycemic control and prolonged disease onset may increase the risk of H. pylori infection. Hence, large-scale cohort studies with a substantial sample size should be performed to further assess this association. This can provide more robust evidence and a better understanding of the association between H. pylori infection and the outcomes of interest.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Buzzetti, R.; Zampetti, S.; Maddaloni, E. Adult-onset autoimmune diabetes: current knowledge and implications for management. Nature reviews. Endocrinology 2017, 13, 674–686. [Google Scholar] [CrossRef] [PubMed]
- Harjutsalo, V.; Sjöberg, L.; Tuomilehto, J. Time trends in the incidence of type 1 diabetes in Finnish children: a cohort study. Lancet 2008, 371, 1777–1782. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, M.; Viik-Kajander, M.; Moltchanova, E.; Libman, I.; LaPorte, R.; Tuomilehto, J. Incidence of childhood type 1 diabetes worldwide. Diabetes Mondiale (DiaMond) Project Group. Incidence of childhood type 1 diabetes worldwide. Diabetes mondiale (DiaMond) project Group. Diabetes care 2000, 23, 1516–1526. [Google Scholar] [CrossRef] [PubMed]
- Songini, M.; Mannu, C.; Targhetta, C.; Bruno, G. Type 1 diabetes in Sardinia: facts and hypotheses in the context of worldwide epidemiological data. Acta diabetologica 2017, 54, 9–17. [Google Scholar] [CrossRef]
- de Ferranti, S.D.; de Boer, I.H.; Fonseca, V.; Fox, C.S.; Golden, S.H.; Lavie, C.J.; Magge, S.N.; Marx, N.; McGuire, D.K.; Orchard, T.J.; et al. Type 1 diabetes mellitus and cardiovascular disease: a scientific statement from the American Heart Association and American Diabetes Association. Circulation 2014, 130, 1110–1130. [Google Scholar] [CrossRef]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef] [PubMed]
- McColl, K.E. Clinical practice. Helicobacter pylori infection. The New England journal of medicine 2010, 362, 1597–1604. [Google Scholar] [CrossRef]
- Khoder, G.; Muhammad, J.S.; Mahmoud, I.; Soliman, S.S.M.; Burucoa, C. Prevalence of Helicobacter pylori and its associated factors among healthy asymptomatic residents in the United Arab Emirates. Pathogens 2019, 8. [Google Scholar] [CrossRef]
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter pylori infection. Helicobacter 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.; Rayner-Hartley, E.; Byrne, M.F. Extraintestinal manifestations of Helicobacter pylori: a concise review. World journal of gastroenterology 2014, 20, 11950–11961. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J.; Zavos, C.; Deretzi, G. The association between Helicobacter pylori infection and insulin resistance: a systematic review. Helicobacter 2011, 16, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Vaira, U.; Gatta, L.; Ricci, C.; D’Anna, L.; Iglioli, M.M. Helicobacter pylori: diseases, tests and treatment. Digestive and liver disease: official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver 2001, 33, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Kouitcheu Mabeku, L.B.; Noundjeu Ngamga, M.L.; Leundji, H. Helicobacter pylori infection, a risk factor for type 2 diabetes mellitus: a hospital-based cross-sectional study among dyspeptic patients in Douala-Cameroon. Scientific reports 2020, 10, 12141. [Google Scholar] [CrossRef] [PubMed]
- Mansori, K.; Moradi, Y.; Naderpour, S.; Rashti, R.; Moghaddam, A.B.; Saed, L.; Mohammadi, H. Helicobacter pylori infection as a risk factor for diabetes: a meta-analysis of case-control studies. BMC gastroenterology 2020, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.C.; Wang, S.S.; Hsieh, Y.T.; Kuo, F.C.; Soon, M.S.; Wu, D.C. Helicobacter pylori infection associated with high HbA1c and type 2 diabetes. European journal of clinical investigation 2013, 43, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.S.; Choi, Y.; Kim, N.; Lim, S.H.; Noh, G.; Kim, K.W.; Park, J.; Jo, H.; Yoon, H.; Shin, C.M.; et al. Long-term effect of the eradication of Helicobacter pylori on the hemoglobin A1c in type 2 diabetes or prediabetes patients. The Korean journal of internal medicine 2022, 37, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xing, Y.; Zhao, L.; Ma, H. The association between Helicobacter pylori infection and glycated hemoglobin A in diabetes: A meta-analysis. Journal of diabetes research 2019, 2019, 3705264. [Google Scholar] [CrossRef]
- Maluf, S.; Salgado, J.V.; Cysne, D.N.; Camelo, D.M.F.; Nascimento, J.R.; Maluf, B.V.T.; Silva, L.D.M.; Belfort, M.R.C.; Silva, L.A.; Guerra, R.N.M.; et al. Increased glycated hemoglobin levels in patients with Helicobacter pylori infection are associated with the grading of chronic gastritis. Frontiers in immunology 2020, 11, 2121. [Google Scholar] [CrossRef]
- de Luis, D.A.; de la Calle, H.; Roy, G.; de Argila, C.M.; Valdezate, S.; Canton, R.; Boixeda, D. Helicobacter pylori infection and insulin-dependent diabetes mellitus. Diabetes research and clinical practice 1998, 39, 143–146. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgins, J.P. Meta-analysis and subgroups. Prevention science: the official journal of the Society for Prevention Research 2013, 14, 134–143. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- El-Eshmawy, M.M.; El-Hawary, A.K.; Abdel Gawad, S.S.; El-Baiomy, A.A. Helicobacter pylori infection might be responsible for the interconnection between type 1 diabetes and autoimmune thyroiditis. Diabetology and metabolic syndrome 2011, 3, 28. [Google Scholar] [CrossRef] [PubMed]
- Zekry, O.A.; Abd Elwahid, H.A. The association between Helicobacter pylori infection, type 1 diabetes mellitus, and autoimmune thyroiditis. The journal of the Egyptian Public Health Association 2013, 88, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Salardi, S.; Cacciari, E.; Menegatti, M.; Landi, F.; Mazzanti, L.; Stella, F.A.; Pirazzoli, P.; Vaira, D. Helicobacter pylori and type 1 diabetes mellitus in children. Journal of pediatric gastroenterology and nutrition 1999, 28, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Toporowska-Kowalska, E.; Wasowska-Królikowska, K.; Szadkowska, A.; Bodalski, J. [Helicobacter pylori infection and its metabolic consequences in children and adolescents with type 1 diabetes mellitus]. Medycyna wieku rozwojowego 2007, 11, 103–108. [Google Scholar] [PubMed]
- Candelli, M.; Rigante, D.; Marietti, G.; Nista, E.C.; Crea, F.; Bartolozzi, F.; Schiavino, A.; Pignataro, G.; Silveri, N.G.; Gasbarrini, G.; Gasbarrini, A. Helicobacter pylori, gastrointestinal symptoms, and metabolic control in young type 1 diabetes mellitus patients. Pediatrics 2003, 111, 800–803. [Google Scholar] [CrossRef] [PubMed]
- Crabtree, J.E. Role of cytokines in pathogenesis of Helicobacter pylori-induced mucosal damage. Digestive diseases and sciences 1998, 43, 46S–55S. [Google Scholar]
- Perdichizzi, G.; Bottari, M.; Pallio, S.; Fera, M.T.; Carbone, M.; Barresi, G. Gastric infection by Helicobacter pylori and antral gastritis in hyperglycemic obese and in diabetic subjects. The new microbiologica 1996, 19, 149–154. [Google Scholar]
- Wang, F.; Liu, J.; Lv, Z. Association of Helicobacter pylori infection with diabetes mellitus and diabetic nephropathy: a meta-analysis of 39 studies involving more than 20,000 participants. Scandinavian journal of infectious diseases 2013, 45, 930–938. [Google Scholar] [CrossRef]
- Esmaeili Dooki, M.R.; Alijanpour Aghamaleki, M.; Noushiravani, N.; Hosseini, S.R.; Moslemi, L.; Hajiahmadi, M.; Pournasrollah, M. Helicobacter pylori infection and type 1 diabetes mellitus in children. Journal of diabetes and metabolic disorders 2020, 19, 243–247. [Google Scholar] [CrossRef]
- Senturk, O.; Canturk, Z.; Cetinarslan, B.; Ercin, C.; Hulagu, S.; Canturk, N.Z. Prevalence and comparisons of five different diagnostic methods for Helicobacter pylori in diabetic patients. Endocrine research 2001, 27, 179–189. [Google Scholar] [CrossRef]
- Pickup, J.C.; Day, C.; Bailey, C.J.; Samuel, A.; Chusney, G.D.; Garland, H.O.; Hamilton, K.; Balment, R.J. Plasma sialic acid in animal models of diabetes mellitus: evidence for modulation of sialic acid concentrations by insulin deficiency. Life sciences 1995, 57, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Valkonen, K.H.; Ringner, M.; Ljungh, A.; Wadström, T. High-affinity binding of laminin by Helicobacter pylori: evidence for a lectin-like interaction. FEMS immunology and medical microbiology 1993, 7, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Bener, A.; Micallef, R.; Afifi, M.; Derbala, M.; Al-Mulla, H.M.; Usmani, M.A. Association between type 2 diabetes mellitus and Helicobacter pylori infection. The Turkish journal of gastroenterology: the official journal of Turkish Society of Gastroenterology 2007, 18, 225–229. [Google Scholar] [PubMed]
- Manco, M.; Putignani, L.; Bottazzo, G.F. Gut microbiota, lipopolysaccharides, and innate immunity in the pathogenesis of obesity and cardiovascular risk. Endocrine reviews 2010, 31, 817–844. [Google Scholar] [CrossRef] [PubMed]
- Man, S.; Ma, Y.; Jin, C.; Lv, J.; Tong, M.; Wang, B.; Li, L.; Ning, Y. Association between Helicobacter pylori infection and diabetes: A cross-sectional study in China. Journal of diabetes research 2020, 2020, 7201379. [Google Scholar] [CrossRef]
- Okuda, M.; Lin, Y.; Kikuchi, S. Helicobacter pylori infection in children and adolescents. Advances in experimental medicine and biology 2019, 1149, 107–120. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the systematic literature review.
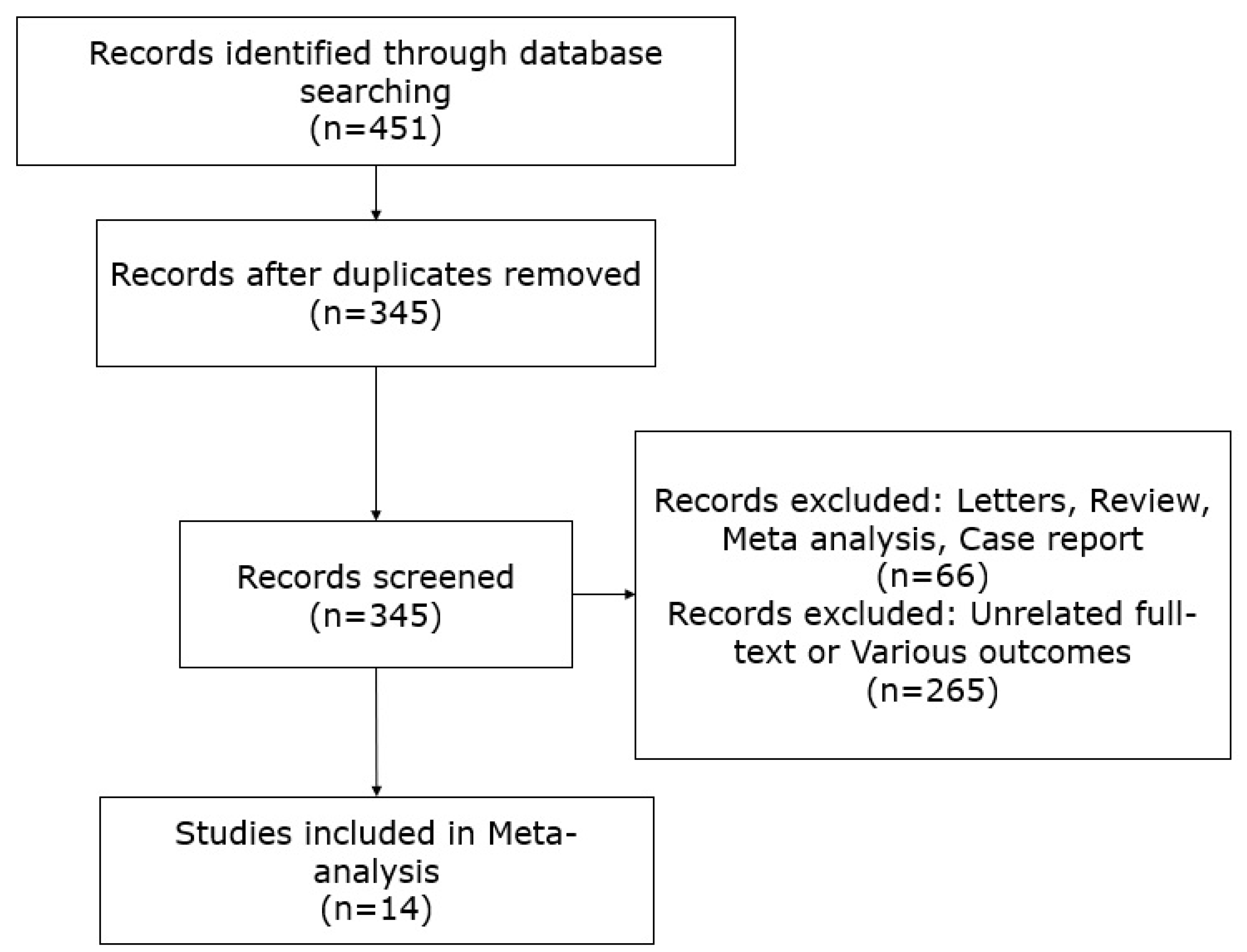
Figure 2.
Funnel plot analysis of H. pylori infection and type 1 diabetes mellitus.
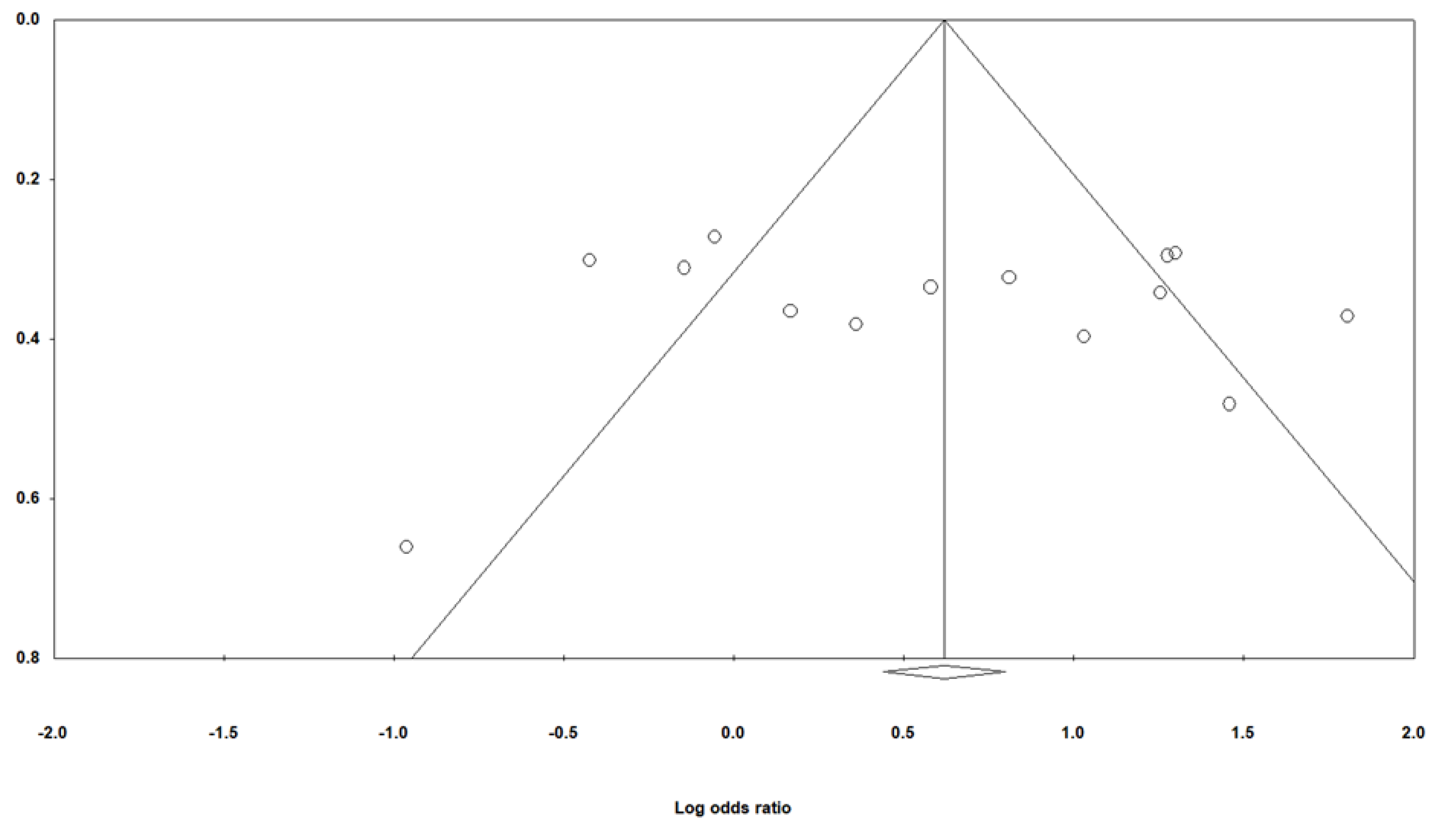
Figure 3.
Correlation analysis of H. pylori infection and type 1 diabetes mellitus.
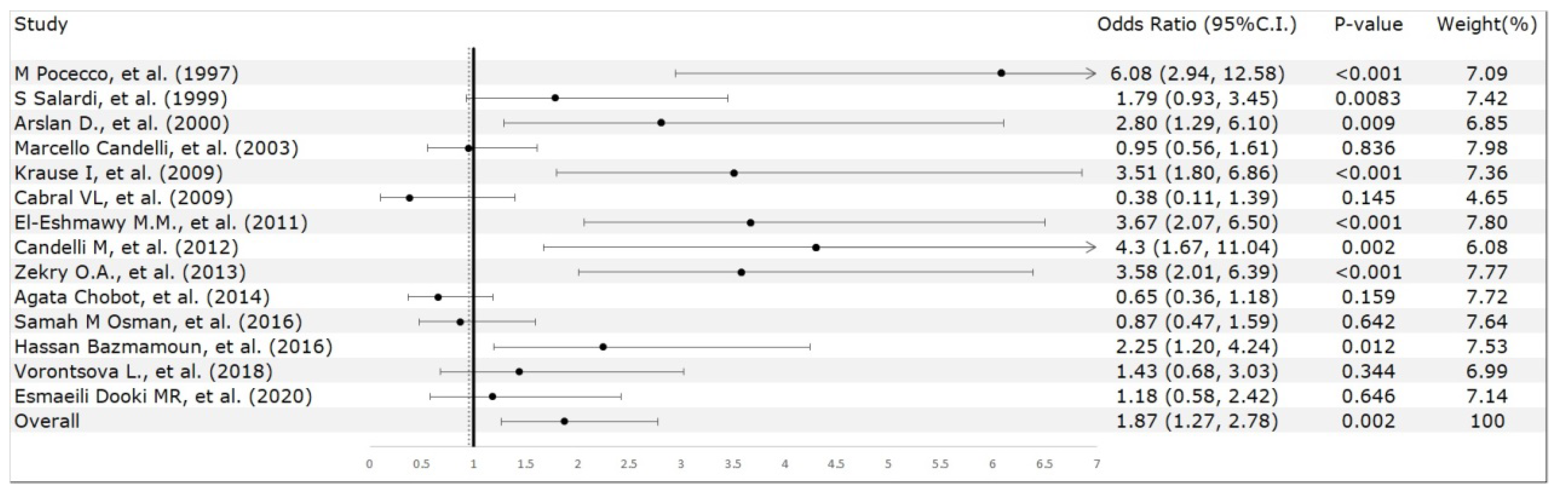
Figure 4.
Correlation analysis of H. pylori infection and diagnostic age.
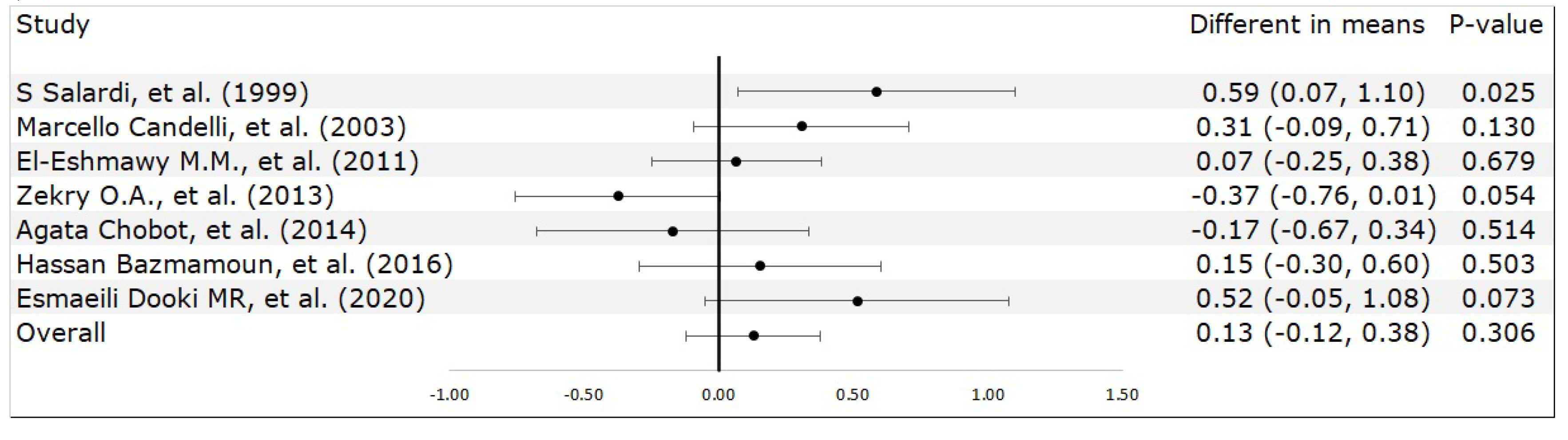
Figure 5.
Correlation analysis of H. pylori infection and hemoglobin A1c levels.

Figure 6.
Correlation analysis of H. pylori infection and diabetes duration.
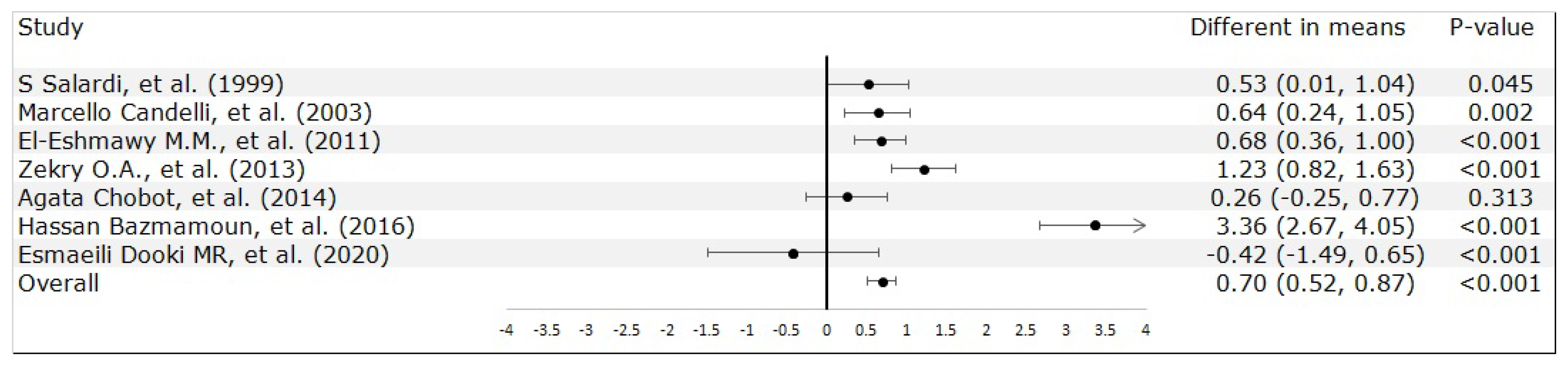

Table 1.
Primary characteristics of the included studies and the association between H. pylori infection and diabetes.
Table 1.
Primary characteristics of the included studies and the association between H. pylori infection and diabetes.
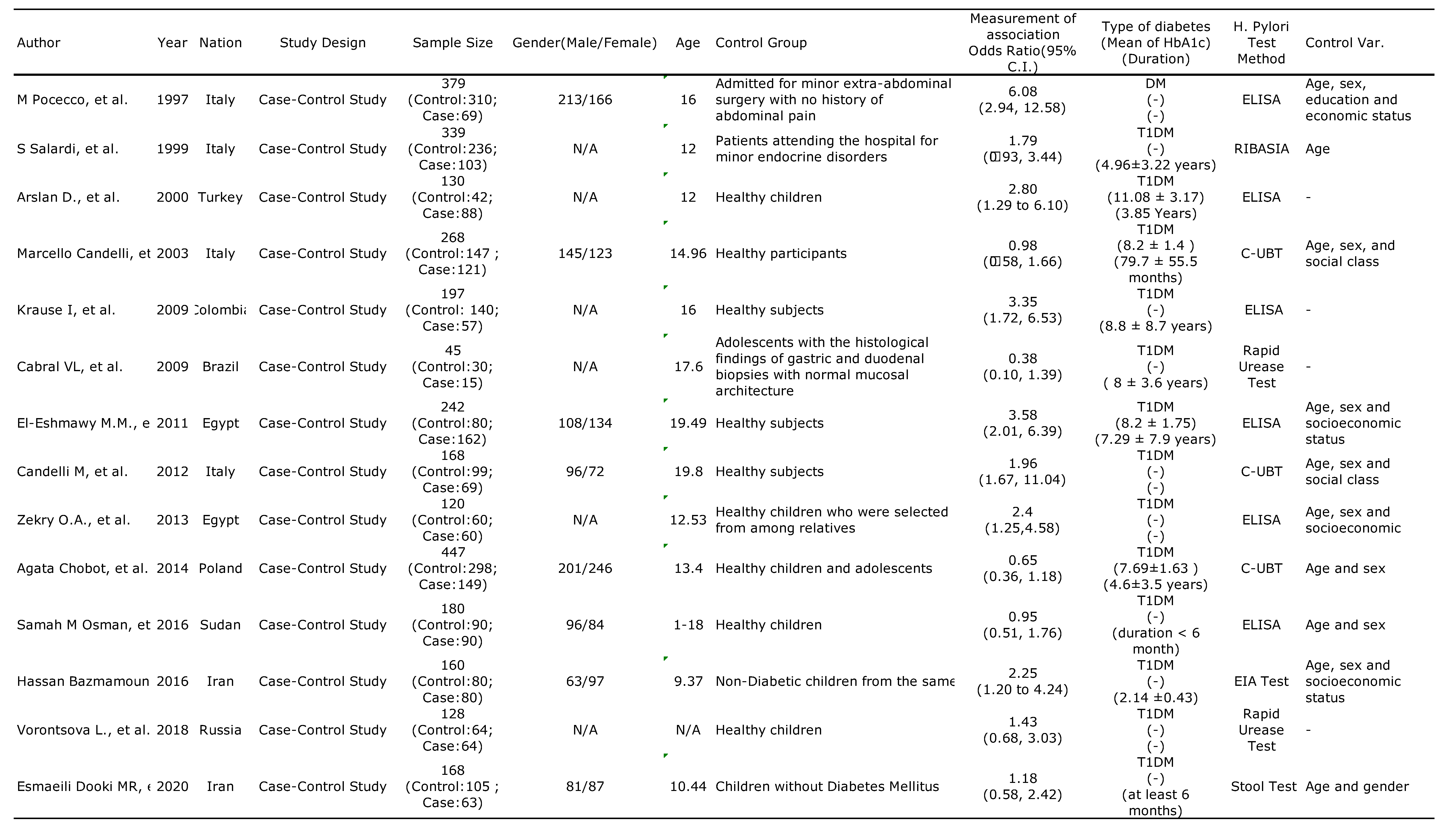
Table 2.
Characteristics of patients with diabetes.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



