
Submitted:
27 July 2023
Posted:
28 July 2023
You are already at the latest version
Abstract
The osteoarthritis (OA), the main cause of disability, is a chronic condition that most frequently affects older adults. As the population ages, the cost of treatment is placing pressure on the healthcare budget. As a result, it is imperative to evaluate the medicines' cost-effectiveness and the influence they have on health resource allocation. Hence, our study aims to summarize the cost and outcome of utilizing glucosamine in OA treatment. Authentic databases like Medline, Cochrane, and Scopus were adopted for the identification process up until July 2023. Our primary inclusion criteria centered on the economic evaluation of Glucosamine in OA treatments with provided the incremental cost-effectiveness ratio (ICER) at least. The Quality of Health Economic Studies (QHES) instrument was applied to grade the quality of the studies. A total of 7 qualified studies were selected and discussed the cost-effectiveness of glucosamine with or without other formulations. All of them demonstrated that glucosamine was cost-effective. There was an in-creasement of QALY when incorporating Glucosamine into conventional care. Moreover, Crystalline Glucosamine Sulfate (pCGS) was more cost-effective than the Other Formulations of Glucosamine (OFG). In overall, utilizing pCGS was more beneficial than OFG in terms both of cost and quality of life.
Keywords:
economic evaluation
; cost-effectiveness
; glucosamine
; osteoarthritis
; systematic review
1. Introduction
Due to its growing prevalence in the present and the future, osteoarthritis (OA) poses a challenge to the healthcare budget. This chronic state of illness, OA, is characterized by degradation of cartilage in joints, causing bones to rub against one another, which ultimately leads to pain, stiffness, edema, disability and thus has a detrimental impact on patient’s quality of life [1−4]. The current global prevalence of osteoarthritis (OA) is more than 7% (528 million people); this rate is even higher and reaches 14% in countries with aging populations and established market economies [3,5]. The global prevalence of OA tends to increase by 48% from 1990 to 2019 in different geographical regions. This rate will continue to increase in the near future in regions with aging populations and established market economies such as Europe, North America [5−11]. For example, the prevalence of osteoarthritis of the knee and hip is highest in North America (5,924 per 100,000 individuals), followed by North Africa, then the Middle East (4,610 per 100,000), then Australia (4,595 per 100,000)[5,6,12]. In contrast, rates of osteoarthritis are much lower in East Sub-Saharan Africa (2,568 per 100,000), Central Sub-Saharan Africa (2,633 per 100,000) and Western Sub-Saharan Africa (2,678 per 100,000) [5,6,12].
Osteoarthritis is the 15th leading cause of disability, leading to years of disability (YLD) for patients with osteoarthritis affecting YLD worldwide, accounting for 2.2% of total global YLD (18.9 million in 2019)[5]. Although osteoarthritis can occur in any joint in the human body, the knee joint is the most frequent, accounting for 365 million cases worldwide and 61% of YLDs lost to knee osteoarthritis, followed by hand osteoarthritis (142 million cases and 24% YLD osteoarthritis), then hip osteoarthritis (33 million and 5.5% of OA YLDs)[5,6,13,14]. As demonstrated by the Vietnam Musculoskeletal Association, the rate of arthritis in people over 35 years old is about 30%, people over 65 years old is about 60% and 85% of people over 80 years old [15]. Based on a study in 2003, the proportion of musculoskeletal pain in an urban population in Vietnam was 14.5% and OA was the most common form of arthritis [16].
Nowadays, the quantity of people with OA is continuing to increase and not only affects the elderly but also many young people. Factors considered to be risk factors for osteoarthritis include age, obesity, sex, malformations, previous joint damage, or employment with a high risk of joint injury[1,7−14,17,18]. Therefore, when the more risk factors you have, the more likely you are to develop osteoarthritis. Obesity in particular is a potential risk factor for developing OA [19]. For example, obesity triples the risk of knee osteoarthritis [18]. In addition, 35% of men and 62% of women reported having knee pain on their own16. According to statistics published by the Dutch Institute for Public Health, the prevalence of knee OA in people 55 and older was 15.6% for male and 30.5% for female [20]. These results demonstrated that women are more likely to get OA than men. Besides, the result of another study showed the range for the prevalence of OA is 20.5% to 68.0% and in several Asian countries, the majority of the Asian inhabitants reported having knee OA in a range of 13.1% to 71.1%[8,21]. Age, sex specifically female, and obesity are risk variables that have been linked to OA. Other significant risk factors for OA included osteoporosis, higher body mass density, muscle function, ethnicity and race, genetics, low levels of education, family history, smoking, lifestyle, and environmental variables.
The OA is a significant public health issue with few viable medical treatments[1−4,13,22,23]. Moreover, it also has an influence on the mortality rate, incidence rate, and medical costs[3,4,13,23]. According to records from 1995, OA was reported to affect more than 1.2 million Australians and to cause severe damage to quality of life and expenses[24]. The cost was pegged up to 1090 million dollars up until 2001 [25]. Globally, osteoarthritis was present in 22.9% of adults over the age of 40 [26]. The number of people with OA is gradually rising as the world's population is getting older [15]. Thus, the economic burden of OA, which comprises of direct and indirect medical costs, is believed to be substantial. The direct costs of osteoarthritis treatment can be as high as 1–2.5% of Gross National Product in countries such as the US, UK, Canada and Australia [27]. Numerous researches have pointed out the degree of economic burden caused by osteoarthritis, for instance, a review by Salmon et al. in 2016 addressed the economic impacts of lower extremity (knee and hip) degenerative joint disease, both in terms of direct and indirect health costs, in different countries of the world from the point of view of of payers and society [28]. Average annual direct medical costs per osteoarthritis patient in countries in Asia, Europe, North America, and Oceania. Around the world, the average cost of osteoarthritis treatment is $13,600. In other regions, these costs range from $700-15,600. The highest annual treatment costs are in North America ($14,000), followed by OA treatment costs in Asia ($8,900), Europe ($1,400) and Australia (Oceania). ($900). The global average annual indirect cost of treatment is $6300, where the indirect cost per patient ranges from $300–17700. Similar to trends with direct costs, countries in North America have the highest average annual indirect costs ($6,500), while these costs are lower in Europe ($5,500) and Asia ($2,300). Indirect costs in Oceania are not reported [28].
In 2013 in the United States, osteoarthritis was the second most expensive medical expenditure of all diseases treated in US hospitals, accounting for 4.3% ($18.4 billion) in total hospitalization costs ($415 billion) [29]. The direct medical costs of osteoarthritis treatment in the United States are estimated at $72 billion (using median cost data from 2008 to 2011) [30]. Although health care costs are much greater in the United States than in other high-income countries, the direct costs of osteoarthritis treatment in those other countries are still substantial [31]. In Australia, for example, direct medical costs for osteoarthritis were estimated at $1.7 billion in 2015, about 2.4% of the costs for arthritis in the United States, despite the population about 7.3% of the population in the United States (2015). In France, the estimated direct cost of OA was €1.64 billion in 2001 [32] and the burden of arthritis was 69.9 million people in the United States in the same time [33,34]. The indirect costs of treating osteoarthritis are also significant. Published estimates of the indirect costs of osteoarthritis in different established market economies include Spain ($1.2 billion), United Kingdom ($6.5 billion), billion) and the United States ($12.7 billion)[35,36].
To reduce symptoms and enhance patients' quality of life, numerous scientific organizations have offered therapeutic options for osteoarthritis, including pharmacological and non-pharmacological therapies[37,38]. In accordance with the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) recommendations, it was advisable to utilize the symptomatic slow-acting drugs (SYSADOAs) from the beginning in OA pharmacological treatment [39]. SYSADOAs groups included many other compounds such as Glucosamine, Chondroitin, Diacerein, and avocado soybean unsaponifiable [39]. For nearly 40 years, glucosamine and chondroitin sulfate (CS), both components of articular cartilage's extracellular matrix, have been utilized medicinally [40]. These substances were used widely in formulations of both pharmaceutical products and cosmetics. It should be emphasized that not all of these substances were clinically proven to be beneficial, though they were claimed to portray therapeutic effects [39]. In the process of investigating glucosamine products, ESCEO highlights that only patented crystalline glucosamine sulfate (pCGS) should be used for prescription-level medications, other formulations of Glucosamine are not recommended [39]. Glucosamine sulfate is one of the alternative solutions in mild-to-moderate OA patients [15]. The assessment of glucosamine's cost-effectiveness from scientific studies mainly concentrated on comparing cost-effectiveness among various formulations or with other therapies, whereas overall reviews about financial efficacy of glucosamine were very limited. In addition, the management agencies relied on pharmacoeconomic-related data to determine the type of resources allocation that would produce the greatest efficacy, hence these evaluations are crucial for setting price limits and reimbursement [41]. Furthermore, since we cannot access the personal data of each patient due to technical, legal issues as well as patient consent, we conduct our assessment based on scientific data.
In the situation where there is an absence of published scientific evidence for the cost-effectiveness of Glucosamine, researchers will have to rely heavily on published research papers and unpublished presentations available by academic or field-related researchers. The primary goal of this study is to evaluate the economic efficacy of Glucosamine in real-world for the treatment of osteoarthritis and to summarize the main findings.
2. Materials and Methods
2.1. Search strategy
The searching process started on 25th October 2022, we searched on highly authentic databases such as Medline (using PubMed), Scopus (using www.scopus.com), and Cochrance (using www.cochrance.org) to find results about health-related quality of life published from inception to 3th July, 2023. Our study aimed to identify all of relevant articles that provide detail information about glucosamine’s economic evaluation, in order to compare these studies together.
The investigation strategy was accessed by using specific keywords for systematic review, searching phrases for measurement features, and a verified methodological search filter for measurement properties [42]. References section of each article was also examined for further relevant studies. Other techniques are also used in the search process such as connecting keywords by Boolean formula (AND, OR), selecting the specified field (title, author, summary, year or all fields,…), checking duplicates, reviewing articles conformity against inclusion criteria. The complete syntax used in this study is: (((((Rheumatoid arthritis) OR (RA)) OR ((osteoarthritis) OR (OA))) AND (glucosamin*))) AND (cost[MeSH Terms]).
2.2. Selection criteria
The inclusion criteria were focused on publications that contained following requirements:
- (1)
- Interventions must use glucosamine as the non-combined formulation at least
- (2)
- English--written articles about cost-effectiveness analysis or any type of economic evaluation
- (3)
- Topic about osteoarthritis therapy with viable duration
- (4)
- Specific information about ICER value at least
- (5)
- Clear conclusion whether Glucosamine was cost-effective or not
Reports that failed to meet the following conditions will be exlcuded:
- (1)
- Studies that combined Glucosamine with other compounds
- (2)
- Not available in English language
- (3)
- Not talk about osteoarthritis treatment, not focus on glucosamine
- (4)
- Not about osteoarthritis treatment
- (5)
- Unclear statement or lack informaton about ICER
2.3. Data extraction
Our study placed most interest on ICER as primary outcome measure. On the basic concept, the incremental cost-effectiveness ratio (ICER) is a specific value that can be expressed by as the price for each quality-adjusted life-year (QALY) gained [43]. To be more specified, one QALY equals to one year of no sickness [43]. On the other hand, the following information such as: first author and year publication, OA subjects, intervention, country, perspective, type of model and tool used, time frame of the study, and main assumptions were also extracted as high-yield data in the examination. Figure 1 shows the entire search process based on abstract and inclusion criteria.
2.4. Quality assessment of selected articles
For the purpose of evaluating the included studies' quality, we employed the Quality of Health Economic Studies (QHES) instrument. The 16 questions on this application were developed in order to examine adequate methodologies, reliable data, and thorough findings in each CEA report [44]. By summing up all the points for "yes" answers to the questions, the quality score is obtained [44]. The score can vary from 0 to 100. Reports with total score <75 were deemed to be of “low” quality, while those with a final value of >75 may qualify as being “high” quality.
3. Results
3.1. Study selection process
On 25th October 2022, the selection process was carried out. We gathered articles from electronic databases while adhering to the established syntax. The searching range period was conducted until July 2023. As a result, 63 articles from PubMed, 35 articles from Cochrane, and 147 articles Scopus were discovered. After that, we eliminated duplicates, remaining 94 documents. Then, in comparison to our criteria for selection, 83 publications did not provide sufficient information about expenses, and 4 papers did not specifically address glucosamine; these were all discarded. Ultimately, a total of 7 studies met the requirements for inclusion. Figure 1 depicts an overview of the selection procedure.
Using keywords “rheumatoid arthritis”, “osteoarthritis”, “glucosamine”, “cost”, we gathered articles from extremely reliable databases that adhered to the established syntax. In total, 245 articles were found including 63 articles from PubMed, 35 from Cochrane, and 147 Scopus. Four investigators divided into two groups to remove duplicate articles and review abstracts and titles of all studies. Articles that are not related to the topic will be disqualified. When there is any disagreement, the Teams will conduct discussion and select based on the criteria of the research paper. Based on this working principle, we have eliminated 53 duplicate articles. Then, in comparison to our criteria for selection, 83 publications did not provide sufficient information about expenses, and 4 papers did not specifically address glucosamine; these were all discarded. After the selection process, a total of 7 studies met the requirements for inclusion. Figure 1 depicts an overview of the selection procedure.
3.2. Characteristic of included studies
As summarized in Table 1, reports tended to examine distinct kinds of glucosamine (pCGS or other form of glucosamine) or to compare different therapies such as analgesics, whereas the financial assessment takes minority position. Additionally, the time of publications lasted from 2004 to 2023. Our subjects included patients diagnosed with Osteoarthritis, with two of the studies were knee-focused.
Table 2a and Table 2b displayed the primary characteristics of the studies that were included. Noting that aging was a major risk factor for osteoarthritis disease, it is important to be aware that the subjects in the published studies were mostly OA patients above 40 years old. As can be observed, the majority of the studies are conducted in industrialized nations such as the UK, Germany, and Spain. The sole country in Southeast Asia is Thailand.
On the other hand, just 4 out of 7 papers in our research—which included societal, health care, and national health care systems—mentioned the perspective of payers. In addition, a variety of models were applied to determine or convert to utility scores. According to research by Bruyère et al. [45−47], utility score and QALYs were estimated from data of published clinical trials using Grootendorst's linear regression model based on WOMAC, basic demographic and severity of OA. The Markov model or a decision tree mathematical model were employed in the other investigations' approaches. Except for Segal et al.'s study, which adopted cost-utility analysis (CUA), the majority of research papers we chose to highlight used cost-effectiveness analysis (CEA). It should be noted that only 3/7 studies presented information about the time horizon. While Scholtissen et al. [41] reported a 6-month time horizon, Luksameesate et al.[15] and Black et al.[48] both documented life time horizons.
Moreover, the length of studies can vary, with at least 6 months and at most 3 years. the increased cost-effectiveness ratio (ICER) was extracted from most of the papers as the main outcome. It can be understood as a measure of disease burden which was considered as a benchmark to evaluate and compare these economic values. The sensitivity analysis was also performed in certain studies. Their findings demonstrates the influence of utility scores, discount rates.
It can be observed that studies take place over a long period of time and with different time periods, so they need to be adjusted to the same time period and the same units of comparison. Therefore, applying the appropriate discount rates is considered to be critical to bring the values back to the present time. The discount rate ranges from 3% to 5%. The discount rate specified in the Luksameesate et al.[15] study was 3%, as recommended by the Guideline for Health Technology Assessment. Discount rates in the Segal et al.[49] study by Black et al.[48] were 3.5% and 5%, respectively.

Table 2.
a. Characteristic of selected studies. b. Characteristic of selected studies (continue).
| a. Characteristic of selected studies | |||||||
|---|---|---|---|---|---|---|---|
| No. | Study, year, and country | Subjects | Intervention | Perspective | Method | Time horizon | Costs of Glucosamine |
| 1 | Bruyère et al.[45], 2023, Thailand | OA patients | pCGS vs. OFG vs. Placebo | Healthcare | CEA | - |
$27.78/powder pCGS, $27.22/tablet pCGS. ;$14.61/powder OFG, $10.80/tablet OFG. |
| 2 | Luksameesate et al.[15], 2022, Thailand | Patients ≥ 45 years old with mild-to-moderate pain ;and no comorbidities |
pCGS combined with etoricoxib vs ;Glucosamine monotherapy |
Societal | CEA | Lifetime | - |
| 3 | Bruyère et al.[46], 2021, Germany | OA patients ;> 40 years old |
pCGS vs. OFG | Healthcare | CEA | - | - |
| 4 | Bruyère et al.[47], 2019, | OA patients ;> 40 years old |
pCGS vs. OFG | Healthcare | CEA | - | 0.9 €/day for pCGS, ;0.55 €/day for OFG |
| 5 | Scholtissen et al.[41], 2010 Spain, Portugal | Knee OA ;patients with average age 63 years old |
GS ;vs Paracetamol vs. placebo |
Healthcare | CEA | 6 months | - |
| 6 | Black et al.[48], 2009, UK | Knee OA ;patients |
GS/GH vs. chondroitin sufate vs. GS and chondroitin | National healthcare system | CEA | Lifetime | £221 (1-year) |
| 7 | Segal et al.[49], 2004, Australia | OA patients | Interventions for arthritis ;including Glucosamine |
National healthcare system | CUA | - | $180 (1-year) |
| b. Characteristic of selected studies (continue) | |||||||
| No. | Study, year, and country | Subjects | Intervention | Model type | Duration | Sensitivity analysis |
Discount ;rate |
| 1 | Bruyère et al.[45], 2023, Thailand | OA patients | pCGS vs. OFG vs. Placebo | Grootendorst ;model |
6 months | - | - |
| 2 | Luksameesate et al.[15], 2022, Thailand | Patients ≥ 45 years old with mild-to-moderate pain ;and no comorbidities |
pCGS combined with etoricoxib vs ;Glucosamine monotherapy |
Markov model | 6 months | One-way; PSA | 3% |
| 3 | Bruyère et al.[46], 2021, Germany | OA patients ;> 40 years old |
pCGS vs. OFG | Grootendorst ;model |
3 years | - | - |
| 4 | Bruyère et al.[47], 2019, | OA patients ;> 40 years old |
pCGS vs. OFG | Grootendorst ;model |
3 years | One-way | - |
| 5 | Scholtissen et al.[41], 2010 Spain, Portugal | Knee OA patients with average age 63 years old | GS vs. Paracetamol vs. placebo | Mathematical – decision model | 6 months | PSA | - |
| 6 | Black et al.[48], 2009, UK | OA patients | Interventions for OA ;including Glucosamine |
Mathematical – decision model | 1 year | - | 5% |
| 7 | Segal et al.[49], 2004, Australia | Knee OA ;patients |
GS sulphate/hydrochloride vs. chondroitin sulphate vs. GS and chondroitin | Cohort model | 1 year | One-way | 3.5% |
OA: osteoarthritis; pCGS: Crystalline Glucosamine Sulfate; OFG: Other Formulations of Glucosamine; PSA: probabilistic sensitivity analysis.
3.3. Quality assessment by QHES instrument
As described in Table S1 (see supplementary material), the QHES scores in 7 studies about Glucosamine in OA treatment ranged from 88 to 95, with an average of 90.6. All 7 studies were scored above 75 which makes these reports can be considered as high-quality studies. Every study was fully written with clear manner, clear objectives. Besides, the results, study method, and the primary outcome are clear and justified. These articles also clearly described unit costs, outcome and the incremental analysis was performed between alternatives for resources and costs. Only 14% of them included the perspective of the analysis while others didn’t. Approximately 29% of these studies were justification given for the discount rate. All of them have a statement disclosing the source of funding for the study.
3.4. Keypoint data related to cost-effectiveness
According to Table 3, in Bruyère et al. [45−47] study 2019, 2021, 2023, a slight increase in QALY was observed over the periods of 3 months, 6 months, and 36 months. In Bruyère et al.,[46] 2021 study, the cost of pCGS in 3 months, 6 months, 36 months was 77.0964 €, 183.0003 €, 2785.2712 €, respectively. In Bruyère et al.,2023[45] study, ICER of pCGS and OFG after using in 3 months was 3,165 USD/QALY and 32,400 USD/QALY, after 6 months of pCGS is 3,069 USD/QALY, meanwhile placebo was better than OFG. The result shows that the use of pCGS is economically viable compared to the threshold of USD 3,260/QALY, while OFG is not economically efficient compared to the threshold. All three Bruyère et al.[45−47] studies suggested that pCGS was more cost-effective than OFG. Early addition of pCGS to the standard care increased 0.87 QALY. Adding pCGS increased efficiency and thus saved money. In Scholtissen's study[41], ICER of Glucosamine compared with paracetamol and placebo was 1376€/QALY, 3617.47€/QALY, respectively. When compared with the threshold of €20,000/QALY, it was found to be more economically viable than using paracetamol. In study of Segal et al.[49] study, after using Glucosamine, the QALY gain was 0.052 and cost was 180.024 $. Glucosamine was more economical than NSAIDs, with ICER $3,462/QALY. Adding Glucosamine to existing care costed 2,346.85£. It has also been shown to be economically viable with ICER 21,335£/QALY compared to the willingness to pay threshold of 22,000£/QALY.
ICER = ΔCost/ΔQALY (incremental costs/incremental QALY gained)
4. Discussion
To delay disease progression and control symptoms efficiently, patients could access pharmacological treatments such as: Acetaminophen, NSAIDs, SYSADOA, intra-articular corticosteroids, or proceed surgical option with total knee arthroplasty (TKA). Statistical approaches for CEA have been developed, and a measure known as the incremental cost-effectiveness ratio (ICER) has gained widespread acceptance among researchers and governments[50]. The ICER is calculated by dividing the cost difference between two strategies by the difference in efficacy. This one-dimensional summary metric assesses the trade-offs between patient outcomes gained and resources spent. It can be defined as the cost of acquiring one extra unit of efficacy. The ICER threshold, typically denoted by, can be interpreted as the maximum amount society is willing to spend for an additional unit of healthcare benefit[51]. Among those medications, glucosamine was proven to slow down development of sickness[52,53] and to be cost-effective as $5,000/QALY25. In addition, our main findings showed that interventions utilizing patented crystalline glucosamine sulfate (pCGS) were more cost-effective than those using alternative glucosamine formulations. Glucosamine sulfate was found to have better expense management than paracetamol in a cost-effectiveness research that comparing it with paracetamol[41]. It can be noticed that cost-effectiveness analysis of Glucosamine was published continuously from 2019-2023. Studies can vary, comparing cost-effectiveness between forms of glucosamine, or between forms of Glucosamine, or paracetamol, NSAIDs, the combination of Glucosamine with other interventions. This shows the potential of using Glucosamine in OA patients. Conducting research from a health care perspective helps governments evaluate and incorporate Glucosamine into government policies.
Most papers required estimation of cost-utility in order to compute quality-adjusted life years (QALY) since there was no direct assessment of cost-utility value or QALY, hence costs would be also derived from accessible data sources. Following Grootendorst's formulation, which was based on age, the number of years since an OA diagnosis, and three separate WOMAC sub-scores (Western Ontario and McMaster University Osteoarthritis Index), health-related cost-utility was calculated. Then, ICER was computed and reviewed. For instance, investigations in 2019 and 2021 found that application of glucosamine sulfate was much more economical than the other formulations after assessing 10 articles using the WOMAC scale (4 studies using pCGS and 6 using non-pCGS formulations)[46,47]. The average ICER of 3 months, 6 months, and 3 years were calculated to be 4,489 €/QALY; 5,347.2 €/QALY; 9,983 €/QALY, respectively[46].
From what we have comprehended so far, there was a lack of data about time horizon in our included studies. According to one report evaluating the role of time horizon in CEA, the author concluded that the ICER ratio value strongly depended on the extent of time horizon using[54]. Its findings revealed that most CEAs were more cost-effective as the time horizon grew[54]. Since osteoarthritis is a chronic condition, a lifetime horizon should be considered to ensure that all costs and benefits are adequately captured. Sensitivity analysis was included in CEA to find values that affect the results. It also shows how reliable it is. It is used to check the results of the model when changing one of the parameters. Sensitivity analysis almost depends on utility score, the cost. Some of them depend on the discount rate, life years lost. In Luksamees et al.[15] study, they gave parameters including the cost of crystalline glucosamine sulfate, cost of TKA, transition probability of diclofenac plus PPI, transition probability of TA injection, transition probability of TKA, utility of knee OA pain. They found that the highest impact is the utility of moderate pain when changing values between 0.35 and 0.77. The cost of TKA is more sensitive than the cost-effectiveness ratio when the cost-effectiveness ratio changes between 78,533 THB and 79,316 THB.
According to Scholtissen et al.[41], the average total costs per patient that used glucosamine was 38.88€, meanwhile paracetamol was €48.56 and placebo was 2.77€. In another study, the estimated mean cost per patient using glucosamine was $180, people using topical capsaicin was $236, COX-2 NSAIDs such as celecoxib was nearly $500 per year[49]. Based on other research, standard treatment plus using glucosamine only cost about 150,000 Thai Baht but standard treatment plus etoricoxib cost up to approximately 420,000 Thai Baht [15]. These results show that the amount needed to pay for when using other medications is much higher than using Glucosamine sulfate.
On the other hand, the study by Luksameesate et al.[15], 2022 in Thailand has also once again validated the intake of pCGS in the standard knee OA treatment was regarded as the sufficient alternative to improve patients illness. As a result, early initiation of pCGS would be less costly and more advantageous than delayed treatment. In addition, this paper also concluded that the combination of pCGS and Etoricoxib in the treatment of knee OA is cost-effective at the willingness-to-pay threshold in Thailand but the combination was only authentic within the country[15]. WTP is based on customer preferences, this range could be utilized to establish a criterion that is generally accepted [55]. The World Health Organization (WHO) recommends a threshold of one to three times the GDP per capita for the cost of investing in one disability-adjusted life year (DALY), which is widely known and frequently mentioned when considering CE standards. The former evaluation assumes that if an intervention can yield one QALY per year for less than the GDP per capita, the subsequent value-added will outweigh the cost of the investment[56,57]. Interventions with an ICER below the accepted ceiling threshold could then be considered as cost-effective.
One study in 2014 mentioned that utilizing glucosamine demonstrated therapeutic effects along with reasonable expenses , but still there haven't been any studies exclusively focused on the economic aspects or cost-related examination for this intervention so far [25]. Thus, our finding proposes a framework for subsequent publications. Also, another report in 2010 concluded that glucosamine sulfate was prioritized as long-term analgesics because of its fair affordability and appropriate safety profile as shown by ICER analysis[41].
Furthermore, the clinical effects of pCGS in controlling OA symptoms have been demonstrated to be remarkably effective in improving pain and functional impairment[39]. Previously, A review of 78 outpatients with knee OA revealed in 2012 that the administration of Glucosamine Sulfate was less money-consuming and greater in efficacy than Glucosamine Hydrochloride[58]. Ultimately, it can be said that the role and cost-effectiveness of Glucosamine Sulfate in the treatment of osteoarthritis has been further emphasized and defined.
However, we must admit there was drawbacks in our research. Firstly, in our system review, the number of studies which we collected are not enough for strengthening cost-effective of Glucosamine, specifically there were 7 studies in total. Secondly, we found some study which did long time ago. Therefore, data may be limited to reflect the present. Lastly, seven studies were done in the UK, Thailand, and some European countries such as Germany, Spain. So, data of cost-effective of Glucosamine are limited.
5. Conclusions
pCGS is cost-effective in the treatment of mild and moderate osteoarthritis. More severe cases of osteoarthritis were not cost-effective. Among different kinds of glucosamine, pCGS was highly cost-effective than OFG. QALY gain was observed when adding glucosamine into conventional treatment.
6. Future Directions
The cost-effectiveness of glucosamine use has been shown to be ICER in the short-term. However, since osteoarthritis is a chronic disease, patients with osteoarthritis will take medication for most of their lives if no alternative therapy is available. Therefore, future research should focus on performing long-term studies on the costs, health outcome and ICER of glucosamine to assess the effectiveness of this use more accurately. Moreover, further researches are still needed to be performed in order to evaluate the actual cost-effectiveness of Glucosamine use in Vietnam and other countries to provide evidences supporting policies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1. Quality assessment of selected reports based on QHES Instrument.
Author Contributions
Conceptualization, Vo, N.X. and Bui, T.T.; methodology, Vo, N.X.; software, Che, U.T.T. and Ngo, T.T.T.; validation, Vo, N.X. and Bui, T.T.; formal analysis, Che, U.T.T. and Ngo, T.T.T.; investigation, Vo, N.X.; resources, Le, N.N.H.; Chu, T.D.P.; Pham, H.L.; Dinh, K.X.A.; Che, U.T.T. and Ngo, T.T.T.; data curation, Le, N.N.H.; Chu, T.D.P.; Pham, H.L.; Dinh, K.X.A.; Che, U.T.T. and Ngo, T.T.T.; writing—original draft preparation, Che, U.T.T.; Ngo, T.T.T. and Bui, T.T.; writing—review and editing, Vo, N.X.; Pham, H.L.; Dinh, K.X.A. and Bui, T.T.; visualization, Vo, N.X. and Bui, T.T.; supervision, Vo, N.X.; project administration, Vo, N.X. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data was collected in PubMed, Scopus and Cochrane database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Litwic, A.; Edwards, M.H.; Dennison, E.M.; Cooper, C. Epidemiology and burden of osteoarthritis. Br Med Bull 2013, 105, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Hutton, C.W. Osteoarthritis: the cause not result of joint failure? Ann Rheum Dis 1989, 48, 958–961. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Institute_for_Health_Metrics_and_Evaluation. Global Burden of Disease Study 2019 (GBD 2019) Data Resources. Available online: https://ghdx.healthdata.org/gbd-2019 (accessed on 17 May 2023).
- Institute_for_Health_Metrics_and_Evaluation. Global Burden of Disease Study 2019 (GBD 2019) Results. Osteoarthritis-level 3 cause. Available online: https://www.healthdata.org/results/gbd_summaries/2019/osteoarthritis-level-3-cause#:~:text=Summary%20Osteoarthritis%20(OA)%20resulted%20in,%25%20of%20OA%20YLDs%2C%20respectively (accessed on 17 May 2023).
- Neogi, T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis Cartilage 2013, 21, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; Bridgett, L.; March, L.; Hoy, D.; Penserga, E.; Brooks, P. The epidemiology of osteoarthritis in Asia. Int J Rheum Dis 2011, 14, 113–121. [Google Scholar] [CrossRef]
- Anderson, L.A.; Goodman, R.A.; Holtzman, D.; Posner, S.F.; Northridge, M.E. Aging in the United States: opportunities and challenges for public health. Am J Public Health 2012, 102, 393–395. [Google Scholar] [CrossRef]
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: the challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef]
- Wortley, D.; An, J.Y.; Heshmati, A. Tackling the Challenge of the Aging Society: Detecting and Preventing Cognitive and Physical Decline through Games and Consumer Technologies. Healthc Inform Res 2017, 23, 87–93. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, regional and national burden of osteoarthritis 1990-2017: a systematic analysis of the Global Burden of Disease Study 2017. Ann Rheum Dis 2020, 79, 819–828. [Google Scholar] [CrossRef]
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Zhang, Y.; Jordan, J.M. Epidemiology of osteoarthritis. Clin Geriatr Med 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Luksameesate, P.; Tanavalee, A.; Taychakhoonavudh, S. An economic evaluation of knee osteoarthritis treatments in Thailand. Front Pharmacol 2022, 13, 926431. [Google Scholar] [CrossRef]
- Minh Hoa, T.T.; Darmawan, J.; Chen, S.L.; Van Hung, N.; Thi Nhi, C.; Ngoc An, T. Prevalence of the rheumatic diseases in urban Vietnam: a WHO-ILAR COPCORD study. J Rheumatol 2003, 30, 2252–2256. [Google Scholar]
- Garstang, S.V.; Stitik, T.P. Osteoarthritis: epidemiology, risk factors, and pathophysiology. Am J Phys Med Rehabil 2006, 85, S2–11. [Google Scholar] [CrossRef]
- Allen, K.D.; Golightly, Y.M. State of the evidence. Curr Opin Rheumatol 2015, 27, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Reyes, C.; Leyland, K.M.; Peat, G.; Cooper, C.; Arden, N.K.; Prieto-Alhambra, D. Association Between Overweight and Obesity and Risk of Clinically Diagnosed Knee, Hip, and Hand Osteoarthritis: A Population-Based Cohort Study. Arthritis Rheumatol 2016, 68, 1869–1875. [Google Scholar] [CrossRef]
- Litwic, A.; Edwards, M.; Dennison, E.; Cooper, C. Epidemiology and Burden of Osteoarthritis. Br Med Bull 2013, 105, 185–199. [Google Scholar] [CrossRef]
- Zamri, N.A.A.; Harith, S.; Yusoff, N.A.M.; Hassan, N.M.; Ong, Y.Q. Prevalence, Risk Factors and Primary Prevention of Osteoarthritis in Asia: A Scoping Review. Elderly Health Journal 2019, 5, 19–31. [Google Scholar] [CrossRef]
- Bijlsma, J.W.; Knahr, K. Strategies for the prevention and management of osteoarthritis of the hip and knee. Best Pract Res Clin Rheumatol 2007, 21, 59–76. [Google Scholar] [CrossRef]
- Andrianakos, A.A.; Kontelis, L.K.; Karamitsos, D.G.; Aslanidis, S.I.; Georgountzos, A.I.; Kaziolas, G.O.; Pantelidou, K.V.; Vafiadou, E.V.; Dantis, P.C.; Group, E.S. Prevalence of symptomatic knee, hand, and hip osteoarthritis in Greece. The ESORDIG study. J Rheumatol 2006, 33, 2507–2513. [Google Scholar] [PubMed]
- survey, A.N.h. Australian Bureau of Statistics: Canberra; 1995. [Google Scholar]
- Segal, L.; Day, S.E.; Chapman, A.B.; Osborne, R.H. Can we reduce disease burden from osteoarthritis? Med J Aust 2004, 180, S11–17. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29-30, 100587. [Google Scholar] [CrossRef] [PubMed]
- March, L.M.; Bachmeier, C.J. Economics of osteoarthritis: a global perspective. Baillieres Clin Rheumatol 1997, 11, 817–834. [Google Scholar] [CrossRef]
- Salmon, J.H.; Rat, A.C.; Sellam, J.; Michel, M.; Eschard, J.P.; Guillemin, F.; Jolly, D.; Fautrel, B. Economic impact of lower-limb osteoarthritis worldwide: a systematic review of cost-of-illness studies. Osteoarthritis Cartilage 2016, 24, 1500–1508. [Google Scholar] [CrossRef]
- Torio CM, Moore BJ. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs 2006.
- Yelin, E.; Weinstein, S.; King, T. The burden of musculoskeletal diseases in the United States. Semin Arthritis Rheum 2016, 46, 259–260. [Google Scholar] [CrossRef]
- Papanicolas, I.; Woskie, L.R.; Jha, A.K. Health Care Spending in the United States and Other High-Income Countries. JAMA 2018, 319, 1024–1039. [Google Scholar] [CrossRef]
- Le Pen, C.; Reygrobellet, C.; Gerentes, I. Financial cost of osteoarthritis in France. The "COART" France study. Joint Bone Spine 2005, 72, 567–570. [Google Scholar] [CrossRef]
- Centers for Disease, C.; Prevention. Prevalence of self-reported arthritis or chronic joint symptoms among adults--United States, 2001. MMWR Morb Mortal Wkly Rep 2002, 51, 948–950. [Google Scholar]
- Lawrence, R.C.; Helmick, C.G.; Arnett, F.C.; Deyo, R.A.; Felson, D.T.; Giannini, E.H.; Heyse, S.P.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998, 41, 778–799. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Gupte, C.; Akhtar, K.; Smith, P.; Cobb, J. The Global Economic Cost of Osteoarthritis: How the UK Compares. Arthritis 2012, 2012, 698709. [Google Scholar] [CrossRef]
- Kotlarz, H.; Gunnarsson, C.L.; Fang, H.; Rizzo, J.A. Osteoarthritis and absenteeism costs: evidence from US National Survey Data. J Occup Environ Med 2010, 52, 263–268. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P.; et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken) 2012, 64, 465–474. [Google Scholar] [CrossRef]
- Zhang, W.; Nuki, G.; Moskowitz, R.W.; Abramson, S.; Altman, R.D.; Arden, N.K.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis Cartilage 2010, 18, 476–499. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Cooper, C.; Al-Daghri, N.M.; Dennison, E.M.; Rizzoli, R.; Reginster, J.Y. Inappropriate claims from non-equivalent medications in osteoarthritis: a position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Aging Clin Exp Res 2018, 30, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Vetter, G. [Topical therapy of arthroses with glucosamines (Dona 200)]. Munch Med Wochenschr 1969, 111, 1499–1502. [Google Scholar]
- Scholtissen, S.; Bruyère, O.; Neuprez, A.; Severens, J.L.; Herrero-Beaumont, G.; Rovati, L.; Hiligsmann, M.; Reginster, J.Y. Glucosamine sulphate in the treatment of knee osteoarthritis: cost-effectiveness comparison with paracetamol. Int J Clin Pract 2010, 64, 756–762. [Google Scholar] [CrossRef]
- Terwee, C.B.; Jansma, E.P.; Riphagen, I.I.; Vet, H.C.W.d. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual Life Res 2009, 18, 1115–1123. [Google Scholar] [CrossRef]
- Shi, J.; Fan, K.; Yan, L.; Fan, Z.; Li, F.; Wang, G.; Liu, H.; Liu, P.; Yu, H.; Li, J.J.; et al. Cost Effectiveness of Pharmacological Management for Osteoarthritis: A Systematic Review. Appl Health Econ Health Policy 2022, 20, 351–370. [Google Scholar] [CrossRef]
- Ofman, J.J.; Sullivan, S.D.; Neumann, P.J.; Chiou, C.F.; Henning, J.M.; Wade, S.W.; Hay, J.W. Examining the value and quality of health economic analyses: implications of utilizing the QHES. J Manag Care Pharm 2003, 9, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Bruyere, O.; Detilleux, J.; Reginster, J.Y. Health Technology Assessment of Different Glucosamine Formulations and Preparations Currently Marketed in Thailand. Medicines (Basel) 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Detilleux, J.; Reginster, J.Y. Cost-Effectiveness Assessment of Different Glucosamines in Patients with Knee Osteoarthritis: A Simulation Model Adapted to Germany. Curr Aging Sci 2021, 14, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Reginster, J.Y.; Honvo, G.; Detilleux, J. Cost-effectiveness evaluation of glucosamine for osteoarthritis based on simulation of individual patient data obtained from aggregated data in published studies. Aging Clin Exp Res 2019, 31, 881–887. [Google Scholar] [CrossRef]
- Black, C.; Clar, C.; Henderson, R.; MacEachern, C.; McNamee, P.; Quayyum, Z.; Royle, P.; Thomas, S. The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation. Health Technol Assess 2009, 13, 1–148. [Google Scholar] [CrossRef]
- Segal L, D.S., Chapman A. Segal L, D.S., Chapman A, Osborne RH. Priority setting in Osteoarthritis. 2004.
- Weinstein, M.C.; Stason, W.B. Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med 1977, 296, 716–721. [Google Scholar] [CrossRef]
- Blumenschein, K.; Johannesson, M.; Yokoyama, K.K.; Freeman, P.R. Hypothetical versus real willingness to pay in the health care sector: results from a field experiment. J Health Econ 2001, 20, 441–457. [Google Scholar] [CrossRef]
- Cohen, M.; Wolfe, R.; Mai, T.; Lewis, D. A randomized, double blind, placebo controlled trial of a topical cream containing glucosamine sulfate, chondroitin sulfate, and camphor for osteoarthritis of the knee. J Rheumatol 2003, 30, 523–528. [Google Scholar]
- Pavelká, K.; Gatterová, J.; Olejarová, M.; Machacek, S.; Giacovelli, G.; Rovati, L.C. Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Arch Intern Med 2002, 162, 2113–2123. [Google Scholar] [CrossRef]
- Kim, D.D.; Wilkinson, C.L.; Pope, E.F.; Chambers, J.D.; Cohen, J.T.; Neumann, P.J. The influence of time horizon on results of cost-effectiveness analyses. Expert Rev Pharmacoecon Outcomes Res 2017, 17, 615–623. [Google Scholar] [CrossRef]
- Iino, H.; Hashiguchi, M.; Hori, S. Estimating the range of incremental cost-effectiveness thresholds for healthcare based on willingness to pay and GDP per capita: A systematic review. PLoS One 2022, 17, e0266934. [Google Scholar] [CrossRef] [PubMed]
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.P.; Hill, S.R. Cost-effectiveness thresholds: pros and cons. Bull World Health Organ 2016, 94, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Ii M IA, Nakamura R. Considering the costs and benefits of medical care (In Japanese). 2019.
- Bai-dang, Z.; Zu-jian, L.; Huan-tian, Z.; Ming-tao, H.; Dong-sheng, L. Cost-effectiveness analysis on the treatment of knee osteoarthritis by glucosamine hydrochloride and glucosamine sulfate. Chinese Journal of Tissue Engineering Research 2012, 16, 9867–9872. [Google Scholar] [CrossRef]
Figure 1.
Process of articles selection.
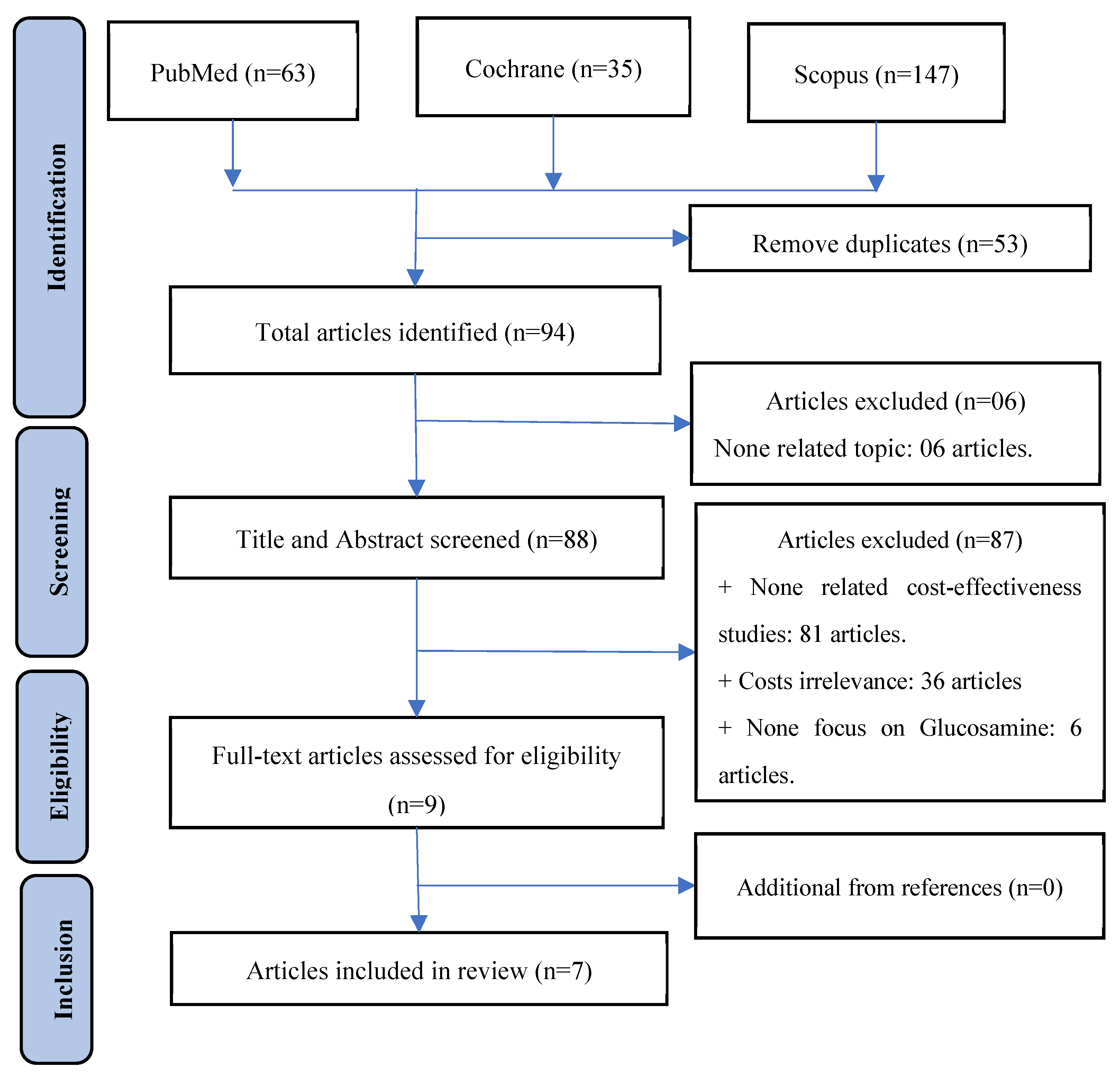
Table 1.
Summary of articles information.
| Years | 2004 | 2009 | 2010 | 2015 | 2019 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|---|---|---|
| Number of articles | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Drugs used | Glucosamine and OTC drugs (NSAIDs, Paracetamol) | Glucosamine | ||||||
| Number of ;articles |
3 | 4 | ||||||
| Type of ;Glucosamine |
pCGS | pCGS and OFG | ||||||
| Number of ;articles |
3 | 4 | ||||||
| OA site | Knee | All | ||||||
| Number of ;articles |
5 | 2 | ||||||
Table 3.
Cost-effectiveness related data.
| No. | Study, year, and country | Comparator | Cost | QALY gain | ICER | Conclusion |
|---|---|---|---|---|---|---|
| 1 | Bruyère et al.[45], 2023, Thailand | pCGS vs. OFG | At 3 months ;pCGS: $53.805 ;OFG: $100.44At 6 months ;pCGS: $126.1359 ; |
At 3 months ;pCGS: 0.017 ;OFG: 0.0031At 6 months ;pCGS: 0.0411 ;OFG: 0.0048 |
At 3 months ;pCGS/PBO: 3165 USD/QALYOFG/PBO: 32,400 USD/QALY ;At 6 months ;pCGS/PBO: 3069 USD/QALY ;OFG/PBO: placebo better |
pCGS is cost-effective at threshold 3260 USD/QALY ;pCGS is more cost-effective than OFG |
| 2 | Luksameesate et al.[15], 2022, Thailand | pCGS + standard care vs. standard care | - | 0.87 | Dominant | The early addition of pCGS into standard care treatment early is cost-saving and more effective compared to standard care alone |
| 3 | Bruyère et al.[46], 2021, Germany | pCGS vs. OFG | At 3 months ;pCGS: €77.0964 ;OFG: €208.854At 6 months ;pCGS: €183.0003 ;At 36 months ;pCGS: €2785.2712 |
At 3 months ;pCGS: 0.0164 ;OFG: 0.0036At 6 months ;pCGS: 0.0413 ;OFG: 0.0044 ;At 36 months ;pCGS: 0.2701 |
At 3 months ;pCGS/PBO: 4,701 €/QALY ;OFG/PBO: 58,015 €/QALY ;At 6 months ;pCGS/PBO: 4,431 €/QALY ;OFG/PBO: Placebo better ;At 36 months ;pCGS/PBO: 10,312 €/QALY |
pCGS is more cost-effective than OFG. |
| 4 | Bruyère et al.[47], 2019, | pCGS vs. OFG | At 3 month ;pCGS: €90.234 ;OFG: €151.009 ;At 6 months ;pCGS: €209.413 ;At 36 monthpCGS: €3162.910 |
At 3 month ;pCGS: 0.0169 ;OFG: 0.00303 ;At 6 months ;pCGS :0.0435 ;OFG: 0.00424 ;At 36 months ;pCGS: 0.2742 ; |
At 3 month ;pCGS/PBO: 5347.2 €/QALY ;OFG/PBO: 49737.4 €/QALY ;At 6 months ;pCGS/PBO: 4807.2 €/QALY ;OFG/PBO: Placebo betterAt 36 monthpCGS/PBO: 11535.5 €/QALY |
pCGS is more cost-effective than OFG. |
| 5 | Scholtissen et al.[41], 2010 ;Spain, Portugal |
GS vs. Paracetamol, ;GS vs. Placebo |
- | - | GS/Paracetamol: ;-1376 €/QALY ;GS/Placebo: ;3617.47 €/QALY |
GS is a highly cost-effective vs. Paracetamol |
| 6 | Black et al.[48], 2009, UK | GS adding conventional vs. conventional care | £2,346.85 | 0.11 | 21,335£/QALY | Addition of GS therapy to current care is cost-effective at threshold 22,000£/QALY |
| 7 | Segal et al.[49], 2004, Australia | GS vs. NSAIDs | $180.024 | 0.052 | 3462 $/QALY | Glucosamine is cost-effective |
OA: osteoarthritis; GS: Glucosamine pCGS: Crystalline Glucosamine Sulfate; OFG: Other Formulations of Glucosamine; NSAIDs: Non-steroidal anti-inflammatory drugs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



