
Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Quantitative research on positive aspects of work-life integration and the well-being of families with children with disabilities is scarce, especially in the national context. The aim of this study was to examine the contributions of some personal and environmental resources in explaining work-to-family (WFF) and family-to-work (FWF) facilitation and mental health of parents of children with disabilities residing in Croatia. The mediational role of WFF and FWF in the relationship between the resources and mental health was tested, while controlling for some general socio-demographic variables. A total of 571 employed parents of a child/children with disabilities completed an online self-assessment questionnaire. The results showed higher WFF (19%) was predicted by higher levels of social support at work, a higher level of education, posttraumatic growth (PTG) of personal strength, and recovery management. Higher FWF (46%) was predicted by higher levels of social support in the family, PTG of personal strength, the emotional regulation strategy of reorienting to planning, optimism, a lower age, the male gender, a greater number of children, and a higher level of education. A higher level of mental health (47%) was predicted directly by higher levels of optimism, recovery management, FWF, emotional regulation strategies of positive refocusing and planning, and a greater number of children, and indirectly by all the predictors of FWF, through a higher level of FWF (but not WFF).
Keywords:
parents of children with disabilities
; mental health
; work-family facilitation
; emotional regulation strategies
; optimism
; posttraumatic growth
; social support
; recovery management
1. Introduction
Mental health implies "a state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community." [1]. The birth of a child with a developmental risk and/or learning that the child has a developmental disability is a traumatic event for parents that requires resources to overcome the trauma and cope with the numerous challenges of caring for a child with an atypical developmental trajectory [2,3]. The challenges include learning about a specific difficulty, finding access to effective treatments, coordinating the implementation of various diagnostic, therapeutic, and intervention procedures, advocating the child's rights in a social, health, and educational context, paying for interventional and therapeutic procedures that are not covered by health insurance and dealing with the high physical and emotional demands of care. When it comes to the parent simultaneously being employed, research results suggest that balancing family and work roles is more difficult for these parents than for parents of typically developing children, and that their employment may be associated with lower levels of well-being and health [4,5]. However, some research results suggest that employment promotes parental well-being since it could serve as a distraction from the complex family environment [6,7]. The issues of integrating work and family roles have been extensively studied in the general population, mostly through the negative aspects in terms of experiences of work-family conflict and imbalance [8,9,10]. Brown and Clark reviewed 54 papers dealing with work and family role balance of parents of children with disabilities up to 18 years of age and warn about the lack of serious quantitative research and of research on the positive aspects of work-family integration, that is, how being employed facilitates family life and vice versa [6]. Additionally, the papers in this review come from countries with heterogeneous organizational policies aimed at balancing work and family roles, so national research on this topic is necessary. This has also been pointed out in the review by Slišković et al. [11]. The application of the principles of positive psychology to the field of developmental disabilities suggests the need to focus on the strengths, possibilities, and opportunities of children with developmental disabilities and their families, instead of the prevailing perspective focused on deficits, stressors, and problems [12,13]. Therefore, in this study, we decided to focus on the positive aspects and explore some personal and environmental strengths and resources that could promote experiences of work-family facilitation and mental health in parents of children with disabilities in the Croatian national context.
Parents of children with disabilities, although exhausted by the demands of care and struggling with the many obstacles they encounter in everyday life, report many positive aspects of parenting children with disabilities [14,15,16,17,18,19]. Seeing a satisfied and happy child who has made even the smallest progress in development, which is normally "taken for granted", is what gives parents strength and contributes to their personal growth and well-being. The positive changes detected in parents of children with developmental disabilities could be paralleled to those found in the model of posttraumatic growth (PTG) [20], reflecting three broad domains: changes in self-perception, interpersonal relationships, and a changed philosophy of life. PTG reflects growth which occurs after struggling with challenging events theorized to disrupt fundamental assumptions about the world being safe, benevolent, and predictable [21]. In line with the PTG model, past research indicates that certain events (e.g., disability diagnosis) may profoundly shock the individual [22], and act as a catalyst for initiating the growth process (e.g., for parents of children diagnosed with Down-Syndrome; [23]. In a one-year qualitative study of parent distress and personal growth [24], parents expressed distress and grief while using coping strategies and resources to manage demands and optimize opportunities for growth. Emotional, cognitive, and behavioral adaptation to the child's condition proved to be an important factor for the well-being of parents of children with disabilities [25].
Another individual protective factor in parents of children with disabilities was the use of adaptive stress coping strategies [17,26] and/or effective emotional regulation strategies [27]. Emotional regulation is an important factor that affects a person's well-being and successful functioning, as well as one’s mental health. The construct of emotional regulation is close to the construct of coping, but emotional regulation refers to both the regulation of negative and positive emotions, while coping is somewhat narrower and refers to a person's ability to deal with stressful situations and reduce negative emotions [28]. There should also be a differentiation between cognitive and behavioral strategies since cognitive processes precede action. Cognitive emotional regulation strategies such as positive reappraisal, putting into perspective, positive refocusing, and planning were shown to help people will more easily tolerate and overcome negative life experiences [29]. Among mothers of adolescents with developmental disabilities, it was shown that coping skills such as active coping/planning, positive reinterpretation/growth, and behavioral/mental disengagement minimized the effects of stressful parent-child interactions [30].
Behavioral and mental disengagement can be viewed through the broader concept of recovery. Recovery refers to restoration processes of an individual’s increased strain level, as a reaction to a stressor or demand, returning to the previous level [31], and managing to recover has been associated with greater well-being [32]. Geurts and Sonnentag [33] addressed the recovery phenomena and presented the Effort–Recovery Model and Allostatic Load Theory [34] as unifying frameworks. Sonnentag and Fritz argued that specific experiences which help with mood repair should underly effective recovery processes [35]. In this context, researchers look at activities (i.e., what people do during their non-work time) and experiences (i.e., what psychological state people are in during their non-work time). When family demands are very high, opportunities for recovery might be very limited, and yet very important [36].
In a qualitative study, semi-structured interviews were conducted on 25 employed parents of children with developmental disabilities, living in Croatia [37], participants were to discuss the factors they believe promote their well-being and help them balance work and private roles. Most of them said that even the slightest departure from everyday life helps them, such as going for coffee alone or with friends, while some parents relax through sports and recreation. Of the personality characteristics that help them balance family and work obligations daily, parents reflected on optimism, emotional stability, patience, combativeness, and organization. Optimism has noticeably been shown to predict higher overall well-being in other studies on parents of children with developmental disabilities as well. Higher levels of optimism predicted increased positive feelings and decreased negative feelings, even after controlling for the levels of parenting stress and child problematic behavior [38]. In parents of autistic children, it predicted lower levels of depressive symptoms, but was protective only for mothers (not for fathers) [39]. In the aforementioned study [37], parents also generally pointed out the benefits of different forms of social support (emotional and instrumental) from various sources (family members, friends, workplace-supervisors and colleagues, the wider society). Social support has also been found to be a protective factor of the well-being of this group of parents in other studies, especially in the family [26,40], and related to work-family balance [6].
Much of the research on work-family/life integration has focused on theoretical models that include individual, work, and family characteristics as antecedents (e.g., structural and psychological stressors, demands, resources, and support), mediator variables related to the interface (positive and negative) of work and family roles, and outcome variables related to the well-being of the individual, family, and organization [41,42]. In its essence, work–family facilitation is the sense that work and family are complementary, that is, that involvement in one domain can beneficially influence functioning of the other domain. It can occur bidirectionally; family can provide gains that enhance work domain functioning (family-to-work facilitation or FWF) and work can provide gains that enhance family domain functioning (work-to-family facilitation or WFF) [43]. Using the Family Resilience Theory, Grzywacz and Bass studied the effects of work-family facilitation on mental health in working adults and showed that adult mental health is optimized when work-family facilitation, especially FWF, is high [44]. This implies that factors promoting greater work-family facilitation also could promote a higher level of mental health. Wayne and colleagues (2007) offer the Resource–Gain–Development (RGD) perspective to explain facilitation and identify its primary antecedents, consequences, and moderators [45]. The RGD perspective specifies that personal characteristics and environmental resources that promote positive domain experiences and the acquisition of gains are key promoters of facilitation. Such personal characteristics are the aspects of oneself that promote positivity and the tendency to experience positive emotional states, seek positive developmental experiences, and earn status and other assets. The environmental resources include object, condition, energy, and support resources that promote positive, dynamic, and enriching environments. Some individuals can obtain more resources from their environment or more effectively use resources and thus receive greater benefits. Thus, theoretically speaking, all the above-mentioned promoters of well-being in parents of children with disabilities could be expected to also promote WFF and FWF. There is empirical evidence for some, directly or indirectly, although not specifically on parents of children with disabilities, except for social support and work-family balance [6]. In research on frontline hotel employees [46], work social support enhanced both directions of work-family facilitation and family social support increased FWF. Both directions of facilitation were associated to higher work performance in the workplace. In research on police officers [47], optimism fostered work-to-family and family-to-work enrichment and psychological health. Work-life balance is shown to be impaired with the lack of recovery activities [48]. In another study [49], relationships between coping and facilitation varied depending on the source domain. Positive thinking was associated with higher WFF and FWF, direct-action was associated with higher FWF, and advice-seeking was related to higher WFF.
In a study on mothers with children with learning disorders, these mothers reported a higher level of family-to-work conflict and a higher level of WFF compared to mothers of children without learning disorders [50]. FWF predicted a greater level of child’s secure attachment to the mother and family cohesion. In another study [51], those with greater work-family balance, that is, lower work-family conflict and higher work-family enrichment (facilitation), had a greater number of children and greater parental and job satisfaction, but lower satisfaction with observed social attitudes towards their disabled child in comparison to other groups of parents according to the levels of work-family conflict and facilitation.
The aim of this study was to examine the contributions of some individual and environmental resources in explaining work-to-family and family-to-work facilitation and mental health of parents of children with disabilities residing in Croatia. We assumed that higher levels of optimism, posttraumatic growth (in terms of personal strength), cognitive emotional regulation strategies of positive reappraisal and reorienting to planning, recovery management, and social support at work and in the family will predict higher levels of WFF, FWF, and mental health. We also set the aim to examine whether WFF and FWF have a mediating role in explaining the relationship between the examined predictors and mental health. In examining these relationships, we controlled for some general socio-demographic variables: gender, age, education, and number of children and assumed correlations between all the predictors and WFF and FWF.
2. Materials and Methods
2.1. Participants
The study sample consisted of 571 employed mothers (N = 517; 90.5%) and fathers (N = 54; 9.5%) who have children with developmental disabilities. A convenient sample was used with all participants required to have a child with an objectively diagnosed developmental disability up to 19 years of age (the age of legal adulthood in Croatia is 18), be employed, and have residence in the Republic of Croatia. The participants were very heterogenous in terms of the type of employment with 384 (67.8%) working full time and 184 (32.2 %) working part time. They were from various regions of the country, mostly from the city of Zagreb (N = 127; 22.2%) and Zagreb County (N = 38; 66.5%), Split County (N = 69; 12.1%), Zadar County (N = 55; 9.6%), Primorje-Gorski Kotar County (N = 42; 7.4%), Osijek-Baranja County (N = 38; 6.7%), Istria County (N = 28; 4.9%), with 14 other regions being represented by 2 (Požega-Slavonia County) to 23 participants (Varaždin and Međimurje Counties). Some other socio-demographic characteristics are shown in Table 1.
2.2. Procedure
After getting approval from the Ethics Committee of the Department of Psychology of XXX, data were collected using an online questionnaire. The questionnaire was distributed through institutions working with children with disabilities and their parents such as the Croatian Welfare Institute, kindergartens, schools, hospitals, special hospitals, schools, and other rehabilitation institutions. Some were reached through social networks and various nationwide associations uniting parents of children with developmental disabilities. Participation in the research was voluntary and anonymous. Participants were also given a chance to send the research group their comments or questions through the email address provided or the Facebook page created for the study.
The research was conducted as part of a project funded by the University of XXX called XXX.
2.3. Measures
Mental health was assessed with the Croatian Brief Mental Health Inventory [52]. It is comprised of five questions aimed at measuring general mental health. Subjects are asked to rate the frequency of each described condition in the past month on a six-point scale (1 - never to 6 - constantly). The questionnaire includes the following domains: general positive affect ("How often were you happy?"), anxiety ("How often were you very nervous?"), depression ("How often did you feel discouraged and sad?" / How often did you feel calm and peaceful?"), and behavioral/emotional control ("How often did you feel so depressed that nothing could cheer you up?"). The total score is the average score on all items, after reversed coding of three items. Thus, a higher score indicates a higher level of general mental health. The Cronbach α in this study is .90.
Work-to-family and family-to-work facilitation was assessed with two subscales from the Work-family spillover scale [53], translated and adapted by Buljan [54]. Each dimension is measured with four items. The work-to-family facilitation items assess the extent to which skills, behavior, or positive mood from the work role have positively influenced one's role in the family (e.g., "The skills you use on your job are useful for things you have to do at home."), while family-to-work facilitation items assess the degree to which positive mood, behavior, sense of achievement, support or resources provided at home positively influence a person's work role (e.g., "The love and respect you get at home makes you feel confident about yourself at work."). Respondents assess, on a 5-point scale (1 – never; 5 – always), how often they experience each described situation in a typical work week. The total score is the average score on each set of the four items, with a higher score indicating greater facilitation. In this study, the Cronbach alpha reliability coefficient for the Work-to-Family Facilitation subscale is α = .82 and for Family-to-Work Facilitation α = .76.
Optimism was assessed with a subscale from the Optimism-Pessimism Scale [55]; adapted version of the Optimism and Pessimism Scale by Chang et al. [56]. The subscale consists of 6 items (e.g., "I always look at things from the positive side") and respondents assess the extent to which each applies to them on a 5-point scale (1 - does not apply to me at all; 5 - applies to me completely). The total score is the average of the scores on all items, with a higher result indicating greater optimism. The Cronbach α in this study is .86.
Emotional regulation strategies of positive refocusing and planning were assessed with two subscales from the Cognitive Emotion Regulation Questionnaire (CERQ) [57]; translation and adaptation by Soldo and Vulić-Prtorić [58]. The questionnaire assesses the cognitive strategies that a person uses after facing a negative, threatening, or stressful life event or situation. Each subscale consists of four items. Positive refocusing refers to thinking about other, more pleasant things instead of the actual event (e.g., "I'm thinking about something nice instead of what happened."). Planning (Reorienting to planning) refers to thinking about the steps that need to be taken for the individual to face the event (e.g., "I am planning what would be the best thing to do."). On a 5-point scale (1 – never; 5 - always), respondents indicate how often they use each of the described ways of thinking after an unpleasant experience. The score is calculated by averaging the corresponding scores for each of the cognitive strategies, with a higher score indicating a more frequent use of a particular strategy. In this study, the Cronbach alpha reliability coefficient for the Positive Refocusing subscale is α = .93 and for the Reorienting to Planning subscale it is α = .82.
Personal strength was assessed with the Personal Strength subscale from the Posttraumatic Growth Questionnaire [59], which is a translated and adapted version of the Posttraumatic Growth Inventory (PTGI) [60]. We adapted the instructions to the studied population, emphasizing that they assess the changes that occurred after being confronted with the child's diagnosis. The subscale consists of 4 items (e.g., " I discovered that I am stronger than I thought."). Respondents assess the extent to which they have experienced the described change on a 6-point scale (0 - I have experienced no change; 5 - I have experienced change to an extremely high degree). The total score is the average of the assessments, with a higher score indicating a higher level of posttraumatic growth in terms of personal strength after the life event. The Cronbach α in this study is .89.
Social support at work and in the family was assessed using 8 items (4 for social support at work and 4 for social support in the family) that were originally part of the Social Support at Work and Family Scale [61]. We selected only the items reflecting support of one’s private life in the work domain (e.g., "My co-workers (superiors, colleagues) understand my personal and family needs.") and of work issues from family members (e.g., "I can speak of my work to my family members (spouse/partner, children, parents, etc.) without embarrassment."). The respondent assesses the level of agreement with each item on a 7-point scale (1 - I do not agree at all; 7 - I completely agree). The total score is the average score on the two sets of four items, after reversely coding one item in each set, and indicates a higher level of perceived social support. The Cronbach α in this study is .83 for social support at work, and .84 for social support in the family.
Recovery management in terms of managing time for self and relaxation and enjoying free time was assessed using two items from the Recovery Management subscale of the Work-Life Crafting Scale (Peeters & Demerouti, 2014; according to Wepfer et al. [48]): "I make sure that I can relax during my time off (e.g., me-time, hobbies, sports)", "I make sure that I do things that I enjoy during my time off (e.g., social activities, sports)". The third item of the original subscale "I take care that the amount of work time and private time are balanced." was excluded due to the conceptual overlap with work-life balance. Respondents were to think about the time they spent when they were not working and gave assessments on how often they do what is described in a typical work week, on a 5-point Likert-scale (1 - never; 5 - always). The total score is the average of the two assessments, with a higher score indicating a greater level of managing to recover or enjoy time for self. The Cronbach α in this study is .92.
The sociodemographic part of the questionnaire included questions on gender, age, level of education, place of residence, marital status, number of children, number of children with disabilities, the level of the child’s disability, the type of profession, and the spouse’s/partner’s employment status.
2.4. Analytical strategies
Preliminary statistical analyses such as reviewing descriptive statistics and bivariate correlations between variables were conducted using the program Statistica 14 [62]. Path analyses were then performed in the program Mplus 8.7 [63] to estimate the hypothesized model, suggesting personal characteristics (resources) such as optimism, emotional regulation strategies (planning and positive refocusing), and posttraumatic growth (personal strength), enjoying time for oneself, and environmental resources such as social support in the family and at work as predictors of mental health indirectly through WFF and FWF. Relationships with covariates (age, gender, education, and number of children) were controlled for. Correlations between independent variables and covariates were specified as well as a correlation between WFF and FWF. The full mediation model was first estimated to avoid just identifying the model, and modification indices were followed to check if there should be additional paths from first level independent variables and mental health (the main dependent variable). The maximum likelihood (ML) parameter estimation method, justified by the descriptive statistics, and full information maximum likelihood (FIML) for missing data imputation (the default) were used. Model fit was examined using the χ2/df ratio, with values up to 3 demonstrating good fit, the Comparative fit index (CFI) and the Tucker-Lewis index (TLI), with values above .90 signifying good fit and above .95 very good fit, and the root mean square error of approximation (RMSEA) and standardized root mean residual (SRMR) with values up to .08 suggesting good fit [64]. The model with satisfactory fit indices and no more modification indices was interpreted and indirect relationships (mediations) were tested by using the bootstrap method (1000 simulations).
3. Results and discussion
3.1. Preliminary analyses
The descriptive statistics of the study variables were calculated and are shown in Table 2. All variable results' distributions were normal according to the skewness and kurtosis values varying between -2 and +2 [65], except for gender, with values not surpassing the values of skewness up to 3 and kurtosis up to 8 suggested by Kline [66]. The obtained values are shifted towards higher results on the variables gender (a much larger number of women than men), posttraumatic growth (personal strength), emotional regulation strategies of planning (slightly for positive refocusing), social support at work and in the family, and mental health. The results are slightly shifted towards lower results on age, number of children, and recovery management. There was from 0 to 7 missing data per variable.
The bivariate Pearson correlations between the study variables were calculated and are shown in Table 3. The results show that all the main study variables (optimism, emotional regulation strategies of positive refocusing and planning, posttraumatic growth in terms of personal strength, recovery management, social support at work and in the family, work-to-family and family-to-work facilitation, and mental health) are in significant positive low to intermediate correlations, except the correlation between the emotional regulation strategy of planning and recovery management. The lowest correlation is .11 between the emotional regulation (ER) strategy of planning on the one hand and WFF and mental health on the other. The highest were between social support in the family and FWF (.56) and optimism and mental health (.58.). There are only a few significant correlations between the socio-demographic variables and main variables. Men tend to report higher levels of recovery management, FWF, and mental health. Older participants tend to report higher levels of recovery management and lower levels of FWF. A higher level of education is associated with a lower level of personal strength and positive refocusing, and with a higher level of WFF. A greater number of children is associated to a higher level of optimism, emotional regulation strategies of positive refocusing and planning, personal strength, FWF, and mental health. Men are somewhat older than the women in the sample, greater age is associated to a higher level of education and greater number of children and a higher education is associated to a lower number of children. The values of the variance inflation factor (VIF), indicating collinearity in a multiple regression with mental health as the dependent variable and the other variables as predictors, are from .06 (gender) to .10 (age) when it comes to the sociodemographic variables The lowest VIF for the main variables is .16 (emotional regulation strategy of planning), then from .24 (work-to-family facilitation) to .32 (social support at work); the values in between are for positive refocusing and recovery management. The highest are .44 for optimism, .46 for social support in the family, and .47 for FWF. When looking at the VIF values without WFF and FWF as predictors, the values are from .05 (gender) to .07 (number of children) for the covariates, and from .13 (reorienting to planning) to .32 for social support in the family and .41 for optimism.
3.2. Testing the hypothesized model
Path analyses was conducted to test the hypothesized model assuming a full mediation, that is, mental health predicted indirectly by the examined personal and environmental resources through WFF and FWF was tested, controlling for the relationships with the examined covariates. Correlations between the examined independent and mediator variables were included. The number of missing data patterns was 8. The model fit indices of the initially specified model were as follows: χ2= 252.507; df = 7; p=.000; CFI = .710; TLI = .000; RMSEA = .248 (90% C.I. .222; .275); SRMR = .060. Only the SRMR indicated good fit of the model to the data. The plausible modification indices suggested adding direct paths with optimism, emotional regulation – positive refocusing and planning, and enjoying free time/time for self. The model fit indices of this model were: χ2= 19.432; df = 3; p=.000; CFI = .981; TLI = .767; RMSEA = .098 (90% C.I. .059; .141); SRMR = .009. Only the CFI and SRMR indicated good fit. There were no plausible modification indices suggested by the program. After excluding non-significant paths (but with p-levels higher than .10), the model fit indices all suggested a good to very good fit of the model to the data: χ2= 29.107; df = 15; p=.016; CFI = .983; TLI = .960; RMSEA = .041 (90% C.I. .017; .062); SRMR = .013. The resulting standardized parameter estimates (STDYX path coefficients and explained variance R2) and their significance are shown in Figure 1. The non-significant paths and the correlations are not shown due to a higher level of clarity of the display. The non-presented standardized parameter estimates (path coefficients), standard errors and significance levels are shown in Table 4. The bootstrap simulation method was performed on this model. All the mediations considering the main variables, shown in Figure 1, are significant at the 95% significance level, which can be seen by the bootstrap confidence intervals not including the zero value (when considering three decimal values) in Table 5.
Interpreting the model results
The results presented in Figure 1, Table 4, and Table 5 confirmed some of the assumed relationships and mediation processes. A higher reported level of WFF is predicted by higher levels of social support at work, a higher level of education, personal strength, and recovery management (listed from the greatest to lowest contribution). The predictors explained 19% of the variance of WFF. A higher level of FWF (46% of the variance) is predicted by higher levels of social support in the family, personal strength, emotional regulation strategy of planning, optimism, and a lower age, the male gender, a greater number of children, and a higher level of education. Greater mental health (47% of the variance) is predicted directly mostly by higher levels of optimism, then by recovery management, FWF, emotional regulation strategies of positive refocusing and planning, and a greater number of children. It is predicted indirectly by higher levels of optimism, planning, personal strength, and social support in the family through a higher level of FWF. It is vivid in Table 4 that WFF is at the sole border of significance according to the p-level of the path coefficient estimate in predicting mental health. However, the bootstrap 95% interval includes zero, so it could not be considered as significant. Issues of multicollinearity should be considered, especially the correlations of optimism to the other independent variable, mostly personal strength and positive refocusing, and of social support in the family and at work. The correlations estimated in the model were in line with those explained previously (Table 3); however, the results of model testing show an additional significant correlation; greater age is associated with a lower level of social support in the family (although the correlation is low; r = -.085).
4. Discussion
The incentives for this research were the need to focus on the strengths, possibilities, and opportunities of families with a child or children with developmental disabilities [12,16], and the scarcity of quantitative studies observing more comprehensively the positive aspects of work-family integration [6], especially in the national context [11]. Thus, the aim of this study was to examine the contributions of some individual and environmental strengths and resources (optimism, posttraumatic growth - personal strength, cognitive emotional regulation strategies of positive reappraisal and reorienting to planning, recovery management, and social support at work and in the family) in explaining both directions of work-family facilitation and mental health of parents of children with disabilities in Croatia. The potential mediating role of WFF and FWF in the relationship between the examined predictors and mental health was also examined, all along with adding some general socio-demographic covariates (gender, age, education, and number of children) to the model. This would be the first study to quantitatively examine the relationships between all the mentioned and the mediating role of WFF and FWF between the resources suggested as predictors and mental health in working parents of children with developmental disabilities. The results of this study confirmed some of our hypotheses about the examined relationships and mediation processes.
4.1. Predicting work-to-family and family-to-work facilitation in parents of children with disabilities in Croatia
The results showed WFF is predicted by higher levels of social support at work, a higher level of education, PTG of personal strength, and recovery management, but not by optimism and the examined emotional regulation strategies, and only 19% of the variance WFF was explained. When it comes to FWF (46%), higher levels are predicted by higher levels of social support in the family, PTG in personal strength, emotional regulation strategy of reorienting to planning, optimism, a lower age, the male gender, a greater number of children, and a higher level of education. It was not predicted by the emotional regulation strategy of positive refocusing, social support of work and recovery management. The results are in line with the Resource–Gain–Development Perspective specifying that personal characteristics and environmental resources that promote positive domain experiences and the acquisition of gains are key promoters of facilitation [45].
Previous research shows that domain specific characteristics, in comparison to cross-domain characteristics, are relatively more important predictors of the effects of the same domain to another domain [67], which can explain the relative contributions of social support at work and in the family to WFF and FWF. Additionally, the measures of social support used in this study contained items referring to social support in each domain aimed towards issues of the other domain, so it is logical to assume that experiencing more support for family issues in the work domain would contribute to the experience that the work domain facilitates family life and vice versa. A higher level of education could be associated with better work conditions, higher positions, greater skills, and more financial resources [68], which could be beneficial for both the work and family domain. The obtained contribution of higher levels of managing to recover, that is, to relax and enjoy activities during one’s free time, to higher reported levels of WFF could be related to a previous finding that the coping strategy of escape used in dealing with work stressors was positively related to WFF [69]. It could reflect that work conditions offer the possibility to manage time for self and to rewind not only from work, but from family obligations. This variable did not have a significant relative contribution to FWF probably because these activities could be connected to activities with the family (so being able to recover contributes to more quality time with the family).
The PTG of personal strength showed to be an important resource for both the experience of WFF and FWF. Reports of the growth of personal strength after dealing with the child’s diagnosis reflect a higher sense of self-confidence, ability to deal with difficulties, a greater acceptance of situations, and therefore greater possibilities to adapt and to obtain the gains and resources of both domains. Also, positive thinking and reorienting to planning how to deal with situations contributed to the experience of the family life facilitating work life, and it is obvious that the examined personal resources were more predictive of FWF in general. One’s family and private life might depend more on personal factors since one has higher control over what is going on in these domains. Perhaps the work domain is generally more complex to manage than the home domain, making planning behavior and staying positive while combating the situations in the family relatively more important for being efficient with time and energy at work than at home [70]. The association of a greater sense of FWF to the male gender, lower age, and more children in the family is also not surprising due to greater vitality in younger people [71], the likely greater support of men’s work in a society still prone to traditional gender roles of men as the main breadwinner [72], and results of previous studies showing greater numbers of children being related to greater work-family enrichment [51]. According to the characteristics of our sample participants, it seems that the greater number of children is related to the presence of a child/children without difficulties in the family, which has been associated with higher well-being in previous studies [73]. The presence of healthy children could be an additional source of satisfaction and support in the family making it easier to balance demands [37]. On the other hand, a lower number of children could reflect the decision not to have more children due to heightened levels of care and the worry of developmental risks for another child [74].
4.2. Predicting mental health in parents of children with disabilities in Croatia and the mediational role of work-to-family and family-to-work facilitation
Higher levels of mental health (47%) were predicted directly mostly by higher levels of optimism, by recovery management, family-to-work facilitation, emotional regulation strategies of positive refocusing and planning, and a greater number of children, but not by PTG of personal strength, social support at work and in the family, and WFF. It was predicted indirectly by all the predictors of FWF, showing the significant mediating role of FWF in the relationship between these predictors and mental health: higher levels of optimism, ER strategy of planning, PTG of personal strength, and social support in the family predicted greater mental health through a higher level of FWF. Neither the predictive nor mediating role of WFF in explaining mental health and its relationships with the examined personal and environmental resources were confirmed, although the contribution is very near to significance.
The protective role of optimism in different aspects of the mental health of parents of children with disabilities has been documented earlier [37,39]. It could be said that this personality trait helps in dealing better with the negative experiences, and growth after such experiences along with adopting health-promoting behaviors and adaptable coping strategies [75]. They also reflect their hope and positivity to others, and thus have better social relationships, which is all good for mental health [76]. Related to this are the results showing the beneficial contribution of the examined cognitive emotional regulation strategies, as adaptive coping strategies reflecting one’s orientation to positive aspects of situations and ways to manage them. Recovery management in parents of children with a developmental disability is viewed as a health-promoting behavior as well [77], and reflects a manner of self-care [78,79]. A meta-analysis (k = 316; independent samples; N = 99 329 participants) showed that relaxation and mastery experiences positively predict personal outcomes such as positive affect, life satisfaction, and well-being [32], which are both comprehended in the measure of recovery management in this study.
The relatively greater importance of family-to-work facilitation for mental health was shown in previous studies, shown to be a family protective factor that buffers the detrimental effects of work-family conflict on mental health [44]. Through the provision of support and love, families can act as a bridge between their working members and the organization/industry in facilitating mental health care [80]. The number of children as a significant predictor of mental health could be explained with the same suggested mechanisms as for predicting FWF (greater support in the family, a reflection of less stress in the family to have more children, sense of hope). The mentioned factors shown to predict WFF, FWF, and mental health in this study are also described through the Family Resilience Theory [81,82], defining family resilience as the capacity of the family to maintain a level of healthy functioning during crisis situations. The theory distinguishes protective family characteristics (employment, distribution of duties within the family, financial status of the family, joint agreements, cohesion), protective processes (spousal support, communication, problem solving, warm supportive relationships), and recovery factors (support in crisis situations, optimism, environmental support). Work-family policies and educative (informative) or training programs that encourage the studied personal and environmental resources should be designed and applied to promote the work-life balance and mental health of employed parents with children with a developmental disability, which would benefit their families, organizations, and the wider community.
4.3. Limitations and future research
Aside from the advantages of this study pointed out throughout the paper, some shortcomings should be pointed out. Although the study included a relatively large number of employed parents of children with disabilities, participation was voluntary and without compensation. Therefore, there is a possibility that those with a greater lack of time, energy, and resources, greater issues of work-family and different life role imbalances and heightened stress levels were underrepresented in the study, that is, could not manage to fill out the questionnaire. On the other hand, the participants may have been very motivated to share their problems related to raising children with disabilities, also limiting the generalizability of the results. Male participants were underrepresented in the study and there were several participants with children without an official diagnosis. Future research should be attempted on more representative samples of the parents in question living in Croatia using population sampling techniques.
The self-assessment nature of data collection also makes the objectivity and reliability of the data. Assessments from other family and/or organizational members could be collected or intervention and observational or diary studies could be conducted. Dyadic relationships could be considered as well, for example, the work-family fit of the spouse/partner. Also, the research was cross-sectional with data collected in one time-point; thus, the data analysis was correlational, making it impossible to give conclusions on any causal relationships. The relationships between the examined variables could be reciprocal or in the opposite direction, for instance, better mental health could be a factor influencing the perceptions of work-family facilitation instead [83]. Also, hypotheses on more specific relationships between the independent variables (besides only correlational) could be tested, for example, whether optimism contributes to posttraumatic growth and more adaptive coping strategies or it is the other way around [75]. Moderating relationships among the same variables and covariates could also be considered.
Other possible, and more independent (to avoid issues of multicollinearity shown in this study), personal and environmental resources could also be observed, especially in the workplace, considering the low explained variance of WFF. Future research could consider other personal characteristics such as other potentially strengthening or adaptive personality traits, other cognitive or behavioral coping strategies, more specific activities during ‘time for self’, preferred ways of managing work and family boundaries, work characteristics such as control and flexibility at work, specific family-friendly organizational policies, positive work culture, work efficacy, etc.
5. Conclusions
In this study, we decided to focus on the positive aspects and explore some personal and environmental strengths and resources that could promote experiences of work-family facilitation and mental health in parents of children with disabilities in the Croatian national context. Path analysis showed that, among the main variables of the study, a higher level of mental health (47% of the variance explained) was predicted directly mostly by higher levels of optimism, by recovery management, family-to-work facilitation (FWF), emotional regulation strategies of positive refocusing and planning, and a greater number of children. It was also predicted indirectly by all the predictors of FWF (46%) (higher levels of optimism, ER strategy of planning, PTG of personal strength, and social support in the family), through a higher level of FWF. It was not significantly predicted by work-to-family facilitation (WFF), which was predicted by PTG of personal strength and recovery management (19% of the variance). The tested model included covariates: gender, age, education, and number of children, showing some significant, but relatively low contributions. Work-family policies and educative (informative) or training programs that encourage the studied personal and environmental resources should be designed and applied to promote the work-life balance and mental health of employed parents with children with a developmental disability, which would benefit their families, organizations, and the wider community. Further research should be conducted to advance knowledge about the positive aspects and promoters of the quality of the life of parents with a child needing special care.
Author Contributions
Conceptualization, A.Š., A.S., A.T., and J.O.; methodology, A.Š., A.S., A.T., J.O., and L.S.; investigation, A.Š., A.S., A.T., and J.O.; formal analysis, A.Š.; resources, A.Š., A.S. and L.S.; writing—original draft preparation, A.Š.; writing—review and editing, A.S., A.T., J.O., and L.S. All the authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of XXX. The results presented in this paper represent only a portion of the findings obtained as part of the University approved and funded project XXX.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Department of Psychology at the University of XXX.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available on request from the research authors.
Acknowledgments
A special thanks to all those who helped with data collection and all the participants who took the time to complete our questionnaire.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mental Health Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 6 July 2023).
- Ionio, C.; Colombo, C.; Brazzoduro, V.; Mascheroni, E.; Confalonieri, E.; Castoldi, F.; Lista, G. Mothers and Fathers in NICU: The Impact of Preterm Birth on Parental Distress. Europe’s Journal of Psychology 2016, 12, 604–621. [CrossRef]
- Starc, B. Parenting in the Best Interests of the Child and Support to Parents | UNICEF Available online: https://www.unicef.org/croatia/en/reports/parenting-best-interests-child-and-support-parents (accessed on 6 July 2023).
- Gérain, P.; Zech, E. Does Informal Caregiving Lead to Parental Burnout? Comparing Parents Having (or Not) Children With Mental and Physical Issues. Front Psychol 2018, 9, 884. [CrossRef]
- Stewart, L.M.; Sellmaier, C.; Brannan, A.M.; Brennan, E.M. Employed Parents of Children with Typical and Exceptional Care Responsibilities: Family Demands and Workplace Supports. J Child Fam Stud 2023, 32, 1048–1064. [CrossRef]
- Brown, T.J.; Clark, C. Employed Parents of Children with Disabilities and Work Family Life Balance: A Literature Review. Child Youth Care Forum 2017, 46, 857–876. [CrossRef]
- Morris, L.A. The Impact of Work on the Mental Health of Parents of Children with Disabilities. Family Relations 2014, 63, 101–121. [CrossRef]
- Bulger, C.A.; Hoffman, M.E. Segmentation/Integration of Work and Nonwork Domains: Global Considerations. In The Cambridge handbook of the global work–family interface; Cambridge University Press: New York, NY, US, 2018; pp. 701–719 ISBN 978-1-108-40126-5.
- Lewis, S.; Beauregard, T.A. The Meanings of Work–Life Balance: A Cultural Perspective. In The Cambridge Handbook of the Global Work–Family Interface; Shockley, K.M., Johnson, R.C., Shen, W., Eds.; Cambridge Handbooks in Psychology; Cambridge University Press: Cambridge, 2018; pp. 720–732 ISBN 978-1-108-41597-2.
- Williams, J.C.; Berdahl, J.L.; Vandello, J.A. Beyond Work-Life “Integration.” Annu Rev Psychol 2016, 67, 515–539. [CrossRef]
- Slišković, A.; Tokić, A.; Šimunić, A.; Ombla, J.; Nikolić Ivanišević, M. Dobrobit Zaposlenih Roditelja Djece s Teškoćama u Razvoju: Pregled Dosadašnjih Spoznaja, Smjernice Za Daljnja Istraživanja i Praktične Implikacije. Contemp. psychol. 25, 47–69.
- Mahmic, S.; Kern, M.L.; Janson, A. Identifying and Shifting Disempowering Paradigms for Families of Children With Disability Through a System Informed Positive Psychology Approach. Front Psychol 2021, 12, 663640. [CrossRef]
- Wehmeyer, M.L. The Oxford Handbook of Positive Psychology and Disability. Oxford Library of Psychology; Oxford University Press, 2013; ISBN 978-0-19-539878-6.
- Beighton, C.; Wills, J. How Parents Describe the Positive Aspects of Parenting Their Child Who Has Intellectual Disabilities: A Systematic Review and Narrative Synthesis. J Appl Res Intellect Disabil 2019, 32, 1255–1279. [CrossRef]
- Lodewyks, M.R. Parent and Child Perceptions of the Positive Effects That a Child with a Disability Has on the Family, University of Manitoba, 2009.
- Lodewyks, M.R. Positive Impacts of Children with Disabilities. Transition 2015, 45.
- Manor-Binyamini, I. Positive Aspects of Coping among Mothers of Adolescent Children with Developmental Disability in the Druze Community in Israel. Journal of Intellectual & Developmental Disability 2016, 41, 97–106. [CrossRef]
- Sheldon, J.P.; Oliver, M.; Yashar, B.M. Rewards and Challenges of Parenting a Child with Down Syndrome: A Qualitative Study of Fathers’ Perceptions. Disability and Rehabilitation 2021, 43, 3562–3573. [CrossRef]
- Strecker, S.; Hazelwood, Z.J.; Shakespeare-Finch, J. Postdiagnosis Personal Growth in an Australian Population of Parents Raising Children with Developmental Disability. Journal of Intellectual & Developmental Disability 2014, 39, 1–9. [CrossRef]
- Tedeschi, R.G.; Shakespeare-Finch, J.; Taku, K.; Calhoun, L.G. Components of the Theoretical Model of Posttraumatic Growth. In Posttraumatic Growth; Routledge, 2018 ISBN 978-1-315-52745-1.
- Janoff-Bulman, R. Posttraumatic Growth: Three Explanatory Models. Psychological Inquiry 2004, 15, 30–34.
- Stewart, M.; Knight, T.; McGillivray, J.; Forbes, D.; Austin, D.W. Through a Trauma-Based Lens: A Qualitative Analysis of the Experience of Parenting a Child with an Autism Spectrum Disorder. Journal of Intellectual & Developmental Disability 2017, 42, 212–222. [CrossRef]
- Counselman-Carpenter, E.A. The Presence of Posttraumatic Growth (PTG) in Mothers Whose Children Are Born Unexpectedly with Down Syndrome. Journal of Intellectual & Developmental Disability 2017, 42, 351–363. [CrossRef]
- Young, S.; Shakespeare-Finch, J.; Obst, P. Raising a Child with a Disability: A One-Year Qualitative Investigation of Parent Distress and Personal Growth. Disability & Society 2019, 35, 629–653. [CrossRef]
- Barnett, D.; Clements, M.; Kaplan-Estrin, M.; Fialka, J. Building New Dreams: Supporting Parents’ Adaptation to Their Child With Special Needs. Infants & Young Children 2003, 16, 184.
- Krakovich, T.; Mcgrew, J.; Yu, Y.; Ruble, L. Stress in Parents of Children with Autism Spectrum Disorder: An Exploration of Demands and Resources. Journal of autism and developmental disorders 2016, 46. [CrossRef]
- Gérain, P.; Zech, E. Informal Caregiver Burnout? Development of a Theoretical Framework to Understand the Impact of Caregiving. Front Psychol 2019, 10, 1748. [CrossRef]
- Tahmouresi, N.; Bender, C.; Schmitz, J.; Baleshzar, A.; Tuschen-Caffier, B. Similarities and Differences in Emotion Regulation and Psychopathology in Iranian and German School-Children: A Cross-Cultural Study. Int J Prev Med 2014, 5, 52–60.
- Garnefski, N.; Kraaij, V. Cognitive Emotion Regulation Questionnaire - Development of a Short 18-Item Version (CERQ-Short). Personality and Individual Differences 2006, 41, 1045–1053. [CrossRef]
- Woodman, A.C.; Hauser-Cram, P. The Role of Coping Strategies in Predicting Change in Parenting Efficacy and Depressive Symptoms among Mothers of Adolescents with Developmental Disabilities. Journal of Intellectual Disability Research 2013, 57, 513–530. [CrossRef]
- Craig, A.; Cooper, R.E. 11 - Symptoms of Acute and Chronic Fatigue. In State and Trait; Smith, A.P., Jones, D.M., Eds.; Academic Press: London, 1992; pp. 289–339 ISBN 978-0-12-650353-1.
- Headrick, L.; Newman, D.A.; Park, Y.A.; Liang, Y. Recovery Experiences for Work and Health Outcomes: A Meta-Analysis and Recovery-Engagement-Exhaustion Model. J Bus Psychol 2023, 38, 821–864. [CrossRef]
- Geurts, S.A.E.; Sonnentag, S. Recovery as an Explanatory Mechanism in the Relation between Acute Stress Reactions and Chronic Health Impairment. Scand J Work Environ Health 2006, 32, 482–492. [CrossRef]
- McEwen, B.S. Stress, Adaptation, and Disease. Allostasis and Allostatic Load. Ann N Y Acad Sci 1998, 840, 33–44. [CrossRef]
- Sonnentag, S.; Fritz, C. The Recovery Experience Questionnaire: Development and Validation of a Measure for Assessing Recuperation and Unwinding from Work. J Occup Health Psychol 2007, 12, 204–221. [CrossRef]
- Sonnentag, S.; Venz, L.; Casper, A. Advances in Recovery Research: What Have We Learned? What Should Be Done Next? J Occup Health Psychol 2017, 22, 365–380. [CrossRef]
- Ombla, J.; Slišković, A.; Nikolić Ivanišević, M.; Šimunić, A.; Ljubičić, M. Kako zaposleni roditelji djece s teškoćama u razvoju usklađuju zahtjeve radne i obiteljske uloge?: Kvalitativno istraživanje. Rev. sociol. (Online) 2023, 53, 67–97. [CrossRef]
- Kurtz-Nelson, E.; McIntyre, L.L. Optimism and Positive and Negative Feelings in Parents of Young Children with Developmental Delay. Journal of Intellectual Disability Research 2017, 61, 719–725. [CrossRef]
- Rafferty, D.; preston, M.; Sullivan, W.; Ekas, N. Chaotic Family Environments and Depressive Symptoms in Parents of Autistic Children: The Protective Role of Optimism. Research in Autism Spectrum Disorders 2022, 96, 102000. [CrossRef]
- Khusaifan, S.J.; El Keshky, M.E.S. Social Support as a Protective Factor for the Well-Being of Parents of Children with Autism in Saudi Arabia. Journal of Pediatric Nursing 2021, 58, e1–e7. [CrossRef]
- Hill, E.J. Work-Family Facilitation and Conflict, Working Fathers and Mothers, Work-Family Stressors and Support. Journal of Family Issues 2005, 26, 793–819. [CrossRef]
- Holmes, E.K.; Thomas, C.R.; Petts, R.J.; Hill, E.J. Chapter 10 - The Work-Family Interface. In Cross-Cultural Family Research and Practice; Halford, W.K., van de Vijver, F., Eds.; Academic Press, 2020; pp. 323–354 ISBN 978-0-12-815493-9.
- Frone, M.R. Work-Family Balance. In Handbook of occupational health psychology; American Psychological Association: Washington, DC, US, 2003; pp. 143–162 ISBN 978-1-55798-927-7.
- Grzywacz, J.G.; Bass, B.L. Work, Family, and Mental Health: Testing Different Models of Work-Family Fit. Journal of Marriage and Family 2003, 65, 248–261.
- Wayne, J.H.; Grzywacz, J.G.; Carlson, D.S.; Kacmar, K.M. Work–Family Facilitation: A Theoretical Explanation and Model of Primary Antecedents and Consequences. Human Resource Management Review 2007, 17, 63–76. [CrossRef]
- Karatepe, O.M.; Bekteshi, L. Antecedents and Outcomes of Work–Family Facilitation and Family–Work Facilitation among Frontline Hotel Employees. International Journal of Hospitality Management 2008, 27, 517–528. [CrossRef]
- Agrawal, M.; Mahajan, R. The Effect of Optimism on the Work-Family Interface and Psychological Health of Indian Police. Policing: An International Journal 2021, 44, 725–740. [CrossRef]
- Wepfer, A.G.; Allen, T.D.; Brauchli, R.; Jenny, G.J.; Bauer, G.F. Work-Life Boundaries and Well-Being: Does Work-to-Life Integration Impair Well-Being through Lack of Recovery? J Bus Psychol 2018, 33, 727–740. [CrossRef]
- Rotondo, D.M.; Kincaid, J.F. Conflict, Facilitation, and Individual Coping Styles across the Work and Family Domains. Journal of Managerial Psychology 2008, 23, 484–506. [CrossRef]
- Al-Yagon, M.; Cinamon, R.G. Work–Family Relations among Mothers of Children with Learning Disorders. European Journal of Special Needs Education 2008, 23, 91–107. [CrossRef]
- Parchomiuk, M. Work-Family Balance and Satisfaction with Roles in Parents of Disabled Children. Community, Work & Family 2022, 25, 353–373. [CrossRef]
- Slišković, A. Kratki upitnik mentalnog zdravlja. In Zbirka psihologijskih skala i upitnika, svezak 10; Ćubela-Adorić, V., Burić, I., Macuka, I., Nikolić Ivanišević, M., Slišković, A., Eds.; Morepress, 2020; pp. 27–38.
- Wayne, J.H.; Musisca, N.; Fleeson, W. Considering the Role of Personality in the Work–Family Experience: Relationships of the Big Five to Work–Family Conflict and Facilitation. Journal of Vocational Behavior 2004, 64, 108–130. [CrossRef]
- Buljan, T. Prediktori usklađivanja obiteljske i radne uloge za vrijeme pandemije koronavirusa. info:eu-repo/semantics/masterThesis, University of Zagreb. University of Zagreb, Faculty of Humanities and Social Sciences. Department of Psychology, 2020.
- Penezić, Z. SKALA OPTIMIZMA - PESIMIZMA (O-P skala). In Zbirka psihologijskih skala i upitnika, svezak 1; Lacković-Grgin, K., Proroković, A., Ćubela, V., Penezić, Z., Eds.; 2002; pp. 15–17.
- Chang, E.C.; D’Zurilla, T.J.; Maydeu-Olivares, A. Assessing the Dimensionality of Optimism and Pessimism Using a Multimeasure Approach. Cogn Ther Res 1994, 18, 143–160. [CrossRef]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative Life Events, Cognitive Emotion Regulation and Emotional Problems. Personality and Individual Differences 2001, 30, 1311–1327. [CrossRef]
- Soldo, L.; Vulić-Prtorić, A. Upitnik Kognitivne Emocionalne Regulacije (CERQ). In Zbirka psihologijskih skala i upitnika, svezak 9; Slišković, A., Burić, I., Ćubela-Adorić, V., Nikolić, M., Tucak Junaković, I., Eds.; Morepress, 2018; pp. 47–58.
- Macuka, I. Upitnik posttraumatskog rasta. In Zbirka psihologijskih skala i upitnika, Svezak 10; Ćubela-Adorić, V., Burić, I., Macuka, I., Nikolić Ivanišević, M., Slišković, A., Eds.; Morepress, 2020; pp. 121–130.
- Tedeschi, R.G.; Calhoun, L.G. The Posttraumatic Growth Inventory: Measuring the Positive Legacy of Trauma. J Trauma Stress 1996, 9, 455–471. [CrossRef]
- Šimunić, A.; Gregov, L.; Proroković, A. Skala socijalne podrške na poslu i u obitelji. In Zbirka psihologijskih skala i upitnika 8; Tucak Junaković, I., Burić, I., Ćubela-Adorić, V., Proroković, A., Slišković, A., Eds.; Morepress, 2016; pp. 45–53.
- TIBCO® Data Science - Workbench 14.1.0 Available online: https://docs.tibco.com/products/tibco-data-science-workbench-14-1-0 (accessed on 6 July 2023).
- Mplus User’s Guide Available online: https://www.statmodel.com/html_ug.shtml (accessed on 6 July 2023).
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Structural Equation Modeling: A Multidisciplinary Journal 1999, 6, 1–55. [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. An Introduction to Structural Equation Modeling. In Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Hair Jr., J.F., Hult, G.T.M., Ringle, C.M., Sarstedt, M., Danks, N.P., Ray, S., Eds.; Classroom Companion: Business; Springer International Publishing: Cham, 2021; pp. 1–29 ISBN 978-3-030-80519-7.
- Kline, R.B. Principles and Practice of Structural Equation Modeling, Second Edition; Guilford Publications, 2005; ISBN 978-1-59385-075-3.
- Lapierre, L.M.; Li, Y.; Kwan, H.K.; Greenhaus, J.H.; DiRenzo, M.S.; Shao, P. A Meta-Analysis of the Antecedents of Work–Family Enrichment. Journal of Organizational Behavior 2018, 39, 385–401. [CrossRef]
- Stryzhak, O. The Relationship between Education, Income, Economic Freedom and Happiness. SHS Web Conf. 2020, 75, 03004. [CrossRef]
- Ratniewski, J. Antecedents of Work-Family Facilitation: The Role of Coping Styles, Organizational and Family Support, and Gender Role Attitudes. Dissertation Abstracts International: Section B: The Sciences and Engineering 2013, 74.
- Lapierre, L.M.; Allen, T.D. Control at Work, Control at Home, and Planning Behavior: Implications for Work–Family Conflict. Journal of Management 2012, 38, 1500–1516. [CrossRef]
- Penninx, B.W.J.H. A Happy Person, a Healthy Person? Journal of the American Geriatrics Society 2000, 48, 590–592. [CrossRef]
- Ciglar, J. Rodne razlike u ravnoteži između posla i obitelji i predikcija zadovoljstva životom. info:eu-repo/semantics/masterThesis, University of Zagreb. Faculty of Humanities and Social Sciences. Department of Psychology, 2021.
- Kimura, M. Social Determinants of Self-Rated Health among Japanese Mothers of Children with Disabilities. Preventive Medicine Reports 2018, 10, 129–135. [CrossRef]
- Kimura, M.; Yamazaki, Y. Having Another Child without Intellectual Disabilities: Comparing Mothers of a Single Child with Disability and Mothers of Multiple Children with and without Disability. J Intellect Disabil 2019, 23, 216–232. [CrossRef]
- Carver, C.S.; Scheier, M.F. Dispositional Optimism. Trends Cogn Sci 2014, 18, 293–299. [CrossRef]
- Laranjeira, C.; Querido, A. Hope and Optimism as an Opportunity to Improve the “Positive Mental Health” Demand. Front Psychol 2022, 13, 827320. [CrossRef]
- Bourke-Taylor, H.M.; Joyce, K.S.; Morgan, P.; Reddihough, D.S.; Tirlea, L. Maternal and Child Factors Associated with the Health-Promoting Behaviours of Mothers of Children with a Developmental Disability. Research in Developmental Disabilities 2021, 118, 104069. [CrossRef]
- Lewis, S.; Willis, K.; Bismark, M.; Smallwood, N. A Time for Self-Care? Frontline Health Workers’ Strategies for Managing Mental Health during the COVID-19 Pandemic. SSM - Mental Health 2021, 2, 100053. [CrossRef]
- Luis, E.; Bermejo-Martins, E.; Martinez, M.; Sarrionandia, A.; Cortes, C.; Oliveros, E.Y.; Garces, M.S.; Oron, J.V.; Fernández-Berrocal, P. Relationship between Self-Care Activities, Stress and Well-Being during COVID-19 Lockdown: A Cross-Cultural Mediation Model. BMJ Open 2021, 11, e048469. [CrossRef]
- Avasthi, A.; Sahoo, S. Impact, Role, and Contribution of Family in the Mental Health of Industrial Workers. Ind Psychiatry J 2021, 30, S301–S304. [CrossRef]
- Masten, A.S.; Coatsworth, J.D. The Development of Competence in Favorable and Unfavorable Environments. Lessons from Research on Successful Children. Am Psychol 1998, 53, 205–220. [CrossRef]
- Masten, A.S. Resilience Theory and Research on Children and Families: Past, Present, and Promise. Journal of Family Theory & Review 2018, 10, 12–31. [CrossRef]
- Hill, E.J.; Allen, S.; Jacob, J.; Bair, A.F.; Bikhazi, S.L.; Van Langeveld, A.; Martinengo, G.; Parker, T.T.; Walker, E. Work—Family Facilitation: Expanding Theoretical Understanding Through Qualitative Exploration. Advances in Developing Human Resources 2007, 9, 507–526. [CrossRef]
Figure 1.
Display of the significant standardized (STDYX) path coefficients and standard errors (in brackets) of the tested relationships between the model variables (*p < .05; **p<.01 N = 571).
Figure 1.
Display of the significant standardized (STDYX) path coefficients and standard errors (in brackets) of the tested relationships between the model variables (*p < .05; **p<.01 N = 571).
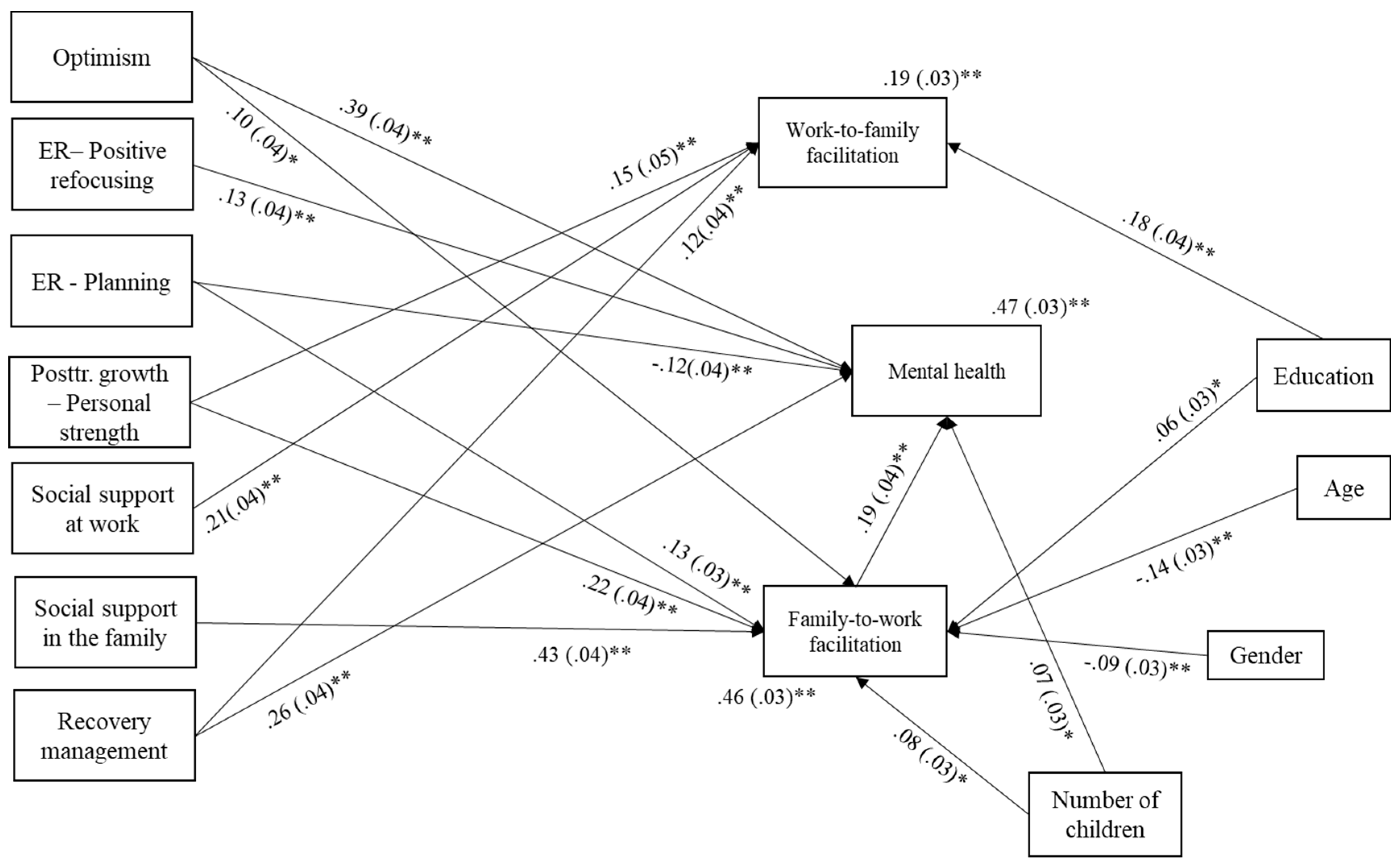

Table 1.
Description of the sample participants (N = 571).
| Characteristics | Descriptive parameters |
|---|---|
| Age | M=40.9, SD=6.15, Min=23 Max=66 |
| Education | Elementary school (N=4); Secondary school (N=237); Bachelor’s degree (N=90) Master’s degree (N=205) Doctoral degree (N=35) |
| Marital status | Extramarital union (N=57) Married (N=450) Separated or divorced (N=46) Single (N=14) Widow/er (N=4) |
| Number of children | Mode=2 (f=267), Min=1, Max=6 |
| Number of children with disabilities | Mode=1 (f=514); Min=1, Max=4 |
| Highest degree of disability among children | 4th ̊- most severe level of impairment (N=204) 3rd ̊ - severe level of impairment (N=158) 2nd ̊ - moderate level of impairment (N=70) 1st ̊ - mild level of impairment (N=35) Do not know/not sure (N=104) |
| Employment sector | Public (N=265) Private (N=306) |
| Partner's employment | Yes (N=463) No (N=24) Caregiver (N=20) |
Table 2.
Descriptive Parameters of the Analyzed Variables (Ntotal = 571).
| N | M | SD | Min | Max | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|---|
| Gender (0-men; 1-women) |
571 | 0.91 | 0.29 | 0.00 | 1.00 | -2.78 | 5.74 |
| Age | 564 | 40.90 | 6.15 | 23.00 | 66.00 | 0.27 | 0.24 |
| Education | 571 | 3.05 | 1.02 | 1.00 | 5.00 | 0.20 | -1.35 |
| Number of children | 571 | 2.20 | 0.99 | 1.00 | 6.00 | 1.05 | 1.57 |
| Optimism | 571 | 3.62 | 0.70 | 1.00 | 5.00 | -0.76 | 1.09 |
| Emotional regulation – Positive refocusing | 571 | 3.24 | 0.86 | 1.00 | 5.00 | -0.26 | -0.09 |
| Emotional regulation – Planning | 571 | 4.05 | 0.64 | 1.00 | 5.00 | -0.62 | 1.34 |
| Posttraumatic growth – Personal strength | 571 | 3.31 | 1.09 | 0.00 | 5.00 | -0.92 | 0.88 |
| Recovery management | 568 | 2.80 | 1.06 | 1.00 | 5.00 | 0.15 | -0.68 |
| Social support at work | 565 | 4.98 | 1.26 | 1.00 | 7.00 | -0.72 | 0.61 |
| Social support in the family | 566 | 5.27 | 1.27 | 1.25 | 7.00 | -0.66 | -0.15 |
| Work-to-family facilitation | 566 | 2.91 | 0.83 | 1.00 | 5.00 | -0.06 | -0.09 |
| Family-to-work facilitation | 563 | 3.41 | 0.82 | 1.00 | 5.00 | -0.27 | -0.03 |
| Mental health | 571 | 3.75 | 0.86 | 1.00 | 6.00 | -0.49 | 0.09 |
Table 3.
Pearson’s Coefficients of Correlations between the Analyzed Variables (N=555; Casewise deletion of missing data).
Table 3.
Pearson’s Coefficients of Correlations between the Analyzed Variables (N=555; Casewise deletion of missing data).
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender (0-men; 1-women) |
-.10 | -.01 | -.04 | .04 | .04 | .06 | .05 | -.15 | -.00 | -.08 | .00 | -.09 | -.09 |
| Age | - | .10 | .12 | -.07 | -.04 | -.05 | -.05 | .09 | -.07 | -.08 | .01 | -.17 | -.04 |
| Education | - | -.15 | -.04 | -.10 | -.01 | -.10 | -.05 | .03 | -.00 | .15 | .00 | -.05 | |
| Number of children | - | .16 | .12 | .09 | .13 | .04 | .05 | .06 | -.02 | .13 | .17 | ||
| Optimism | - | .47 | .34 | .52 | .35 | .36 | .39 | .27 | .45 | .58 | |||
| ER – Positive refocusing | - | .19 | .38 | .23 | .16 | .20 | .17 | .26 | .40 | ||||
| ER – Planning | - | .26 | .05 | .13 | .15 | .11 | .29 | .11 | |||||
| PTG – Personal strength | - | .26 | .22 | .25 | .25 | .42 | .44 | ||||||
| Enjoying time for self | - | .32 | .38 | .26 | .29 | .46 | |||||||
| Social support at work | - | .48 | .33 | .35 | .29 | ||||||||
| Social support in the family | - | .18 | .56 | .42 | |||||||||
| Work-to-family facilitation |
- | .35 | .18 | ||||||||||
| Family-to-work facilitation |
- | .42 | |||||||||||
| Mental health | - |
Note. Correlations in bold are significant at the p <.05 level. ER – emotional regulation; PTG – posttraumatic growth.
Table 4.
Standardized (STDYX) Parameter Estimates, Standard Errors and Significance Levels for the examined Model Paths and Correlations not shown in Figure 1 (N=571).
Table 4.
Standardized (STDYX) Parameter Estimates, Standard Errors and Significance Levels for the examined Model Paths and Correlations not shown in Figure 1 (N=571).
| Model relationship | Standardized estimate (STDYX) | Standard error (STDYX) | Two-tailed p-value (STDYX) |
|---|---|---|---|
| Non-significant path coefficients | |||
| Optimism → Work-to-family facilitation | .090 | .050 | .084 |
| Work-to-family facilitation → Mental health | -0.073 | .037 | .051 |
Table 5.
Non-standardized Estimates of the Indirect Effects.
| Indirect effects: | Non-standardized estimates of the indirect effect | 95% confidence interval (k=1000) |
|---|---|---|
| Optimism → Family-to-work facilitation → Mental health | 0.020 | 0.005 ; 0.046 |
| Emotional regulation: Planning → Family-to-work facilitation → Mental health | 0.042 | 0.019 ; 0.074 |
| Posttraumatic growth: Personal strength → Family-to-work facilitation → Mental health | 0.041 | 0.021 ; 0.069 |
| Social support in the family → Family-to-work facilitation → Mental health | 0.070 | 0.040 ; 0.105 |
Note. k – Number of bootstrapped samples.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



