
Submitted:
28 May 2023
Posted:
31 May 2023
You are already at the latest version
Abstract
Background: Although Tuberculosis (TB) is one of the oldest diseases known to mankind, many practitioners are still unaware of various aspects of management of TB including drug resistant TB. To be able to make an impact on the disease burden we need to understand the knowledge, attitude and practices (KAP) of practitioners, both in government and private sector, towards TB case management. Methodology: A random cross-sectional survey of 99 respondents to assess the KAP towards TB case management using a digital semi-structured questionnaire which was pre-tested and administered to allopathic practitioners from across States in North and Central India. Results: 77% responders were government doctors and 23% were private practitioners. Chest physicians accounted for 61% of the responders. 26% of government and 78% of private doctors relied on sources which are difficult to validate for their knowledge on drug resistant TB management. There were large variations seen in knowledge on modes of transmission, standard precautions, extent of drug resistant TB, diagnostics as well as treatment regimen for drug resistant TB. Conclusion: The knowledge of both sector doctors especially amongst private practitioners with respect to the awareness of extent, diagnosis, and treatment and infection control measures for drug resistant TB is suboptimal which translates to poor diagnostic, therapeutic and infection control choices amongst private practitioners. If India has to achieve the targets for TB Elimination by 2025, serious work needs to be done to upgrade the knowledge of the private sector doctors on drug resistant tuberculosis. The Ministry of Health and Family Welfare, GoI needs to have regular educational programs for the private practitioners coupled with awareness campaigns and frequent surveys to assess the knowledge, attitude and practices being followed in the private sector for TB management including drug resistant TB.
Keywords:
Tuberculosis
; Drug Resistant
; Management
; Awareness
BACKGROUND
Tuberculosis (TB), one of humanity's oldest diseases, is one of the top 10 causes of death worldwide. It is a bacterial infection caused by Mycobacterium tuberculosis. It mostly affects the lungs (Pulmonary TB) however it can also affect other body organs [1]. About a quarter of the world’s population is infected with M. tuberculosis [18]. India has the world's largest tuberculosis (TB) epidemic, accounting for 23% of global incident active TB patients and 27% of global "missing" patients, or about 1 million patients per year who have not been notified to the Government of India's Revised National TB Control Programme (RNTCP) [2].
According to a study based on data from the National Family Health Survey (NFHS-4), the self-reported incidence of tuberculosis in India is 304/100,000 people [4]. Anti-TB medicines have been used for decades and strains that are resistant to one or more of the medicines have been documented in every country surveyed. Drug resistance emerges when anti-TB medicines are used inappropriately, through incorrect prescription by health care providers, poor quality drugs, and patients stopping treatment prematurely [19]. Extensively Drug Resistant TB (XDR-TB) is primarily an iatrogenically induced problem, and understanding the epidemiological and risk factors associated with it is critical to combating this scourge [3]. African autopsy studies confirm the high prevalence of undiagnosed tuberculosis, subclinical tuberculosis, and tuberculosis comorbidity with HIV, pyogenic pneumonia, and other infectious and non-communicable diseases. This unacceptable state of affairs indicates that current approaches to diagnosing, treating, managing, and preventing tuberculosis are inadequate and must be reconsidered [5].
To enable adequate identification and treatment of TB including drug resistant TB, an understanding of the Knowledge, Attitude and Practices (KAP) of practitioners both in the government and private sectors is paramount as it can form the basis of informed planning for training programs and guide the national program towards TB Elimination.
OBJECTIVES
- (1)
- To assess practitioners’ knowledge, attitudes and practices (KAP) in the diagnosis and management of drug resistant TB patients in both the government and private sectors.
- (2)
- To assess practitioners' perspectives on strengthening the National TB Elimination Programme (NTEP) with respect to knowledge and awareness regarding drug resistant TB.
METHODOLOGY:
The study is a random cross-sectional survey through a digitally administered predesigned, pre-tested semi-structured questionnaire.
The data collection was done during the active phase of the Covid Pandemic (October 2020 – October 2021), therefore the questionnaire was shared through WhatsApp to various physicians’ groups covering maximum specialities.
Questions pertaining to the following areas were elicited in the questionnaire:
- Drug resistant TB: its transmission and extent of problem
- Case definition/ diagnosis of drug resistant TB
- Treatment of drug resistant TB
- Infection control practices & XDR-TB
Inclusion criteria included the complete responses from allopathic doctors who had at least completed MBBS from the States in North and Central India was accepted for evaluation. Data analysis done using descriptive statistics including frequencies, percentages and proportions. A total of 106 responses were received. After data cleaning and applying the inlcusion and exclusion criteria a total of 99 responses were accepted for analysis.
The analysis is shown below with a breakup between the doctors in public and private sector as the responses were starkly different between the two groups.
Responder Demographics:
- 76.7% (76) and 23.3% (23) doctors were from the Government and private sector respectively.
Speciality wise breakup is given in Table 1:
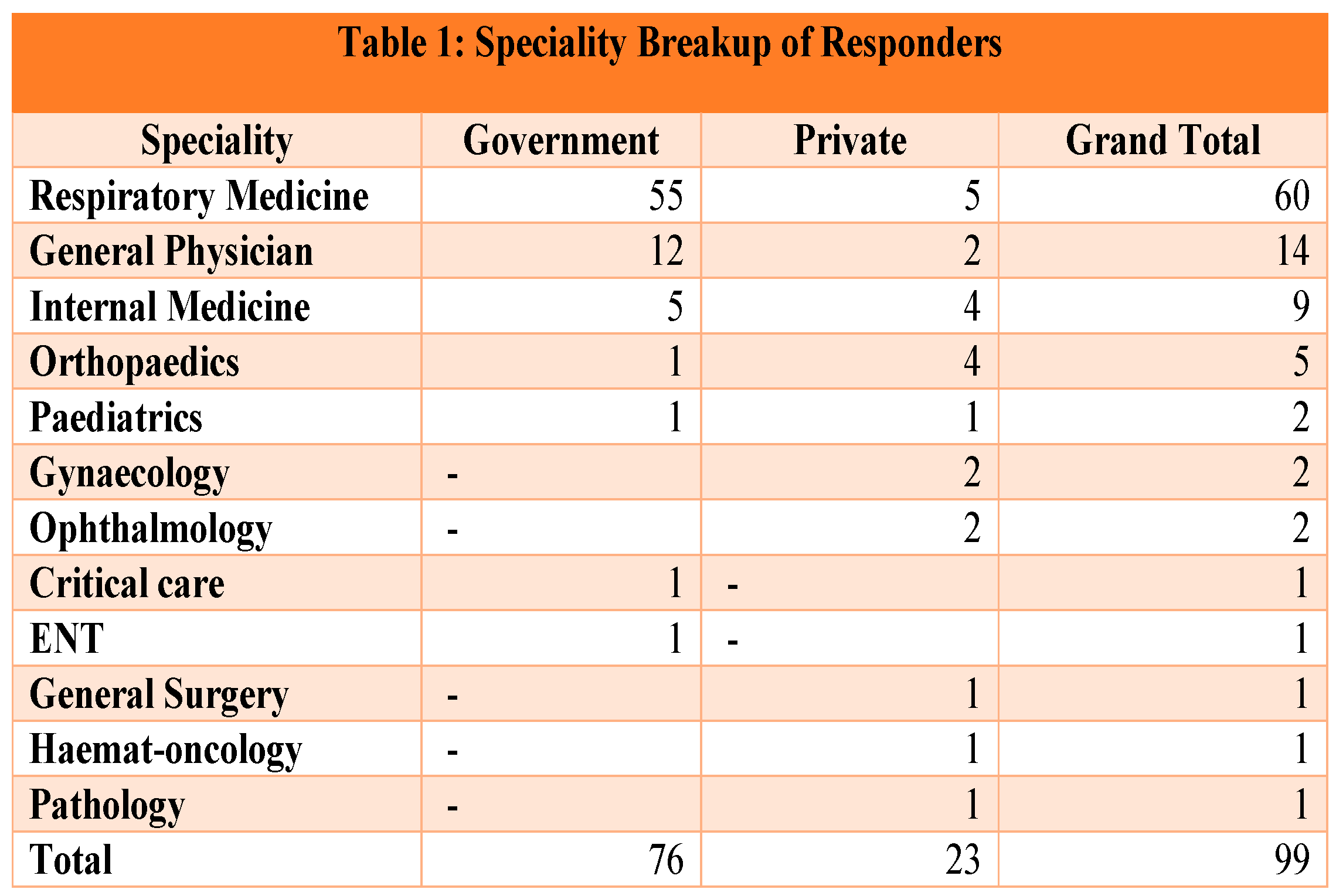
Majority of responders were Respiratory Medicine specialists (61%). From the private sector the responders were more spread out among specialities.
The States represented were Delhi (51), Madhya Pradesh (9), Haryana (8), Rajasthan (7), Punjab (6), Uttar Pradesh (6), Gujarat (5), Maharashtra (3), Uttarakhand (1), Himachal Pradesh (1), Chandigarh (1) and Jharkhand (1).
RESULTS:
Main source of Information for Drug Resistant TB:
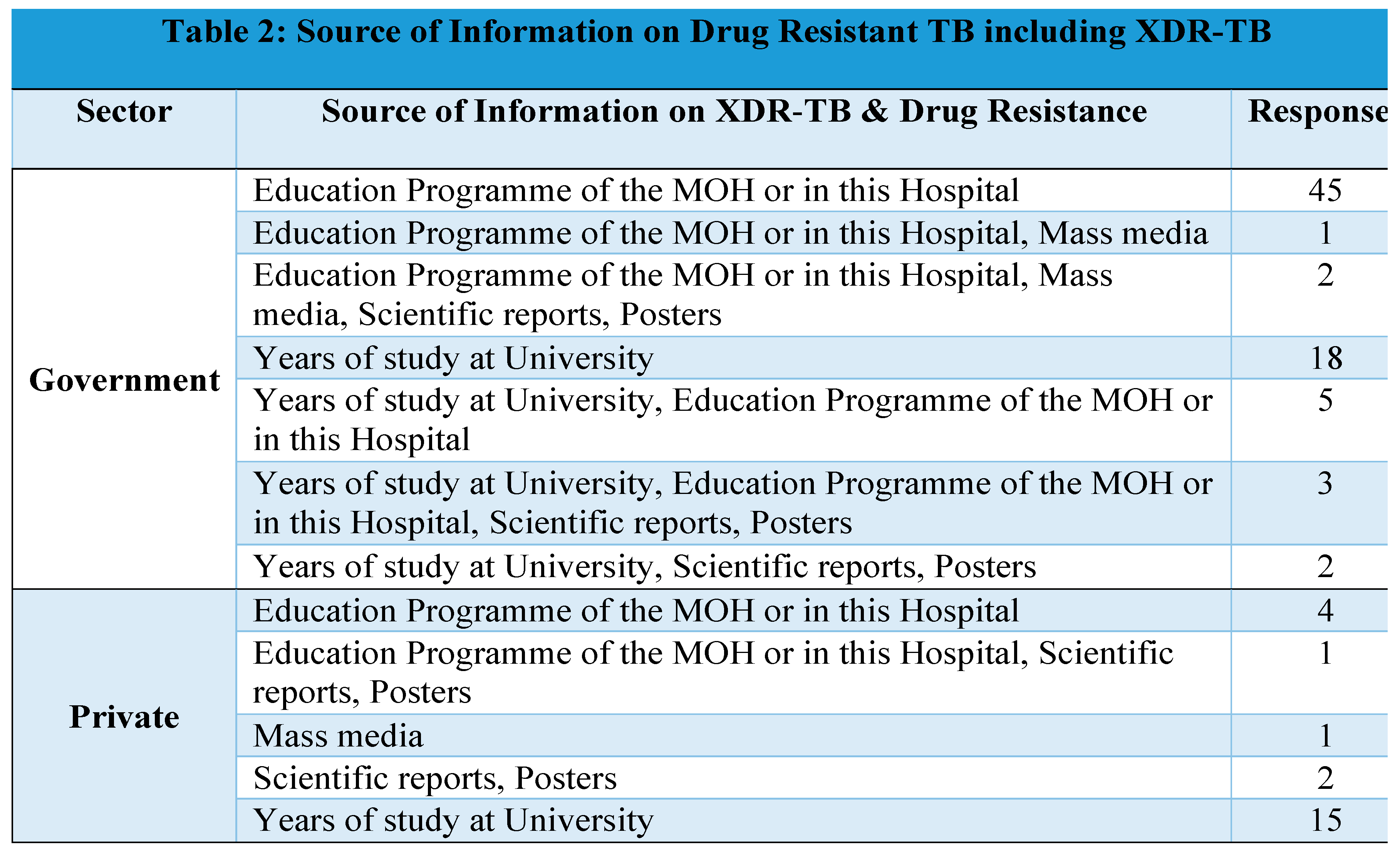
Though there are multiple sources of information for the doctors for updated knowledge on drug resistant TB. The major sources were as below:
- Government doctors: Educational Program of MOH/ their hospitals
- Private doctors: Learnings at the University
This indicates lack of uniformity in updated knowledge as well as warrants an urgent need for educational programs for the private doctors on drug resistant TB.
Proportion of doctors treated MDR: While 58% (44/76) of public sector doctors had treated MDR-TB patients, more than 61% (14/23) of private sector doctors had not treated any MDR TB cases.
The results are segmented into 4 categories as below:
- Drug resistant TB: its transmission and extent of problem
- Case definition/ diagnosis of drug resistant TB
- Treatment of drug resistant TB
- Infection control practices & XDR-TB
- A.
- DRUG RESISTANT TB: ITS TRANSMISSION AND EXTENT OF PROBLEM:
Transmission of XDR-TB:
- Role of environment: The doctors uniformly agreed that there is a major role of environmental cleanliness and overcrowding in spreading XDR TB
-
Mode of Transmission: 56% believe XDR-TB spreads through droplet spread. 37% were of the opinion that XRD TB is an airborne infection.
- ○
- Government Doctors mainly said it is spread by droplet infection, whereas private sector doctor’s opinion was divided among the available options.
- ○
- Surprisingly 1/7th (14%) of the respondents also belive that it is spread through indirect contact or water borne.
- ○
- The variety of responses suggest lack of clarity regarding the mode of transmission espeically when it comes to multidrug resistant TB.
-
Role of improper medication:
- ○
-
Almost all the respondents correctly identified that improper intake of TB medication increases the risk of XDR-TB.

Knowledge on Prevalence & Extent of Problem:
- 60% of the public sector and 83% of the private doctors believe that XDR-TB is not common in India.
-
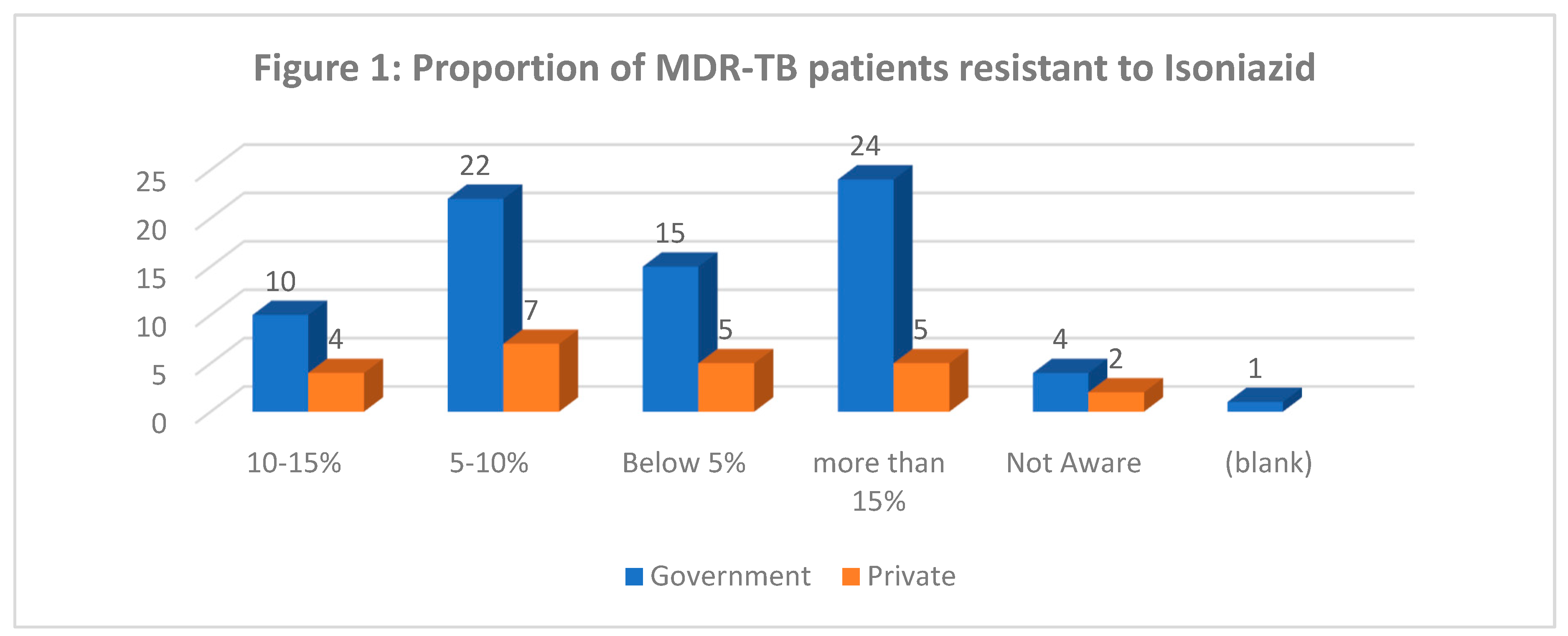
31 % Government doctors think that more than 15 % patients of MDR-TB patients are resistant to isoniazid, whereas 29% private doctors think only 5-10% MDR-TB patients are resistant to isoniazid (Figure 1)
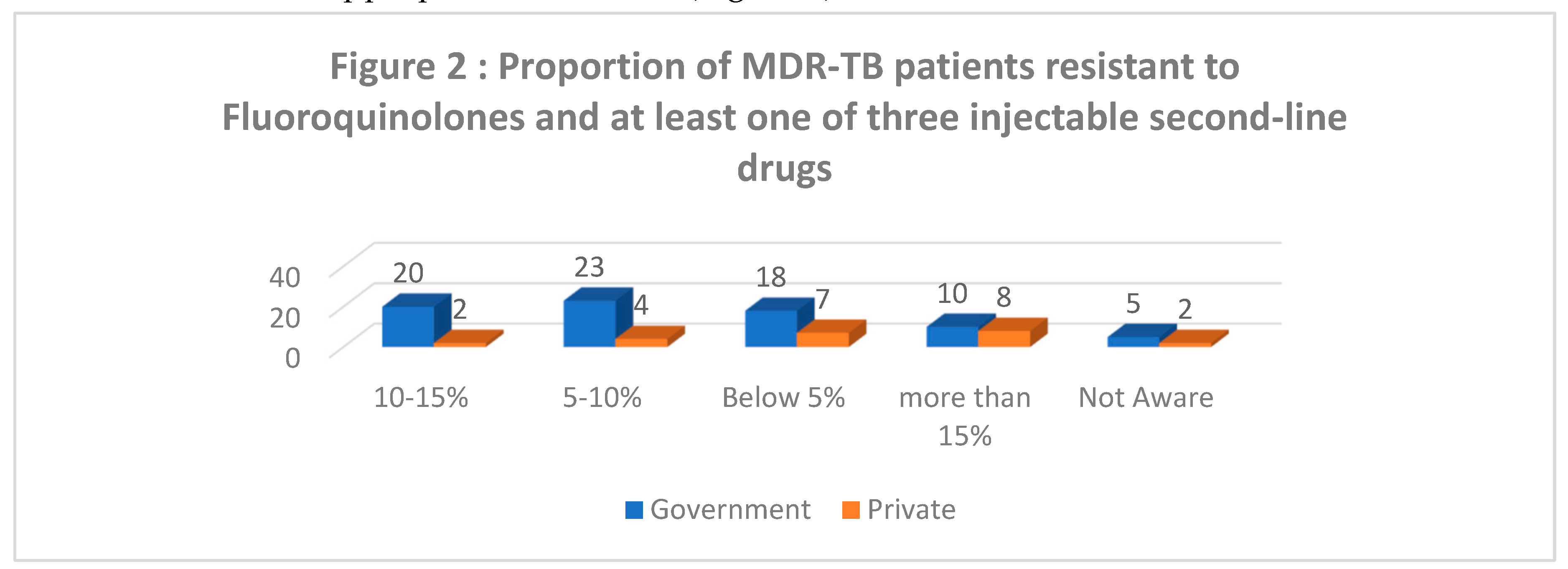
Awareness regarding drug resistance for multiple second line drugs shows a lot of variation indicative of lack of appropriate awareness (Figure 2).
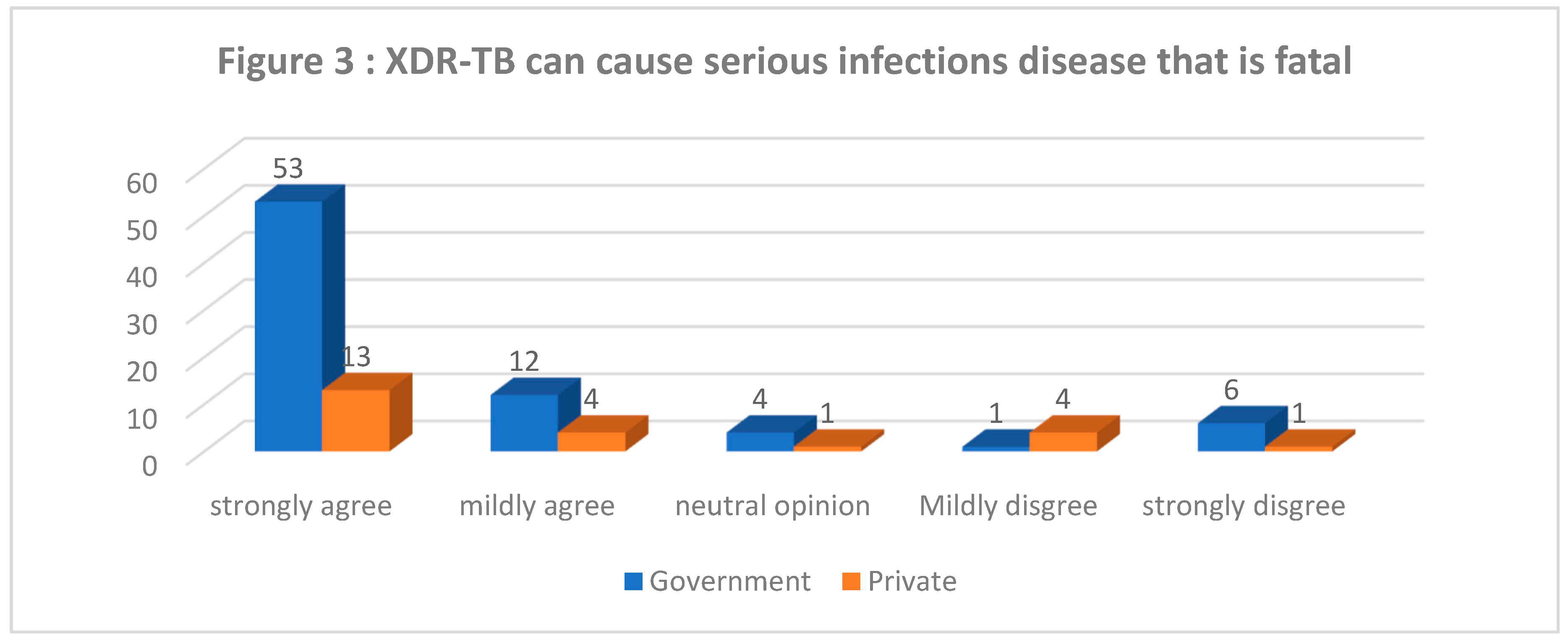
- Nature of XDR-TB infections (Figure 3): 70% government doctors and 64% private doctors strongly agree that XDR-TB can cause serious infections disease that is fatal
-
Felt Need for Raising Awareness:
- ○
- Almost all the doctors (98% - 97/99) feel the need for increased awareness among the community regarding XDR-TB.
- ○
-
All the doctors felt the need for continuing medical education of practitioners on recent advances in the field of XDR-TB control.
In recent years XDR-TB has emerged as a new challenge in TB management in many countries including India. Its incidence in India is still largely unknown because of a lack of national surveillance due to unavailability of universal drug sensitivity testing [6] as well as lack of adequate dissemination of knowledge among medical fraternity.
- B.
- CASE DEFINITION/ DIAGNOSIS OF DUG RESISTANT TB:
-
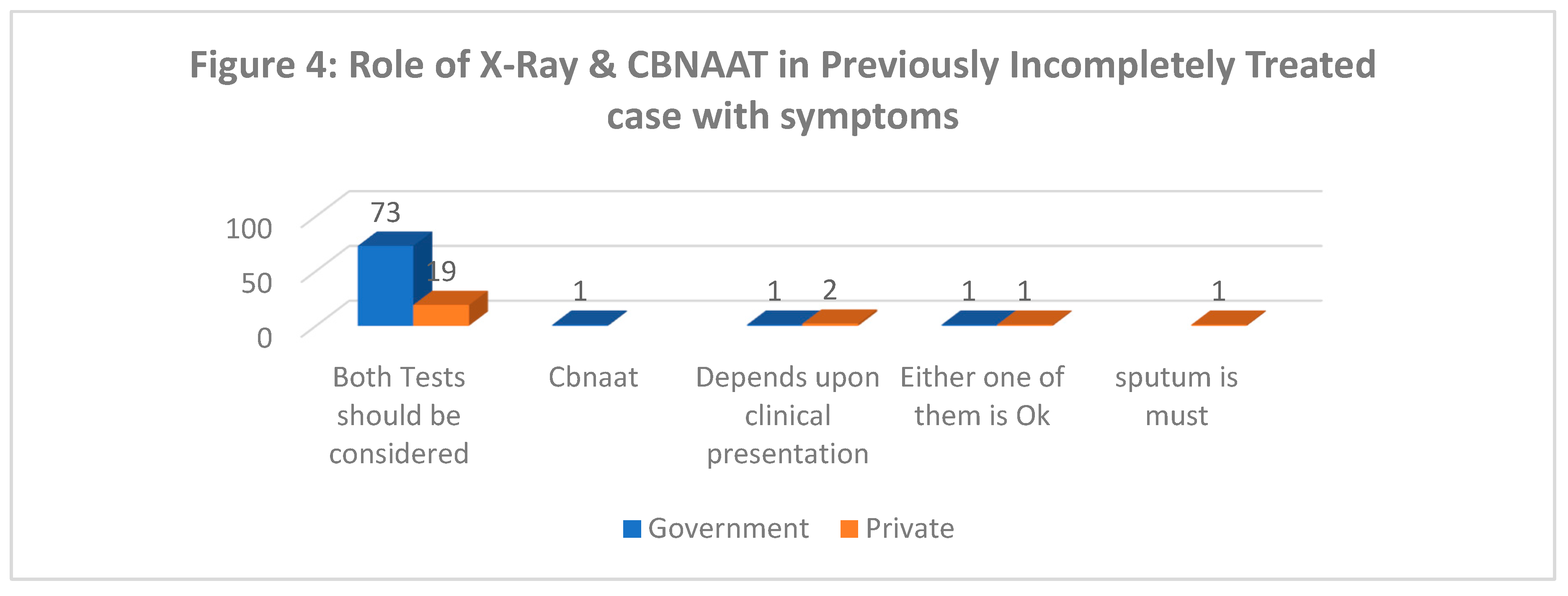
Role of X-Ray and CBNAAT in diagnosis of TB in a symptomatic patient of incompletely treated TB (Figure 4): 96% government and 79% private doctors think that X-ray has a supportive role in diagnosis of TB and that both X-Ray and CBNAAT should considered.
-
Case definition of XDR-TB:
- ○
- 84% of government and 96% private doctors were correctly able to identify the case definition of XDR-TB.
- ○
- Overall, 13% of doctors were unable to give correct case definition which could lead to missing of possible XDR suspect.
- ○
- Operational case definition used: Resistance to Rifampicin and Isoniazid, plus any Fluoroquinolone and at least one of three injectable second-line drugs i.e., Amikacin, Kanamycin, or Capreomycin
-
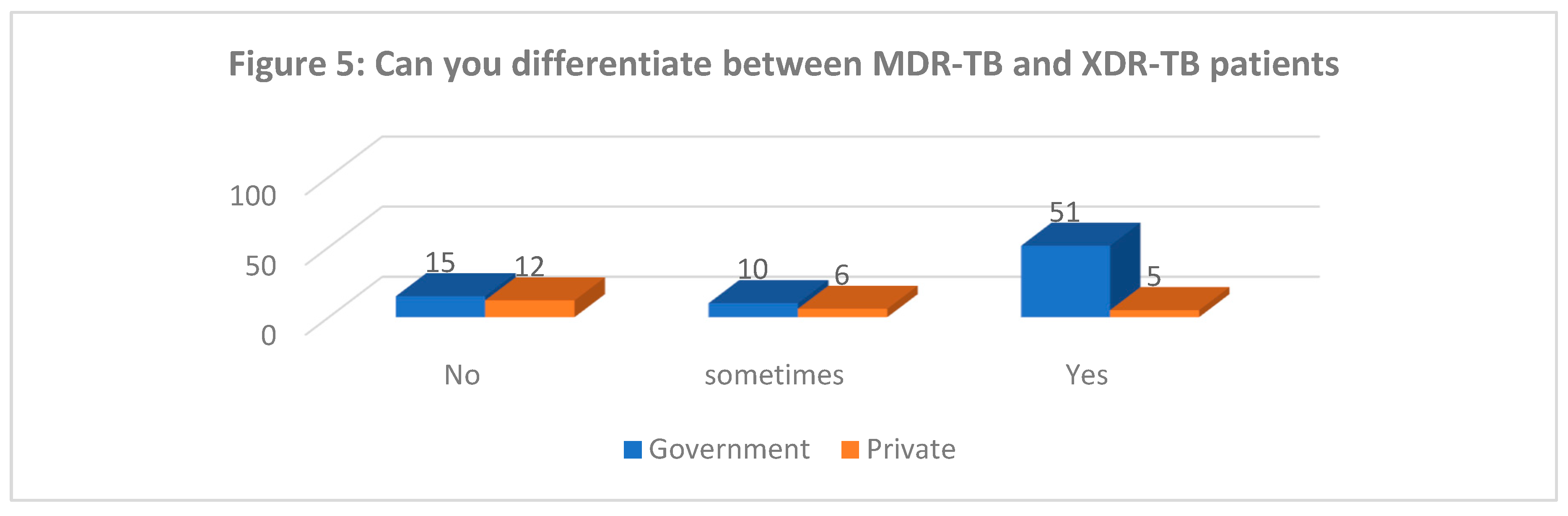
Differentiating between MDR and XDR TB (Figure 5): Majority of private doctors and almost 1/6th of government doctors felt they are unable to differentiate between MDR and XDR TB.
- Getting Cultures done for XDR Suspects: While all Government doctors were sending cultures for XDR suspects a small proportion (13%) of private practitioners even when suspecting XDR-TB do not send for cultures prior to treatment.
-
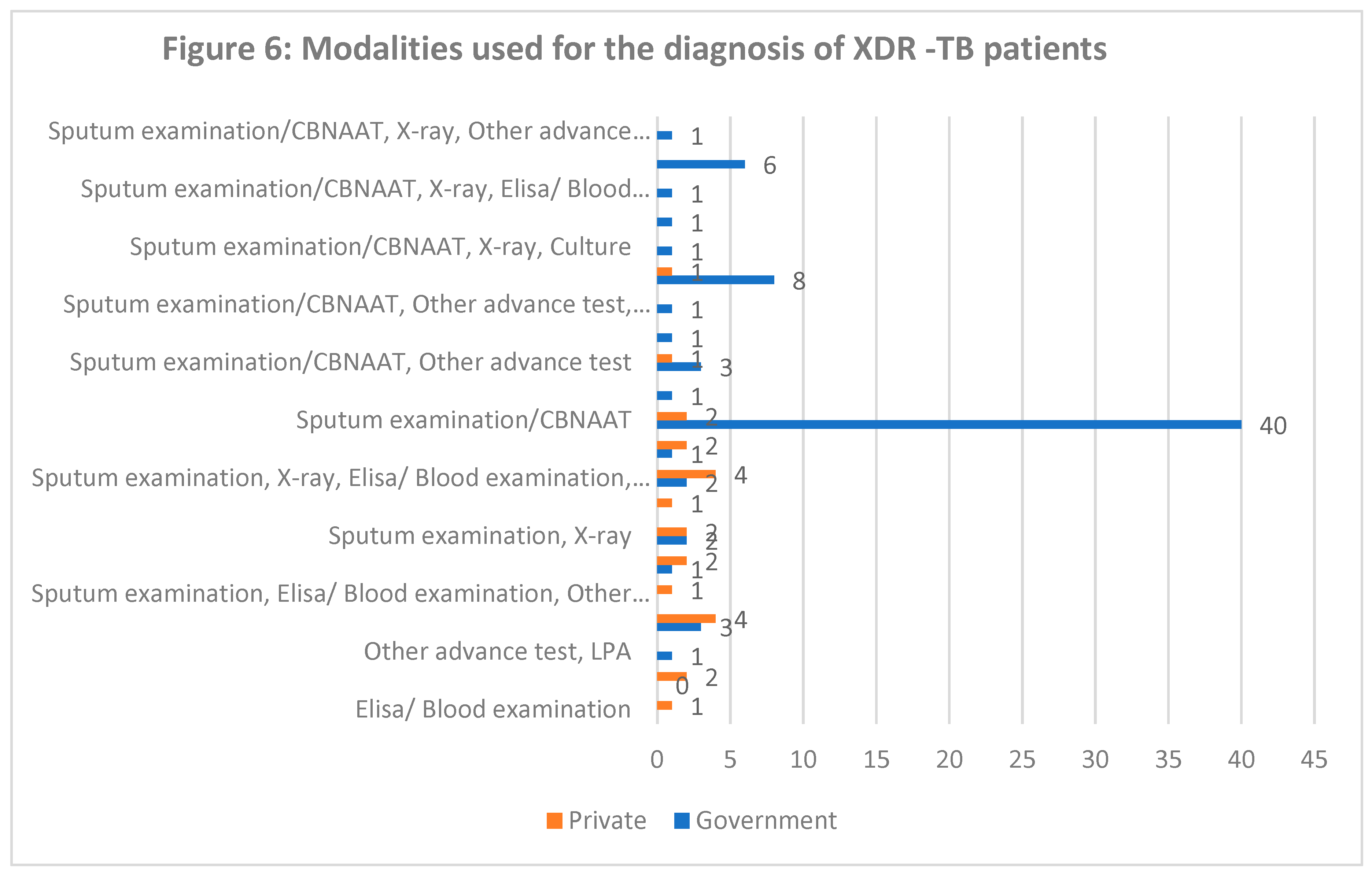
Diagnostics Used for XDR-TB (Figure 6): A Wide variation can be seen in the options for diagnosing XDR-TB with many limiting to Sputum examination, CBNAAT or even X-Ray. Only 1/3rd of the respondents identified advanced tests beyond these above tests for diagnosing XDR-TB.
We can see that despite having knowledge about case definition of XDR-TB a good proprotion of practitioners expressed inability to differentiate between MDR and XDR TB as well as a small proportion is not using advanced tests for XDR diagnosis.
- C.
- TREATMENT OF DRUG RESISTANT TB:
-
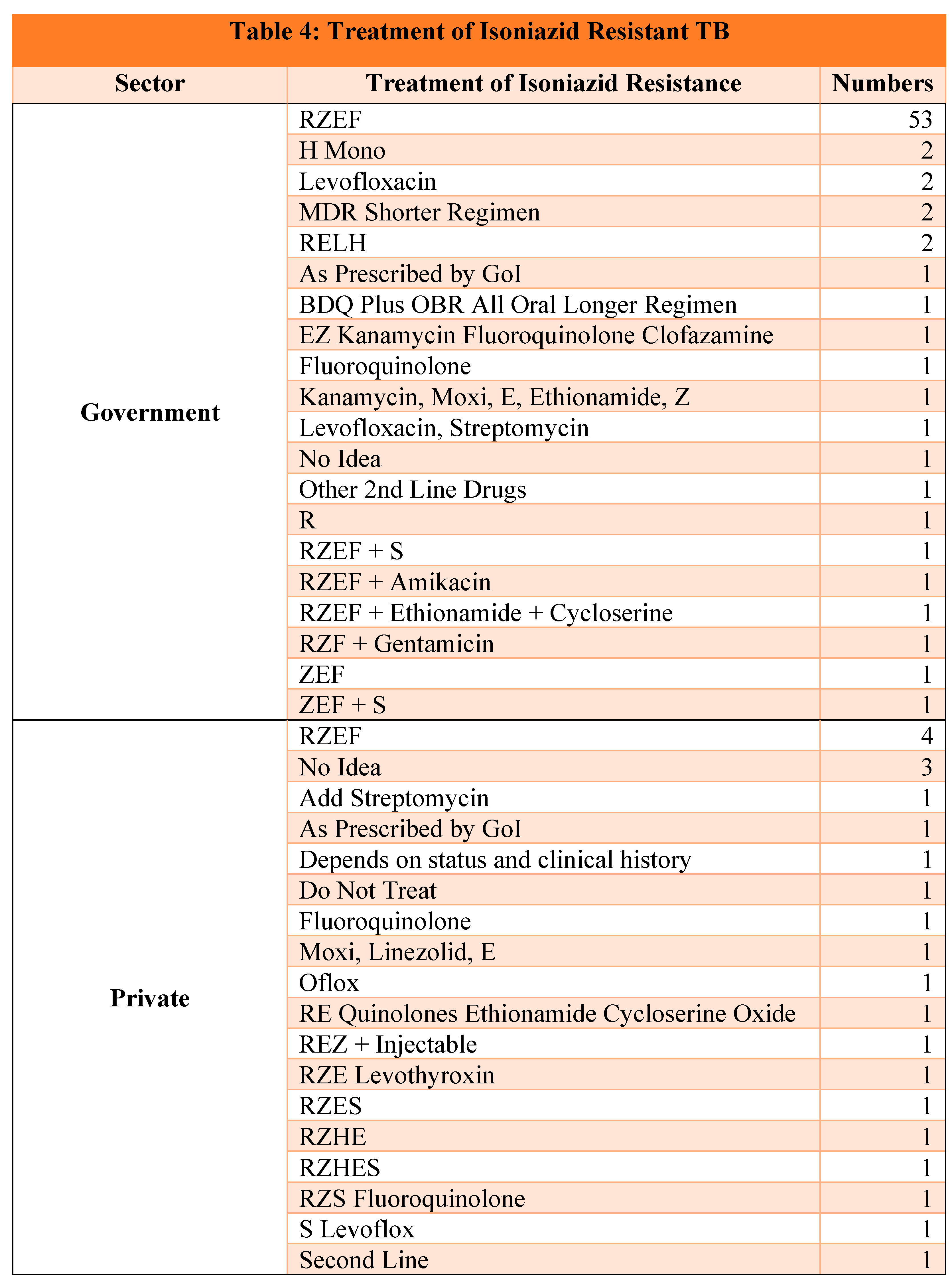
Treatment of Isoniazid Resistant TB (Table 4): On one hand 70% of the government doctors were able to correctly identify the combination of Rifampicin, Pyrazinamide, Ethambutol and Fluoroquinolone as the treatment of choice for Isoniazid resistant TB, on the other hand only 17% of private doctors were able to do so and there was a lot of variation in their treatment choices which is a clear indicator of low awareness regarding drug resistant TB treatment.
-
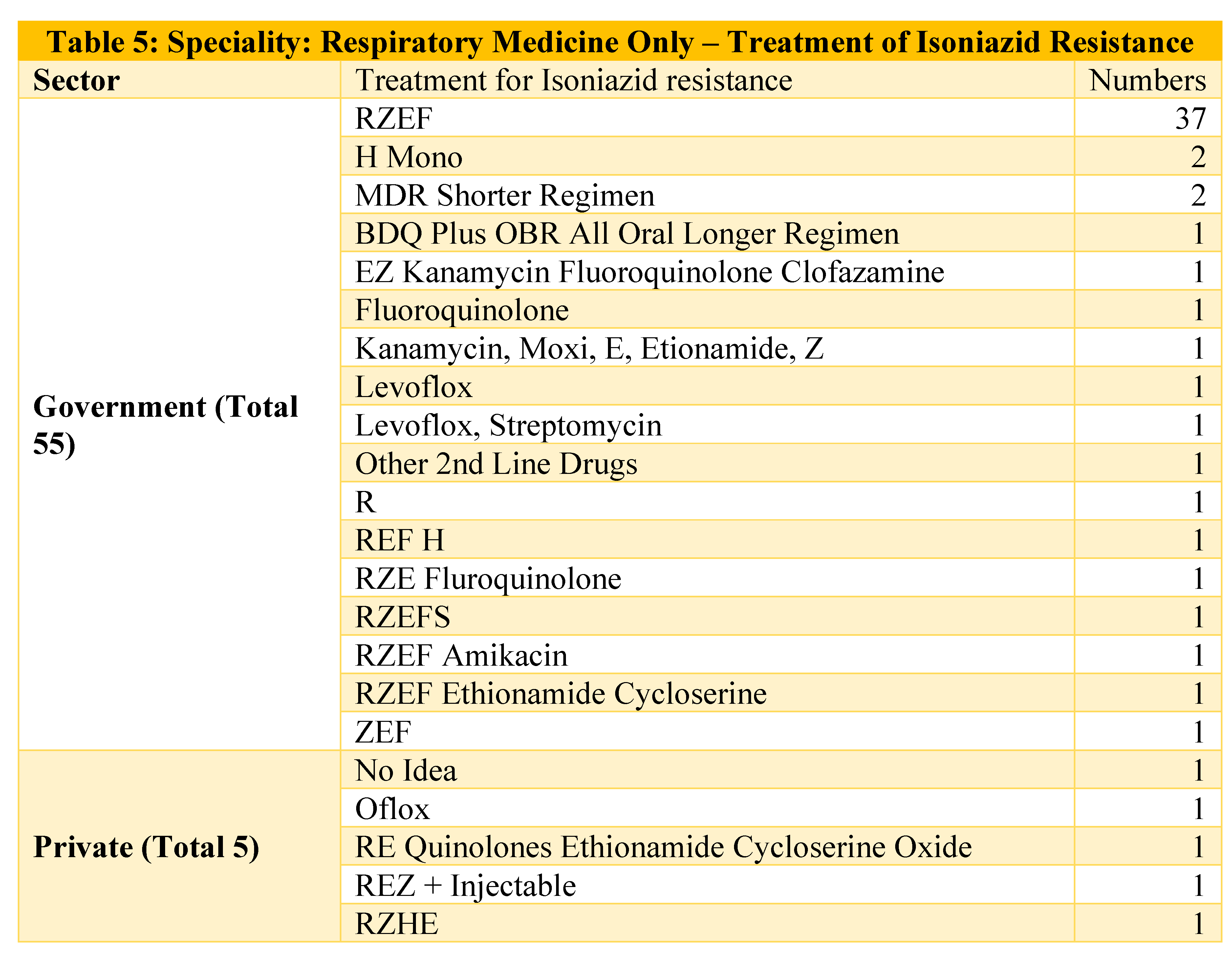
Even when we see the options given by Respiratory Medicine specialists we see a wide variation in the responses. (Table 5)
-
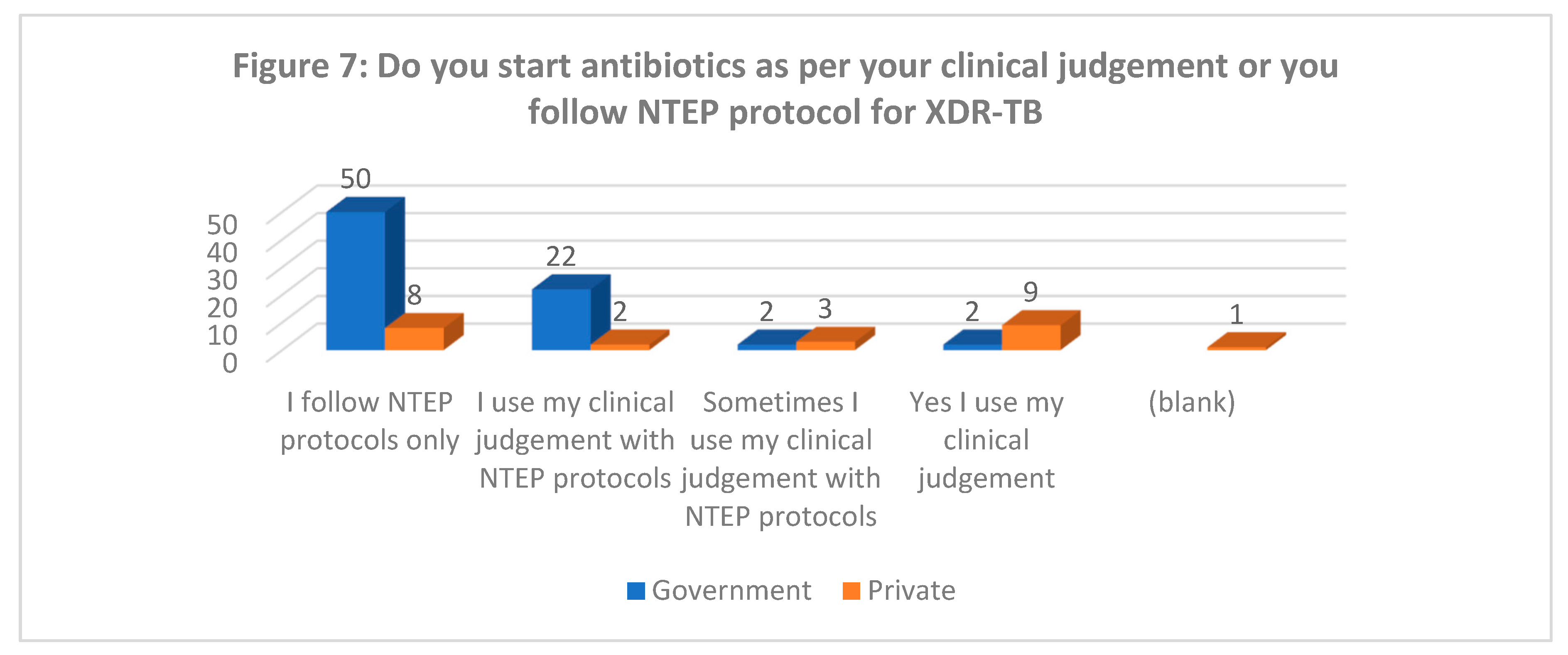
Whether following standardized regimen (Figure 7): Although majority (95%) of government doctors follow NTEP prescribed regimen for treating XDR-TB, the private doctors were divided in their treatment choices with almost similar (~40%) each following NTEP regimen or follow their own clinical judgement. This is similar to the various regimen found in various studies for treatment of TB [16].
-
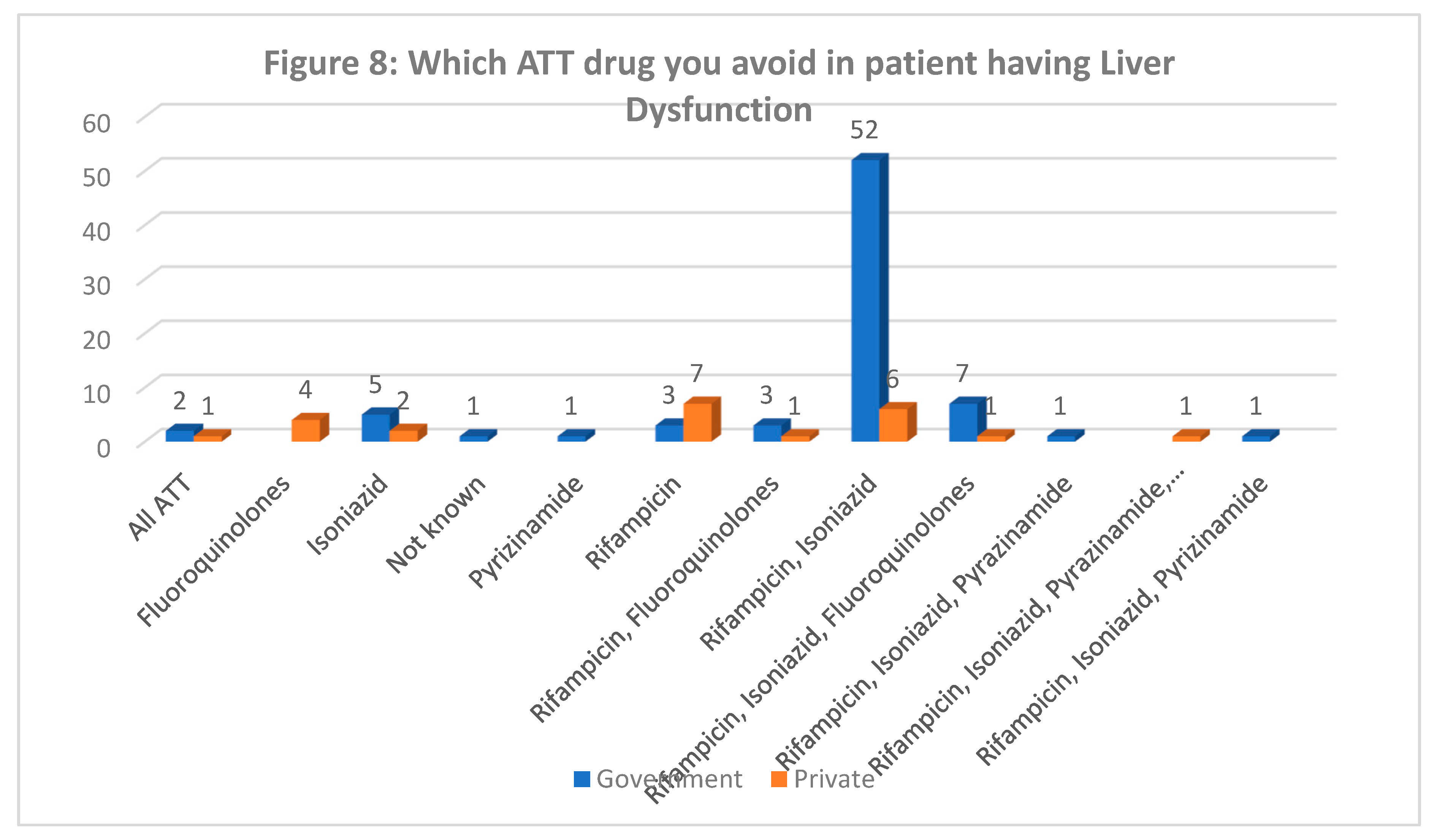
Drugs to be used in Liver Dysfunction (Figure 8): While 68% government doctors identified rifampicin and isoniazid to be avoided in liver dysfunction, the opinion was divided in the private sector doctors which points to reduced awareness among private doctors as compared to government doctors.
- D.
- INFECTION CONTROL PRACTICES & XDR-TB:
-
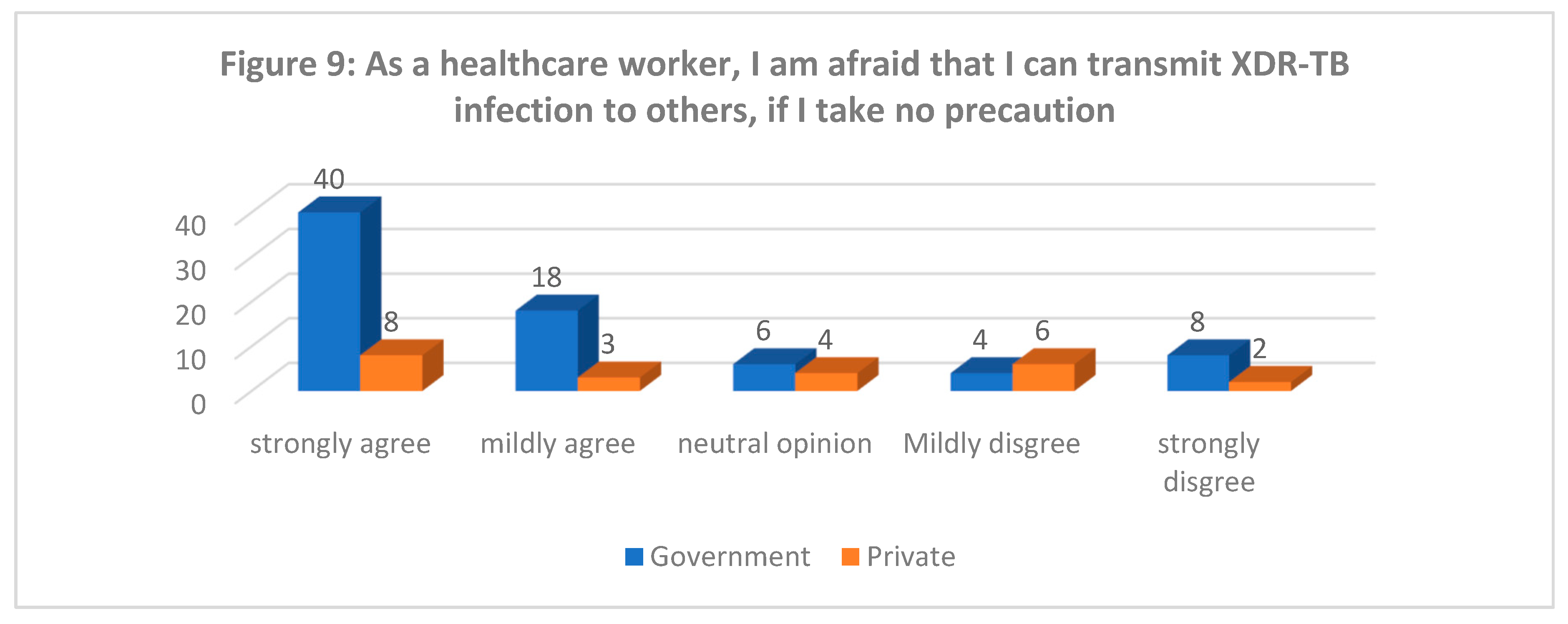
Risk as a Healthcare Worker (Figure 9): 53% government and 35% private doctors strongly agree that until they take precautions, they can transmit XDR infection to others.
Standards Precautions for XDR-TB Prevention:
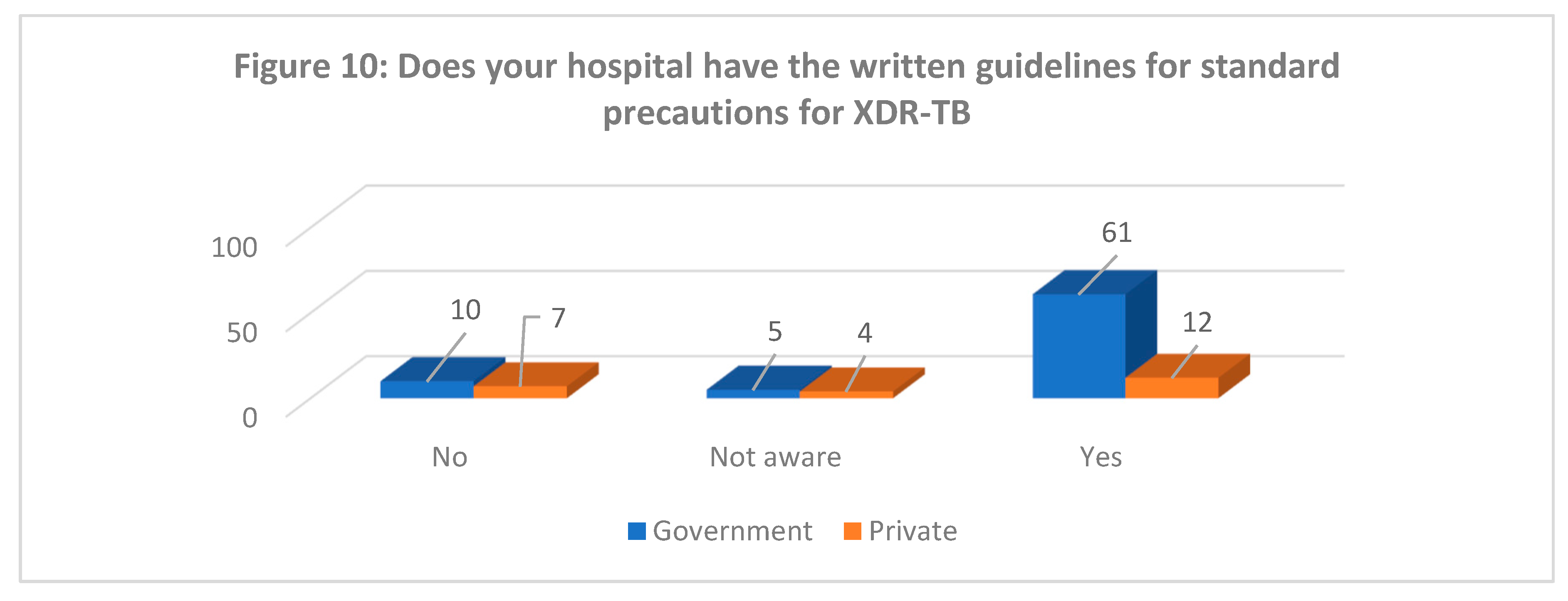
Availability of Guidelines for Standards Precautions (Figure 10): While most government hospitals doctors (80%) know about the written down guidelines for standards precautions for XDR-TB in their hospital, only half (51% of doctors) in private sector was aware about it.
- ○
- Knowledge of Standard Guidelines for XDR-TB prevention: Majority (83%) of the Government and 57% of private doctors pointed out correctly the standard precautions to prevent transmission.
- ○
- Use of Personal Protective Equipment (PPE) while dealing with XDR (Figure 11): 61% and 54% of government and private doctors respectively informed regarding routinely using PPE while dealing with XDR patients.
- ○
-
Isolation of XDR-TB from other patients: While 91% of government doctors said they isolate XDR-TB patients, only 58% private doctors did so.

-
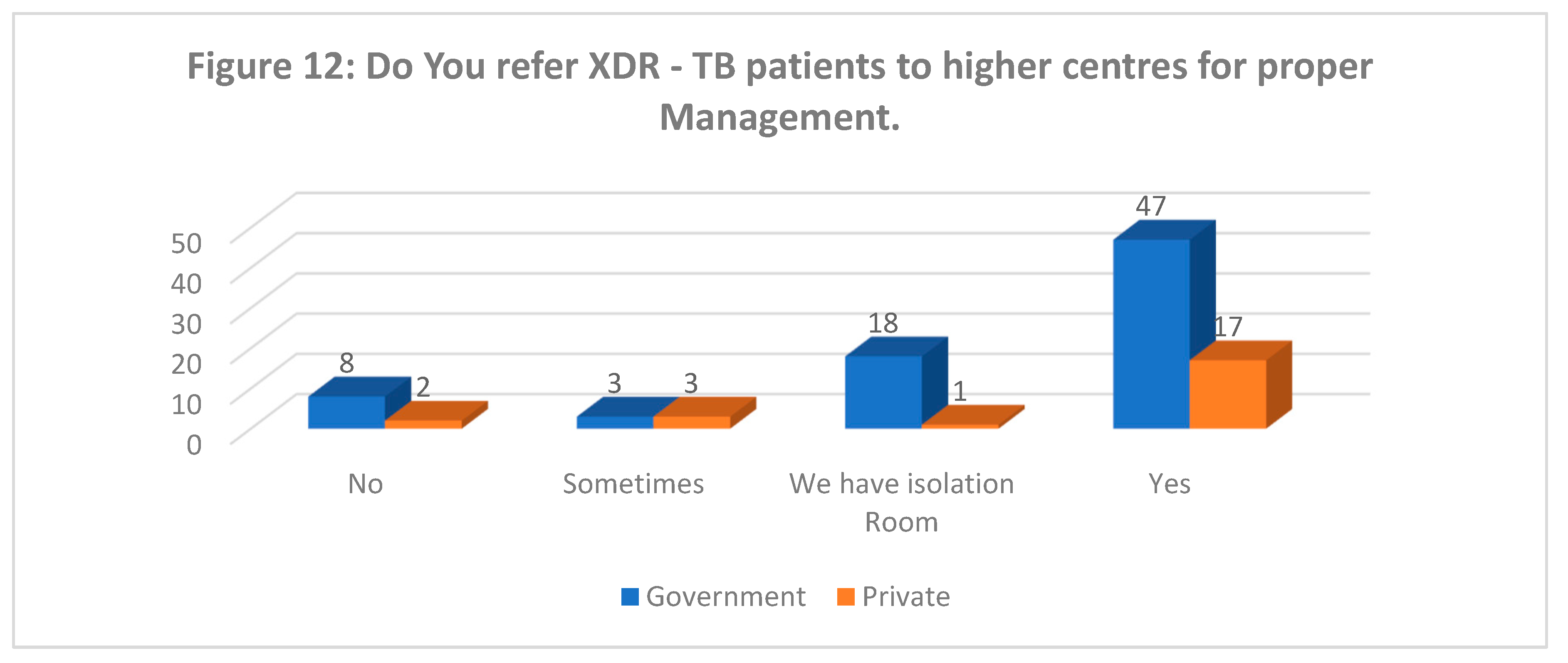
Referral to higher centre for management of XDR-TB (Figure 12): Despite understanding the risk associated with XDR-TB few doctors (10%) still do not refer these patients to higher centres for management even though they may not have isolation facilities available in their hospital.
DISCUSSION:
Sources of information for drug resistant TB:
The majority of private sector doctors 18/23 (78%) said that their primary source of information was other than the one provided by the Ministry of Health. Even 20/76 (26%) of government doctors said that their primary source of information regarding drug resistant TB including XDR-TB was other than Ministry of Health education program. For these doctors the main source included primarily learning during the university and other meetings, posters and mass media. Overall, 58% of government and 39% of private doctors had earlier treated MDR-TB patients.
Considering India’s commitment towards TB Elimination by 2025 and that more than 1/3rd of all TB patients being treated by the private sector [20] it would be paramount that these private physicians be actively involved in educational programs for the upgradation of knowledge regarding TB with specific focus on drug resistant TB.
- A. Drug resistant TB: its transmission and extent of problem
A large variation was observed amongst the responses for the mode of spread of XDR-TB which included options like airborne, direct or indirect contact and water borne for 61% of private doctors and 40% of government doctors.
Almost all the doctors agree on the role of proper medication for reducing XDR-TB and believe that improper medication leads to XDR-TB.
Awareness regarding extent of the disease as well as the prevalence of Isoniazid resistance and fluroquinolone and second line injectable resistance in MDR TB patients was also low. This is in line with what was identified more than a decade ago in Pune by Tushar et.al. [21]
53/76 (70%) of government and 13/23 (57%) of private doctors opined that XDR-TB was a serious threat and had fatal consequences. 53% and 35% of government and private doctors respectively believe that as healthcare workers they may transmit XDR—TB to others.
All the doctors agreed that there should be awareness regarding XDR-TB in the community and also 98% of doctors agreed that there need to be more educational program for updation of knowledge of doctors on XDR-TB management.
Considering that India has about half a million “missing” cases every year that are not notified and remain undiagnosed or unaccounted for as well as being inadequately diagnosed and treated in private sector [17], this is a cause for alarm since a vast majority of cases initially reach the private sector for management due to various reasons.
If India has to achieve the targets for TB Elimination by 2025 it needs to give a serious look into increasing educational programs by the Ministry of Health for private sector doctors as well as many doctors within the government system who are still not covered by such training programs. Involvement of the Indian Medical Association which has been active partner for the NTEP over the years in increasing the knowledge of private practitioners on drug resistant TB could go a long way in improvement of the current status. [22]
- B. Case definition/ diagnosis of drug resistant TB
96% government and 76% private doctors identified that both CBNAAT and X-rays have a role in diagnosing TB in a previously incompletely treated case of TB. The situation has definitely improved over the years in many areas especially through the involvement of NGOs who connect the private practitioners with the rapid diagnostic tests like The EQUIP Public-Private Model in Chennai, India [24], whereas the situation remains the same in many areas [23].
Although 96% of private doctors were able to correctly identify the case definition of XDR-TB but when it comes to practice 57% of then stated that they were not able to differentiate between MDR-TB and XDR-TB. Also, despite knowledge that they need to have drug susceptibility testing done to identify XDR-TB 13% of private doctors do not send for cultures for suspected XDR-TB cases.
Only 1/3rd of the doctors was able to correctly identify that advanced tests were required to diagnose XDR-TB. There was a wide variation in the options for diagnosing XDR-TB with many limiting to Sputum examination, CBNAAT or even X-Ray.
This calls for an immediate focus on increasing the capacity of private sector to correctly identify and test for drug resistant TB alongwith access to the advanced tests for their patients.
- C. Treatment of drug resistant TB
For the treatment of standalone isoniazid resistant TB there were more than 15 treatment protocols given by the private sector with only 4/23 (17%) answering for the rifampicin, pyrazinamide, ethambutol and fluoroquinolone (RZEF) regimen. Even in the government sector there were more than 15 regimen being used with 53/76 (70%) using the RZEF regimen.
37/55 (67%) of government chest physicians used the RZEF regimen with more than 15 other regimens being used. The 5 chest physicians in the private sectors all had different regimens.
Government doctors mainly use NTEP regimen for treatment of XDR-TB, whereas the private doctors were divided in their treatment choices with almost similar (~40%) each following NTEP regimen or follow their own clinical judgement. This is similar to the various regimen found in various studies for treatment of TB in the private sector in Mumbai by Udwadia et.al. [16].
Many practitioners mainly private doctors were unable to identify the drugs not to be used in liver dysfunction which by itself has serious ramifications for treatment of patients with liver failure or dysfunction.
The variations in treatment regimen and inability to identify hepatotoxic drugs is another call for increased awareness and education programs for private doctors.
- D. Infection control practices & XDR-TB
Only half of the private doctors knew about availability of standard guidelines for precautions for XDR-TB in their hospital.
Despite having knowledge of infection control measures for XDR-TB 57% of private doctors do not wear appropriate PPEs while caring for XDR-TB patients and 26% of the private doctors also do not isolate XDR-TB patients from other patients.
14% of government and 22% of private doctors are not referring the XDR-TB patients to higher centres even when they do not have proper facilities and isolation for such patients.
This gap between having knowledge regarding the seriousness of the disease and still not being able to follow the required preventive measures requires consolidated efforts to ensure compliance both in the government and private sector through regular interventions including trainings, monitoring and evaluation activities etc.
CONCLUSION:
There is a gap between the knowledge of both sector doctors, more in private practitioners, with respect to the awareness of extent, diagnosis, treatment and infection control measures for drug resistant TB. This translates into low levels of good practices seen through the responses from private sector doctors. Since private sector is an integral part of the strategy towards TB Elimination by 2025, the Ministry of Health and Family Welfare needs to engage the private practitioners in a fruitful manner which should include awareness campaigns and programs to ensure updated knowledge of drug resistant TB and its management. Also monitoring of the impact of such activities need to be integrated into the NTEP to ensure we are able to track the practical improvement in TB case management by practitioners.
References
- Thakur G, Thakur S, Thakur H. Status and challenges for tuberculosis control in India - Stakeholders' perspective. Indian J Tuberc. 2021;68(3):334-339.
- Subbaraman R, Nathavitharana RR, Satyanarayana S, et al. The Tuberculosis Cascade of Care in India's Public Sector: A Systematic Review and Meta-analysis. PLoS Med. 2016;13(10):e1002149. Published 2016 Oct 25. [CrossRef]
- Prasad R, Singh A, Balasubramanian V, Gupta N. Extensively drug-resistant tuberculosis in India: Current evidence on diagnosis & management. Indian J Med Res. 2017;145(3):271-293.
- Dhamnetiya D, Patel P, Jha RP, Shri N, Singh M, Bhattacharyya K. Trends in incidence and mortality of tuberculosis in India over past three decades: a joinpoint and age-period-cohort analysis. BMC Pulm Med. 2021;21(1):375. Published 2021 Nov 16. [CrossRef]
- Schito M, Migliori GB, Fletcher HA, et al. Perspectives on Advances in Tuberculosis Diagnostics, Drugs, and Vaccines. Clin Infect Dis. 2015;61Suppl 3(Suppl 3):S102-S118. [CrossRef]
- Michael JS, John TJ. Extensively drug-resistant tuberculosis in India: a review. Indian J Med Res. 2012;136(4):599-604.
- Ryu YJ. Diagnosis of pulmonary tuberculosis: recent advances and diagnostic algorithms. Tuberc Respir Dis (Seoul). 2015;78(2):64-71. [CrossRef]
- Sachdeva K, Shrivastava T. CBNAAT: A Boon for Early Diagnosis of Tuberculosis-Head and Neck. Indian J Otolaryngol Head Neck Surg. 2018;70(4):572-577. [CrossRef]
- Che Y, Song Q, Yang T, Ping G, Yu M. Fluoroquinolone resistance in multidrug-resistant Mycobacterium tuberculosis independent of fluoroquinolone use. Eur Respir J. 2017;50(6):1701633. Published 2017 Dec 7.
- Paleckyte, A., Dissanayake, O., Mpagama, S. et al. Reducing the risk of tuberculosis transmission for HCWs in high incidence settings. Antimicrob Resist Infect Control 10, 106 (2021).
- Sharma SK, Jelly P, Bhadoria AS, Thakur K, Gawande K. Awareness and perception regarding tuberculosis among patients and their relatives attending a tertiary care hospital in Uttarakhand: A hospital-based exploratory survey. J Family Med Prim Care. 2020;9(3):1555-1561. Published 2020 Mar 26. [CrossRef]
- J. R. Andrews, N. S. Shah, N. Gandhi, T. Moll, and G. Friedland, “Multidrug-resistant and extensively drug-resistant tuberculosis: implications for the HIV epidemic and antiretroviral therapy rollout in South Africa,” Journal of Infectious Diseases, vol. 196, no. 3, pp. S482–S490, 2007.
- Steingart K, Schiller I, Horne D, Pai M, Boehme, CC, Dendukuri N. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults (Review). Cochrane Database Syst Rev 2014;(1).CD 009593.
- Migliori GB, Nardell E, Yedilbayev A, D’Ambrosio L, Centis R, Tadolini M, et al. Reducing tuberculosis transmission: a consensus document from the World Health Organization Regional Office for Europe. Eur Respir J 2019;53:1900391. [CrossRef]
- Schaberg T, Rebhan K, Lode H. Risk factors for side effects of isoniazid-rifampicin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur Respir J. 1996;9:2026–30.
- Zarir F. Udwadia, Lancelot M. Pinto, Mukund W. Uplekar. Tuberculosis Management by Private Practitioners in Mumbai, India: Has Anything Changed in Two Decades?; Plos One Published: August 9, 2010; https://. [CrossRef]
- TUBERCULOSIS CONTROL MEASURES IN URBAN INDIA STRENGTHENING DELIVERY OF COMPREHENSIVE PRIMARY HEALTH SERVICES. Ranjani Gopinath, Rajesh Bhatia, Sonalini Khetrapal, Sungsup Ra, and Giridhara R. Babu, No 80, December 2020; ADB SOUTH ASIA WORKING PAPER SERIES. (ADB: ASIAN DEVELOPMENT BANK).
- Global Tuberculosis Report 2020, World Health Organization.
- https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
- India TB Report 2022, Ministry of Health and Family Welfare, Government of India.
- Tushar Sahasrabudhe, Tinku Joseph, Shailesh Meshram, Ankur Pathak. Awareness about MDR-TB in private medical practitioners of Pune City, European Respiratory Journal 2012 40: P2683.
- National Strategic Plan for Tuberculosis Elimination 2017-2025, Central TB Division, Ministry of Health & Family Welfare, Government of India.
- Manjula Kanakaraju, Sharath Burugina Nagaraja, Srinath Satyanarayana, Yella Ramesh Babu, Akshaya Kibballi Madhukeshwar, Somashekar Narasimhaiah, "Chest Radiography and Xpert MTB/RIF® Testing in Persons with Presumptive Pulmonary TB: Gaps and Challenges from a District in Karnataka, India", Tuberculosis Research and Treatment, vol. 2020, Article ID 5632810, 10 pages, 2020. [CrossRef]
- Ramya Ananthakrishnan, M. D'Arcy Richardson, Susan van den Hof, Radha Rangaswamy, Rajeswaran Thiagesan, Sheela Auguesteen and Netty Kamp. Successfully Engaging Private Providers to Improve Diagnosis, Notification, and Treatment of TB and Drug-Resistant TB: The EQUIP Public-Private Model in Chennai, India. Global Health: Science and Practice March 2019, 7(1):41-53. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



