
Submitted:
25 May 2023
Posted:
26 May 2023
You are already at the latest version
Abstract
Low back pain (LBP) is a health problem that affects 70-80% of the population in Western countries. Because of the biomechanical relationship between the lumbar region and the hip, it is thought that strengthening the muscles of this joint could improve the symptoms of people with LBP. The objective of the study is to evaluate the current evidence on the efficacy of hip strengthening exercises to reduce pain and disability in people with LBP. Clinical trials were collected from PubMed, PEDro, and Scopus databases published up to September 2022. Based on Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines and using CASpe and PEDro tools for methodological quality assessment, we selected studies that included hip strengthening exercises as part of LBP treatment and measured pain and/or disability parameters. Among the 966 records identified in the search, a total of 7 studies met the established selection criteria. Overall, participants who performed hip strengthening exercises had significantly improved in pain and disability. The methodological quality of the included studies was assessed as “good”. In conclusion, the addition of hip muscle strengthening exercises iterating LBP effectively improving pain and disability.
Keywords:
Low back pain
; hip
; strengthening
; treatment
; pain
; disability.
1. Introduction
Low back pain (LBP) is an increasingly common condition worldwide but in practical terms it is estimated that 70-80% of the population from countries of the Western world will suffer LBP at some point in their lives, especially affecting women over 30 years old [1,2]. Considerably this makes LBP the second most frequent chronic skeletal muscle pathology after osteoarthritis. A history of LBP was the most consistent and main cause of a restricted range of motion (ROM), long-term disability, and decreased quality of life (QoL) [1,3]. It is noteworthy that the overall healthcare cost analysis of LBP is estimated in a range of 100 billion dollars per year including direct tangible costs, indirect costs of labor, productivity slowdown, and monetary compensations in the United States of America [4]. Although most episodes of LBP usually resolve spontaneously a few days after its onset, a substantial proportion of patients, approximately 5-10% of the population will develop chronic (duration > 3 months) or recurrent pain [1,2]. In 85% of cases, LBP is considered as non-specific pain defined "A pain of non-specific cause which varies in intensity, as it is posture and physical activity related. It usually appears with movement and may be associated with referred or radiated pain” [1]. This type of LBP is often associated with psychosocial factors and abnormal pain-coping behaviors [1].
One of the main problems of low back pain are the variety of treatments which occasionally are not harmonized with what has been reported by scientific evidence worsening the results, chronifying pain and substantially increasing healthcare costs[2,5]. During acute phase (first 2-3 days) low back pain must be treated with rest and drugs (anti-inflammatory and/or analgesics), but if the pain persists, maintaining rest favor chronification [1]. For this reason, therapeutic exercise could currently be established as the most useful intervention in the treatment of LBP [6]. Therapeutic exercise in LBP would relieve pain, improve functionality, and reduce the risk of recurrence. It is necessary to consider the entire spectrum of different exercise therapies including motor control exercises, balance, aerobic training, stretching, and muscle strengthening [6].
The lumbar spine is biomechanically connected to the pelvic and hip joint, making it difficult to determine the provenance of symptoms in clinical practice [7]. The normal ROM of the hip is often altered in patients with LBP, making it impossible to correctly transmit load from the lower limb (LL) to the trunk [8,9]. This is usually due to shortening of the flexor muscles, which limits coxofemoral extension and therefore increases lumbar extension leading to lordosis [8,9]. On the other hand, it is common to find strength deficiency of the hip abductor and extensor muscles in patients suffering from LBP [9,10,11]. This shortage is usually compensated by over use of the hamstring muscles, which can lead to their curtailment and increased compensatory movements of the spine [9]. For this reason recently studies and guidelines have begun to include hip strengthening exercises (HSE) as part of LBP treatment [8]. The objective of this systematic review is to analyze the existing scientific evidence on the effectiveness of hip muscle strengthening (HMS) and related pain reduction or disability in people with LBP.
2. Materials and Methods
2.1. Search Strategy
For articles selection, a structured search was carried out using the electronic databases Medline (PubMed), "Physiotherapy Evidence Database" (PEDro) and Scopus until September 2022. The PICOs model was used according to the standard methods proposed by the “Preferred Reporting Item Guidelines for Systematic Reviews and Meta-Analyses” (PRISMA) [12] as follows: P (population): adults over 18 years who suffer from LBP; I (intervention): hip strengthening exercises (HSE); C (comparison): control/placebo group, without treatment or with any other treatment technique that does not involve the hip; O (outcomes): effects on pain (Visual Analogue Scale [VAS] and Numeric Pain Rating Scale [NPRS]), level of disability (Roland-Morris Disability Questionnaire [RMDQ], Oswestry Disability Index [ODI], and Patient-specific functional Scale [PSFS]), strength and resistance of the lumbar and hip muscles (dynamometry), flexibility of the hip muscles, gait analysis, balance and QoL); S (study design): clinical trial or randomized clinical trial.
The search strategy contained a combination of “Medical Subject Headings” (MeSH) and free words for related key concepts including: (“low back pain” OR “Mechanical” OR “ache, low back” OR “aches, low back” OR “Chronic low back pain” OR “lumbago” OR “non-specific low back pain” OR “lumbar instability”) AND (“hip” OR “hip mobility” OR “hip flexibility” OR “hip extensibility” OR “hip strength” OR “hip strengthening” OR “hip treatment” OR “hip intervention” OR “hip exercises” OR “gluteus” OR “aquatic exercise”) AND (“randomized controlled trial” OR “clinical trial” OR “trial”). Two authors (G.S. and D.F.-L.) independently performed the search for published studies and a third reviewer (I.R.) resolved disagreements about records. All the studies obtained in the 3 databases were compared in order to limit the search as much as possible and avoid repetition of studies. A review of all existing meta-analyses and systematic reviews was carried out to avoid losing studies due to lack of data search terms. Full text articles were retrieved and checked for compliance with inclusion and exclusion criteria.
2.2. Selection Criteria
- Inclusion Criteria
For inclusion in this review, studies had to: 1) access adult population with LBP; 2) treat using HSE being the main intervention or in conjunction with other interventions; 3) compare with the group without intervention, with placebo treatment or receiving another type of treatment non related to hip; 4) include studies reporting primary or secondary outcomes related to pain (VAS and NPRS) and level of disability (RMDQ, ODI and PSFS); 5) clinical trials or randomized clinical trials with a score of 6 or more on the Critical Appaisal Skills Programe (CASpe) questionnaire and the PEDro scale; 6) published in Spanish or English.
- b.
- Exclusion criteria
Studies were excluded from the review if they 1) included population under 18 years or no age specified; 2) reported that subjects had specific LBP (tumors, hernias, ankylosing spondylitis, fractures, etc.); 3) were reviews, meta-analyses, editorials and non-original studies; 4) did not have an affirmative answer to the first three questions of the CASPe questionnaire; 5) reported insufficient data or did not access to the full text.
2.3. Extraction and synthesis of data
A checklist for data extraction was developed from each study included in the review. The following study details were extracted: first author's last name; year of publication; country where the study was conducted; design; sample size; sex; age; height; weight; intervention in the control group (CG) and intervention group (IG), focusing especially on the HSE protocol (exercises, volume and intensity, frequency, session time, study duration, and supervision); measurement scales used; and final results. Two researchers (G.S and I.R) carried out the data extraction process with the help of a spreadsheet. In case of disagreements, a third author (D.F.-L.) participated in the process.
2.4. Assessment of methodological quality
3. Results
3.1. Selection of studies
The search identified 966 potentially relevant studies in the three databases, 325 from PubMed, 92 from PEDro, and 549 from Scopus. After eliminating duplicates and reading the titles, 912 articles were discarded. In a second phase, 47 were eliminated due to: being non-clinical trials (n = 7), not training hip muscles (n = 26), not having a representative population (n = 6), not measuring pain and/or disability (n = 5), not presenting a CG (n = 2) and not being written in Spanish or English (n = 1). Additionally, the bibliographies of the included articles and some of the discarded ones were reviewed to search for new studies, but none of interest were found. Therefore, after this search, 7 articles were obtained that will be included in the systematic review (Figure 1).
3.2. Assessment of methodological quality
All the included studies met the minimum methodological quality requirements with a score equal or greater than 6, that is, “good”. The scores varied between 7 and 10 points on the CASPe scale (Table 1) and between 6 and 9 on the PEDro scale (Table 2).
Due to the type of intervention that is intended to be studied, none of them meet the requirement of complete blinding, since the therapists will always know the treatment, they are performing and, therefore, to which group each patient belongs. However, blinding was maintained by study personnel in charge of data analysis in all studies except the one developed by Bade et al. [15] and Kim et al. [16] kept the participants blinded; while in those of Jeong et al. [17] and Lee et al. [18] nothing is specified about blinding.
3.3. Characteristics of participants and interventions
The characteristics of the participants are shown in Table 3. The total number of volunteers were 517, 230 women and 200 men aged between 18 and 77 years. 5 of the studies used a sample composed of both men and women [15,16,19,20,21], one of them did not specify the number of participants of each sex [18] and the remaining study included only women [17].
All the studies compare HMS exercise programs (IG) and those directed by chest or of general nature (CG). Only the trial by Cai et al. [19] applied the HMS as the sole treatment of the GI. In the remaining 6 studies, the IG, in addition to the HMS exercise program, receives the same treatment as the CG consisting of manual therapy of the lower back and/or hip joint, strengthening and resistance exercises of the trunk muscles, peripheral nervous system (PNS) mobilizations, aerobic exercise, fitness, education, motor control exercises, and lumbar stabilization (Table 3).
Table 4 shows the specific characteristics of the HMS protocols used in the IG. The study carried out by Cai et al. [19] was the only one to include strengthening exercises for the muscles involved in the knee joint. For their part, Kim et al. [16] divided the IG into two subgroups, one of them performed HMS exercises and the other static stretching of the hamstrings, iliopsoas, piriformis, and tensor fasciae latae. All the studies focused on the work of the abductor and extensor muscles [15,16,17,19,20,21], and only Lee et al. [18] added the adductor muscles and the rotators. The duration of the intervention was similar in all studies with a minimum of 5 weeks [20] and a maximum of 8 weeks [19].
3.4. Evaluation of the results
- pain
Six [15,16,18,19,20,21] of the 7 studies included in the review measured changes in pain with a total of 230 CG and 222 IG participants. 4 studies [16,18,20,21] used the VAS scale to measure pain and the remaining 2 [15,19] used the NPRS scale. In all of them an improvement or even pain relief was observed after the intervention in the IG, but the difference between groups was only statistically significant (p < 0.05) in 3 [15,16,19] and 2 did not find any difference [20,21] (Table 3).
- b.
- Disability level
The level of disability was taken into account by the 7 studies [15,16,17,18,19,20,21], with 250 participants belonging to the CG and 267 to the IG. Of these 7 studies, 1 [20] used the Roland-Morris questionnaire, 4 [15,17,18,21] used the original or modified ODI, while Kim et al. [16] used both and the last one [19] used the PSFS scale. As in pain, all the trials obtained improvements in the IG, however, this improvement was significantly greater (p < 0.05) in the IG compared to the CG only in 4 [15,16,17,19] (Table 3).
- c.
- Other parameters evaluated
As can be seen in Table 3, 3 of the 7 studies analyzed the strength of the hip muscles through dynamometry [19,20,21]. However, even though all the studies found improvements in the IG in comparison to the baseline, none were able to demonstrate statistically significant changes (p > 0.05) compared to the CG. In parallel, Cai et al. [19] and Jeong et al. [17] studied lumbar resistance and strength, respectively, and both found two statistically significant improvements (p < 0.05) in the IG comparatively to the CG. In relation to these improvements in the lumbar musculature, Kim et al. (16) have reported a statistically significant decrease (p < 0.05) in lumbar instability measured through the IG PSLRT scale with a stretching protocol compared to the CG. This same trial demonstrated statistically significant increases (p < 0.05) in the two IG versus the CG of QoL, studied with the SF-36 scale.
4. Discussion
All seven studies that met the inclusion/exclusion criteria found that HMS treatment of LBP may be effective in reducing both pain and disability in contrast to other non-hip interventions. Additionally, no unwanted effects have been reported in any of the subjects included in the studies, postulating HMS as a safe and effective therapeutic exercise option.
According to the World Association for the Study of Pain (IASP), pain is considered “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” [22]. Pain is subjective and should not always be eliminated as it acts as a defense mechanism, protecting the body from dangerous situations. However, sometimes pain becomes a source of suffering specially appearing in the absence of tissue damage, frequently due to psychological disorders [22,23]. For its part, disability related to LBP makes it difficult to perform activities of daily living (ADL) and work tasks [24]. Additionally, LBP can lead the individual to social isolation and avoid daily activities, reducing their self-efficacy and increasing the chances of developing depressive symptoms and disability [25]. Five of the studies [15,16,17,18,19] found statistically significant improvements (p < 0.05) in both pain and disability compared to the CG and 7 [15,16,17,18,19,20,21] in the IG compared to baseline. This incongruity observed in results are likely due to the intensity, frequency, and duration of the interventions. The number of weekly sessions carried out in the study by Fukuda et al. [20] were 2 and Kendall et al. [21] only indicates that 1 face-to-face session was given weekly, without specifying the number of weekly sessions at home, the duration of the sessions, or details about the volume and intensity (number of exercises, series, repetitions, rest times, etc.) of the same. This differs with the number of weekly sessions carried out in the interventions of the studies that obtained improvements in comparation to the CG, ranging from 3 to 7 [15,16,17,18,19]. Additionally, the duration of treatment was shorter, Fukuda et al. [20] conducted a 5-week intervention and Kendall et al. [21] a 6 weeks, while the duration in the rest of the studies was 6 to 8 weeks [15,16,17,18,19].
Although the mechanism by which HMS exercises reduce pain and disability levels is not well understood, it may be due to the increase in pelvic stability provided by strengthening of the gluteal muscles [11,26]. The gluteus medius and minimus are responsible for controlling the position and stability of both the hip and the pelvis, so their weakness can lead to biomechanical changes in the coxolumbopelvic complex, contributing to LBP [26]. Mainly it will lead to the lateral descent of the pelvis while walking, which is known as the trendelenburg sign. This will cause an abnormal distribution of weight load on the intervertebral discs and lumbar joints [26]. Additionally, gluteal weakness can lead to less control of the hip in the transverse plane, increasing internal rotation and adduction of the femur, which leads to an increase in pelvic anteversion and again results in abnormal load distribution at the lumbar level [8] (Figure 2). However, for the correct functioning of the coxolumbopelvic complex, not only an adequate level of force is necessary, but it is also important that the hip and lumbar ROM are maintained [8]. Techniques to increase ROM such as manual therapy or stretching could be useful adjuncts to improve pain and disability in patients with LBP, as shown in 3 studies included in this review [15,16,18]. In this sense, Kim et al. [16] divided the IG into two, one performed static stretching of the hip muscles and the other HMS, both found statistically significant improvements (p < 0.05) with respect to the CG and the baseline, with no differences between the two IG in count pain and disability. However, he found statistically significant increases (p < 0.05) compared to the CG in QoL and lumbar stability in the IG who performed stretching. These increases were not observed in the IG with HMS exercises, demonstrating the importance of preserving the lumbar and pelvic-femoral ROM in the treatment of LBP.
The results described in the 7 studies included in this review are consistent with those reported by Tataryn et al. [27] who obtained improvements in pain and disability both in the IG and in the CG, however these are higher in the IG. This author carried out a systematic review with meta-analysis in which they intended to compare the effectiveness of exercises to strengthen the posterior chain of the LL and general exercise programs. This could be explained because LBP is associated with alterations in muscle activation patterns, strength, endurance, flexibility, and poor physical condition. This is confounded in part to conscious or unconscious avoidance behaviors for fear of worsening the problem [28,29]. This inactivity usually means a decrease in lumbopelvic stability and a greater load on the lumbar joints [29]. Therefore, exercise, whether for motor control, strength, flexibility or resistance, will be effective in the treatment of LBP, improving pain and function. Thus, strength training is considered essential to increase lumbopelvic stability, while aerobic exercise seems to be especially important in improving mood and reducing depression. Overall this is considered a very important risk factor in chronification of pain [28,29].
4.1. Potential applications
Considering the different protocols and results obtained in this study, we have developed therapeutic exercise intervention protocol with the aim of guiding clinical practice (Table 5). The training sessions should be structured in 3 parts, warm-up with joint mobility exercises and muscle activation. The main part where the HMS exercises will be carried out, such as squats, Monster Walk, gluteal kick, Lateral Clam, gluteal bridge, and finally returning through relaxation exercises towards a calmer state. Importantly static stretching and manual therapy of the coxofemoral joint are crucial through these sessions. Therefore, we would fulfill the key points of LBP treatment that we have developed throughout the discussion, specifically the HMS of gluteus and the maintenance of the hip ROM. At the same time, it would also be interesting to include exercises to strengthen lumbar muscles, motor control and manual therapy techniques specifically targeting the lumbar spine. In relation to the workload, 2 to 3 series of 8-12 repetitions per exercise should be performed with a minute of rest between series and an intensity of 75-80% of one maximum repetition (RM). The duration of the sessions is approximately 60 minutes and may be done 3-4 weekly sessions.
4.2. Limitations and Strengths
The authors of this review acknowledge some limitations. First, the number of manuscripts that met the inclusion/exclusion criteria was limited. Given the type of intervention studied, it was impossible for the therapists to remain blinded and only the trial by Kim et al. [16] achieved blinding of patients. However, in order to minimize the risk of bias, the PRISMA method [12] was followed and the search was carried out in 3 databases. The CASPe [14] and PEDro [13] tools were used for quality assessment, methodology and to ensure that the selected studies met the minimum quality criteria.
Finally, the results should be interpreted considering the great heterogeneity in the studies as in terms of interventions (type of exercises, intensity, volume, frequency, duration of the sessions and duration of the intervention) along with the characteristics of the sample (age, sex and level of physical activity).
5. Conclusions
The results presented in this systematic review showed that the inclusion of HMS exercises in an exercise protocol that involves the whole musculature or specifically targets the lower back provides significant improvements in the reduction of pain and disability in patients with LBP, without causing injury.
Author Contributions
Conceptualization G.S. and I.R.; methodology G.S, R.M.C., and D.F.-L.; investigation G.S., I.R., R.C.M.; resources G.S, R.M.C., and I.R.; data curation G.S, E.L.-C., and D.L.-F.; writing – original draft preparation G.S. and D.F.-L.; Writing – review and editing D.L.-F., E.L.-C and R.M.C.; visualization and supervision G.S. and D.F.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the Neurobiology Research Group from the Department of Cellular Biology, Genetics, Histology and Pharmacology, Faculty of Medicine, The University of Valladolid, for their collaboration on the infrastructures and material that was necessary to carry out the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Casado-Moral, M.; Moix, J.; Vidal, J. Etiology, chronification and treatment of low back pain. Clínica y Salud 2022, 19, 379–392. [Google Scholar]
- Seguí, M.; Gérvas, J. Low Back Pain. Med Fam Semer 2002, 28, 21–41. [Google Scholar]
- Heredia-Elvar, J.R.; Segarra, V.; García-Orea, G.P.; Campillos, J.A.; Sampietro, M.; Moyano, M.; Da Silva, M.E. Proposal for the Design of Functional Rehabilitation Programs in the Population with Low Back Pain by the Physical Exercise Specialist. Int J Phys Exerc Heal Sci Trainers 2016.
- Katz, J.N. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg Am 2006, 88, 21–24. [Google Scholar] [CrossRef]
- Moix, J.; Cano-Vindel, A. Evidence-based clinical practice guideline for nonspecific low back pain. Ansiedad y estres 2006, 12, 116–128. [Google Scholar]
- Hernández, G.A.; Salas, J.D.Z. Exercise as a treatment for low back pain management. Rev Salud Publica (Bogota) 2017, 19, 123–128. [Google Scholar] [PubMed]
- Marín-Peña, O.; Fernández-Tormos, E.; Dantas, P.; Rego, P.; Pérez-Carro, L. Anatomy and function of the coxofemoral joint. Arthroscopic anatomy of the hip. Rev Española Artrosc y Cirugía Articul 2016, 23, 3–10. [Google Scholar] [CrossRef]
- Hatefi, M.; Babakhani, F.; Ashrafizadeh, M. The effect of static stretching exercises on hip range of motion, pain, and disability in patients with non-specific low back pain. J Exp Orthop 2021, 8, 55. [Google Scholar] [CrossRef]
- McGregor, A.H.; Hukins, D.W.L. Lower limb involvement in spinal function and low back pain. J Back Musculoskelet Rehabil 2009, 22, 219–222. [Google Scholar] [CrossRef]
- Nadler, S.F.; Malanga, G.A.; Bartoli, L.A.; Feinberg, J.H.; Prybicien, M.; Deprince, M. Hip muscle imbalance and low back pain in athletes: influence of core strengthening. Med Sci Sports Exerc 2002, 34, 9–16. [Google Scholar] [CrossRef]
- de Jesus, F.L.A.; Fukuda, T.Y.; Souza, C.; Guimarães, J.; Aquino, L.; Carvalho, G.; Powers, C.; Gomes-Neto, M. Addition of specific hip strengthening exercises to conventional rehabilitation therapy for low back pain: a systematic review and meta-analysis. Clin Rehabil 2020, 34, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzleff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moseley, A.M.; Elkins, M.R.; Van der Wees, P.J.; Pinheiro, M.B. Using research to guide practice: The Physiotherapy Evidence Database (PEDro). Brazilian J Phys Ther 2020, 24, 384–391. [Google Scholar] [CrossRef]
- Cabello, J.B.; Maciá, L. Critical reading of clinical evidence. 2015, 184.
- Bade, M.; Cobo-Estevez, M.; Neeley, D.; Pandya, J.; Gunderson, T.; Cook, C. Effects of manual therapy and exercise targeting the hips in patients with low-back pain-A randomized controlled trial. J Eval Clin Pract 2017, 23, 734–740. [Google Scholar] [CrossRef]
- Kim, B.; Yim, J. Core Stability and Hip Exercises Improve Physical Function and Activity in Patients with Non-Specific Low Back Pain: A Randomized Controlled Trial. Tohoku J Exp Med 2020, 251, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Jeong, U.C.; Sim, J.H.; Kim, C.Y.; Hwang-Bo, G.; Nam, C.W. The effects of gluteus muscle strengthening exercise and lumbar stabilization exercise on lumbar muscle strength and balance in chronic low back pain patients. J Phys Ther Sci 2015, 27, 3813–3816. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, S.Y. Effects of hip exercises for chronic low-back pain patients with lumbar instability. J Phys Ther Sci 2015, 27, 345–348. [Google Scholar] [CrossRef]
- Cai, C.; Yang, Y.; Kong, P.W. Comparison of Lower Limb and Back Exercises for Runners with Chronic Low Back Pain. Med Sci Sports Exerc 2017, 49, 2374–2384. [Google Scholar] [CrossRef]
- Fukuda, T.Y.; Aquino, L.M.; Pereira, P.; Ayres, I.; Feio, A.F.; de Jesus, F.L.A.; Gomes-Neto, M. Does adding hip strengthening exercises to manual therapy and segmental stabilization improve outcomes in patients with nonspecific low back pain? A randomized controlled trial. Brazilian J Phys Ther 2021, 25, 900–907. [Google Scholar] [CrossRef]
- Kendall, K.D.; Emery, C.A.; Wiley, J.P.; Ferber, R. The effect of the addition of hip strengthening exercises to a lumbopelvic exercise programme for the treatment of non-specific low back pain: A randomized controlled trial. J Sci Med Sport 2015, 18, 626–631. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, J.S.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; Song, X.J.; Stevens, B.; Sullivan, M.D.; Tutelman, P.R.; Ushida, T.; Vader, K. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Romera, E.; Perena, M.; Perena, M.; Rodrigo, M. Pain neurophysiology. Rev Soc Esp Dolor 2000, 7, 11–17. [Google Scholar]
- Santiago, C.; Perez, K.; Castro, N. Low back pain and its relation to disability index in a rehabilitation hospital. Rev Cient Méd 2018, 21, 13–20. [Google Scholar]
- Salvetti, M.G.; Pimenta, C.A.; Braga, P.E.; Corrêa, C.F. Disability related to chronic low back pain: prevalence and associated factors. Rev da Esc Enferm da USP 2012, 46, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Sadler, S.; Cassidy, S.; Peterson, B.; Spink, M.; Chuter, V. Gluteus medius muscle function in people with and without low back pain: a systematic review. BMC Musculoskelet Disord 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Tataryn, N.; Simas, V.; Catterall, T.; Furness, J.; Keogh, J.W.L. Posterior-Chain Resistance Training Compared to General Exercise and Walking Programmes for the Treatment of Chronic Low Back Pain in the General Population: A Systematic Review and Meta-Analysis. Sport Med 2021, 7, 1–17. [Google Scholar] [CrossRef]
- Rainville, J.; Hartigan, C.; Jouve, C.; Martinez, E. The influence of intense exercise-based physical therapy program on back pain anticipated before and induced by physical activities. Spine J 2004, 4, 176–183. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin Rehabil 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of study selection for the literature review (PRISMA)
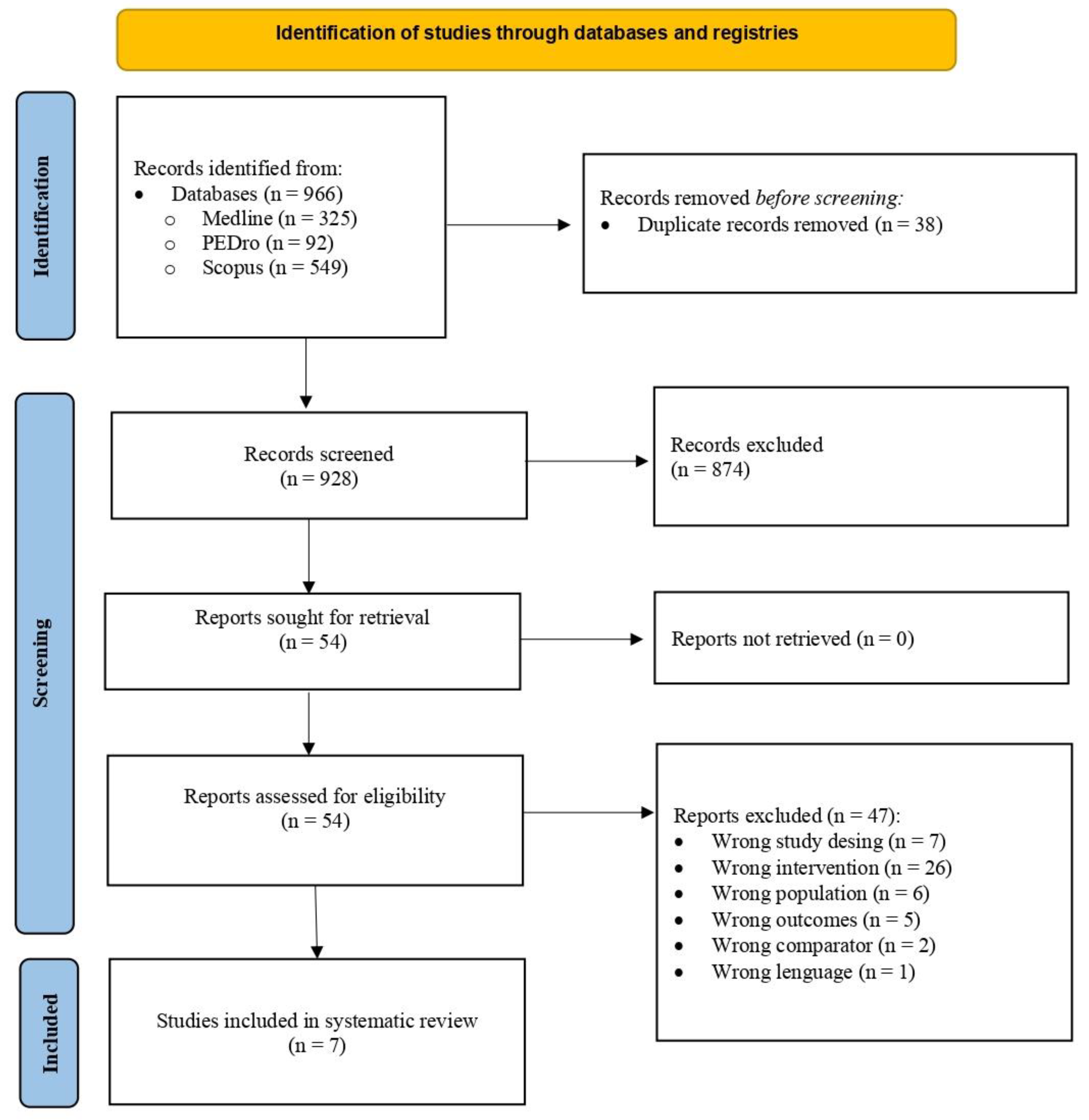
Figure 2.
Description of the mechanism for gluteal weakness increases low back pain.
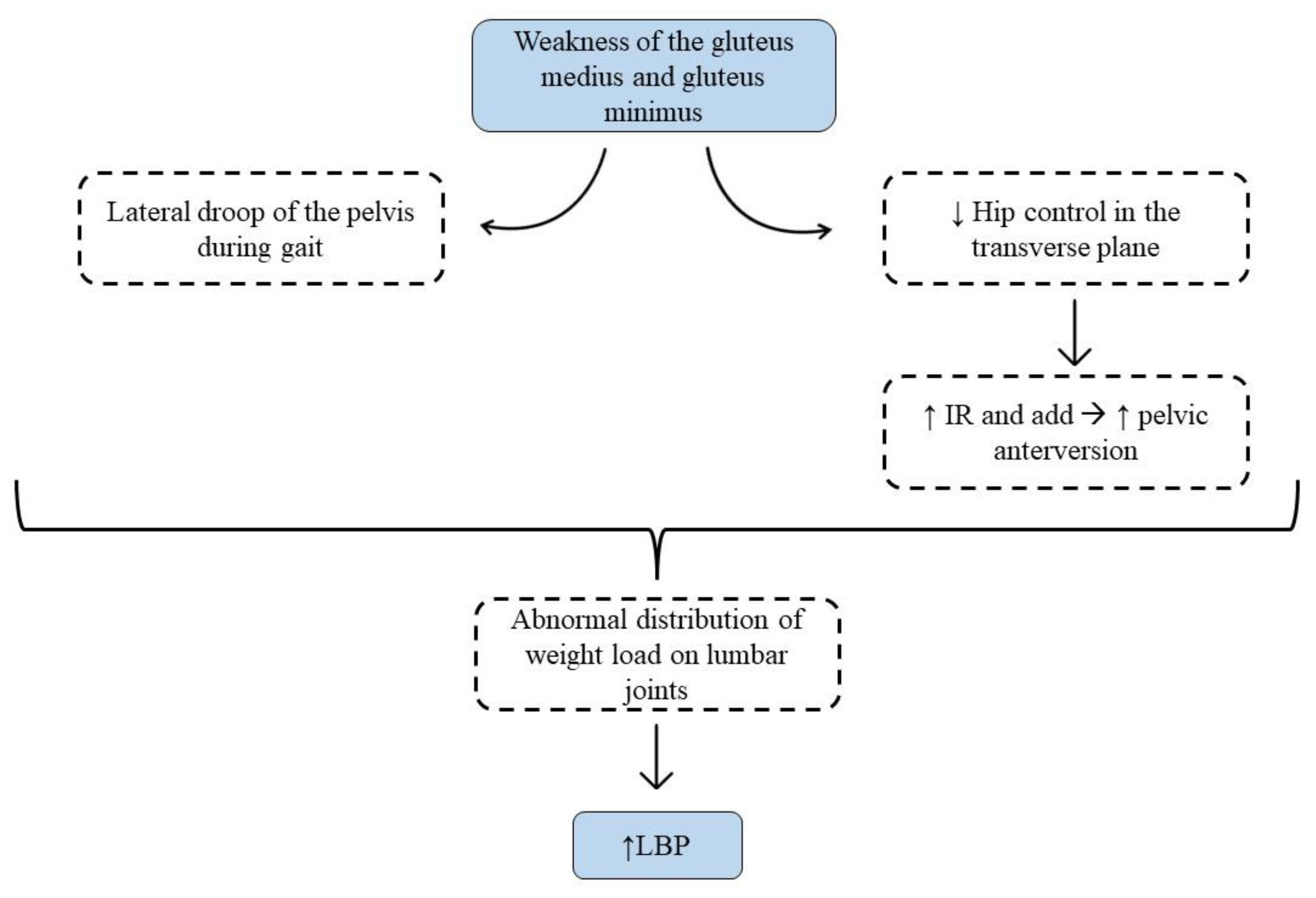

Table 1.
Results of methodological quality assessment of included studies – Critical Appraisal Skills Programme (CASP).
Table 1.
Results of methodological quality assessment of included studies – Critical Appraisal Skills Programme (CASP).
| Study | Ítem | Total | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| Bade M et al. 2016 [15] | Yes | Yes | Yes | No | Yes | Yes | No | p < 0.05 | Yes | Yes | Yes | 9 |
| Cai C et al. 2017 [19] | Yes | Yes | Yes | No | Yes | Yes | Yes | 95%CIp < 0.01 | No | Yes | Yes | 9 |
| Fukuda TY et al. 2021 [20] | Yes | Yes | Yes | No | Yes | Yes | No | 95% CI | Yes | Yes | No | 8 |
| Jeong UC et al. 2015 [17] | Yes | Yes | Yes | No | Yes | Yes | Yes | p < 0.01 | No | Yes | Yes | 9 |
| Kendal KD et al. 2014 [21] | Yes | Yes | Yes | No | Yes | Yes | No | 95% CI | Yes | Yes | No | 8 |
| Kim B et al. 2020 [16] | Yes | Yes | Yes | No | Yes | Yes | Yes | p < 0.05 | Yes | Yes | Yes | 10 |
| Lee SW et al. 2014 [18] | Yes | Yes | Yes | No | Yes | Yes | Yes | p < 0.01 | Yes | Yes | Yes | 10 |
CASP questionnaire items → 1: Clearly defined question; 2: Random assignment; 3: Patients considered until the end; 4: Blinding; 5: Similar groups at baseline; 6: Equally treated groups; 7: Longer treatment effect; 8: Accuracy of effect; 9: Applicability to your setting or local population; 10: All outcomes considered; 11: Benefits justify risk and cost. Abbreviations → CI: confidence interval.
Table 2.
Results of methodological quality assessment of included studies –Physiotherapy Evidence Database (PEDro).
Table 2.
Results of methodological quality assessment of included studies –Physiotherapy Evidence Database (PEDro).
| Study | Ítem | Total | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| Bade M et al. 2016 [15] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Cai C et al. 2017 [19] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 8 |
| Fukuda TY et al. 2021 [20] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 9 |
| Jeong UC et al. 2015 [17] | No | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Kendall KD et al. 2014 [21] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 9 |
| Kim B et al. 2020 [16] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | 9 |
| Lee SW et al. 2014 [18] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 6 |
PEDro Questionnaire items → 1: Eligibility criteria; 2: Random assignment; 3: Hidden allocation; 4: Baseline comparison; 5: Blind subjects; 6: Blind therapist; 7: Blind evaluators; 8: Adequate follow-up; 9: Intention-to-treat analysis; 10: Comparison between groups; 11: Point estimates and Variability.
Table 3.
Summary of studies included in the systematic review, participants and intervention characteristics.
Table 3.
Summary of studies included in the systematic review, participants and intervention characteristics.
| First author, year and country of publication | Study design | Participants (baseline sample side and characteristics) | Intervention | Outcomes | Results |
|---|---|---|---|---|---|
| Bade M et al. 2017, USA [15] | Random controlled trial | ni=90 (37♀ y 53♂) NSLBP ≥ 2 in NPRS and disability ≥ 20% in ODI. CG: ni =43; 16♀ y 27♂ (11 dropout → nf =32) Age (mean ± SD): 48,1 ± 2,4 y Height (mean ± SD): 1,7 ± 0,0m Weight (mean ± SD): 78,5 ± 3,1 Kg Symptoms duration (media ± SD): 19,7 ± 7,2 Wk IG: ni =47; 21♀ y 26♂ (7 dropout → nf =40) Age (mean ± SD): 44,8 ± 2,3 y Height (mean ± SD): 1,7 ± 0,0m Weight (mean ± SD): 81,3 ± 4,7 Kg Symptoms duration (media ± SD): 20,3 ± 6,5 Wk |
CG: MT, coordination, strengthening and resistance trunk ex., PNS mobilizations, tractions, aerobic ex., flexion ex., fitness, centralization and directional preference ex. and procedures. GI: CG Intervention + HM strengthening + hip MT (mobilizations degree III-IV, 30 sec/technique; A-P mobilization with traction, traction and mobilization P-A in PP) |
Pain: NPRS Disability: ODI GROC PASS |
CG: Changes with baseline ↓ NPRS ↓ ODI IG: Changes with baseline ↓ NPRS ↓ ODI GI vs GC ↓* NPRS ↓* ODI ↓* GROC ↔ PASS |
| Cai C et al. 2017, Singapore [19] | Random controlled trial, simple blind | ni =84 (42♀ y 42♂) NSCLBP CG: -LE: ni =28 (4 dropout → nf =24) Age (mean ± SD): 26,1 ± 4,1 y Weight (mean ± SD): 61,7 ± 10,8 Kg BMI (mean ± SD): 21,8 ± 2,4 Kg/m2 -LS: ni =28 (3 dropout → nf =25) Age (mean ± SD): 26,9 ± 6,4 y Weight (mean ± SD): 60,3 ± 12,1 Kg BMI (mean ± SD): 21,9 ± 2,4 Kg/m2 IG: ni =28 (3 dropout → nf = 25) Age (mean ± SD): 28,9 ± 5,3 y Weight (mean ± SD): 61,7 ± 12,6 Kg BMI (mean ± SD): 21,7 ± 2,4 Kg/m2 |
CG: -LE: Lumbar extensor strengthening ex. -LS: lumbopelvic motor control ex. IG: HM and knee strengthening ex. |
Pain: NPRS Disability: PSFS LL strength: dynamometry LE resistance: EMG Activation of trunk stabilizing muscles: US |
CG (LE y LS): Changes with baseline ↓* NPRS ↑* PSFS ↑ LL strength ↑* LE resistance ↑* Activation of trunk stabilizing muscles IG: Changes with baseline ↓* NPRS ↑* PSFS ↑* LL strength ↑* LE resistance ↑* Activation of trunk stabilizing muscles IG vs CG (LE y LS) ↓* NPRS ↑* PSFS ↑ LL strength ↑* LE endurance ↔ Activation of trunk stabilizing muscles |
| Fukuda TY et al. 2021, Brazil [20] | Random controlled trial, simple blind | ni =70 (37♀ y 33♂) NSCLBP CG: ni =35 (3 dropout → nf =32) Age (mean ± SD): 35,2 ± 12,5 y Height (mean ± SD): 1,6 ± 0,1m Weight (mean ± SD): 72,6 ± 15,6 Kg BMI (mean ± SD): 25,3 ± 4,6 Kg/m2 Symptoms duration (mean ± SD): 6,9 ± 8,1 month IG: ni =35 (4 dropout → nf =31) Age (mean ± SD): 40,2 ± 12,4 y Height (mean ± SD): 1,7 ± 0,1m Weight (mean ± SD): 75,8 ± 15,9 Kg BMI (mean ± SD): 25,9 ± 5,4 Kg/m2 Symptoms duration (mean ± SD): 8,1 ± 8,9 month |
CG: MT (P-A-C mobilization degree III of L1-L5, 5 reps/1min following Maitland method and myofascial liberation) Segmentary lumbar stabilization ex. IG: CG intervention + HM strengthening ex. |
Pain: VAS Disability: RMDQ HM strength: dynamometry Kinematic analysis of gait (LL, trunk and pelvis) |
CG: Changes with baseline ↓ VAS ↓ RMDQ ↑ HM strength ↔ Kinematic analysis IG: changes with baseline ↓ VAS ↓ RMDQ ↑ HM strength ↔ Kinematic analysis IG vs CG ↔ VAS ↔ RMDQ ↔ HM strength ↔ Kinematic analysis |
| Jeong UC et al. 2015, Korea [17] | Random controlled trial | ni =40♀ NSLBP ≥ 5 in VAS and disability ≥ 20% in ODI. CG: ni =20♀ (0 dropout → nf =20) Age (mean ± SD): 41,2 ± 6,7 y Height (mean ± SD): 159,9 ± 4,7cm Weight (mean ± SD): 56,6 ± 4,2 Kg IG: ni =20♀ (0 dropout → nf =20) Age (mean ± SD): 41,2 ± 5,5 y Height (mean ± SD): 161,5 ± 6,0 cm Weight (mean ± SD): 59,7 ± 7,2 Kg |
CG: Lumbar stabilization ex. (2 sets/20reps/10 sec) IG: CG intervention + HM strengthening ex. |
Disability: ODI Lumbar strength: M3 Balance: Tetrax |
CG: Changes with baseline ↓ ODI ↑ Lumbar strength ↑ Balance IG: Changes with baseline ↓ ODI ↑Lumbar strength ↑ Balance IG vs CG ↓* ODI ↑* Lumbar strength ↑* Balance |
| Kendall KD et al. 2014, Canada [21] | Random controlled trial | ni =80 (42♀ y 38♂) NSCLBP ≥ 5 in VAS CG: ni =40; 18♀ y 22♂ (4 dropout → nf =36) Age (95%CI): 33 (33, 41) y Height (95%CI): 172 (169, 175) cm Weight (95%CI): 73 (68, 78) Kg Symptoms duration (95%CI): 4 (3, 6) y IG: ni =40; 24♀ y 16♂ (5 dropout → nf =35) Age (95%CI): 41 (37, 45) y Height (95%CI): 170 (167, 173) cm Weight (95%CI): 77 (71, 83) Kg Symptoms duration (95%CI): 7 (4, 10) y |
CG: Lumbopelvic motor control (transverse, multifidus and pelvic floor coordination) IG: CG intervention + HM strengthening ex. |
Pain: VAS Disability: ODI HM strength: Dynamometry Trendelenburg Test |
CG: Changes with baseline ↓* VAS ↓* ODI ↔ HM strength ↔ Trendelenburg Test IG: Changes with baseline ↓* VAS ↓* ODI ↑* HM strength ↔ Trendelenburg Test IG vs CG ↔ VAS ↔ ODI ↑* HM strength ↔ Trendelenburg test |
| Kim B et al. 2020, Korea [16]. | Randomized controlled trial, doble blind | ni =75 (32♀ y 34♂) NSCLBP ≥ 3 in VAS CG: ni =25 (5 dropout → nf =20) Age (mean ± SD): 47,7 ± 8,5 y Height (mean ± SD): 167,7 ± 8,1cm Weight (mean ± SD): 67,6 ± 8,7 Kg BMI (media ± SD): 23,9 ± 1,0 Kg/m2 IG: -SIG: ni =25 (3 dropout → nf =22) Age (mean ± SD): 47,0 ± 9,4 y Height (mean ± SD): 166,5 ± 2,1 cm Weight (mean ± SD): 66,0 ± 9,2 Kg BMI (mean ± SD): 23,6 ± 1,5 Kg/m2 -FIG: ni =25 (1 dropout → nf =24) Age (mean ± SD): 47,5 ± 9,7 y Height (mean ± SD): 164,7 ± 8,2 cm Weight (mean ± SD): 65,4 ± 10,4 Kg BMI (mean ± SD): 23,9 ± 1,6 Kg/m2 |
CG: Core stability ex. (30 min, 3 session/sem, 6 sem, 10reps/7-8sec) Placebo (light palpation of the lumbosacral region) IG: -SIG: core stability ex. + HM strengthening ex. FIG: core stability ex. + HM static stretching ex. |
Pain: VAS Disability: ODI y RMDQ Lumbar instability: PSLRT HM flexibility: TTT, MTT, OT, FAIRT Balance: OLST QoL: SF-36 |
CG: Changes with baseline ↓* VAS ↓* ODI y RMDQ ↑*PSLRT ↑* HM flexibility ↑* OLST ↑* SF-36 SIG y FIG: Changes with baseline ↓* VAS ↓* ODI y RMDQ ↑*PSLRT ↑* HM flexibility ↑* OLST ↑* SF-36 SIG vs CG ↓* VAS ↓* ODI y RMDQ ↔PSLRT ↔ HM flexibility ↑* OLST ↑* SF-36 FIG vs CG ↓* VAS ↓* ODI y RMDQ ↑*PSLRT ↑* HM flexibility ↑* OLST ↑* SF-36 FIG vs SIG ↔VAS ↔ ODI y RMDQ ↑*PSLRT ↑* HM flexibility ↔ OLST ↔ SF-36 |
| Lee SW et al. 2014, Korea [18]. | Randomized controlled trial | ni =78 CLBP CG: ni =31 (6 dropout → nf = 25) -CGLS: ni =20 (4 dropout → nf =16) Age (mean ± SD): 50,0 ± 11,4 y Height (mean ± SD): 161,9 ± 7,7 cm Weight (mean ± SD): 60,9 ± 9,8 Kg BMI (mean ± SD): 23,2 ± 2,8 Kg/m2 -CGIN: ni =11 (2 dropout → nf =9) Age (mean ± SD): 59,3 ± 17,3 y Height (mean ± SD): 161,0 ± 8,3 cm Weight (mean ± SD): 59,5 ± 10,0 Kg BMI (mean ± SD): 22,8 ± 2,9 Kg/m2 IG: ni = 47 (3 dropout → nf =44) -IGLS: ni =25 (2 dropout → nf =23) Age (mean ± SD): 54,9 ± 10,6 y Height (mean ± SD): 161,0 ± 7,1 cm Weight (mean ± SD): 61,9 ± 9,8 Kg BMI (mean ± SD): 23,8 ± 2,8 Kg/m2 -IGIN: ni =22 (1 dropout → nf =21) Age (mean ± SD): 61,0 ± 13,2 y Height (mean ± SD): 159,7 ± 6,0 cm Weight (mean ± SD): 59,4 ± 8,9 Kg BMI (mean ± SD): 23,3 ± 2,6 Kg/m2 |
CG: Lumbar stability ex. (4 ex./ 4 sets/ 4reps/ 10 sec, 30 sec rest. IG: CG intervention + HM strengthening ex. + hip mobility ex. |
Pain: VAS Disability: modified ODI |
CG: Changes with baseline ↓* VAS ↓* ODI IG: Changes with baseline ↓* VAS ↓* ODI IG vs CG ↓ VAS ↓ ODI |
Abbreviations: ↓: decrease; ↑: increase; ↔: without change; *: Statistically significant change (p < 0,05); ni: initial sample side; nf: final sample side; ♀: women; ♂: men; CG: control group; IG: intervention group; SD: Standard Deviation; m: meters; Kg: kilograms; Wk: week; y: year; cm: centimetre; BMI: body mass index; NSLBP: non-specific low back pain; NSCLBP: non-specific chronic low back pain; CLBP: chronic low back pain; NPRS: Numeric Pain Rating Scale; ODI: Oswestry disability index; MT: manual therapy; ex.: exercise; PNS: peripheral nervous system; HM: hip muscles; A-P: antero-posterior; P-A: postero-anterior; PP: prone position; GROC: Global Rating of Change; PASS: Patient acceptable symptom state; LE: lumbar extensor; LS: lumbar stability; PSFS: patient-specific functional scale; LL: lower limb; EMG: electromyography; US: ultrasound; P-A-C: postero-anterior-central; L1: first lumbar vertebra; L5: fifth lumbar vertebra; reps: repetitions; min: minutes; RMDQ: Roland-Morris Disability Questionnaire; VAS: Visual Analogue Scale; sec: second; CI: confidence interval; SIG: strength intervention group; FIG: flexibility intervention group; PSLRT: passive straight leg raising test; TTT: Toe touch test; MTT: Modified Thomas Test; OT: Ober test; FAIRT: Flexion adduction internal rotation test; OLST: one leg standing test; QoL: Quality of life; IN: lumbar instability.
Table 4.
Characteristics of hip muscles strengthening interventions.
| First author, year and country of publication | Exercise | Volume and intensity | Frequency (days/week) | Time (minutes/session) | Duration (weeks) | Supervision |
|---|---|---|---|---|---|---|
| Bade M et al. 2017, USA. [15] | Clam in side lying with ER Quadruped hip extension Unilateral bridge Home ex. |
2 sets of 12-15 reps | 7 -Home ex. Twice a day |
- | - | Yes -Home ex. with instructions |
| Cai C et al. 2017, Singapore [19] | Device for strengthening hip abd and extensor and knee extensor Home ex.: -single-leg squat -Wall sit |
Supervised: 3 sets of 10 reps, 2 min rest 10 RM Home ex.: 3 sets of 10 rep, 2,5Kg single-leg squat, 5Kg wall sit |
Supervised:2 Home ex.: 5 |
45 | 8 | Yes -Home ex. with instructions |
| Fukuda et al. 2021, Brazil [20] | Clam in side lying with ER Lateral straight leg rise with ankle weight Squat with ER Monster Walk with ER |
3 sets of 10 reps 70% RM Ex. with ER: maximum resistance that enables 10 reps |
2 | 45 | 5 | Yes |
| Jeong UC et al. 2015, Korea [17] | Gluteus maximus and gluteus medius ex. 3 wk without resistance and 3 wk with resistance | 2 sets of 15 reps | 3 | 50 | 6 | Yes |
| Kendal KD et al. 2014, Canada [21] | Controlled with US (not specified) Home ex.: open and close kinetic chain hip ex. |
Not specified |
Supervised:1 Home ex.: Not specified |
Not specified | 6 | Yes -Home ex. with instructions |
| Kim B et al 2020, Korea [16] | FIG: HM static stretching (hamstring, iliopsoas, piriformis, tensor fasciae latae) SIG: HM strengthening ex. (side lying hip abd with IR, prone heel squeeze, quadruped hip extension, standing gluteal squeeze) |
3 reps of 30 sec 10 sec rest |
3 | 45 | 6 | Yes |
| Lee SW et al. 2014, Korea [18] | To increase ROM: 4 open kinetic chain hip ex. 6 strengthening ex. with ER |
3 sets of 10 reps, 1 min rest 75% RM |
3 | ROM ex.: 20 Strengthening ex.: Not specified |
6 | Yes |
Abbreviations: ER: elastic resistance; Reps: repetitions; ex.: exercise; abd: abduction, add: adduction; min: minutes; sec: seconds; RM: Maximal repetition; Kg: kilogrames; Wk: week; US: ultrasound; FIG: flexibility intervention group; SIF: strength intervention group; HM: hip muscle; ROM: Range of Movement.
Table 5.
Hip muscle strengthening intervention protocol in patients with LBP.
| Warm-up | Central part | Return to calm | |
|---|---|---|---|
| Exercises | Joint mobility Muscular activation |
HM strengthening: Squat Monster Walk Quadruped hip extension Clam in side lying Bridge |
Relax Static stretch Manual therapy |
| Intensity | Minimum | 75-80% RM | |
| Volume | 2-3 sets / 8-12 reps for ex. 1 minute rest |
||
| Time | 5-10 minutes | 45-50 minutes | 5-10 minutes |
| Frequency | 3-4 days/week, with 1-2 days of rest between sessions. | ||
| Observations | The volume and intensity should be increased as the patient improves, increasing the number of repetitions and/or loads (elastic resistance or weight) | ||
| Abbreviations | RM: maximal repetition; reps: repetitions | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



