
Submitted:
17 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Background: Non-specific low back pain is a discomfort that affects individuals at any point in their lives. The study aim was to find the effects of Myofascial Release and Joint Mobilization on muscle thickness through ultrasonography in individuals experiencing non-specific low back pain. Methods: This double-blinded randomized clinical trial was conducted on 84 participants via convenient sampling. The interventions were given among three groups; joint mobilization, myofascial release and a combination of joint mobilization and myofascial release, with a common treatment of lumbar heating for 15 minutes and trunk stabilization exercises. Data was collected on a two-week treatment regimen (Days 1, 4, 8, and 12) and a one-month follow-up. Ultrasound evaluations were used to measure the thickness of deep Lumbar muscles at rest and contraction i.e. transverse abdominis (rTrA, cTrA) and lumbar multifidus (rLM, cLM). Repeated measure ANOVA was utilized to analyze follow-ups within groups and between groups, with post-hoc tests conducted to identify specific differences. Results: Significant increases in muscle thickness were observed over time in the transverse abdominis, with improvements in both rTrA (right, p = 0.001; left, p = 0.001) and cTrA (right, p = 0.001; left, p = 0.008). The lumbar multifidus also demonstrated significant changes, with increases in rLM (right, p = 0.001; left, p = 0.047) and cLM (right, p = 0.004; left, p = 0.037). However, the group main effects showed no significant differences on muscle thickness between the groups. Conclusions: Joint mobilization demonstrated increased effectiveness in improving muscle thickness relative to myofascial release and combining both treatments for individuals with non-specific low back pain. Future studies should address the sample diversity, gender distribution, and muscle composition assessment along with demographic and lifestyle factors.
Keywords:
Functional Disability
; Joint Mobilization
; Muscle Thickness
; Myofascial Release
; Non-Specific Low Back Pain
; Pain
; Range of Motion
1. Introduction
Nonspecific low back pain (NSLBP) is characterized by pain and discomfort localized between the costal margin and the lower gluteal folds, with or without radiation to the lower extremities, and is one of the prevalent health concerns among 4.2% and 19.6% of the population worldwide [1,2]. Patients with NSLBP have increased facet joint restrictions, myofascial thickening and reduced flexibility along the Lumbar region compared to healthy individuals, making them more susceptible to dysfunctions, due to its connections with surrounding structures [3]. Fascial dysfunctions such as inflammation, fibrosis, adhesions, fat infiltration, and structural abnormalities, underscore the critical role of the lumbopelvic fascia in the development of NSLBP [4,5,6].
Myofascial systems in the lumbar region that symbolize the tensegrity framework, formed by the fascia and deep muscles of the back, are essential for structural equilibrium, kinematics, and movement of the body [7]. These systems, particularly through the fascia with the transversus abdominis and multifidus, have direct connections to the facet joints, facilitating movement in the lumbopelvic region and enabling force transmission between the appendicular and axial skeletons [8,9]. Transversus abdominis and Lumbar Multifidus (LM), being local stabilizers, muscles are more prone to weakness compared to the global mobilizers, i.e. erector spinae, which tend to exhibit increased activity and force generation for gross movements [10]. Consequently, restrictions within these systems can lead to joint dysfunction by limiting movement and impairing overall biomechanical function [11].
Multiple treatment approaches can be used to treat NSLBP including pharmacological interventions, alternative medicine and conventional treatments [12]. Manual therapy such as Joint mobilization (JM) and Myofascial Release (MFR) has gained attention in recent years because of side-effects of pharmacological interventions [13]. JM is considered as an effective manual therapy approach for NSLBP, implies gentle oscillatory movements to joints, and elicit physiological responses such as pain relief, improved joint flexibility, reduced pain sensitivity, and modifications in muscle contraction or activity levels [14]. It modifies internal mechanical tension between vertebras [15] and assists individuals with NSLBP in temporarily alleviating discomfort [16], and impairment when compared to alternative therapies [17]. Despite variability in outcomes, JM is one of the therapeutic approaches in NSLBP [18,19].
Myofascial Release (MFR) is a type of manual therapy specifically targeting the myofascial system to enhance patient fitness and alleviate pain intensity, decrease muscle activity through the mechanical activation of mechanoreceptors located within the connective tissue, ultimately increase flexibility [8,9], and facilitate sliding between layers of soft tissues [7]. From a practical perspective, MFR entails gradually stretching the patient's muscles and fascia by hand to release the myofascial system from tension and dysfunction [20]. Studies demonstrate that even a single, isolated MFR treatment can improve lumbar spine range of motion, lower pain levels [21] and reduce the tightness of erector spinae and multifidus [22].
Ultrasound imaging is a non-invasive method that allows the visualization of tissue structures by using the reflection of ultrasound waves from heterogeneous tissues, allowing for quantitative assessment of subcutaneous structures, connective tissues, and muscles [23]. Previous studies have successfully utilized ultrasonography to analyze muscle thickness in the lumbar region both at rest and during contraction, as an indicator of muscle function and activation among healthy individuals [23,24]. However, there remains a gap to identify the effects of manual therapy treatment approaches i.e. JM and MFR on the TrA and LM muscles in patients with NSLBP [25].
This study aims to investigate the effects of joint mobilization (JM), myofascial release (MFR), and their combination on the thickness of the transversus abdominis [26] and lumbar multifidus (LM) muscles in individuals with non-specific low back pain (NSLBP).The findings could enhance clinical practice by delivering quantitative data on muscle thickness, offering insights for more effective treatment strategies, validating the effectiveness of ultrasonography in assessments, and promoting manual therapies as safer alternatives to pharmacological interventions
2. Materials and Methods
This randomized clinical trial was conducted at Al-Razi Healthcare and Riphah Rehabilitation Center, Lahore from April 25, 2021, to November 30, 2022, following the ethical guidelines established by the ethical committee of Riphah International University, Pakistan. The trial received approval from the Institutional Review Board (Ethics No. REC/RCR & AHS/23/36), ensuring adherence to the ethical standards set by the World Medical Association and the Helsinki Declaration of 1975. Additionally, the trial was registered on ClinicalTrials.gov (NCT04860726), https://clinicaltrials.gov/study/NCT04860726.
Sample size: The sample size was primarily determined through a pilot study involving 30 participants (10 in each group) and calculated using the n4studies software. The outcome measure used for sample size estimation was the "1-month reading thickness of contracted lumbar multifidus at the L4-L5 level on the right". By using a two-tailed independent test, expected mean change in the JM group, μ1 = 4.04 and variance = 0.60, expected mean change in the MFR group, μ2 = 4.50, variance = 0.54, Alpha (a) = 0.05, Z (0.975) = 1.96, Beta (β) = 0.20, Z (0.8)
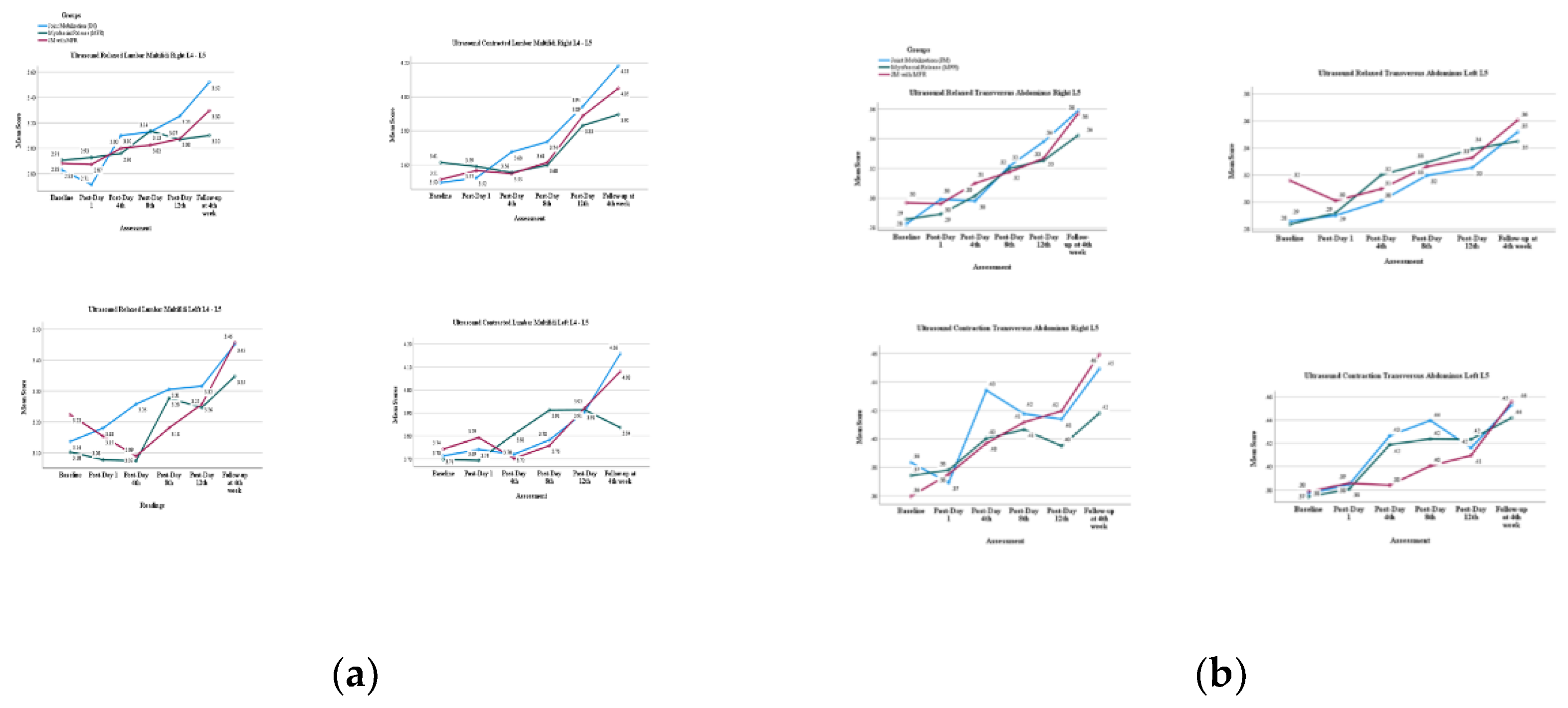
Based on these calculations, each group was planned to consist of 25 participants, total 75 participants across the three groups. To account for potential attrition, an additional 20% was incorporated, resulting in an adjusted sample size of 90. Following the study, 6 participants dropped out, leading to a final sample size of 84 participants [27].
Selection Criteria: The following selection criteria was considered in this study; Participants aged 20-50, diagnosed with NSLBP, who had not undergone any form of physical therapy or exercise regimen in the preceding three months, had NSLBP for less than three months, had refrained from the use of analgesics and non-steroidal anti-inflammatory drugs for the past 1 week [28], and those with disability rating Roland Morris disability questionnaire ≥8 were included [29]. Individuals with problems such as tumors, constitutional symptoms, integumentary issues, cauda equina syndromes or previously diagnosed with systemic issues, specific neuromusculoskeletal conditions, a recent history of trauma, prior surgical procedures, nerve blocks in the lumbosacral region, pregnant females or given birth within the last six months, and the inability to lie prone or supine for at least twenty minutes were excluded to overcome confounders [30]. All participants underwent a thorough screening and assessment process, in standing, supine, prone, and sitting positions. This evaluation incorporated special tests such as the straight leg raise (SLR), cross SLR, FABER (Flexion, Abduction, and External Rotation) test, femoral nerve stretch test, and a back inspection for potential deformities. To uphold study integrity, individuals with positive results on any of these assessments were excluded [28].
Data collection procedure: Data was collected on Day 1 (before and after treatment), at day 4,8 and 12 after the intervention , and follow up after a month. Participants were recruited after the informed consent, either through responses to flyers or referrals from general practitioners. The study adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines, as illustrated in Figure 1. Steps were taken to maintain the anonymity and confidentiality of the data collected. Patients were randomly allocated into three groups using an online randomization tool (https://www.randomizer.org), which ensures that each participant was assigned a number. The computer-generated allocation sequence was created prior to the start of the study, following the criteria established by GD Ruxton [31]. To maintain double blinding, both participants and assessors were blinded to group assignments, minimizing bias and ensuring the accuracy of the results. An independent assessor with more than five years’ experience in manual therapy were then randomly assigned to the experimental group.
Outcome measure: Muscle thickness was assessed using ultrasonography to evaluate the Transversus Abdominis and Lumbar Multifidus (LM) muscles.
Muscle thickness Assessment: Ultrasound imaging was performed in B-mode with a Toshiba Aplio MX ultrasound machine, using a 7-15 MHz linear probe and a 2-5 MHz curvilinear probe over the TrA and LM muscles, both at rest and contraction. Participants were in supine position for the TrA muscle thickness at rest. The transducer was placed slightly above the iliac crest along the mid-axillary line with hips and knees extended. To assess contraction, they were instructed "Raise your leg off the table without bending your knee approximately 8 inches” [32]. LM muscle thickness at rest was measured in prone position with a pillow under the abdomen to reduce lumbar curvature, at the L4-L5 zygapophyseal joint level. For contraction, LM thickness was assessed during a contralateral arm lift task, holding a weight proportional to body mass, similar to the mentioned position with elbows flexed at 90°, shoulders abducted at 120° and were instructed "Lift your arm approximately 2 inches off the table,"[30]. All procedures at rest and contraction were rehearsed once before image acquisition.
Intervention: A total of four treatment sessions according to the designated treatment groups, each lasting for 20 minutes, over a period of two-week (Days 1, 4, 8, and 12), were provided to the participants. In addition to their assigned interventions, all participants received standardized physical therapy, of heating pad for 15 minutes and trunk stabilization exercises [4].
1- Joint Mobilization: Participants were positioned prone, with arms either alongside the body or extending off the couch, and the head was turned comfortably to one side. The therapist applied the posteroanterior glides at L4-L5 facet joints using the hypothenar and fifth metacarpal of one hand, with the other hand superimposed. The treatment included oscillatory rocking motion of the upper trunk along a vertical axis with 3 sets of 10 repetitions each, using the concept of Maitland’s Vertebral Joint Mobilization. Grade III has large amplitude, nearing tissue stretch limits, whereas Grade IV has smaller amplitudes, pushing tissue to, or even beyond, its stretching capacity [33].
2- Myofascial Release: Participants adopted a side-lying position for contralateral evaluation. Utilizing ultrasound, the midpoint of the lateral raphe (LR) of the thoracolumbar fascia was identified between the TrA and the posterior musculofascial junction [25]. Manual pressure was vertically applied for 90-120 seconds following the technique outlined in "The Myofascial Release Manual" [34].
3- Combination of Joint Mobilization and Myofascial Release Participants were administered intervention of lumbar joint mobilization (Maitland PA Grade III & IV) with myofascial release
Data Analysis: All analysis was conducted using IBM SPSS version 26. Descriptive statistics were used to summarize the mean and standard deviation. The normality of the data was assessed through the Kolmogorov-Simrov test. Repeated measures ANOVA was utilized to analyze follow-ups within groups and between groups, with post-hoc tests. Percentage changes in outcome measures within each group were calculated using mean and standard deviation. Interventionary studies involving animals or humans, and other studies that require ethical approval, must list the authority that provided approval and the corresponding ethical approval code.
3. Results

Table 1.
Between group comparison of baseline characteristics.
| Joint Mobilization (JM) (n= 28) |
Myofascial Release (MFR) (n=27) |
Joint Mobilization with Myofascial Release (JM+MFR) (n=29) |
p-value | |
|---|---|---|---|---|
| Age of the patient (years) | 29.07 ± 6.82 | 32.52±10.04 | 28.90±8.47 | 0.212 |
| Height of patient | 167.81 ± 8.12 | 162.10±6.56 | 165.12±8.07 | 0.026 |
| Weight of patient (kg) | 70.05 ± 14.68 | 68.60±13.23 | 65.08±13.53 | 0.382 |
| BMI of patient (kg/m2 ) | 25.09± 4.78 | 26.08±4.53 | 23.90±4.97 | 0.237 |
| Working hour | 9.14±2.90 | 9.33±3.56 | 9.69±4.54 | 0.855 |
| RMDQ 1 | 16.55±4.42 | 15.67±4.63 | 16.31±5.06 | 0.937 |
1 Body Mass Index (BMI), Roland Morris disability questionnaire (RMDQ).
Repeated measures ANOVA (Table 2) results for the Transversus Abdominis and Lumbar Multifidus (LM) muscles, both at rest and during contraction, measurements showed statistically significant increases (p < 0.001) from baseline to follow-up assessments, particularly in the Joint Mobilization (JM) group. These findings indicate a positive effect of the intervention on muscle thickness across all evaluated variables, with the most notable improvements observed in the Joint Mobilization treatment.
Figure 3.
Time main effect of muscle thickness across three groups (JM, MFR, JM+MFR) on : (a) lumbar multifidus; (b) tramsverse abdominus.
Figure 3.
Time main effect of muscle thickness across three groups (JM, MFR, JM+MFR) on : (a) lumbar multifidus; (b) tramsverse abdominus.
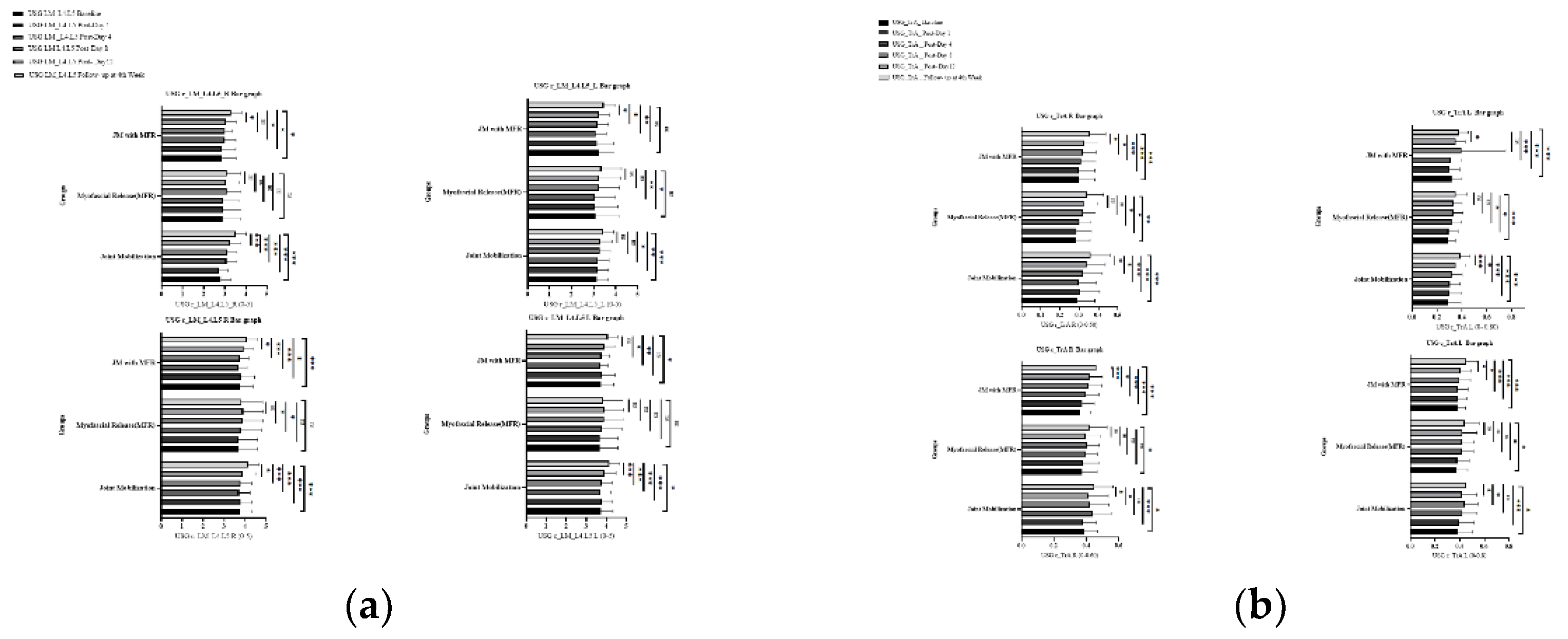
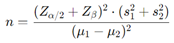
Table 3 displays the percentage changes in muscle activity for resting and contracting Transversus Abdominis and Lumbar Multifidus (LM) across the Joint Mobilization (JM), Myofascial Release (MFR), and combined JM+MFR groups. While muscle thickness improved in all groups, no significant differences were observed between the treatments, indicating similar effects across the interventions. Notably, the right TrA at L5 showed a percentage change of 21.4% for JM, 34.9% for MFR, and 33.0% for JM+MFR, highlighting the most significant improvement with MFR. Overall, these results suggest that both JM and MFR can enhance muscle thickness, but the combined approach does not significantly outperform the individual therapies.
Figure 4.
Group main effect of muscle thickness across three groups (JM, MFR, JM+MFR) on : (a) lumbar multifidus; (b) transversus abdominus.
Figure 4.
Group main effect of muscle thickness across three groups (JM, MFR, JM+MFR) on : (a) lumbar multifidus; (b) transversus abdominus.
4. Discussion
This study aims to assess the effects of Joint Mobilization (JM), Myofascial Release (MFR), and their combination (JM+MFR) on muscle thickness in individuals with non-specific low back pain (NSLBP). By measuring changes in muscle thickness, the research seeks to provide a clearer understanding of how these interventions may influence muscle thickness and contribute to the management of NSLBP.
Both interventions; joint mobilization and myofascial release demonstrated positive outcomes on muscle thickness by minimizing spinal stiffness and fascial adhesions, with joint mobilization exhibiting significant effects. Joint mobilization at lumbar facet joints promotes multifidus activation directly and transverses abdominis through thoracolumbar fascia by regaining spinal mobility, enhancing proprioception, neuromuscular control and activation during functional tasks [35]. These findings are consistent with Choi et al., reported significant improvements in muscle performance and lumbar stability following joint mobilization [36]. On the other hand, fascial adhesions in the thoracolumbar fascia and lateral raphe, reduce the recruitment of adjoining muscles, are decreased by MFR. Ajimsha et al., highlighted the efficacy of myofascial release in improving myofascial flexibility, blood circulation, and pain [37] that could be a contributing reason to increase muscle thickness as seen in this study.
Increases in rTrA and cTrA thickness were observed in all groups: JM, MFR, and JM+MFR, yet no distinct differences between the groups were found. Statistical analysis confirmed a significant effect of time (p < 0.05) on muscle thickness, indicating that the interventions improved muscle thickness after a series of follow ups. However, group main effects and time-group interactions were not significant (p > 0.05), suggesting all groups demonstrated improvements but no single treatment consistently outperformed the others at different follow-up points. This aligns with previous research suggesting that the manual interventions can enhance the activation of stabilizing muscles, though the degree of effectiveness may be similar across different treatment modalities [38]. In Contrast, Lin et al, conducted a study on thoracic spine, found a significant group main effect and time into group interactions stating significant differences between mobilization and soft tissue release group [39,40]. Additionally, the current study found insignificant differences at every measurement point between the groups compared to the Lin et al, representing a substantial temporal effect at every measured point [39].
The thickness of rLM and cLM is significant in JM and JM+MFR compared to MFR among NSLBP as within group difference indicates the anatomical distribution of LM in close vicinity to Lumbar facets and enhanced mobility after joint mobilization may have increased tissue elasticity of the surrounding muscles. The results are consistent with the study focused on joint manipulation as the manual treatment approach representing improvement in thickness of LM. This may be due to g-motoneuron modulation through mobilization as one of the underlying processes of improvement [41]. Mitchell UH et al., found no association between LM and JM among healthy patients compared to NSLBP patients. Lumbar dysfunction may be a reason for change in thickness of LM that was improved after the interventions in the current study [42].
In this study, all the interventions across TrA and LM showed improvements of percentage change more dominantly on the right side, rTrA, rLM and cLM compared to the left, cTrA. These differences may be due to dominant side of the body may be attributed to compensatory mechanisms and the connections to fascial realignments during lumbar stabilization tasks, specifically, the left TrA may engage more due to the additional load on the right side, resulting in increased muscle recruitment [43,44]. Consequently, the LM, particularly on the right side, demonstrated a greater impact during day to day activities owing to involvement of right posterior back line [45]. This finding emphasizes the vital importance of focusing on the TrA and LM to improve lumbopelvic stability during complex functional movements, leading to increased muscle thickness and activation of motor unit recruitment on the dominant side [46,47].
The transversus abdominis and lumbar multifidus (LM) muscles reveals insights into physiological responses and methodological factors affecting outcomes. Notably, the right TrA (rTrA) thickness increased significantly from baseline measurements (0.28 ± 0.09) to follow-up (0.36 ± 0.10) after joint mobilization, indicating enhanced muscle engagement linked to the intervention. However, temporary declines observed between Day 1 and Day 4 could suggest short-lived fatigue or localized inflammation [48]. In the case of the right LM (rLM), an initial reduction in thickness from 3.52 ± 0.54 to 2.73 ± 0.43, followed by a recovery to 4.18 ± 0.58, corresponds with the body's acute response to therapeutic loading and the adaptations that follow [49]. Individual variability in baseline muscle function, recovery abilities, and biomechanics may explain these patterns [50]. Moreover, the timing of assessments in relation to treatment could reflect temporary rather than consistent changes in muscle condition [51].
For the TrA, significant improvements in muscle thickness were observed in all treatment groups, with JM showing greater effectiveness than both JM+MFR and MFR. In contrast, for the LM, JM again outperformed JM+MFR, while no significant effects were detected in the MFR group. One reason for the effectiveness of the JM approach could be its direct impact on stabilizing the lumbar region and facilitating joint mobility through enhanced fascial attachments. This stabilization likely promotes better activation of adjacent muscles, contributing to improved outcomes [52]. In contrast, the JM+MFR group showed different results, potentially due to the combined interventions. While MFR alone did not produce significant changes in the LM, the additional benefits of JM may have amplified the effects on muscle activation and coordination. The lack of significant change in multifidus could be related to the small size of LM and the limitations of the MFR technique itself. Furthermore, employing measures such as cross-sectional area might yield more precise evaluations of muscle girth changes due to these interventions in LM [53,54]. Future research, to delineate these effects, which could enhance our understanding of effective rehabilitation strategies.
Limitations and Recommendations: The study encountered limitations primarily stemming from the non-homogenous sample size as it affects both internal and external validity by limiting the generalizability of the population. Additionally, the gender ratio was not addressed which limits the understanding of any particular needs of each intervention as well as leads to gender selection biases. Furthermore, consistency changes in the muscles (fatty deposits or fibrous/connective tissue infiltration) were not assessed during USG. Expand measurements beyond muscle thickness to include a cross-sectional area for a more detailed understanding in the future. Consider variables such as age, a lack of physical activity, obesity, blood flow, and participation in gym activities to explore correlations with muscle thickness for future studies. Future research should take a more comprehensive approach by thoroughly assessing participants' daily activities, work environments, and ergonomic practices.
5. Conclusions
Joint mobilization demonstrated increased effectiveness in improving muscle thickness relative to myofascial release and combining both treatments for individuals with non-specific low back pain. Overall, these findings provide valuable insights into the management of NSLBP by targeting deep lumbar region muscles, specifically the transverse abdominis and lumbar multifidus.
Author Contributions
Hafiz Muhammad Waseem Javaid, Syed Shakil-ur-Rehman, Muhammad Kashif, Muhammad Salman Bashir, and Wajeeha Zia participated in the design, drafting, writing, and collection and assembly of data. Syed Shakil-ur-Rehman and Muhammad Kashif contributed to the conception and study design. Muhammad Salman Bashir and Wajeeha Zia were involved in calculating the sample size and performing statistical analysis. Hafiz Muhammad Waseem Javaid and Muhammad Kashif assisted in the design of the study and helped draft and format the manuscript. Syed Shakil-ur-Rehman and Hafiz Muhammad Waseem Javaid contributed to critical revisions of the article for significant intellectual content. All authors participated in data interpretation, editing, critical revisions, and approval of the final manuscript, ensuring accountability for its accuracy.
Funding
This research received no external funding.
Institutional Review Board Statement
Riphah International University's Institutional Review Board (Ethics No. REC/RCR & AHS/23/36) approved the study in compliance with the ethical standards of the World Medical Association and the Helsinki Declaration of 1975.
Informed Consent Statement
Informed consent was obtained from each subject before participating in the study.
Data Availability Statement
The data supporting the findings of this study are available upon request from the corresponding author due to privacy and ethical restrictions. No new data were generated in this study. Further inquiries regarding data access can be directed to kashif.shaffi@riphah.edu.pk ; wasim8001@gmail.com.
Acknowledgments
I would like to express my sincere gratitude to Maham Pervaiz, Ahmed Shahbaz, Hamna Sarfraz, Syeda Saba Zaidi, and Abeera Shakeel for their invaluable administrative and technical support throughout this research. Their contributions greatly facilitated the completion of our work and enriched the overall research experience.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| cLM | Contracting Lumbar Multifidus |
| cTrA | Contracting Transversus Abdominis |
| JM | Joint Mobilization |
| JM+MFR | Joint Mobilization with Myofascial Release |
| L | Left |
| LM | Lumbar Multifidus |
| MFR | Myofascial Release |
| R | Right |
| rLM | Resting Lumbar Multifidus |
| RMDQ | Roland Morris Disability Questionnaire |
| rTrA | Resting Transversus Abdominis |
| TA | Transversus Abdominis |
| USG | Ultrasonography |
References
- Harrianto R. Biomechanical aspects of nonspesific low back pain. Universa Medicina. 2010;29(3):177-87. [CrossRef]
- Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Revista de saude publica. 2015;49:73. [CrossRef]
- Myers T, Earls J. Fascial Release for Structural Balance, Revised Edition: Putting the Theory of Anatomy Trains into Practice: North Atlantic Books; 2017.
- Freiwald J, Magni A, Fanlo-Mazas P, Paulino E, Sequeira de Medeiros L, Moretti B, et al. A role for superficial heat therapy in the management of non-specific, mild-to-moderate low back pain in current clinical practice: A narrative review. Life. 2021;11(8):780. [CrossRef]
- Gatton M, Pearcy M, Pettet G, Evans J. A three-dimensional mathematical model of the thoracolumbar fascia and an estimate of its biomechanical effect. J Biomech. 2010;43(14):2792-7. [CrossRef]
- Wilke J, Krause F, Vogt L, Banzer W. What is evidence-based about myofascial chains: a systematic review. Arch Phys Med Rehabil. 2016;97(3):454-61. [CrossRef]
- Ożóg P, Weber-Rajek M, Radzimińska A. Effects of isolated myofascial release therapy in patients with chronic low back pain—A systematic review. J Clin Med. 2023;12(19):6143. [CrossRef]
- Arguisuelas M, Lisón J, Doménech-Fernández J, Martínez-Hurtado I, Coloma PS, Sánchez-Zuriaga D. Effects of myofascial release in erector spinae myoelectric activity and lumbar spine kinematics in non-specific chronic low back pain: Randomized controlled trial. Clin biomech. 2019;63:27-33. [CrossRef]
- Arguisuelas MD, Lisón JF, Sánchez-Zuriaga D, Martínez-Hurtado I, Doménech-Fernández J. Effects of myofascial release in nonspecific chronic low back pain: a randomized clinical trial. Spine. 2017:. [CrossRef]
- Mehyar F, Santos M, Wilson SE, Staggs VS, Sharma NK. Immediate effect of lumbar mobilization on activity of erector spinae and lumbar multifidus muscles. J Chiropr Med. 2017;16(4):271-8. [CrossRef]
- Tamartash H, Bahrpeyma F, Dizaji MM. Effect of remote myofascial release on lumbar elasticity and pain in patients with chronic nonspecific low back pain: A randomized clinical trial. J Chiropr Med. 2023;22(1):52-9. [CrossRef]
- do Nascimento PR, Costa LO, Araujo AC, Poitras S, Bilodeau M. Effectiveness of interventions for non-specific low back pain in older adults. A systematic review and meta-analysis. Physiotherapy. 2019;105(2):147-62. [CrossRef]
- Sharma C, Sachan K. Exercise Therapy Protocols in Treatment of Non-Specific Low Back Pain-A Literature Review. Indian J Physiother Rehabil. 2024;3(4):204-11.
- Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531-8. [CrossRef]
- Lin C-F, Jankaew A, Tsai M-C, Liao J-C. Immediate effects of thoracic mobilization versus soft tissue release on trunk motion, pain, and lumbar muscle activity in patients with chronic low back pain. J Bodyw Mov Ther. 2024;40:1664-71. [CrossRef]
- Fagundes Loss J, de Souza da Silva L, Ferreira Miranda I, Groisman S, Santiago Wagner Neto E, Souza C, et al. Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial. Chiropr Man Therap. 2020;28:1-10. [CrossRef]
- Outeda LR, Cousiño LAJ, Carrera IdC, Caeiro EML. Effect of the maitland concept techniques on low back pain: a systematic review. Coluna. 2022;21(2):e258429. [CrossRef]
- Furlan AD, Yazdi F, Tsertsvadze A, Gross A, Van Tulder M, Santaguida L, et al. A systematic review and meta-analysis of efficacy, cost-effectiveness, and safety of selected complementary and alternative medicine for neck and low-back pain. EBCAM. 2012;2012(1):953139. [CrossRef]
- Bronfort G, Haas M, Evans RL, Bouter LM. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. Spine J. 2004;4(3):335-56. [CrossRef]
- Manheim C. The myofascial release manual. 4 ed: Taylor & Francis; 2024.
- Tozzi P, Bongiorno D, Vitturini C. Fascial release effects on patients with non-specific cervical or lumbar pain. J Bodyw Mov Ther. 2011;15(4):405-16. [CrossRef]
- Ożóg P, Weber-Rajek M, Radzimińska A, Goch A. Analysis of muscle activity following the application of myofascial release techniques for low-back pain—a randomized-controlled trial. J Clin Med. 2021;10(18):4039. [CrossRef]
- Langevin HM, Konofagou EE, Badger GJ, Churchill DL, Fox JR, Ophir J, et al. Tissue displacements during acupuncture using ultrasound elastography techniques. Ultrasound Med Biol 2004;30(9):1173-83. [CrossRef]
- Tamartash H, Bahrpeyma F, Dizaji MM. Effect of Myofascial Release Technique on Lumbar Fascia Thickness and Low Back Pain: A Clinical Trial. J Mod Rehabil. 2022;16(3):244-51. [CrossRef]
- Chen Y-H, Chai H-M, Shau Y-W, Wang C-L, Wang S-F. Increased sliding of transverse abdominis during contraction after myofascial release in patients with chronic low back pain. Man ther. 2016;23:69-75. [CrossRef]
- Lopez P, Radaelli R, Taaffe DR, Newton RU, Galvão DA, Trajano GS, et al. Resistance training load effects on muscle hypertrophy and strength gain: systematic review and network meta-analysis. Med Sci Sports Exerc. 2020;53(6):1206. [CrossRef]
- Ngamjarus C. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med J. 2016;68(3):160-70.
- Hussein DAMM, Choy APCY, Singh DD, Cardosa DMS, Mansor PM, Hasnan DN, et al. Malaysian Low Back Pain Management Guideline [Available from: https://www.masp.org.my/index.cfm?&menuid=23.
- Payares K, Lugo LH, Restrepo A. Validation of the Roland Morris questionnaire in Colombia to evaluate disability in low back pain. Spine. 2015;40(14):1108-14. [CrossRef]
- Koppenhaver SL, Hebert JJ, Fritz JM, Parent EC, Teyhen DS, Magel JS. Reliability of rehabilitative ultrasound imaging of the transversus abdominis and lumbar multifidus muscles. Arch Phys Med Rehabil. 2009;90(1):87-94. [CrossRef]
- Ruxton G. Allocation concealment as a potentially useful aspect of randomised experiments. Behav Ecol Sociobiol. 2017;71:1-3. [CrossRef]
- Narouei S, hossein Barati A, hossein Alizadeh M, Akbari A, Ghiasi F. Intrarater reliability of rehabilitative ultrasound imaging of the gluteus maximus, lumbar multifidus and transversus abdominis muscles in healthy subjects. Sport Sci 2016;1(1-2016):1-11.
- Hengeveld E, Banks K. Maitland's Vertebral Manipulation: Management of Neuromusculoskeletal Disorders-Volume 1: Health Sci; 2013.
- Barnes MF. The basic science of myofascial release: morphologic change in connective tissue. J Bodyw Mov Ther. 1997;1(4):231-8.
- Hicks GE, Simonsick EM, Harris TB, Newman AB, Weiner DK, Nevitt MA, et al. Trunk muscle composition as a predictor of reduced functional capacity in the health, aging and body composition study: the moderating role of back pain. J Gerontol A Biol Sci Med Sci. 2005;60(11):1420-4. [CrossRef]
- Choi W, Lee J, Lee S. Effects of lumbar joint mobilization on trunk function, postural balance, and gait in patients with chronic stroke: A randomized pilot study. J Back Musculoskelet Rehabil. 2023;36(1):79-86. [CrossRef]
- Ajimsha M, Al-Mudahka NR, Al-Madzhar J. Effectiveness of myofascial release: systematic review of randomized controlled trials. J Bodyw Mov Ther. 2015;19(1):102-12.
- Azadinia F, Takamjani IE, Kamyab M, Kalbassi G, Sarrafzadeh J, Parnianpour M. The effect of lumbosacral orthosis on the thickness of deep trunk muscles using ultrasound imaging: A randomized controlled trial in patients with chronic low back pain. Am J Phys Med. 2019;98(7):536-44.
- Lin C-F, Jankaew A, Tsai M-C, Liao J-C. Immediate effects of thoracic mobilization versus soft tissue release on trunk motion, pain, and lumbar muscle activity in patients with chronic low back pain. J Bodyw Mov Ther. 2024;40:1664-71.
- Shah YK. The effects of myofascial manual therapy on muscle activity and blood flow in people with low back pain: University of Kent (United Kingdom); 2017.
- Brenner AK, Gill NW, Buscema CJ, Kiesel K. Improved activation of lumbar multifidus following spinal manipulation: a case report applying rehabilitative ultrasound imaging. J Orthop Sports Phys Ther. 2007;37(10):613-9. [CrossRef]
- Kirsebom O, Jones S, Strömberg D, Martínez-Pinedo G, Langanke K, Röpke F, et al. This is a self-archived version of an original article. This version may differ from the original in pagination and typographic details. Phys Rev Lett. 2019;123:262701. [CrossRef]
- Mikołajowski G, Pałac M, Wolny T, Linek P. Lateral abdominal muscles shear modulus and thickness measurements under controlled ultrasound probe compression by external force sensor: a comparison and reliability study. Sensors. 2021;21(12):4036. [CrossRef]
- Tsartsapakis I, Bagioka I, Fountoukidou F, Kellis E. A Comparison between Core Stability Exercises and Muscle Thickness Using Two Different Activation Maneuvers. J Funct Morphol Kinesiol. 2024;9(2):70.
- Myers TW. Anatomy trains: myofascial meridians for manual and movement therapists: Elsevier Health Sciences; 2009.
- Bohunicky S, Rutherford L, Harrison K-L, Malone Q, Glazebrook CM, Scribbans TD. Immediate effects of myofascial release to the pectoral fascia on posture, range of motion, and muscle excitation: a crossover randomized clinical trial. J Man Manip Ther. 2024:1-11. [CrossRef]
- Pfluegler G, Kasper J, Luedtke K. The immediate effects of passive joint mobilisation on local muscle function. A systematic review of the literature. Musculoskeletal Sci Pract. 2020;45:102106. [CrossRef]
- Ferreira PH, Ferreira ML, Hodges PW. Changes in recruitment of the abdominal muscles in people with low back pain: ultrasound measurement of muscle activity. Spine. 2004;29(22):2560-6. [CrossRef]
- Hides J, Stanton W, McMahon S, Sims K, Richardson C. Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. J Orthop Sports Phys Ther. 2008;38(3):101-8.
- Nourbakhsh MR, Arab AM. Relationship between mechanical factors and incidence of low back pain. J Orthop Sports Phys Ther. 2002;32(9):447-60. [CrossRef]
- De Martino E, Hides J, Elliott JM, Hoggarth M, Zange J, Lindsay K, et al. Lumbar muscle atrophy and increased relative intramuscular lipid concentration are not mitigated by daily artificial gravity after 60-day head-down tilt bed rest. J Appl Physiol. 2021;131(1):356-68. [CrossRef]
- Puentedura EJ, Landers MR, Hurt K, Meissner M, Mills J, Young D. Immediate effects of lumbar spine manipulation on the resting and contraction thickness of transversus abdominis in asymptomatic individuals. J Orthop Sports Phys Ther. 2011;41(1):13-21. [CrossRef]
- Ciccotelli J. Lumbopelvic Biomechanics and Muscle Performance in Individuals with Unilateral Transfemoral Amputation: Implications for Lower Back Pain: University of Nevada, Las Vegas; 2023.
- Barker PJ, Guggenheimer KT, Grkovic I, Briggs CA, Jones DC, Thomas CDL, et al. Effects of tensioning the lumbar fasciae on segmental stiffness during flexion and extension: Young Investigator Award winner. Spine. 2006;31(4):397-405. [CrossRef]
Figure 1.
CONSORT.
Figure 2.
Therapist applying lumbar joint mobilization (Maitland PA Grade III & IV) and myofascial release to target Lateral Raphe.
Figure 2.
Therapist applying lumbar joint mobilization (Maitland PA Grade III & IV) and myofascial release to target Lateral Raphe.
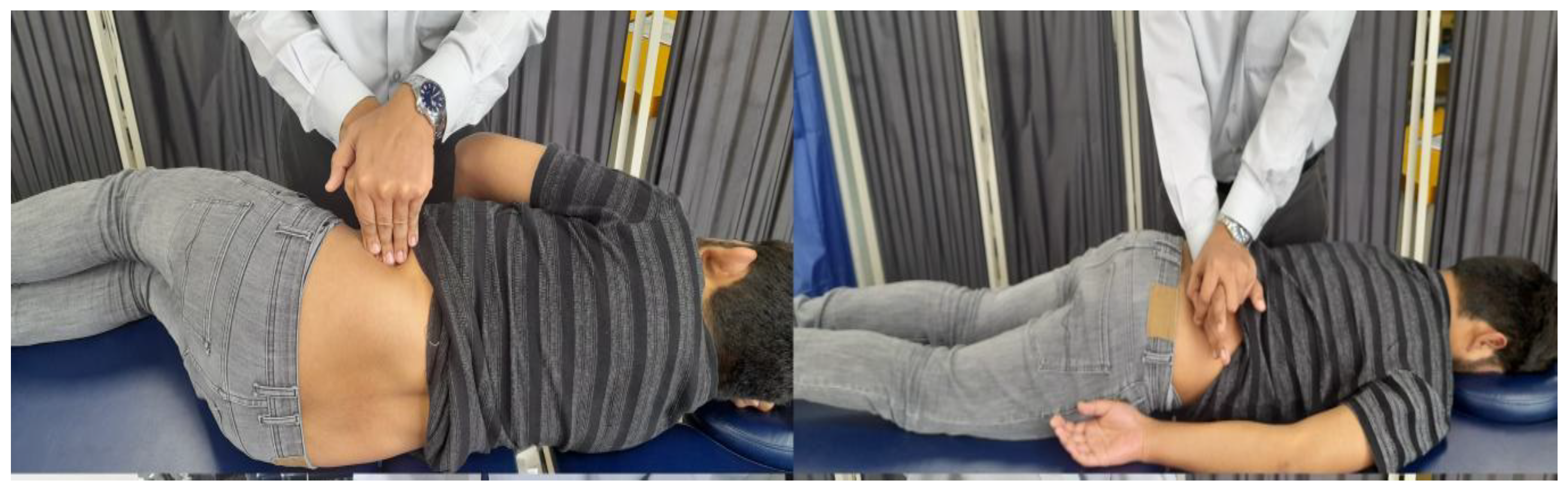
Table 2.
Mean Score comparison within and between groups, and Time and Group Interaction.
| Assessment | RM-ANOVA | Time main effect | Group Main effect | Time *Group interaction effect | |||||||||||||
| Groups | Baseline | Post-Day 1 | Post-Day 4th | Post-Day 8th | Post-Day 12th | Follow-up in 4th week | Sig. | F-value (Effect Size) | Sig. | F-value (Effect Size) | Sig. | F-value (Effect Size) | Sig. | ||||
| USG2 | rTrA | R | L5 | JM | 0.28±0.09 | 0.31±-0.10 | 0.30±0.09 | 0.32±0.10 | 0.34±0.10 | 0.36±0.10 | 0.001 | 19.57 (0.207) | 0.000 | 0.244 (0.006) | 0.784 | 0.36 (0.009) | 0.904 |
| MFR | 0.28±0.07 | 0.29±0.08 | 0.30±0.06 | 0.32±0.06 | 0.33±0.07 | 0.34±0.08 | 0.001 | ||||||||||
| JM+MFR | 0.29±0.08 | 0.30±0.09 | 0.31±0.08 | 0.32±0.70 | 0.33±0.07 | 0.35±0.08 | 0.001 | ||||||||||
| Sig. | 0.84 | 0.71 | 0.82 | 0.97 | 0.82 | 0.76 | |||||||||||
| L | JM | 0.28 ±0.09 | 0.30±0.10 | 0.30±0.08 | 0.32±0.08 | 0.33±0.08 | 0.35 ±0.07 | 0.001 | 43.76 (0.369) | 0.016 | 0.273 (0.034) | 0.273 | 0.39 (0.10) | 0.646 | |||
| MFR | 0.28 ±0.06 | 0.29±0.08 | 0.32±0.08 | 0.33±0.08 | 0.34±0.35 | 0.34 ±0.09 | 0.001 | ||||||||||
| JM+MFR | 0.32 ±0.08 | 0.30±0.08 | 0.31±0.08 | 0.40±0.35 | 0.33±0.08 | 0.36 ±0.07 | 0.227 | ||||||||||
| Sig. | 0.30 | 0.92 | 0.72 | 0.37 | 0.82 | 0.75 | |||||||||||
| cTrA | R | L5 | JM | 0.38±0.08 | 0.38±0.09 | 0.44±0.11 | 0.42±0.12 | 0.41±0.12 | 0.44±0.11 | 0.001 | 17.19 (0.186) | 0.000 | 0.229 (0.006) | 0.796 | 1.33 (0.034) | 0.235 | |
| MFR | 0.37±0.09 | 0.38±0.10 | 0.40±0.70 | 0.41±0.07 | 0.40±0.10 | 0.41±0.10 | 0.090 | ||||||||||
| JM+MFR | 0.35±0.06 | 0.38±0.07 | 0.40±0.08 | 0.41±0.08 | 0.42±0.08 | 0.45±0.09 | 0.001 | ||||||||||
| Sig. | 0.44 | 0.99 | 0.15 | 0.78 | 0.62 | 0.33 | |||||||||||
| L | JM | 0.37 ±0.12 | 0.39±0.13 | 0.42±0.12 | 0.44±0.11 | 0.42±0.12 | 0.45 ±0.11 | 0.008 | 17.69 (0.191) | 0.221 | 0.056 (0.001) | 0.936 | 1.12 (0.029) | 0.350 | |||
| MFR | 0.37±0.09 | 0.38±0.10 | 0.42±0.10 | 0.42±0.10 | 0.42±0.12 | 0.44 ±0.12 | 0.004 | ||||||||||
| JM+MFR | 0.37 ±0.06 | 0.39±0.07 | 0.38±0.08 | 0.40±0.09 | 0.41±0.08 | 0.45 ±0.09 | 0.001 | ||||||||||
| Sig. | 0.96 | 0.88 | 0.30 | 0.31 | 0.89 | 0.87 | |||||||||||
| rLM | R | L4.L5 | JM | 3.52±0.54 | 2.73±0.43 | 3.08±0.50 | 3.12±0.47 | 3.25±0.53 | 4.18±0.58 | 0.001 | 1.52 (0.020) | 0.001 | 1.490 (0.038) | 0.232 | 1.49 (0.038) | 0.231 | |
| MFR | 3.59±0.84 | 2.92±0.88 | 2.92±0.73 | 3.10±0.69 | 3.07±0.59 | 3.89±0.76 | 0.265 | ||||||||||
| JM+MFR | 3.51±0.55 | 2.87±0.64 | 3.00±0.52 | 3.02±0.35 | 3.08±0.47 | 4.05±0.53 | 0.008 | ||||||||||
| Sig. | 0.92 | 0.56 | 0.60 | 0.40 | 0.36 | 0.03 | |||||||||||
| L | JM | 3.14 ±0.53 | 3.18±0.49 | 3.21±0.49 | 3.28±0.47 | 3.32±0.52 | 3.45 ±0.47 | 0.047 | 6.34 (0.078) | 0.001 | 0.288 (0.008) | 0.751 | 0.846 (0.015) | 0.736 | |||
| MFR | 3.07 ±1.06 | 3.05±1.05 | 3.05±0.94 | 3.24±0.92 | 3.25±0.97 | 3.35 ±0.91 | 0.063 | ||||||||||
| JM+MFR | 3.22 ±0.72 | 3.15±0.75 | 3.10±0.49 | 3.18±0.48 | 3.26±0.45 | 3.45 ±0.53 | 0.093 | ||||||||||
| Sig. | 0.78 | 0.80 | 0.65 | 0.83 | 0.92 | 0.79 | |||||||||||
| cLM | R | L4.L5 | JM | 3.53±0.54 | 3.56±0.49 | 3.68±0.48 | 3.74±0.51 | 3.95±0.66 | 4.18±0.59 | 0.001 | 17.98 (0.193) | 0.000 | 0.316 (0.008) | 0.730 | 1.01 (0.026) | 0.417 | |
| MFR | 3.59±0.84 | 3.58±0.85 | 3.52±0.81 | 3.55±0.81 | 3.83±0.70 | 3.89±0.76 | 0.063 | ||||||||||
| JM+MFR | 3.51±0.55 | 3.57±0.58 | 3.55±0.43 | 3.61±0.44 | 3.89±0.40 | 4.05±0.53 | 0.001 | ||||||||||
| Sig. | 0.87 | 0.99 | 0.58 | 0.49 | 0.79 | 0.26 | |||||||||||
| L | JM | 3.74 ±0.58 | 3.78±0.54 | 3.71±0.53 | 3.78±0.52 | 3.91±0.58 | 4.16 ±0.51 | 0.003 | 6.19 (0.76) | 0.001 | 0.239 (0.003) | 0.890 | 1.102 (0.029) | 0.360 | |||
| MFR | 3.68 ±0.89 | 3.68±0.91 | 3.80±0.97 | 3.88±0.95 | 3.91±0.95 | 3.82 ±0.98 | 0.287 | ||||||||||
| JM+MFR | 3.74 ±0.63 | 3.79±0.65 | 3.70±0.38 | 3.76±0.42 | 3.92±0.49 | 4.10 ±0.48 | 0.037 | ||||||||||
| Sig. | 0.94 | 0.82 | 0.82 | 0.75 | 0.99 | 0.22 | |||||||||||
2 Joint Mobilization (JM), Myofascial Release (MFR), Joint Mobilization with Myofascial Release (JM+MFR), Lumbar Multifidus, Transverses Abdominis , Ultrasonography (USG), Resting Transverses Abdominis (rTrA), Contracting Transverses Abdominis (cTrA), Resting Lumbar Multifidus (rLM), Contracting Lumbar Multifidus (cLM), R= Right (R), Left (L).
Table 3.
Percentage changes and multiple comparisons.
| Percentage change | Multiple Comparison Test -Mean Difference with significance | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| JOINT MOBILIZATION (JM) | MYOFASCIAL RELEASE (MFR) | JOINT MOBILIZATION with MYOFASCIAL RELEASE (JM+MFR) | (JM) vs (MFR) | (JM) vs (JM+MFR) | (MFR) vs (JM+MFR) | ||||
| Mean ± S.D | M.D (Sig.) | ||||||||
| USG 3 | rTrA | R | L5 | 21.4±28.3 | 34.9±29.8 | 33.0±35.5 | 0.006 (1.00) | -0.0010 (1.00) | -0.0067 (1.00) |
| L | 32.49±51.28 | 30.27±34.55 | 25.19±33.59 | -0.0059 (1.00) | -0.0236 (0.62) | -0.0177 (1.00) | |||
| cTrA | R | L5 | 18.6±24.2 | 25.4±29.7 | 22.9±31.2 | 0.016 (1.00) | 0.0075 (1.00) | -0.0084 (1.00) | |
| L | 29.56±37.45 | 29.03±32.43 | 22.72±26.95 | 0.0056 (1.00) | 0.0137 (1.00) | 0.0081 (1.00) | |||
| rLM | R | L4.L5 | 22.9±26.1 | 18.9±33.0 | 21.9±28.5 | 0.075 (1.00) | -0.066 (0.87) | -0.0087 (0.99) | |
| L | 12.36±17.56 | 13.47±29.08 | 13.40±30.76 | 0.087 (1.00) | 0.0476 (1.00) | -0.039 (1.00) | |||
| cLM | R | L4.L5 | 15.6±20.6 | 20.9±31.0 | 18.2±22.9 | 0.078 (1.00) | 0.063 (1.00) | -0.016 (1.00) | |
| L | 13.56±22.04 | 7.65±20.99 | 1.85±24.51 | 0.026 (1.00) | 0.004 (1.00) | -0.023 (1.00) | |||
3 Joint Mobilization (JM), Myofascial Release (MFR), Joint Mobilization with Myofascial Release (JM+MFR), Lumbar Multifidus, Transverses Abdominis , Ultrasonography (USG), Resting Transverses Abdominis (rTrA), Contracting Transverses Abdominis (cTrA), Resting Lumbar Multifidus (rLM), Contracting Lumbar Multifidus (cLM), R= Right (R), Left (L).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



