
Submitted:
22 May 2023
Posted:
23 May 2023
You are already at the latest version
Abstract
Background: In this paper, it was aimed to evaluate the biomarker potential as well as the effect of the prognostic nutritional index (PNI), which is calculated using the albumin level reflecting nutritional status and lymphocyte count reflecting immune status, in determining the prognosis of metastatic castration-sensitive prostate cancer (mCSPC).
Methods: This retrospective observational study included the complete data of 108 patients with mCPSC who were treated for at least three months between January 1, 2010, and June 1, 2021. The relationship between cancer specific survival (CSS), overall survival (OS), progression free survival (PFS) and PNI was evaluated. Kaplan-Meier method for OS, PFS, and CSS, as well as univariate and multivariate Cox regression models were used in statistical analyses.
Results: The median age of 108 patients included in the study was 68.54 (61.05-74.19) years. While 71.3% (n = 77) of the patient population were high-volume according to CHAARTED, 52.8% (n = 57) were high-risk based on LATITUDE. 49.75 was determined as the best cut-off point for the PNI. OS (months) was found to be significantly lower in patients with low PNI (median: 34.93, 95% CI: 21.52–48.34) compared to patients with high PNI (median: 65.60, 95% CI: 39.36–91.83) (p=0.016). Patients with high PNI (median: 48.20, 95% CI: 34.66–61.73) had significantly better CSS (months) than patients with low PNI (median: 27.86, 95% CI: 24.16–31.57) (p=0.001).
Conclusions: PNI calculated at the time of diagnosis strongly predicts OS and CSS but not PFS in patients with mCSPC.
Keywords:
prostate cancer
; prognostic nutritional index
; inflammation
; prognosis
1. Introduction
Prostate cancer (PCa) is the most common cancer in the male. It also ranks second for cancer-related deaths in men [1]. Despite all therapy methods, local or locally advanced PCa may develop biochemical recurrence, local recurrence, or metastasis. The primary method in the therapy of metastatic castration sensitive PCa (mCSPC) is testosterone suppressive therapies (androgen deprivation therapy, ADT). ADT can be administered surgically (bilateral orchiectomy) or medically (luteinizing hormone-releasing hormone [LHRH] analogues) [2]. Addition of docetaxel or new generation hormonal agents (enzalutamide, abiraterone, apalutamide) to this therapy can provide a survival advantage [3]. Almost all patients with CSPC, despite these efforts, progress to the metastatic castration resistant PCa (mCRPC) stage [4]. Once the patients enter the CRPC stage, survival is around 24 months, but this period has begun to lengthen after new generation hormonal agents were included in treatment [5]. Upon passing the metastatic stage, sites of metastasis and Gleason score are important in determining the disease burden and risk [6]. In 2015, Sweeney et al. investigated the addition of chemotherapy (docetaxel) to ADT in patients with metastatic mCSPC. The patients were divided into two groups, high-volume, and low-volume, according to the region and number of metastases. In this study, patients with four or more bone metastases (with at least one outside the vertebral column and pelvis) or solid organ metastases were considered high-volume. In this study, the survival benefit of chemotherapy in the mCSPC stage was shown in patients with high-volume disease, but this benefit was not demonstrated in low-volume patients [7]. Similarly, in the LATITUDE study conducted by Fizazi et al. (2019), which investigated the benefit of adding abiraterone acetate to ADT in patients diagnosed with mCSPC and whose final analysis was published in 2019, patients were divided into two groups, as low and high risk according to Gleason score, the number of metastases and presence of visceral metastasis. In this study, the presence of three or more bone metastases or visceral metastases in patients with a Gleason score of ≥ 8 was considered high-risk disease. As expected, it was demonstrated that a significant survival benefit was provided in high-risk patients by adding abiraterone to ADT [8]. Today, criteria from these two studies are widely utilized both in predicting the prognosis of prostate carcinoma patients and deciding who should be treated intensively. However, there are studies demonstrating that there may be significant discordance between the criteria of these two studies [9]. The issue of which study criteria are better at predicting survival remains unclear. No biomarkers that can help determine survival in mCSPC are known, apart from markers such as the CHAARTED and LATITUDE criteria, Gleason score, PSA level, PSA response to therapy, and tumor volume in predicting survival and therapeutic benefit. Recent studies have shown that prognosis in various cancer types is also affected by patient-related inflammation, immunocompetence, and nutrition. The correlation between nutrition and cancer prognosis is particularly evident [10]. Lymphocyte, neutrophil, thrombocyte, and C-reactive protein levels as nutritional and inflammatory parameters and their use with certain formulas are quite common in cancer patients. Studies on the prognostic value of inflammatory parameters are still ongoing [11]. Albumin level reflects nutritional status, while lymphocyte counts reflect immune status. It is known that albumin levels and lymphocyte count, and their ratios to hematological parameters such as platelets and neutrophils, have prognostic importance in advanced cancer patients [12]. An important biomarker that uses a combination of these parameters and was proven to affect survival in various cancer types is the PNI [13]. PNI is a marker that can be easily calculated using serum albumin level and peripheral blood lymphocyte count. This biomarker is useful in showing nutritional and immunological status related to survival and prognosis in many cancers [14]. However, there are insufficient clinical studies regarding its association with survival in mCSPC. Most of the studies on this subject were performed on patients with mCRPC [15]. A different cut-off point for PNI was used in each study [16]. Considering this information, this study aimed to examine the relationship between the PNI, which may serve as a new marker, and the survival of prostate carcinoma, which currently does not have significant biomarkers.
2. Material and Methods
This retrospective, observational study included 201 patients who were treated for a diagnosis of prostate adenocarcinoma at Health Sciences University (HSU) Tepecik Training and Research Hospital between January 1, 2010, and June 1, 2021. Inclusion criteria for the study were as follows: (i) patients diagnosed with stage 4 CSPC, (ii) patients monitored in the clinic for at least three months, (iii) patients who had no therapy for mCSPC (ADT, docetaxel, or any new generation hormonal agents) and (iv) PNI score can be calculated from laboratory parameters. At the time of diagnosis, the presence of inflammatory or autoimmune disease (rheumatoid arthritis, autoimmune hepatitis, diseases that require chronic corticosteroid or immunosuppressive therapy such as rheumatoid arthritis, autoimmune hepatitis, inflammatory bowel disease), chronic hematological disease, second primary synchronous malignancy (except for carcinoma in situ and non-melanoma skin cancer), systemic therapy for any cancer diagnosis and no remission within the past five years, treatment for serious cardiovascular disease (stage 3 or 4 according to the New York Heart Society classification), and patients with missing data in the hospital database were disqualifying factors for the study. 93 patients who did not meet the specified criteria were excluded from the study, and 108 patients who met the study criteria were included. Since our study was a retrospective, observational study, the sample size was not calculated. The study protocol was approved by the decision of the HSU Tepecik Training and Research Hospital Non-Interventional Research Ethics Committee, dated 16.08.2021, and numbered 2021/08-07.
The dependent variable in the study was the prognostic nutritional index calculated with albumin and lymphocyte values at the time of diagnosis. The independent variables were PSA level, systemic therapies added to ADT, age, number of comorbidities, and tumor burden according to CHAARTED and LATITUDE trial criteria. Sociodemographic and clinicopathological data, as well as laboratory parameters of the patients, were obtained retrospectively from the hospital database. Current laboratory parameters at diagnosis (before prostate biopsy) of 108 patients who met the inclusion criteria were recorded. PNI was calculated as 10 * serum albumin (g/dl) + 0.005 * total lymphocyte count (per mm3) [13]. To evaluate the presence of clinical metastases, contrast-enhanced computed tomography of the abdomen and thorax, bone scintigraphy, and PSMA/PET results in the hospital database were scanned. The patients were grouped as low and high volume according to the CHAARTED trial criteria and as low and high risk according to the LATITUDE trial criteria.
CSS data were obtained by calculating the time from the date of initiation of systemic therapies for metastatic disease to the date of death or last patient visit, which one occurred first. OS data were obtained by calculating the time from the first diagnosis to death or the last follow-up visit. The time elapsed from the date of therapy initiation with the diagnosis of CSPC to the first PSA elevation or the first radiological progression (whichever occurred first) was considered progression-free survival (PFS).
Statistical Analysis
Receiver operating characteristic (ROC) curve analysis was applied to select the most appropriate cut-off point for PNI to determine patients at high risk of cancer-related death (Figure 1). Accordingly, the best cut-off point for PNI was determined as “49.75”. The patients were divided into two groups, those with and above the 49.75 and those below the 49.75 value, then compared in terms of OS, CSS, and PFS. In addition to descriptive statistics, chi-square and Fisher's exact tests were used for categorical variables to evaluate the data. Conformity of continuous data to normal distribution was quantified by Kolmogorov-Smirnov and Shapiro-Wilk tests. Mann-Whitney u test was used to determine the differences between the variables indicated by the measurement. The Kaplan-Meier method was used to estimate CSS, PFS, and OS, while the log-rank test was performed to investigate the difference in survival. To evaluate the effect of PNI on survival, univariate and multivariate Cox regression models were applied to identify the best predictive variables. The Median follow-up time in the study was calculated using reverse Kaplan-Meier. SPSS (version 25.0) package program was used to analyze all data. Statistical significance was determined as p<0.05 in all tests.
3. Results
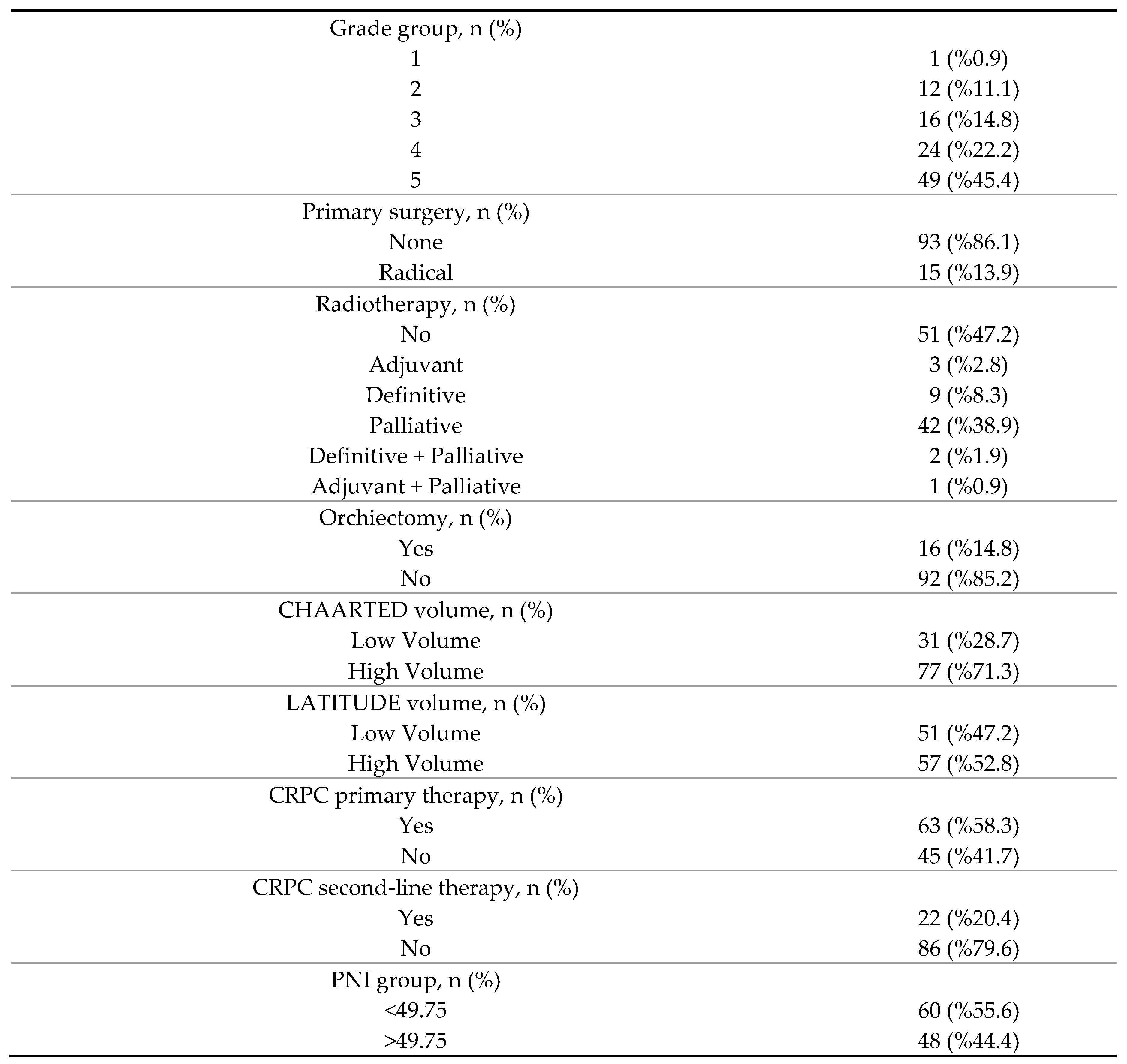
The median age of the 108 patients included in this study was 68.54 (61.05-74.19) years and the median PSA at the time of diagnosis was 110.60 (35.28-154.52) μg/L. The proportion of patients who received chemotherapy in the castration-sensitive stage was 44.4% (n=48). Of the patients, 86.1% (n=93) did not have a history of primary surgery. While 46.3% (n=50) of the study group did not possess any comorbidities, 33.3% (n=36) had one and 20.4% (n=22) had two or more comorbidities. Other descriptive and clinicopathological features of the patients are presented in Table 1.
The best PNI cut-off value for CSS was calculated with the ROC curve. The PNI=49.75 was taken as the cut-off value, and classification (low-high) was performed according to this value. When the serum PSA level at diagnosis, as well as risk levels (low risk-high risk) according to age and LATITUDE study, were analyzed in terms of low and high PNI values (<49.75 and >49.75), no significant difference was observed between the groups (p >0.05) (Table 2). Additionally, the PNI group was evaluated based on the volume levels (low volume vs high volume) from the CHAARTED study. According to the analysis results, patients with low volume have higher PNI values, while patients with high volume have lower PNI values. The difference between the groups was statistically significant (p=0.002). When metastasis regions (M1a, M1b, M1c) were examined in terms of PNI values, it was observed that PNI values decreased, moving from M1a to M1c disease (p=0.017). Disease volume and risk discordance were evaluated according to the CHAARTED and LATITUDE studies. Of patients, 27.3% in the high-volume group as defined by the CHAARTED criteria were in the low-risk group as defined by the LATITUDE criteria. On the other hand, 3.2% of our patients in the high-risk group, as defined by the LATITUDE criteria, were in the low-volume disease group as defined by the CHAARTED criteria (p<0.001).
OS (months) was found to be significantly lower in patients with low PNI (median: 34.93, 95% CI: 21.52–48.34) compared to patients with high PNI (median: 65.60, 95% CI: 39.36–91.83) (p=0.016) (Figure 1). Patients with high PNI (median:48.20, 95% CI:34.66–61.73) had significantly better CSS (months) than patients with low PNI (median:27.86, 95% CI:24.16–31.57) (p=0.001) (Figure 2). In addition, there was no statistically significant difference in PFS between patients with high PNI values (median: 24.60, 95% CI: 10.15–39.05) and patients with low PNI values (median: 20.03, 95% CI: 11.06 – 29.03) (p=0.092) (Figure 3). Although not statistically significant, patients with high PNI values had numerically higher PFS than those with low values.
In the high and low PNI groups, the overall survival was analyzed according to metastasis sites (M1a, M1b, M1c). Longer OS was observed in patients with high PNI (Figure 4) than in patients with low PNI (Figure 5) in each group (p<0.001). OS was compared in terms of LATITUDE risk groups and CHAARTED volume groups, and PNI groups. According to CHAARTED criteria, the OS of low-volume patients in both high and low PNI groups was significantly higher than those of high-volume patients (p<0.001) (Figure 6 and Figure 7). A similar result was found when the assessment was performed according to the LATITUDE risk classification (p<0.001) (Figure 8 and Figure 9).
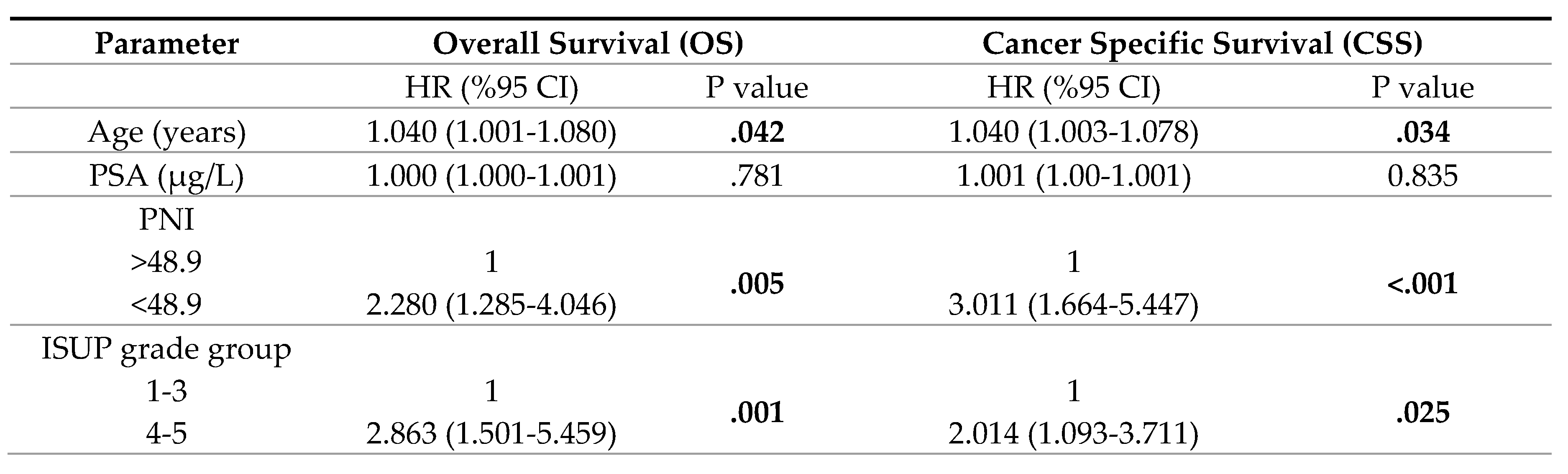
In univariate analyses, decreased PNI, high volume disease according to CHAARTED, and higher risk disease according to LATITUDE were associated with worse OS (p =0.018, p<0.001, p<0.001, respectively) and worse CSS (p =0.001, p<0.001, p<0.001, respectively) (Table 3). ISUP grade group 4-5 was associated with a worse prognosis only for OS (p=0.006). In Multivariate analyses, the HRs of PNI was found to be 2.280 (95% CI: 1.285-4.046) for OS and 3.011 (95%CI: 1.664-5.447) for CSS, respectively (Table 4). Age was determined to be an independent prognostic factor for OS and CSS (HR: 1.040, 95% CI: 1.001-1.080, p=0.042; HR: 1.040, 95% CI: 1.003-1.078, p=0.034, respectively).
4. Discussion
Owing to the new treatment modalities developed and widely used in recent years, the median OS in prostate cancer has exceeded 5 years [17]. Many studies showed that chemo-hormonal therapy with docetaxel and ADT, widely applied, especially in the mCSPC stage, provides an OS advantage of approximately 17 months [7]. Similar results were obtained with abiraterone, enzalutamide, and apalutamide in the mCSPC patients [18]. Many biomarkers were studied to determine which patients would benefit more from these therapies or live longer. However, no biomarker could replace parameters such as CHAARTED and LATITUDE criteria, Gleason score, PSA level, PSA response to therapies, and TNM stage, which are currently used for prognosis determination. Therefore, the search for new biomarkers continues unabated. In this study, we also found that PNI, identified in searches for biomarkers and has a close relationship with prognosis in many cancer types, affects survival in patients diagnosed with mCSPC, independently of all other prognostic factors. The cut-off points for PNI, with different cut-off points used in many studies, were accepted as 49.75 in our study. CSS and OS of patients above this value were significantly better than those below this value. The PNI cut-off value was taken as 50.2 in a study by Li et al in 2020 that included 208 patients. In this study, Li et al. (2020) found that patients with a PNI of 50.2 and above had better CSS, OS, and PFS duration than patients below this value [19]. Like this study, there was a significant difference in OS and CSS between patients with high and low PNI values in our study. Moreover, this difference was valid for all M1a, M1b, and M1c patients. However, although the PNI value had a numerically positive effect on PFS in our study, no statistically significant effect was found.
It is now known that the number of lymphocytes that can simply be measured in blood and the number of lymphocytes around the tumor (tumor-infiltrating lymphocytes) have prognostic importance [20]. Similarly, blood albumin levels also have prognostic importance [21]. The low number of lymphocytes in the blood may help us predict that the anti- tumoral immune response against the tumor will be weak. Likewise, it is known that inflammation caused by the tumor and some cytokines released secondary to this inflammation reduce blood albumin levels and may play a role in tumor progression [22]. Considering all these, PNI may be a biomarker combining the prognostic power of low albumin and low lymphocyte values. The fact that the PNI level affects survival independently of all factors in our study supports this theory.
The criteria for the LATITUDE and CHAARTED study, the prognostic and predictive importance of which is now clearly known, are remarkably similar. However, it is known that there may be significant discordance between the criteria in these two studies [23]. In our study, 21 (27.3%) of the high-volume patients according to the CHAARTED criteria were low-risk according to the LATITUDE criteria, while only 1 (3.2%) of the low-volume patients according to the CHAARTED criteria were high-risk according to the LATITUDE criteria. When the high-low volume and risk status, and PNI value were compared based on these two studies, no significant relationship was found between the LATITUDE criteria and PNI. Considering the CHAARTED criteria, the probability of having a PNI value above 49.75 in low-volume patients was significantly higher than in high-volume patients. When the univariate analysis results were examined, it was concluded that, contrary to this finding, the criteria from both studies affected survival. It is obvious that these two prognostic criteria should be further investigated with larger studies.
Another important finding in our study is that only 58.3% of the patients who progressed to the mCRPC stage were able to receive first-line therapy and 20.4% received second-line systemic therapy for mCRPC. In other words, once patients pass to the mCRPC stage, both the chance of obtaining systemic therapies and having a long survival decrease [24]. At this point, PNI can act as an important biomarker. There are also some limitations of this study. First, due to the retrospective design of the study, its reliability is lower than a prospective study. Since most patients were diagnosed before the CHAARTED and LATITUDE studies, systemic therapies not added to ADT for most patients in the castration-sensitive stage may have affected the results. PNI is a marker that can be affected by many parameters such as nutritional status, infections, and inflammation. It is not yet known whether giving nutritional support to patients with low PNI influence the PNI value or will have an effect on survival. Our study cannot answer this question due to its retrospective design. The small number of patients is also among the limitations.
5. Conclusions
The PNI calculated at the time of diagnosis affects OS and CSS in mCSPC. It is projected that PNI, an easily calculable and extremely cost-effective biomarker, may have a place as a practical method for the determination of prognosis in prostate carcinoma. Studies on this subject with larger case series may provide more precise results.
Author Contributions
HIE, MK, EK, IO: Methodology, Writing-Original draft preparation, Writing-Reviewing and Editing, Critical Review, HSS: Conceptualization, Methodology, Writing-Original draft preparation, Writing-Reviewing and Editing, Critical Review. MEA: Statistical analysis, Software, Visualization, Investigation, Validation, Writing-Original draft preparation, Critical Review. The final manuscript was reviewed and approved by all authors.
Funding
None.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no potential conflicts of interest.
References
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021;71:209-249.
- Shore ND, Antonarakis ES, Cookson MS, et al. Optimizing the role of androgen deprivation therapy in advanced prostate cancer: Challenges beyond the guidelines. Prostate 2020;80:527-544.
- Ferro M, Lucarelli G, Crocetto F, et al. First-line systemic therapy for metastatic castration-sensitive prostate cancer: An updated systematic review with novel findings. Crit Rev Oncol Hematol 2021;157:103198.
- Cornford P, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol 2021;79:263-282.
- Aly M, Leval A, Schain F, et al. Survival in patients diagnosed with castration-resistant prostate cancer: a population-based observational study in Sweden. Scand J Urol 2020;54:115-121.
- Francini E, Gray KP, Xie W, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate 2018;78:889-895.
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med 2015;373:737-746.
- Fizazi K, Tran N, Fein L, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol 2019;20:686-700.
- Semiz HS, Keskinkılıç M, Ellez HI, Arayıcı ME, Karaoglu A. Approach to the Therapy of Metastatic Castration-Sensitive Prostate Carcinoma: A Single Center Experience. JBACHS 2022;6:296-304.
- Tan CS, Read JA, Phan VH, Beale PJ, Peat JK, Clarke SJ. The relationship between nutritional status, inflammatory markers and survival in patients with advanced cancer: a prospective cohort study. Support Care Cancer 2015;23:385-91.
- Yapar Taskoylu B, Avci E, Gokcen Demiray A, et al. Relationship between neutrophil/lymphocyte, platelet/lymphocyte, CRP/Albumin ratio and survival in ovarian cancer. Pam Med J 2021;14:666-674.
- Shu W, Tao W, Chunyan H, et al. Preoperative nutritional evaluation of prostate cancer patients undergoing laparoscopic radical prostatectomy. PLoS One 2022;17:e0262630.
- Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon GekaGakkaishi Zasshi 1984;85:1001–5.
- Yan L, Nakamura T, Casadei-Gardini A, Bruixola G, Huang YL, Hu ZD. Long-term and short-term prognostic value of the prognostic nutritional index in cancer: a narrative review. Ann Transl Med 2021;9:1630.
- Fan L, Wang X, Chi C, et al. Prognostic nutritional index predicts initial response to treatment and prognosis in metastatic castration-resistant prostate cancer patients treated with abiraterone. Prostate 2017;77:1233-1241.
- Küçükarda A, Gökyer A, Gökmen İ, et al. Prognostic nutritional index is an independent prognostic factor for therapy response, survival and drug choice in metastatic castration-resistant prostate cancer treated with abiraterone acetate or enzalutamide [published online ahead of print, 2022 March 4]. Actas Urol Esp (Engl Ed) 2022;S:2173-5786(21)00158-X.
- Fizazi K, Foulon S, Carles J, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet 2022;399:1695-1707.
- Velho PI, Bastos DA, Antonarakis ES. New approaches to targeting the androgen receptor pathway in prostate cancer. Clin Adv Hematol Oncol 2021;19:228-240.
- Li B, Lu Z, Wang S, et al. Pretreatment elevated prognostic nutritional index predicts a favorable prognosis in patients with prostate cancer. BMC Cancer 2020;20:361.
- Kobayashi H, Shiota M, Sato N, et al. Differential prognostic impact of complete blood count-related parameters by prior use of novel androgen receptor pathway inhibitors in docetaxel-treated castration-resistant prostate cancer patients. Anticancer Drugs 2022;33:e541-e547.
- Yalav O, Topal U, Unal AG, Eray IC. Prognostic significance of preoperative hemoglobin and albumin levels and lymphocyte and platelet counts (HALP) in patients undergoing curative resection for colorectal cancer. Ann Ital Chir 2021;92:283-292.
- Zhao H, Wu L, Yan G, et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Target 2021;6:263.
- Kawahara T, Yoneyama S, Ohno Y, et al. Prognostic Value of the LATITUDE and CHAARTED Risk Criteria for Predicting the Survival of Men with Bone Metastatic Hormone-Naïve Prostate Cancer Treated with Combined Androgen Blockade Therapy: Real-World Data from a Japanese Multi-Institutional Study. Biomed Res Int 2020;2020:7804932.
- de Bono JS, Smith MR, Saad F, et al. Subsequent Chemotherapy and Treatment Patterns After Abiraterone Acetate in Patients with Metastatic Castration-resistant Prostate Cancer: Post Hoc Analysis of COU-AA-302. Eur Urol 2017;71:656-664.
Figure 1.
Overall survival in patients with low PNI compared to patients with high PNI.
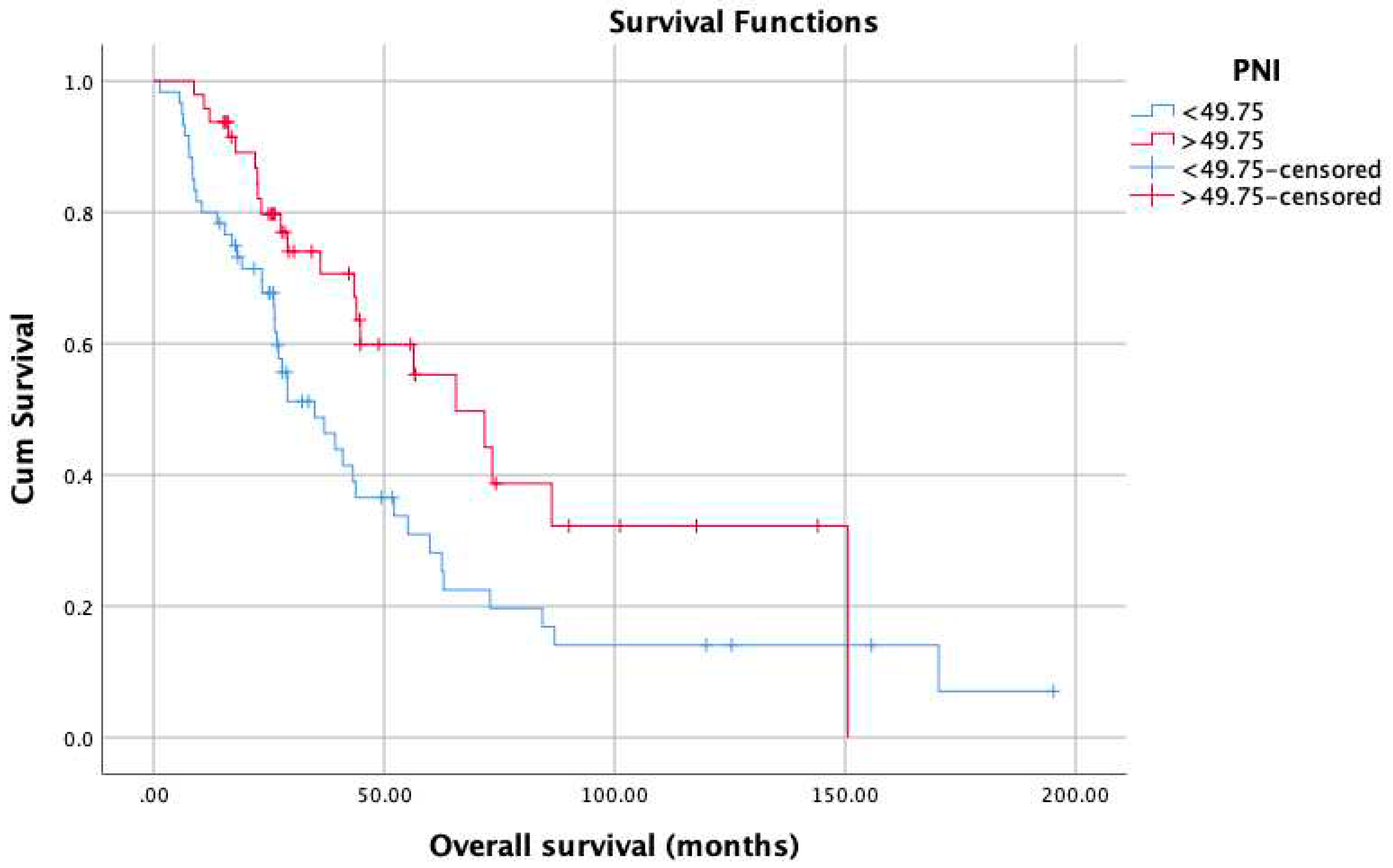
Figure 2.
Cancer spesific survival in patients with low PNI compared to patients with high PNI.
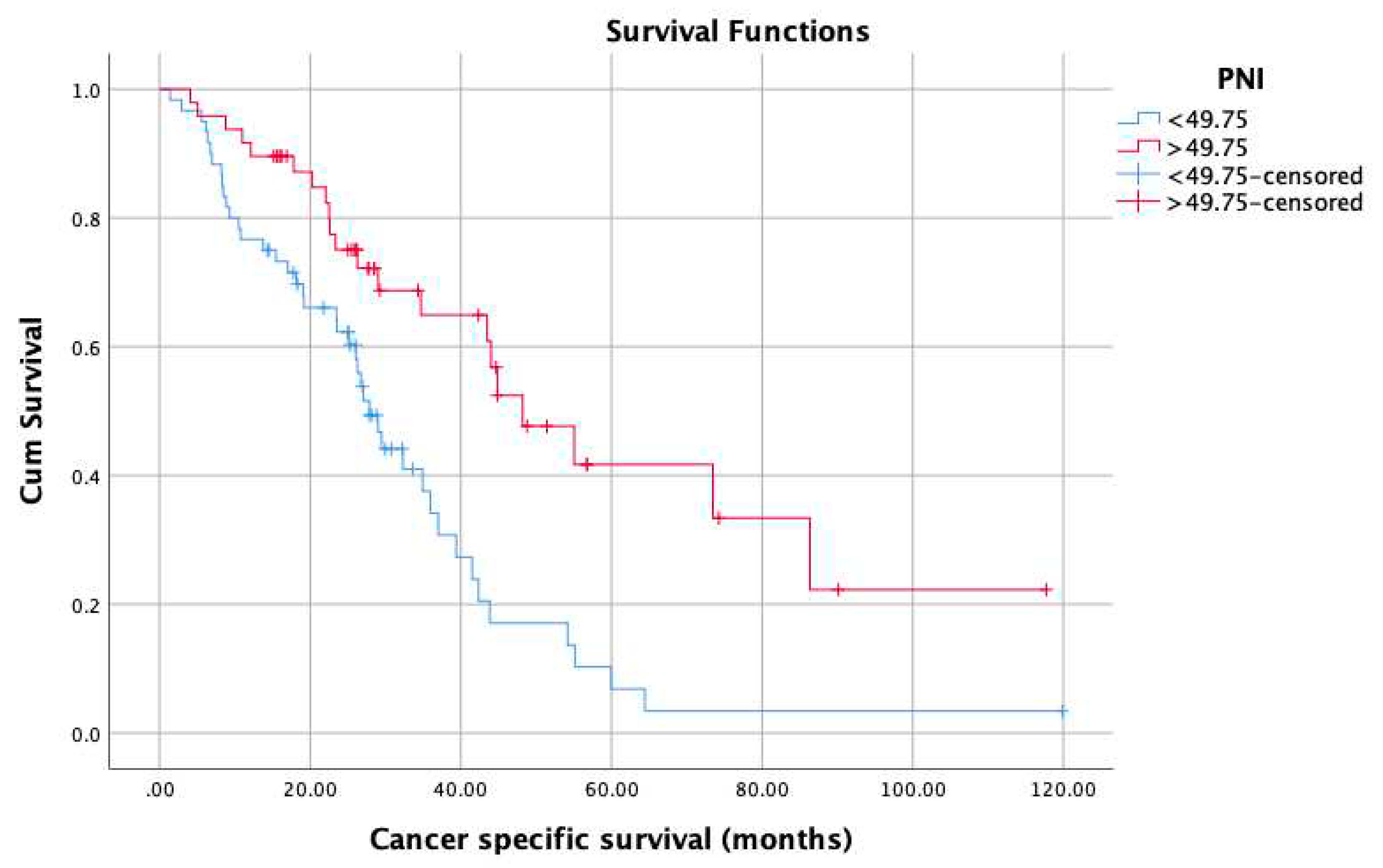
Figure 3.
Progression free survival survival in patients with low PNI compared to patients with high PNI.
Figure 3.
Progression free survival survival in patients with low PNI compared to patients with high PNI.
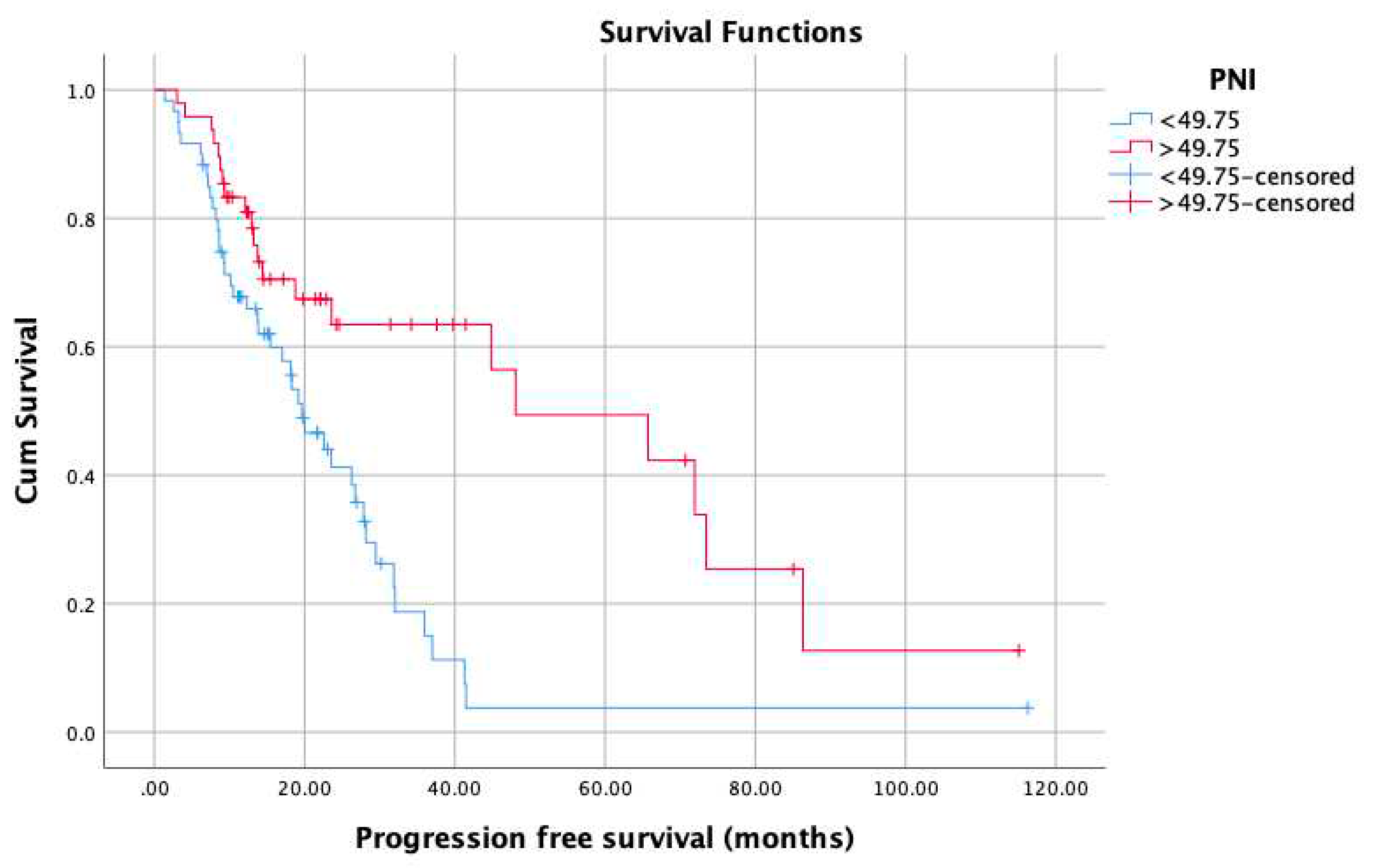
Figure 4.
Overall survival in the low PNI groups according to metastasis sites (M1a, M1b, M1c).
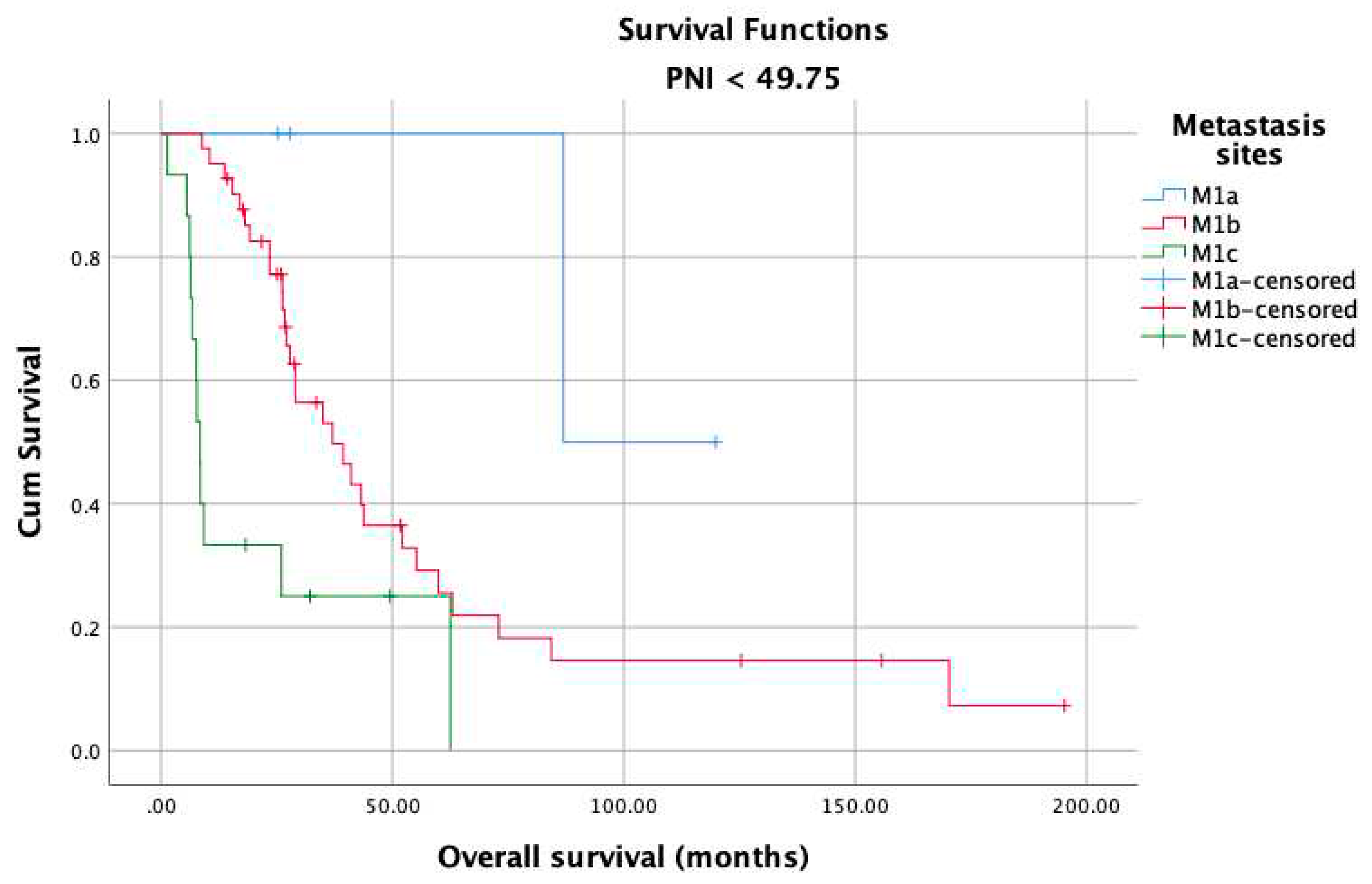
Figure 5.
Overall survival in the high PNI groups according to metastasis sites (M1a, M1b, M1c).
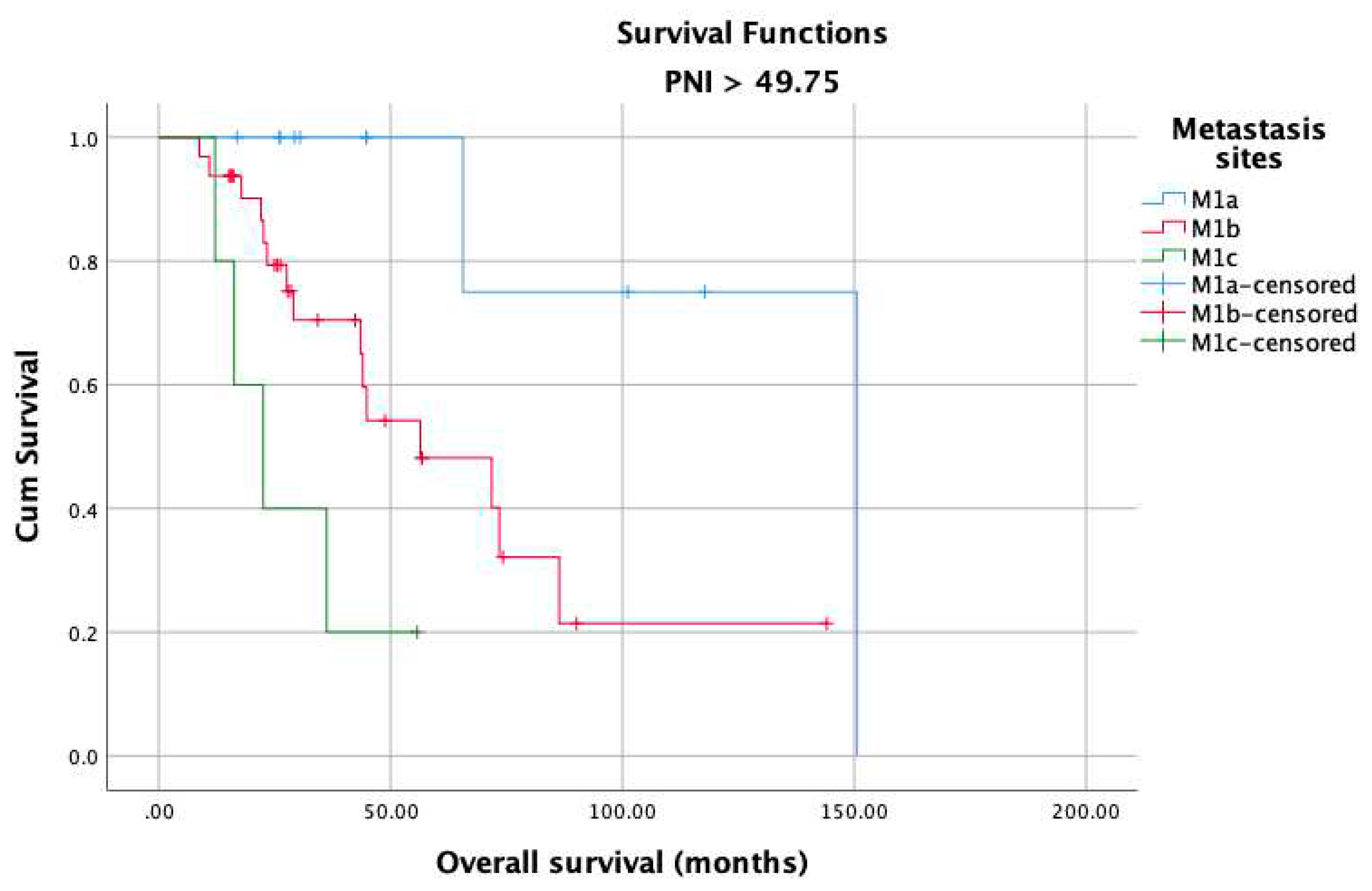
Figure 6.
Overall survival in the low PNI groups according to CHAARTED volume levels.
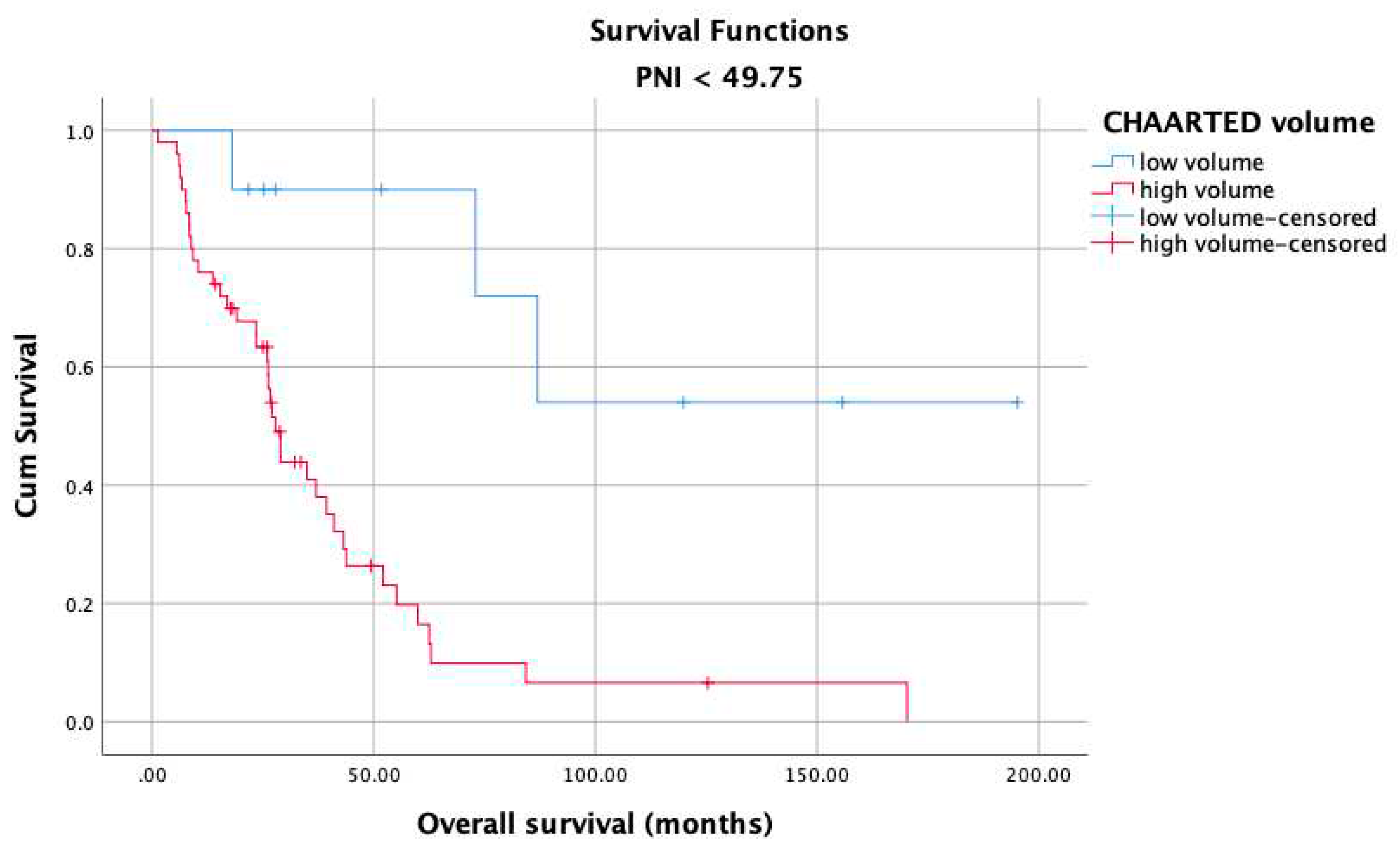
Figure 7.
Overall survival in the high PNI groups according to CHAARTED volume levels;.
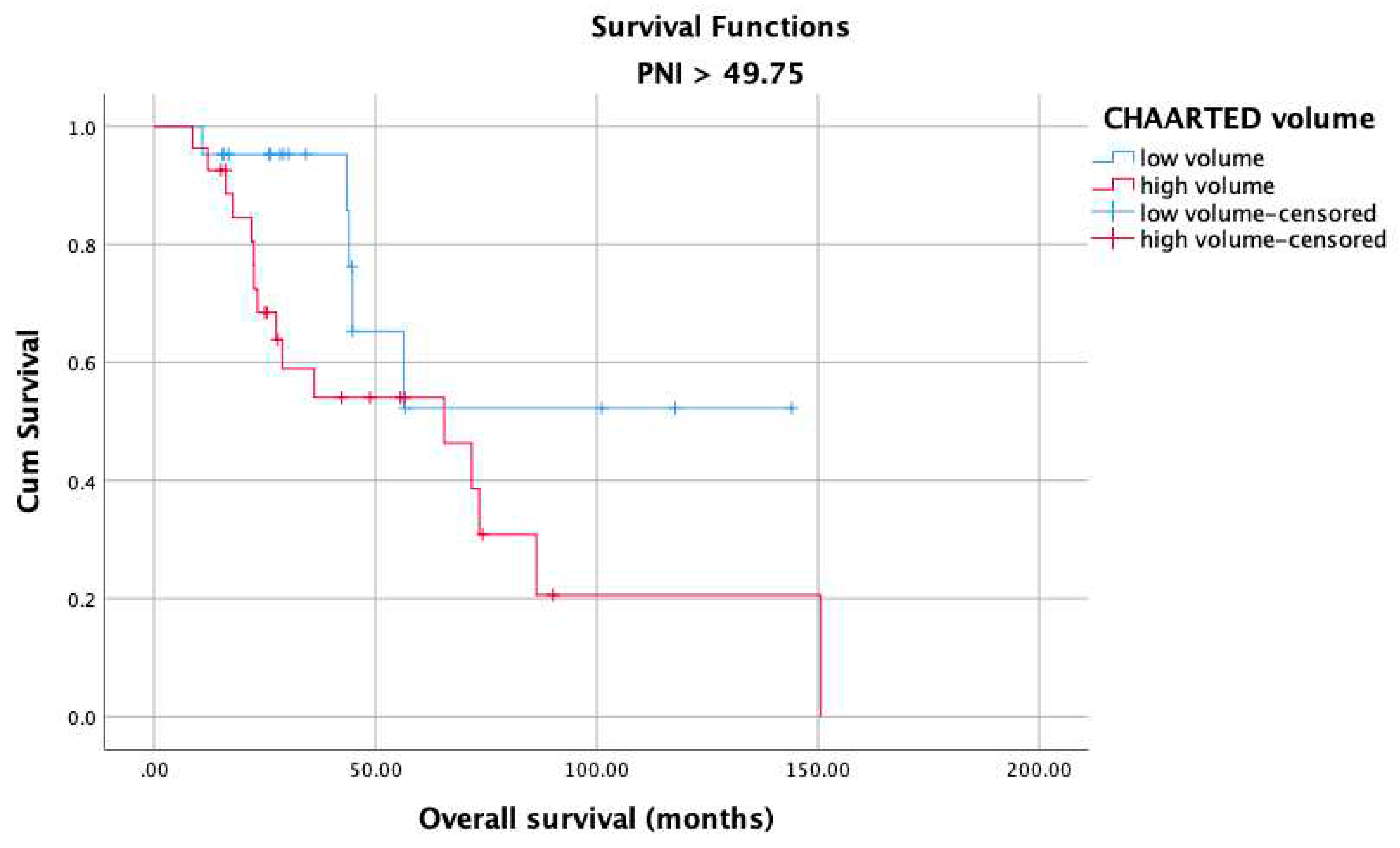
Figure 8.
Overall survival in the low PNI groups according to LATITUDE risk levels.
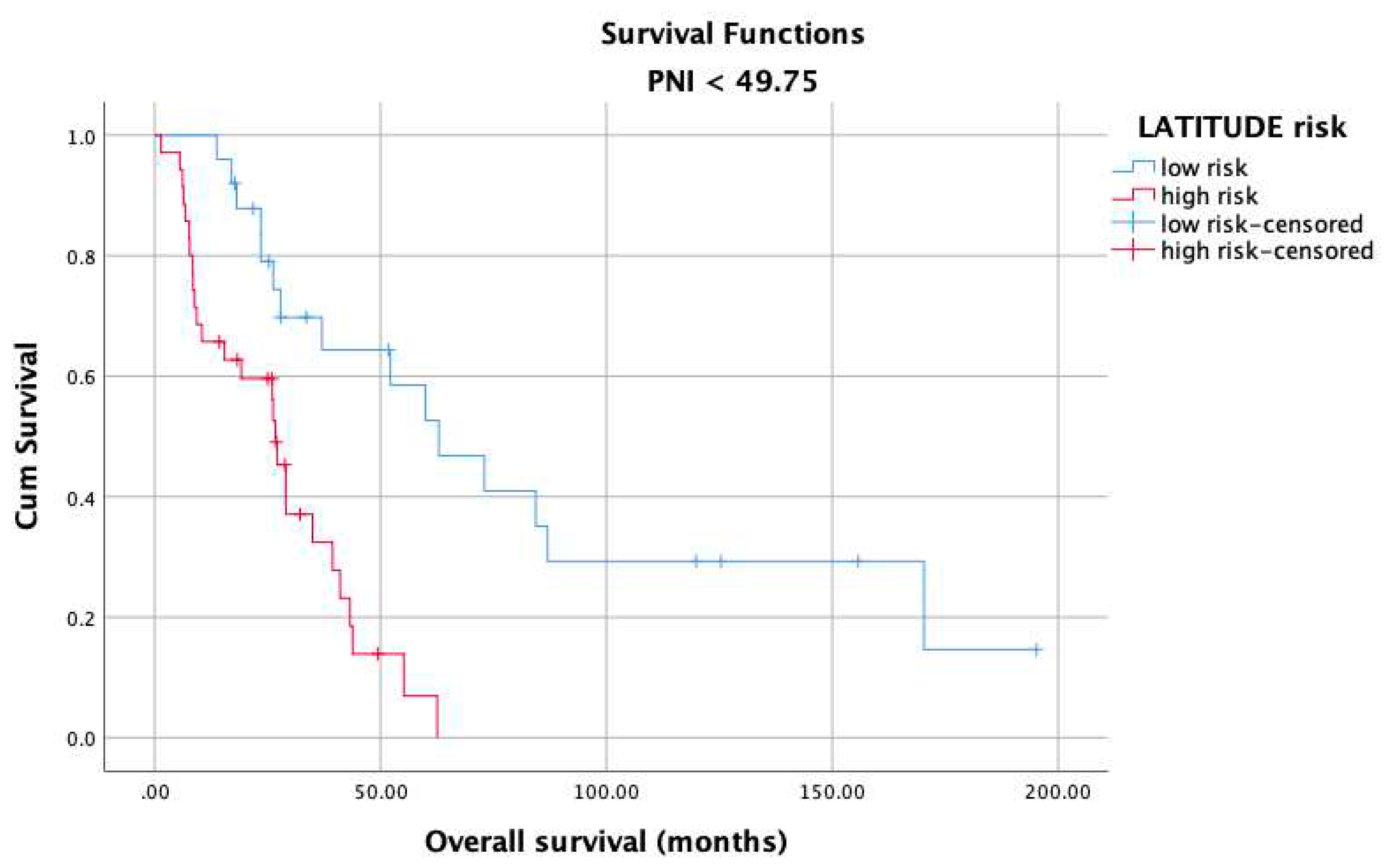
Figure 9.
Overall survival in the high PNI groups according to LATITUDE risk levels.
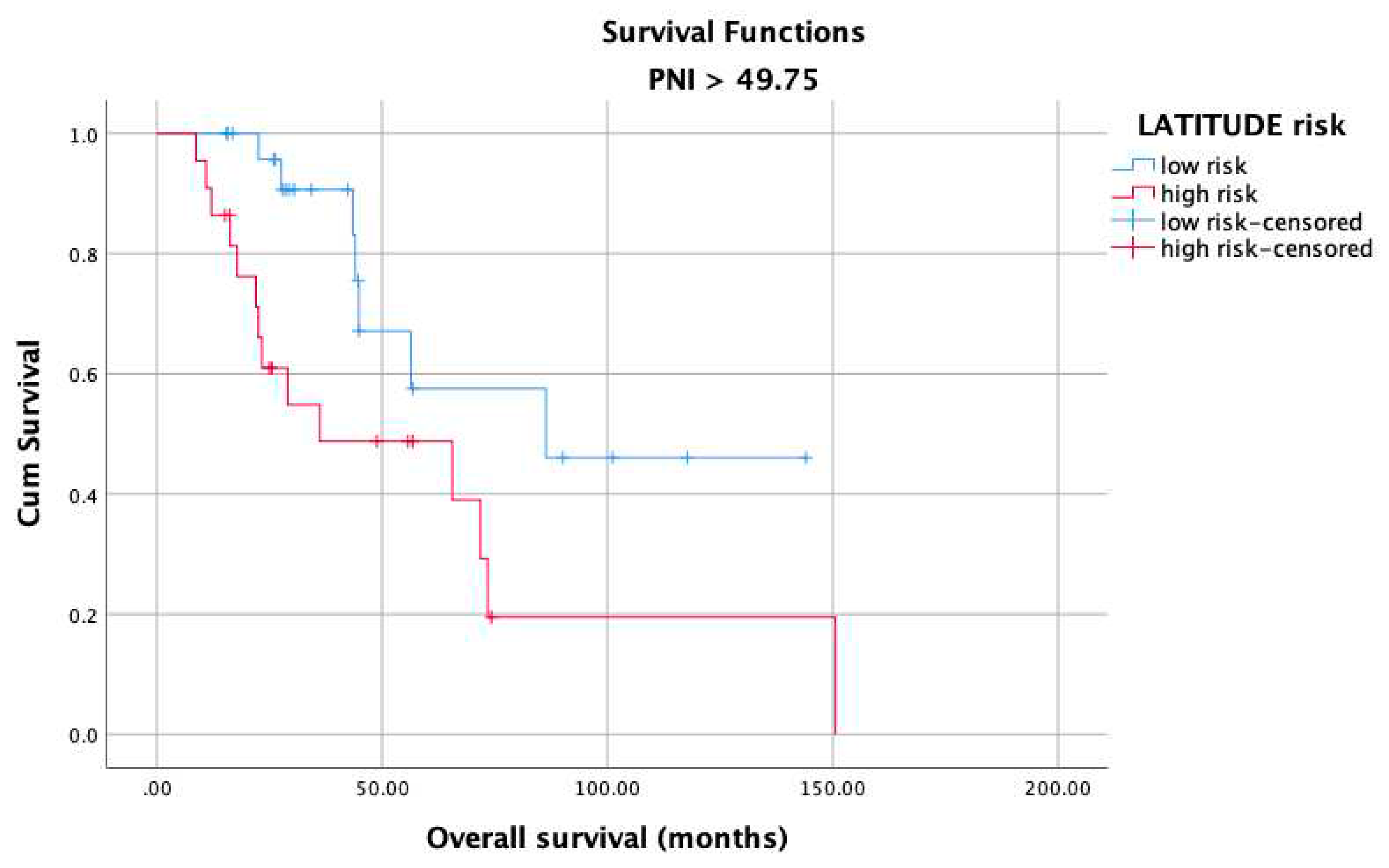

Table 1.
Descriptive and clinicopathological features of the study group.
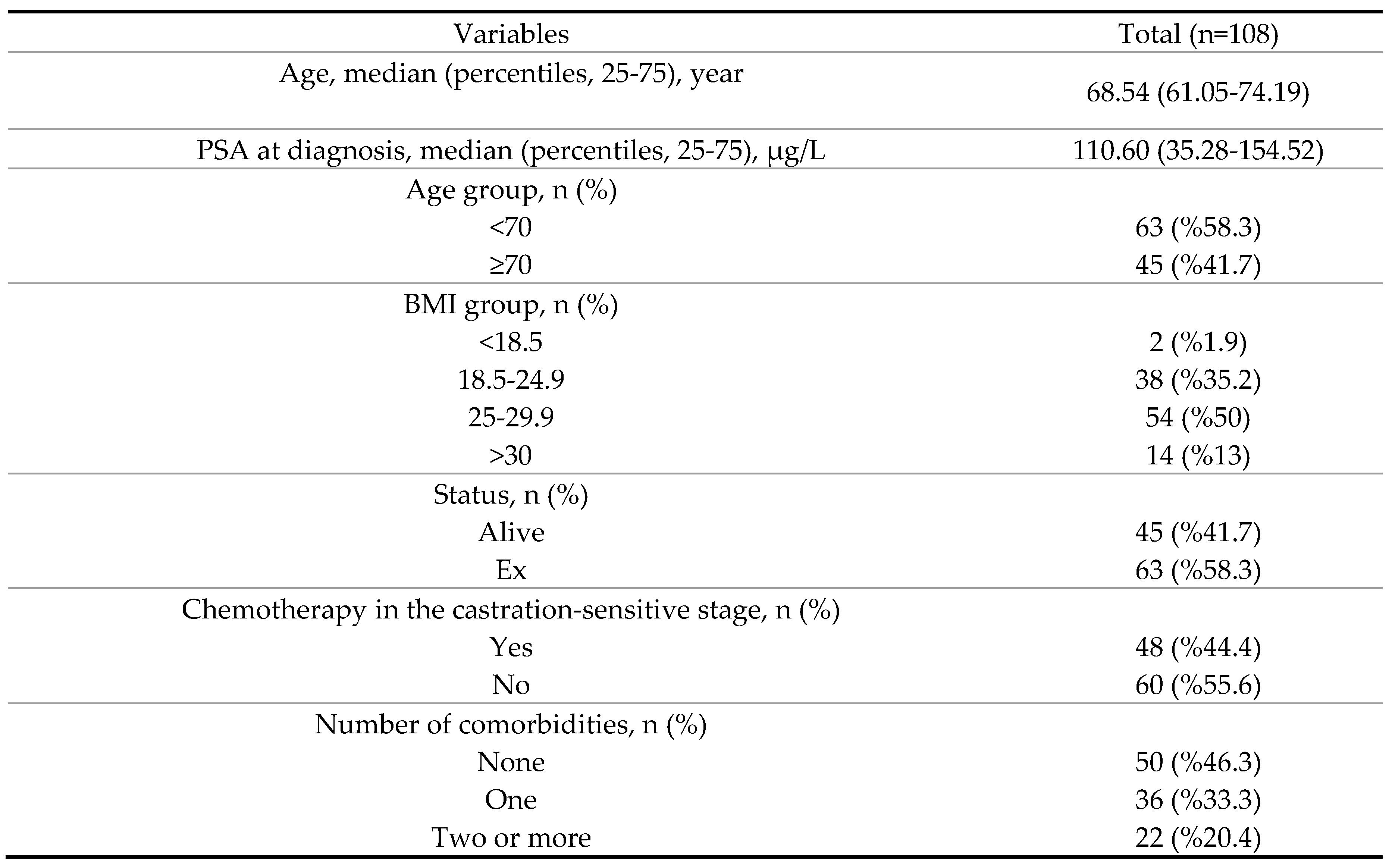
CRPC: castration-resistant prostate carcinoma, BMI: body mass index.
Table 2.
Clinical characteristics of prostate cancer patients according to PNI.
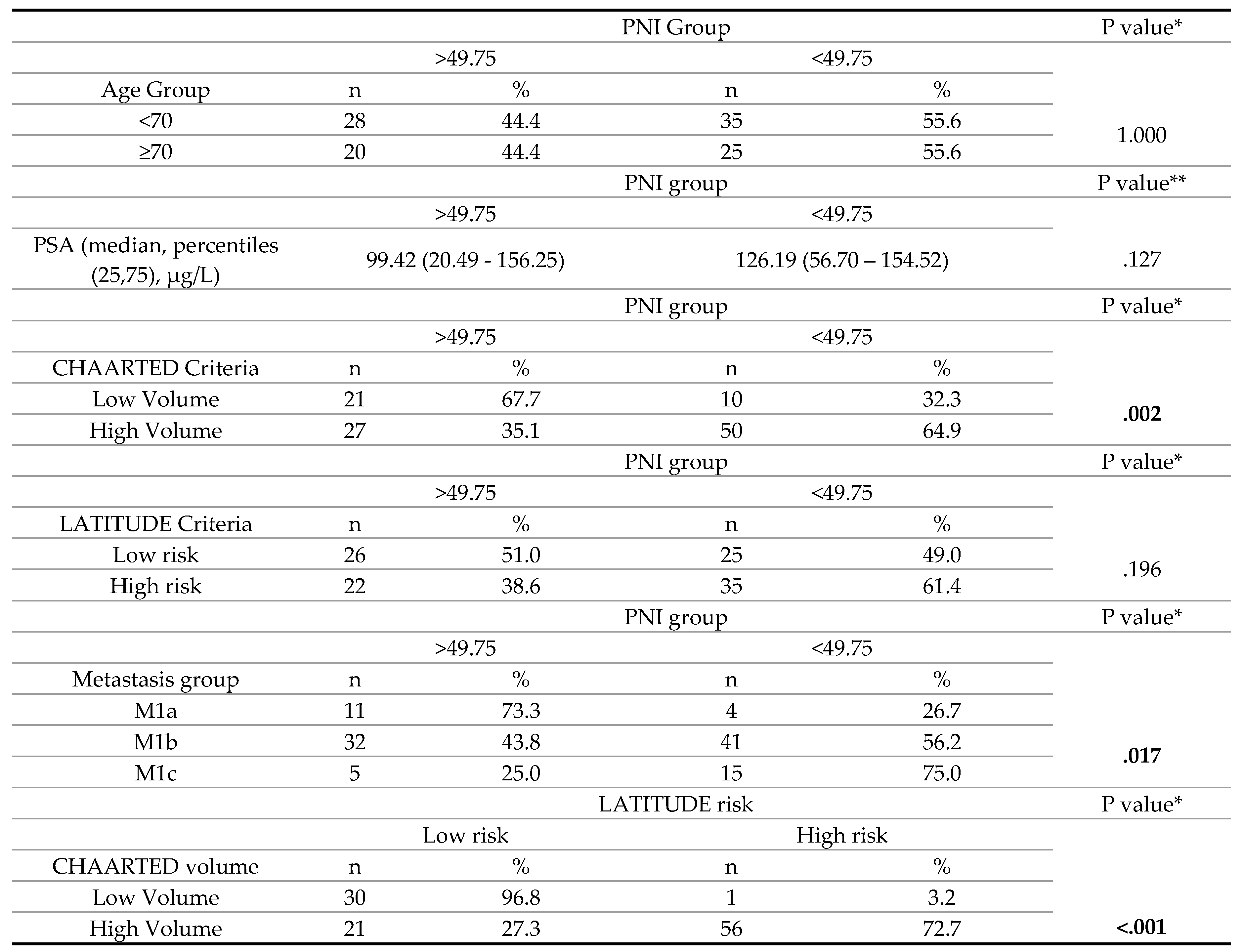
*Chi-square test. **Mann Whitney U test.
Table 3.
Univariate analysis of various clinical parameters in prostate cancer patients.
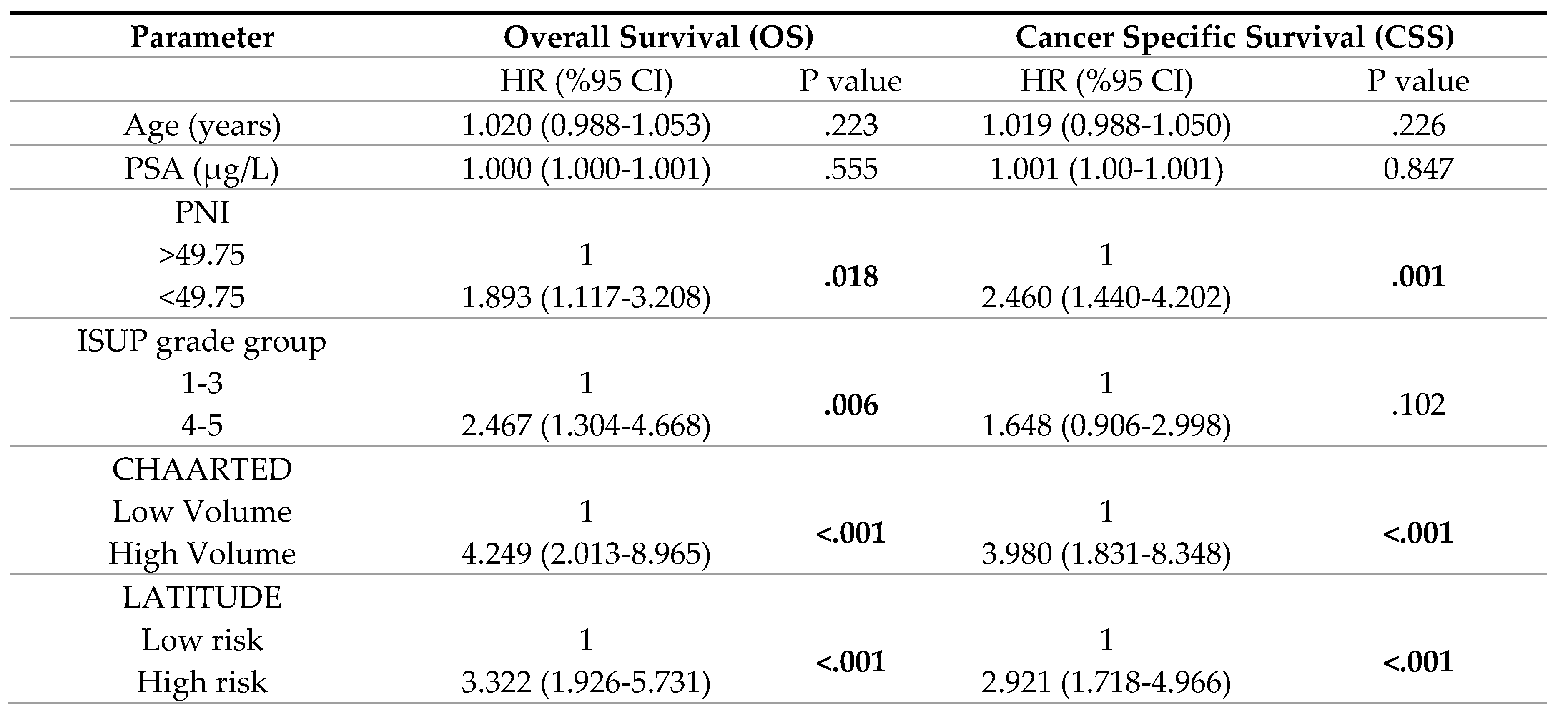
Table 4.
Multivariate analysis of various clinical parameters in prostate cancer patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



