
Submitted:
19 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
Radical prostatectomy (RP) is one of the recommended treatments to achieve oncological outcomes in localized prostate cancer. However, radical prostatectomy is a major abdominopelvic surgery. Venous thromboembolism (VTE) is a well-known complication associated with surgical procedures including RP. There is a lack of consensus regarding VTE prophylaxis in urological procedures. The aim of this systematic review was to investigate different aspects of VTE in post-Radical Prostatectomy patients. A comprehensive literature search was performed, and relevant data were extracted. The primary aim was to perform a systematic review and meta-analysis (wherever possible) of VTE occurrence in post-RP patients in relation to surgical approach, pelvic lymph node dissection, and type of prophylaxis (mechanical or combined prophylaxis). The secondary aim was to investigate- the incidence and other risk factors of VTE in post-RP patients. A total of 16 studies were included for quantitative analysis. Statistical methods for analysis included the DerSimonian-Laird random effects. We were able to conclude that the overall incidence of VTE in post-radical prostatectomy is 1% and minimally invasive procedures (MIS), including laparoscopic as well as robotic procedures for radical prostatectomy and RP without pelvic lymph node dissection (PLND) are associated with less risk of developing VTE. Additional pharmacological prophylaxis to mechanical methods may not be necessary in all cases and should be considered in high-risk patients only.
Keywords:
Prostate cancer
; Radical prostatectomy
; Venous thromboembolism
; Mechanical prophylaxis
; Pharmacological prophylaxis
1. Introduction:
Urological cancer surgical procedures have evolved remarkably over the years, the open surgical methods have now largely been replaced by endoscopic or minimally invasive procedures including laparoscopy and robot-assisted methods. Perioperative venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), represents a serious and potentially fatal complication after urological cancer surgeries [1,2]. DVT incidence, without prophylaxis, has been estimated to be 10-40% among medical and general surgical patients [3]. PE results in approximately 10% of hospital deaths- the most common cause of inpatient deaths [4]. Furthermore, VTE accounts for the most common preventable cause of hospital-related deaths [5,6,7]. National Surgical Quality Improvement Program (NSQIP) data revealed a 2.5-fold increased risk of VTE within 30 days in abdominal procedures compared to procedures such as breast surgery [8]. One of the common abdominal urological cancer surgeries is radical prostatectomy (RP), performed for prostate cancer (PCa), which also evolved from open to robotic-assisted surgery. Ultrasound evaluation of VTE occurrence in post-RP patients is estimated at 20% [9].
Thromboprophylaxis helps in reducing morbidity and mortality in surgical patients, using either mechanical methods to promote venous outflow from the legs or pharmacological prophylaxis (PP) in the form of antithrombotic drugs [10]. The efficacy of thromboprophylaxis in decreasing the incidence of venous thromboembolic events has been demonstrated in randomized controlled clinical trials [11]. Similarly, meta-analyses by various specialties looking into VTE prophylaxis in abdomen/pelvic surgeries concluded that anticoagulants such as low molecular weight heparins (LMWH) decrease the relative risk of VTE by approximately 50%. However, LMWH administration also increases the relative risk of major bleeding by approximately 50% [12,13]. Regarding prophylaxis after RP, there is a lack of high-quality evidence or standard practice across the globe. In the UK, 98% of patients receive PP after RP, while only 17.8% receive PP after RP in the USA [11,14]. One US study found that 30% of patients post-RP received no VTE prophylaxis [14].
The aim of this systematic review was to investigate different aspects of VTE in post-RP patients. The primary aim was to perform a systematic review and meta-analysis (wherever possible) of overall VTE occurrence in post-RP patients as well as VTE occurrence in relation to surgical approach, pelvic lymph node dissection, and type of prophylaxis (mechanical or combined prophylaxis). The secondary aim was to investigate the impact of other risk factors of VTE in post-RP patients.
2. Material and Methods
2.1. Protocol and registration:
This systematic review is registered with the PROSPERO International Registry (CRD42022364222).
2.2. Evidence Acquisition:
The inclusion criteria for studies included the following-
- Population: Male patients, prostatectomy for prostate cancer,
- Intervention: Pharmacological/ Combined Prophylaxis (PP) for VTE
- Comparator/Control: No Prophylaxis or Mechanical Prophylaxis for VTE
The exclusion criteria for studies included the following-
- Population: Prostatectomy for non-prostate cancer or part of other surgery like cystoprostatectomy.
- Intervention: If the interventions are ill-defined or structural methods are inadequate.
- Comparator/ Control: Studies that lacked proper grouping into control, and intervention.
- Study Design: Studies that did not fulfill the above criterion and lacked any defined outcomes.
2.3. Outcome measures:
-
Primary Outcomes- VTE occurrence with
- Overall Incidence of VTE in post-RP patients
- Surgical approach. (Open, Minimally Invasive)
- Pelvic Lymph node dissection (PLND)
- Prophylaxis (No prophylaxis, Mechanical only, Pharmacological only, Combined).
- Secondary Outcomes-
Risk factors for VTE in Post-RP patients including age, body mass index (BMI), smoking, personal or family history of VTE
2.4. Search Methods:
We followed the “Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)-2020 protocol, for this systematic review [15]. The PRISMA Checklist for this review is shown in Supplementary Table 1. An electronic search was carried out into MEDLINE, EMBASE, and Cochrane Library with results from Cochrane CENTRAL, ClinicalTrials.gov, and the International Clinical Trials Registry Platform (ICTRP). There was no date or language limit. Search terms included ‘Prostatectomy’, ‘Radical’, ‘Cancer’, ‘Venous thromboembolism’, ‘Deep Vein Thrombosis’, ‘Pulmonary Embolism’, ‘Prophylaxis’, ‘Pharmacological’, ‘Mechanical’, and ‘surgical procedures.’ Boolean operators (‘And’/ ‘Or’) were used. The search strategy is attached as Supplementary Table 2.
2.5. Study Selection:
Rayyan software (a free web tool designed to help researchers speed up the process of screening and selecting studies) was used to aid in the process of duplicate removal, and initial screening, and facilitate author collaboration. After deleting duplicates, following the inclusion and exclusion criterion, studies were shortlisted. Full-text papers of the shortlisted studies were reviewed by the SQ3R (Survey, Question, read, recite, review) technique. The process of reviewing studies was completed independently by three authors (M.W, A.M, S.Mu, J.A). In case of any disagreements, the discussion was carried out with the rest of the authors (S.Ma, G.N, B.S) to reach a consensus.
2.6. Data Extraction:
The data was initially divided into two parts. The first part included a detailed description of all the studies included. The second part included grouping data into columns- the number of patients, type of surgical approach procedure, pelvic lymph node dissection, post-op VTE Prophylaxis (Duration/ Type of medication), and additional VTE (Mechanical). Data extraction was performed by two authors independently (M.W, A.M).
2.7. Quality assessment:
For quality assessment of the studies included, the Newcastle-Ottawa Scale (NOS) was used [16].
2.8. Statistical analysis:
It was carried out in three parts-
- a.
- Statistical evaluation of overall VTE occurrence
The meta-analysis pooled together the results from the different studies, calculating the overall percentage of patients in which the outcomes occurred. Due to the rare occurrence of the outcomes, the Freeman-Tukey double arcsine transformation was performed before analysis. This was used to stabilize the variances when the proportions were close to zero, and a normal approximation to the binomial distribution did not hold.
The DerSimonian-Laird random-effects method was used for the analysis, regardless of the degree of heterogeneity between the study results. Heterogeneity between studies was assessed based on the significance of the between-study heterogeneity and on the size of the I2 value. Substantial heterogeneity was assumed if the I2 value was above 50%.
- b.
- Statistical evaluation of VTE occurrence depending on the type of surgical procedure (Open/ Minimally Invasive Surgery (MIS)) and whether PLND was performed or not
Meta-analysis methods were used to pool together the within-study differences in the outcome of different procedures. The outcome of interest was the occurrence of VTE, which was binary in nature. Differences between procedures were expressed as a relative risk.
The DerSimonian-Laird random-effects method was used for the analysis, regardless of the degree of heterogeneity between the study results. Heterogeneity between studies was assessed based on the significance of the between-study heterogeneity and on the size of the I2 value. Substantial heterogeneity was assumed if the I2 value was above 50%.
Data was collected from a series of studies. However, not all studies collected data from more than one type of procedure, and thus a comparison between procedures was based on data from a more limited number of studies. The data collected enabled two different comparisons to be made:
- MIS procedures vs. Open procedures
- Procedures using PLND vs. procedures without PLND
- c.
- Statistical Evaluation of VTE occurrence depending on the method of prophylaxis used (mechanical or combined).
The systematic review found only two studies that collected data on both methods, and that could be used in a within-study comparison. However, additional studies collected data on either one method or the other. To be able to include all studies in the analysis, a within-study comparison was not made. Instead, the occurrence of VTE was pooled separately for the mechanical and combined methods. The difference in VTE occurrence between methods was assessed based on the significance of the between-group heterogeneity. Similar statistical methods were used as described already for overall VTE occurrence.
3. Results
3.1. Study selection results:
In the initial search, 394 studies were identified. A total of 18 were removed (Including 15 duplicates). 376 studies were screened. After the title and abstract review, 302 studies were excluded. Full-text retrieval was sought for 74 studies, however, we could retrieve only 72. Out of 72 studies, 41 studies were excluded after a full-text review. 31 remaining studies were scrutinized for eligibility criteria, and in the end, 16 studies were included in the systematic review. The PRISMA-2020, flow diagram is shown in Figure 1.
3.2. Quality assessment results:
The quality assessment results of the included studies are shown in Table 1
3.3. Study characteristics:
All sixteen studies included are summarized in Table 2, highlighting the study type, period of study, main characteristics/ methodology, and conclusions.
3.4. Clinic-pathological results:
The results are summarized in Supplementary Table 3. The main highlight is that surgery was usually performed for T2-stage of prostate cancer (54%).
3.5. Demographics and VTE risk factors
The VTE risk factors including age, BMI, personal history of VTE as well as family VTE are summarized with remarks in Table 3. The age was described in 13 studies, with the mean age of patients undergoing surgery being 64 years (60-72 years). Six studies provided details about BMI. The average BMI was 27.6%. Personal history of VTE had been investigated by 3 studies, with the average being 2.3% and family history of VTE in one study, 4.0%. Three studies investigated smoking and were found in 30% of patients. Lastly, only one study investigated Caprini’s score in their cohort of patients.
3.6. Surgical Procedure results:
Out of 16 studies, 15 have mentioned detailed surgical approaches offered for radical prostatectomy (Open/Laparoscopic/ Robotic). 11 studies have described the results of pelvic lymph node dissection in their cohort of patients. Results are summarized in Table 4.
3.7. Thromboprophylaxis and VTE episodes
The results of different types of thromboprophylaxis as well as the number of VTE episodes are provided in Table 5. Fourteen studies have provided details about VTE prophylaxis (95,052 patients). Of these patients, 22.4% did not receive any form of VTE prophylaxis. 41.8% of patients received mechanical prophylaxis followed by 30% of patients receiving combined (mechanical as well as pharmacological) prophylaxis and lastly, 5.7% of patients received only pharmacological prophylaxis Figure 2.
3.8. Surgical approaches and VTE episodes
Total VTE episodes in open RP were discussed in 11 studies with a mean VTE incidence of 1.5%. 8 studies discussed VTE episodes in MIS having a mean incidence of 0.9%. 8 studies investigated DVT incidence in post-RP patients and this was 0.3%. 13 studies described PE incidence in post-RP patients and had a mean value of 1.5%. These results are tabulated in Table 6.
3.9. Duration and timing of Thromboprophylaxis
In most studies, mechanical prophylaxis was initiated in patients prior to surgery and continued till patient discharge from the hospital. In some studies, patients were also encouraged to ambulate on discharge [20].
3.10. Statistical Results
- a.
- Statistical outcome of overall VTE occurrence
A summary of the meta-analysis results is summarized in Table 7. The first figures are the number of studies with valid data included in each analysis. Subsequently, details of the heterogeneity are reported, both in terms of the significance and the I2 values. The next figures are the pooled percentage of patients in which the outcome occurred for each method, presented with a corresponding confidence interval. The pooled results suggested that, for all patients combined, the occurrence of VTE was 1.0% (95% CI: 0.5% to 1.5%). The graphical illustration of the meta-analysis results is shown in Figure 3.
- b.
- Statistical outcome of VTE occurrence depending on the type of surgical procedure (Open/MIS) and whether PLND was performed or not.
A summary of the meta-analysis results is summarized in Table 8. The first figures are the number of studies with valid data included in each analysis. Subsequently, details of the heterogeneity are reported in terms of the significance and the I2 values. The final columns give the differences in outcome between the two risk groups. The pooled difference in outcome between groups is expressed as a relative risk. The pooled figure is presented along with a corresponding confidence interval. The final column shows the p-values indicating the significance of the differences between risk groups.
The analysis suggested a statistically significant difference in outcome between MIS and Open procedures, based on data from 5 studies. The pooled results suggested a lesser occurrence of VTEs in MIS procedures compared to Open procedures. The number of VTEs was just over a third lower (0.63 times as large) in the MIS group when compared to the Open Group. There was little heterogeneity between the different studies. A graphical illustration of the meta-analysis results is shown in Figure 4.
There were two studies providing sufficient data to compare patients where PLND was used and not used. The data suggested some evidence that VTE was more common with the use of PLND. However, the result did not quite reach statistical significance. The pooled results suggested that a VTE was 2.8 times more likely when PLND was performed compared to when it wasn’t. There was little heterogeneity between the two studies. A graphical illustration of the results is shown in Figure 5.
- c.
- Statistical outcome of VTE occurrence depending on the method of prophylaxis used (mechanical or combined).
The meta-analysis pooled together the results from studies with patients undergoing mechanical and combined prophylaxis methods. A summary of the meta-analysis results is summarised in Table 9. The first figures are the number of studies with valid data included in each analysis. Subsequently, details of the heterogeneity are reported in terms of the significance and the I2 values. The next figures are the pooled percentage of patients with VTE for each method, presented with a corresponding confidence interval. The final column shows the p-values indicating the significance of the differences in VTE between groups.
The pooled results suggested that 0.7% of patients underwent a VTE for the mechanical method, whilst 1.0% underwent VTE for the combined method. There was no statistical difference in VTE occurrence between the two methods. A graphical illustration of the results is shown in Figure 5.
4. Discussion
Venous thromboembolism (VTE) is a complex multifactorial clinical entity associated with significant morbidity and mortality and can present either as deep venous thrombosis (DVT) and/or concomitant pulmonary embolism (PE) [33]. VTE in malignancies is multifactorial-it can be cancer related as well as individual-related. A hypercoagulable state is induced directly by activating the blood clotting cascade and inducing pro-coagulant and inhibiting anticoagulant properties of endothelial cells, platelets, monocytes, and macrophages [34].
VTE does have a considerable impact on morbidity, mortality, and economic cost, and has led to the development of VTE risk stratification tools such as the Caprini risk assessment [33]. In addition to VTE risks associated with major surgical procedures and underlying malignancy, American Heart Association (AHA) has identified additional factors including prior VTE, age, obesity, immobility, and family history. Regarding the VTE risks associated with major surgical procedures and underlying malignancy, American Heart Association (AHA) has identified additional factors including prior VTE, age, obesity, immobility, and family history. VTE risk stratification in surgical patients according to the Seventh American College of Chest Physicians Conference on Antithrombotic and Thrombolytic Therapy is provided in Supplementary Table 4.
Thromboprophylaxis, whether mechanical, pharmacological, or combination is widely practiced across surgical specialties based on substantial evidence from randomized control trials (RCTs). However, there has been a lack of urology-specific evidence, leading to conflicting recommendations both nationally and internationally [35]. This gets more complicated when individual urological procedures are considered for VTE prophylaxis. In the case of RP, the European Association of Urology (EAU) 2022 has provided guidelines for VTE prophylaxis based on available literature [36]. The EAU has considered a few factors including patient VTE risk factors (Low/Medium/ High), type of surgical intervention (Open/laparoscopic/Robotic), Extent of surgery (No PLND/Standard PLND/Extended PLND), and availability of evidence for it. The summarized results are tabulated in Table.10. The studies and research used for EAU guidelines are mainly non-urological and rightly they have admitted that the evidence base is limited for this guideline. On the other hand, the National Institute for Health, and Care Excellence (NICE), UK, recommends VTE Prophylaxis to people undergoing abdominal (gastrointestinal, gynecological, urological) surgery who are at increased risk of VTE. It recommends mechanical VTE prophylaxis on admission for people undergoing abdominal surgery either anti-embolism stockings or intermittent pneumatic compression (until the patient is ambulatory). It also recommends Pharmacological VTE prophylaxis for people undergoing abdominal surgery, including-7 days for non-cancer and 28 days (Extended) for major cancer surgery postoperatively [37]. American urological society (AUA) recommends mechanical prophylaxis during MIS urological procedures, and pharmacological prophylaxis is reserved for high-risk patients only. For open urological procedures, AUA recommends the consideration of combined prophylaxis [38].
To our knowledge, this meta-analysis is the first of its kind specifically dealing with VTE prophylaxis in radical prostatectomy patients. We were able to establish a statistically significant higher incidence of VTE in open RP in comparison to MIS prostatectomy procedures. A similar observation has also been noticed in other abdominal procedures as well [39]. This analysis also revealed a higher incidence of VTE in patients undergoing RP as well as PLND. A study in 2011 including 773 patients, also demonstrated that there is a significant association between venous thromboembolism and radical prostatectomy plus pelvic lymph node dissection compared to radical prostatectomy only [40]. Lastly, we were able to establish that combined prophylaxis (Mechanical and pharmacological) does not have an advantage over mechanical prophylaxis in RP. This implies that PP is not indicated for the routine MIS approach for RP procedures. This is a finding which has not been confidently proven before this meta-analysis.
Additionally, we did find that there are other well-established factors that can contribute to VTE occurrences in post-RP patients as well, including age, personal and family history of VTE. Some of the studies in this meta-analysis have discussed these contributing factors, however, the data was not enough to perform a statistical analysis. These have been summarized in Table 3. These factors are essential in stratifying high-risk cohorts of patients.
Lastly, we found that the duration of VTE prophylaxis after RP has been quite variable across the globe. This is an issue that has been a bone of contention across surgical specialties both within and outside, and unfortunately, has been as such for more than a decade [41].
To summarize, this meta-analysis and the systematic review revealed that VTE events in RP procedures were reduced by switching to MIS procedures in comparison to open procedures. Additionally, PLND increases the risk of VTE and should be considered a high-risk factor while stratifying patients for consideration of VTE prophylaxis. Lastly, PP in cases of RP does not have an added advantage to mechanical prophylaxis. This systematic review forms a basis and provides a platform for future, randomized controlled trials taking into account all variables for consideration of globally acceptable guidelines for VTE prophylaxis in RP surgeries.
The limitations of this study include the scarcity of research available, the heterogenous nature of studies, and the non-uniformity of VTE prophylaxis practices across the globe for RP. In the future, there is a need for a multicentric randomized control trial to establish a VTE risk scoring system for RP patients and VTE prophylaxis guidelines to bring uniformity to this controversial practice.
5. Conclusion
This systematic review concludes that the overall incidence of VTE post-RP is 1%. The incidence of VTE in patients undergoing RP for prostate cancer is significantly less in minimally invasive (Laparoscopic/Robotic) procedures in comparison to open. Patients need to be stratified into risk groups using pre-existing guidelines and risk categories while PLND should be considered an additional risk factor. Additional PP to mechanical methods may not be necessary in all cases and should be considered in high-risk patients only.
Author Contributions
Mudassir M. Wani: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Resources; Visualization; Writing – original draft; Writing – review & editing. Abdullah Al-Mitwalli: Investigation; Methodology; Project administration. Subhabrata Mukherjee: Investigation; Methodology; Project administration. Ghulam Nabi: Validation; Writing – review & editing. Bhaskar K Somani : Validation; Writing – review & editing. Jayasimha Abbaraju: Investigation; Methodology; Project administration. Sanjeev Madaan: Conceptualization; Data curation; Formal analysis; Project administration; Resources; Supervision; Validation; Writing – review & editing.
Acknowledgments
The authors express their gratitude to Paul Bassett, statistician, and director of Stats Consultancy Ltd., for providing support in data analysis and statistical work. We are also thankful to Genny Franklin, Clinical Librarian, Dartford and Gravesham NHS Trust, Dartford, UK, for helping in the evidence search.
References
- Guyatt, G. H.; Eikelboom, J. W.; Gould, M. K.; Garcia, D. A.; Crowther, M.; Murad, M. H.; Kahn, S. R.; Falck-Ytter, Y.; Francis, C. W.; Lansberg, M. G.; Akl, E. A.; Hirsh, J. Approach to Outcome Measurement in the Prevention of Thrombosis in Surgical and Medical Patients. Chest 2012, 141, e185Se194S. [Google Scholar] [CrossRef] [PubMed]
- Kibel, A. S.; Loughlin, K. R. Pathogenesis and Prophylaxis of Postoperative Thromboembolic Disease in Urological Pelvic Surgery. The Journal of Urology 1995, 1763–1774. [Google Scholar] [CrossRef]
- Geerts, W. H.; Heit, J. A.; Clagett, G. P.; Pineo, G. F.; Colwell, C. W.; Anderson, F. A.; Wheeler, H. B. Prevention of Venous Thromboembolism. Chest 2001, 119. [Google Scholar] [CrossRef] [PubMed]
- Geerts, W. H.; Pineo, G. F.; Heit, J. A.; Bergqvist, D.; Lassen, M. R.; Colwell, C. W.; Ray, J. G. Prevention of Venous Thromboembolism. Chest 2004, 126. [Google Scholar] [CrossRef]
- Zhan, C. Excess Length of Stay, Charges, and Mortality Attributable to Medical Injuries during Hospitalization. JAMA 2003, 290, 1868. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, G.; Léandri, P.; Gautier, J. R.; Quintens, H.; Gabay-Torbiero, L.; Tap, G. Radical Retropubic Prostatectomy: Complications and Quality of Life (429 Cases, 1983-1989). European Urology 1991, 19, 186–191. [Google Scholar] [CrossRef]
- Brenner, D. W.; Fogle, M. A.; Schellhammer, P. F. Venous Thromboembolism. Journal of Urology 1989, 142, 1403–1411. [Google Scholar] [CrossRef]
- De Martino, R. R.; Goodney, P. P.; Spangler, E. L.; Wallaert, J. B.; Corriere, M. A.; Rzucidlo, E. M.; Walsh, D. B.; Stone, D. H. Variation in Thromboembolic Complications among Patients Undergoing Commonly Performed Cancer Operations. Journal of Vascular Surgery 2012, 55, 1035–1040. [Google Scholar] [CrossRef]
- Beyer, J.; Wessela, S.; Hakenberg, O.; Wirth, M.; Schellong, S. Incidence and Disease Pattern of Venous Thrombembolism after Radical Prostatectomy. Blood 2005, 106, 1627–1627. [Google Scholar] [CrossRef]
- O’Donnell, M.; Weitz, J. I. Thromboprophylaxis in Surgical Patients. Canadian journal of surgery. Journal canadien de chirurgie 2003, 46, 129–135. [Google Scholar]
- Pridgeon, S.; Allchorne, P.; Turner, B.; Peters, J.; Green, J. Venous Thromboembolism (VTE) Prophylaxis and Urological Pelvic Cancer Surgery: A UK National Audit. BJU International 2014, 115, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Tikkinen, K. A. O.; Craigie, S.; Agarwal, A.; Violette, P. D.; Novara, G.; Cartwright, R.; Naspro, R.; Siemieniuk, R. A. C.; Ali, B.; Eryuzlu, L.; Geraci, J.; Winkup, J.; Yoo, D.; Gould, M. K.; Sandset, P. M.; Guyatt, G. H. Procedure-Specific Risks of Thrombosis and Bleeding in Urological Cancer Surgery: Systematic Review and Meta-Analysis. European Urology 2018, 73, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Violette, P. D.; Cartwright, R.; Briel, M.; Tikkinen, K. A. O.; Guyatt, G. H. Guideline of Guidelines: Thromboprophylaxis for Urological Surgery. BJU International 2016, 118, 351–358. [Google Scholar] [CrossRef]
- Weinberg, A.; Wright, J.; Deibert, C.; Lu, Y.-S.; Hershman, D.; Neugut, A.; Spencer, B. Nationwide Practice Patterns for the Use of Venous Thromboembolism Prophylaxis among Men Undergoing Radical Prostatectomy. World Journal of Urology 2013, 32, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Page, M. J.; McKenzie, J. E.; Bossuyt, P. M.; Boutron, I.; Hoffmann, T. C.; Mulrow, C. D.; Shamseer, L.; Tetzlaff, J. M.; Akl, E. A.; Brennan, S. E.; Chou, R.; Glanville, J.; Grimshaw, J. M.; Hróbjartsson, A.; Lalu, M. M.; Li, T.; Loder, E. W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L. A. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. British Medical Journal 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. 2013. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- Patel, H. D.; Faisal, F. A.; Trock, B. J.; Joice, G. A.; Schwen, Z. R.; Pierorazio, P. M.; Johnson, M. H.; Bivalacqua, T. J.; Han, M.; Gorin, M. A.; Carter, H. B.; Partin, A. W.; Pavlovich, C. P.; Allaf, M. E. Effect of Pharmacologic Prophylaxis on Venous Thromboembolism after Radical Prostatectomy: The PREVENTER Randomized Clinical Trial. European Urology 2020, 78, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Valverde-Martinez, S.; Gonzalez-Rayo, L.-A.; Padilla-Fernandez, B.; Pereira-Bruno, J.; Coelho, H.; Montesino-Semper, M.; Müller-Arteaga, C.; Alvarez-Ossorio-Fernandez, J.-L.; Migliorini, F.; Garcia-Cenador, M.-B.; Lorenzo-Gomez, M.-F. Profilaxis Farmacológica de La Tromboembolia Venosa En La Prostatectomía Radical. Medicina Clínica 2020, 154, 113–118. [Google Scholar] [CrossRef]
- Weinberg, A.; Wright, J.; Deibert, C.; Lu, Y.-S.; Hershman, D.; Neugut, A.; Spencer, B. Nationwide Practice Patterns for the Use of Venous Thromboembolism Prophylaxis among Men Undergoing Radical Prostatectomy. World Journal of Urology 2013, 32, 1313–1321. [Google Scholar] [CrossRef]
- Tollefson, M. K.; Karnes, R. J.; Rangel, L.; Carlson, R.; Boorjian, S. A. Blood Type, Lymphadenectomy and Blood Transfusion Predict Venous Thromboembolic Events Following Radical Prostatectomy with Pelvic Lymphadenectomy. Journal of Urology 2014, 191, 646–651. [Google Scholar] [CrossRef]
- Chan, S. Y. S.; Leung, V. F. Y.; Yee, C. H.; Chan, E. S. Y.; Hou, S. S. M.; Chu, W.; Ng, C. F. Incidence of Postoperative Deep Vein Thrombosis after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective Study in Chinese Patients. International Urology and Nephrology 2014, 46, 2139–2142. [Google Scholar] [CrossRef]
- Chalmers, D. J.; Scarpato, K. R.; Staff, I.; Champagne, A.; Tortora, J.; Wagner, J. R.; Kesler, S. S. Does Heparin Prophylaxis Reduce the Risk of Venous Thromboembolism in Patients Undergoing Robot-Assisted Prostatectomy? Journal of Endourology 2013, 27, 800–803. [Google Scholar] [CrossRef] [PubMed]
- Abel, E. J.; Wong, K.; Sado, M.; Leverson, G. E.; Patel, S. R.; Downs, T. M.; Jarrard, D. F. Surgical Operative Time Increases the Risk of Deep Venous Thrombosis and Pulmonary Embolism in Robotic Prostatectomy. JSLS : Journal of the Society of Laparoendoscopic Surgeons 2014, 18, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.; Wyke, S.; Lynch, C. Hospital Episode Statistics Data Analysis of Postoperative Venous Thromboembolus in Patients Undergoing Urological Surgery: A Review of 126,891 Cases. The Annals of The Royal College of Surgeons of England 2013, 95, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, M.; Garmo, H.; Holmberg, L.; Bill-Axelson, A.; Carlsson, S.; Akre, O.; Stattin, P.; Adolfsson, J. Thromboembolic Events Following Surgery for Prostate Cancer. European Urology 2013, 63, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Eifler, J. B.; Levinson, A. W.; Hyndman, M. E.; Trock, B. J.; Pavlovich, C. P. Pelvic Lymph Node Dissection Is Associated with Symptomatic Venous Thromboembolism Risk during Laparoscopic Radical Prostatectomy. Journal of Urology 2011, 185, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- BEYER, J.; WESSELA, S.; HAKENBERG, O. W.; KUHLISCH, E.; HALBRITTER, K.; FROEHNER, M.; WIRTH, M. P.; SCHELLONG, S. M. Incidence, Risk Profile and Morphological Pattern of Venous Thromboembolism after Prostate Cancer Surgery. Journal of Thrombosis and Haemostasis 2009, 7, 597–604. [Google Scholar] [CrossRef]
- Grasso, M.; Confalonieri, S.; Blanco, S.; Grasso, A.; Angelo, S. Preoperative Blood Donation Program and Postoperative Low Molecular Weight Heparine (LMWH) Prophylaxis in Patients Undergoing Radical Prostatectomy. Archivos Españoles de Urología (Ed. impresa) 2009, 62. [Google Scholar] [CrossRef] [PubMed]
- Cindolo, L.; Salzano, L.; Mirone, V.; Imbimbo, C.; Longo, N.; Kakkos, S. K.; Reddy, D. J. Thromboprophylaxis in Radical Retropubic Prostatectomy: Efficacy and Patient Compliance of a Dual Modality. Urologia Internationalis 2009, 83, 12–18. [Google Scholar] [CrossRef]
- Nakamura, K.; Kasraeian, A.; Yacoub, S.; Pendleton, J.; Anai, S.; Rosser, C. J. The Use of Enoxaparin to Prevent Venous Thromboembolism in Patients Undergoing Radical Retropubic Prostatectomy: Feasibility and Utility. International braz j urol 2007, 33, 347–354. [Google Scholar] [CrossRef]
- Koya, M. P.; Manoharan, M.; Kim, S. S.; Soloway, M. S. Venous Thromboembolism in Radical Prostatectomy: Is Heparinoid Prophylaxis Warranted? BJU International 2005, 96, 1019–1021. [Google Scholar] [CrossRef]
- Cisek, L. J.; Walsh, P. C. Thromboembolic Complications Following Radical Retropubic Prostatectomy Influence of External Sequential Pneumatic Compression Devices. Urology 1993, 42, 406–408. [Google Scholar] [CrossRef] [PubMed]
- Salous, A. K.; Reyad, A.; Sweeney, K.; Mavanur, A. A Significant Proportion of Venous Thromboembolism Events in General Surgical Patients Occurs after Discharge: Analysis of the ACS-NSQIP Essentials Database. Perioperative Medicine 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, A.; Piotr Skrudlik; Kowalski, F.; Lipowski, P.; Ostrowska, M.; Adamczyk, P.; Adamowicz, J.; Drewa, T.; Juszczak, K. Current Thromboprophylaxis in Urological Cancer Patients during COVID Pandemic. Central European Journal of Urology 2022. [CrossRef]
- Violette, P. D.; Cartwright, R.; Briel, M.; Tikkinen, K. A. O.; Guyatt, G. H. Guideline of Guidelines: Thromboprophylaxis for Urological Surgery. BJU International 2016, 118, 351–358. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines. Edn. presented at the EAU Annual Congress Amsterdam 2022. ISBN 978-94-92671-16-5.
- NICE. Recommendations | Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or pulmonary embolism | Guidance | NICE. Nice.org.uk. https://www.nice.org.uk/guidance/ng89/chapter/Recommendations#interventions-for-people-having-abdominal-thoracic-or-head-and-neck-surgery.
- Forrest, J. B.; Clemens, J. Q.; Finamore, P.; Leveillee, R.; Lippert, M.; Pisters, L.; Touijer, K.; Whitmore, K. AUA Best Practice Statement for the Prevention of Deep Vein Thrombosis in Patients Undergoing Urologic Surgery. Journal of Urology 2009, 181, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Barber, E. L.; Gehrig, P. A.; Clarke-Pearson, D. L. Venous Thromboembolism in Minimally Invasive Compared with Open Hysterectomy for Endometrial Cancer. Obstetrics & Gynecology 2016, 128, 121–126. [Google Scholar] [CrossRef]
- Eifler, J. B.; Levinson, A. W.; Hyndman, M. E.; Trock, B. J.; Pavlovich, C. P. Pelvic Lymph Node Dissection Is Associated with Symptomatic Venous Thromboembolism Risk during Laparoscopic Radical Prostatectomy. Journal of Urology 2011, 185, 1661–1666. [Google Scholar] [CrossRef]
- Muntz, J. Duration of Deep Vein Thrombosis Prophylaxis in the Surgical Patient and Its Relation to Quality Issues. The American Journal of Surgery 2010, 200, 413–421. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 Flow diagram.
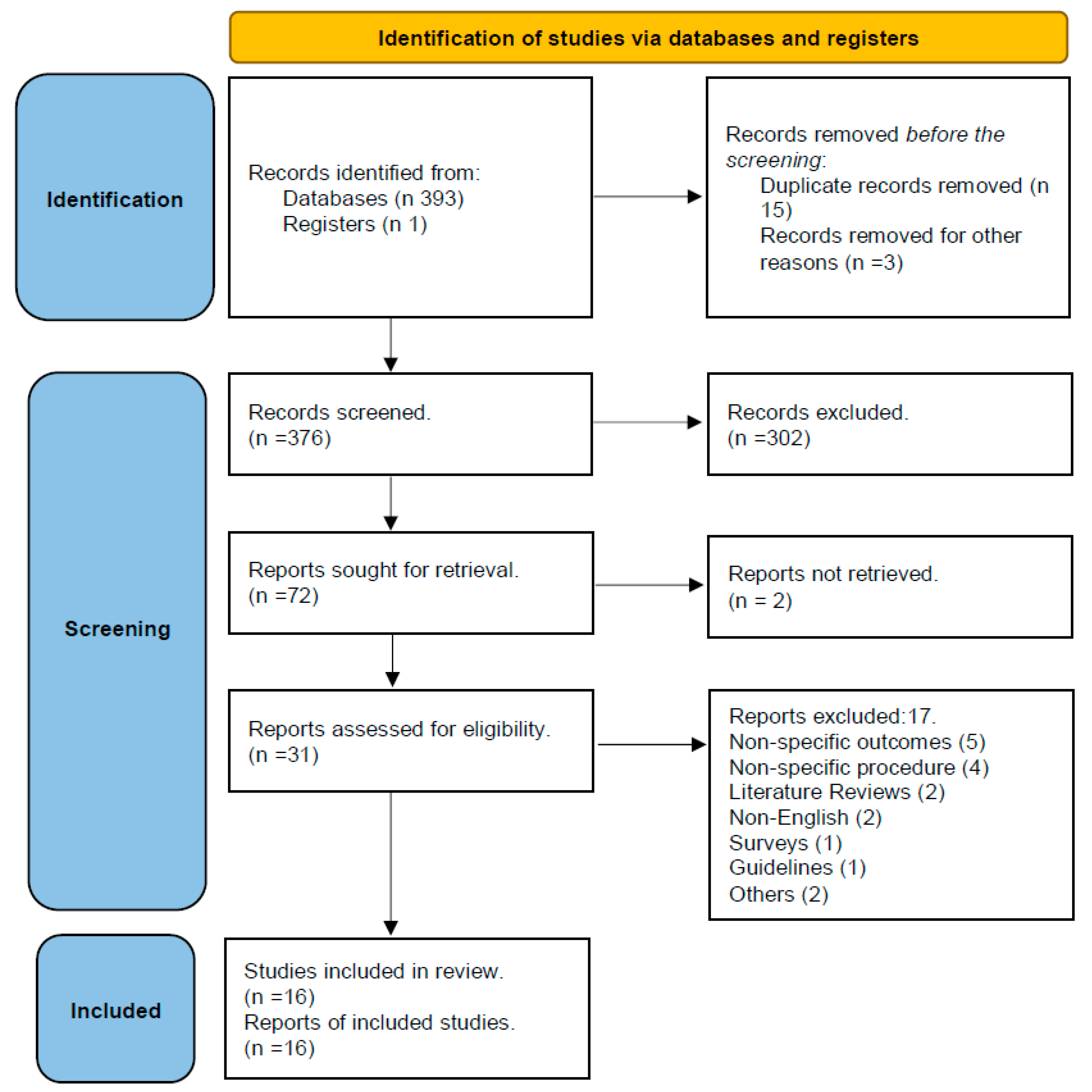
Figure 2.
VTE Prophylaxis distribution in Post-RP patients.
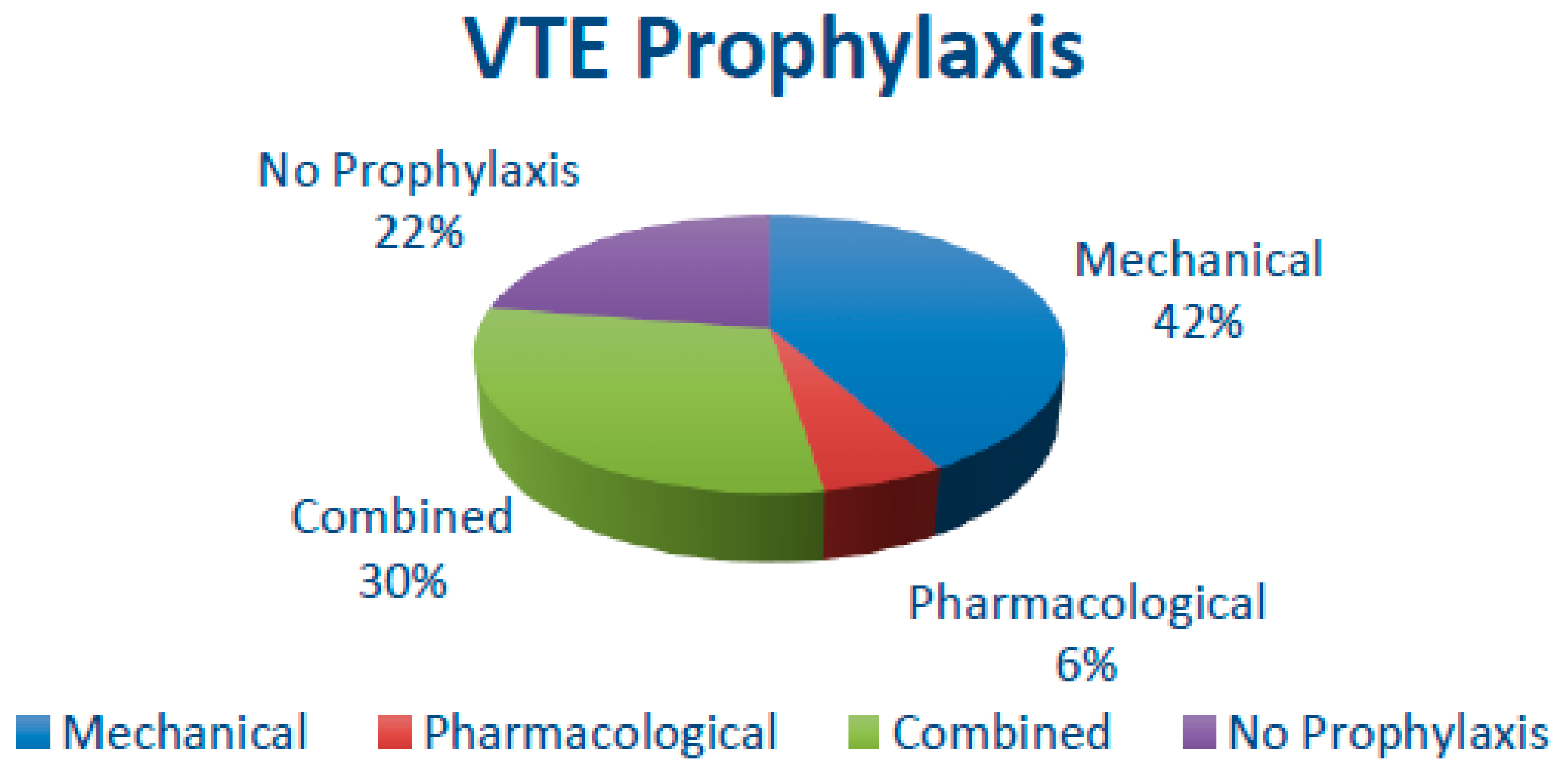
Figure 3.
Overall VTE Occurrence.
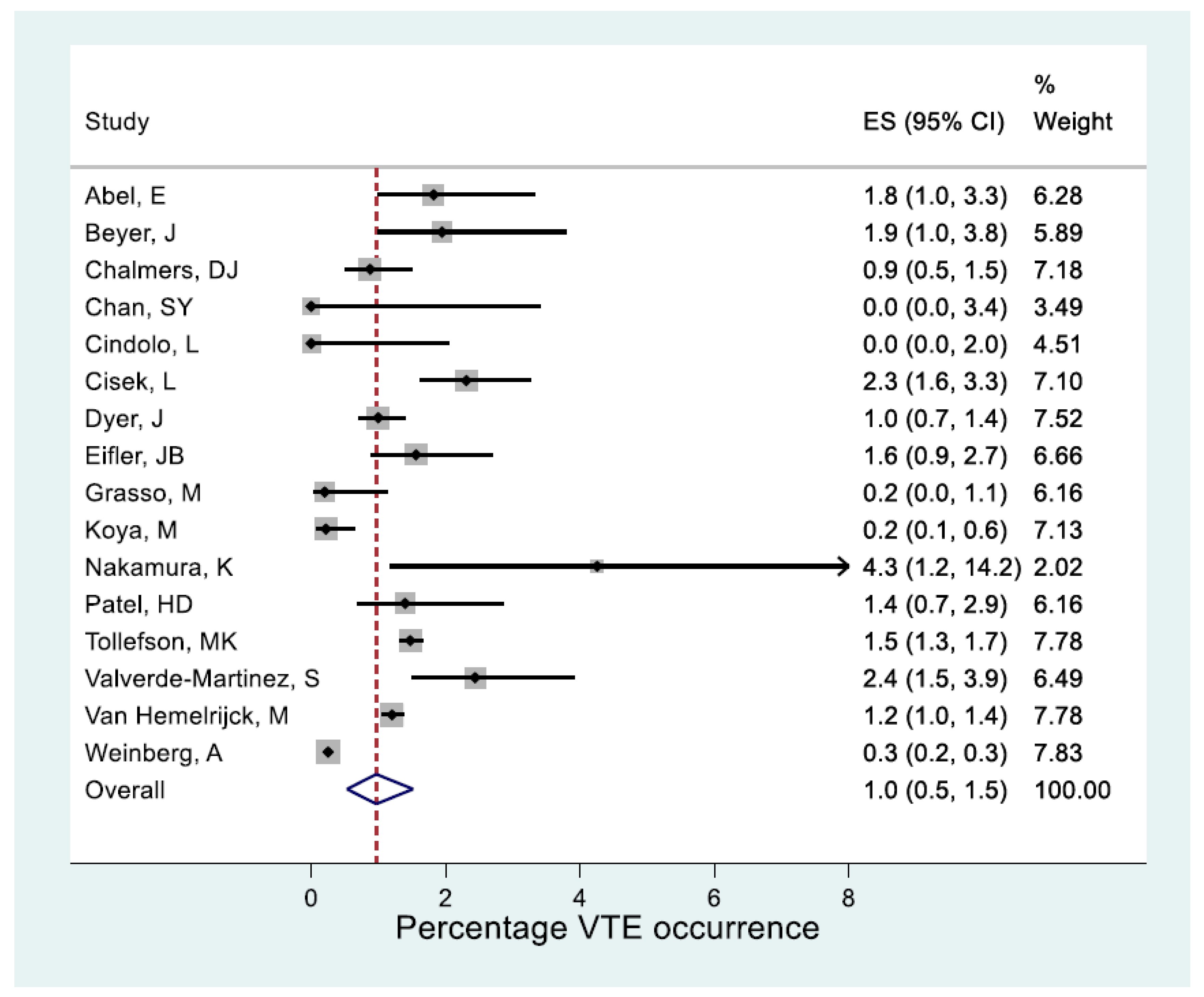
Figure 4.
VTE in MIS and Open Surgery.

Figure 5.
VTE in procedures with and without PLND.
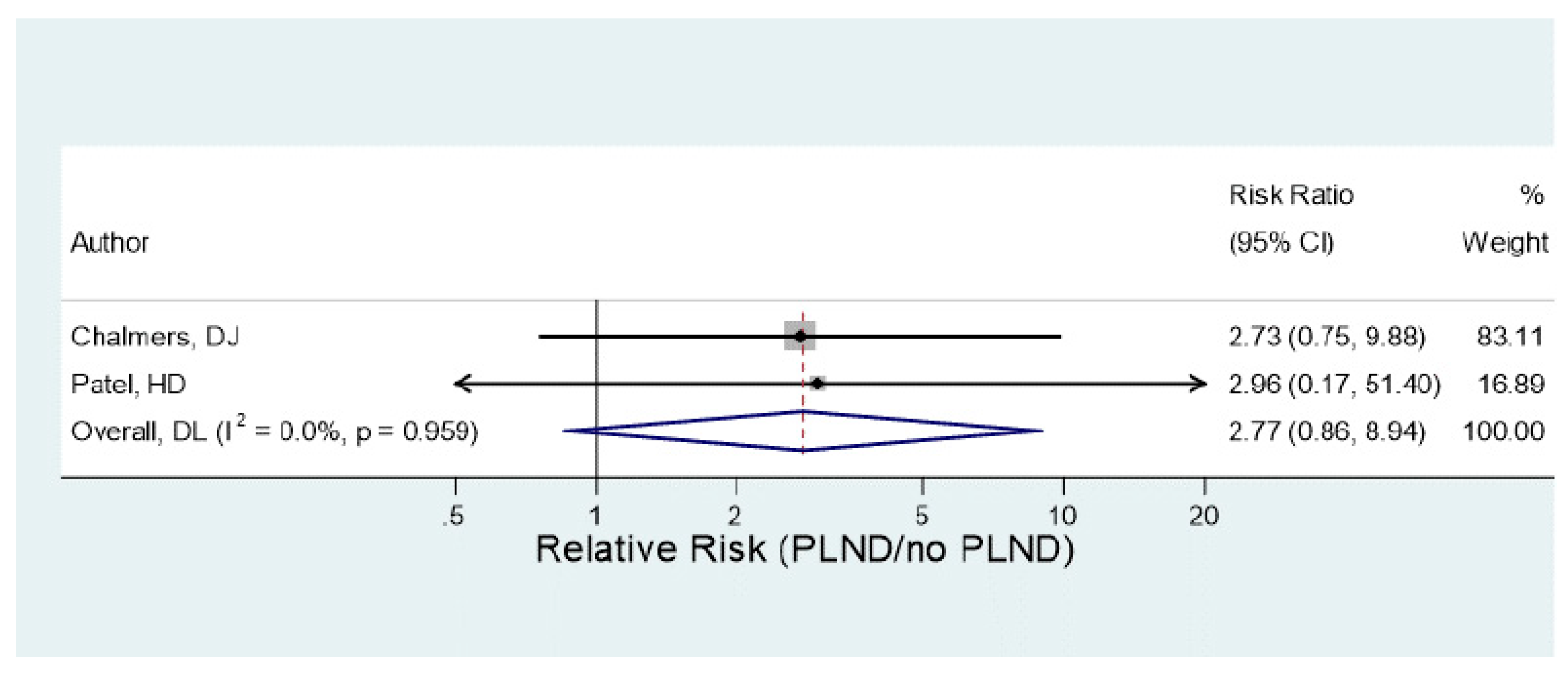

Table 1.
Newcastle Ottowa Scale.
| Author | Number of awarded stars in each domain | ||
|---|---|---|---|
| Selection | Comparability | Outcome | |
| (1) Patel, H. D [17] | **** | ** | ** |
| (2) Valverde-Martinez, S. [18] | *** | * | ** |
| (3) Weinberg, A. [19] | *** | ** | |
| (4) Tollefson, M. K. [20] | *** | ** | |
| (5) Chan, S. [21] | ** | ** | |
| (6) Chalmers, D. J. [22] | *** | ** | |
| (7) Abel ,E.[23] | *** | ** | |
| (8) Dyer, J [24] | ** | * | |
| (9) Van Hemelrijck, M.[25] | ** | ** | |
| (10) Eifler, J. B .[26] | ** | ** | |
| (11) Beyer, J. [27] | *** | ** | |
| (12) Grasso, M. [28] | ** | * | |
| (13) Cindolo, L.[29] | ** | * | |
| (14) Nakamura, K. [30] | ** | * | |
| (15)Koya, M. [31] | *** | * | |
| (16) Cisek, L.[32] | ** | * | |
Table 2.
Study Characteristics.
| Study | Study Type/ Time |
Study Characteristics | Conclusion |
|---|---|---|---|
|
(1) Patel, H. D. [17] |
RCT (2017-18) |
|
|
|
(2) Valverde-Martinez, S. [18] |
Retrospective (2013-14) |
|
|
|
(3) Weinberg, A. [19] |
Observational (2000-10) |
|
|
|
(4) Tollefson, M. K [20] |
Retrospective (1987-2010) |
|
|
|
(5) Chan, S.Y. [21] |
Prospective (2007-2010) |
|
|
|
(6) Chalmers, D. J. [22] |
Prospective (2007-2011) |
|
|
|
(7) Abel, .E [23] |
Retrospective (2007-2011) |
|
|
|
(8) Dyer, J. [24] |
Retrospective (2009-2010) |
|
|
|
(9) Van Hemelrijck, M. [25] |
Retrospective (2002-2010) |
|
|
|
(10) Eifler, J. B. [26] |
Retrospective (2001-2009) |
|
|
|
(11) Beyer, J. [27] |
Prospective (2001-2003) |
|
|
|
(12) Grasso, M. [28] |
Retrospective (1999-2006) |
|
|
|
(13) Cindolo, L. [29] |
Prospective (2004-2006) |
|
|
|
(14) Nakamura, K . [30] |
Prospective (2003-2005) |
|
|
|
(15) Koya, M . [31] |
Prospective (1992-2004) |
|
|
|
(16) Cisek, L . [32] |
Prospective (1982-1993) |
|
|
| BMI-Body Mass Index; DVT-Deep Vein Thrombosis; HES- Hospital Episode Statistics; LMHW-Low Molecular Weight heparin; IPC- Intermittent pneumatic compression; ORP-Open Radical Prostatectomy; PCa- Prostate Cancer; PCS- Pneumatic Compression Stocking; PLND- Pelvic Lymph Node dissection; PP-Pharmacological Prophylaxis; RARP-Robot-assisted radical prostatectomy; SCD- Sequential Compression Device; VTE-Venous thromboembolism; | |||
Table 3.
Demographics and VTE risk factors.
| Study | Total patients | Mean Age | Mean BMI kg/m2 |
Family history (%) |
VTE Back- ground (%) |
Smoking | Overall risk assessment (in %) |
Caprini Score | Remarks in relation to VTE risk factors/ Scores | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | Int | High | |||||||||
| (1) Patel, H. D. [17] | 501 | 62 | 27.4 | - | - | - | - | - | - | 6 | The study concluded that most patients with prostate cancer undergoing RP are relatively healthy, our study suggests that PP may be deferred based on surgeon preference up to a Caprini score of 7; PP may be justified for higher-risk patients with scores of 8. |
| (2) Valverde-Martinez, S. [18] | 610 | 64.1 | 28.03 | - | - | - | 94.8 | 4.1 | 1.1 | - | This study concluded that with respect to the PP used in different thromboembolic risk groups, there were differences in the low-risk group but not in the intermediate and high-risk groups; this was probably due to the fact that this group covered 95% of the cases in the series |
| (3) Weinberg, A. [19] | 94,709 | - | - | - | - | - | - | - | - | - | - |
| (4) Tollefson, M. K [20] | 18,472 | 63 | 27.7 | - | - | - | - | - | - | - | They concluded that patients with VTE were significantly older than those not diagnosed with VTE (median age 65 vs 63 years, p <0.001). |
| (5) Chan, S.Y [21] | 109 | 65.7 | <23 (33) >23 (67) |
- | - | 18.1 | - | - | - | - | This study concluded that there was no difference in the incidence of DVT between patients with a history of smoking or diabetes or a high body mass (BMI) index and those without. |
| (6) Chalmers, D. J . [22] | 1486 | 59.9 | 28.1 | - | - | - | - | - | - | - | In this study, BMI was not found to be associated with VTE. |
| (7) Abel, E. [23] | 549 | 59.8 | - | - | 1.6 | 43.8 | - | A 5-point increase in body mass index was associated with an increased risk of VTEs (odds ratios of 2.0). | |||
|
(8)Dyer, J. [24] |
3,213 | 72.5 | - | - | - | - | - | - | - | - | - |
| (9) Van Hemelrijck, M [25] | 16,304 | - | - | - | 0.6 | - | - | - | - | - | A previous history of VTE is a risk factor in patients undergoing RP. |
| (10)Eifler, J. B [26] | 773 | 57.8 | 27.3 | - | - | - | - | - | - | - | A high incidence of VTE was found in patients with BMI in the top quartile who concomitantly underwent PLND. |
| (11) Beyer, J [27] | 411 | 65.0 | 27.0 | 4.0 | 4.8 |
- | - | - | - | A statistically higher risk was found in patients with a personal history of VTE, however, family history was not found with increased risk. | |
| (12) Grasso, M. [28] | 500 | 65.0 | - | - | - | - | - | - | - | - | - |
| (13) Cindolo, L.[29] | 184 | 69.0 | >25 (30%) | - | - | 28 | - | - | - | - | - |
| (14) Nakamura, K . [30] | 47 | 64.0 | - | - | - | - | - | - | - | - | - |
|
(15)Koya, M . [31] |
1364 | 60.8 | - | - | - | - | - | - | - | - | - |
|
(16) Cisek, L. [32] |
1300 | - | - | - | - | - | - | - | - | - | - |
Table 4.
Details about surgical procedures.
| Study | Total Procedures | Open | Laparoscopic | Robotic | Unknown | PLND (%) |
|---|---|---|---|---|---|---|
| (1) Patel, H. D [17] | 501 | 124 | - | 377 | - | 83.5 (419) |
| (2) Valverde-Martinez, S. [18] | 610 | 268 | 311 | 31 | - | - |
| (3) Weinberg, A. [19] | 94,709 | 68,244 | - | 26,465 | - | - |
| (4) Tollefson, M. K. [20] | 18,472 | 16,374 | - | 2,098 | - | 100 |
| (5) Chan, S. [21] | 109 | - | - | 109 | - | 33.94 (37) |
| (6) Chalmers, D. J. [22] | 1486 | - | - | 1486 | - | 55 |
| (7) Abel ,E.[23] | 549 | - | - | 549 | - | 12.9 (71/549) |
| (8) Dyer, J [24] | 3,213 | - | - | - | 3213 | - |
| (9) Van Hemelrijck, M.[25] | 16304 | 11137 | - | 5167 | - | 21.6 (3258/16304) |
| (10) Eifler, J. B .[26] | 770 | - | 770 | - | - | 60.8 (468/770) |
| (11) Beyer, J. [27] | 411 | 411 | - | - | - | 100 |
| (12) Grasso, M. [28] | 500 | 500 | - | - | - | - |
| (13) Cindolo, L.[29] | 184 | 184 | - | - | - | 100 |
| (14) Nakamura, K. [30] | 47 | 47 | - | - | - | 87 (41/47) |
| (15)Koya, M. [31] | 1373 | 1373 | - | - | - | 67 (920/1373) |
| (16) Cisek, L.[32] | 1300 | 1300 | - | - | - | - |
| Total | 140,541 | 100,088 (71.21%) |
1084 (0.77%) |
36,156 (25.72%) |
3213 (2.28%) |
33.82% (6229/18417) |
Table 5.
Thromboprophylaxis and VTE Episodes.
| Thromboprophylaxis | VTE Symptomatic Episodes (in %) |
|||||||
|---|---|---|---|---|---|---|---|---|
| N | M | P | C | N | M | P | C | |
| (1) Patel, H. D [17] | - | 250 | - | 251 | - | 2.0 | - | 0.8 |
| (2) Valverde-Martinez, S. [18] | 94 | 25 | 516 | 21 | 2.5 | |||
| (3) Weinberg, A. [19] | 20438 | 35591 | 4945 | 7720 | 0.25 | |||
| (4) Tollefson, M. K. [20] | - | - | - | 18472 | 1.47 | |||
| (5) Chan, S. [21] | - | 109 | - | - | 0.09 | |||
| (6) Chalmers, D. J. [22] | - | 564 | - | 922 | - | 1.0 | - | 0.7 |
| (7) Abel ,E.[23] | - | 540 | - | 9 | 1.8 | |||
| (8) Dyer, J [24] | - | - | - | - | 1.0 | |||
| (9) Van Hemelrijck, M.[25] | - | - | - | - | 1.2 | |||
| (10) Eifler, J. B .[26] | - | 770 | - | - | 1.5 | |||
| (11) Beyer, J. [27] | - | - | - | 411 | 1.9 | |||
| (12) Grasso, M. [28] | - | - | - | 500 | 0.2 | |||
| (13) Cindolo, L.[29] | - | - | - | 184 | 0 | |||
| (14) Nakamura, K. [30] | - | - | - | 47 | 4 | |||
| (15)Koya, M. [31] | - | 1373 | - | - | 0.21 | |||
| (16) Cisek, L.[32] | 784 | 516 | - | - | 2.3 | |||
Table 6.
Surgical approach and VTE incidence.
| Study | VTE Incidence procedure specific |
DVT Incidence (in %) |
PE Incidence (in %) |
PLND (VTE) |
Post Op Bleeding Episodes (in %) |
|||
|---|---|---|---|---|---|---|---|---|
| O | MIS | O | MIS | O | MIS | |||
| (1) Patel, H. D. [17] | 2.4 | 1.1 | - | - | 1.7 | 1.1 | ||
| (2) Valverde-Martinez, S [18] | 2.5 | - | 1.4 | - | - | |||
| (3) Weinberg, A. [19] | 0.3 | 0.2 | - | 0.1 | 0.1 | - | - | |
| (4) Tollefson, M. K. [20] | 1.5 | 1.0 | - | 1.8 | 1.47 | - | ||
| (5) Chan, S.Y [21] | - | 0.9 | - | 0.0 | - | - | ||
| (6) Chalmers, D. J .[22] | - | 0.9 | - | - | 1.2 | - | ||
| (7) Abel, E. [23] | - | 1.8 | - | - | 0.5 | - | - | |
| (8) Dyer, J. [24] | 1.0 | - | - | - | - | |||
| (9) Van Hemelrijck, M. [25] | 1.5 | 0.8 | 0.9 | 0.6 | 0.6 | 0.2 | - | - |
| (10)Eifler, J. B. [26] | - | - | 0 | 1.5 | - | - | ||
| (11) Beyer, J. [27] | 1.9 | - | 0.9 | 0.9 | - | - | ||
| (12) Grasso, M. [28] | 0.2 | - | 0 | 0.2 | - | - | ||
| (13) Cindolo, L. [29] | 0 | - | 0 | 0 | - | - | ||
| (14) Nakamura, K. [30] | 4 | - | 0 | 4 | - | 2.1 | ||
| (15)Koya, M .[31] | 0.21 | - | 0.21 | 0 | - | - | ||
| (16) Cisek, L .[32] | 2.3 | - | 0.45 | 1.3 | - | - | ||
DVT-Deep Vein Thrombosis; MIS-Minimally Invasive Surgery; O-open surgery; PE-Pulmonary Embolism; PLND-Pelvic Lymph Node Dissection; VTE-Venous Thrombo-embolism;.
Table 7.
Summary of meta-analysis results for overall VTE occurrence.
| Outcome | Method | Number | Heterogeneity | Outcome occurrence | |
|---|---|---|---|---|---|
| Studies | p-value | I2 | % (95% CI) | ||
| VTE | All combined | 16 | <0.001 | 97% | 1.0 (0.5, 1.5) |
Table 8.
Summary of meta-analysis results for VTE occurrence based on approach and PLND.
| Comparison | Number | Heterogeneity | Group difference | ||
|---|---|---|---|---|---|
| Studies | p-value | I2 | RR (95% CI) (*) | P-value | |
| MIS / Open | 5 | 0.55 | 0% | 0.63 (0.52, 0.77) | <0.001 |
| PLND / no PLND | 2 | 0.96 | 0% | 2.79 (0.86, 8.94) | 0.09 |
(*) Relative risks expressed as per the ‘Comparison’ column.
Table 9.
Summary of meta-analysis results for VTE occurrence by Prophylaxis method.
| Prophylaxis | Number | Heterogeneity | VTE occurrence | Method diff. | |
| method | Studies | p-value | I2 | % (95% CI) | P-value |
| Mechanical | 5 | 0.002 | 76% | 0.7 (0.1, 1.6) | 0.42 |
| Combined | 6 | 0.07 | 51% | 1.0 (0.5, 1.6) | |
Table 10.
EAU guidelines for VTE prophylaxis.
| Open Radical Prostatectomy (+/- PLND) | |||
|---|---|---|---|
| Pharmacological# | Low Risk | Suggests | weak, moderate-quality evidence |
| Medium / High Risk | Recommends | strong, moderate- or high-quality evidence | |
| Mechanical* | All patients | Suggested | weak, low-quality evidence |
| Open radical prostatectomy with extended PLND | |||
| Pharmacological# | All patients | Recommends | strong, moderate, or high-quality evidence |
| Mechanical* | All patients | Suggests | weak, low-quality evidence |
| Laparoscopic Radical prostatectomy (Without PLND) | |||
| Pharmacological# | Low Risk | Recommends (Against) | strong, moderate-quality evidence |
| Medium and high risk | Suggests (Against) | weak, moderate- or high-quality evidence | |
| Mechanical* | Low risk | Suggests (Against) | weak, low-quality evidence |
| Medium and high risk | Suggests | weak, low-quality evidence | |
| Laparoscopic Radical prostatectomy (With Standard PLND) | |||
| Pharmacological# | Low Risk | Recommends (Against) | strong, moderate-quality evidence |
| Medium Risk | Suggests (Against) | weak, moderate- or high-quality evidence | |
| High Risk | Recommends | strong, high-quality evidence | |
| Mechanical* | All patients | Suggests | weak, low-quality evidence |
| Laparoscopic Radical prostatectomy (With Extended PLND) | |||
| Pharmacological# | Low Risk | Suggests (Against) | weak, moderate-quality evidence |
| Medium Risk | Suggests | weak, high-quality evidence | |
| High Risk | Recommends | strong, high-quality evidence | |
| Mechanical* | All patients | Suggested | weak, low-quality evidence |
| Robotic Radical prostatectomy (Without PLND) | |||
| Pharmacological# | Low Risk | Recommends (Against) | strong, moderate-quality evidence |
| Medium and High Risk | Suggests (Against) | weak, moderate-quality evidence | |
| Mechanical* | Low Risk | Suggests (Against) | weak, low-quality evidence |
| Medium and High Risk | Suggests | weak, low-quality evidence | |
| Robotic Radical prostatectomy (With Standard PLND) | |||
| Pharmacological# | Low Risk | Recommends (Against) | strong, moderate-quality evidence |
| Medium Risk | Suggests | weak, moderate-quality evidence | |
| High Risk | Suggests | weak, moderate-quality evidence | |
| Mechanical* | All patients | Suggests | weak, low-quality evidence |
| Robotic Radical prostatectomy (With Extended PLND) | |||
| Pharmacological# | Low Risk | Suggests (Against) | weak, moderate-quality evidence |
| Medium Risk | Suggests | weak, moderate-quality evidence | |
| High Risk | Recommends | strong, moderate-quality evidence | |
| Mechanical* | All patients | Suggests | weak, low-quality evidence |
| Pharmacological#- For 4 weeks post-operatively Mechanical*- Until ambulation | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



