
Submitted:
06 May 2023
Posted:
08 May 2023
You are already at the latest version
Abstract
Functional gastrointestinal disorders (FGIDs) are common in children and adolescents. In recent years, interest in the role of diet in the treatment of FGIDs has increased. Currently, interest focus-es on the low-FODMAP diet (LFD), the fructose- or lactose-restricted diet (FRD or LRD), the glu-ten-free diet (GFD), and the Mediterranean diet (MD). In this review, we focus on the role of these dietary patterns in the FGIDs most commonly diagnosed in clinical practice, namely irritable bowel syndrome (IBS), functional abdominal pain (FAP), functional dyspepsia (FD), and func-tional constipation (FC). Fifteen clinical trials were systematically reviewed (both RCTs and sin-gle arm clinical trials). We demonstrated the lack of high-quality intervention trials. Based on current evidence, low-FODMAP diet, LRD, FRD, or GFD have no place in daily practice for the management of children and adolescents with FGIDs. Nevertheless, some patients with IBS or RAP may have some benefit from the use of a low-FODMAP diet or FRD/LRD. Limited data sug-gest that MD may be promising in the management of FGIDs, especially in IBS patients, but more data are required to investigate the mechanisms of its protective effects.
Keywords:
Functional gastrointestinal disorders
; IBS
; dyspepsia
; constipation
; abdominal pain
; low-FODMAP diet
; fructose or lactose restricted diet
; gluten-free diet
; Mediterranean diet
1. Introduction
Functional gastrointestinal disorders (FGIDs) are common in children and adolescents [1]. Since there are not biomarkers or specific tests to diagnose FGIDs, their diagnosis is based on symptom-based criteria [2]. The Rome IV criteria [3,4] are the current criteria used to diagnose FGIDs that replaced the previous published Rome III criteria [5,6]. Depending to the criteria used, the prevalence rates vary in childhood, ranging from 9.9% to 29% [7,8,9].
With regard to the pathogenetic mechanism of FGIDs, the literature provides new aspects regarding a possibly multifactorial pathogenesis of FGIDs, although it remains elusive. A biopsychosocial (systems) model seems to better explain this notion, suggesting that early life factors may influence the clinical presentation of the disorder and clinical outcome [10]. Possible factors include genetic predisposition [11], altered gut-brain axis and gut motility [12], gut hypersensitivity [13], gut inflammation/infection [14], altered microbiome composition [15], psychological conditions [16], and environmental triggers such as food [10,17].
FGIDs are considered separate but overlapping diseases in both children and adults under the Rome criteria IV [18]. In children and adolescents, FGIDs result in a significant symptom burden [3], which is of public health concern since they are associated with functional disability, reduced quality of life, anxiety, school absenteeism, parental work absenteeism, and a notable increase in health care costs [7].
Currently available treatment options include fiber supplementation [19], probiotics [20], cognitive behavioral therapy [21], psychosocial interventions [22], fecal microbiota transplantation [23], centrally and peripherally acting neuromodulators (such as antidepressants) [24], laxatives [25], antispasmodics, and prokinetics [26]. However, in recent years, there has been renewed interest in the role of specific dietary patterns in the treatment of FGIDs. Currently, interest is focused on a low-FODMAP diet [27], a fructose or lactose restricted diet (FRD or LRD) [28], a gluten-free diet (GFD) [29] and the Mediterranean diet (MD) [30].
In the present systematic review, we provide an up-to-date overview of the efficacy of specific dietary patterns as a treatment option in ameliorating functional gastrointestinal (GI) symptoms of the most commonly diagnosed FGIDs in clinical practice, namely IBS, functional abdominal pain (FAP), functional dyspepsia (FD), and functional constipation (FC) in children and adolescents aged 3 to 18 years old.
2. Materials and Methods
A systematic literature search was performed up to 01/04/2023, using specific keywords in the databases of US National Library of Medicine (PubMed.gov) and Scopus (www.scopus.com). Two independent researchers (C.N.K and V-Μ.K.) identified all relevant publications. Studies were assessed using a hierarchical approach based on the title, abstract and finally on the full texts of the studies. The Medical Subject Heading (MeSH) keywords used were: Rome III-IV criteria, FGIDs, IBS, functional abdominal pain [recurrent abdominal pain (RAP) or continuous (CAP)], functional dyspepsia, functional constipation, Mediterranean diet, low-FODMAP diet, gluten-free diet, fructose intolerance/malabsorption, lactose intolerance/malabsorption, fructose and/or lactose restricted diet, low-fructose diet, low-lactose diet, diet, nutrition, RCT, clinical trial as well as combinations of the above terms in children or adolescents. The reference list of the retrieved articles or reviews was used to search for other relevant studies. The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [31] were followed in the present study.
2.1. Inclusion and Exclusion Criteria
Inclusion criteria: intervention studies, namely randomized (with crossover or parallel design) (RCTs) and non-randomized controlled clinical trials (non-RCTs) or single-arm trials were included. All studies were written in English assessing the effects of any of the corresponding types of diet, namely low-FODMAP diet, fructose or lactose restricted diet, GFD and MD on children and adolescents (aged 3 to 18 years old) with at least one FGIDs, i.e., IBS, FAP (RAP or CAP), FD, and FC. FGIDs diagnosis was in alignment with Rome III-IV criteria or other precise definition provided by the authors while excluding any known pre-existing GI symptoms or organic conditions.
Exclusion criteria: case-control, cross-sectional, non-human studies, case-reports, studies in adult population, editorial, commentary, abstracts, review articles or meta-analysis were excluded.
2.2. Data extraction
The assessment of all relevant studies was made through the Rayyan web tool. Data from the eligible studies were independently and blindly extracted by two investigators (C.N.K. and A.P.) in duplicates. Any disagreements we resolved after discussion between investigators. For all studies, we extracted information on inclusion and exclusion criteria, authors, journal and year of publication, methods (study design), study sample, patient population characteristics (number, age, diagnostic criteria [if available], type of FGID), intervention (type, duration of intervention, dietary dosage [if available], control (number, description), follow-up, outcomes measured, tools used to measure the outcomes of each study and study results.
2.3. Outcome Measured
The primary outcome from the included studies was the efficacy of a low-FODMAP diet, FRD or LRD, GFD and MD in improving abdominal pain (i.e., number, frequency or severity of pain or otherwise stated by the authors).
Secondary outcomes included changes in other GI symptoms (i.e. distension, gas production, vomiting, nausea), stool consistency, quality of life (QoL) and interference in daily activities.
All measurements should have been defined by authors using a validated defined measurement tool.
2.4. Study Quality
The Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I) tool [32] was used to assess the risk of bias of non-RCTs/ single arm clinical trials, based on the following domains: 1) bias due to confounding, 2) bias in selection of participants into the study, 3) bias in classification of interventions, 4) bias due to deviations from intended interventions, 5) bias due to missing data, 6) bias in measurement of the outcome, 7) bias in selection of the reported results. The overall judgement of the quality of non-randomized clinical trials was based on the worst level of bias that each study received for a particular domain [33].
For RCTs, the Cochrane Risk of Bias Tool (ROB2) [34] was used to assess their quality, based on the following criteria: 1) bias due to randomization process, 2) bias due to deviations from indented interventions, 3) bias due to missing data, 4) bias in measurement of the outcome, 5) bias in selection of the reported results. For RCTs with crossover design, the ROB2 for crossover trials was used [35].
The overall bias of the included studies was categorized as “low risk of bias” if all domains of the study were at low risk, “some concerns” if at least one domain of some concerns existed for this result but with not at high risk domains and “high risk of bias” if at least one domain of the study was at high risk or multiple domains raise some concerns [34,35].
3. Results
In total, 84 full-text studies were assessed for eligibility. Of those, 15 clinical trials met the inclusion and exclusion criteria and were selected for the present systematic review. In specific, 6 studies evaluated the efficacy of a low-FODMAP diet [36,37,38,39,40,41,42], 5 the efficacy of FRD/LRD [28,43,44,45,46], 3 trials the efficacy of the GFD [47,48,49] and 1 the efficacy of the MD [50]. The flowchart is shown in Figure 1.
With regard to the quality of the eligible studies (i.e., nonRCTs/single arm clinical trials, RCTs with a crossover design and other RCTs) are shown in the supplementary material, Figures S1–S3, accordingly. Based on the tools used, 3/15 studies showed “low” risk of bias, 8/15 showed moderate risk (i.e., raised “some concerns” in one or multiple domains), while 4/15 characterized as with “serious” risk of bias.
3.1. Low-FODMAP diet
The low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) diet is a widely accepted approach for the management of IBS in adults [51], recommended also by the American College of Gastroenterology [52,53]. The main dietary sources of FODMAPs include certain fruit, vegetables, legumes and artificial sweeteners [51]. The symptoms in some patients are mainly generated through a) the unabsorbed fructose, polyols and lactose that increase small intestinal water content and thus the intestinal motility and b) the indigestible fructans and galacto-oligosaccharides that undergo rapid microbial fermentation causing increased gas production, flatulence and abdominal distension [54].
Although, numerous pooled data highlight the efficacy of this diet for the management of symptoms adult patients with FGIDs [51,55,56], current data in pediatrics are insufficient showing conflicting results [57].
In total, 6 relevant studies were found in pediatrics; 3 studies evaluated the efficacy of a low-FODMAP diet on GI outcomes in IBS patients [36,37,38] and 3 studies assessed its role on FAP or FC or FD [39,40,42]. Four studies were RCTs [36,38,40,42] and 2 studies were non-randomized clinical trials [37,39]. FGIDs diagnosis was based on Rome III criteria in 4 studies [36,37,39,40] and in Rome IV in 2 studies [38,42]. Only two studies reported the exact amount of FODMAPs given to the study participants [36,38]; that was 0.15 g/kg/day (maximum 9 g/day) [36] or 0.5g/per meal [38], accordingly. The duration of intervention varied from 48h to 2 months.
With regard to our primary outcomes (i.e., improvements in number, frequency or severity of abdominal pain), the effect of a low-FODMAP diet on abdominal pain intensity was reported in 5 included trials [36,37,38,39,40], pain frequency in 2 studies [37,40] and number of abdominal pain episodes in 2 studies [36,39]. A positive effect of a low-FODMAP diet on the primary outcomes was found in 4/5 trials [36,37,38,39] but only 2 trials [36,38] made between group comparisons, whereas no effect was reported in 1 trial [40]. In terms of secondary outcomes, no effects of the low-FODMAP were observed on stool consistence. GI symptoms were reported in 4 trials [37,38,39,42] using various tools, of which half reported significant effects [38,39] and half no effects of the low-FODMAP diet on GI symptoms [37,42] compared to baseline or the control group. One study [39] reported less interference with daily activities after following a low-FODMAP diet compared to baseline values. Health-related quality of life, was not reported in any study. The reported adherence to the low-FODMAP diet across the studies was 80% to 100%. The main characteristics of the studies are shown in Table 1.
Specifically, in a small open-label pilot study [37], researchers evaluated the effects of a low-FODMAP diet in 8 children with IBS. Pain frequency, pain severity, and pain-related interference with activities decreased significantly in all children while on the low-FODMAP diet compared to baseline. However, four children (50%), defined as responders, showed a more robust response to the diet (>50% decrease in abdominal pain frequency while on a low-FODMAP diet) [37]. In a double-blind, crossover randomized controlled trial (RCT) [36] conducted by the same research group, 33 children with IBS randomly assigned to either a low-FODMAP diet or a typical American childhood diet for 48h, with a 5-day washout period between the intervention diets. Researchers demonstrated a lower number of abdominal pain episodes in children on a low-FODMAP diet compared to children on the typical American childhood diet and baseline. Both the pilot and the RCT studies suggested that baseline gut microbiome composition and microbial metabolic capacity may play a role in responsiveness to the diet. Responders in the RCT had a baseline microbiome composition enriched with taxa (such as Bacteroides, Ruminococcaceae, Faecalibacterium prausnitzii and Dorea) known for their greater saccharolytic metabolic capacity compared to non-responders, who were uniquely enriched at baseline with the Turicibacter genus from the Turicibacteraceae family.
In another RCT [38], 60 children with IBS were randomly divided into two groups to follow either a low FODMAP diet or a standard gastrointestinal tract protective diet (i.e., defined as a diet to provide age-appropriate protein, calorie, vitamin and mineral intake) for 2 months. Children were also reassessed for their symptoms and clinical status 2 months after the discontinuation of the intervention (4 months from baseline). Abdominal pain was evaluated using the Visual Analogue Scale (VAS), while the clinical status of each patient was assessed by their doctor using the Clinical Global Impression Improvement (CGI-I) scale. After intervention, both VAS and GGI-I improved significantly in the low-FODMAP group compared to the control group. However, 2 months after the discontinuation of the intervention, both VAS and GGI-I were worse in the low-FODMAP diet compared to the control group, suggesting that benefits from the adherence to a low-FODMAP does not sustain in the long term in children with IBS.
As far as FAP is concerned, a double-blind RCT evaluated the effectiveness of the low-FODMAP diet in improving GI symptoms in 27 children with FAP diagnosed using Rome III criteria [40]. Patients were allocated to a low-FODMAP diet or a control diet based on the National Institute for Health and Care Excellence (NICE) guidelines for 4 weeks. At the end of the study, there were no between groups significant changes in the abdominal pain intensity and frequency as well as in stool frequency and consistency.
Only a tendency toward these improvements was observed within the low-FODMAP group. Of note, significant reduction of symptoms as well as in stool consistency were observed within the NICE group throughout the consecutive weeks of the diet. Contrary to what has been previously reported among children with IBS, researchers suggested that differences in pathophysiological mechanisms underlying these entities (e.g. presence of visceral hypersensitivity in IBS but not in FAP) could explain the non-effectiveness of the low-FODMAP diet in patients with FAP. However, among the limitations of the study, was also the small sample size in the low-FODMAP group that resulted in low statistical power in this group.
The efficacy of a low-FODMAP diet and GI outcomes in children with various FAPDs (FAP, IBS, or FD) have been also explored in an open-label prospective study [39]. Although patients were analyzed as a united group without a control group, researchers reported improvements in abdominal pain episodes, abdominal pain intensity and GI symptoms as well as interference with daily activities, after 2 weeks of the dietary intervention. Moreover, 13/20 reported substantial adherence, 6/20 a good adherence and 1/10 fair adherence to the low-FODMAP diet.
The effectiveness of a low-FODMAP diet on GI symptoms has been also evaluated in children with autism spectrum disorders (ASD) who have FC and/or abdominal pain [42]. Through a pilot single-site RCT [42], researchers concluded that a low-FODMAP diet for 2 weeks was effective in reducing not only the rates of constipation but other GI problems too (such as stomach pain and hurt, gas and bloating, stomach discomfort when eating, nausea and vomiting, and diarrhea) in children with ASD compared to habitual diet. However, these improvements in GI symptoms did not connect to behavioral improvements in the participants. Of note, the low-FODMAP diet did not impact the nutrient intake of children’s diet, although the dietary adequacy at baseline was insufficient due to the related food selectivity, picky eating, and sensory problems commonly found in such population.
Overall, the studies assessing the effects of a low-FODMAP diet with on the number, frequency or severity of abdominal pain or other GI symptoms in children with FGIDs are insufficient to support any therapeutic recommendations. Evidence is of low quality, due to small sample sizes with a few studies being RCTs, whereas the tools used to assess GI outcomes varied across studies, which limits the uniform evaluation of the published results. Nevertheless, concerning specific FGIDs, a low-FODMAP diet may offer some benefit in selected children with IBS.
3.2. Fructose restricted diet
Fructose and lactose malabsorption are considered as possible causes of recurrent abdominal pain (RAP) [45]. Lactose malabsorption (LM) is a frequent clinical condition caused by lactase-reduced activity (i.e., hypolactasia). The undigested lactose is fermented by the colonic flora, causing digestive symptoms. Fructose malabsorption (FM) is caused by the insufficient absorption and subsequent bacterial fermentation of fructose in the intestinal lumen [58].
Worldwide prevalence of LM is estimated to be 68% with varied rates across the countries[59]. Yet, only a small percentage of people seems to be lactose intolerant (LI) [60]. The same is true for FM, as only a small percentage of children and adults present with symptoms after fructose ingestion (fructose intolerance, FI). Symptoms that usually caused after lactose or fructose ingestion include flatulence, diarrhea, abdominal pain and abdominal distension, symptoms similar to patients with FGIDs [61]. The likelihood of developing symptoms after fructose or lactose ingestion is multifactorial and seems to depend on the lactose/fructose dose, lactase expression and the intestinal microbiome [60]. Hydrogen breath tests (HBTs), remain the most popular diagnostic method for assessing these conditions [62], although with often false-negative results in children [61]. Nevertheless, it has been found that children with visceral hypersensitivity associated with IBS and FAP may have LI/FI [63,64]. Consequently, in clinical practice, a FRD or a LRD are being proposed as less restrictive diets for the management of FGIDs, given that a low-FODMAP diet could compromise the nutritional adequacy and lead to poor eating behaviors in children [65].
In total, 5 studies were included in the present analysis; 3 evaluated the role of a FRD [28,43,44], 1 the role of a LRD [46], whereas 1 assessed the role of both FRD and LRD [45] in improving GI outcomes in patients with FGIDs. Three studies [28,43,45] included children with RAP, 1 study [44] enrolled patients with chronic abdominal pain and 1 study [46] was on IBS patients. Two studies were uncontrolled clinical trials [43,44] two RCTs [28,46] and one was randomized placebo-controlled trial [45]. The latter [45] was the only study that reported the exact amount (i.e., 25g of fructose and lactose with 2g of glucose) allowed at the FRD and LRD trials. The duration of intervention varied from 2 weeks to 6 months.
With regard to our primary outcomes, abdominal pain severity was reported in 3 studies [28,43,46], whereas pain frequency was reported in 2 studies [28,43]. No studies were found evaluating the number of abdominal pain episodes. A positive effect of a FRD on primary outcomes was found in 2 trials [28,43] compared to baseline, whereas a positive effect of the LRD on primary outcomes was shown in 1 study [46] compared to the control group. With regard to secondary outcomes, stool frequency and missed school days per week were reported in 1 study [43], in which a positive effect of a FRD was reported compared to baseline values. GI symptoms improvements after following a FRD were found in 2 studies [43,44] compared to baseline values, whereas results from the randomized placebo-controlled trial [45] showed no effect of either a FRD or LRD on GI symptoms. The adherence to the FRD/LFD across the studies was underreported, but based on provided data an adherence >80% was noted. The characteristics of the studies are shown in Table 2.
In a single arm clinical trial [43], 75 children with RAP for more than 3 months and positive fructose-HBTs received a FRD for 4 weeks. The FRD group received a detailed dietary advice with a list of allowed and not allowed foods and an option to call dietitian in case of questions (no exact fructose dosage reported). At the end of the study, pain frequency per week (1 vs. 4, p<0.001) and the intensity of pain (3 vs. 6, p < 0.001) as expressed by median changes reduced compared to baseline. Daily stool frequency, nausea, problems to fall asleep, missed school days also improved significantly (all p<0.05).
The same research team, 2 years later, conducted a two-site prospective blinded RCT [28]. 116 children with RAP for more than 3 months and a positive fructose-HBTs were placed to either a FRD or a regular diet (RD) for 2 weeks. What was new in this study, apart from the control group, was that children with positive fructose-HBTs within the FRD group, continued the FRD for 2 additional weeks at the end of the initial intervention (4 weeks from baseline). All subjects in the FRD group were advised to reduce fructose intake through a dietitian-led counselling. No exact dosage of fructose reported by authors. Abdominal pain intensity, changes in pain frequency and a secondary symptom score (SSS) assessing life quality parameters were evaluated through appropriate questionnaires. Unfortunately, no between groups comparisons were provided by the authors. At the end of 2 weeks, abdominal pain intensity was reduced within the FRD group (p<0.001) compared to baseline. Interestingly, in both children with positive and negative fructose-HBTs abdominal pain improved within this group at 4 weeks. No changes were observed in the RD group. Both groups reduced pain frequency (74% vs. 57 %) compared to baseline. SSS also improved from 6 to 3.5 (p<0.002) in the FRD group, with children with negative fructose-HBTs showing significant improvement in SSS (p<0.004) compared to baseline. No statistical changes were found within the control group in the SSS.
Similarly, Escobar et al [44], carried out a single arm clinical trial which aimed to assess the role of a FRD in resolving GI symptoms of children with chronic abdominal pain. 121 patients with positive fructose-HBTs received a FRD for 2 months. At the end of the study, 93/121 patients (76.9%) reported resolution of GI symptoms with FRD (P<0.0001). However, 55/101 patients (54.4%) with negative F-BHT also reported resolution of symptoms without a FRD, although the results did not reach significance (p=0.37).
In contrast to previously reported studies, Gijsbers et al [45] failed to prove any causal relationship between resolution of GI symptoms and FRD or LRD after conducting a randomized double-blind placebo-controlled trial [45]. Initially, 210 children with RAP were investigated for LM/LI or FM/FI. 57 (27%) were found to have positive lactose-HBT and 79 (65%), positive fructose-HBT. After assessing all patients through an elimination phase followed by an open provocation phase, 6 children with LM/LI and 8 children with FM/FI were eligible for a randomized double-blind placebo-controlled trial in order to assess the role of a FRD or LRD on resolving GI symptoms in patients with RAP. At the end of the study, all patients in both groups tested negative, although GI symptoms continued. Patients showed improvements in their symptoms only in the elimination phase of the study.
With regard to LI/LM, Gremse et al [46], conducted a double-blind crossover RCT in children with IBS and positive lactose-HBTs aiming to prove a causal association between lactose ingestion and GI symptoms. 33 patients received either 240mL of lactose-hydrolyzed milk or lactose-containing milk along with LRD for 2 weeks. At the end of the study, abdominal pain decreased in the intervention compared to the control group (4.1±1.4 vs. 7.5±2.7, p=0.021). Nevertheless, although 23/30 reported more symptoms within the control group, there were 7/30 who reported less or no symptoms, although compliant with the non-restricted diet.
Overall, the effective role of FRD or LRD on GI outcomes of children and adolescents with FGIDs (mainly in patients with RAP and IBS) is not clear. The coexistence and clinical importance of LI/LM or FI/FM in children with FGIDs remains unanswered. Current data depend on uncontrolled clinical trials or RCTs using separate paired tests against baseline which possibly cause misleading conclusions [66]. Some patients with RAP or IBS may benefit from dietary fructose or lactose restriction but the degree of the restriction or the amount of fructose or lactose that is allowed to be consumed without causing GI discomfort, is poorly defined. Therefore, more data are required to draw strict conclusion on the beneficial effects (if any) of FRD or LRD in children and adolescents with FGIDs.
3.3. Gluten Free diet
Lately, there has been renewed interest in the role of gluten sensitivity as a potential trigger of GI symptoms in adults with IBS [67,68]. There are some RCTs [69,70] suggesting that adult patients with IBS may have intestinal (e.g. bloating and abdominal pain) and extra-intestinal symptoms (e.g. headache, anxiety, fibromyalgia-like syndrome and skin rash) subsequent to the ingestion, despite the lack of celiac disease or wheat allergy [71,72]. This clinical condition is known as non-celiac gluten or wheat sensitivity (NCGS), although the term NCGS remain debatable as it is unclear if gluten is the only wheat component to cause development of the GI symptoms [73]. NCGS may be present in children with an estimated prevalence to be under 6%, although the true prevalence is difficult to determine [74]. This is because no specific diagnostic markers for NCGS or a standardized diagnostic procedure exist and therefore, the NCGS diagnosis usually requires observed double-blind, placebo- controlled provocation testing [75].
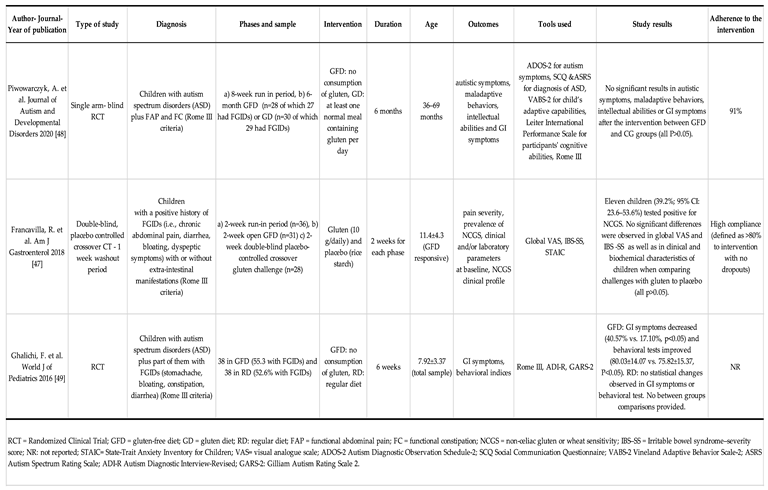
Currently, 3 trials have been published investigating the effects of the GFD on FGIDs in the pediatric population [47,48,49]. Two studies were RCTs [48,49] and 1 was a double-blind placebo controlled clinical trial [47]. Two studies [44,47] assessed the role of GFD on GI outcomes in children with several FGIDs and 1 study [48] on children with FAP/FC. The duration of intervention varied from 48h to 2 months.
Only 1 study evaluated the changes in the abdominal pain severity after following a GFD compared to placebo (10g of gluten challenge), showing no effects. Regarding our secondary outcomes, no effects of the GFD on GI symptoms were noticed in 2 studies compared to controls [47,48], whereas significant effects were noticed in 1 study compared to baseline values [49]. No reports were made regarding stool consistency or QoL. The reported adherence to the GFD was 80-91%. The main characteristics of the studies are shown in Table 3.
In a randomized double-blind placebo-controlled crossover trial [47], researchers screened 1,114 children with chronic functional GI symptoms (i.e., chronic abdominal pain, diarrhea, bloating, dyspeptic symptoms diagnosed based on Rome III criteria) with or without extra-intestinal manifestations. 1,078 (96.7%) did not present any correlation of symptoms with gluten ingestion and excluded. The remaining 36 children followed a 3-phase trial a) run-in phase - 2 weeks of exposure to a gluten-containing diet for baseline evaluation - in which 5 children presented with an improvement of symptoms (global VAS<3) and excluded; b) an open GFD phase - 2 weeks of gluten elimination in which 31 continued, 3 did not respond and excluded from the next phase and; c) a placebo-controlled crossover trial after 1 week of washout from the GFD in which 28 children entered. Based on the Salerno criteria (global VAS variation >30% between the gluten and the placebo challenge groups), 11 children (39.2%; 95% CI: 23.6–53.6%) tested positive, suggesting that 1 in 100 who were referred for chronic GI symptoms had NCGS. However, no differences were observed in global VAS and IBS severity scores as well as in clinical and biochemical characteristics of children when comparing challenges with gluten to placebo.
The GFD (and/or casein-free diet) has been also tested in children with ASD as a possible therapeutic approach based on the hypothesis that the elimination of the peptides derived from the metabolism of gluten and casein may ameliorate behavioral and GI symptoms in this population [48].
In a RCT [49] 80 children with ASD were randomly subdivided into a GFD or a regular diet (RD) for 6 weeks. 38 children in each group completed the study. At baseline, 55.3% of the GFD group and 52.6% of the RD group had GI symptoms (e.g. stomachache, bloating, constipation, diarrhea) as diagnosed using Rome III criteria. At the end of the study, the prevalence of GI symptoms decreased significantly (40.57% vs. 17.10%, p<0.05) within the GFD group, but no statistical changes observed within the RD group (42.45% vs. 44.05%, p>0.05). Behavioral improvements were also noticed within the GFD group (80.03±14.07 vs. 75.82±15.37, P<0.05) but not in the RD group (79.92±15.49 vs. 80.92±16.24, p>0.05). Unfortunately, researchers did not publish any between group comparisons.
In contrast to the previous published study, in a single-blinded RCT [48], Piwowarczyk et al aimed to determine whether a GFD compared to a gluten-containing diet (GD) could influence autistic symptoms, maladaptive behaviors, intellectual abilities and GI symptoms in children with ASD. Only abdominal pain and constipation were reported by the participants based on Rome III criteria. After 8 weeks of an run-in GFD period, the GFD group continued this diet and the GD group consumed at least one normal meal containing gluten per day for 6 months. Overall, researchers did not reveal any significant differences in autistic symptoms, maladaptive behaviors, intellectual abilities or GI symptoms after the intervention between the GFD and CG groups.
Overall, intervention data on the role of GFD for the treatment of FGIDs in paediatrics are scarce. Current evidence from intervention studies do not support the use of the GFD for the treatment of patients with FGIDs. More RCTs are needed to explore the effectiveness (if any) of GFD in selected children with FGIDs.
3.4. Mediterranean diet
The MD is primarily a plant-based dietary pattern characterized by high consumption of whole grains, fruits, vegetables, legumes, nuts and seeds, moderate amounts of dairy products and fish, red meat and meat products are consumed in low quantities, while olive oil represents the main source of fat [76]. A robust evidence, based on meta-analyses of epidemiological studies and RCTs have proven the beneficial role of the greater adherence to the MD to a reduced risk of overall mortality, cardiovascular diseases, cancer incidence, neurodegenerative diseases, obesity and diabetes [77]. The underlying mechanisms mediating the health benefits of the MD in health are attributable to the high intake of several bioactive compounds found in the MD, such as fiber, polyphenols, flavonoids, monounsaturated and polyunsaturated fatty acids [78].
With regard to FGIDs, data coming mainly from epidemiological studies in adults [79,80] support that the higher adherence to the MD is associated with a lower prevalence and less odds of having FGIDs compared to low adherence. This further suggests that MD could play a preventive role in the development of GI symptoms in those patients. However, limited evidence exist on the association between the MD and FGIDs in pediatrics [30]. Two epidemiological studies [9,65] have explored this association along with the recently published results from our research team [9]. These studies confirmed what is already known from the adult population; good adherence to the MD is associated with a significant lower prevalence of FGIDs in both children and adolescents.
Clinical trials evaluating the efficacy of the MD in children and adolescents with FGIDs are lacking. Only 1 relevant open-label RCT [50] was found in the present review. Researchers subdivided 100 patients with IBS (diagnosed based on Rome IV criteria) into a MD group (with a good adherence to the MD, difined as KIDMED score ≥ 8 points), or a regular diet for 6 months. A 100-scale VAS total score was used to evaluate IBS symptoms, the IBS-symptoms-severity-score questionnaire (IBS-SSS) to assess the severity of IBS symptoms and the IBS-QoL questionnaire (IBS-QoL) to evaluate patients’ QoL. MD was well-tolerated by the patients without any adverse events. At the end of study, within the MD group, the IBS-SSS and IBS-QoL scores improved compared to baseline, with no statistical changes in the regular diet group. Comparisons between groups at the end of study also showed that IBS patients in the MD group compared to the regular diet group had less total score on IBS symptoms (P<0.001), fewer IBS-SSS (p<0.001) and higher IBS-QoL scores (p=0.03) [50].
Overall, the MD seems to be promising as a therapeutic approach in patients with FGIDs and especially for patients with IBS. Although results come literally from one RCT, the MD seems to be a well-known and tolerated dietary pattern without causing any adverse events in patients. However, future well-designed clinical trials are needed to verify current data.
4. Discussion
4.1. Summary of the primary and secontary outcomes
In the present study, we systematically reviewed 15 clinical trials (both RCTs and non-randomized single arm clinical trials) to determine the efficacy of specific dietary patterns (i.e., a low-FODMAP diet [36,37,38,39,40,41,42], a FRD or LRD [28,43,44,45,46], a gluten-free diet [47,48,49] and the Mediterranean diet [50]), as a therapeutic option for children with FGIDs. We concluded that no high-quality intervention trials exist as the current evidence according to the tools (i.e., ROB2 and ROBINS-I) used to assess the risk of bias, was low (raise some concerns) to very low (serious concerns).
Bearing in mind these limitations, we found that there is insufficient evidence to support the use of a low-FODMAP diet or a FRD/LRD in children and adolescents with FGIDs. However, these dietary plans may offer some benefit in alleviating abdominal pain in some children with IBS or RAP. Moreover, the GFD should not be recommended for improving abdominal pain in children and adolescents in FGIDs as current studies show no effects. The MD seems to be promising as a therapeutic approach in patients with IBS, although results come literally from one intervention study. Overall, current evidence does not offer a robust background to draw firm recommendations on specific dietary patterns that children and adolescents with FGIDs could follow in order to improve their symptoms or other GI outcomes. Future well-designed intervention studies are needed before transferring any of the available data into clinical practice.
With regard to secondary outcomes, no effects of the low-FODMAP were shown on stool consistence in children with FGIDs. However, Chumpitazi et al [36,37], suggested that baseline gut microbiome composition and microbial metabolic capacity may play a role in responsiveness to the diet. Less interference with daily activities were also found while children were on a low-FODMAP diet. Mixed results were reported in term of the efficacy of the FRD in improving GI and stool consistency in children with FGIDs. Moreover, results from RCTs showed no effect of the GFD on GI symptoms, although improvements were seen when compared to baseline values. Finally, a positive effect of the MD was reported on IBS symptoms and QoL in patients with IBS compared to controls.
4.2. Literature documention
In accordance to the present study, one previous relevant systematic review of RCTs [81] concluded that there are several methodological limitations of the available clinical trials on the efficacy of using a low-FODMAP for the treatment of children with FGIDs. Researchers concluded that the choice of the comparator diet (usually a non-standardized treatment for children with FGIDs compared to a placebo diet that is considered the gold standard method), as well as other domains (e.g. the success of blinding after follow-up, the carry over effects in crossover studies, the optimal duration of intervention) were with a high risk of bias [81].
In the present study, assessing the role not only of a low-FODMAP diet, but other dietary patterns too in children with FGIDs, the current evidence was found to be low to very low [e.g. only 2 randomized double-blind placebo-controlled trial were found (one on GFD and one on FRD); a regular diet as a control diet was used only in 4 of the included controlled studies [28,42,49,50]; 2/3 crossover RCTs had “some concerns” arising from period and carry over effects]. Furthermore, only 5 of the eligible studies [38,40,43,44,49] was in agreement with the recommendations published by the Rome Foundation for the appropriate intervention period (i.e., 4 weeks and preferably 6 weeks or more) when conducting a clinical trial in such patients. Most studies had rather too short (≤ 2weeks) or too long (i.e., 6 months) intervention periods which could further limit the address of the indented outcomes.
Currently, most of the available reviews in the literature assessing the efficacy of dietary interventions in patients with FGIDs, have focused on the role of the low-FODMAP diet [57,82,83] or the use of dietary supplements e.g. fiber [84], probiotics, prebiotics or synbiotics [85,86,87], vitamin D supplementation [71] or they are not focused in pediatrics per se [88,89]. Although not in the purposes of the present review, fiber supplementation has been found to have a positive effect in the management of FGIDs in children [84], although for specific FGIDs (e.g. FC), their use is not recommended [90]. Nevertheless, most frequent dietary recommendations given in children and adolescents with FGIDs in tertiary care or primary care are the use of fiber supplementation and a low-FODMAP diet [91]. Given that improvements in diet are considered as a first line approach for the management of several diseases [92,93], there is a need of better justification of the dietary patterns that could be used in FGIDs in pediatrics.
In consistency with the present review, the position paper published in 2022 by the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) [57], suggested that there is insufficient evidence to recommend the use of the low-FODMAP diet for the treatment of FGIDs in children, apart from some patients with IBS. Currently, a FRD or a LRD are being proposed in clinical practice as less restrictive diets [48], but as showed by the present study, only some RAP or IBS patients may benefit from fructose restriction. Nevertheless, a major problem of the studies assessing the effects of a low-FODMAP diet or a FRD/FLD diet in patients with FGIDs is that the degree of the restriction or the exact amount of FODMAPs/fructose/lactose that is allowed to be consumed without causing GI discomfort, is poorly defined. In the present review, only two studies reported the FODMAP content of the diet used; 0.15g/Kg/day (maximum 9g/day) or less than 0.5g/meal. In adults, differing FODMAP content has been tested depending the diet used; that is 7.6g/day, 15.2g/day and 22.4g/day for a low-FODMAP Diet, traditional dietary advice and GFD respectively. A suggested threshold for symptom improvements in adults is of 12 g FODMAPs/day [29]. However, this has yet to be confirmed in pediatrics. Accordingly, in the only double blind placebo control diet evaluating a FRD/FLD in children with FGIDs, 25g of either fructose or lactose was given, but several children continued to report abdominal symptoms upon fructose or lactose provocation.
We found no evidence of positive effects of GFD for the management of children with FGIDs. Currently, a strict gluten-free diet is a life-long necessity only for the treatment of patients with celiac disease [94]. Whether children and adolescents with IBS and NCGS could benefit from gluten elimination is not known. In one double blind placebo controlled study [47] in children with various FGIDs (included in the present review), gluten challenge with 10g did not result in any GI improvements compared to placebo. However, gluten/placebo challenges in adults have shown mixed results [95]. For example, worst GI symptoms have been reported in adult patients with IBS and NCGS who blindly exposed to gluten (68%), compared to the placebo group (40%) [96]. However, in another study after a 2-week assignment to a low-FODMAP diet, different doses of gluten challenge (low: 2g/d vs. high:16g/d) did not cause any differences in GI symptoms in adult patients with IBS and NCGS [97].
We found little evidence for MD being effective for the treatment of FGIDs in children and adolescents. Although data come from one trial, two epidemiological studies in pediatrics [9,98] have explored this association showing promising results. A cross-sectional study [9] conducted by our research team included 1972 children aged 4 to 9 years old and 2450 subjects aged 10 to 18 years old from six Mediterranean countries (i.e., Croatia, Greece, Israel, Italy, North Macedonia, and Serbia). The study aimed to reveal any associations between participants’ FODMAPS intake or adherence to the MD. Higher compliance to the MD (as assessed by KIDMED score) was associated with lower odds of having FGIDs. In specific, each one unit increase in the KIDMED score was associated with 17% less possibility of having FGIDs in children aged 4 to 9 years old and 7% in children aged 10 to 18 years old [9]. A significant association was also found between the MD and FC as well as postprandial distress syndrome in both age groups. However, this was not the case with the FODMAP diet, as no significant associations were found between FGIDs and FODMAPs, in both age groups. Agakidis et al, [98], through a prospective cohort study of 1116 children and adolescents, also showed similar associations. For each one unit increase in the KIDMED score there was 8.9% less likelihood of having FGIDs after adjusting for age.
Overall, as evident in the literature, the prescription of a specific dietary pattern in children (as in adults) should involve a specialized pediatric dietitian in order to explain and supervise the adherence to the diet, a parameter that could also affect the potential outcomes of a study [57,99]. Nevertheless, in clinical practice of children and adolescents with FGIDs provided with dietary recommendations, only 20% seems to receive an educational consult by a dietitian [91]. In this systematic review, most studies reported the involvement of a dietitian, with the researchers suggesting a substantial to good adherence (i.e., more than 80%) to most dietary patterns [36,38,39,40,43,47], although a subsequent number of studies did not report any data [28,42,44,46]. Indeed, in a recent literature review [100] assessing the adherence rates to dietary interventions in FGIDs patients, the reported range of adherence was 30%-100% but only one study in pediatrics was included and data were mainly derived from studies implementing a low-FODMAP diet.
4.3. Strengths and limitations
This systematic review has some limitations and some important strengths. The limitations of the present study are mostly associated to the low and very low quality of the studies included (most studies were characterized as having “some concerns” or “serious concerns”). Indeed, in order to increase the number of relevant studies identified (so that to improve the reliability of the study outcomes), we included non-randomized, single arm clinical trials which are generally considered intrinsically unsuited to demonstrate the benefit of a new treatment without the presence of a control group. We tried to address these issues by using up to date tools (i.e., Cochrane ROB2 and ROBINS-I) for assessing the risk of bias in the included studies. However, in some sections (e.g. MD) only one study was reported due to limited available data. Moreover, only three out of fifteen studies used the latest published criteria for the diagnosis of FGIDs, i.e., ROME IV criteria (most of trials used the ROME III criteria) and this is something that should be taken into consideration when interpreting the current study findings. Therefore, more future well-designed intervention studies are needed to overcome all these limitations.
The most important strength of the present study is that the methodology used was based on the high-quality standards of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) whereas for the agreement of study selections, clearly designated steps based on the Rayyan tool were used.
5. Conclusions
In the present study, we systematically reviewed 15 clinical trials (both RCTs, non-RCTs and single arm clinical trials) to determine the efficacy of specific dietary patterns (i.e., a low-FODMAP diet, a FRD or LRD, a GFD and the MD), as therapeutic options for children with FGIDs. We demonstrated the lack of high-quality intervention trials. Based on the current evidence low-FODMAP diet, LRD, FRD or GFD do not have a place in the daily practice for the management of children and adolescents with FGIDs. Nevertheless, some patients with IBS or RAP may have some benefit from the use of a low-FODMAP diet or a FRD/LRD. Limited data suggest that MD may be promising in treating FGIDs, especially in IBS patients, but more data are required to draw conclusions on its protective effects.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Risk of bias of the eligible non-RCTs/single arm clinical trials using the Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I). Figure S2: Risk of bias of the eligible RCTs with crossover design using the Cochrane Risk of Bias Tool (ROB-2) tool for crossover. trials, Figure S3: Risk of bias of the eligible RCTs using the Cochrane Risk of Bias Tool (ROB-2).
Author Contributions
“Conceptualization, C.N.K.; methodology, C.N.K; investigation, C.N.K; writing—original draft preparation, C.N.K.; writing—review and editing, CNK, VΜK and AP; supervision, A.P. All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”.
Institutional Review Board Statement
The present study did not require ethical approval.
Conflicts of Interest
“The authors declare no conflict of interest.”
References
- Lewis, M.L.; Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A. Prevalence of functional gastrointestinal disorders in children and adolescents. The Journal of pediatrics 2016, 177, 39–43.e33. [Google Scholar] [CrossRef] [PubMed]
- Baaleman, D.F.; Di Lorenzo, C.; Benninga, M.A.; Saps, M. The Effects of the Rome IV Criteria on Pediatric Gastrointestinal Practice. Current Gastroenterology Reports 2020, 22, 21. [Google Scholar] [CrossRef] [PubMed]
- Robin, S.G.; Keller, C.; Zwiener, R.; Hyman, P.E.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Shulman, R.J.; Hyams, J.S.; Palsson, O. Prevalence of pediatric functional gastrointestinal disorders utilizing the Rome IV criteria. The Journal of pediatrics 2018, 195, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology 2016, 150, 1456–1468.e1452. [Google Scholar] [CrossRef]
- Hyman, P.E.; Milla, P.J.; Benninga, M.A.; Davidson, G.P.; Fleisher, D.F.; Taminiau, J. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology 2006, 130, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef]
- Vernon-Roberts, A.; Alexander, I.; Day, A.S. Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Boronat, A.C.; Ferreira-Maia, A.P.; Matijasevich, A.; Wang, Y.-P. Epidemiology of functional gastrointestinal disorders in children and adolescents: a systematic review. World Journal of Gastroenterology 2017, 23, 3915. [Google Scholar] [CrossRef]
- Strisciuglio, C.; Cenni, S.; Serra, M.R.; Dolce, P.; Kolacek, S.; Sila, S.; Trivic, I.; Bar Lev, M.R.; Shamir, R.; Kostovski, A. , et al. Diet and Pediatric Functional Gastrointestinal Disorders in Mediterranean Countries. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef]
- Camilleri, M.; Carlson, P.; McKinzie, S.; Zucchelli, M.; D'Amato, M.; Busciglio, I.; Burton, D.; Zinsmeister, A.R. Genetic susceptibility to inflammation and colonic transit in lower functional gastrointestinal disorders: preliminary analysis. Neurogastroenterol Motil 2011, 23, 935–e398. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A.; Ryu, H.J.; Bhatt, R.R. The neurobiology of irritable bowel syndrome. Mol Psychiatry 2023. [Google Scholar] [CrossRef] [PubMed]
- Azpiroz, F.; Bouin, M.; Camilleri, M.; Mayer, E.A.; Poitras, P.; Serra, J.; Spiller, R.C. Mechanisms of hypersensitivity in IBS and functional disorders. Neurogastroenterol Motil 2007, 19, 62–88. [Google Scholar] [CrossRef]
- Burns, G.L.; Hoedt, E.C.; Walker, M.M.; Talley, N.J.; Keely, S. Physiological mechanisms of unexplained (functional) gastrointestinal disorders. The Journal of Physiology 2021, 599, 5141–5161. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.; Collins, S.M.; Bercik, P. The microbiota-gut-brain axis in functional gastrointestinal disorders. Gut Microbes 2014, 5, 419–429. [Google Scholar] [CrossRef]
- Koloski, N.; Holtmann, G.; Talley, N.J. Is there a causal link between psychological disorders and functional gastrointestinal disorders? Expert Rev Gastroenterol Hepatol 2020, 14, 1047–1059. [Google Scholar] [CrossRef] [PubMed]
- Defrees, D.N.; Bailey, J. Irritable bowel syndrome: epidemiology, pathophysiology, diagnosis, and treatment. Primary Care: Clinics in Office Practice 2017, 44, 655–671. [Google Scholar] [CrossRef]
- Velasco-Benítez, C.A.; Gómez-Oliveros, L.F.; Rubio-Molina, L.M.; Tovar-Cuevas, J.R.; Saps, M. Diagnostic Accuracy of the Rome IV Criteria for the Diagnosis of Functional Gastrointestinal Disorders in Children. Journal of Pediatric Gastroenterology and Nutrition 2021, 72. [Google Scholar] [CrossRef]
- Horvath, A.; Dziechciarz, P.; Szajewska, H. Systematic review of randomized controlled trials: fiber supplements for abdominal pain-related functional gastrointestinal disorders in childhood. Ann Nutr Metab 2012, 61, 95–101. [Google Scholar] [CrossRef]
- Capozza, M.; Laforgia, N.; Rizzo, V.; Salvatore, S.; Guandalini, S.; Baldassarre, M. Probiotics and Functional Gastrointestinal Disorders in Pediatric Age: A Narrative Review. Front Pediatr 2022, 10, 805466. [Google Scholar] [CrossRef]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468. [Google Scholar] [CrossRef]
- Palermo, T.M. Pain prevention and management must begin in childhood: the key role of psychological interventions. Pain 2020, 161, S114. [Google Scholar] [CrossRef] [PubMed]
- Pinn, D.; Aroniadis, O.; Brandt, L. Is fecal microbiota transplantation (FMT) an effective treatment for patients with functional gastrointestinal disorders (FGID)? Neurogastroenterology & Motility 2015, 27, 19–29. [Google Scholar]
- Bonilla, S.; Nurko, S. Focus on the use of antidepressants to treat pediatric functional abdominal pain: current perspectives. Clinical and experimental gastroenterology 2018, 365–372. [Google Scholar] [CrossRef]
- Korterink, J.J.; Rutten, J.M.; Venmans, L.; Benninga, M.A.; Tabbers, M.M. Pharmacologic treatment in pediatric functional abdominal pain disorders: a systematic review. The Journal of pediatrics 2015, 166, 424–431.e426. [Google Scholar] [CrossRef]
- Singh, R.; Zogg, H.; Ghoshal, U.C.; Ro, S. Current Treatment Options and Therapeutic Insights for Gastrointestinal Dysmotility and Functional Gastrointestinal Disorders. Front Pharmacol 2022, 13, 808195. [Google Scholar] [CrossRef] [PubMed]
- Tuck, C.J.; Reed, D.E.; Muir, J.G.; Vanner, S.J. Implementation of the low FODMAP diet in functional gastrointestinal symptoms: A real-world experience. Neurogastroenterol Motil 2020, 32, e13730. [Google Scholar] [CrossRef] [PubMed]
- Wirth, S.; Klodt, C.; Wintermeyer, P.; Berrang, J.; Hensel, K.; Langer, T.; Heusch, A. Positive or negative fructose breath test results do not predict response to fructose restricted diet in children with recurrent abdominal pain: results from a prospective randomized trial. Klinische Pädiatrie 2014, 226, 268–273. [Google Scholar] [CrossRef]
- Rej, A.; Avery, A.; Aziz, I.; Black, C.J.; Bowyer, R.K.; Buckle, R.L.; Seamark, L.; Shaw, C.C.; Thompson, J.; Trott, N. , et al. Diet and irritable bowel syndrome: an update from a UK consensus meeting. BMC Medicine 2022, 20, 287. [Google Scholar] [CrossRef]
- Cenni, S.; Sesenna, V.; Boiardi, G.; Casertano, M.; Di Nardo, G.; Esposito, S.; Strisciuglio, C. The Mediterranean Diet in Paediatric Gastrointestinal Disorders. Nutrients 2023, 15, 79. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Annals of internal medicine 2009, 151, W-65–W-94. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. bmj 2016, 355. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P. Assessing risk of bias in a non-randomized study. Cochrane handbook for systematic reviews of interventions 2019, 621–641. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: a revised tool for assessing risk of bias in randomised trials. bmj 2019, 366. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Li, T.; Sterne, J. Revised Cochrane risk of bias tool for randomized trials (RoB 2): Additional considerations for crossover trials. Cochrane Methods 2021, 1–6. [Google Scholar]
- Chumpitazi, B.P.; Cope, J.L.; Hollister, E.B.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Versalovic, J.; Shulman, R.J. Randomised clinical trial: gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with the irritable bowel syndrome. Alimentary pharmacology & therapeutics 2015, 42, 418–427. [Google Scholar]
- Chumpitazi, B.P.; Hollister, E.B.; Oezguen, N.; Tsai, C.M.; McMeans, A.R.; Luna, R.A.; Savidge, T.C.; Versalovic, J.; Shulman, R.J. Gut microbiota influences low fermentable substrate diet efficacy in children with irritable bowel syndrome. Gut microbes 2014, 5, 165–175. [Google Scholar] [CrossRef]
- Dogan, G.; Yavuz, S.; Aslantas, H.; Ozyurt, B.; Kasirga, E. Is low FODMAP diet effective in children with irritable bowel syndrome? Northern clinics of Istanbul 2020, 7. [Google Scholar]
- Baranguan Castro, M.L.; Ros Arnal, I.; Garcia Romero, R.; Rodriguez Martinez, G.; Ubalde Sainz, E. [Implementation of a low FODMAP diet for functional abdominal pain]. An Pediatr (Engl Ed) 2019, 90, 180–186. [Google Scholar] [CrossRef]
- Boradyn, K.M.; Przybyłowicz, K.E.; Jarocka-Cyrta, E. Low FODMAP diet is not effective in children with functional abdominal pain: a randomized controlled trial. Annals of Nutrition and Metabolism 2020, 76, 334–344. [Google Scholar] [CrossRef]
- Cyrkot, S.; Marcon, M.; Brill, H.; Mileski, H.; Dowhaniuk, J.; Frankish, A.; Carroll, M.W.; Persad, R.; Turner, J.M.; Mager, D.R. FODMAP intake in children with coeliac disease influences diet quality and health-related quality of life and has no impact on gastrointestinal symptoms. International Journal of Food Sciences and Nutrition 2021, 72, 956–967. [Google Scholar] [CrossRef]
- Nogay, N.H.; Walton, J.; Roberts, K.M.; Nahikian-Nelms, M.; Witwer, A.N. The effect of the low FODMAP diet on gastrointestinal symptoms, behavioral problems and nutrient intake in children with autism spectrum disorder: A randomized controlled pilot trial. Journal of Autism and Developmental Disorders 2021, 51, 2800–2811. [Google Scholar] [CrossRef] [PubMed]
- Wintermeyer, P.; Baur, M.; Pilic, D.; Schmidt-Choudhury, A.; Zilbauer, M.; Wirth, S. Fructose malabsorption in children with recurrent abdominal pain: positive effects of dietary treatment. Klin Padiatr 2012, 224, 17–21. [Google Scholar] [CrossRef]
- Escobar Jr, M.A.; Lustig, D.; Pflugeisen, B.M.; Amoroso, P.J.; Sherif, D.; Saeed, R.; Shamdeen, S.; Tuider, J.; Abdullah, B. Fructose intolerance/malabsorption and recurrent abdominal pain in children. Journal of pediatric gastroenterology and nutrition 2014, 58, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Gijsbers, C.F.; Kneepkens, C.M.; Buller, H.A. Lactose and fructose malabsorption in children with recurrent abdominal pain: results of double-blinded testing. Acta Paediatr 2012, 101, e411–e415. [Google Scholar] [CrossRef] [PubMed]
- Gremse, D.A.; Greer, A.S.; Vacik, J.; Dipalma, J.A. Abdominal Pain Associated with Lactose Ingestion in Children with Lactose Intolerance. Clinical Pediatrics 2003, 42, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Francavilla, R.; Cristofori, F.; Verzillo, L.; Gentile, A.; Castellaneta, S.; Polloni, C.; Giorgio, V.; Verduci, E.; D'angelo, E.; Dellatte, S. Randomized double-blind placebo-controlled crossover trial for the diagnosis of non-celiac gluten sensitivity in children. Official journal of the American College of Gastroenterology| ACG 2018, 113, 421–430. [Google Scholar] [CrossRef]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-free diet in children with autism spectrum disorders: a randomized, controlled, single-blinded trial. Journal of Autism and Developmental Disorders 2020, 50, 482–490. [Google Scholar] [CrossRef]
- Ghalichi, F.; Ghaemmaghami, J.; Malek, A.; Ostadrahimi, A. Effect of gluten free diet on gastrointestinal and behavioral indices for children with autism spectrum disorders: a randomized clinical trial. World J Pediatr 2016, 12, 436–442. [Google Scholar] [CrossRef]
- Al-Biltagi, M.; El Amrousy, D.; El Ashry, H.; Maher, S.; Mohammed, M.A.; Hasan, S. Effects of adherence to the Mediterranean diet in children and adolescents with irritable bowel syndrome. World J Clin Pediatr 2022, 11, 330–340. [Google Scholar] [CrossRef]
- Black, C.J.; Staudacher, H.M.; Ford, A.C. Efficacy of a low FODMAP diet in irritable bowel syndrome: systematic review and network meta-analysis. Gut 2022, 71, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Moayyedi, P.; Lacy, B.E.; Lembo, A.J.; Saito, Y.A.; Schiller, L.R.; Soffer, E.E.; Spiegel, B.M.; Quigley, E.M. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Official journal of the American College of Gastroenterology| ACG 2014, 109, S2–S26. [Google Scholar] [CrossRef]
- Moayyedi, P.; Marsiglio, M.; Andrews, C.N.; Graff, L.A.; Korownyk, C.; Kvern, B.; Lazarescu, A.; Liu, L.; MacQueen, G.; Paterson, W.G. Patient engagement and multidisciplinary involvement has an impact on clinical Guideline development and decisions: a comparison of two irritable bowel syndrome guidelines using the same data. Journal of the Canadian Association of Gastroenterology 2019, 2, 30–36. [Google Scholar] [CrossRef]
- Mullin, G.E.; Shepherd, S.J.; Chander Roland, B.; Ireton-Jones, C.; Matarese, L.E. Irritable bowel syndrome: contemporary nutrition management strategies. Journal of parenteral and enteral nutrition 2014, 38, 781–799. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75.e65. [Google Scholar] [CrossRef] [PubMed]
- van Lanen, A.-S.; de Bree, A.; Greyling, A. Efficacy of a low-FODMAP diet in adult irritable bowel syndrome: a systematic review and meta-analysis. European journal of nutrition 2021, 60, 3505–3522. [Google Scholar] [CrossRef] [PubMed]
- Thomassen, R.; Luque, V.; Assa, A.; Borrelli, O.; Broekaert, I.; Dolinsek, J.; Martin-de-Carpi, J.; Mas, E.; Miele, E.; Norsa, L. An ESPGHAN Position Paper on the Use of Low-FODMAP Diet in Pediatric Gastroenterology. Journal of Pediatric Gastroenterology and Nutrition 2022, 75, 356–368. [Google Scholar] [CrossRef]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and methane-based breath testing in gastrointestinal disorders: the North American Consensus. The American journal of gastroenterology 2017, 112, 775. [Google Scholar] [CrossRef]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2017, 2, 738–746. [Google Scholar] [CrossRef]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef]
- Kwiecień, J.; Hajzler, W.; Kosek, K.; Balcerowicz, S.; Grzanka, D.; Gościniak, W.; Górowska-Kowolik, K. No Correlation between Positive Fructose Hydrogen Breath Test and Clinical Symptoms in Children with Functional Gastrointestinal Disorders: A Retrospective Single-Centre Study. Nutrients 2021, 13, 2891. [Google Scholar] [CrossRef]
- Gibson, P.R.; Newnham, E.; Barrett, J.S.; Shepherd, S.J.; Muir, J.G. Review article: fructose malabsorption and the bigger picture. Aliment Pharmacol Ther 2007, 25, 349–363. [Google Scholar] [CrossRef]
- Lozinsky, A.C.; Boé, C.; Palmero, R.; Fagundes-Neto, U. Fructose malabsorption in children with functional digestive disorders. Arq Gastroenterol 2013, 50, 226–230. [Google Scholar] [CrossRef]
- Pawłowska, K.; Umławska, W.; Iwańczak, B. Prevalence of Lactose Malabsorption and Lactose Intolerance in Pediatric Patients with Selected Gastrointestinal Diseases. Adv Clin Exp Med 2015, 24, 863–871. [Google Scholar] [CrossRef]
- Pensabene, L.; Salvatore, S.; Turco, R.; Tarsitano, F.; Concolino, D.; Baldassarre, M.E.; Borrelli, O.; Thapar, N.; Vandenplas, Y.; Staiano, A. Low FODMAPs diet for functional abdominal pain disorders in children: critical review of current knowledge. Jornal de pediatria 2019, 95, 642–656. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Comparisons against baseline within randomised groups are often used and can be highly misleading. Trials 2011, 12, 264. [Google Scholar] [CrossRef]
- Volta, U.; Pinto-Sanchez, M.I.; Boschetti, E.; Caio, G.; De Giorgio, R.; Verdu, E.F. Dietary Triggers in Irritable Bowel Syndrome: Is There a Role for Gluten? J Neurogastroenterol Motil 2016, 22, 547–557. [Google Scholar] [CrossRef]
- Koumbi, L.; Giouleme, O.; Vassilopoulou, E. Non-Celiac Gluten Sensitivity and Irritable Bowel Disease: Looking for the Culprits. Current Developments in Nutrition 2020, 4. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: a double-blind randomized placebo-controlled trial. Official journal of the American College of Gastroenterology| ACG 2011, 106, 508–514. [Google Scholar] [CrossRef]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D'alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: exploring a new clinical entity. Official journal of the American College of Gastroenterology| ACG 2012, 107, 1898–1906. [Google Scholar] [CrossRef]
- de Bruijn, C.M.; Rexwinkel, R.; Gordon, M.; Sinopoulou, V.; Benninga, M.A.; Tabbers, M.M. Dietary interventions for functional abdominal pain disorders in children: a systematic review and meta-analysis. Expert Review of Gastroenterology & Hepatology 2022, 16, 359–371. [Google Scholar]
- Barbaro, M.R.; Cremon, C.; Wrona, D.; Fuschi, D.; Marasco, G.; Stanghellini, V.; Barbara, G. Non-Celiac Gluten Sensitivity in the Context of Functional Gastrointestinal Disorders. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Devulapalli, C.S. Gluten-free diet in children: a fad or necessity? Archives of Disease in Childhood 2021, 106, 628–629. [Google Scholar] [CrossRef]
- Devulapalli, C.S. Non-coeliac gluten sensitivity in children. Tidsskr Nor Laegeforen 2020, 140. [Google Scholar] [CrossRef]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J. , et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts' Criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: a cultural model for healthy eating. The American journal of clinical nutrition 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. European Journal of Clinical Nutrition 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. British journal of pharmacology 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Zito, F.P.; Polese, B.; Vozzella, L.; Gala, A.; Genovese, D.; Verlezza, V.; Medugno, F.; Santini, A.; Barrea, L.; Cargiolli, M. Good adherence to mediterranean diet can prevent gastrointestinal symptoms: A survey from Southern Italy. World journal of gastrointestinal pharmacology and therapeutics 2016, 7, 564. [Google Scholar] [CrossRef]
- Elmaliklis, I.-N.; Liveri, A.; Ntelis, B.; Paraskeva, K.; Goulis, I.; Koutelidakis, A.E. Increased functional foods’ consumption and Mediterranean diet adherence may have a protective effect in the appearance of gastrointestinal diseases: a case–control study. Medicines 2019, 6, 50. [Google Scholar] [CrossRef]
- Stróżyk, A.; Horvath, A.; Szajewska, H. FODMAP dietary restrictions in the management of children with functional abdominal pain disorders: A systematic review. Neurogastroenterology & Motility 2022, 34, e14345. [Google Scholar]
- Brown, S.C.; Whelan, K.; Gearry, R.B.; Day, A.S. Low FODMAP diet in children and adolescents with functional bowel disorder: A clinical case note review. JGH Open 2020, 4, 153–159. [Google Scholar] [CrossRef]
- Turco, R.; Salvatore, S.; Miele, E.; Romano, C.; Marseglia, G.L.; Staiano, A. Does a low FODMAPs diet reduce symptoms of functional abdominal pain disorders? A systematic review in adult and paediatric population, on behalf of Italian Society of Pediatrics. Italian Journal of Pediatrics 2018, 44, 53. [Google Scholar] [CrossRef]
- Axelrod, C.H.; Saps, M. The Role of Fiber in the Treatment of Functional Gastrointestinal Disorders in Children. Nutrients 2018, 10, 1650. [Google Scholar] [CrossRef]
- Pärtty, A.; Rautava, S.; Kalliomäki, M. Probiotics on Pediatric Functional Gastrointestinal Disorders. Nutrients 2018, 10, 1836. [Google Scholar] [CrossRef]
- Korterink, J.J.; Ockeloen, L.; Benninga, M.A.; Tabbers, M.M.; Hilbink, M.; Deckers-Kocken, J.M. Probiotics for childhood functional gastrointestinal disorders: a systematic review and meta-analysis. Acta Paediatrica 2014, 103, 365–372. [Google Scholar] [CrossRef]
- Hojsak, I.; Kolaček, S.; Mihatsch, W.; Mosca, A.; Shamir, R.; Szajewska, H.; Vandenplas, Y.; van den Akker, C.H.; Berni Canani, R.; Dinleyici, E.C. Synbiotics in the Management of Pediatric Gastrointestinal Disorders: Position Paper of the ESPGHAN Special Interest Group on Gut Microbiota and Modifications. Journal of Pediatric Gastroenterology and Nutrition 2023, 76, 102–108. [Google Scholar] [CrossRef]
- Scarpato, E.; Auricchio, R.; Penagini, F.; Campanozzi, A.; Zuccotti, G.V.; Troncone, R. Efficacy of the gluten free diet in the management of functional gastrointestinal disorders: a systematic review on behalf of the Italian Society of Paediatrics. Italian Journal of Pediatrics 2019, 45, 9. [Google Scholar] [CrossRef]
- Axelrod, C.H.; Saps, M. Global Dietary Patterns and Functional Gastrointestinal Disorders. Children (Basel) 2020, 7. [Google Scholar] [CrossRef]
- Tabbers, M.; DiLorenzo, C.; Berger, M.; Faure, C.; Langendam, M.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. Journal of pediatric gastroenterology and nutrition 2014, 58, 258–274. [Google Scholar] [CrossRef]
- Alfaro Cruz, L.; Minard, C.; Guffey, D.; Chumpitazi, B.P.; Shulman, R.J. Does a Minority of Children With Functional Gastrointestinal Disorders Receive Formal Diet Advice? Journal of Parenteral and Enteral Nutrition 2020, 44, 1525–1529. [Google Scholar] [CrossRef]
- López-Gil, J.F.; García-Hermoso, A.; Sotos-Prieto, M.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; Kales, S.N. Mediterranean diet-based interventions to improve anthropometric and obesity indicators in children and adolescents: a systematic review with meta-analysis of randomized controlled trials. Advances in Nutrition 2023. [Google Scholar] [CrossRef] [PubMed]
- Bouhanick, B.; Sosner, P.; Brochard, K.; Mounier-Véhier, C.; Plu-Bureau, G.; Hascoet, S.; Ranchin, B.; Pietrement, C.; Martinerie, L.; Boivin, J.M. , et al. Hypertension in Children and Adolescents: A Position Statement From a Panel of Multidisciplinary Experts Coordinated by the French Society of Hypertension. Frontiers in Pediatrics 2021, 9. [Google Scholar] [CrossRef]
- Mearin, M.L.; Agardh, D.; Antunes, H.; Al-Toma, A.; Auricchio, R.; Castillejo, G.; Catassi, C.; Ciacci, C.; Discepolo, V.; Dolinsek, J. , et al. ESPGHAN Position Paper on Management and Follow-up of Children and Adolescents With Celiac Disease. J Pediatr Gastroenterol Nutr 2022, 75, 369–386. [Google Scholar] [CrossRef]
- Llanos-Chea, A.; Fasano, A. Gluten and Functional Abdominal Pain Disorders in Children. Nutrients 2018, 10, 1491. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten Causes Gastrointestinal Symptoms in Subjects Without Celiac Disease: A Double-Blind Randomized Placebo-Controlled Trial. Official journal of the American College of Gastroenterology | ACG 2011, 106, 508–514. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No Effects of Gluten in Patients With Self-Reported Non-Celiac Gluten Sensitivity After Dietary Reduction of Fermentable, Poorly Absorbed, Short-Chain Carbohydrates. Gastroenterology 2013, 145, 320–328.e323. [Google Scholar] [CrossRef] [PubMed]
- Agakidis, C.; Kotzakioulafi, E.; Petridis, D.; Apostolidou, K.; Karagiozoglou-Lampoudi, T. Mediterranean Diet Adherence is Associated with Lower Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Howatson, A.; Wall, C.; Turner-Benny, P. The contribution of dietitians to the primary health care workforce. Journal of Primary Health Care 2015, 7, 324–332. [Google Scholar] [CrossRef]
- Alfaro-Cruz, L.; Heitkemper, M.; Chumpitazi, B.P.; Shulman, R.J. Literature review: dietary intervention adherence and adherence barriers in functional gastrointestinal disorder studies. Journal of Clinical Gastroenterology 2020, 54, 203–211. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the.systematic review based on PRISMA guidelines.
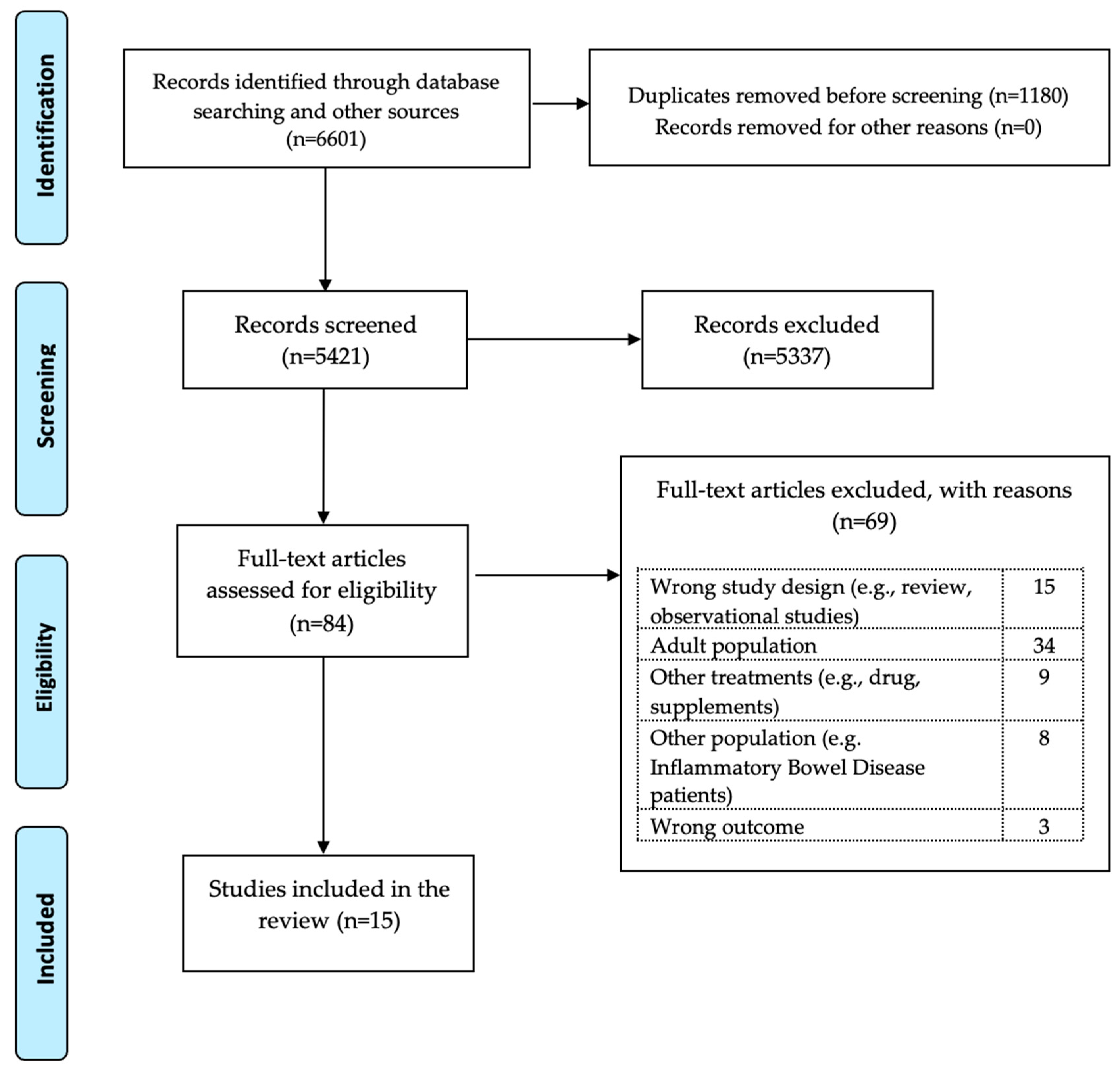

Table 1.
Characteristics of the studies assessing the role of a low-FODMAP diet for the treatment of FGIDs in children and adolescents.
Table 1.
Characteristics of the studies assessing the role of a low-FODMAP diet for the treatment of FGIDs in children and adolescents.
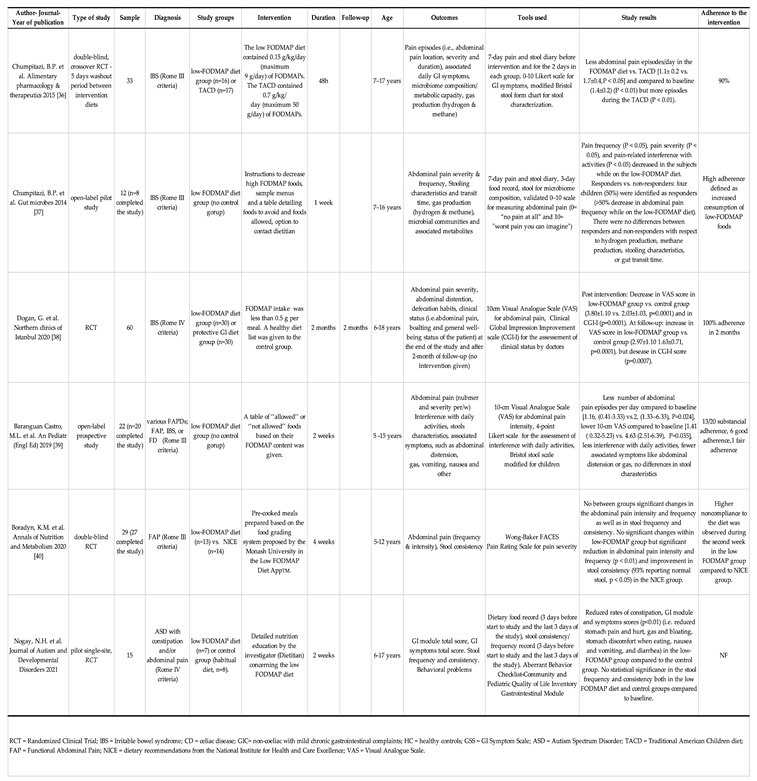
Table 2.
Characteristics of the studies assessing the efficacy of a fructose or lactose restricted diet for the treatment of FGIDs in children.
Table 2.
Characteristics of the studies assessing the efficacy of a fructose or lactose restricted diet for the treatment of FGIDs in children.
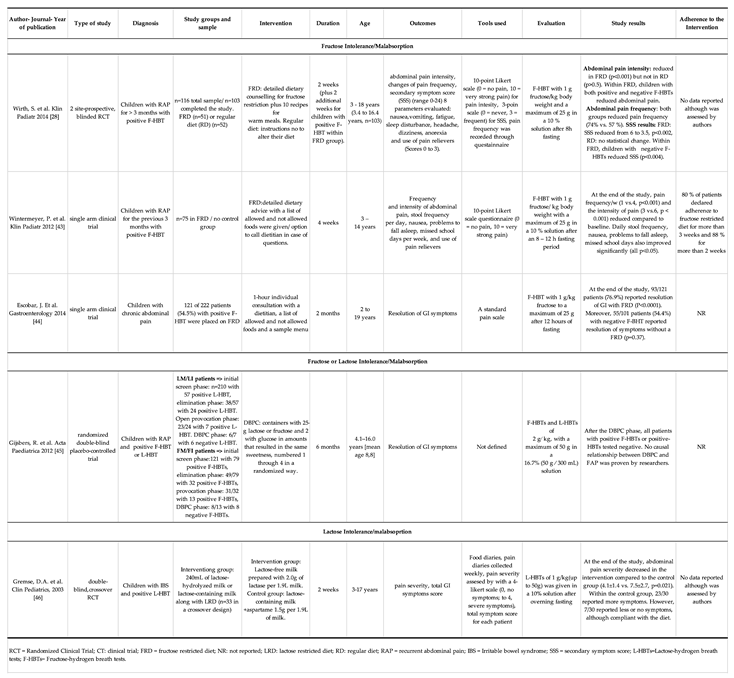
Table 3.
Characteristics of the studies assessing the efficacy of the GFD for the treatment of FGIDs in children.
Table 3.
Characteristics of the studies assessing the efficacy of the GFD for the treatment of FGIDs in children.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



