
Submitted:
28 April 2023
Posted:
28 April 2023
You are already at the latest version
Abstract
Renal cell carcinoma (RCC) is the second most common cancer of the urinary system. The current therapeutic strategies are based on partial or total nephrectomy and/or targeted therapies based on immune checkpoint inhibitors to which patients are often refractory. Preventive and screening strategies are not existing and the few available biomarkers for RCC are characterized by the lack of sensitivity, outlining the need of novel noninvasive and sensitive biomarkers for an early diag-nosis and a better disease monitoring. Blood liquid biopsy (LB) is a non- or minimally invasive procedure for a more representative view of tumor heterogeneity than the tissue biopsy, poten-tially allowing real-time monitoring of cancer evolution. Growing interest is focused on the extra-cellular vesicles (EVs) secreted by either healthy or tumoral cells and recovered in a variety of bio-logical matrices, blood included. EVs are involved in cell-to-cell crosstalk transferring their mRNAs, miRNAs, and proteins content. In particular, transferred miRNAs may regulate the tu-morigenesis and proliferation also impacting on resistance to apoptosis, thus representing poten-tial useful biomarkers. Here we present the latest efforts in the identification of circulating miR-NAs in blood samples, focusing on the potential use of EV derived miRNAs as RCC diagnostic, prognostic markers.
Keywords:
renal cell carcinoma
; liquid biopsy
; blood
; extracellular vesicles
; microRNA
; biomarker
; diagnostics
; prognosis
; prediction
1. Renal Cell Carcinoma: clinical diagnosis and staging
Renal cell carcinoma (RCC) is the second most frequent cancer in the urological system [1] and represents about 3% of all tumors affecting adults in western world [2]. Every year 64,000 new RCC cases are diagnosed and 14,000 mortality cases due to this malignancy are registered in the United States (US), projecting to increase in burden worldwide [3]. RCC early diagnosis is critical to reduce mortality rate, however the disease is characterized by an asymptomatic clinical course with most cases accidentally diagnosed during clinical evaluations for other concomitant pathologies [2]. Nevertheless, some clinical signs could be related with RCC, such as polycythemia, hypercalcemia, hypertension and Cushing’s syndrome, respectively correlated to erythropoietin, parathyroid-related hormone, renin and ACTH over-production by cancer. Furthermore, leukocytosis, fever and weight loss are common symptoms, while only about 10% of cases show the “classic triad” of RCC symptomatology, consisting of flank pain, hematuria, and palpable masses [4].
The incidence of the disease varies widely throughout the world and appears to be highest in more developed countries. White people have a lower risk of RCC than Native, African and Hispanic Americans probably due to the disparities in diets, lifestyles, socioeconomic conditions, education, and economical possibility for healthcare. Risk factors connected to RCC could be distinguished in (a) unmodifiable such as age, race and gender and (b) modifiable that include diet, alcohol, occupational exposure and drugs [4]. Peak incidence is mostly around sixty and eighty, when the average is 64 years in the US [3].
Unmodifiable and modifiable risk factors are often related: RCC is doubly diagnosed in men where some modifiable risks such as hypertension, tobacco smoking and obesity are more frequently observed.
RCC originates from kidney cortex, in particular from the epithelial cells of renal tubular [3,4] and is commonly classified into three main histopathological subtypes: (1) clear cell renal cell carcinoma (ccRCC) represents the 75% of all RCC cases and the 90% of all RCC deaths due to tendency to metastasize [2]; it derives from renal cancer progenitors, namely RCC cancer stem cells (CSCs) and it is often associated with distant disease to bones, liver and lung through hematologic way [4]; (2) around 10% of diagnosis consists in papillary renal cell carcinoma (pRCC) characterized by histological sub-classification in type I and II, where the first has a tropism for lymphatic recurrence; (3) chromophobe renal cell carcinoma (chRCC) is the less aggressive subtype and represents the 5% of all RCC [4]. The RCC stage at diagnosis is an important prognostic factor. Indeed, for organ-confined tumors (stage I) over the 90% of individuals survive at 5 years from onset, while the survival percentage is reduced to 72,5% for regional disease (stage II/III). Unfortunately, about 30% of RCC are diagnosed at metastatic disease (stage IV) where the prognosis is poor with a 5-year survival rate of 12% [4].
2. RCC treatments: advances and challenges in the lack of biomarkers
RCC is a chemo- and radio-resistant neoplasia. The current therapeutic strategies are based on the surgical approach of radical and/or partial nephrectomy that remain the only effective therapy for clinically localized RCC [5]. Traditionally, these tumors have been treated aggressively, most often with radical nephrectomy, however it predisposes patients to chronic kidney disease with attendant cardiovascular risks and increased mortality [6]. Nephron-sparing approaches such as partial nephrectomy, thermal ablation and active surveillance have also emerged as viable options for the management of these patients [7]. Treatment options are thus individualized and related to disease features (above all tumor stage, size and grade) [2,4,8], weighing the risks and benefits of partial versus radical nephrectomy. Nevertheless, RCC is characterized by a high rate of relapse and unfortunately about 20-50% of those treated with curative intent will progress to stage IV. Features related to a worse prognosis are the tumor size (>7cm), the tumor necrosis, a fat invasion, the performance status (KPS < 80) together with nodal metastases and age [4]. The lack of sensitivity to chemotherapy and radiation therapy prompted efforts into novel treatment options. In the last few years, the therapeutic approach for metastatic RCC (mRCC) in the first-line setting is radically changed due to novel combinatory approaches impacting on both immunity and intracellular molecular pathways inhibition.
Those approaches are targeting the peculiar hyper-vascularity of RCC and trigger the immune cell infiltration by immune checkpoint inhibitors, with or without anti-angiogenic tyrosine kinase inhibitor (TKI)-based combinations [9]. Thus, the current standard of care for frontline advanced ccRCC includes an “immuno-oncology” (IO) combination that may include a vascular endothelial growth factor (VEGF) inhibitor with a checkpoint inhibitor (VEGF-IO) or of two checkpoint inhibitors together (IO-IO) that showed efficacy and safety [10,11]. Interestingly, the anti-angiogenic TKI in RCC are given without actionable mutations to screen. They are oral drugs able to block angiogenesis pathway by binding VEGF receptor, c-MET, RET. For RCC, TKIs can be distinguished in three generations drugs, according to spectrum of action and side effects: sunitinib, pazopanib and sorafenib (first-generation); axitinib and tivozanib (second-generation) and cabozantinib (third-generation) [12].
ICIs can stimulate the host immune response against cancer, through PD1 inhibitors (Nivolumab and Pembrolizumab) or anti-CTLA4 inhibitors (Ipilimumab). The first group can block the interaction PD1/PD-L1 able to downregulate the host T cells and therefore the immune response [11]. Many studies investigated the role of PD-L1 expression as a biomarker, such as Iacovelli et al [13] who performed a meta-analysis of six studies on 1323 patients, showing a high level of PD-L1 expression associated with a higher risk of death. Indeed, PD-L1 expression may be considered as a negative prognostic factor in RCC [14].
However, the response and tolerance to these combination treatments are not always satisfying, probably due to the lack of recognized molecular targets, an intra-tumoral heterogeneity and different RCC molecular subtypes.
The therapeutic strategy is based on the clinical prognostic score (IMDC, MSKK criteria), drug toxicities, patients’ comorbidities, and preference. In fact, nowadays the International mRCC Database Consortium risk model remains the only prospectively known predictive biomarker in mRCC [15].
Although targeted therapies represent the standard treatment options for RCC, nearly all patients treated with targeted drugs will eventually experience disease progression. Unfortunately, a significant number of RCC patients are primarily refractory to targeted therapeutics, showing neither disease stabilization nor clinical benefits, probably due to the intra-tumoral heterogeneity and molecular subtypes [15,16].
Therefore, the identification of new promising biomarkers in RCC is an urgent clinical need that leads clinicians and researchers to investigate the role of cell components as microRNAs secreted by tumor cells and packaged into extracellular vesicles (EVs) released in biological fluids [17].
3. Liquid biopsy in RCC
For decades, surgical tissue-biopsy has firmly been considered the gold standard for solid tumor diagnosis, however it may become a diagnostic obstacle for its invasiveness, unrepeatability and especially for its peculiarity to immortalize that moment without taking into account the tumor heterogeneity and dynamism [18]. The molecular tumor pattern can dynamically evolve over time, driven by microenvironmental stimuli and clonal selection under treatment pressure, rendering future therapeutic decisions based on tissue biopsy suboptimal [19,20].
Over the past decade, liquid biopsy (LB) revolutionized the field of clinical oncology, providing the ease in tumor sampling and continuous tumor monitoring [21].
Thus, LB is gaining relevance in the clinical scenario in cancer for early detection and treatment stratification, as well as residual disease and recurrence monitoring [20].
In particular, overall survival in mRCC patients remains low despite the development of novel targeted therapeutic approaches. LBs could provide an attractive and non-invasive method to determine the risk of recurrence or metastatic dissemination during follow-up and thus improve clinical outcomes and quality of life of RCC patients [22]. Several biological body fluids, such as blood, urine, saliva, breast milk and other patient samples, can be collected and used for clinical investigations, as they contain numerous biomarkers. Peripheral blood, as well as other biological fluids, can be a source of cancer material, such as circulating tumor cells (CTCs), circulating tumor DNA (ctDNA) and tumor-derived EVs [23] (Figure 1).
The identification of biomarkers in LB could enable continuous and real-time collection of RCC patients’ information for diagnosis, prognosis assessment, treatment monitoring and response evaluation [24].
Many studies have attempted to use LB as a routine method for the clinical diagnosis of RCC and for the prediction of patients’ grades, stages, and survival to identify high-risk patients for metastasis and recurrence [25,26,27,28,29]. In particular, in recent decades most efforts have been spent in analyzing CTCs and ctDNA [30,31], however their low level in the blood makes their capture and analysis very difficult [24].
EVs and miRNAs are emerging as a platform with potentially broader and complementary applications in LB [32].
4. Extracellular vesicles: biogenesis and role in RCC
EVs are small lipid bilayer-enclosed vesicles, released continuously by all viable cells, in physiological and pathological conditions [33]. According to ISEV guidelines, the term EVs includes three different subtypes of vesicles based on their biogenesis and size [34]: (a) exosomes have a diameter of 30-150 nm and originate by the fusion between intracytoplasmic multi-vesicular bodies (MVB) and cellular plasma membrane; (b) microvesicles with a size of 100-1000 nm generate directly from the plasma membrane by budding process; (c) apoptotic bodies are larger than 1000 nm and are released by dying cells [35] (Figure 2). A list of minimal information for studies of EVs was provided from MISEV-2014 [36] and updated in MISEV-2018 [35] pointing out EVs separation/isolation and characterization techniques and functional studies.
EVs can transport tumor-derived material, including lipids, a wide variety of RNA (microRNAs, mRNAs and long non coding-RNAs), DNA, proteins, enzymes and metabolites. They play a key role in cell-to-cell communication [37] by transferring their information to nearby or long distance recipient cells, influencing their phenotype and functions [38].
These small messengers are involved in tumorigenesis and tumor metastasis due to their widespread distribution throughout the blood and lymphatic circulation. Several studies indicate that tumor released EVs may orchestrate tumor progression stimulating proliferation, angiogenesis, chemo-resistance and immune-escape [19,39,40]. In addition, EVs are highly stable in biological fluids and protect their content from RNase and protease activity thanks to their lipid bilayer structure [41].
Recently, EVs showed an increasing interest in the field of urological malignancies [42]. A growing number of studies are focusing on EV cargoes, particularly miRNAs, in relation to diagnostic accuracy, treatment prognosis, treatment response as well as numerous biological processes [43,44].
The recent knowledge is related to the biological role of EVs shed by RCC tumor cells in RCC progression, such as angiogenesis, immune escape and tumor growth [45].
Horie K et al analyzed the hypoxic conditions in RCC that stimulate the release of tumor cells-derived EVs. Their results suggested the possibility that carbonic anhydrase 9 (CA9) enriched in exosomes and released from hypoxic RCC may enhance angiogenesis in microenvironment, thereby contributing to cancer progression [46]. In addition, RCC-EVs were studied for their modulation of vascular permeability affecting metastatization, thanks to their enrichment in the azurocidin protein (AZU1) significantly higher in serum EVs from ccRCC patients compared to those from healthy donors [47].
More, specific pro-tumorigenic roles have been attributed to EVs released by CD105+ renal CSCs, due to their cargo enriched in several pro-angiogenic mRNAs and miRNAs [48]. Those cargos can also impact other tumor microenvironmental cells, as demonstrated by Lindoso et al, considering the participation of renal CSC-derived EVs in the interaction between tumor and stroma. They found that CSC-derived EVs promoted phenotypical changes in stromal cells characterized by an increased expression of genes associated with cell migration, matrix remodeling, angiogenesis and tumor growth [49]. Grange et al. additionally demonstrated the impact of CSC-derived EVs isolated from RCC as main mediators for additional tumor microenvironment element, impacting on monocyte differentiation into dendritic cells [50].
A specific role for renal CSC-derived EVs has been additionally described for the formation of the pre-metastatic niche, which consist of a complex network of information exchanges. These EVs may sustain an unfavorable outcome of the tumor by enhancing tumor vascularization and by contributing to the establishment of a pre-metastatic niche [48]. More recently, it has been demonstrated that renal CSC EVs were enriched by miRNAs influencing cell growth, tumor invasion and metastases, thus giving to circulating miRNAs a promising role of biomarkers in RCC [45].
5. MicroRNA (miRNA): from free circulating to EV packaged biomarkers in RCC
MicroRNAs (miRNAs) are small noncoding RNA molecules of 18–22 nucleotides capable of post-transcriptionally regulating protein translation, due to an increased mRNA degradation [38,39]. For this reason, the biological role of miRNAs is usually associated with the role of their target mRNAs. Since a single miRNA can positively or negatively modulate numerous target mRNAs, they result as biological regulators of many cell functions including cell growth and proliferation, resistance to apoptosis and therefore they play a key role in tumorigenesis and tumor progression, representing potential useful biomarkers [2,51,52].
Over the last few years, the aberrant expression of miRNAs in cancer development has been dissected, identifying some miRNAs highly expressed in cancer cells with an oncogenic role and miRNAs acting as tumor suppressors. The deregulation of both groups of miRNAs contribute to tumor development mechanisms: oncogenic miRNAs are commonly overexpressed in cancerous tissues as well as tumor suppressor miRNAs are conversely downregulated in tumors [2].
Their stability in body fluids increases when they are packaged within EVs [53]. The utility of circulating miRNAs in RCC has been previously evaluated [54], nevertheless, recently, further evidence has been added to this emerging field, focusing on EV encapsulated miRNAs from blood samples.
Expression profile of several miRNAs has revealed their valid potential as diagnostic noninvasive markers in human RCC since they resulted differentially expressed in tumor when compared with normal counterpart, but also between primary and metastatic tumors [2]. It has a great clinical relevance in RCC, since a considerable number of ccRCC patients are diagnosed with metastatic disease, reducing the effectiveness of actual therapies. In advanced stages, limited treatment options often lead to poor prognosis. For this reason, the development of new molecular biomarkers can significantly improve the early RCC diagnosis and prognosis. Experimental evidence also revealed the potential prognostic value of different miRNAs correlated to overall-survival of RCC patients. However, the miRNA prognostic signature is debated due to lack of uniformity among studies regarding the identification of clinically significant miRNAs. The discrepancy may be due to the use of different cohorts of patients, so comorbid conditions and genetic differences, which are unrelated to RCC, may substantially influence the results [55].
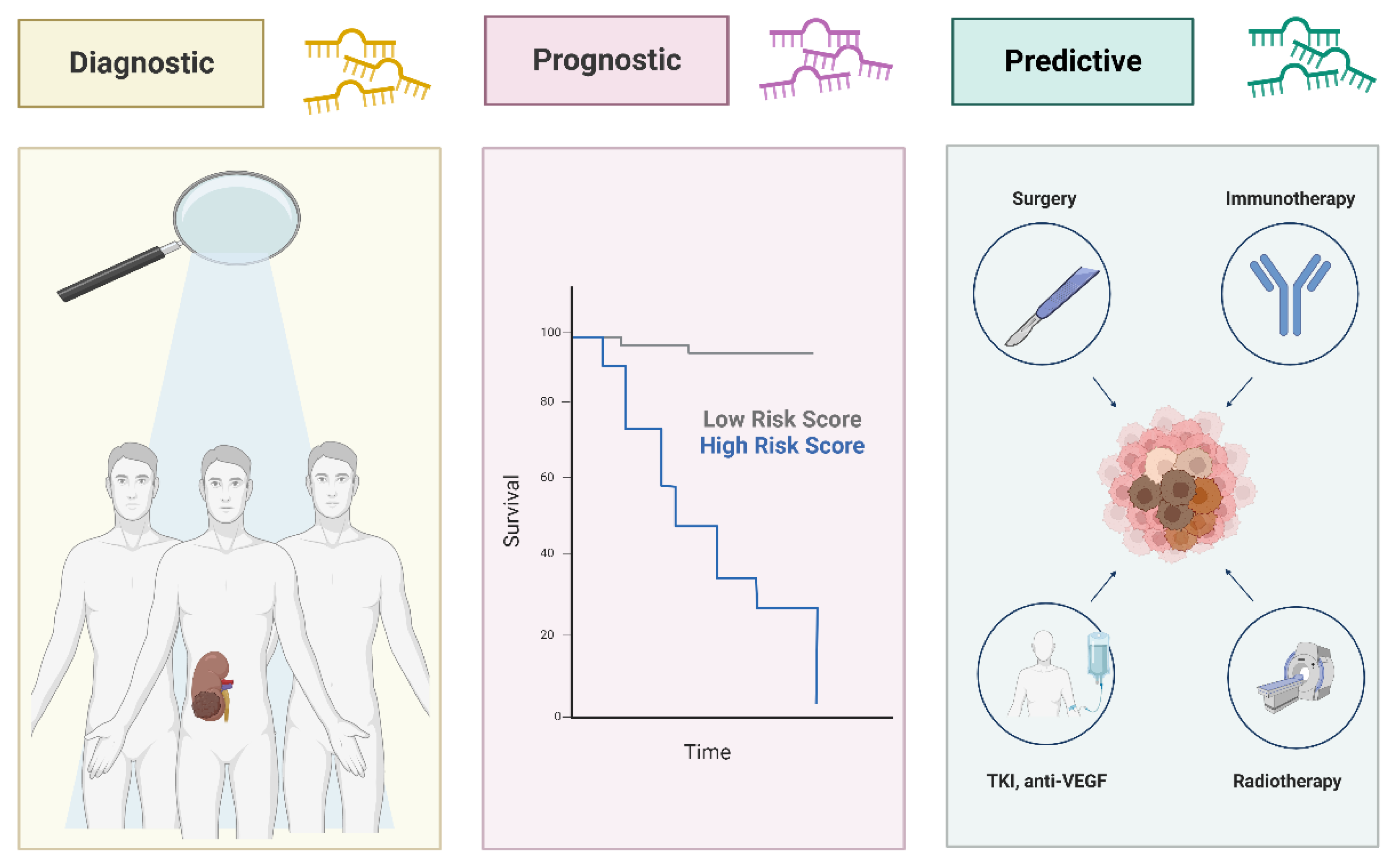
An improving challenge of recent studies is to find potential biomarkers able to increase sensitivity to chemo-radiotherapy, predicting patient’s response and resistance to targeted therapy. Circulating miRNAs might also be involved in acquiring resistance to treatment in RCC. Their promising role as predictors of response to therapy may acquire considerable importance in RCC, providing clinicians with crucial information to determine the optimal treatment plan and thus avoiding severe side effects of ineffective overtreatment [56] (Figure 3).
We reviewed the studies on free or encapsulated miRNAs differentially expressed in blood samples of RCC patients compared to normal controls, as summarized in Table 1. We observed that most of the studies analyzed the miRNAs expression within serum and plasma, without focusing on EV-derived miRNAs.
Tusong et al reported the over-expression of miR-21 and miR-106a in RCC patients’ serum compared to healthy controls and their significant reduction a month after surgery compared with the pre-operative group. This outcome suggests the potential diagnostic and predictive role of serum miR-21 and miR-106a as non-invasive biomarkers for RCC [57]. MiR-21 has been given much attention, due to an important role in a variety of malignant tumors. The correlation between the upregulation of miR-21 in serum of ccRCC patients and their clinical stage was described in literature [58], however, the underlying mechanisms are not well understood. Liu et al reported that upregulated miR-21 in serum predicates advanced clinic-pathological features and poor prognosis in patients with RCC through the p53/p21-cyclin E2-Bax/caspase-3 signaling pathway [59].
Cheng et al showed the upregulation of miR-21, miR-34a and miR-224 and the downregulation of miR-141 in the sera of patients with ccRCC, reporting their consistence of expression profile with those of the corresponding tumor tissue samples.

Table 1.
Deregulated microRNAs in blood samples of RCC patients as potential diagnostic, prognostic or predictive biomarkers.
Table 1.
Deregulated microRNAs in blood samples of RCC patients as potential diagnostic, prognostic or predictive biomarkers.
| miRNA | Expression Changes in RCC |
Source | Therapeutic Role | Reference |
|---|---|---|---|---|
| miR-106 | Up-regulated | Serum | Diagnostic, Predictive |
Tusong et al., 2017 [51] |
| miR-122-5p | Up-regulated | Serum | Prognostic | Heinemann et al., 2018 [72] |
| miR-1233 | Up-regulated | Exosomes- Serum |
Diagnostic, Predictive |
Zhang et al., 2018 [60] |
| Up-regulated | Plasma | Diagnostic, Prognostic |
Dias et al., 2017 [56] | |
| Up-regulated | Serum | Diagnostic | Wulfken et al., 2011 [59] | |
| miR-141 | Down-regulated | Serum | Diagnostic | Cheng et al., 2013 [52] |
| miR-144-3p | Up-regulated | Plasma | Diagnostic, Prognostic |
Lou et al., 2017 [69] |
| miR-149-3p | Up-regulated | Exosomes- Plasma |
Diagnostic | Xiao et al., 2020 [58] |
| miR-150 | Down-regulated | Plasma | Prognostic | Chanudet et al., 2017 [73] |
| miR-182-5p | Down-regulated | Serum | Diagnostic | Huang et al., 2020 [61] |
| miR-187 | Down-regulated | Plasma | Diagnostic, Prognostic |
Zhao et al., 2013 [70] |
| miR-193a-3p | Up-regulated | Serum | Diagnostic | Wang et al., 2015 [63] |
| miR-196a | Up-regulated | Serum | Diagnostic, Prognostic |
Huang et al., 2020 [68] |
| miR-206 | Up-regulated | Serum | Prognostic | Heinemann et al., 2018 [72] |
| miR-20b-5p | Down-regulated | Serum | Diagnostic | Huang et al., 2020 [68] |
| miR-21 | Up-regulated | Serum | Diagnostic, Predictive |
Tusong et al., 2017 [51] |
| Up-regulated | Serum | Diagnostic, Prognostic |
Cheng et al., 2013 [52] | |
| Up-regulated | Serum | Diagnostic, Prognostic |
Liu et al., 2017 [53] | |
| miR-210 | Up-regulated | Serum | Diagnostic, Predictive |
Fedorko et al., 2015 [64] |
| Up-regulated | Exosomes- Serum |
Diagnostic, Predictive |
Zhang et al., 2018 [60] | |
| Up-regulated | Plasma | Diagnostic, Prognostic |
Dias et al., 2017 [56] | |
| Up-regulated | Serum | Diagnostic | Iwamoto et al., 2014 [66] | |
| Up-regulated | Serum | Diagnostic, Predictive |
Zhao et al., 2013 [65] | |
| miR-218 | Up-regulated | Plasma | Diagnostic | Dias et al., 2017 [56] |
| miR-22 | Down-regulated | Serum | Diagnostic, Prognostic, Predictive |
Li et al., 2017 [77] |
| miR-221 | Up-regulated | Plasma | Diagnostic, Prognostic |
Teixeira et al., 2014 [57] |
| Up-regulated | Plasma | Diagnostic, Prognostic |
Dias et al., 2017 [56] | |
| miR-222 | Up-regulated | Plasma | Diagnostic | Teixeira et al., 2014 [57] |
| miR-224 | Up-regulated | Serum | Diagnostic | Cheng et al., 2013 [52] |
| Up-regulated | Serum | Diagnostic | Huang et al., 2020 [61] | |
| miR-28-5p | Down-regulated | Serum | Diagnostic | Wang et al., 2015 [63] |
| miR-30a-5p | Down-regulated | Serum | Diagnostic | Huang et al., 2020 [68] |
| miR-34a | Up-regulated | Serum | Diagnostic | Cheng et al., 2013 [52] |
| miR-34b-3p | Down-regulated | Serum | Diagnostic | Huang et al., 2020 [61] |
| miR-362 | Up-regulated | Serum | Diagnostic | Wang et al., 2015 [63] |
| miR-378 | Up-regulated | Serum | Diagnostic, Predictive |
Fedorko et al., 2015 [64] |
| Down-regulated | Serum | Diagnostic | Wang et al., 2015 [63] | |
| Up-regulated | Serum | Diagnostic | Redova et al., 2012 [62] | |
| miR-424-3p | Up-regulated | Exosomes- Plasma |
Diagnostic | Xiao et al., 2020 [58] |
| miR-451 | Down-regulated | Serum | Diagnostic | Redova et al., 2012 [62] |
| miR-483-5p | Down-regulated | Plasma | Diagnostic, Prognostic, Predictive |
Wang et al., 2021 [76] |
| miR-508-3p | Down-regulated | Serum | Diagnostic | Liu et al., 2019 [54] |
| miR-572 | Up-regulated | Serum | Diagnostic | Wang et al., 2015 [63] |
| miR-625-3p | Down-regulated | Serum | Diagnostic | Zhao et al., 2019 [55] |
| miR-765 | Down-regulated | Plasma | Predictive | Xiao et al., 2020 [67] |
| miR-885-5p | Up-regulated | Serum | Diagnostic | Liu et al., 2019 [54] |
| miR-92a-1-5p | Down-regulated | Exosomes- Plasma |
Diagnostic | Xiao et al., 2020 [58] |
| miR-1293 | Down-regulated | EVs- Plasma |
Prognostic, Predictive |
Dias et al., 2020 [75] |
| miR-301a-3p | Up-regulated | EVs- Plasma |
Prognostic, Predictive |
Dias et al., 2020 [75] |
| miR-let-7i-5p | Down-regulated | Exosomes- Plasma |
Prognostic | Du et al., 2017 [74] |
| miR-183-5p | Up-regulated | Serum | Diagnostic, Prognostic |
Zhang et al., 2015 [71] |
Interestingly, only the miR-21 expression levels in the serum of the patients were correlated with the patients' clinical stage, while miR-224 expression levels were correlated with gender. However, this study showed that miR-34a, miR-224, miR-21 and miR-141 could be considered as potential ccRCC tumor markers [58].
A diagnostic role has been attributed to several miRNAs, such as: miR-625-3p, miR-508-3p, miR-885-5p, dysregulated in serum of ccRCC patients [60,61]; miR-218 and miR-222 upregulated in plasma of patients [62,63]; miR-149-3p, miR-424-3p and miR-92a-1-5p that are significantly abnormal in exosomes from plasma of RCC patients [64]; miR-1233 that appeared upregulated in serum [65], exosomes from serum [66] and plasma [62] samples of RCC patients. Huang et al identified miR-182-5p, miR-224-5p and miR-34b-3p as potential diagnostic biomarkers after three-stage selection [67]; similarly, a diagnostic role was successfully validated by Redova et al for miR-378 and miR-451, due to the increased and decreased expression respectively in serum of RCC patients, enabling their potential use as biomarkers for distinguishing between RCC and healthy controls [68].
The late diagnosis of RCC primarily due to a lack of early-stage diagnostic encouraged researchers to discover novel miRNA signatures that differentiates RCC from healthy controls with a high degree of accuracy. In particular, Whang et al in 2015 focused on a 5-miRNA panel including miR-28-5p, miR-362, miR-572, miR-193a-3p and miR-378, demonstrating their potential value as an auxiliary clinical diagnostic tool to detect also early-stage RCC, for which surgery is most effective [69]. Next to a diagnostic role, in the same year other researchers dissected the prognostic and predictive value of miR-378 together with miR-210, describing their significant decrease in the time period of three months after radical nephrectomy [62,66,70,71,72].
More recently, the upregulation of miR-765 was described in plasma of ccRCC patients after tumor resection, suggesting its tumor suppressor role and identifying the proteolipid protein 2 (PLP2) as a candidate downstream target gene [73]. In the same year, Huang and his team suggested the diagnostic ability of miR-196a, miR-20b-5p and miR-30a-5p in the serum of 110 RCC patients and 110 healthy controls. Additionally, analyzing the clinical role of each miRNA, they showed the significant correlation of miR-196a-5p expression with the Fuhrman grade and the clinical stage, demonstrating its potential involvement in the oncogenesis and tumor progression of RCC [74]. A diagnostic and prognostic significance was defined for miR-144-3p [75], miR-187 [76], miR-221 [62,63] and miR-183-5p. In particular, it was demonstrated that the cells of patients with high levels of this miRNA in the blood poorly responded to the cytotoxicity induced by NK cells, suggesting that targeting miR-183-5p may be an effective way to enhance the outcome of NK cell-based immunotherapy [77].
In contrast to other studies, Heinemann et al did not only compare the serum of patients with ccRCC and healthy donors, but also a group of patients with benign renal tumors (BRT). As a result, the downregulation of miR-122-5p and miR-206 in serum of both ccRCC and BRT groups compared to controls suggested their doubtful role in diagnosis. However, they demonstrated their prognostic value, showing that high levels of miR-122-5p and miR-206 were associated with a significantly shorter period of progression-free, cancer-specific, and overall survival [78]. Plasma miRNA signatures specifically associated with late-stage disease were provided by researchers, contributing evidence that circulating miRNAs, such as miR-150 and miR-let-7b-5p, are associated with the progression of renal carcinoma and may contribute to disease monitoring [79,80].
The comparison of plasma of ccRCC patients with localized and metastatic disease before and after surgery suggested that EVs content varies depending on the presence or absence of the disease. An increased level of miR-301a-3p and a decreased expression of miR-1293 may be potential biomarkers of metastatic disease [81]. Two studies, encompassing two distinct miRNAs, specifically miR-22 and miR-483-5p, significantly related their deregulation with the tumor stage and clinicopathological parameters, showing diagnostic, prognostic and predictive functions [82,83]. Taken together, these findings revealed the potential role of miRNAs as promising biomarkers in RCC. They could provide a novel therapeutic front of view and their translation into clinical practice would be of great relevance in this neoplasia.
5. Conclusions
RCC is considering one of the most unfavorable tumor disease, due to the late diagnosis and the poor prognosis. Nowadays, specific biomarkers validated for RCC early detection are not available and the actual treatments are often unable to avoid recurrence of disease. LB could provide an attractive and non-invasive tool to assist the research for biomarkers in RCC tumors to capture a larger amount of the molecular heterogeneity compared to tissue biopsy and give prompt information on the risk of recurrence/relapse during follow-up.
Many efforts are directed towards the research for circulating miRNAs that play a role in almost all aspects of cancer biology and development. In particular, miRNAs packaged in EVs and released in blood flow could allow to expand the spectrum of potential biomarkers for future using in diagnosis and prognosis of RCC and in prediction of therapeutic response.
However, nowadays there are no miRNAs widely applied as biomarker in the clinical setting, partly due to the lack of isolation and quantification standardized protocols, the heterogeneity of the study cohorts and the variety of body fluids under investigation. Several studies analyzed plasma and serum-derived miRNAs, without focusing on the vesicle compartment. EV-derived miRNAs appear to be more stable than free miRNAs, as EVs seem to protect them from degradation by macrophages. The EVs double-layered membrane and nanoscale size allow the miRNA stability, thus prolonging their circulation half-life and enhancing their biological activity [84]. After release, EVs are taken up by neighboring or distant cells, and the miRNAs encapsulated modulate several processes, as interfering with tumor immunity and the microenvironment, possibly facilitating tumor growth, invasion, metastasis, angiogenesis and drug resistance [85]. Therefore, EV-derived miRNAs have a significant function in regulating cancer progression. More investigations on this matter are warranted. Nonetheless, the most exciting but challenging application will be to utilize EVs and their cargo as a clinical tool to diagnose and monitor disease. Thus, EV-derived miRNAs could provide a novel therapeutic tool in RCC clinical practice, where the lack of adequate biomarkers makes functional investigations urgently needed.
Author Contributions
IM: VC, MO, CN, CC, CAB and MGV participated in the literature search, wrote the manuscript parts, and prepared the figures and tables. MD, RS and MGV conceived the manuscript concept, wrote and final edited the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was funded in parts by grants from Associazione ASEOP (MD, CC), Progetto MIUR Dipartimenti Eccellenti 2022 (MD) and from the European Union - NextGenerationEU through the Italian Ministry of University and Research under PNRR - M4C2-I1.3 Project PE_00000019 "HEAL ITALIA" (MD, GG, CAB).
Acknowledgments
VC is grateful to Prof. Carmen Jerónimo (Portuguese Oncology Institute of Porto, Portugal) and her team for the support and inspiration on EV investigations.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shi, L.; Wang, M.; Li, H.; You, P. MicroRNAs in Body Fluids: A More Promising Biomarker for Clear Cell Renal Cell Carcinoma. Cancer Manag Res 2021, 13, 7663–7675. [Google Scholar] [CrossRef] [PubMed]
- Spadaccino, F.; Gigante, M.; Netti, G.S.; Rocchetti, M.T.; Franzin, R.; Gesualdo, L.; Castellano, G.; Stallone, G.; Ranieri, E. The Ambivalent Role of MiRNAs in Carcinogenesis: Involvement in Renal Cell Carcinoma and Their Clinical Applications. Pharmaceuticals (Basel) 2021, 14, 322. [Google Scholar] [CrossRef] [PubMed]
- Singh, D. Current Updates and Future Perspectives on the Management of Renal Cell Carcinoma. Life Sci 2021, 264, 118632. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; Saginala, K.; Mohammed, A.; Vakiti, A.; Rawla, P.; Barsouk, A. Epidemiology of Renal Cell Carcinoma. World J Oncol 2020, 11, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Liao, Z. Comparison of Radical Nephrectomy and Partial Nephrectomy for T1 Renal Cell Carcinoma: A Meta-Analysis. Urol Int 2018, 101, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Alam, R.; Patel, H.D.; Osumah, T.; Srivastava, A.; Gorin, M.A.; Johnson, M.H.; Trock, B.J.; Chang, P.; Wagner, A.A.; McKiernan, J.M.; et al. Comparative Effectiveness of Management Options for Patients with Small Renal Masses: A Prospective Cohort Study. BJU International 2019, 123, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.C.; Novick, A.C.; Belldegrun, A.; Blute, M.L.; Chow, G.K.; Derweesh, I.H.; Faraday, M.M.; Kaouk, J.H.; Leveillee, R.J.; Matin, S.F.; et al. Guideline for Management of the Clinical T1 Renal Mass. Journal of Urology 2009, 182, 1271–1279. [Google Scholar] [CrossRef]
- Marchioni, M.; Rivas, J.G.; Autran, A.; Socarras, M.; Albisinni, S.; Ferro, M.; Schips, L.; Scarpa, R.M.; Papalia, R.; Esperto, F. Biomarkers for Renal Cell Carcinoma Recurrence: State of the Art. Curr Urol Rep 2021, 22, 31. [Google Scholar] [CrossRef]
- Borchiellini, D.; Maillet, D. Clinical Activity of Immunotherapy-Based Combination First-Line Therapies for Metastatic Renal Cell Carcinoma: The Right Treatment for the Right Patient. Bulletin du Cancer 2022, 109, 2S4–2S18. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Rini, B.I.; Beckermann, K.E. Emerging Targets in Clear Cell Renal Cell Carcinoma. Cancers (Basel) 2022, 14, 4843. [Google Scholar] [CrossRef]
- Tung, I.; Sahu, A. Immune Checkpoint Inhibitor in First-Line Treatment of Metastatic Renal Cell Carcinoma: A Review of Current Evidence and Future Directions. Front Oncol 2021, 11, 707214. [Google Scholar] [CrossRef]
- Iaxx, R.; Lefort, F.; Domblides, C.; Ravaud, A.; Bernhard, J.-C.; Gross-Goupil, M. An Evaluation of Cabozantinib for the Treatment of Renal Cell Carcinoma: Focus on Patient Selection and Perspectives. Ther Clin Risk Manag 2022, 18, 619–632. [Google Scholar] [CrossRef] [PubMed]
- Iacovelli, R.; Nolè, F.; Verri, E.; Renne, G.; Paglino, C.; Santoni, M.; Cossu Rocca, M.; Giglione, P.; Aurilio, G.; Cullurà, D.; et al. Prognostic Role of PD-L1 Expression in Renal Cell Carcinoma. A Systematic Review and Meta-Analysis. Target Oncol 2016, 11, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, J.; Sundqvist, P.; Kosuta, V.; Fält, A.; Giunchi, F.; Fiorentino, M.; Davidsson, S. PD-L1 Expression Is Associated With Poor Prognosis in Renal Cell Carcinoma. Applied Immunohistochemistry & Molecular Morphology 2020, 28, 213. [Google Scholar] [CrossRef]
- Dudani, S.; Savard, M.-F.; Heng, D.Y.C. An Update on Predictive Biomarkers in Metastatic Renal Cell Carcinoma. Eur Urol Focus 2020, 6, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Makhov, P.; Joshi, S.; Ghatalia, P.; Kutikov, A.; Uzzo, R.G.; Kolenko, V.M. RESISTANCE TO SYSTEMIC THERAPIES IN CLEAR CELL RENAL CELL CARCINOMA: MECHANISMS AND MANAGEMENT STRATEGIES. Mol Cancer Ther 2018, 17, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Grange, C.; Brossa, A.; Bussolati, B. Extracellular Vesicles and Carried MiRNAs in the Progression of Renal Cell Carcinoma. Int J Mol Sci 2019, 20, 1832. [Google Scholar] [CrossRef]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Math, M.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; et al. Intratumor Heterogeneity and Branched Evolution Revealed by Multiregion Sequencing. N Engl J Med 2012, 366, 883–892. [Google Scholar] [CrossRef]
- Martins, V.R.; Dias, M.S.; Hainaut, P. Tumor-Cell-Derived Microvesicles as Carriers of Molecular Information in Cancer. Curr Opin Oncol 2013, 25, 66–75. [Google Scholar] [CrossRef]
- Yu, W.; Hurley, J.; Roberts, D.; Chakrabortty, S.K.; Enderle, D.; Noerholm, M.; Breakefield, X.O.; Skog, J.K. Exosome-Based Liquid Biopsies in Cancer: Opportunities and Challenges. Ann Oncol 2021, 32, 466–477. [Google Scholar] [CrossRef]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid Biopsy: A Step Closer to Transform Diagnosis, Prognosis and Future of Cancer Treatments. Molecular Cancer 2022, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Lakshminarayanan, H.; Rutishauser, D.; Schraml, P.; Moch, H.; Bolck, H.A. Liquid Biopsies in Renal Cell Carcinoma—Recent Advances and Promising New Technologies for the Early Detection of Metastatic Disease. Front Oncol 2020, 10, 582843. [Google Scholar] [CrossRef] [PubMed]
- Michela, B. Liquid Biopsy: A Family of Possible Diagnostic Tools. Diagnostics (Basel) 2021, 11, 1391. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, L.; Zheng, J.; Li, Z.; Li, S.; Wang, K.; Chen, X. Liquid Biopsy at the Frontier in Renal Cell Carcinoma: Recent Analysis of Techniques and Clinical Application. Mol Cancer 2023, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Bade, R.M.; Schehr, J.L.; Emamekhoo, H.; Gibbs, B.K.; Rodems, T.S.; Mannino, M.C.; Desotelle, J.A.; Heninger, E.; Stahlfeld, C.N.; Sperger, J.M.; et al. Development and Initial Clinical Testing of a Multiplexed Circulating Tumor Cell Assay in Patients with Clear Cell Renal Cell Carcinoma. Mol Oncol 2021, 15, 2330–2344. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, P.V.; Berchuck, J.E.; Korthauer, K.; Spisak, S.; Nassar, A.H.; Abou Alaiwi, S.; Chakravarthy, A.; Shen, S.Y.; Bakouny, Z.; Boccardo, F.; et al. Detection of Renal Cell Carcinoma Using Plasma and Urine Cell-Free DNA Methylomes. Nat Med 2020, 26, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, J.P.; Constâncio, V.; Salta, S.; Lobo, J.; Barros-Silva, D.; Carvalho-Maia, C.; Rodrigues, J.; Braga, I.; Henrique, R.; Jerónimo, C. LiKidMiRs: A DdPCR-Based Panel of 4 Circulating MiRNAs for Detection of Renal Cell Carcinoma. Cancers (Basel) 2022, 14, 858. [Google Scholar] [CrossRef]
- Peter, M.R.; Zhao, F.; Jeyapala, R.; Kamdar, S.; Xu, W.; Hawkins, C.; Evans, A.J.; Fleshner, N.E.; Finelli, A.; Bapat, B. Investigating Urinary Circular RNA Biomarkers for Improved Detection of Renal Cell Carcinoma. Front Oncol 2021, 11, 814228. [Google Scholar] [CrossRef]
- Kohli, M.; Tan, W.; Vire, B.; Liaud, P.; Blairvacq, M.; Berthier, F.; Rouison, D.; Garnier, G.; Payen, L.; Cousin, T.; et al. Prognostic Value of Plasma HPG80 (Circulating Progastrin) in Metastatic Renal Cell Carcinoma. Cancers (Basel) 2021, 13, 375. [Google Scholar] [CrossRef]
- Wang, Z.-L.; Zhang, P.; Li, H.-C.; Yang, X.-J.; Zhang, Y.-P.; Li, Z.-L.; Xue, L.; Xue, Y.-Q.; Li, H.-L.; Chen, Q.; et al. Dynamic Changes of Different Phenotypic and Genetic Circulating Tumor Cells as a Biomarker for Evaluating the Prognosis of RCC. Cancer Biol Ther 2019, 20, 505–512. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Uemura, M.; Fujita, M.; Maejima, K.; Koh, Y.; Matsushita, M.; Nakano, K.; Hayashi, Y.; Wang, C.; Ishizuya, Y.; et al. Clinical Significance of the Mutational Landscape and Fragmentation of Circulating Tumor DNA in Renal Cell Carcinoma. Cancer Sci 2019, 110, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Li, Y.; Wang, M.; Gu, J.; Xu, W.; Cai, H.; Fang, X.; Zhang, X. Exosomes as a New Frontier of Cancer Liquid Biopsy. Molecular Cancer 2022, 21, 56. [Google Scholar] [CrossRef] [PubMed]
- Zaborowski, M.P.; Balaj, L.; Breakefield, X.O.; Lai, C.P. Extracellular Vesicles: Composition, Biological Relevance, and Methods of Study. Bioscience 2015, 65, 783–797. [Google Scholar] [CrossRef]
- Zaborowski, M.P.; Balaj, L.; Breakefield, X.O.; Lai, C.P. Extracellular Vesicles: Composition, Biological Relevance, and Methods of Study. BioScience 2015, 65, 783–797. [Google Scholar] [CrossRef]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal Information for Studies of Extracellular Vesicles 2018 (MISEV2018): A Position Statement of the International Society for Extracellular Vesicles and Update of the MISEV2014 Guidelines. Journal of Extracellular Vesicles 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Lötvall, J.; Hill, A.F.; Hochberg, F.; Buzás, E.I.; Di Vizio, D.; Gardiner, C.; Gho, Y.S.; Kurochkin, I.V.; Mathivanan, S.; Quesenberry, P.; et al. Minimal Experimental Requirements for Definition of Extracellular Vesicles and Their Functions: A Position Statement from the International Society for Extracellular Vesicles. J Extracell Vesicles 2014, 3, 26913. [Google Scholar] [CrossRef] [PubMed]
- Peinado, H.; Lyden, D. Metastasis. 2017, 30, 836–848. 30. [CrossRef]
- Qian, Z.; Shen, Q.; Yang, X.; Qiu, Y.; Zhang, W. The Role of Extracellular Vesicles: An Epigenetic View of the Cancer Microenvironment. BioMed Research International 2015, 2015. [Google Scholar] [CrossRef]
- Grange, C.; Tapparo, M.; Collino, F.; Vitillo, L.; Damasco, C.; Deregibus, M.C.; Tetta, C.; Bussolati, B.; Camussi, G. Microvesicles Released from Human Renal Cancer Stem Cells Stimulate Angiogenesis and Formation of Lung Premetastatic Niche. Cancer Research 2011, 71, 5346–5356. [Google Scholar] [CrossRef]
- Lindoso, R.S.; Collino, F.; Camussi, G. Extracellular Vesicles Derived from Renal Cancer Stem Cells Induce a Pro-Tumorigenic Phenotype in Mesenchymal Stromal Cells. Oncotarget 2015, 6, 7959–7969. [Google Scholar] [CrossRef]
- Skotland, T.; Sagini, K.; Sandvig, K.; Llorente, A. An Emerging Focus on Lipids in Extracellular Vesicles. Advanced Drug Delivery Reviews 2020, 159, 308–321. [Google Scholar] [CrossRef]
- Rimmer, M.P.; Gregory, C.D.; Mitchell, R.T. Extracellular Vesicles in Urological Malignancies. Biochim Biophys Acta Rev Cancer 2021, 1876, None. [Google Scholar] [CrossRef] [PubMed]
- Barth, D.A.; Drula, R.; Ott, L.; Fabris, L.; Slaby, O.; Calin, G.A.; Pichler, M. Circulating Non-Coding RNAs in Renal Cell Carcinoma—Pathogenesis and Potential Implications as Clinical Biomarkers. Front Cell Dev Biol 2020, 8, 828. [Google Scholar] [CrossRef]
- Butz, H.; Nofech-Mozes, R.; Ding, Q.; Khella, H.W.Z.; Szabó, P.M.; Jewett, M.; Finelli, A.; Lee, J.; Ordon, M.; Stewart, R.; et al. Exosomal MicroRNAs Are Diagnostic Biomarkers and Can Mediate Cell–Cell Communication in Renal Cell Carcinoma. European Urology Focus 2016, 2, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Grange, C.; Brossa, A.; Bussolati, B. Extracellular Vesicles and Carried MiRNAs in the Progression of Renal Cell Carcinoma. International Journal of Molecular Sciences 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Horie, K.; Kawakami, K.; Fujita, Y.; Sugaya, M.; Kameyama, K.; Mizutani, K.; Deguchi, T.; Ito, M. Exosomes Expressing Carbonic Anhydrase 9 Promote Angiogenesis. Biochem Biophys Res Commun 2017, 492, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Jingushi, K.; Uemura, M.; Ohnishi, N.; Nakata, W.; Fujita, K.; Naito, T.; Fujii, R.; Saichi, N.; Nonomura, N.; Tsujikawa, K.; et al. Extracellular Vesicles Isolated from Human Renal Cell Carcinoma Tissues Disrupt Vascular Endothelial Cell Morphology via Azurocidin. Int J Cancer 2018, 142, 607–617. [Google Scholar] [CrossRef]
- Grange, C.; Tapparo, M.; Collino, F.; Vitillo, L.; Damasco, C.; Deregibus, M.C.; Tetta, C.; Bussolati, B.; Camussi, G. Microvesicles Released from Human Renal Cancer Stem Cells Stimulate Angiogenesis and Formation of Lung Premetastatic Niche. Cancer Research 2011, 71, 5346–5356. [Google Scholar] [CrossRef]
- Lindoso, R.S.; Collino, F.; Camussi, G. Extracellular Vesicles Derived from Renal Cancer Stem Cells Induce a Pro-Tumorigenic Phenotype in Mesenchymal Stromal Cells. Oncotarget 2015, 6, 7959–7969. [Google Scholar] [CrossRef]
- Grange, C.; Tapparo, M.; Tritta, S.; Deregibus, M.C.; Battaglia, A.; Gontero, P.; Frea, B.; Camussi, G. Role of HLA-G and Extracellular Vesicles in Renal Cancer Stem Cell-Induced Inhibition of Dendritic Cell Differentiation. BMC Cancer 2015, 15, 1009. [Google Scholar] [CrossRef]
- Jansson, M.D.; Lund, A.H. MicroRNA and Cancer. Mol Oncol 2012, 6, 590–610. [Google Scholar] [CrossRef]
- Peng, Y.; Croce, C.M. The Role of MicroRNAs in Human Cancer. Signal Transduct Target Ther 2016, 1, 15004. [Google Scholar] [CrossRef] [PubMed]
- Challagundla, K.B.; Wise, P.M.; Neviani, P.; Chava, H.; Murtadha, M.; Xu, T.; Kennedy, R.; Ivan, C.; Zhang, X.; Vannini, I.; et al. Exosome-Mediated Transfer of MicroRNAs within the Tumor Microenvironment and Neuroblastoma Resistance to Chemotherapy. J Natl Cancer Inst 2015, 107, djv135. [Google Scholar] [CrossRef] [PubMed]
- Ellinger, J.; Gevensleben, H.; Müller, S.C.; Dietrich, D. The Emerging Role of Non-Coding Circulating RNA as a Biomarker in Renal Cell Carcinoma. Expert Rev Mol Diagn 2016, 16, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Lokeshwar, S.D.; Talukder, A.; Yates, T.J.; Hennig, M.J.P.; Garcia-Roig, M.; Lahorewala, S.S.; Mullani, N.N.; Klaassen, Z.; Kava, B.R.; Manoharan, M.; et al. Molecular Characterization of Renal Cell Carcinoma: A Potential Three-MicroRNA Prognostic Signature. Cancer Epidemiology, Biomarkers & Prevention 2018, 27, 464–472. [Google Scholar] [CrossRef]
- Tsiakanikas, P.; Giaginis, C.; Kontos, C.K.; Scorilas, A. Clinical Utility of MicroRNAs in Renal Cell Carcinoma: Current Evidence and Future Perspectives. Expert Rev Mol Diagn 2018, 18, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Tusong, H.; Maolakuerban, N.; Guan, J.; Rexiati, M.; Wang, W.-G.; Azhati, B.; Nuerrula, Y.; Wang, Y.-J. Functional Analysis of Serum MicroRNAs MiR-21 and MiR-106a in Renal Cell Carcinoma. Cancer Biomark 2017, 18, 79–85. [Google Scholar] [CrossRef]
- Cheng, T.; Wang, L.; Li, Y.; Huang, C.; Zeng, L.; Yang, J. Differential MicroRNA Expression in Renal Cell Carcinoma. Oncol Lett 2013, 6, 769–776. [Google Scholar] [CrossRef]
- Liu, Z.; Lu, Y.; Xiao, Y.; Lu, Y. Upregulation of MiR-21 Expression Is a Valuable Predicator of Advanced Clinicopathological Features and Poor Prognosis in Patients with Renal Cell Carcinoma through the P53/P21-cyclin E2-Bax/Caspase-3 Signaling Pathway. Oncology Reports 2017, 37, 1437–1444. [Google Scholar] [CrossRef]
- Liu, S.; Deng, X.; Zhang, J. Identification of Dysregulated Serum MiR-508-3p and MiR-885-5p as Potential Diagnostic Biomarkers of Clear Cell Renal Carcinoma. Mol Med Rep 2019, 20, 5075–5083. [Google Scholar] [CrossRef]
- Zhao, L.; Liu, K.; Pan, X.; Quan, J.; Zhou, L.; Li, Z.; Lin, C.; Xu, J.; Xu, W.; Guan, X.; et al. MiR-625-3p Promotes Migration and Invasion and Reduces Apoptosis of Clear Cell Renal Cell Carcinoma. Am J Transl Res 2019, 11, 6475–6486. [Google Scholar]
- Dias, F.; Teixeira, A.L.; Ferreira, M.; Adem, B.; Bastos, N.; Vieira, J.; Fernandes, M.; Sequeira, M.I.; Maurício, J.; Lobo, F.; et al. Plasmatic MiR-210, MiR-221 and MiR-1233 Profile: Potential Liquid Biopsies Candidates for Renal Cell Carcinoma. Oncotarget 2017, 8, 103315–103326. [Google Scholar] [CrossRef]
- Teixeira, A.L.; Ferreira, M.; Silva, J.; Gomes, M.; Dias, F.; Santos, J.I.; Maurício, J.; Lobo, F.; Medeiros, R. Higher Circulating Expression Levels of MiR-221 Associated with Poor Overall Survival in Renal Cell Carcinoma Patients. Tumor Biol. 2014, 35, 4057–4066. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.-T.; Lai, W.-J.; Zhu, W.-A.; Wang, H. MicroRNA Derived from Circulating Exosomes as Noninvasive Biomarkers for Diagnosing Renal Cell Carcinoma. Onco Targets Ther 2020, 13, 10765–10774. [Google Scholar] [CrossRef] [PubMed]
- Wulfken, L.M.; Moritz, R.; Ohlmann, C.; Holdenrieder, S.; Jung, V.; Becker, F.; Herrmann, E.; Walgenbach-Brünagel, G.; Ruecker, A. von; Müller, S.C.; et al. MicroRNAs in Renal Cell Carcinoma: Diagnostic Implications of Serum MiR-1233 Levels. PLOS ONE 2011, 6, e25787. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ni, M.; Su, Y.; Wang, H.; Zhu, S.; Zhao, A.; Li, G. MicroRNAs in Serum Exosomes as Potential Biomarkers in Clear-Cell Renal Cell Carcinoma. Eur Urol Focus 2018, 4, 412–419. [Google Scholar] [CrossRef]
- Huang, G.; Li, X.; Chen, Z.; Wang, J.; Zhang, C.; Chen, X.; Peng, X.; Liu, K.; Zhao, L.; Lai, Y.; et al. A Three-MicroRNA Panel in Serum: Serving as a Potential Diagnostic Biomarker for Renal Cell Carcinoma. Pathol. Oncol. Res. 2020, 26, 2425–2434. [Google Scholar] [CrossRef]
- Redova, M.; Poprach, A.; Nekvindova, J.; Iliev, R.; Radova, L.; Lakomy, R.; Svoboda, M.; Vyzula, R.; Slaby, O. Circulating MiR-378 and MiR-451 in Serum Are Potential Biomarkers for Renal Cell Carcinoma. J Transl Med 2012, 10, 55. [Google Scholar] [CrossRef]
- Wang, C.; Hu, J.; Lu, M.; Gu, H.; Zhou, X.; Chen, X.; Zen, K.; Zhang, C.-Y.; Zhang, T.; Ge, J.; et al. A Panel of Five Serum MiRNAs as a Potential Diagnostic Tool for Early-Stage Renal Cell Carcinoma. Sci Rep 2015, 5, 7610. [Google Scholar] [CrossRef]
- Fedorko, M.; Stanik, M.; Iliev, R.; Redova-Lojova, M.; Machackova, T.; Svoboda, M.; Pacik, D.; Dolezel, J.; Slaby, O. Combination of MiR-378 and MiR-210 Serum Levels Enables Sensitive Detection of Renal Cell Carcinoma. Int J Mol Sci 2015, 16, 23382–23389. [Google Scholar] [CrossRef]
- Zhao, A.; Li, G.; Péoc’h, M.; Genin, C.; Gigante, M. Serum MiR-210 as a Novel Biomarker for Molecular Diagnosis of Clear Cell Renal Cell Carcinoma. Exp Mol Pathol 2013, 94, 115–120. [Google Scholar] [CrossRef]
- Iwamoto, H.; Kanda, Y.; Sejima, T.; Osaki, M.; Okada, F.; Takenaka, A. Serum MiR-210 as a Potential Biomarker of Early Clear Cell Renal Cell Carcinoma. International Journal of Oncology 2014, 44, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Wang, C.; Chen, K.; Wang, T.; Xing, J.; Zhang, X.; Wang, X. MiR-765 Functions as a Tumour Suppressor and Eliminates Lipids in Clear Cell Renal Cell Carcinoma by Downregulating PLP2. EBioMedicine 2020, 51, 102622. [Google Scholar] [CrossRef]
- Huang, G.; Li, H.; Wang, J.; Peng, X.; Liu, K.; Zhao, L.; Zhang, C.; Chen, X.; Lai, Y.; Ni, L. Combination of Tumor Suppressor MiR-20b-5p, MiR-30a-5p, and MiR-196a-5p as a Serum Diagnostic Panel for Renal Cell Carcinoma. Pathol Res Pract 2020, 216, 153152. [Google Scholar] [CrossRef] [PubMed]
- Lou, N.; Ruan, A.-M.; Qiu, B.; Bao, L.; Xu, Y.-C.; Zhao, Y.; Sun, R.-L.; Zhang, S.-T.; Xu, G.-H.; Ruan, H.-L.; et al. MiR-144-3p as a Novel Plasma Diagnostic Biomarker for Clear Cell Renal Cell Carcinoma. Urologic Oncology: Seminars and Original Investigations 2017, 35, 36–e7. [Google Scholar] [CrossRef]
- Zhao, J.; Lei, T.; Xu, C.; Li, H.; Ma, W.; Yang, Y.; Fan, S.; Liu, Y. MicroRNA-187, down-Regulated in Clear Cell Renal Cell Carcinoma and Associated with Lower Survival, Inhibits Cell Growth and Migration Though Targeting B7-H3. Biochemical and Biophysical Research Communications 2013, 438, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Di, W.; Dong, Y.; Lu, G.; Yu, J.; Li, J.; Li, P. High Serum MiR-183 Level Is Associated with Poor Responsiveness of Renal Cancer to Natural Killer Cells. Tumor Biol. 2015, 36, 9245–9249. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, F.G.; Tolkach, Y.; Deng, M.; Schmidt, D.; Perner, S.; Kristiansen, G.; Müller, S.C.; Ellinger, J. Serum MiR-122-5p and MiR-206 Expression: Non-Invasive Prognostic Biomarkers for Renal Cell Carcinoma. Clin Epigenetics 2018, 10, 11. [Google Scholar] [CrossRef]
- Chanudet, E.; Wozniak, M.B.; Bouaoun, L.; Byrnes, G.; Mukeriya, A.; Zaridze, D.; Brennan, P.; Muller, D.C.; Scelo, G. Large-Scale Genome-Wide Screening of Circulating MicroRNAs in Clear Cell Renal Cell Carcinoma Reveals Specific Signatures in Late-Stage Disease. International Journal of Cancer 2017, 141, 1730–1740. [Google Scholar] [CrossRef]
- Du, M.; Giridhar, K.V.; Tian, Y.; Tschannen, M.R.; Zhu, J.; Huang, C.-C.; Kilari, D.; Kohli, M.; Wang, L. Plasma Exosomal MiRNAs-Based Prognosis in Metastatic Kidney Cancer. Oncotarget 2017, 8, 63703–63714. [Google Scholar] [CrossRef]
- Dias, F.; Teixeira, A.L.; Nogueira, I.; Morais, M.; Maia, J.; Bodo, C.; Ferreira, M.; Silva, A.; Vilhena, M.; Lobo, J.; et al. Extracellular Vesicles Enriched in Hsa-MiR-301a-3p and Hsa-MiR-1293 Dynamics in Clear Cell Renal Cell Carcinoma Patients: Potential Biomarkers of Metastatic Disease. Cancers (Basel) 2020, 12, 1450. [Google Scholar] [CrossRef]
- Wang, X.-G.; Zhu, Y.-W.; Wang, T.; Chen, B.; Xing, J.-C.; Xiao, W. MiR-483-5p Downregulation Contributed to Cell Proliferation, Metastasis, and Inflammation of Clear Cell Renal Cell Carcinoma. The Kaohsiung Journal of Medical Sciences 2021, 37, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Sha, Y.; Zhang, X. MiR-22 Functions as a Biomarker and Regulates Cell Proliferation, Cycle, Apoptosis, Migration and Invasion in Renal Cell Carcinoma. Int J Clin Exp Pathol 2017, 10, 11425–11437. [Google Scholar]
- Sun, I.O.; Bae, Y.-U.; Lee, H.; Kim, H.; Jeon, J.S.; Noh, H.; Choi, J.-S.; Doh, K.-O.; Kwon, S.H. Circulating MiRNAs in Extracellular Vesicles Related to Treatment Response in Patients with Idiopathic Membranous Nephropathy. Journal of Translational Medicine 2022, 20, 224. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Shi, K.; Yang, S.; Liu, J.; Zhou, Q.; Wang, G.; Song, J.; Li, Z.; Zhang, Z.; Yuan, W. Effect of Exosomal MiRNA on Cancer Biology and Clinical Applications. Mol Cancer 2018, 17, 147. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Peripheral Blood collection in RCC patients. Liquid biopsy, in particular peripheral blood, can be a source of cancer material: circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), and extracellular vesicles (EVs), released by tumors into the bloodstream. Figure was generated with BioRender.
Figure 1.
Peripheral Blood collection in RCC patients. Liquid biopsy, in particular peripheral blood, can be a source of cancer material: circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), and extracellular vesicles (EVs), released by tumors into the bloodstream. Figure was generated with BioRender.
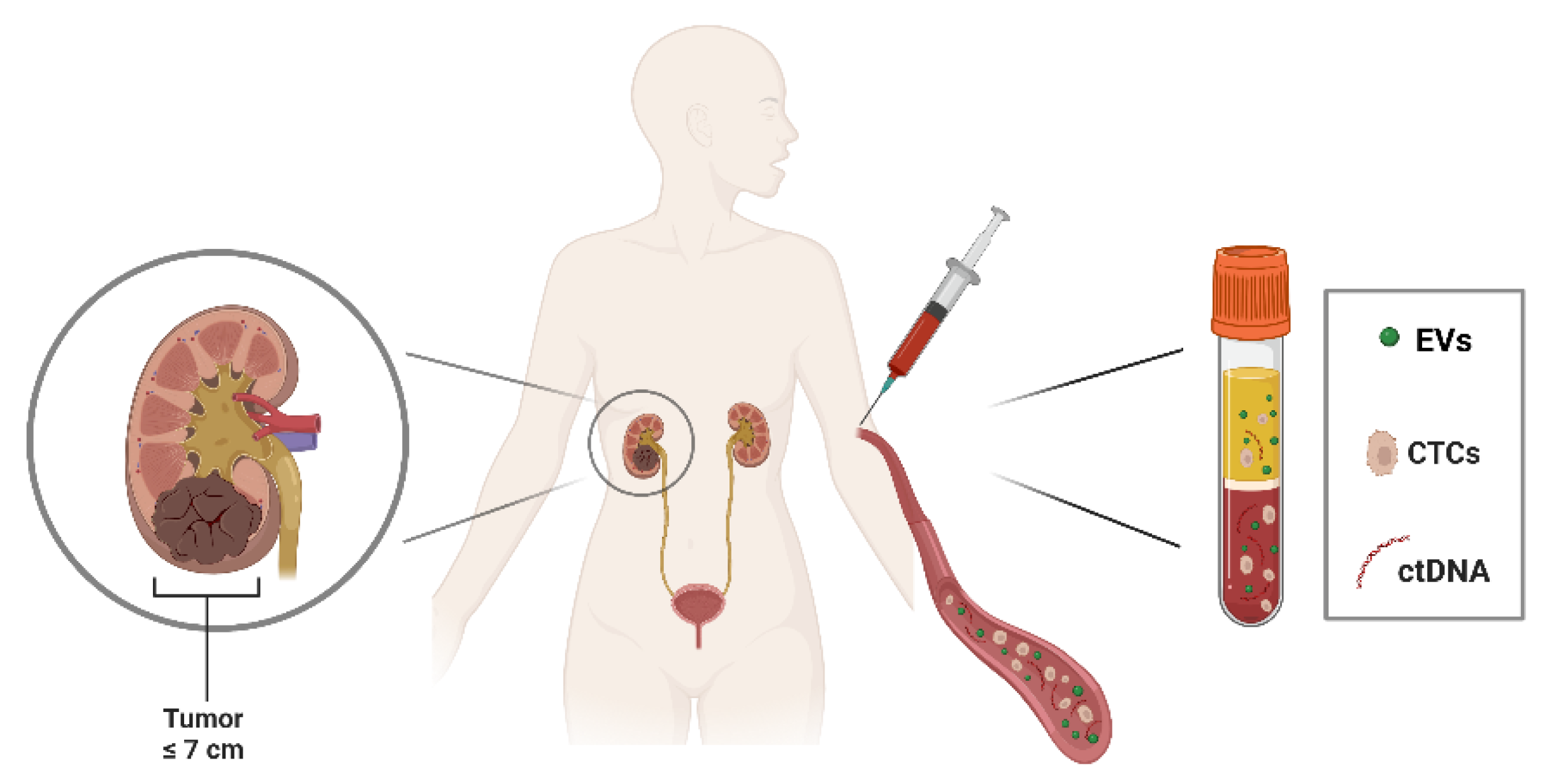
Figure 2.
Biogenesis and structure of extracellular vesicles (EVs). EVs include three different sub-populations: exosomes are intraluminal vesicles released after fusion of a multivesicular body (MVB) with the cell membrane through exocytosis; microvesicles are formed by outward shedding of the cell membrane into extracellular space; apoptotic bodies are generated when cells undergo apoptosis. EVs subtypes vary in size and composition and carry different cargoes such as nucleic acids and cytosolic proteins. They are also characterized by membrane proteins such as tetraspanins that identify the exosomal population. Figure was generated with BioRender.
Figure 2.
Biogenesis and structure of extracellular vesicles (EVs). EVs include three different sub-populations: exosomes are intraluminal vesicles released after fusion of a multivesicular body (MVB) with the cell membrane through exocytosis; microvesicles are formed by outward shedding of the cell membrane into extracellular space; apoptotic bodies are generated when cells undergo apoptosis. EVs subtypes vary in size and composition and carry different cargoes such as nucleic acids and cytosolic proteins. They are also characterized by membrane proteins such as tetraspanins that identify the exosomal population. Figure was generated with BioRender.
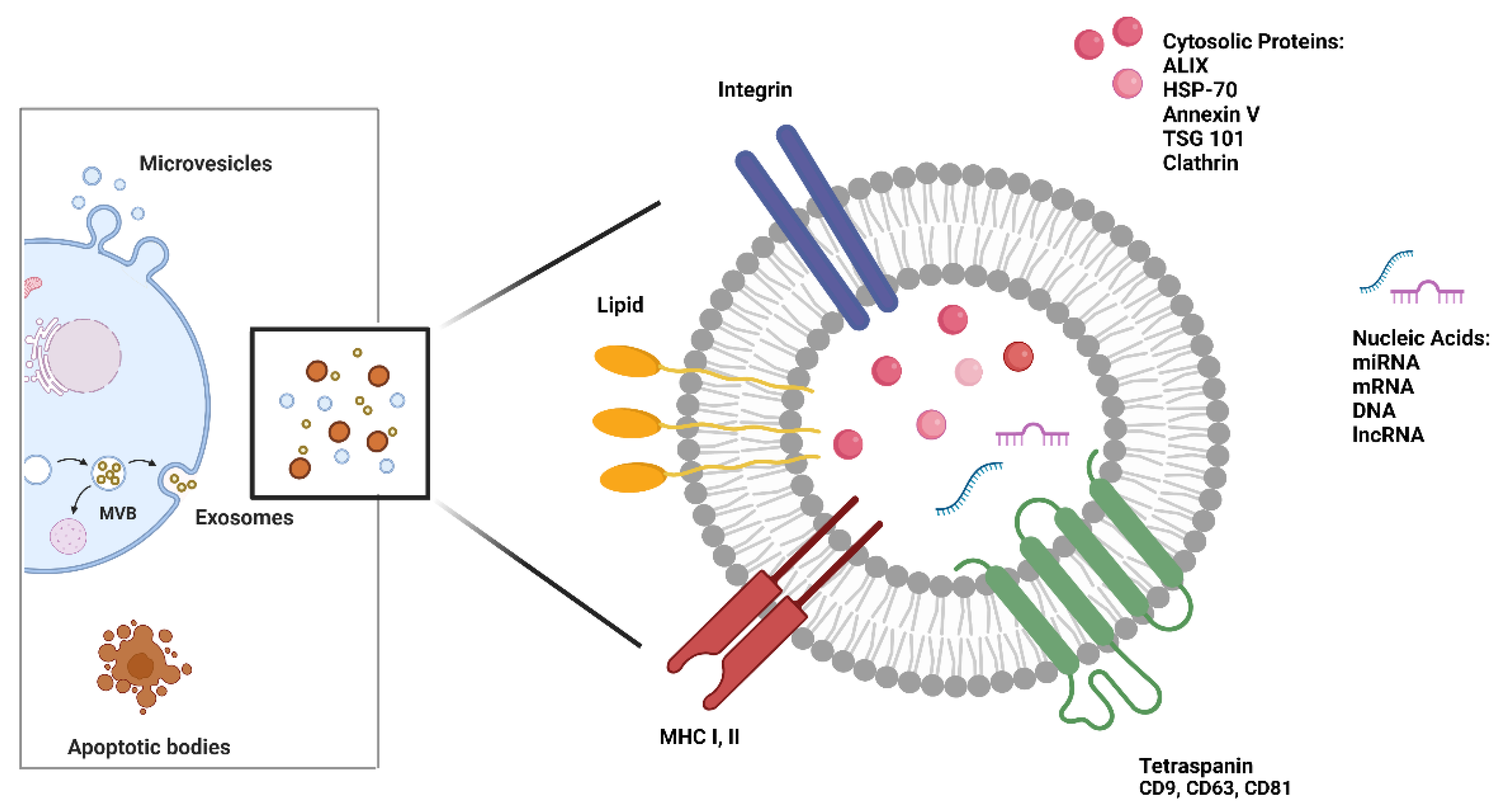
Figure 3.
Circulating microRNAs (miRNAs) are potential biomarkers for RCC. MiRNAs are emerging as promising biomarkers in RCC due to their potential triple role in clinical setting: several miRNAs result differentially expressed in tumor when compared with normal counterpart, showing a valid diagnostic value; experimental evidence also revealed the potential prognostic value of several miRNAs for appraisal of survival of RCC patients; their promising role as predictors of response to therapy may acquire a key importance in RCC providing clinicians with crucial information to determine the best treatment plan. Figure was generated with BioRender.
Figure 3.
Circulating microRNAs (miRNAs) are potential biomarkers for RCC. MiRNAs are emerging as promising biomarkers in RCC due to their potential triple role in clinical setting: several miRNAs result differentially expressed in tumor when compared with normal counterpart, showing a valid diagnostic value; experimental evidence also revealed the potential prognostic value of several miRNAs for appraisal of survival of RCC patients; their promising role as predictors of response to therapy may acquire a key importance in RCC providing clinicians with crucial information to determine the best treatment plan. Figure was generated with BioRender.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



