
Submitted:
11 April 2023
Posted:
12 April 2023
You are already at the latest version
Abstract
Background: Irish dance is growing in popularity, evolving to a more athletic and demanding dance style. Aims: To conduct a systematic review, previously registered with PROSPERO, to identify prevalence, incidence, and injury pattern among Irish dancers and analyse associated risk factors. Methods: Six online databases, plus two dance-specific science publications were searched systematically. Studies were included if the pattern of injuries among Irish dancers were evaluated or the factors associated with injury were analysed, published in English or Portuguese, in peer-reviewed scientific journals. Four reviewers assessed the quality and level of evidence using the Downs and Black criteria and a modified Oxford Centre of Evidence-Based Medicine 2009 model, respectively. Results: Eleven articles were included, 8 level 3c (cross-sectional) and 3 level 3b (prospective). Mean DB percentage score was 63% ± 7,2%. Prevalence ranged from 72,2% to 92,6%, affecting mostly the foot/ankle complex. Only 2 articles reported incidence, which ranged from 3,4–10,6 injuries/1000 hours danced depending on injury definition. Psychological factors, elite level, and insufficient/poor sleep were associated with musculoskeletal injury. Conclusions: Injury prevalence and incidence is high in Irish dancers, with the foot and ankle more affected. Due to heterogeneity in injury definitions, methods, and populations, along with the need for improvement in studies quality, recommendations were made for future research.
Keywords:
Irish dance
; injuries
; risk factors
; injury prevention
; epidemiology
; prevalence
; incidence
; surveillance system
1. Introduction
Irish dance has gained popularity all over the world and has become an extremely athletic and competitive activity [1,2]. This dance style is characterised for ballistic and explosive movements, numerous jumps, and rapid leg movement while the upper body remains upright, with the arms held at the side [3,4].
Irish and ballet dance styles have similar technique characteristics such as an ex-tended landing posture at initial contact (e.g., hip and knee extension, foot and ankle plantar flexion and erected spine), however ballet dancers have to smoothly “roll through their feet” upon landing using the demi-plié (hip and knee flexion and ankle dorsiflexion) [5,6]. On the other hand Irish dancers land on a plantar flexed foot position with an extended knee not taking advantage of the plié [1,7], which has been associate to dissipate landing forces [6] as well as to a pliable landing [8].
Due to the demanding characteristics of Irish dance and increasing competitiveness, it might increase the risk of injury, particularly in the lower extremities. However, there is only one systematic review (2013), regarding injuries in Irish dancers, that included two studies with limited quality and level of evidence [9]. Since then, there has been an increasing research regarding the epidemiology of Irish dance injuries [3,4,10,11,12,13,14,15,16].
A new systematic review including the most recent research will allow to further advance knowledge in this growing dance style; which is crucial for the development of effective injury prevention and intervention programs [17,18].
The main purpose of this study was to conduct a systematic review, to identify the injury pattern among Irish dancers and analyse the associated factors, comprising the most recent available evidence.
2. Materials and Methods
2.1. Protocol and Registration
This systematic review was conducted following the recommendations of PRISMA Statement for Reporting Systematic Reviews and Meta-Analysis [19]. The protocol was registered in advance with PROSPERO International prospective register of systematic reviews (registration number CRD42020163302).
2.2. Eligibility Criteria
Observational, prospective, retrospective, and cross-sectional studies published in English and Portuguese, in peer-reviewed scientific journals were included. Studies were included if they evaluated the pattern of injuries among Irish dancers and/or analysed factors associated with injury among Irish dancers. Case reports of injuries among Irish dancers or focusing on a specific injury or body part were excluded.
The main outcome measures included injury frequency (prevalence, incidence, injury rates); occurrence pattern of musculoskeletal injuries (which injuries, its nature, severity, and anatomic distribution); mechanism of injury; main associated factors. To include all relevant information no restrictions were applied to types of outcome measures nor to definitions of injury or type of data collection tools.
2.3. Search Strategy
Studies were identified by searching the following selected electronic databases: SCOPUS, PubMed, Web of science, Scielo, Lilacs and B-on, from their year of inception up to February 2020. The search strategy was also extended to two dance-specific science publications (Journal of Dance Medicine and Science and Medical Problems of Performing Artists). Additionally, a manual search of the references of articles identified in the database searches were screened. The last search was run in September 2020. One reviewer (ARP) developed and conducted the search. The following search keywords were used: “irish” AND “danc*” AND “injur*” OR “pain”. To search all databases, search terms were altered when necessary, e.g. “dance” or “dancer” or “dancing” instead of “danc*”. In the search strategy for PubMed the following query was used: irish danc* AND (injur* OR pain).
2.4. Selection Process
Screening was performed by reviewer ARP. Citations were imported to Mendeley Reference Manager (version 1.19.4) and duplicates were removed. When titles and abstracts revealed potential for inclusion, full text articles were obtained and independently assessed for eligibility by four reviewers (ARP, SS, AMA and RO), all Physiotherapists with experience in systematic reviews. Disagreements between reviewers were resolved by consensus.
2.5. Data Collection Process
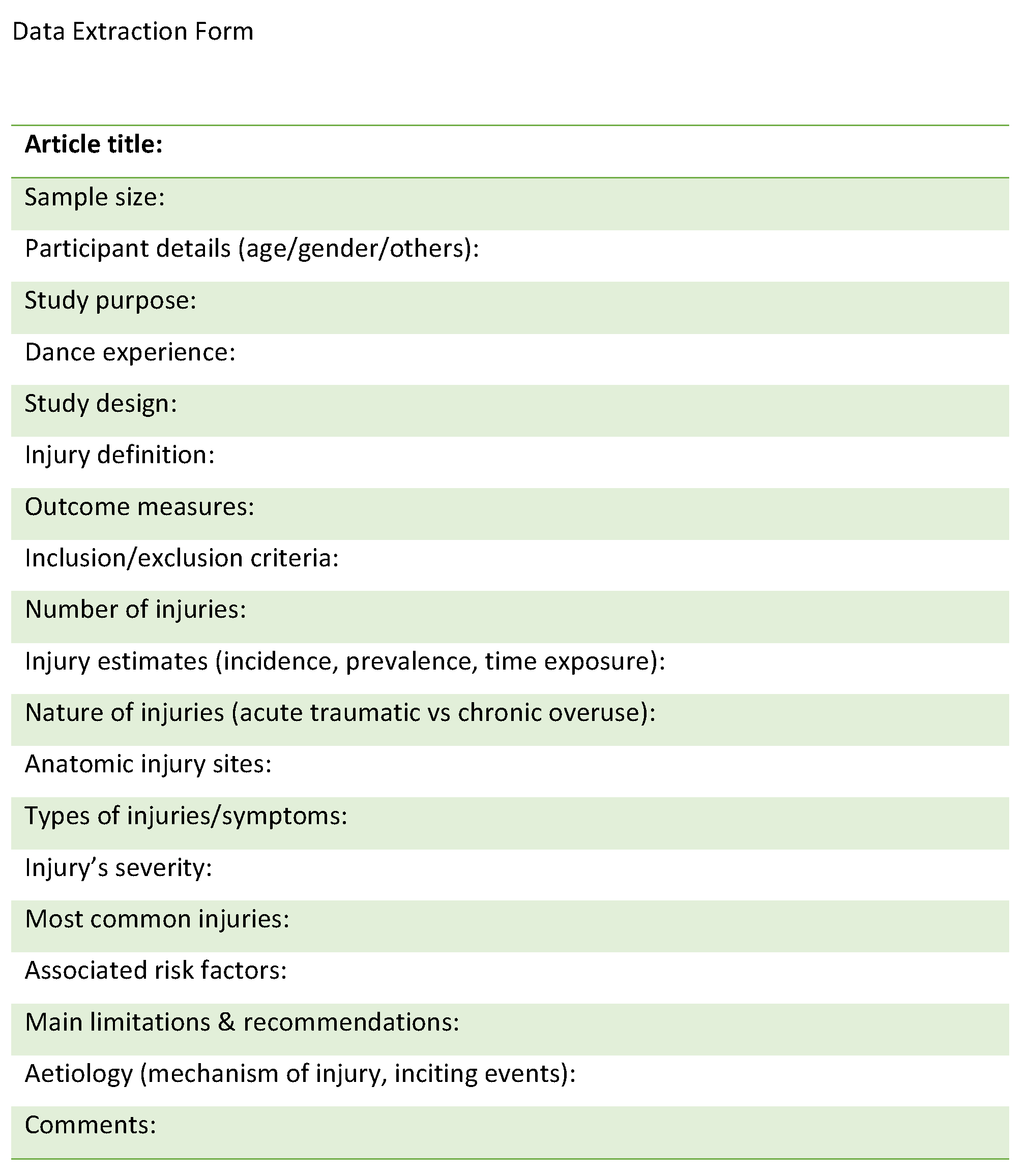
A data extraction form was created (Appendix A) and pilot-tested on each included paper by one reviewer (ARP). Corrections were discussed with another reviewer (RO) to improve data collection. Data were independently extracted and cross-checked by three reviewers (ARP, AMA and RO) and recorded in an Excel spreadsheet. Disagreements between individual judgements were resolved by consensus between reviewers.
For this systematic review, prevalence was defined as the proportion of existing cases and period prevalence was defined as the proportion of dancers that reported the condition of interest at any time during that given window. Incidence was defined as the number of new injuries in the population that develop during a defined period [20]. In articles where prevalence or period prevalence was not provided this was calculated providing the proportion of injured dancers during the study time frame.
2.6. Study Quality Assessment
There is a lack of a single tool for assessing susceptibility to bias of observational epidemiological studies [21]. Existing tools for assessing risk of reporting biases in studies have many limitations, for example they are not developed to appraise different study designs, i.e. each tool can be applied to a limited types of study designs, nor there is one single tool that appraises all sources of bias [22]. Risk of bias and quality of included studies were assessed using the Downs and Black (DB) quality assessment tool [23] and were conducted by four independent reviewers (ARP, CMC, SS and AMA). With the purpose to reduce checklists’ limitations in assessing the risk of bias [24], besides DB checklist, it was also asked to reviewers to access any potential source of bias in included studies.
The checklist was modified due to the included studies design. Twelve items were not applied to the included studies (items 4, 8, 9, 13–15, 17, 19, 23-24, 26-27) as they are related to intervention studies, and items 5, 21, and 22 were omitted for studies that did not provide an independent control group. The maximum achievable score for the included studies was 16. Scores were then presented as percentage scores [25].
The level of evidence of each study was categorised based on the Differential Diagnosis/Symptom Prevalence Study guidelines by the Oxford Centre for Evidence-Based Medicine (OCEBM) 2009 model [26]. The 2009 model has been considered more appropriate for the current dance science literature regarding the hierarchy of evidence and has been applied in previous systematic reviews [27,28]. As defined in inclusion criteria, levels 1a, 2a, 3a (systematic reviews), 4 (case series) and 5 (opinion-based papers) were not included. Cross-sectional studies were included in level 3, since this was the study design more frequently identified, thus the 2009 OCEBM model was modified adding the level 3c [27,28]. To access selective reporting bias, every article was examined for missing outcomes listed in the methods section that were not presented in the results [19].
3. Results
Results of the selection process are displayed in Figure 1. After full text screening, based on eligibility criteria, four articles were excluded, three were focused on a specific body area [7,29,30] and one was a case series study [31]. The manual search of the references of articles identified in the initial searches yielded no further articles. As findings of three studies were reported in six publications, a total of 11 articles were considered eligible for review, representing eight studies (for more information, see Table S1).
3.1. Study Characteristics
Characteristics of the 11 included articles are detailed in Table S1. Study design, data source and participant details are summarized in Table 1. Four articles did not present an explicit injury definition [2,10,12,15], four articles used injury definitions based on time-loss from dance, rehearsal, performance, training, or competition [3,13,14,32]. One article used a medical attention injury definition [16] and two articles defined injury as “any pain or injury that impacted upon their ability to dance” [4,11].
The included studies involved 865 participants and the mean number of participants per study was 108 (range 21-255). The overall sex ratio was 5,7/1 (female/male), and the total number of females reported was 735 (range 20-247) and males was 130 (range 0-67). Most samples were recruited from Irish dance schools [3,10,11,14,15], followed by University-level institutes of dance [4,12], performing productions, the An Coimisiun le Rinci Gaelacha and social media [3,14] or during a competition [32]. Medical records were from an academic sports medicine centre of a single company [2] and clinics at the investigators’ hospital [16].

Table 1.
Study Design, Data Source and Participant Details for Included Studies.
| Author (Year) | Study Design (Data Source) |
Sample size (n=) | Age (means ± SD (range) years | Sex (F/M) | Level | Dance experience (means ± SD years) |
|---|---|---|---|---|---|---|
| McGuinness et al. (2006) | Cross-sectional Retrospective (questionnaire 5y) | 159 | 18 ± 3 (15-27) | 142/17 | Competitors | 11 ± 4 (1-20) |
| Noon et al. (2010) | Cross-sectional retrospective (chart review 7y) | 69 | 13,1 (8-23) | 69/0 | 3 (compete in small, local competitions), 4 (as well as regional competitions) and 5 (qualify for international competitions) | Not reported |
| Stein et al. (2013) | Cross-sectional retrospective (medical records 11y) + Cross-sectional Retrospective (questionnaire) | 255 | 13,7 ± 5 (4 – 47), 95%<19 | 247/8 | Not reported | Not reported |
| Cahalan et al. (2013) | Cross-sectional (retrospective online questionnaire – entire career) | 178 | >18 72% (25-34) | 111/67 | Professional | 13,2 ± 3,4 |
| Eustergerling et al. (2015) | Cross-sectional retrospective questionnaire (1y) | 36 | 16 (12–46) | 35/1 | 22 elite/14 non-elite | Not reported |
| Cahalan et al. (2015) Cahalan et al. (2016) |
Cross-sectional retrospective (questionnaire 5y + physical screening) | 104 (questionnaire) 84 (physical screening) | Median (IQR) prof. 23 (21; 27,5), stud. 20 (19,22), comp. 20 (18,5; 20) | % prof. 50/50 stud. 85,7/14,3 comp. 80/20 |
Elite. 36 (34,6%) professionals, 28 (26,9%) students, 40 (38,5%) competitive | Prof. 17,5 ± 5,6 stud. 13,8 ± 5,3 comp. 13,0 ± 3,8 |
| Prospective cohort (1y) (online questionnaire every month) | 84 | Median (IQR) 20 (19-23,5) | 66/18 | Elite: Professional-15; Students-31; Competitive-38 | 14 (approx.) | |
| Cahalan, Kearney et al. (2018) Cahalan, Comber et al. (2019) |
Prospective (questionnaire every week over 1 year) | 21 ID + 29 CD | 21,5 ± 1,7 | 20/1 | Pre-professional students (full time students university) | “extensive dance experience” |
| Cross-sectional (retrospective questionnaire 1y + physical screening) | 27 ID | Median (IQR) 21(3) | 24/3 | Pre-professional students (full time students university) | “extensive dance experience” | |
| Cahalan, Bargary et al. (2019) Cahalan, Bargary et al. (2018) |
Prospective (questionnaire every week over 1 year) | 37 | 13-17 | 33/4 | Elite | Competing at open (elite) level for a period of at least 1 year |
| Cross-sectional (retrospective questionnaire 1y + physical screening) | 37 | 13-17 | 33/4 | Elite | Competing at open (elite) level for a period of at least 1 year |
Note. ID = Irish Dancers; CD = Contemporary Dancers.; IQR = interquartile range.
3.2. Risk of Bias and Level of Evidence
Table 2 presents the level of evidence and DB scores after adjustments for consensus between reviewers. The mean DB percentage score and standard deviation was 63% ± 7.2%. Four articles that did not report or give any injury definition [2,10,12,15], and none of included articles described confounders in each group of subjects to be compared (where applicable). Also, two articles did not provide measures of dispersion [2,16], and two did not report probability values [2,15].
Included articles failed in external validity as they had non-random sampling methods: convenience sampling [4,11,12,32], and volunteer sampling [3,10,13,14,15]. Furthermore, small sample size might be a limitation in included studies. Only one study mentioned a sample size calculation to determine an adequate sample size, but it was not referred how the calculation was proceeded [15].
Most articles accomplished internal validity concerning study bias, although one did not describe statistical analysis [2]. Plus, in two articles it was not possible to determine if the main outcome measures used were valid and reliable, as not all used questionnaires were validated [14,32] and one had a recall period of the entire career [14].
None of included articles met the DB criterion for reporting adjustment for confounding. Three studies, in statistical analysis, used multivariate regression modelling [3,11,13], however it is not clear that the purpose was adjustment for confounders, as no list of confounders were provided.
Level of evidence of most articles (8/11) were classified as level 3c (i.e., cross-sectional study design) [2,10,12,13,14,15,16,32]. The remaining three articles were classified as level 3b,prospective study design with limited population [3,4,11].
Table 2.
Modified Downs and Black Quality Assessment Tool Scores and Level of Evidence.
| Items/ Reference |
McGuinness et al. (2006) | Noon et al. (2010) | Stein et al. (2013) | Cahalan et al. (2013) | Eustergerling et al. (2015) | Cahalan et al. (2015) | Cahalan et al. (2016) | Cahalan, Bargary et al. (2018) | Cahalan, Kearney et al. (2018) | Cahalan, Comber et al. (2019) | Cahalan, Bargary et al. (2019) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Reporting | |||||||||||
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2 | 1 | 0a | 1 | 1 | 0 a | 1 | 1 | 0 a | 1 | 0 a | 1 |
| 3 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | NA | 0 |
| 6 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 7 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| External Validity |
|||||||||||
| 11 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Internal Validity (Bias) |
|||||||||||
| 16 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 18 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 20 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Internal Validity (Confounding) |
|||||||||||
| 21 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 1 |
| 22 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | NA | 1 |
| 25 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Score | 10 | 7 | 10 | 10 | 10 | 11 | 11 | 10 | 11 | 8 | 11 |
| Percentage Score (%) | 63 | 44 | 63 | 63 | 63 | 69 | 69 | 63 | 69 | 67 | 69 |
| Level of Evidence | 3c | 3c | 3c | 3c | 3c | 3c | 3b | 3c | 3b | 3c | 3b |
Note. NA: not applicable. a No injury definition.
3.3. Injury Estimates
The period prevalence varied from one year [3,10,11,12,15], five years [13,32] to the entire career [14] (ranges 72,2%-92,6%) (Figure 2), with more inclusive injury definitions presenting higher prevalence. Due to the heterogeneity of populations, time frame period, and different injury definitions in the included studies, an overall summary prevalence estimate could not be calculated.
From the three included prospective studies, two provided injury incidence according to two different injury definitions. When injuries were defined as any pain or injury, incidence ranged from 9,3-10,6 injuries per 1000 hours danced [4,11]. When injuries had a time-loss definition, injury incidence ranged from 3,4-4,5 injuries per 1000 hours danced [4,11].
3.4. Anatomical Location
Detailed anatomical location by each article is available in Table S1. The foot and ankle are the most affected body areas (25%-68%). Knee accounted for 9,6%-20% of injuries, followed by head/trunk (0%-33,9%), lower leg (0%-18,4%), hip/groin (2%-14%), and thigh (0%-12,3%). Upper extremity comprised 0%-5% of all injuries. Due to a different injury anatomical location classification across studies, anatomical locations were grouped into broader categories as presented in Figure 3. These categories of body regions were based on the International Olympic Committee consensus statement recommendations [20] along with the available information from the included studies.
3.5. Type of Injuries
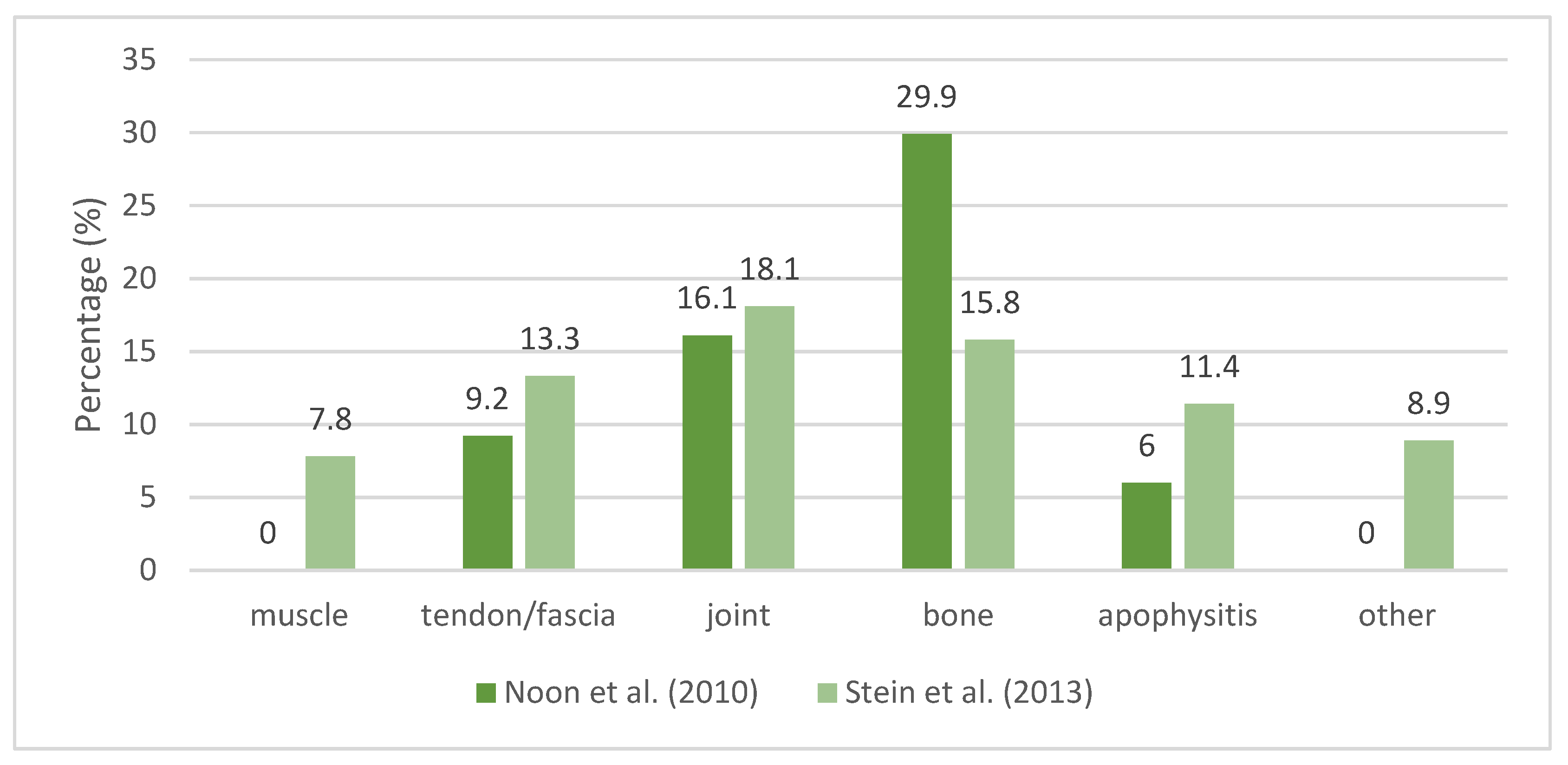
In studies where data source were medical records (Figure 4), Noon et al. [2] found stress fractures to be the most prevalent injury (29,9% of total injuries), affecting sesamoids, metatarsals, navicular, first proximal phalanx, and tibia. Patellofemoral pain syndrome (PFPS), Sever condition, ankle sprains, posterior tibialis tendonitis, and plantar fasciitis were the following most frequent diagnosis.
Stein et al. [16] reported that the most frequent type of injuries were tendon injury, apophysitis, patella pain or instability, stress injury (including medial tibial stress syndrome, stress reaction, and stress fracture), muscle injury, ligament injury and fracture (excluding stress fractures).
Figure 4.
The Distribution (%) of Injury Types Reported in Medical Records.
From the studies where data were self-reported (Figure 5), the most common type of injury was joint injuries, followed by muscle injuries and bone injuries. Frequently reported injuries in more than one study (self-reported injuries) are muscle strains, plantar fasciitis, tendinopathies, ankle sprains, stress fractures, patellofemoral pain, apophysitis and shin splints.
3.6. Nature, Severity and Aetiology of Injuries
Only three studies reported nature of injuries. Noon et al. [2] stated that the majority of injuries were overuse without providing magnitudes, Stein et al. [16] reported that 79,6% of injuries were overuse and 20,4% were acute or traumatic, and Cahalan et al. [12] reported the injury onset, where 33,3% were sudden onset, 36,4% gradual onset and 30,3% unsure or not stated.
Severity definitions, when provided, were all based on time-loss from dance performance and rehearsal. Most injuries were mild or moderate except in one study [13]. Mechanism of injury was not described in detail in any of the included studies. McGuinness and Doody [32] found that most injuries occurred before a major competition (58%) or when new steps were introduced (21%). In professional Irish dancers [14] 49,2% were injured mid-way through a production run and 10,8% had become injured in the rehearsal period of the production run. The most serious injuries occurred near the end of tour (20,8%) and in the early stages of touring (20%).
3.7. Associated Factors
4. Discussion
This systematic review highlights the high number of injuries affecting Irish dancers, mostly in the foot and ankle, with an overuse nature. Also, some risk factors were identified and the analysis of included studies methodology lead to recommendations for future studies.
4.1. Summary of Evidence
4.1.1. Prevalence/Incidence
Self-reported injury prevalence is higher in Irish dancers than in preprofessional [33] and professional ballet dancers [34], and tap dancers [35]. However, the included studies used different injury definition, population, and time frame period. The low prevalence (59%) of self-reported injuries (time-loss definition) in tap dancers [35] compared to Irish dancers might be because tap dance steps generate lower ground reaction forces (mean 2,06 ± 0.55 body weight), joint forces, and moments compared to Irish dance steps, whereas in Irish dance, it has been observed high ground reaction forces [36,37,38], and individual peak forces reaching up to 9,86 times body weight [38].
Three factors might underestimate injury prevalence in included studies: (i) a large recall period in retrospective studies, that may lead to errors of omission as minor injuries tend to be forgotten [39], (ii) time-loss injury definition [33,40,41], (iii) dancers not reporting all their injuries or complains and dancing through pain. This may be partially explained due to fear of stop dancing and a culture of injury/pain concealment, perseverance, and accepting or ignoring injury as well as the belief that pain is an inherent part of dancing [10,34,42,43].
The injury incidence was reported only in two studies [4,11] with different age group samples, and using small samples (n=21 and n=37), which make it difficult to draw any conclusions. Both studies report injury incidence higher than other dance styles [33,44,45,46,47,48] when using a non time-loss injury definition, although when using a time-loss definition, incidence fall within the same values for ballet [49,50].
4.1.2. Occurrence Pattern of Musculoskeletal Injuries
The higher number of injuries happened in the lower extremity (LE), where the foot and ankle are the most affected anatomical structures. Irish dance puts a tremendous demand on the LE, particularly in the foot-ankle complex [36,37,38]. Its explosive work, and associated effect of fatigue and subsequently increased anterior shear and compressive forces in the ankle [51], as well as the landing strategy used in Irish dance (e.g., extended knees and plantar flexed ankles) may play a key role to expose the foot-ankle complex to repetitive forces. For instance, Irish dance technique requires an extended landing posture, and dancing constantly on the toe tips and metatarsal heads, with repetitive forefoot push off [7,31]. Contrastingly, ballet dancers have a landing strategy adequate for better shock absorption: increased forefoot strategy at initial contact followed by an increased range of motion at the ankle and knee joints [52]. This likely prevents Irish dancers from attenuating ground reaction forces, as the foot-ankle complex excursion contributes to mitigate the landing forces [53,54], as well as hip and knee flexion [55,56].
Two studies report a high proportion of bone injuries, in particular stress fractures (29,9% of total injuries) [2], and stress injuries (10,1% of total injuries) [16] reported by healthcare professionals. This difference might be due to different sample characteristics, diagnostic methods (magnetic resonance imaging, clinical), and level/intensity of training. Moreover, Noon et al. [2] mention that most dancers (79,7%) had multiple recorded injuries, and a repeat injury was counted as a second injury, which might over represent the proportion of stress fractures. While one study the sample was composed of female dancers from a single Irish dance company (n=69) [2], the other was composed of 255 dancers from 37 different schools [16], therefore may be more representative.
Stress fractures, as an overuse injury, result from submaximal, repetitive loading [57]. Noon et al. [2] relates the high proportion of sesamoid stress fractures to repetitive stamping, frequent jumps and high-impact landings and compensatory turnout (foot pronation and metatarsophalangeal joint valgus rather than external hip rotation). Indeed, activities with repeated submaximal stresses and new or excessive exercise patterns with limited rest are risk factors for stress fractures [58].
Footwear and hard surface training are also potential risk factors for stress fractures [59]. It was found that the different footwear worn by Irish dancers exert significantly different forces on the dancers’ feet, particularly in the forefoot region, with soft shoe resulting in higher plantar loads, compared to hard shoe and dance trainer [60]. Also, it was observed that split sole sneakers (also known as dance trainers) were associated with a decreased incidence of injury in Irish dancers [32]. The frequent time spent dancing on soft shoes, plus dancing on a hard surface, along with the repetitive movements with considerable impact, without plié on landing, may indicate that excessive external training load contributes to stress fractures in Irish dancers.
Patella pain or instability and PFPS accounted for 10,8% and 11% of injuries [2,16]. In a retrospective chart review study characterising knee injury pattern in young Irish dancers, the most frequent diagnoses (53,5% of knee injuries) were related to patellar tracking disorders, including PFPS, hypermobile patella, and patellar sub-luxation [29]. In ballet, it is well documented the effects of forcing lower extremities turnout, through compensatory strategies elsewhere along the kinetic chain, leading to feet pronation, external tibial torsion, valgus knee stress, increased Q angle, and lateral patellar tracking [61,62]. As turned-out lower extremities is a common characteristic of Irish dance and ballet, it could be implicated in patellar tracking disorders in Irish dancers.
Also, Irish dance repetitive movements with considerable load might contribute for overuse injuries, in particular PFPS, especially when fatigued, with Irish dancers presenting a significant greater external knee-flexion moments in landing [51]. Besides, Irish dancers can have a demanding calendar of practice and competition, with irregular spikes and dips in dance exposure [4,10]. Thus, it is paramount to monitor and manage workload, to ensure gradual adaptation to the required loads, prevent spikes in loads, and to enhance physical qualities [63]. Moreover, periodisation of training should be implemented for prevention of overtraining, underperformance, and increased injury occurrence [64].
The six included studies describing self-reported injury type have considerable variability, as the data were provided by dancers that may have a diagnosis from a licensed healthcare practitioner or may not. This means that data depended on recall (in retrospective surveys) and could not always have an accurate or valid diagnosis, thus raising questions about the validity of these results [17], especially taking into account that injury diagnosis is not very reliably recalled [65]. Three articles have long recall periods making them more vulnerable to effects of recall bias [13,14,32]. In one study it was asked to recall the three most recent injuries in the previous five years [32], which can result in dancers reporting the most serious injuries to them, and missing those with least impact. Also, the referred six studies did not use a validated questionnaire, or it was not possible to determine the validity and reliability of the questionnaire to obtain injury type data.
Considering all the mentioned methodological limitations, results show a trend to muscle and joint to be the most affected by injury, followed by bone. It should be noted that injury types presented in the category “other (not discriminated)” represent a considerable proportion, that may possibly influence the observed results, further limiting their interpretation. In addition, two articles are part of the same study, with the same sample but different study design: one prospective [11], and the other cross-sectional [10]. Three studies report that a large proportion of dancers were unaware of diagnosis [4,11,13] which further limits the possibility to draw conclusions about injury type.
None of included articles described mechanism of injury in detail. Nature of injuries were reported in only three studies: mostly overuse [2,16] or with a gradual onset [12]. Despite nature of injuries are not reported in other included studies, it can be hypothesised that types of injuries are mostly overuse in nature. Although the injury mechanism is not described, frequently reported injuries in included studies (e.g., plantar fasciitis, tendinopathies, stress fractures, PFPS, apophysitis and shin splints) are injuries usually caused by repetitive microtrauma, thus with more potential for prevention.
Irish and ballet dances are highly demanding and the nature of injury in both is predominantly by overuse [47,66]. Together with insufficient physical preparation, poor planning of training/rehearsals [28], faulty technical execution [67], repetitive movements without adequate rest [68], competitive environment, perfectionist mindsets, and consequent psychosocial distress [69,70], along with dancer’s increased pain tolerance [71], can make them vulnerable to overuse injuries. Additionally, it seems that Irish dancers do not benefit of the landing technique used in ballet to mitigate the landing forces, most likely aggravating the risk for overuse injuries in the LEs.
For development of injury prevention programs it is essential to better understand the causes of an injury in a specific context, and the risk factors [72,73]. Given the complexity of mechanisms precipitating an injury, especially overuse injuries, multidisciplinary approaches and a combination of different research approaches are needed [73,74].
Cahalan and colleagues [3,4,11,13,14] provide an insight of Irish dancer’s perceived causes of injuries. The most frequently mentioned self-perceived cause of injury was overuse and fatigue, which is in accordance with the literature regarding dance [75,76] and circus [77]. This is an important clue that training load should be monitored and managed, as it is already practiced in the sports field [78,79,80].
Most injuries’ severity appears to be mild, although that is not clear. Studies used a time-loss severity definition which has some limitations. First, dancers may be able to participate before an injury has fully resolved with technique adaptations [20], or they can “soldier on” with their injury [14], or injuries might not result in absence from dance [4]. Second, many injuries are of gradual onset, chronic or recurrent, not reflecting the true severity, as dancers can have low time-loss, but be affected in content and intensity of training/performance. The above-mentioned aspects would tend to underestimate the absolute severity of injuries if one considered full healing as the gold standard [20].
4.1.3. Associated Factors
Most included studies analysing risk factors had a cross-sectional design and/or only reported associations or used univariate tests. This approach is not adequate to the multifactorial nature of sports/dance injuries and does not address the complex interactions among several risk factors. Nevertheless, these studies provide data to guide the identification of risk factors that can be analysed in longitudinal studies, with analytical approaches that incorporate repeated measures (monitoring variables over time) and using a multivariate statistical approach.
Regarding demographic factors, only two studies examined the relation between gender and injury, with conflicting results. Age also remains inconclusive, but there is a trend to more injuries with increasing age. In ballet dancers, evidence about age as a risk factor is inconclusive as well [27,28]. Although gender and age are non-modifiable factors, it is important to know if they can influence other variables, so they can be adjusted for confounding.
In the included studies examining dance exposure, results do not suggest a relation to injury. These data were collected on retrospective questionnaires, with possible errors associated to recall, and there was a great variability in the cohort regarding: the number of hours/week spent at dancing classes, the number of hours/week spent practicing at home; and the number of competitions/year [32]. The number of participants in the prospective cohort study is small (n=27), and dance exposure was self-reported [4].
On the other hand, in the prospective study with elite adolescent Irish dancers, increased weekly hours of dance training were associated with a decreased total number of weeks injured, suggesting dance load as a protective factor [11]. In this cohort weekly dance exposure was also low (mean=7,9 hours/week), comparing to ballet. In elite level ballet company, dancers can perform a mean of 34 hours per week [81], and pre-professional ballet dancers can perform an average of 30,3 hours per week [82].
Dance exposure has been identified as a possible risk factor in ballet and contemporary dancers, albeit evidence remains inconclusive [27]. Although there is evidence of a relationship between training load and injury in competitive athletes [83], load as a single factor does not explain nor is predictive of all injuries [84], because of the complexity and multifactorial nature of injury aetiology [85]. Load could be analysed coupled with other variables to identify dynamic interactions [84,85]. Two of the included studies examining dance exposure simply compared means [4,32], and one used statistical tests that assume linearity of relationships [11].
Also, the included studies only used an external measure of training load (dance hours/week). Hours per week of dance is likely not the best external load measure for comparison with other dance styles, because of the ballistic and explosive nature of Irish dance.
Only one study investigated the impact of physical growth on injury in elite Irish dancers. This prospective study found no relationship between total number of injuries or the total number of weeks injured, and change in weight or height [11]. In elite adolescent ballet dancers it was found that rate of growth (foot length change) is likely associated with a small to moderate increase in risk of lumbar and lower extremity overuse injury [86]. Since apophysitis is frequently reported in included studies, it would be plausible to find a relation between rate of growth and injury in Irish dancers. Some possible explanations are the different methodology to access growth, and the age of the included study cohort (aged 13-17) and the median growth in height (3, IQR=2, 7 cm), which may reflect that most of these dancers were not in the period around the peak height velocity, when there is an increased risk of injuries in elite sporting populations [87,88,89]. Also, the dance exposure in the Irish dance cohort was low (mean=7,9 hours/week), and most participants reported their sleep quality as being good or very good [11].
Irish dancers competing at a higher level seem to be at higher risk of injury. One study found that dancers at an elite level were more likely to report an injury than dancers who were non elite (OR=6.33, CI 1.27–31.57) [15]. Additionally, it was observed that the average number of injuries per dancer increased as the dancer’s skill level increased [2]. This might be related to the increased dance exposure of higher levels, the more complex and demanding choreography, as well as the greater competitiveness and related psychosocial stressors. Conversely, years of participation in Irish dance do not appear to relate with injury.
Cross-training was examined as possibly related to lower injury rates in four studies, but no significant correlation was found [3,13,14,15]. Neither studies provide the components of cross-training activities reported, and dancers undertook little weekly cross-training or none at all [10,11,14].
Performing a warm-up and cool-down were associated with a decreased incidence of ankle injury [32]. In a prospective study, failing to always perform a warm-up was significantly associated (p=0,042) with foot and ankle pain and injury in elite adult Irish dancers [90]. Two studies found no significant correlation with injury, but there was a great compliance with warm-up and cool-down in this cohort [14], which makes it difficult to assess their impact on injury, and the proportion of dancers who perform a warm-up or cool-down was not provided [15]. Also, none of referred studies described in detail the components of warm-up or cool-down. Therefore, despite the limitations of included studies, performing a warm-up and cool-down is likely an important factor for injury prevention.
None of the three included studies examining physical factors found significant associations with pain/injury. This is conflicting with the evidence regarding ballet dancers, where several physical factors were identified, such as anthropometrics, poor aerobic capacity, hypermobility, degree of turnout, core and LE weakness, and range of motion discrepancies of the LE [27,28,91,92].
Firstly, two articles report data from the same study (one is cross-sectional and the other is prospective), and physical variables were within normal values [3,13]. Also, in the prospective study, physical variables were measured only at the baseline which does not account for temporality [93], as they could change over time.
Secondly, some physical variables measured might not be sensible or adequate for the Irish dance population. For example, the Movement Competency Screen includes movements that might not be relevant for Irish dancers, such as the push up, because Irish dancers keep their arms close to the torso while dancing and the injury proportion of the upper extremities is negligible. Also, physical endurance was measured with plank [10], which does not address other important muscle groups. For instance, calf endurance would likely be important to access, since Irish dancers are most of the time on toes (standing on the forefoot with ankle plantar flexion) and repeatedly jump and land also on toes.
Thirdly, injury aetiology is complex and multifactorial [85,94], and it is unlikely that a single physical factor will predict injury. Included studies examining physical factors focused on the contribution of isolated factors.
Regarding general health complains, most of included studies reported consistently an association with injury [3,4,11,13]. These results emphasise the importance of including general health complains (beyond musculoskeletal complains) in screening tools for dancers.
From the strongest level of evidence in included studies (i.e., prospective cohort design), findings are in accordance with the literature [95,96,97] as insufficient sleep was associated with more pain/injury [3], and participants with better sleep, had fewer days lost due to injury [4]. In other cohort there was no association with sleep quality and injury, but most dancers reported good or very good sleep quality [11].
Psychosocial factors were moderately represented in included studies, with only Cahalan and co-workers examining these factors. The number of psychological health complains or problems were significantly associated with injury [13,14] or close to statistical significance (p = 0,054) [3].
It was also identified that psychological distress was common among professional Irish dancers, with “general anxiety”, “tension with other people”, “stress due to external factors,” “performance anxiety”, and “overuse of drugs or alcohol,” frequently reported when working as a professional Irish dancer [14]. In elite adult Irish dancers, it was found that scoring poorly on two subscales of the Athletic Coping Skills Inventory (coping with adversity, and goal setting and mental preparation) was significantly associated with foot and ankle pain and injury [90].
In elite adolescent athletes, self-esteem is a risk factor for injury [98], assessed by the Competence-Based Self-Esteem Scale, which describes contingent self-esteem dependent on competence as well as self-criticism and feeling of insufficiency [99]. Most Irish dancers participate in competition-based activity [43], and it has been observed that some competitive Irish dancers are ego-motivated [12], possibly experiencing shame and loss of self-esteem when they cannot achieve expected results [100].
Despite all the evidence about the importance of psychosocial factors in injury risk, and recommendations to include them in screening [101] as well as in injury epidemiology research [72,85], non-physical factors still need to be better integrated [17,102]. A better knowledge of psychological, social and contextual factors not only are crucial for studying injury aetiology but also for injury recovery, and for risk factors management in injury prevention strategies [43,103,104,105]. Furthermore, Irish dancers rarely point out psychological factors as perceived causes of injuries [3,4,11,13,14], and therefore education might play a relevant role to increase awareness.
Overall, associated factors identified in this systematic review require an in-depth investigation, due to the heterogeneity of factors assessed, different methods, and low level of evidence of included studies (mostly cross-sectional). Moreover, those with prospective design did not use repeated measures, and one prospective study did not measure exposure, preventing from calculating incidence and risk.
None of included studies clearly identify potential confounders. Despite it is debatable that confounding should be addressed only in studies with causal questions [106,107], we argue that in studies investigating non-causal associations should, at least, be identified/anticipated and analysed the role of additional variables, for example, with subgroup stratification or using a multivariate statistical approach [108,109]. This would help the reasoning for designing studies investigating why dancers sustain injuries, providing evidence for the development of intervention programs for injury prevention.
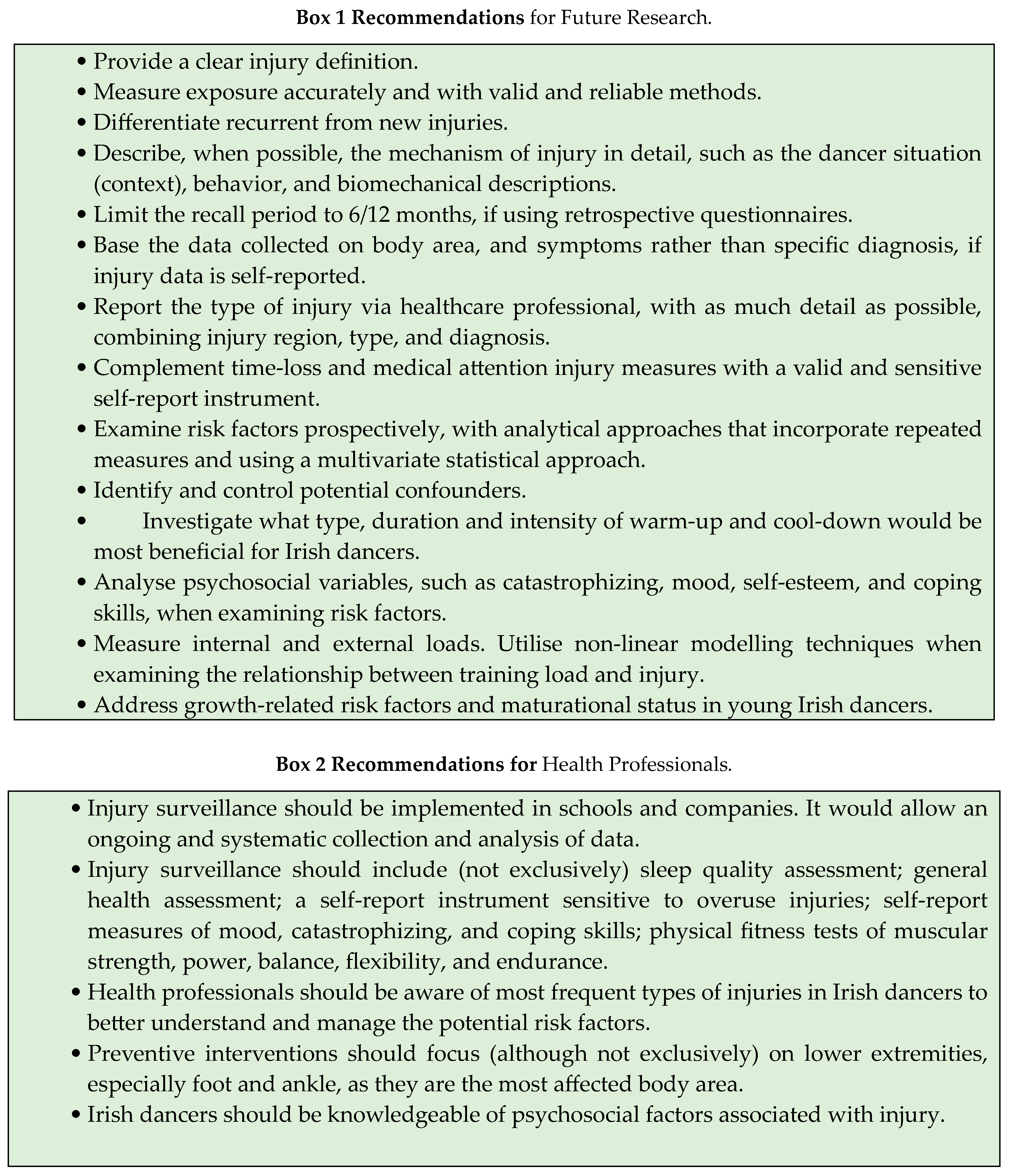
Based on the findings of this systematic review, a summary of recommendations for future research is presented in Box1, as well as recommendations for health professionals (Box2).
4.4. Limitations
This SR has some limitations which are related to methodological aspects and level of evidence of the included studies. Heterogeneity in injury definition, outcome measures, and methods of data collection hampers comparison. Four studies did not report a clear injury definition, compromising validity. Most studies used retrospective questionnaires, and three had a recall period superior to one year, which makes them prone to recall bias [65]. Many dancers did not have an injury diagnosis, and the accuracy of self-reported injury is highly questionable [17]. Also, in most studies it was not possible to determine the validity and reliability of the questionnaire to obtain injury type data. Female dancers were 5,7 times more represented in included studies, thus results may not be generalisable to male dancers.
Studies analysing associated factors did not control for potential confounders, limiting the accuracy of results [110]. Also, most included studies did not assess of potential interaction of risk factors, and none used repeated measures. Most studies were conducted by the same authors, and three studies resulted in six articles, decreasing the overall sample size. Injury recurrence and injury mechanism was not fully explored in most of included studies.
In this systematic review only studies written in English or Portuguese language were included published in peer-reviewed scientific journals, to assure quality and validity.
5. Conclusions
In the present systematic review, it is notorious the high number of injuries affecting Irish dancers, mostly in the foot and ankle, which is likely explained by the great demands placed on these functional units. Bone or muscle/joint injuries were the most common type, depending on the reported data method, and psychological factors, elite level, failure to complete a warm-up, health complains, and insufficient/poor sleep are associated with injury. Considering that Irish dance is such a demanding dance style, especially for the LE, and that there is still lacking studies of high level of evidence, more studies are needed to improve performance and reduce injuries in this growing population of dancers.
Quality of studies must be improved by providing a clear injury definition, use of validated tools, and measuring exposure, to allow for calculating incidence and risk. Studies examining risk factors, should use a methodology that considers the multifactorial nature of dance injuries and the complex interactions among risk factors. Future studies should use a prospective study design, with analytical approaches that incorporate repeated measures and use a multivariate statistical approach. An effort should be done to identify and control for confounders.
Although some advances in Irish dance injury epidemiology were made, there is still lacking high-quality studies to allow deep knowledge in this area to enable the development and implementation of effective injury prevention and intervention programmes. Because of the high levels of injury in Irish dancers, and the evolution to an athletic style, Irish dance schools and companies would benefit of an injury surveillance system.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Consensus Data Extracted
Author Contributions
Conceptualization and methodology, A.R.P. and R.O.; formal analysis, A.R.P., S.S., C.C., A.M.A. and R.O.; investigation and writing—original draft preparation, A.R.P.; writing—review and editing, A.R.P., C.C., A.M.A. and R.O.; supervision, R.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data can be requested from the authors.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
References
- Foley, C. Perceptions of Irish Step Dance: National, Global, and Local. Danc. Res. J. 2001, 33, 34. [CrossRef]
- Noon, M.; Hoch, A.Z.A.Z.A.Z.; McNamara, L.; Schimke, J. Injury Patterns in Female Irish Dancers. PM R 2010, 2, 1030–1034. [CrossRef]
- Cahalan, R.; O’Sullivan, P.; Purtill, H.; Bargary, N.; Ni Bhriain, O.; O’Sullivan, K. Inability to Perform Because of Pain/Injury in Elite Adult Irish Dance: A Prospective Investigation of Contributing Factors. Scand. J. Med. Sci. Sport. 2016, 26, 694–702. [CrossRef]
- Cahalan, R.; Kearney, P.; Ni Bhriain, O.; Redding, E.; Quin, E.; McLaughlin, L.C.L.C.L.C.; O’ Sullivan, K. Dance Exposure, Wellbeing and Injury in Collegiate Irish and Contemporary Dancers: A Prospective Study. Phys. Ther. Sport 2018, 34, 77–83. [CrossRef]
- Gans, A. The Relationship of Heel Contact in Ascent and Descent from Jumps to the Incidence of Shin Splints in Ballet Dancers. Phys. Ther. 1985, 65, 1192–1196. [CrossRef]
- Orishimo, K.F.; Kremenic, I.J.; Pappas, E.; Hagins, M.; Liederbach, M. Comparison of Landing Biomechanics between Male and Female Professional Dancers. Am. J. Sports Med. 2009, 37, 2187–2193. [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, P.; O’Sullivan, K. Foot and Ankle Pain and Injuries in Elite Adult Irish Dancers. Med. Probl. Perform. Art. 2014, 29, 198–206. [CrossRef]
- Ward, R.E.; Fong Yan, A.; Orishimo, K.F.; Kremenic, I.J.; Hagins, M.; Liederbach, M.; Hiller, C.E.; Pappas, E. Comparison of Lower Limb Stiffness between Male and Female Dancers and Athletes during Drop Jump Landings. Scand. J. Med. Sci. Sport. 2019, 29, 71–81. [CrossRef]
- Cahalan, R.; O’Sullivan, K. Musculoskeletal Pain and Injury in Irish Dancing: A Systematic Review. Physiother. Pract. Res. 2013, 34, 83–92. [CrossRef]
- Cahalan, R.; Bargary, N.; O’Sullivan, K. Pain and Injury in Elite Adolescent Irish Dancers: A Cross-Sectional Study. J. Danc. Med. Sci. 2018, 22, 91–99. [CrossRef]
- Cahalan, R.; Bargary, N.; O’Sullivan, K. Dance Exposure, General Health, Sleep and Injury in Elite Adolescent Irish Dancers: A Prospective Study. Phys. Ther. Sport 2019, 40, 153–159. [CrossRef]
- Cahalan, R.; Comber, L.; Gaire, D.; Quin, E.; Redding, E.; Ni Bhriain, O.; O’Sullivan, K. Biopsychosocial Characteristics of Contemporary and Irish University-Level Student Dancers A Pilot Study. J. Danc. Med. Sci. 2019, 23, 63–71. [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, P.; O’Sullivan, K. A Cross-Sectional Study of Elite Adult Irish Dancers: Biopsychosocial Traits, Pain, and Injury. J. Dance Med. Sci. 2015, 19, 31–43. [CrossRef]
- Cahalan, R.; O’Sullivan, K. Injury in Professional Irish Dancers. J. Danc. Med. Sci. 2013, 17, 150–158. [CrossRef]
- Eustergerling, M.; Emery, C. Risk Factors for Injuries in Competitive Irish Dancers Enrolled in Dance Schools in Calgary, Canada. Med. Probl. Perform. Art. 2015, 30, 26–29. [CrossRef]
- Stein, C.J.; Tyson, K.D.; Johnson, V.M.; Popoli, D.M.; D’Hemecourt, P.A.; Micheli, L.J. Injuries in Irish Dance. J. Dance Med. Sci. 2013, 17, 159–164. [CrossRef]
- Liederbach, M.; Hagins, M.; Gamboa, J.M.; Welsh, T.M. Assessing and Reporting Dancer Capacities, Risk Factors, and Injuries: Recommendations from the IADMS Standard Measures Consensus Initiative. J. Dance Med. Sci. 2012, 16, 139–153.
- Van Mechelen, W. Sports Injury Surveillance Systems: “One Size Fits All?” Sport. Med. 1997, 24, 164–168. [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339. [CrossRef]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee Consensus Statement: Methods for Recording and Reporting of Epidemiological Data on Injury and Illness in Sport 2020 (Including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 32. [CrossRef]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for Assessing Quality and Susceptibility to Bias in Observational Studies in Epidemiology: A Systematic Review and Annotated Bibliography. Int. J. Epidemiol. 2007, 36, 666–676.
- Page, M.J.; McKenzie, J.E.; Higgins, J.P.T. Tools for Assessing Risk of Reporting Biases in Studies and Syntheses of Studies: A Systematic Review. BMJ Open 2018, 8, 1–16. [CrossRef]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [CrossRef]
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bradley, J.M.; Baxter, G.D.; McDonough, S.M. Failure of a Numerical Quality Assessment Scale to Identify Potential Risk of Bias in a Systematic Review: A Comparison Study. BMC Res. Notes 2015, 8. [CrossRef]
- Moita, J.P.; Nunes, A.; Esteves, J.; Oliveira, R.; Xarez, L. The Relationship between Muscular Strength and Dance Injuries: A Systematic Review. Med. Probl. Perform. Art. 2017, 32, 40–50. [CrossRef]
- Howick, J.; Phillips, B.; Ball C, et al. Oxford Centre for Evidence-Based Medicine: Levels of Evidence Secondary Oxford Centre for Evidence-Based Medicine: Levels of Evidence 2009. 2009, 2009.
- Kenny, S.J.; Whittaker, J.L.; Emery, C.A. Risk Factors for Musculoskeletal Injury in Preprofessional Dancers: A Systematic Review. Br. J. Sports Med. 2016, 50, 997–1003. [CrossRef]
- Biernacki, J.; Stracciolini, A.; Fraser, J.; Micheli, L.; Sugimoto, D. Risk Factors for Lower-Extremity Injuries in Female Ballet Dancers. Clin. J. Sport Med. 2018, 1. [CrossRef]
- Beasley, M.A.; Stracciolini, A.; Tyson, K.D.; Stein, C.J. Knee Injury Patterns in Young Irish Dancers. Med. Probl. Perform. Art. 2014, 29, 70–73. [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, K. Biopsychosocial Factors Associated with Foot and Ankle Pain and Injury in Irish Dance: A Prospective Study. Med. Probl. Perform. Art. 2017, 32, 111–117. [CrossRef]
- Walls, R.J.J.; Brennan, S.A.A.; Hodnett, P.; O’Byrne, J.M.M.; Eustace, S.J.J.; Stephens, M.M.M.; O’Byrne, J.M.; Eustace, S.J.J.; Stephens, M.M.M. Overuse Ankle Injuries in Professional Irish Dancers. Foot Ankle Surg. 2010, 16, 45–49. [CrossRef]
- McGuinness, D.; Doody, C. The Injuries of Competitive Irish Dancers. J. Danc. Med. Sci. 2006, 10, 35–39.
- Kenny, S.J.; Palacios-Derflingher, L.; Whittaker, J.L.; Emery, C.A. The Influence of Injury Definition on Injury Burden in Preprofessional Ballet and Contemporary Dancers. J. Orthop. Sports Phys. Ther. 2018, 48, 185–193. [CrossRef]
- Jacobs, C.L.; Cassidy, J.D.; Côté, P.; Boyle, E.; Ramel, E.; Ammendolia, C.; Hartvigsen, J.; Schwartz, I. Musculoskeletal Injury in Professional Dancers: Prevalence and Associated Factors: An International Cross-Sectional Study. Clin. J. Sport Med. 2017, 27, 153–160. [CrossRef]
- Mayers, L.; Judelson, D.; Bronner, S. The Prevalence of Injury among Tap Dancers. J. Danc. Med. Sci. 2003, 7, 121–125.
- Shippen, J.M.; May, B. Calculation of Muscle Loading and Joint Contact Forces during the Rock Step in Irish Dance. J. Danc. Med. & Sci. Off. Publ. Int. Assoc. Danc. Med. & Sci. 2010, 14, 11–18.
- Radcliffe, C.R.; Coltman, C.E.; Spratford, W.A. The Effect of Fatigue on Peak Achilles Tendon Force in Irish Dancing-Specific Landing Tasks. Sport. Biomech. 2021, 00, 1–14. [CrossRef]
- Christensen, S.K.; Johnson, A.W.; Van, N.; Corey, T.E.; Mcclung, M.S.; Hunter, I. Characteristics of Eight Irish Dance Landings Considerations for Training and Overuse Injury Prevention. J. Danc. Med. Sci. 2021, 25, 30–37. [CrossRef]
- Junge, A.; Dvorak, J. Influence of Definition and Data Collection on the Incidence of Injuries in Football. Am. J. Sports Med. 2000, 28, 40–46. [CrossRef]
- Bronner, S.; Ojofeitimi, S.; Mayers, L. Comprehensive Surveillance of Dance Injuries A Proposal for Uniform Reporting Guidelines for Professional Companies. J. Danc. Med. Sci. 2006, 10, 69–80.
- Clarsen, B.; Bahr, R. Matching the Choice of Injury/Illness Definition to Study Setting, Purpose and Design: One Size Does Not Fit All! Br. J. Sports Med. 2014, 48, 510–512. [CrossRef]
- Mainwaring, L.; Krasnow, D.; Kerr, G. And The Dance Goes On: Psychological Impact of Injury. J. Danc. Med. Sci. 2001, 5, 105–115.
- Higginbotham, O.; Cahalan, R. The Collegiate Irish Dancer’s Experience of Injury: A Qualitative Study. Med. Probl. Perform. Art. 2020, 35, 1–9. [CrossRef]
- Gamboa, J.M.; Robert, L.A.; Fergus, A. Injury Patterns in Elite Preprofessional Ballet Dancers and the Utility of Screening Programs to Identify Risk Characteristics. J. Orthop. Sports Phys. Ther. 2008, 38, 126–136. [CrossRef]
- Luke, A.C.; Kinney, S.A.; D’Hemecourt, P.A.; Baum, J.; Owen, M.; Micheli, L.J. Determinants of Injuries in Young Dancers. Med. Probl. Perform. Art. 2002, 17, 105–112.
- Allen, N.; Ribbans, W.; Nevill, A.; Wyon, M. Musculoskeletal Injuries in Dance: A Systematic Review. Int. J. Phys. Med. Rehabil. 2014, 03. [CrossRef]
- Smith, P.J.; Gerrie, B.J.; Varner, K.E.; McCulloch, P.C.; Lintner, D.M.; Harris, J.D. Incidence and Prevalence of Musculoskeletal Injury in Ballet A Systematic Review. 2015, 1–9. [CrossRef]
- Vassallo, A.J.; Trevor, B.L.; Mota, L.; Pappas, E.; Hiller, C.E. Injury Rates and Characteristics in Recreational, Elite Student and Professional Dancers: A Systematic Review. J. Sports Sci. 2019, 37, 1113–1122. [CrossRef]
- Caine, D.; Bergeron, G.; Goodwin, B.J.; Thomas, J.; Caine, C.G.; Steinfeld, S.; Dyck, K.; André, S. A Survey of Injuries Affecting Pre-Professional Ballet Dancers. J. Dance Med. Sci. 2016, 20, 115–126. [CrossRef]
- Allen, N.; Nevill, A.; Brooks, J.; Koutedakis, Y.; Wyon, M. Ballet Injuries: Injury Incidence and Severity over 1 Year. J. Orthop. Sports Phys. Ther. 2012, 42, 781–790. [CrossRef]
- Wild, C.Y.; Grealish, A.; Hopper, D. Lower Limb and Trunk Biomechanics after Fatigue in Competitive Female Irish Dancers. J. Athl. Train. 2017, 52, 643–648. [CrossRef]
- Azevedo, A.M.; Oliveira, R.; Vaz, J.R.; Cortes, N. Professional Dancers Distinct Biomechanical Pattern during Multidirectional Landings. Med. Sci. Sports Exerc. 2019, 51, 539–547. [CrossRef]
- Azevedo, A.M.; Oliveira, R.; Vaz, J.R.; Cortes, N. Oxford Foot Model Kinematics in Landings: A Comparison between Professional Dancers and Non-Dancers. J. Sci. Med. Sport 2020, 23, 347–352. [CrossRef]
- Self, B.P.; Paine, D. Ankle Biomechanics during Four Landing Techniques. Med. Sci. Sport. Exerc. 2001, 33, 1338–1344.
- Blackburn, J.T.; Padua, D.A. Sagittal-Plane Trunk Position, Landing Forces, and Quadriceps Electromyographic Activity. J. Athl. Train. 2009, 44, 174–179. [CrossRef]
- Devita, P.; Skelly, W. Effect of Landing Stiffness on Joint Kinetics and Energetics in the Lower Extremity. Med. Sci. Sports Exerc. 1992, 24, 108–115.
- Saunier, J.; Chapurlat, R. Stress Fracture in Athletes. Jt. Bone Spine 2018, 85, 307–310. [CrossRef]
- Abbott, A.; Bird, M.L.; Wild, E.; Brown, S.M.; Stewart, G.; Mulcahey, M.K. Part I: Epidemiology and Risk Factors for Stress Fractures in Female Athletes. Phys. Sportsmed. 2020, 48, 17–24. [CrossRef]
- Goulart, M.; O’Malley, M.J.; Hodgkins, C.W.; Charlton, T.P. Foot and Ankle Fractures in Dancers. Clin. Sports Med. 2008, 27, 295–304. [CrossRef]
- Trégouët, P.; Merland, F. The Effects of Different Shoes on Plantar Forces in Irish Dance. J. Danc. Med. Sci. 2013, 17, 41–46.
- Ahonen, J. Biomechanics of the Foot in Dance A Literature Review. J. Danc. Med. Sci. 2008, 12, 99–108.
- Cimelli, S.N.; Curran, S.A. Influence of Turnout on Foot Posture and Its Relationship to Overuse Musculoskeletal Injury in Professional Contemporary Dancers: A Preliminary Investigation. J. Am. Podiatr. Med. Assoc. 2012, 102, 25–33. [CrossRef]
- Gabbett, T.J. The Training-Injury Prevention Paradox: Should Athletes Be Training Smarter and Harder? Br. J. Sports Med. 2016, 50, 273–280. [CrossRef]
- Wyon, M. Preparing to Perform: Periodization and Dance. J. Dance Med. Sci. 2010, 14, 67–72.
- Gabbe, B.J.; Finch, C.; Bennell, K.L.; Wajswelner, H. How Valid Is a Self Reported 12 Month Sports Injury History? Br. J. Sports Med. 2003, 37, 545–547. [CrossRef]
- Caine, D.; Goodwin, B.J.; Caine, C.G.; Bergeron, G. Epidemiological Review of Injury in Pre-Professional Ballet Dancers. J. Danc. Med. Sci. 2015, 19, 140–149. [CrossRef]
- Russell, J.A. Preventing Dance Injuries: Current Perspectives. Open access J. Sport. Med. 2013, 4, 199–210. [CrossRef]
- Sobrino, F.J.; de la Cuadra, C.; Guillen, P. Overuse Injuries in Professional Ballet: Injury-Based Differences Among Ballet Disciplines. Orthop. J. Sport. Med. 2015, 3, 1–7. [CrossRef]
- Grove, J.R.; Main, L.C.; Sharp, L. Stressors, Recovery Processes, and Manifestations of Training Distress in Dance. J. Danc. Med. Sci. 2013, 17, 70–78. [CrossRef]
- McEwen, K.; Young, K. Ballet and Pain: Reflections on a Risk-Dance Culture. Qual. Res. Sport. Exerc. Heal. 2011, 3, 152–173. [CrossRef]
- Lampe, J.; Borgetto, B.; Groneberg, D.A.; Wanke, E.M. Prevalence, Localization, Perception and Management of Pain in Dance: An Overview. Scand. J. Pain 2018, 18, 567–574. [CrossRef]
- Bahr, R.; Krosshaug, T. Understanding Injury Mechanisms: A Key Component of Preventing Injuries in Sport. Br. J. Sports Med. 2005, 39, 324–329. [CrossRef]
- Bolling, C.; Mechelen, W. Van; Pasman, H.R.; Verhagen, E. Context Matters : Revisiting the First Step of the ‘ Sequence of Prevention ’ of Sports Injuries. Sport. Med. 2018, 48, 2233–2240. [CrossRef]
- Krosshaug, T.; Andersen, T.E.; Olsen, O.E.O.; Myklebust, G.; Bahr, R. Research Approaches to Describe the Mechanisms of Injuries in Sport: Limitations and Possibilities. Br. J. Sports Med. 2005, 39, 330–339. [CrossRef]
- Bowling, A. Injuries to Dancers: Prevalence, Treatment and Perceptions of Causes. BMJ 1989, 298, 731–734. [CrossRef]
- McCabe, T.R.; Ambegaonkar, J.P.; Redding, E.; Wyon, M. Fit to Dance Survey: A Comparison with Dancesport Injuries. Med. Probl. Perform. Art. 2014, 29, 102–110. [CrossRef]
- Bolling, C.; Mellette, J.; Pasman, H.R.; Van Mechelen, W.; Verhagen, E. From the Safety Net to the Injury Prevention Web: Applying Systems Thinking to Unravel Injury Prevention Challenges and Opportunities in Cirque Du Soleil. BMJ Open Sport Exerc. Med. 2019, 5, 1–9. [CrossRef]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring Athlete Training Loads: Consensus Statement. Int. J. Sports Physiol. Perform. 2017, 12, 161–170. [CrossRef]
- Halson, S.L. Monitoring Training Load to Understand Fatigue in Athletes. Sport. Med. 2014, 44, 139–147. [CrossRef]
- West, S.W.; Clubb, J.; Torres-Ronda, L.; Howells, D.; Leng, E.; Vescovi, J.D.; Carmody, S.; Posthumus, M.; Dalen-Lorentsen, T.; Windt, J. More than a Metric: How Training Load Is Used in Elite Sport for Athlete Management. Int. J. Sports Med. 2020. [CrossRef]
- Allen, N.; Nevill, A.; Brooks, J.; Koutedakis, Y.; Wyon, M. Ballet Injuries: Injury Incidence and Severity over 1 Year. J. Orthop. Sports Phys. Ther. 2012, 42, 781–790. [CrossRef]
- Ekegren, C.L.; Quested, R.; Brodrick, A. Injuries in Pre-Professional Ballet Dancers: Incidence, Characteristics and Consequences. J. Sci. Med. Sport 2014, 17, 271–275. [CrossRef]
- Eckard, T.G.; Padua, D.A.; Hearn, D.W.; Pexa, B.S.; Frank, B.S. The Relationship Between Training Load and Injury in Athletes: A Systematic Review; Springer International Publishing, 2018; Vol. 48; ISBN 0123456789.
- Gabbett, T.J. Debunking the Myths about Training Load, Injury and Performance: Empirical Evidence, Hot Topics and Recommendations for Practitioners. Br. J. Sports Med. 2020, 54, 58–66. [CrossRef]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex Systems Approach for Sports Injuries: Moving from Risk Factor Identification to Injury Pattern Recognition - Narrative Review and New Concept. Br. J. Sports Med. 2016, 50, 1309–1314. [CrossRef]
- Bowerman, E.; Whatman, C.; Harris, N.; Bradshaw, E.; Karin, J. Are Maturation, Growth and Lower Extremity Alignment Associated with Overuse Injury in Elite Adolescent Ballet Dancers? Phys. Ther. Sport 2014, 15, 234–241. [CrossRef]
- Johnson, D.M.; Williams, S.; Bradley, B.; Sayer, S.; Murray Fisher, J.; Cumming, S. Growing Pains: Maturity Associated Variation in Injury Risk in Academy Football. Eur. J. Sport Sci. 2020, 20, 544–552. [CrossRef]
- Wik, E.H.; Martínez-Silván, D.; Farooq, A.; Cardinale, M.; Johnson, A.; Bahr, R. Skeletal Maturation and Growth Rates Are Related to Bone and Growth Plate Injuries in Adolescent Athletics. Scand. J. Med. Sci. Sport. 2020, 30, 894–903. [CrossRef]
- Van Der Sluis, A.; Elferink-Gemser, M.T.; Coelho-E-Silva, M.J.; Nijboer, J.A.; Brink, M.S.; Visscher, C. Sport Injuries Aligned to Peak Height Velocity in Talented Pubertal Soccer Players. Int. J. Sports Med. 2014, 35, 351–355. [CrossRef]
- Cahalan, R.; Purtill, H.; O’Sullivan, K. Biopsychosocial Factors Associated with Foot and Ankle Pain and Injury in Irish Dance: A Prospective Study. Med. Probl. Perform. Art. 2017. [CrossRef]
- Campbell, R.S.; Lehr, M.E.; Livingston, A.; McCurdy, M.; Ware, J.K. Intrinsic Modifiable Risk Factors in Ballet Dancers: Applying Evidence Based Practice Principles to Enhance Clinical Applications. Phys. Ther. Sport 2019, 38, 106–114. [CrossRef]
- Kenny, S.J.; Palacios-Derflingher, L.; Shi, Q.; Whittaker, J.L.; Emery, C.A. Association between Previous Injury and Risk Factors for Future Injury in Preprofessional Ballet and Contemporary Dancers. Clin. J. Sport Med. 2017, 29, 209–217. [CrossRef]
- Verhagen, E.; Van Dyk, N.; Clark, N.; Shrier, I. Do Not Throw the Baby out with the Bathwater; Screening Can Identify Meaningful Risk Factors for Sports Injuries. Br. J. Sports Med. 2018, 52, 1223–1224. [CrossRef]
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A Dynamic Model of Etiology in Sport Injury : The Recursive Nature of Risk and Causation. 2007, 17, 215–219.
- Adam, M.U.; Brassington, G.S.; Steiner, H.; Matheson, G.O. Psychological Factors Associated with Performance-Limiting Injuries in Professional Ballet Dancers. J. Danc. Med. Sci. 2004, 8, 43–46.
- Gao, B.; Dwivedi, S.; Milewski, M.D.; Cruz, A.I. Lack of Sleep and Sports Injuries in Adolescents: A Systematic Review and Meta-Analysis. J. Pediatr. Orthop. 2019, 39, e324–e333. [CrossRef]
- Watson, A.M. Sleep and Athletic Performance. Curr. Sports Med. Rep. 2017, 16, 413–418. [CrossRef]
- von Rosen, P.; Frohm, A.; Kottorp, A.; Fridén, C.; Heijne, A. Multiple Factors Explain Injury Risk in Adolescent Elite Athletes: Applying a Biopsychosocial Perspective. Scand. J. Med. Sci. Sport. 2017, 27, 2059–2069. [CrossRef]
- Johnson, M.; Blom, V. Development and Validation of Two Measures of Contingent Self-Esteem. Individ. Differ. Res. 2007, 5, 300–328.
- Elison, J.; Partridge, J. a Relationships between Shame-Coping, Fear of Failure, and Perfectionism in College Athletes. J. Sport Behav. 2012, 35, 19–39.
- Hamilton, L.H.; Solomon, R.; Solomon, J. A Proposal for Standardized Psychological Screening of Dancers. J. Danc. Med. Sci. 2006, 10, 40–45.
- Truong, L.K.; Bekker, S.; Whittaker, J.L. Removing the Training Wheels: Embracing the Social, Contextual and Psychological in Sports Medicine. Br. J. Sports Med. 2020, 0, 1–2. [CrossRef]
- Mainwaring, L.M.; Finney, C. Psychological Risk Factors and Outcomes of Dance Injury A Systematic Review. J. Danc. Med. Sci. 2017, 21, 87–96.
- Truong, L.K.; Mosewich, A.D.; Holt, C.J.; Le, C.Y.; Miciak, M.; Whittaker, J.L. Psychological, Social and Contextual Factors across Recovery Stages Following a Sport-Related Knee Injury: A Scoping Review. Br. J. Sports Med. 2020, 54, 1149–1156. [CrossRef]
- Wiese-Bjornstal, D.M. Psychology and Socioculture Affect Injury Risk, Response, and Recovery in High-Intensity Athletes: A Consensus Statement. Scand. J. Med. Sci. Sport. 2010, 20, 103–111. [CrossRef]
- Kamper, S.J. Types of Research Questions: Descriptive, Predictive, or Causal. J. Orthop. Sports Phys. Ther. 2020, 50, 468–469. [CrossRef]
- Meuli, L.; Dick, F. Understanding Confounding in Observational Studies. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 737. [CrossRef]
- Bahr, R.; Holme, I. Risk Factors for Sports Injuries - A Methodological Approach. Br. J. Sports Med. 2003, 37, 384–392. [CrossRef]
- Nielsen, R.O.; Simonsen, N.S.; Casals, M.; Stamatakis, E.; Mansournia, M.A. Methods Matter and the ‘ Too Much , Too Soon ’ Theory ( Part 2 ): What Is the Goal of Your Sports Injury Research ? Are You Describing , Predicting or Drawing a Causal Inference ? Br J Sport. Med 2020, 0, 2–4.
- Dekkers, O.M.; Vandenbroucke, J.P.; Cevallos, M.; Renehan, A.G.; Altman, D.G.; Egger, M. COSMOS-E: Guidance on Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology. PLoS Med. 2019, 16, 1–24. [CrossRef]
Figure 1.
PRISMA Flow Diagram of Study Selection.
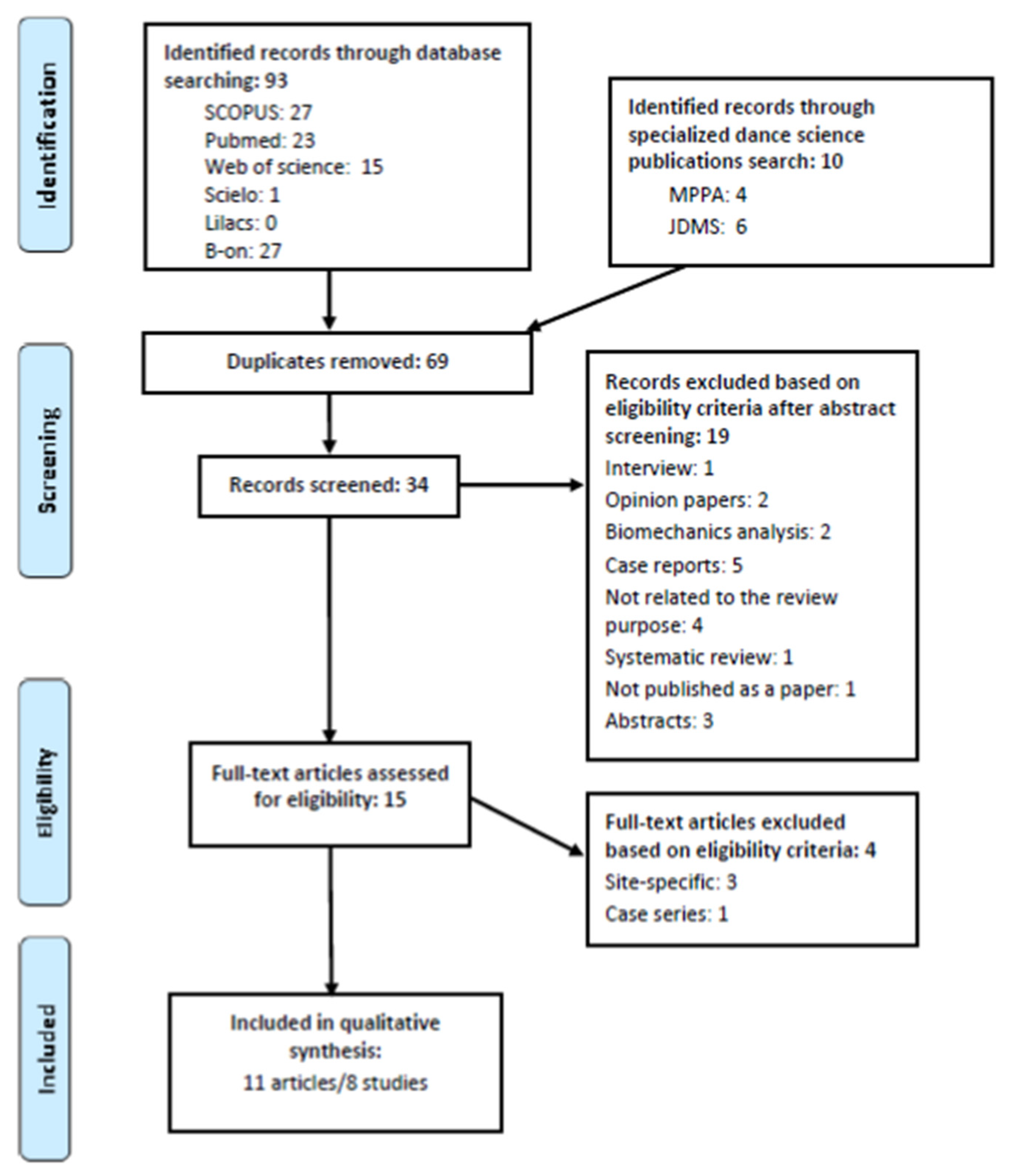
Figure 2.
Period Prevalence by Article with Injury Definition Type, Population and Time Frame.
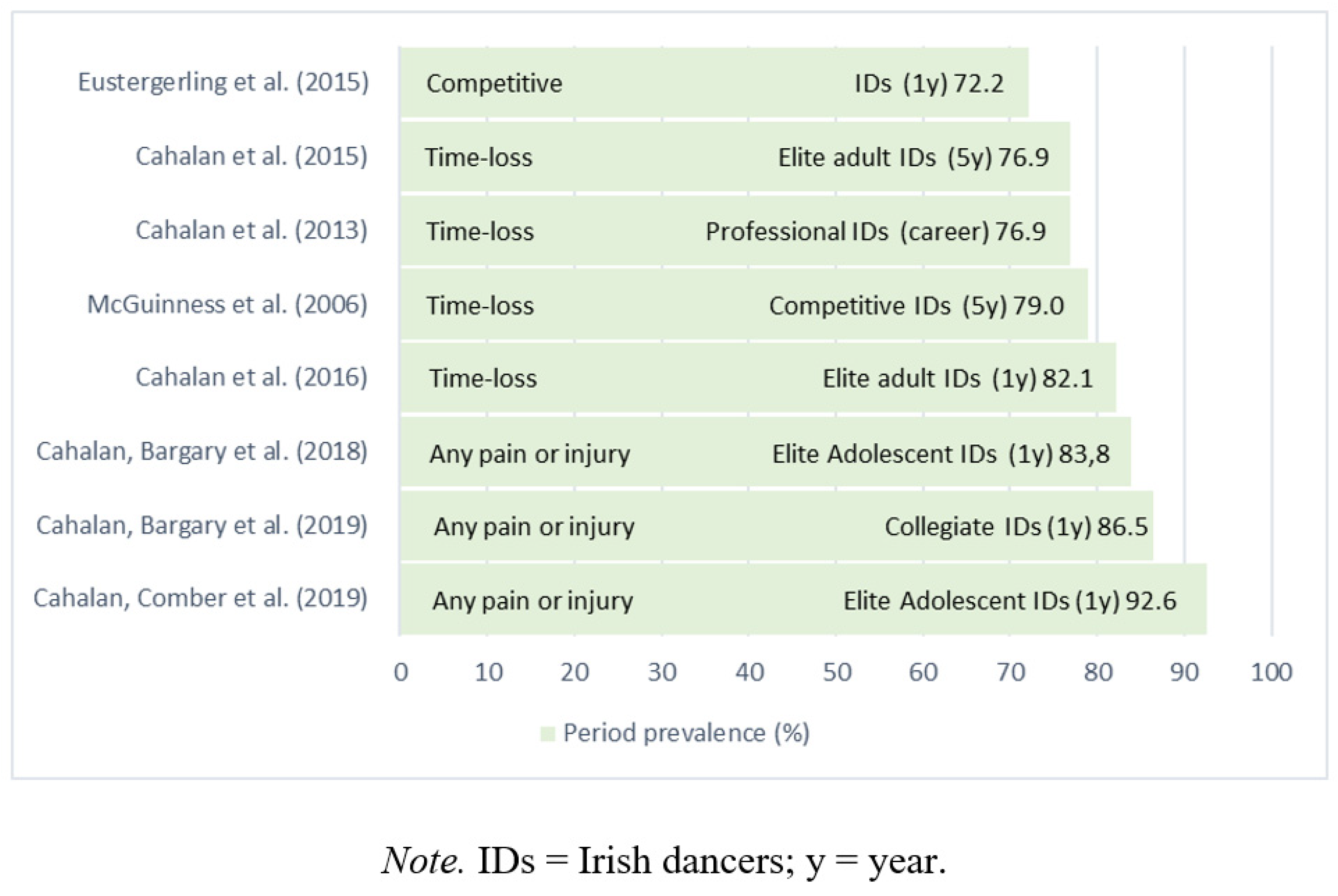
Figure 3.
Anatomical Injury Distribution.
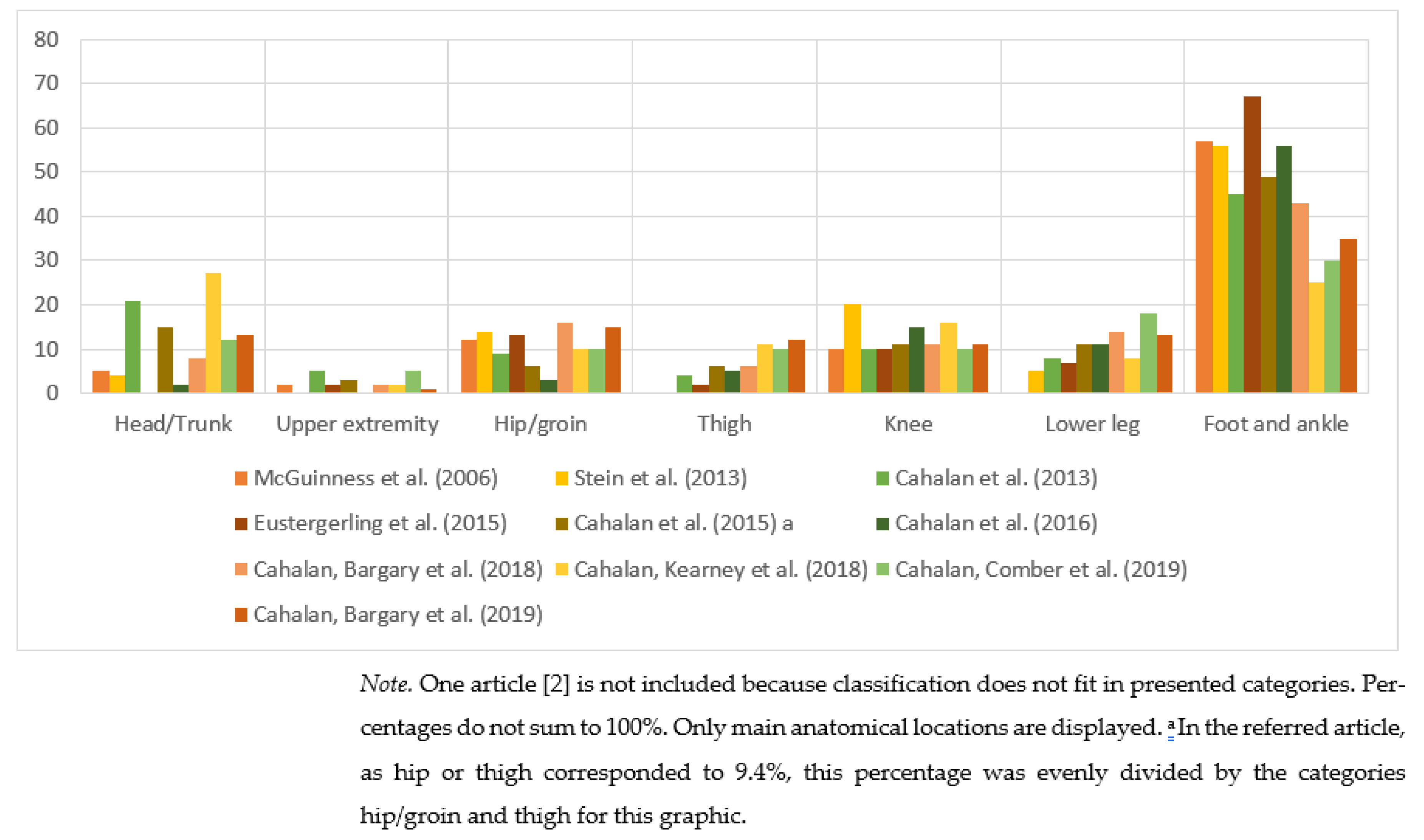
Figure 5.
The Percentage Distribution of Self-Reported Injury Types.
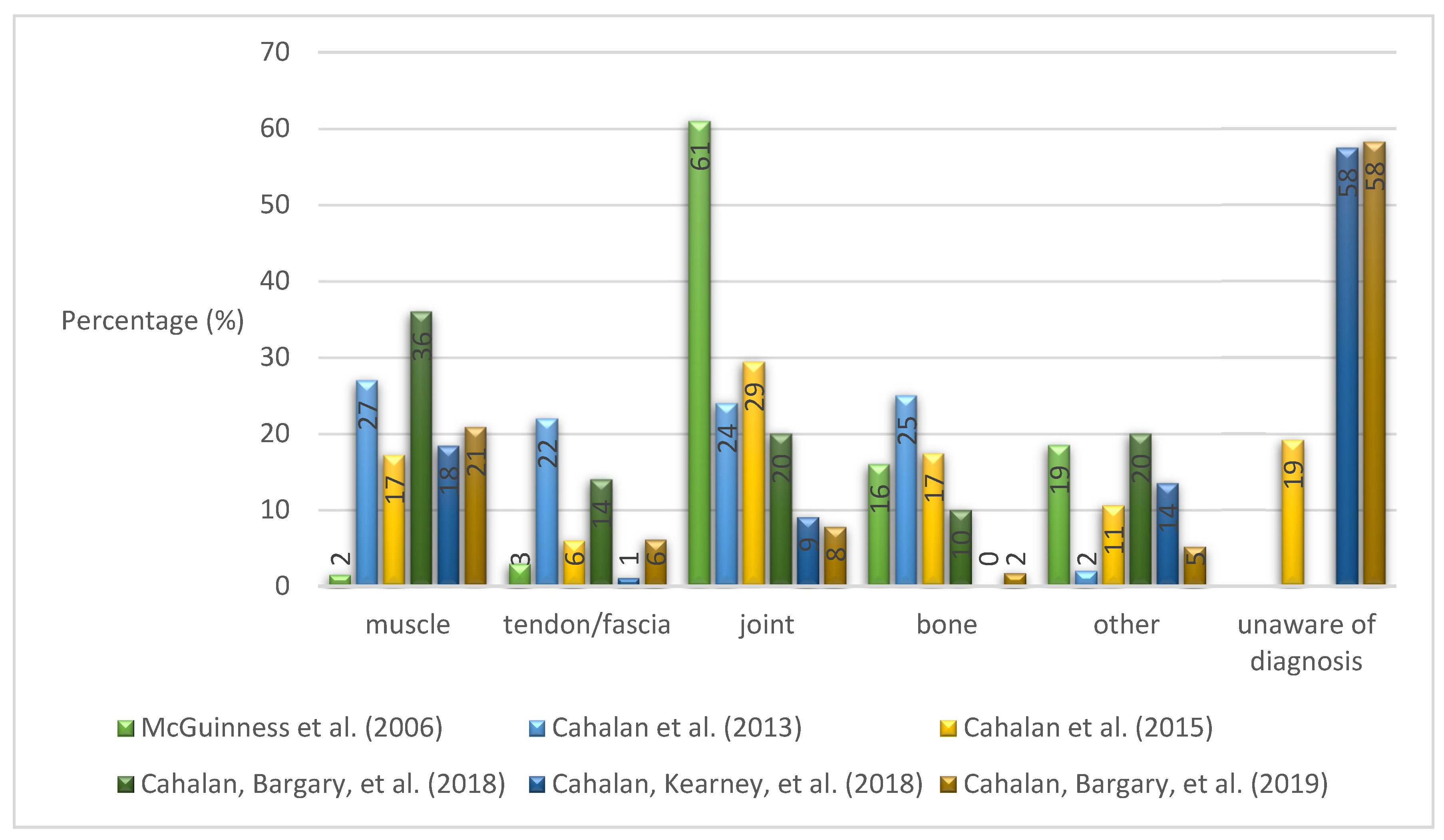
Table 3.
Training Related Factors and Statistical Approach.
| Authors | McGuinness et al. (2006) | Cahalan et al. (2013) | Eustergerling et al. (2015) | Cahalan et al. (2015) | Cahalan et al. (2016) | Cahalan, Bargary et al. (2018) | Cahalan, Kearney et al. (2018) | Cahalan, Bargary et al. (2019) | |
|---|---|---|---|---|---|---|---|---|---|
| Factors | |||||||||
| Use of split sole sneakers | ↓ | ||||||||
| Cool down | ↓ | = | = | ||||||
| Warm up | ↓ | = | ↑ failure to complete | ||||||
| Cross-training | = | = | = | = | = | ||||
| Dance exposure | = | = | = | ↓ | |||||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, mulivariate | Multivariate | Univariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | 3c | 3b | 3b | |
Note. = not significant; ↑ risk factor (correlated with injury); ↓ protective factor (negatively correlated with injury).
Table 4.
Individual Factors and Statistical Approach.
| Authors | McGuinness et al. (2006) | Cahalan et al. (2013) | Eustergerling et al. (2015) | Cahalan et al. (2015) | Cahalan et al. (2016) | |
|---|---|---|---|---|---|---|
| Factors | ||||||
| Elite level | ↑ | |||||
| Years dancing/experience | = | ↑ | = | = | ↑ | |
| Sex | = | ↑ ♀ | ||||
| Age | = | ↑ | ↑ | = | ||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, mulivariate | Multivariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | |
Note. = not significant; ↑ risk factor (correlated with injury).
Table 5.
Psychological Factors and Statistical Approach.
| Authors | McGuinness et al. (2006) | Cahalan et al. (2013) | Eustergerling et al. (2015) | Cahalan et al. (2015) | Cahalan et al. (2016) | Cahalan, Bargary et al. (2018) | |
|---|---|---|---|---|---|---|---|
| Factors | |||||||
| Psychological problems/complains | ↑ | ↑ | = | ||||
| Lower mood | ↑ | = | = | ||||
| Higher catastrophizing | ↑ | = | = | ||||
| Higher levels of anger-hostility | = | ↑ | ↑ | ||||
| Statistics | Univariate | Univariate | Odds ratios (association) | Univariate, mulivariate | Multivariate | Univariate | |
| Level of evidence | 3c | 3c | 3c | 3c | 3b | 3c | |
Note. = not significant; ↑ risk factor (correlated with injury);.
Table 6.
General Health and Sleep Related Factors and Statistical Approach.
| Authors | Cahalan et al. (2013) | Cahalan et al. (2015) | Cahalan et al. (2016) | Cahalan, Bargary et al. (2018) | Cahalan, Kearney et al. (2018) | Cahalan, Bargary et al. (2019) | |
|---|---|---|---|---|---|---|---|
| Factors | |||||||
| Higher nr of subjective health complaints | ↑ | ↑ | = | ||||
| A higher level of general everyday pain | ↑ | ||||||
| More body parts affected by pain/injury | ↑ | ↑ | ↑ | ||||
| Always/often dancing in pain | = | ↑ | ↑ | ||||
| Insufficient/poor sleep | ↑ | ↓ better sleep | = | ||||
| General health scores | ↓ | ||||||
| Nr of weeks participants reported poor/very poor general health | ↑ | ||||||
| Statistics | Univariate | Univariate, mulivariate | Multivariate | Univariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3c | 3b | 3c | 3b | 3b | |
Note. = not significant; ↑ risk factor (correlated with injury); ↓ protective factor (negatively correlated with injury).
Table 7.
Physical Factors and Statistical Approach.
| Authors | Cahalan et al. (2015) | Cahalan et al. (2016) | Cahalan, Bargary et al. (2018) | Cahalan, Bargary et al. (2019) | |
|---|---|---|---|---|---|
| Factors | |||||
| Physical screening tests | = | = | = | ||
| Change in weight or height | = | ||||
| Statistics | Univariate mulivariate |
Multivariate | Univariate | Multivariate | |
| Level of evidence | 3c | 3b | 3c | 3b | |
Note. = not significant; ↑ risk factor (correlated with injury).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



