
Submitted:
27 January 2023
Posted:
30 January 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Childhood hygiene education has resulted in individuals engaging in hand washing and mask wearing to cope with COVID-19. Individuals can form sustainable development-related habits through childhood education.
Keywords:
childhood education
; Hygiene
; COVID-19
; preventive behaviours
; staying at home
; mask wearing
; hand washing
; public goods
1. Introduction
Ideally, people had better prepare for unexpected events like pandemic prior to the shock. Education is expected to alter the risk perceptions of individuals and affect the production of health outcomes. Educational level played critical role on people’s preparedness for COVID-19 pandemic disaster [2]. Risk perception and precautionary behavior against pandemics can be dynamic in time [3]. However, effect of the education persists for longer period once the hygiene habit is formed [1,4], which contributes to sustainability of society.
People can more smoothly cope with its occurrence if they take the precaution of epidemic disease. According to Ikeda et al [5], people highly care about hygiene such as regular handwashing in Japan, reducing risk of contracting an infection. Lee et al. explored the role of hygiene school education in childhood on regular hand-washing behaviors during the COVID-19 pandemic [1]. They found that hand-washing education in primary school is positively related to various preventive behaviors in adulthood during the COVID-19 pandemic but also prior to the pandemic. This finding was observed using the dataset collected from April to August 2020 at early stage of COVID-19.
According to study of H1N1 2009 influenza pandemic, government promoted campaign to educate the public about using hand sanitizers, hand washing techniques, and wearing mask. Accordingly, past-experience of the pandemic facilitated hand washing behaviors, which provide long-lasting effects on health outcomes [4]. COVID-19 pandemic continued to influence various aspect of daily life until end of 2022 at least. People learn COVID-19 from their experience and public campaign. Further, COVID-19 vaccination has been implemented in 2021 throughout Japan and most of people are vaccinated. Hence, the risk of COVID-19 infection reduced, which influences degree of engaging in preventive behaviors [6,7,8].
All in all, the situation has been drastically changed from the early stage. It is necessary to consider how and the extent on which effect of childhood education on preventive behaviors changed using data covering longer period than Lee et al. [1]. In this short note, we use monthly individual-level longitudinal data to re-examine findings of Lee et al. [1]. The research question is; How did hygiene practice education in childhood influence preventive behaviors in adulthood during COVID-19 pandemic period covering March 2020- September 2022.
2. Materials and Methods
2.1. Materials
Shortly after COVID-19 infection was detected in Japan in January 2020, we decided to collect data through online surveys by commissioning the research company INTAGE. INTAGE was chosen for their good reputation due to their abundant experience with academic research. In the early stages of the COVID-19 pandemic (March 13–16, 2020), the first wave of queries was conducted to gather 4,359 observations. INTAGE recruited participants for the survey from among pre-registered individuals, with a participation rate of 54.7 %. Respondents were randomly selected to fill the pre-specified quotas by identifying a representative of the Japanese adult population (ages 18–78 years), and data was collected on household income, age, gender, educational background, and area of residence. This sampling method was chosen because individuals aged 17 years and below were too young to be registered with INTAGE, and data from individuals over 78 years of age could not be reliably collected mainly because they were unlikely to use the Internet. Consequently, the sample population was restricted to ages 18–78 years.
Longitudinal panel data were constructed as follows. Internet surveys were conducted nearly monthly on 26 occasions (‘waves’) between March 2020 and September 2022 with the same individuals. Surveys were not conducted for three months between July-September 2020 because of a shortage of research funds. After acquiring additional funding, surveys continued in October 2020 (6th wave) and included an additional question on primary school education to examine the effect of childhood education on preventive measures. The first survey by Lee et al. was conducted between April 28–30 [1]. By comparison, we conducted our first survey one month earlier, between March 13–27. From March to April 2020, the COVID-19 situation in Japan changed drastically, making this a notable distinction [9,10,11,12]. During the study period, some respondents stopped taking the surveys and were removed from the sample pool. We limited samples used for analysis to respondents who participated from the first to the 26th wave to follow the same individuals. Further, we restricted the sample to those who answered various questions, such as primary household income, job type, and education in primary school. In particular, many respondents did not remember experiencing hand-washing education in primary school. Eventually, the number of respondents was reduced to 996, and the total number of observations used in this study was 25,896.
2.2. Method
Table 1 describes the key variables used in the estimation and reports their means and standard deviations. The survey questionnaire contained basic questions about demographics, such as birth year, gender, educational background, household income, and jobs.
The estimated function takes the following form:
Yit = α0 + α1 WASHING EDUCATIONit + α2 SCHOOL UNIFORMit + kt + uit
Yit is the outcome variable for individual i and wave t and α denotes the regression parameters. uit is the error term. The estimation method was the ordinary least squares model. The behaviour of individuals depends on the situation. For instance, residents were strongly requested to stay at home during states of emergency. There were also cycles of increasing and decreasing numbers of new infections, which were common in all parts of Japan [11,12]. kt represents the characteristics of the situation at each time point. To control for this, we used 25 time point dummies.
Y is the outcome variable captured by the three proxy variables STAYING HOME, HAND WASHING, and WEARING MASK. The respondents were asked the following questions about preventive behaviours:
‘Within a week, to what degree have you practiced the following behaviours? Please answer based on a scale of 1 (I have not practiced this behaviour at all) to 5 (I have completely practiced this behaviour)’.
- (1)
- Staying home
- (2)
- Wearing a mask
- (3)
- Washing my hands thoroughly
The answers to these questions served as proxies for the following variables for preventive behaviours: staying home, frequency of hand washing, and degree of mask wearing. Larger values indicate that respondents are more likely to engage in preventive behaviours.
The key confounding variable is WASHING EDUCATION, which is ‘1’ if teachers supervised pupils to ensure that they washed their hands during primary school, otherwise it is ‘0’. In this study 48% of respondents had experienced hand-washing practice in primary school (Table 1). Previous studies have found that the experience of wearing school uniforms during primary school is positively correlated with pro-social inclinations in adulthood [13]. Therefore, the experience of school uniforms may be correlated with preventive behaviours in adulthood, so SCHOOL UNIFORM is also included as a confounding variable. The statistical software used in this study was Stata/MP 15.0.
3. Results
3.1. Baseline Estimation
Table 2 shows the estimation results and coefficient of confounders. We found a positive correlation for WASHING EDUCATION for all dependent variables. The relationship between WASHING EDUCATION and both HAND WASHING and WEARING MASK were found to be statistically significant, whereas STAYING HOME is not. The coefficient of HAND WASHING is 0.198, meaning that those who experienced hand-washing education in primary school are more likely to wash their hands by 1.987 points on a 5-point scale compared to those who did not. The effect of hand-washing education on HAND WASHING was approximately two times larger than that of WEARING MASK (0.109). We did not find statistical significance for SCHOOL UNIFORM on any dependent variable.
3.2. Changes of Preventive Behaviours
Figure 1, Figure 2 and Figure 3 show that preventive behaviours drastically increased during the early stage of COVID-19, especially during the first state of emergency, as indicated by the solid vertical line. Subsequently, in Figure 1 and Figure 2, hand washing and mask wearing were maintained at high levels throughout the study period. This is in contrast with the findings in Japan that precautionary behaviour in response to the 2009 (H1N1) influenza pandemic fluctuated [3].
Those who experienced hand-washing practices in primary school were more likely to engage in hand washing and mask wearing during the COVID-19 pandemic. The effect of hand-washing education on mask wearing was smaller and less statistically significant than that on hand-washing. This may be because hand-washing education is more likely to form a habit of washing hands than wearing masks. Wearing masks in crowded places is effective in mitigating pandemics, whereas wearing masks in open air is much less effective [14]. People wear masks outdoors, partly because of peer pressure.
Hand-washing education played a critical role in forming lasting habits of health-protective behaviours such as hands-washing and mask wearing. By contrast, Figure 3 shows the fluctuating cycles of staying at home. Furthermore people became overall less likely to stay home after the COVID-19 vaccine was implemented, as indicated by the dashed vertical line. People are unlikely to form a habit of staying home, which is congruent with Ibuka et al. [3]. There was no difference in staying home between those who had experienced hygiene education practice and those who did not.
4. Discussion
4.1. Implication
The purpose of this study is to consider how school practices in primary schools influenced preventive behaviours during the COVID-19 pandemic using data covering March 2020 to September 2022. Preventive behaviours reduce one’s own risk of being infected, but also the risk of infecting others. Therefore, preventive behaviours against pandemic spread can also be considered an investment in public goods to benefit society [15]. Lee et al. found that hand washing led people to display preventive behaviours even before COVID-19 (Appendix 7) [1]. Considering their and our findings together, hygiene education resulted in a habit of hygiene preventive behaviours and persisted regardless of pandemic severity.
Lee et al. [1] found that hand-washing education is positively associated with various preventive behaviours, including wearing masks and staying at home. In contrast to Lee et al., this study found clear differences in educational impact according to the type of preventive behaviour. In the questionnaire used by Lee et al., detailed questions about primary school education and various preventive behaviours were included. The respondents may have perceived the researchers’ intentions, which may have influenced their responses. For example, their questions about hygiene practice in primary school may have functioned as a ‘nudge’ that unintentionally influenced respondents to meet the goals of the researchers and respond accordingly. In our study, questions about preventive behaviours were included in all waves, whereas questions about primary school education were blended into various questions only in the 6th wave onward. Hence, before the 6th wave, respondents may not have perceived our goals to associate childhood education with preventive behaviours. In order to directly compare our results with those of Lee et al., we analysed data from the 1st through 5th waves which are almost equivalent to the period they studied, conducting estimations using the same specifications (Table 3).
Staying at home was not significantly correlated with hand-washing education during childhood. This might be because staying at home is a different type of preventive behaviour than hand washing. People stay home only when their benefits exceed their costs. People sacrifice various experiences through outdoor activities in the real world if they stay at home. In economic terms, this sacrifice is considered an ‘opportunity cost’ of staying home. As the opportunity cost is not reduced even if one experiences hand-washing education in childhood, individuals will stay at home only if their benefits outweigh their costs regardless of hygiene education. Additionally, staying at home weakens social ties and reduces social capital because of a reduction in social interaction through face-to-face communication. As is widely acknowledged, social ties and social capital are positively associated with health status [16,17,18]. Therefore, it is important to distinguish staying at home from other preventive behaviours.
The formation of hand-washing habits through hygiene education in childhood reduces its psychological costs. In this case, people do not need to change their lifestyle to engage in basic preventive behaviours such as hand washing, regardless of the severity of the pandemic. Basic hygiene practices in childhood have reduced stress in life during the pandemic.
4.2. Strength
We constructed longitudinal data to cover a longer period than previous studies in Japan, where preventive behaviours were not enforced with penalties [1,3]. Lee et al. did not examine the effects of the emergence and spread of the COVID-19 vaccine on preventive behaviours [1]. Preventive behaviours of individuals were thought to change in response to the emergence of the COVID-19 vaccine. However, individuals continue to wash their hands and wear masks long after vaccine implementation. This clearly suggests these preventive behaviours are stable.
4.3. Limitation
Many respondents did not remember experiencing hand-washing education in primary school. We have deleted them from the data pool used for analysis. There was a difference in the characteristics of respondents who answered the questionnaire and those who did not. This may have resulted in selection biases. Furthermore, answers to the questionnaire seem to depend not only on the facts, but also on the respondent’s misapprehension. Therefore, recall bias may occur. Another variable of school education would show statistical significance if biases had a significant effect on the results. However, SCHOOL UNIFORM is not significantly correlated with preventive behaviours, which is clearly different from the results of WASHING EDUCATION. This suggests, to a certain extent, the biases are minor.
Wearing masks are less effective in open air than indoors [14]. In contrast to Lee et al. [1], we used only three proxies for preventive behaviours. Therefore, we did not scrutinise how hand washing and mask wearing changed in different situations.
In contrast to hand washing, the benefit of mask wearing depends on the situation. Wearing masks in the open air has limited effectiveness [14]. In mid-summer, wearing masks increased the risk of heatstroke. In this situation, the cost of wearing a mask is higher than its benefits. It is, therefore, important to examine mask-wearing behaviour in various situations in future studies.
5. Conclusions
Preventive behaviours play a vital role in coping with unexpected pandemics such as COVID-19. We concluded that people can form sustainable development-related habits through childhood hygiene practice education.
Author Contributions
EY and FO participated in the conceptualisation of the study and analysed the patient data. YT designed the panel survey and performed data collection. EY wrote the main text and made the tables for the original manuscript. All authors reviewed, edited, and approved the final manuscript. The authors are responsible for any errors in this study.
Funding
This study was supported by the Fostering Joint International Research B (Grant No. 18KK0048) and the Grant-in-Aid for Scientific Research S (Grant No. 20H05632) from the Japan Society for the Promotion of Science to Yoshiro Tsutsui and Fumio Ohtake, respectively.
Institutional Review Board Statement
This study was conducted with the ex-ante approval of the Ethics Committee of the Graduate School of Economics, Osaka University, and all methods were carried out in accordance with the relevant guidelines and regulations. The ethics approval number of Osaka University for this study is R021014. Informed consent for study participation was obtained from all subjects.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and analysed in this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Lee, S.Y.; Sasaki, S.; Kurokawa, H.; Ohtake, F. The School Education, Ritual Customs, and Reciprocity Associated with Self-Regulating Hand Hygiene Practices during COVID-19 in Japan. BMC Public Health 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Cvetković, V.M.; Nikolić, N.; Radovanović Nenadić, U.; Öcal, A.; Noji, E.K.; Zečević, M. Preparedness and Preventive Behaviors for a Pandemic Disaster Caused by COVID-19 in Serbia. Int. J. Environ. Res. Public. Health 2020, 17, 4124. [Google Scholar] [CrossRef]
- Ibuka, Y.; Chapman, G.B.; Meyers, L.A.; Li, M.; Galvani, A.P. The Dynamics of Risk Perceptions and Precautionary Behavior in Response to 2009 (H1N1) Pandemic Influenza. BMC Infect Dis 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Agüero, J.; Beleche, T. Health Shocks and Their Long-Lasting Impact on Health Behaviors: Evidence from the 2009 H1N1 Pandemic in Mexico. J Health Econ 2017, 54, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, N.; Saito, E.; Kondo, N.; Inoue, M.; Ikeda, S.; Satoh, T.; Wada, K.; Stickley, A.; Katanoda, K.; Mizoue, T.; et al. What Has Made the Population of Japan Healthy? Lancet 2011, 378, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Hossain, Md.E.; Islam, Md.S.; Rana, Md.J.; Amin, Md.R.; Rokonuzzaman, M.; Chakrobortty, S.; Saha, S.M. Scaling the Changes in Lifestyle, Attitude, and Behavioral Patterns among COVID-19 Vaccinated People: Insights from Bangladesh. Hum. Vaccin. Immunother. 2022, 18. [Google Scholar] [CrossRef]
- Wright, L.; Steptoe, A.; Mak, H.W.; Fancourt, D. Do People Reduce Compliance with COVID-19 Guidelines Following Vaccination? A Longitudinal Analysis of Matched UK Adults. J Epidemiol Community Health (1978) 2022, 76, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Liu, X.; Jin, T.; Zhao, P.; Miao, D.; Lei, H.; Su, B.; Xue, P.; Xie, J.; Li, Y. Weakening Personal Protective Behavior by Chinese University Students after COVID-19 Vaccination. Build. Environ. 2021, 206, 108367. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsutsui, Y. How Does the Impact of the COVID-19 State of Emergency Change? An Analysis of Preventive Behaviors and Mental Health Using Panel Data in Japan. J. Jpn. Int. Econ. 2022, 64, 101194. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, E.; Tsutsui, Y. The Impact of Postponing 2020 Tokyo Olympics on the Happiness of O-MO-TE-NA-SHI Workers in Tourism: A Consequence of COVID-19. Sustainability (Switzerland) 2020, 12. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsutsui, Y. School Closures and Mental Health during the COVID-19 Pandemic in Japan. J. Popul. Econ. 2021, 34, 1261–1298. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, E.; Tsutsui, Y. The Impact of Closing Schools on Working from Home during the COVID-19 Pandemic: Evidence Using Panel Data from Japan. Rev. Econ. Househ. 2021, 19, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Ito, T.; Kubota, K.; Ohtake, F. Reciprocal and Prosocial Tendencies Cultivated by Childhood School Experiences: School Uniforms and the Related Economic and Political Factors in Japan. Int. J. Educ. Dev. 2021, 83, 102396. [Google Scholar] [CrossRef]
- Javid, B.; Bassler, D.; Bryant, M.B.; Cevik, M.; Tufekci, Z.; Baral, S. Should Masks Be Worn Outdoors? The BMJ 2021, 373. [Google Scholar] [CrossRef] [PubMed]
- Cato, S.; Iida, T.; Ishida, K.; Ito, A.; McElwain, K.M.; Shoji, M. Social Distancing as a Public Good under the COVID-19 Pandemic. Public. Health 2020, 188, 51–53. [Google Scholar] [CrossRef] [PubMed]
- Kawach, I.; Berkman, L. Social Cohesion, Social Capital, and Health. Social. Epidemiol. 2000, 174, 290–319. [Google Scholar]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social Capital and Self-Rated Health: A Contextual Analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I. Social Ties and Mental Health. J. Urban. Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hand-washing behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
Figure 1.
Hand-washing behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
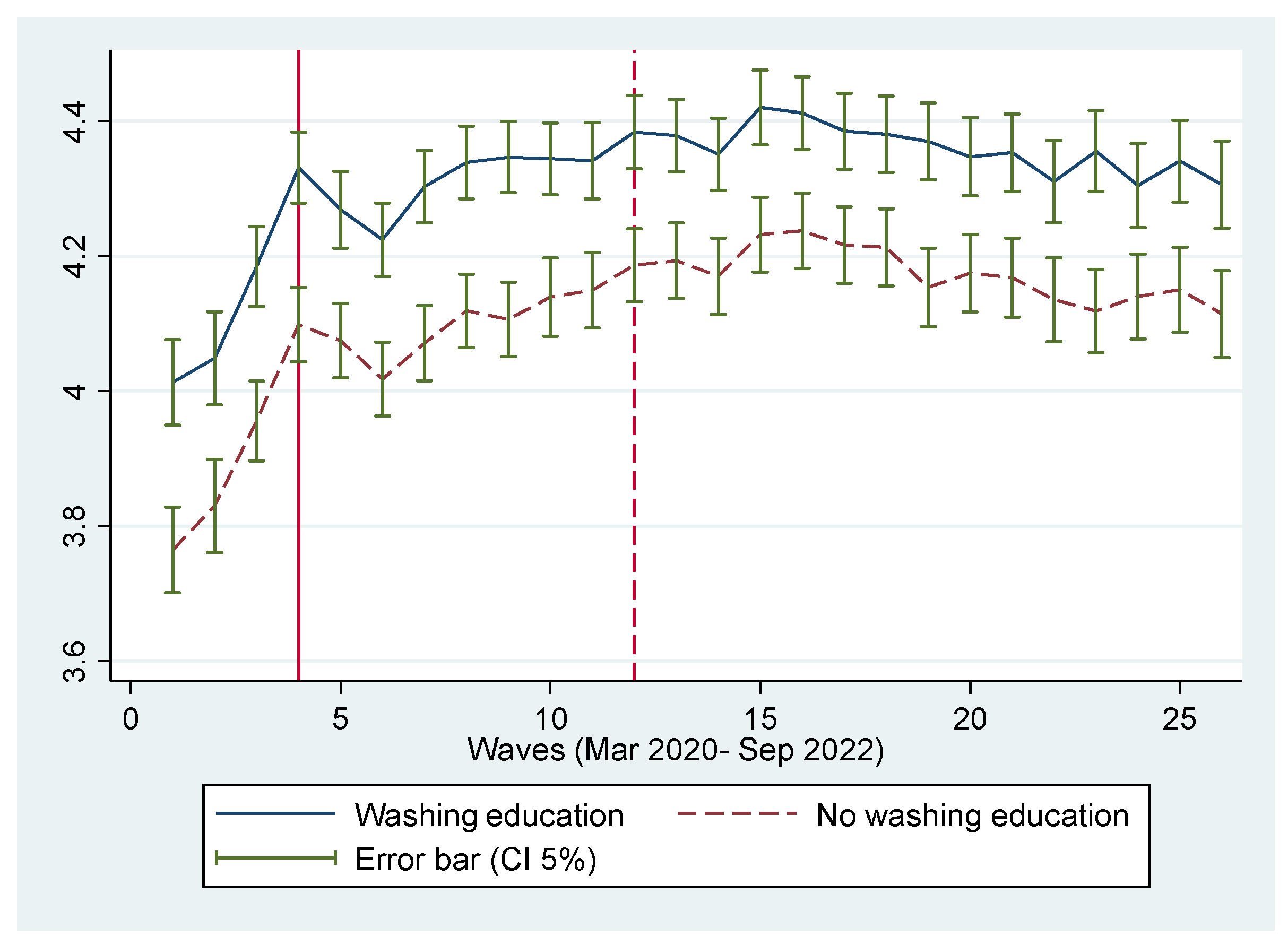
Figure 2.
Mask-wearing behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
Figure 2.
Mask-wearing behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
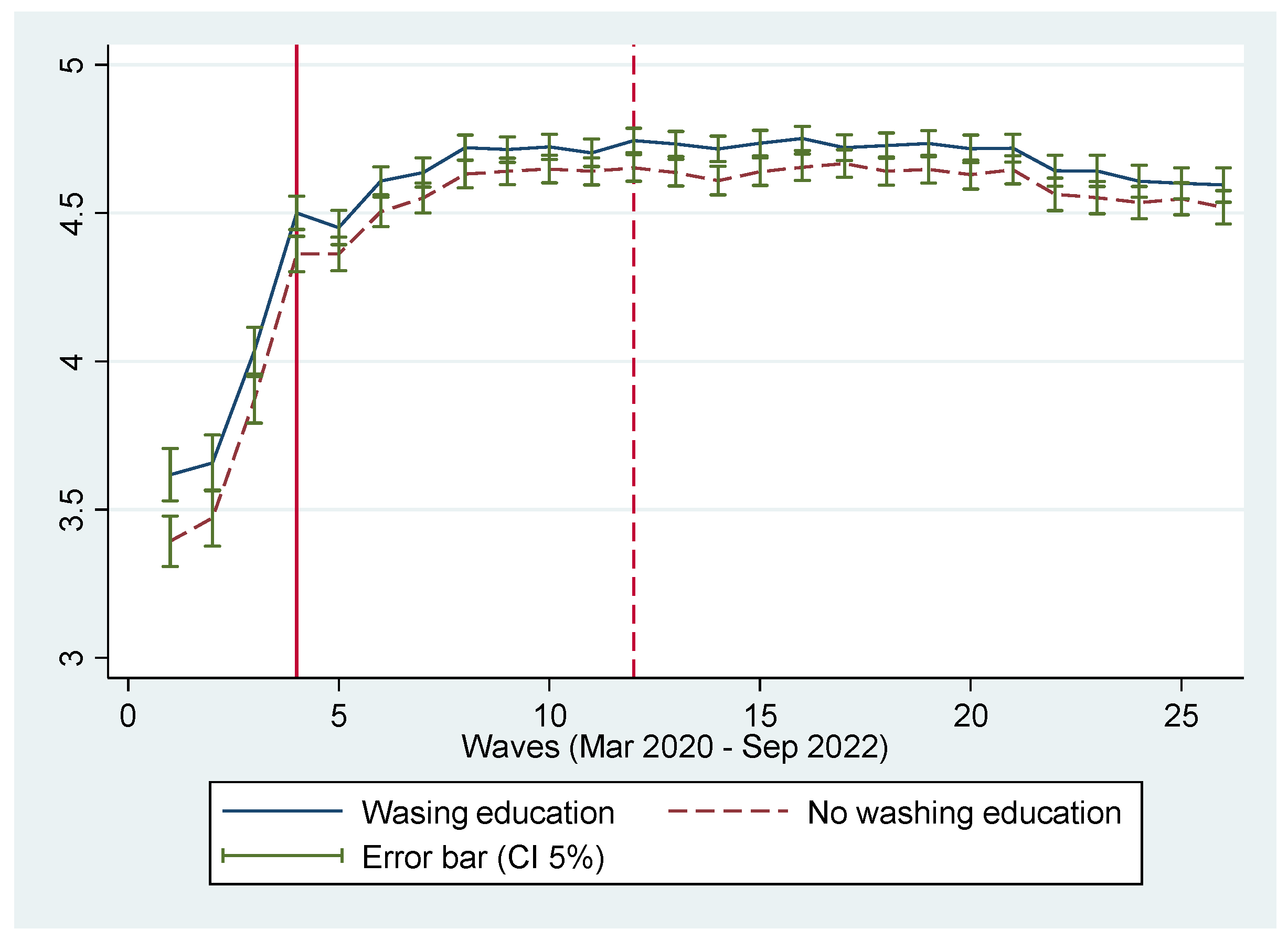
Figure 3.
Staying at home behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
Figure 3.
Staying at home behaviour. Note: The solid vertical line indicates when the first state of emergency was declared in Japan. The dashed vertical line shows when COVID-19 vaccination was implemented.
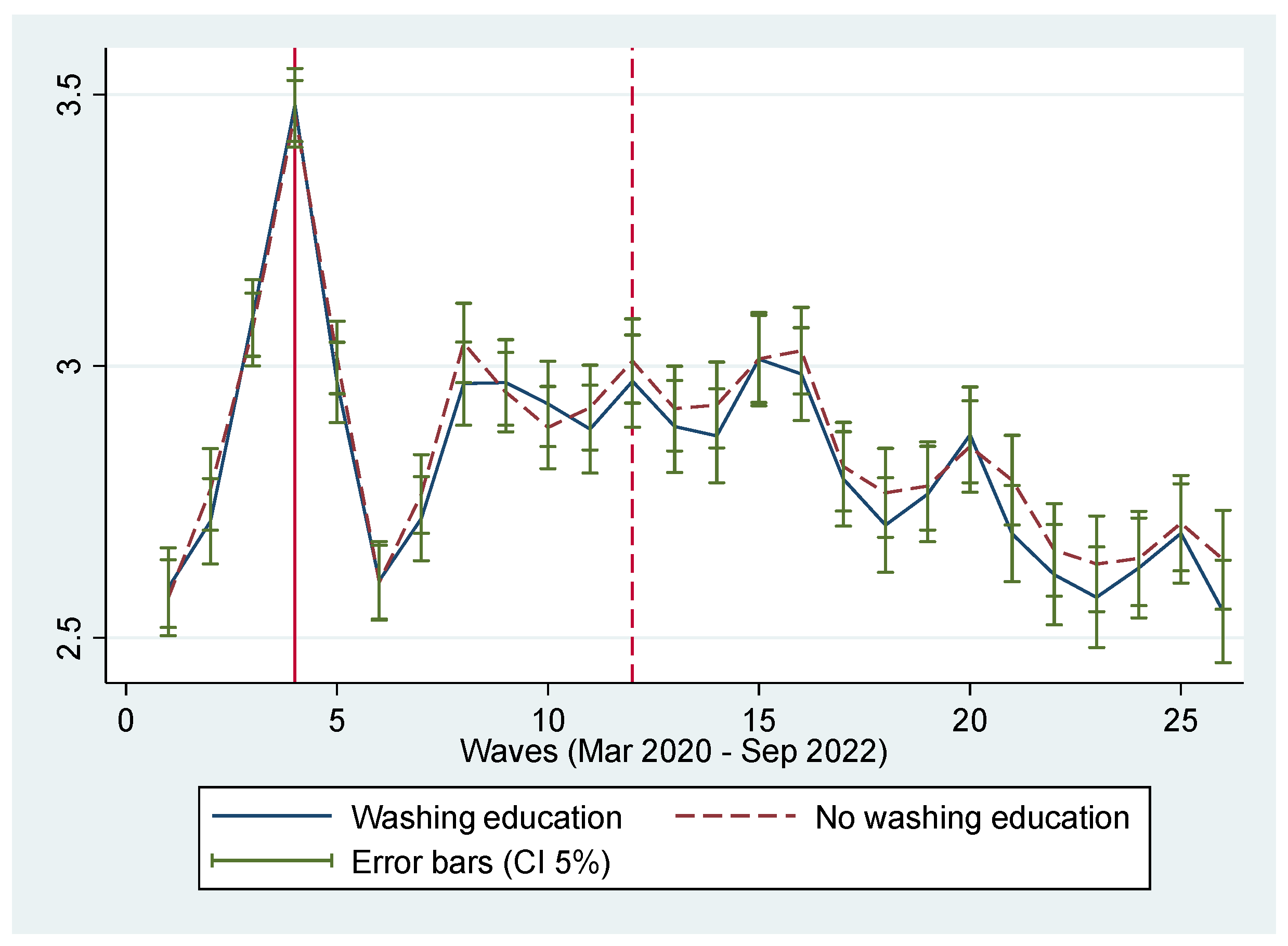

Table 1.
Definitions of key variables.
| Variables | Definition | ||
| Outcome variables | Mean | s.d. | |
| STAYING HOME | In the last week, how consistent were you at ‘not going out of home’? Please choose among 5 choices. 1 (not completed at all) to 5 (completely consistent). |
4.21 | 0.91 |
| WEARING MASK | In the last week, how consistent were you at ‘wearing a mask’? Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
4.54 | 0.19 |
| HAND WASHING |
In the last week, how consistent were you at ‘washing your hands’? Please choose among 5 choices. 1 (not completed at all) to 5 (completely achieved). |
2.91 | 1.29 |
| Confounders (Independent variables) | |||
| WASHING EDUCATION | Did everyone in your class was supervised by teachers to ensure that they washed their hands in turn? 1 (Yes) or 0 (No) |
0.48 | 0.49 |
| SCHOOL UNIFORM | Did you wear school uniforms in primary school? 1 (Yes) or 0 (No) |
0.20 | 0.40 |
Table 2.
Dependent variables are preventive behaviours (Data: 1st to 26th wave).
| (1)HAND WASHING | (2)WEARING MASK | (3)STAYING HOME | |
| WASHING EDUCATION | 0.197***(0.126-0.267) | 0.109***(0.051-0.167) | 0.072(−0.032-0.186) |
| SCHOOL UNIFORM | 0.026(−0.067- 0.119) | 0.026(−0.065-0.061) | −0.002(−0.193-0.100) |
| Time Fixed Effects | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes |
| Adj R2Obs. | 0.1125,896 | 0.1925,896 | 0.1425,896 |
Note: Numbers without parentheses are coefficients of the confounding variables. Numbers within parentheses are 95% CI. The model includes various control variables, such as age, gender, dummies for household income, job dummies, number of deaths, and number of infected people in residential prefectures. However, these results have not been reported. “Yes” means that these variables are included. ***p<0.01.
Table 3.
Dependent variables are preventive behaviours (Data: 1st to 5th wave).
| (1) HAND WASHING |
(2) WEARING MASK |
(3) STAYING HOME |
|
| WASHING EDUCATION | 0.196*** (0.103-0.289) |
0.121* (−0.008-0.251) |
0.037 (−0.069-0.136) |
| SCHOOL UNIFORM | −0.029 (−0.127- 0.069) |
−0.069 (−0.190-0.051) |
−0.013 (−0.135-0.109) |
| Time Fixed Effects | Yes | Yes | Yes |
| Control variables | Yes | Yes | Yes |
| Adj R2 Obs. |
0.11 4,980 |
0.17 4,980 |
0.14 4,980 |
Note: Numbers without parentheses are coefficients of the confounding variables. Numbers within parentheses are 95% CI. The model includes various control variables, such as age, gender, dummies for household income, job dummies, number of deaths, and infected persons in residential prefectures. However, these results have not been reported. “Yes” means that these variables are included. *p<0.10. ***p<0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



