Submitted:
03 January 2023
Posted:
06 January 2023
Read the latest preprint version here
Abstract
Background: Real-time remote monitoring of pulmonary artery pressures has previously shown to reduce heart failure (HF) related hospitalisations and to improve quality of life of selected HF patients. The value of CardioMEMS in Southern Europe, where healthcare costs are significantly lower, remains uncertain. Objective: To evaluate the cost-effectiveness of the CardioMEMS HF system in the Spanish healthcare setting. Methodology: This single-centre study included 35 HF patients with a CardioMEMS device (treatment group) and compared them with similar patients receiving standard HF treatment (control group). The Propensity Score Matching method was used and the comparators were found using the variables age, sex, New York Heart Association class, left ventricular ejection fraction, and diabetes mellitus. Cost-effectiveness was measured as the incremental cost per quality-adjusted life year gained. Results: The CardioMEMS HF system outperformed usual management with a net monetary value difference of 2,731€ per patient at 1 year. The incremental cost per quality-adjusted life year gained was 15,896€. Results were consistent in the sensitivity analyses performed. Conclusion: This analysis suggests that remote monitoring of pulmonary artery pressure with CardioMEMS HF system is a cost-effective strategy in the Spanish healthcare setting.
Keywords:
cost-effectiveness evaluation
; heart failure
; telemonitoring
; pulmonary artery pressure
; hemodynamic monitoring
1. Introduction
Heart failure (HF) is a major public health problem and a leading cause of hospitalisation in Western countries. The prevalence of HF is approximately 2% in the adult population in Spain, rising to ≥10% among people >80 years of age.1 The most common cause of hospitalisation in HF patients is HF decompensation, which leads to a progressive deterioration of myocardial function and quality of life and also represents the most important determinant of HF associated costs in our country.2
Despite improvements in HF therapy, the 12-month hospitalisation rates remain very high in this population, ranging from 32% to 44% for ambulatory and hospitalised patients, respectively.3 Remote monitoring emerged as a viable way to overcome the long interval between office visits and to keep patients safe by identifying disease progression in time to prevent hospitalisation.4
The CardioMEMS HF System (St. Jude Medical, Inc., Atlanta, GA, USA) is the first system to provide real-time remote monitoring of pulmonary artery pressures (PAP), with the goal of maintaining this pressure within a therapeutic range by adjusting medications in response to pressure trends. Unlike other implantable devices, the CardioMEMS pressure sensor does not require a battery and therefore, continues to function indefinitely.
In a randomised controlled trial of 550 New York Heart Association (NYHA) class III HF patients with a previous HF hospitalisation, those whose treatment was guided by PAP measurements (treatment group) achieved a 33% reduction in HF-related hospitalisations over an average study duration of 15 months compared with the control arm, who had the device implanted but in whom the data were not used to guide management. The treatment group also had a higher reduction in mean PAP and a greater improvement in quality of life.5
In 2014 CardioMEMS was approved for use in the United States of America by the Food and Drug Administration and in 2016 the Heart Failure Association of the European Society of Cardiology (ESC) included the system in the ESC guidelines for the diagnosis and treatment of acute and chronic HF, indicating that the device may be considered for monitoring symptomatic patients with a previous HF hospitalisation in order to reduce the risk of recurrent hospitalisation (class IIb recommendation, level of evidence B).6
A recent cost-utility analysis suggested that the CardioMEMS HF system is a cost-effective strategy for HF patients in the United Kingdom.7 However, the value of CardioMEMS in Southern Europe, where healthcare costs are significantly lower, remains uncertain and this might lead to an underutilization of the device. In this context, the aim of this study was to estimate the cost-effectiveness of CardioMEMS in Spain.
2. Methods
Study and location
The study was carried out at a tertiary hospital in the Northern area of Barcelona. This hospital was a pioneer in the use of pulmonary pressure sensors in Spain and currently follows the largest number of patients with the CardioMEMS device implanted in Spain, accounting for more than half of the devices implanted.
Comparators
Patients with a CardioMEMS device (treatment group) were compared with patients receiving standard heart failure treatment (control group). All patients were followed in regular follow-up visits at the HF clinic, including a minimum of one visit with a nurse every 3 months and one visit with a physician (cardiologist, internist, or family physician) every 6 months.
For the treatment group, after CardioMEMS implantation, a range of optimal values of PAP was established considering the pulmonary capillary wedge pressure and the transpulmonary gradient of each patient. These PAP thresholds were adjusted during the first week of follow-up. Subsequently, the HF specialist nurses reviewed the PAP values daily and when the established range was exceeded, the cardiologist assessed the possibility of adjusting the diuretic or vasodilator treatment.
During the baseline visit, patients provided written consent for the use of their clinical data for research purposes. Demographic, clinical, echocardiographic, and analytical data were recorded in a specific database (Ethical Committee number PI-18-037).
The Propensity Score Matching8, 9 was used in order to obtain a control group similar in characteristics and size to the treatment group. The analysis of the number of HF admissions was carried out over a period of one year. Additional calculations were made in order to assess the accumulated costs over five years; for those calculations, a 3.5% discount rate was considered as per the National Institute of Health and Care Excellence recommendations.10
The study was performed in compliance with the laws that protect personal data, in accordance with the international guidelines on clinical investigations from the World Medical Association’s Declaration of Helsinki.
Statistical analysis
Categorical variables are expressed as absolute numbers and percentages. Continuous variables are expressed as the mean ± standard deviation, for normal distributions, or the median and interquartile range, for non-normal distribution. Normal distributions were assessed with normal Quantile-Quantile plots. Comparisons between groups were performed with the chi-squared test, for categorical variables, and the student t-test or U Mann-Whitney test, for continuous variables.
The Propensity Score Matching method was used to assess the difference in the number and duration of admissions between groups. The comparators were found using the variables age, sex, NYHA class, left ventricular ejection fraction, and diabetes mellitus.
Patients who died during the first year after implantation of the device were excluded from the study. As for patient admissions, only those related to HF were taken into account.
Although the matching procedure aimed to have 2 similar match controls for each patient with a CardioMEMS device, 3 patients could not be matched taking into account the input variables. Additionally, there were patients for whom the matching procedure found only one match and others for whom it found both. Therefore, the control population is not exactly the same as the treatment population, but very similar, and of a similar size to the CardioMEMS population: 28 patients have 2 matches, 2 patients have 1 match and 5 patients have no matches, leaving 1.65 matches for each treatment patient.
Selection, measurement and valuation of resources and costs
The costs assessed in the clinical study were chosen based on the description of costs from previous studies. To do so, a literature review of CardioMEMS cost-effectiveness analysis (ranging from 2011 to 2021) was conducted. As shown in Table I, four of the six research papers found were conducted in the United States of America, one in different countries of the European Union (United Kingdom, the Netherlands, Belgium, Italy and Germany) and one in Argentina. The mean and median Incremental Cost-Effectiveness Ratio (ICER), converting currency and adjusting for inflation, were of €34,432 and €23,236 respectively; as for the QALY gained after the implant of the CardioMEMS device, the mean and median values were 0.42 and 0.39 respectively.5, 7, 11-14

Table I.
Summary from the literature review.
| Study | Year | Currency | QALY benefit | ICER * | Complication cost * | Complication risk |
|---|---|---|---|---|---|---|
| Abraham et al. | 2011 | USD | 0,30 | €15.801,09 | - | 1,39% |
| Sandhu et al. | 2016 | USD | 0,28 | €77.484,34 | - | - |
| Martinson et al. | 2016 | USD | 0,40 | €20.075,32 | €6.256,26 | - |
| Schmier et al. | 2017 | USD | 0,58 | €47.925,24 | - | - |
| Cowie et al. | 2017 | EUR | 0,57 | €26.398,57 | €2.438,02 | 2,72% |
| Alcaraz et al. | 2021 | ARS | 0,37 | €18.913,27 | €1.087,79 | - |
| Mean: | 0,42 | €34.432,97 | €3.260,69 | 2,06% | ||
| Median: | 0,39 | €23.236,95 | €2.438,02 | 2,06% |
QALY: Quality-Adjusted Life Years; ICER: Incremental Cost-Effectiveness Ratio; * Adjusted for currency and inflation.
Table II shows a valuation of the costs and resources. The cost of the device and its pillow, including taxes, totalled €12,650. The implant procedure totalled €1,528, counting the use and costs derived from the haemodynamics room (including the salary of the interventional cardiologist), according to public prices.13 Outpatient costs, including monitoring, regular visits and possible hospitalisations, are taken into account. Monitoring costs were accounted for as a nurse's 30-minute salary, which is the daily time a nurse needs to consult the pulmonary pressures of CardioMEMS patients (this process is repeated 5 days a week). Regular visits were appointed both with the Heart Failure Cardiologist (every 6 months) and the nurse (every 3 months). Both regular appointments were accounted for as an outpatient visit under public prices at €80 per visit.15 However, both the control and CardioMEMS group underwent monitoring every 6 months with the specialist and every 3 months with the nurse; the monitoring process at the study hospital is more intensive than that of other HF Units.
Table II.
Cost and resources description.
| Parameter | Cost | Source(s) | ||
|---|---|---|---|---|
| CardioMems HF device (each) | 11.440 € | Own | ||
| Pillow (each) | 1.210 € | Own | ||
| Implant procedure | 1.528 € | [15] | ||
| Outpatient costs | ||||
| Monitoring by the nurse (30’ daily, five days a week) | 16,31 € | [20] | ||
| Regular visits with the nurse (Every 4 months) | 80 € | [15] | ||
| Regular visits with the cardiologist (Every 6 months) | 80 € | [15] | ||
| Hospitalisation (per day) | 674 € | [15] | ||
The hospitalisation per day price is an average of €674. No hospital admission costs were accounted for as patients were discharged on the same day of implantation.
Regarding benefits, a gain of 0.3 QALY was taken as reference according to the CHAMPION trial,5 with the social valuation of a unitary QALY in Spain at €25,000.16-17
Currency, price date, and conversion
The costs, resources and benefits of the study and its evaluation were valued in euros (€) as of 2022. The currencies were converted to 2022 euros per the price dates in each study. The reporting of this study follows the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) framework for economic evaluations.18
3. Results
Study population
From September 2019 to November 2021, 42 patients from the HF clinic had a CardioMEMS device implanted. Of these, 7 died during the first year of follow-up (two of them due to cardiovascular causes, none of them HF) and were not included in the study. The control group was selected using Propensity Score Matching and included 58 patients previously admitted to the same HF clinic from January 2001 to November 2021.
CardioMEMS patients were predominantly women, aged 76.1±7.5 years, with preserved and reduced left ventricular ejection fraction (mean LVEF 46±15%), and they were mostly classified as NYHA class III (65.7%). The matched control group presented similar characteristics although ischemic heart disease was more prevalent and there were significant differences in mineralocorticoid receptor antagonist use and devices. Baseline demographics, clinical characteristics, and treatments of the included patients in both groups are shown in Table III.
Table III.
Baseline demographic and clinical characteristics of treatment and matched control groups.
Table III.
Baseline demographic and clinical characteristics of treatment and matched control groups.
| CardioMEMS (n=35) | Matched cohort (n=58) | P-value* | |
|---|---|---|---|
| Age (years) | 76.1±7.5 | 75.4±8.5 | 0.66 |
| Male | 16 (45.7) | 26 (44.8) | 0.93 |
| BMI (Kg/m2) | 29.3±5.5 | 27.6±5.4 | 0.14 |
| LVEF (%) | 46±15 | 51±14 | 0.11 |
| NYHA class II III |
12 (34.3) 23 (65.7) |
20 (34.5) 38 (65.5) |
0.98 0.98 |
| Ischemic aetiology | 8 (22.8) | 28 (48.3) | 0.015 |
| Hypertension | 29 (82.9) | 40 (69.0) | 0.14 |
| Dyslipidaemia | 26 (74.3) | 24 (41.4) | 0.002 |
| Diabetes mellitus | 12 (34.3) | 19 (32.8) | 0.88 |
| Atrial fibrillation | 23 (65.7) | 21 (36.2) | 0.006 |
| COPD | 7 (20.0) | 11 (19.0) | 0.90 |
| Anaemia# | 18 (51.4) | 35 (60.3) | 0.40 |
| Serum creatinine (mg/dl) | 1.29±0.49 | 1.32±0.44 | 0.80 |
| Baseline HF medication Loop diuretic ACEI/ARB/ARNI Beta-blocker Digitalis Hydralazine MRA |
34 (97.1) 26 (74.3) 24 (68.6) 7 (20.0) 8 (22.9) 26 (74.3) |
51 (87.9) 46 (79.3) 26 (44.8) 19 (33.2) 6 (10.3) 10 (17.2) |
0.12 0.57 0.026 0.18 0.10 <0.001 |
| NT-proBNP (pg/ml) | 1806 [976-2825] | 1595 [717-3047] | 0.92 |
| ICD | 7 (20.0) | 2 (3.4) | 0.009 |
| CRT | 7 (20.0) | 1 (1.7) | 0.006 |
Data in mean ± SD, median (IQR) or n (%). *Based on student t test, Mann-Whitney U test or chi-square test. #According to W.H.O. criteria (<13 g/dl in men and <12 g/dl in women). ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin II receptor blocker; ARNI: angiotensin receptor and neprilysin inhibitor; BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRT: cardiac resynchronization therapy; HF: heart failure; ICD: implantable cardiac defibrillator; LVEF: left ventricular ejection fraction; MRA: mineralcorticoid receptor antagonist; NYHA: New York Heart Association; NT-proBNP: N-terminal pro-B-type natriuretic peptide.
Clinical impact
Considering both the control and treatment groups, there was a reduction of 1.25 HF hospitalisations per year for patients with CardioMEMS (0.1) over those without (1.35). Only 2 of the 35 patients with the CardioMEMS had a hospital admission due to HF. On the contrary, hospital admissions were 9.96 days longer for those with the device (22.0 vs. 12.04 days, respectively).
Costs and benefits for the first year
Table IV shows the comparison between costs and benefits for patients with and without the CardioMEMS HF System for the first year. For the treatment group, the device and its implant account for the majority of the costs, while in the control group the hospitalisation costs comprised most of the costs. As for the outpatient costs, both the treatment and control groups had regular appointments with nurses and the cardiologist.
Table IV.
Cost and benefits for patients with and without CardioMEMS, first year.
| With CardioMEMS | % | Without CardioMEMS | % | |||
|---|---|---|---|---|---|---|
| CardioMEMS | Device | 11.440 € | 70,9% | 0 € | 0% | |
| Pillow | 1.210 € | 8% | 0 € | 0% | ||
| Implant procedure | 1.528 € | 9% | 0 € | 0% | ||
| Total device cost | 14.178 € | 87,9% | 0 € | 0% | ||
| Outpatient costs | Monitoring | 69 € | 0,43% | 0 € | 0,00% | |
| Nurse | 240 € | 1,49% | 240 € | 2,11% | ||
| Cardiologist | 160 € | 0,99% | 160 € | 1,41% | ||
| Total outpatient cost | 469 € | 2,87% | 400 € | 3,52% | ||
| Hospitalisation | 1.483 € | 9,19% | 10.955 € | 96,48% | ||
| Total costs | 16.129 € | 100,00% | 11.355 € | 100,00% | ||
| QALY (0,3) | 7.500 € | 100,00% | 0 € | 0,00% | ||
| Total benefits | 7.500 € | 100,00% | 0 € | 0,00% | ||
| Net monetary value per patient | 8.629 € | 11.355 € | ||||
QALY: Quality-Adjusted Life Years.
Valuing a 0,3 QALY benefit from the treatment at €7,50015-16 indicates that the patient costs are €2,726 lower for the treatment group during the first year of treatment.
Comparison of accumulated costs over 5 years
Considering the QALY benefits (applied by the end of the first year of the study), a constant cost of hospitalisation for both groups and a 3,5% discount rate, the accumulated costs of the control group would exceed those of the CardioMEMS group during the second year of treatment due to the much higher costs and risk of hospitalisation of the control group, as shown in Figure I.
Figure I.
Cost evolution over 5 years.

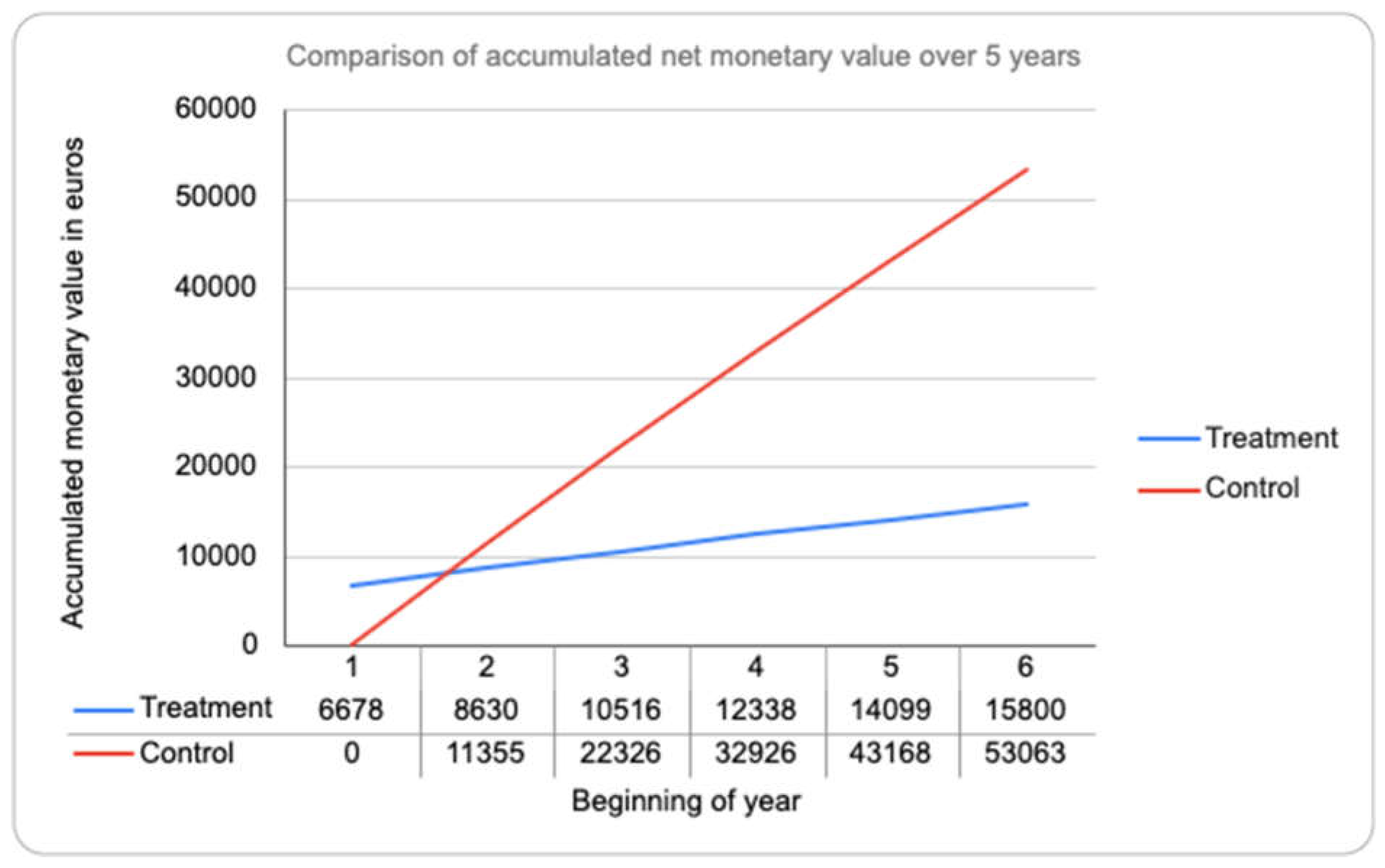
While the initial costs are higher for the CardioMEMS group due to the high costs of the device, they are rapidly outgrown by the costs of the control group, which are mainly driven by hospitalisation costs, as shown in Figure II. By the end of year 5, the accumulated estimated costs for the CardioMEMS and control groups are of €15,800 and €53,063, respectively.
Figure II.
Accumulated monetary value over 5 years.
Sensitivity analysis
A sensitivity analysis was performed in order to evaluate how the results could be affected by changes in key assumptions or variables. The variations were made on the QALY benefits for the treatment group (given how the literature shows different QALY benefits), the hospitalisation costs for the control group (which, as the control patients were drawn from a cohort, are prone to variation) and the device costs (which could be prone to price variations in the future).
Table V shows an ICER analysis variating the hospitalisation costs for the control group (either 50% under or over the base costs) and the QALY benefits (either the 0,3 QALY benefit of the CHAMPION trial, the median 0,4 QALY benefit drawn from the literature or a high 0,5 QALY benefit).
Table V.
Incremental Cost-Effectiveness Ratio for variations in hospitalisation costs for the control group and the QALY benefits for the treatment group.
Table V.
Incremental Cost-Effectiveness Ratio for variations in hospitalisation costs for the control group and the QALY benefits for the treatment group.
| Base (0,3) QALY benefit | Median (0,4) QALY benefit | High (0,5) QALY benefit | |
| -50% hospitalisation costs | 34.154,98 € | 25.616,24 € | 20.492,99 € |
| Base hospitalisation costs | 15.896,32 € | 11.922,24 € | 9.537,79 € |
| +50% hospitalisation costs | -2.362,34 € | -1.771,75 € | -1.417,40 € |
QALY: Quality Adjusted Life Years.
Table VI shows a ratio of the first year treatment patient costs over the control patient costs, also variating the control hospitalisation costs and the QALY benefits (and, unlike the previous ICER, adding the possibility of no QALY benefits).
Table VI.
Ratio of treatment over control costs for variations in hospitalisation costs for the control group and QALY benefits for the treatment group.
Table VI.
Ratio of treatment over control costs for variations in hospitalisation costs for the control group and QALY benefits for the treatment group.
| 0 QALY benefit | Base (0,3) QALY benefit | Median (0,4) QALY benefit | |
| -50% hospitalisation costs | 2,74 | 1,47 | 1,04 |
| Base hospitalisation costs | 1,42 | 0,76 | 0,54 |
| +50% hospitalisation costs | 0,96 | 0,51 | 0,36 |
QALY: Quality Adjusted Life Years.
Finally, Table VII shows an ICER yet again variating hospitalisation costs for the control patients and now variating device costs for the treatment patients, assuming a base 0,3 QALY benefit.
Table VII.
Incremental Cost-Effectiveness Ratio for variations in hospitalisation costs for the control group and the devices costs for the treatment group.
Table VII.
Incremental Cost-Effectiveness Ratio for variations in hospitalisation costs for the control group and the devices costs for the treatment group.
| -25% device costs | Base device costs | +25% device costs | |
| -50% hospitalisation costs | 22.339,98 € | 34.154,98 € | 45.969,98 € |
| Base hospitalisation costs | 4.081,32 € | 15.896,32 € | 27.711,32 € |
| +50% hospitalisation costs | -14.177,34 € | -2.362,34 € | 9.452,66 € |
Some of the ICERs in the sensitivity analysis are negative; without any context, this could indicate that either the CardioMEMS treatment is more costly and less effective than the usual management, or that its costs are lesser and it is more effective. However, given the cost structure and valuation of both the treatment and control patients’ costs, and that these negative ratios appear only when the hospitalisation costs of the control group are further increased, it is the latter: when these costs are increased, the CardioMEMS treatment is both less costly and more effective than usual care.
4. Discussion
To our knowledge, this is the first study to perform a cost-effective analysis of the CardioMEMS system in a HF clinic from Southern Europe. Remote monitoring of PAP with CardioMEMS was associated with a strong reduction in HF hospitalisations at 1 year.
Considering the benefit in QALY and the HF admissions prevented, the CardioMEMS system outperformed usual management with a net monetary value difference of 2,731€ per patient at 1 year. The calculated cost per extra QALY gained with remote PAP monitoring is 15.896€, much lower than the current cost-effectiveness threshold accepted in Spain (25.000€).16
Results were consistent in most of the different sensitivity analyses performed, modifying QALY benefits for the treatment group, hospitalisations’ costs for the control group and device costs (Tables V to VII). Hospital admissions for the treatment group were considerably longer than those of the matched control group. A possible explanation is that patients who are admitted despite hemodynamic-guided treatment are more complex and require longer admissions.
Table VIII shows the cost structure along that of the six other studies conducted since the CHAMPION trial. The actual cost shown in this article is similar to the studies by Schmier et al., Cowie et al. and Alcaraz et al., all published after 2017 and all very similar in their cost structure: device, implantation, complications, monitoring, usual cost of heart failure treatment and possible hospitalisations. This work has considered all these costs except for complications (due to their small number in our cohort, as only one patient had a vascular complication) and introduced costs related to regular visits with the nurse and HF cardiologist. Regarding the valuation of costs, ours were most similar to those described in Cowie et al, probably due to a similar context in terms of healthcare.
The CHAMPION trial found that the CardioMEMS implant had a benefit of 0.3 QALY for the patient; we used it as an effectiveness benchmark for our study. However, it could be considered a low-range benefit compared to the mean and median of other published articles, at a benefit of 0,42 and 0,39 QALY respectively. This could mean that the effectiveness is higher than what we have considered, making the ratio of cost per effectiveness lower (as shown in the ICER). In that sense, the sensitivity analysis provided in the results section, and particularly Table VI, has been useful to compare the cost-effectiveness ratios with different effectiveness benchmarks.
Limitations
These results should be interpreted in the context of several potential limitations. Despite having more implants than any other healthcare centre in Southern Europe and being responsible for over half of the implants performed in Spain, the sample is limited and from a single centre. We have tried to mitigate these limitations by matching each treated patient with two non-treated patients of similar characteristics. Despite the propensity match, there were some small differences between the two study groups, partly due to the control group coming from a historical cohort. Of note, a common follow-up protocol with the HF nurse and doctor was applied to all patients, limiting possible bias introduced by different management strategies.
Patients who died during the first year of follow-up were excluded in order to analyse HF hospitalisations during the first year, so the study is limited to completers of one year follow-up. Thus, there is a potential selection bias with a less severe HF population. Furthermore, the study only included NYHA class II and III HF patients, so the results may not be applicable to NYHA class I and IV patients.
Finally, the relative reduction in HF hospitalisations in the CardioMEMS subgroup was greater than that observed in the CHAMPION trial, but similar to other recent reports.19 For this reason a sensitivity analysis was performed with variations in hospitalisation costs for the control group.
Implications moving forward
HF hospitalisation costs in Spain are lower in relation to the United Kingdom and the United States of America. Therefore, one could think the potential savings by avoiding admissions with remote PAP monitoring are also lower. This belief currently leads to an underutilization of this invasive remote monitoring strategy in Southern Europe in comparison to other countries. Our results suggest that the CardioMEMS HF system is also a cost-effective strategy for HF patients in the Spanish healthcare setting.
5. Conclusions
This analysis suggests that remote monitoring of PAP with CardioMEMS HF system is a cost-effective strategy in the Spanish healthcare setting. Considering the benefit in QALY and in HF admissions prevented, the CardioMEMS system outperforms usual management for selected patients with high risk of HF hospitalisation.
Conflicts of Interest
Authors Antoni Bayes Genis and Pau Codina have received speaker's fees from Abbott. Author José Ángel Vicente Gómez is a recipient of a Collaboration Grant from the Spanish Ministry of Education and Vocational Training.
References
- Sicras-Mainar A, Sicras-Navarro A, Palacios B, Varela L, Delgado JF. Epidemiology and treatment of heart failure in Spain: the HF-PATHWAYS study. Rev Esp Cardiol (Engl Ed). 2022 Jan;75(1):31-38. English, Spanish. [CrossRef]
- Escobar C, Varela L, Palacios B, et al. Costs and healthcare utilisation of patients with heart failure in Spain. BMC Health Serv Res. 2020 Oct 20;20(1):964. [CrossRef]
- Maggioni AP, Dahlström U, Filippatos G, et al. Heart Failure Association of the European Society of Cardiology (HFA). EURObservational Research Programme: regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur J Heart Fail. 2013 Jul;15(7):808-17. [CrossRef]
- Bayes-Genis A, Codina P, Abdul-Jawad Altisent O, at al. Advanced remote care for heart failure in times of COVID-19 using an implantable pulmonary artery pressure sensor: the new normal. Eur Heart J Suppl. 2020 Dec 23;22(Suppl Pt t):P29-P32. [CrossRef]
- Abraham WT, Adamson PB, Bourge RC, et al. CHAMPION Trial Study Group. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet. 2011 Feb 19;377(9766):658-66. [CrossRef]
- Ponikowski P, Voors AA, Anker SD, et al. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016 Jul 14;37(27):2129-2200. [CrossRef]
- Cowie MR, Simon M, Klein L, Thokala P. The cost-effectiveness of real-time pulmonary artery pressure monitoring in heart failure patients: a European perspective. Eur J Heart Fail. 2017 May;19(5):661-669. [CrossRef]
- Martens EP, Pestman WR, de Boer A, Belitser SV, Klungel OH. Systematic differences in treatment effect estimates between propensity score methods and logistic regression. Int J Epidemiol 2008;37:1142–1147. [CrossRef]
- Heinze G, J ̈uni P. An overview of the objectives of and the approaches to propensity score analyses. Eur Heart J 2011;32:1704–1708. [CrossRef]
- National Institute of Health and Care Excellence. Reviewing our methods for health technology evaluation: consultation. 2020. Available at: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/chte-methods-consultation (accessed on 12 December 2022).
- Sandhu AT, Goldhaber-Fiebert JD, Owens DK, Turakhia MP, Kaiser DW, Heidenreich PA. Cost-effectiveness of implantable pulmonary artery pressure monitoring in chronic heart failure. JACC Heart Fail. 2016;4(5):368-375. [CrossRef]
- Martinson M, Bharmi R, Dalal N, Abraham WT, Adamson PB. Pulmonary artery pressure-guided heart failure management: US cost-effectiveness analyses using the results of the Champion Clinical Trial. Eur J Heart Fail. 2016;19(5):652-660. [CrossRef]
- Schmier JK, Ong KL, Fonarow GC. Cost-effectiveness of remote cardiac monitoring with the CARDIOMEMS Heart Failure System. Clin Cardiol. 2017;40(7):430-436. [CrossRef]
- Alcaraz A, Rojas-Roque C, Prina D, et al. Improving the monitoring of chronic heart failure in Argentina: Is the implantable pulmonary artery pressure with cardiomems heart failure system cost-effective? Cost Eff Resour Alloc. 2021;19(1). [CrossRef]
- Generalitat de Catalunya. Ordre SLT/71/2020, de 2 de juny, per la qual es regulen els supòsits i conceptes facturables i s'aproven els preus públics corresponents als serveis que presta l'Institut Català de la Salut. 2020. Available at: https://cido.diba.cat/legislacio/10263520/ordre-slt712020-de-2-de-juny-per-la-qual-es-regulen-els-suposits-i-conceptes-facturables-i-saproven-els-preus-publics-corresponents-als-serveis-que-presta-linstitut-catala-de-la-salut-departament-de-salut (accessed on 13 December 2022).
- Vallejo-Torres L, García-Lorenzo B, Serrano-Aguilar P. Estimating a cost-effectiveness threshold for the Spanish NHS. Health Econ. 2018;27(4):746-761. [CrossRef]
- Vallejo-Torres L, García-Lorenzo B, Rivero-Arias O, Pinto-Prades JL. The societal monetary value of a QALY associated with EQ-5D-3L health gains. Eur J Health Econ. 2020;21(3):363-379. [CrossRef]
- Husereau D, Drummond M, Augustovski F, et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Eur J Health Econ. 2022;23(8):1309-1317. [CrossRef]
- Shavelle DM, Desai AS, Abraham WT, et al. CardioMEMS Post-Approval Study Investigators. Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmonary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes From the CardioMEMS Post-Approval Study. Circ Heart Fail. 2020 Aug;13(8):e006863. [CrossRef]
- Institut Català de Salut. LLIBRE DE RETRIBUCIONS 2022, PERSONAL ESTATUTARI DE L’ICS. 2022. Available at: https://administraciopublica.gencat.cat/web/.content/funcio-publica/empleats-publics/retribucions/2022/Llibre-de-retribucions-2022.pdf (accessed on 15 December 2022).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



