Submitted:
31 December 2021
Posted:
04 January 2022
You are already at the latest version
Abstract
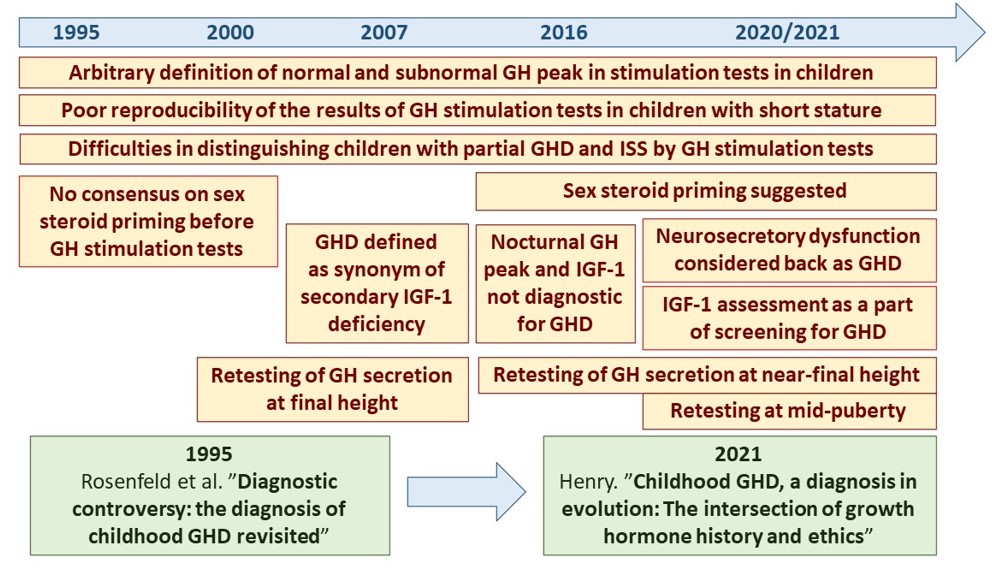
According to current guidelines, growth hormone (GH) therapy is strongly recommended in children and adolescents with GH deficiency (GHD) in order to accelerate growth rate and attain normal adult height. The diagnosis of GHD requires demonstration of decreased GH secretion in stimulation tests, below the established threshold value. Currently, GHD in children is classified as secondary insulin-like growth factor-1 (IGF-1) deficiency. Most of children diagnosed with isolated GHD presents with normal GH secretion at the attainment of near-final height or even in mid-puberty. The most important clinical problems, related to the diagnosis of isolated GHD in children and to optimal duration of rhGH therapy include: arbitrary definition of subnormal GH peak in stimulation tests, disregarding factors influencing GH secretion, insufficient diagnostic accuracy and poor reproducibility of GH stimulation tests, discrepancies between spontaneous and stimulated GH secretion, clinical entity of neurosecretory dysfunction, discrepancies between IGF-1 concentrations and results of GH stimulation tests, significance of IGF-1 deficiency for the diagnosis of GHD, a need for validation IGF-1 reference ranges. Many of these issues have remained unresolved for 25 years or even longer. It seems that finding solutions to them should optimize diagnostics and therapy of children with short stature.
Keywords:
short stature
; growth hormone deficiency
; insulin-like growth factor-1
; growth hormone stimulation tests
; neurosecretory dysfunction
; final height
; retesting
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



