Submitted:
15 June 2026
Posted:
16 June 2026
You are already at the latest version
Abstract
(1) Background/Objectives: Blood-based biomarkers have emerged as practical tools for identifying Alzheimer’s disease (AD) pathology in patients with mild cognitive impairment (MCI). Among them, plasma phosphorylated tau217 (p-tau217) demonstrates strong associations with cerebral amyloid deposition. In parallel, the easy Z-score Imaging System (eZIS), a quantitative brain perfusion SPECT analysis tool, has been widely used to detect characteristic AD-related hypoperfusion patterns. Although both measures reflect distinct AD processes, the relationship between plasma p-tau217 and eZIS in MCI remains unclear. (2) Methods: This retrospective study included 62 patients with MCI who underwent plasma p-tau217 testing and brain perfusion SPECT with eZIS analysis. Associations between plasma p-tau217 and the three eZIS indices (severity, extent, and ratio) were evaluated. Exploratory subgroup analyses were performed using a previously reported plasma p-tau217 threshold of 0.63 pg/mL. In addition, a validation sub-cohort of 21 participants who underwent plasma p-tau217 testing, eZIS, and amyloid PET was analyzed to assess concordance with cerebral amyloid pathology. (3) Results: Among the three eZIS indices, severity demonstrated the highest sensitivity relative to elevated plasma p-tau217 levels. However, all eZIS indices showed limited discriminative performance. Optimal eZIS cutoff values derived from the present cohort were higher than previously reported thresholds. In the amyloid PET-validated sub-cohort, plasma p-tau217 demonstrated closer concordance with amyloid positivity than any individual eZIS parameter. The reduced performance of eZIS appeared to be associated with advanced age, substantial vascular burden, white matter lesions, and cerebral atrophy. (4) Conclusions: Plasma p-tau217 showed a stronger association with cerebral amyloid pathology than eZIS indices in this elderly MCI cohort. Nevertheless, eZIS may provide complementary information regarding downstream neurodegenerative and cerebrovascular processes that are not directly captured by plasma biomarkers. This integrated approach highlights plasma p-tau217 as a primary screening tool for amyloid pathology to guide disease-modifying therapies (DMTs), alongside eZIS for tracking follow-up mixed co-pathologies.
Keywords:
Alzheimer’s disease
; mild cognitive impairment
; plasma p-tau217
; amyloid PET
; eZIS
; cerebral perfusion SPECT
; plasma biomarkers
; neurodegeneration
1. Introduction
The recent advent of disease-modifying therapies (DMTs) has fundamentally shifted the clinical paradigm of Alzheimer’s disease (AD), making early and accurate diagnosis paramount, especially at the stage of mild cognitive impairment (MCI) [1,2]. Because the therapeutic benefits of these interventions diminish markedly once high tau burden accumulates and irreversible neurodegeneration occurs, utilizing reliable biomarkers to detect incipient pathological changes is now essential [3].
Although amyloid and tau positron emission tomography (PET) and cerebrospinal fluid (CSF) biomarkers are currently considered reference standards for in vivo assessment of AD pathology, their high costs and limited availability create significant barriers to broader clinical accessibility and early intervention. Consequently, single-photon emission computed tomography (SPECT) has emerged as a more practical, widely available, and affordable alternative. SPECT facilitates AD diagnosis by detecting regional cerebral hypoperfusion in AD-signature areas, such as the temporoparietal junction, posterior cingulate cortex, and precuneus. Historically, the clinical utility of SPECT was hindered by its reliance on subjective visual interpretation. To address this, the easy Z-score Imaging System (eZIS), introduced by Matsuda et al. in 2007, provided an objective and quantitative method for evaluating hypoperfusion [4,5,6]. Today, it remains widely available in many countries and continues to play an important role in dementia evaluation. The clinical application of eZIS has been extensively validated for distinguishing very early-stage AD, predicting the progression from MCI to dementia, and differentiating among other neurodegenerative disorders [7,8,9,10,11,12,13,14,15].
To detect early pathological changes more efficiently, plasma biomarkers have shown tremendous clinical potential [16]. This is particularly relevant in Asian populations, where cultural reluctance regarding spinal procedures often hinders the widespread application of cerebrospinal fluid (CSF) biomarkers, highlighting the critical need for blood-based alternatives [17]. Standalone plasma p-tau217 assays have demonstrated high concordance with established amyloid biomarkers (amyloid PET and CSF Aβ42/40) and strong discriminative ability in preclinical AD, offering lower costs and technical barriers compared to ratio-based tests [18,19,20,21,22,23,24,25,26,27,28,29,30,31].
While the robust correlation between plasma p-tau217 and amyloid PET is well-documented, and the relationship between eZIS and amyloid PET has been independently established [7,8,9], the direct diagnostic concordance between plasma p-tau217 and eZIS remains an unexplored gap in the literature. Clarifying this relationship is essential for translating research findings into practical clinical diagnostic criteria. Furthermore, little is known regarding how these biomarkers behave in clinically heterogeneous MCI populations characterized by advanced age, white matter disease, brain atrophy, and vascular comorbidities [32].
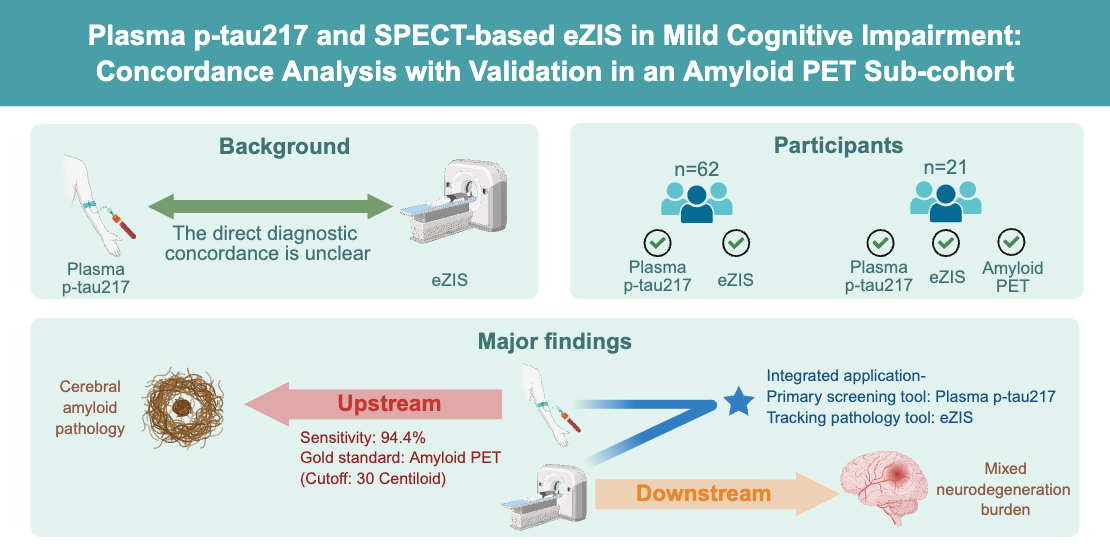
Therefore, the primary aim of this study is to conduct a head-to-head evaluation of the diagnostic concordance between plasma p-tau217 levels and eZIS parameters. To ensure the reliability of the correlations between these blood-based biomarkers and brain imaging characteristics, all assessments were conducted within a strictly limited time interval. Additionally, we evaluated a unique validation sub-cohort that underwent plasma p-tau217 testing, eZIS analysis, and amyloid PET imaging, allowing for a direct comparison of these biomarkers against cerebral amyloid pathology. Through this multimodal approach, we sought to clarify the complementary and distinct contributions of blood-based and imaging-based biomarkers in the assessment of MCI, see Figure 1.
2. Materials and Methods
2.1. Subjects and Research Procedure
This retrospective study recruited individuals with MCI who presented at the memory clinic of National Cheng Kung University Hospital (NCKUH). The clinical diagnosis of MCI was established by a senior behavioral neurologist.
Initially, the study design did not impose a strict temporal limitation between blood sampling for plasma p-tau217 and the SPECT (eZIS) imaging, resulting in testing intervals extending up to eight years in some cases. However, preliminary evaluations revealed that such extended gaps introduced profound heterogeneity into the dataset. As established in the literature, changes in regional cerebral blood flow, as reflected by eZIS parameters, are inherently nonlinear [33,34], and the accumulation rate of plasma p-tau217 varies significantly across different stages of disease progression [20]. Consequently, these extended intervals severely compromised the diagnostic concordance and distributional stability between the two modalities. To balance sample size with methodological rigor and minimize confounding effects associated with divergent disease progression trajectories, a strict temporal restriction was enforced. Ultimately, the inclusion criteria for the overall cohort required: (1) a Clinical Dementia Rating (CDR) [35] score of 0.5, and (2) a temporal interval of less than two years between the plasma p-tau217 assay and SPECT imaging.
To further investigate the diagnostic concordance against the established gold standard, we evaluated a highly characterized multimodal validation sub-cohort comprising participants who additionally underwent amyloid PET imaging. For this specific subset (n = 21), the temporal restriction between the blood test and SPECT was relaxed to maximize sample inclusion. Because amyloid PET serves as the definitive pathological anchor, it provided a robust objective basis for the head-to-head comparison with plasma p-tau217 and eZIS, thereby mitigating potential biases introduced by the extended time interval. Detailed demographic and interval characteristics for this sub-cohort are elaborated in the Results section.
General exclusion criteria for all participants included a history of stroke, hydrocephalus, traumatic brain injury, severe chronic kidney disease (stages 4-5), and major psychiatric disorders, including clinical depression. The detailed participant selection process and study workflow are illustrated in Figure 2.
2.2. Clinical Diagnosis
A diagnosis of MCI was made according to Petersen’s criteria: (1) memory complaint, preferably corroborated by an informant; (2) impaired memory function for age and education; (3) preserved general cognitive function; (4) intact activities of daily living; (5) not demented [36].
2.3. Examination Tools
2.3.1. Cognitive Assessments
2.3.2. Brain Perfusion SPECT and eZIS Analysis
Brain perfusion SPECT imaging was performed approximately 20 minutes after intravenous administration of 740 MBq (20 mCi) of Tc-99m ethyl cysteinate dimer (ECD). Image acquisition was performed using a dual-head gamma camera equipped with low-energy high-resolution collimators. Regional cerebral blood flow abnormalities were analyzed using the easy Z-score Imaging System (eZIS), a voxel-based analytical platform developed for objective quantification of AD-associated hypoperfusion patterns. Three predefined eZIS indices were calculated:
- Severity: Severity represents the mean positive Z-score within the predefined AD-specific volume of interest (VOI) and reflects the magnitude of regional cerebral blood flow reduction.
- Extent: Extent represents the percentage of voxels within the AD-specific VOI demonstrating significant hypoperfusion (Z-score 2).
- Ratio: Ratio represents the proportion of significantly hypoperfused voxels within the AD-specific VOI relative to those within the entire brain and reflects the specificity of hypoperfusion distribution.
Accuracies for discrimination between healthy controls and patients with very early AD were 85%, 86%, and 80%, respectively. Cutoff values for discrimination were 1.19, 14.2%, and 2.22 for severity, extent, and ratio, respectively. These thresholds were used for exploratory analyses only [4,5,13,14,15].
2.3.3. Plasma p-tau 217 Measurements
Plasma p-tau217 levels were quantified using the ALZpath Simoa assay. To account for the diurnal variation of plasma p-tau217 reported in previous studies, blood samples were collected during morning clinic hours whenever possible [39,40]. Patients were stratified into high- and low-level groups based on a plasma p-tau217 cutoff value of 0.63 pg/mL [41,42,43].
2.3.4. Amyloid PET Imaging
A subset of participants underwent amyloid PET imaging as part of their clinical evaluation. Following intravenous administration of 300 MBq of F-18 florbetaben, PET acquisition was performed approximately 90 minutes post-injection using a Biograph mCT Flow PET/CT scanner (Siemens Healthineers, Erlangen, Germany). Quantitative image analysis was performed using the Centiloid (CL) scale. Based on contemporary recommendations, a Centiloid value of 30 was used to define amyloid positivity [3].
2.3.5. MRI Assessment
Brain MRI examinations were reviewed for the presence and severity of white matter hyperintensities. Periventricular and deep white matter hyperintensities were visually graded according to the Fazekas scale (Grade 0: absent; Grade 1: punctate; Grade 2: beginning confluence; Grade 3: large confluent) [44,45,46]. The Fazekas scale was visually interpreted by author ILH.
2.3.6. TRODAT Imaging
A subset of participants underwent Tc-99m TRODAT-1 SPECT imaging as part of routine clinical evaluation. Following intravenous administration of 925 MBq (25 mCi) Tc-99m TRODAT-1, SPECT imaging was performed approximately 4 hours after injection. The following quantitative measures were recorded: the right striatal TRODAT-1 binding ratio, the left striatal TRODAT-1 binding ratio, and the striatal asymmetry index. Given the limited number of available examinations, TRODAT findings were analyzed descriptively.
2.4. Statistical Analysis
All statistical analyses were performed using Prism version 10 (GraphPad Software, Boston, MA, USA).
Continuous variables were summarized as mean standard deviation or median with interquartile range, as appropriate. Categorical variables were summarized as counts and percentages. The Mann-Whitney U test and Fisher’s exact test were used for continuous and categorical variables, respectively. A two-tailed p-value0.05 was considered statistically significant.
Further analysis can be separated into three parts. First, we evaluated the diagnostic performance of each indicator by calculating its sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Second, the Youden index was utilized to determine the optimal cutoff values for our study cohort, which were then compared against the established reference cutoffs. Third, we calculated the overall diagnostic accuracy of each indicator, defined as the proportion of correctly classified subjects (true positives and true negatives) out of the total sample [47].
3. Results
3.1. Clinical Features
We identified 62 MCI patients who met the research criteria, including 38 patients with high plasma p-tau217 level and 24 patients with low plasma p-tau217 level, defined by the threshold of plasma p-tau217 0.63 pg/mL. The demographic and clinical characteristics are listed in Table 1. Due to the complexity of the demographic data table, a simplified distribution of participants across various categories, stratified by plasma p-tau217 and eZIS three indicators, is presented in Appendix Table A1, Table A2 and Table A3.
Additionally, we identified 21 MCI patients who met the criteria for the multimodal validation sub-cohort, comprising 18 mild cognitive impairment due to Alzheimer’s disease (AD MCI) and 3 mild cognitive impairment due to non-Alzheimer’s disease (non-AD MCI) cases, as defined by an amyloid PET Centiloid (CL) threshold of 30. The demographic and clinical characteristics of this specific sub-cohort are detailed in Table 2. Compared with the overall cohort, this subgroup demonstrated a high prevalence of amyloid positivity, consistent with referral bias in clinical amyloid PET utilization. The mean Centiloid value was markedly higher among amyloid-positive participants than among amyloid-negative participants.
3.2. Outcomes
3.2.1. The Relation Between the eZIS Three Indicators and Plasma p-tau217
The relationship between plasma p-tau217 concentrations and the three eZIS indices was evaluated in the entire cohort. Participants with higher plasma p-tau217 concentrations tended to demonstrate higher eZIS severity, extent, and ratio values. However, substantial overlap was observed between groups, indicating considerable heterogeneity within the MCI population. Among the three eZIS indices, severity demonstrated the strongest association with elevated plasma p-tau217 levels. The mean severity value was numerically higher in the high p-tau217 group than in the low p-tau217 group, although the difference did not reach statistical significance. Similarly, extent and ratio values were also numerically higher in the high p-tau217 group but exhibited broad distributions and overlapping interquartile ranges. These findings suggest that although cerebral perfusion abnormalities and plasma p-tau217 levels may be biologically related, the two biomarkers likely capture distinct aspects of disease progression.
Exploratory diagnostic performance analyses were performed using previously established eZIS reference thresholds. Among the three eZIS indices, severity demonstrated the highest sensitivity relative to elevated plasma p-tau217 levels. Although severity demonstrated the greatest sensitivity, specificity remained modest for all indices. Overall, concordance between plasma p-tau217 status and eZIS abnormalities was limited, suggesting that these biomarkers do not provide interchangeable information. Diagnostic performance metrics were listed in Table 3.
Following the results, we tried to use the Youden index to find out the ideal eZIS cutoffs in this study. The AUC for each index is approximately 0.57, see Figure 3, Figure 4 and Figure 5. The new cutoffs are 1.78, 21.46, and 3.805 for severity, extent, and ratio, respectively. Compared with the original cutoffs, 1.19, 14.2, and 2.22 for severity, extent, and ratio, the new cutoffs are relatively higher than the original ones. Since we excluded stroke patients, the relatively high values of the three indices are most likely caused by chronic vascular pathology, as indicated by the MRI reports and Fazekas scale results.
3.2.2. The Amyloid PET Positive Probability, eZIS, and Plasma p-tau217
The availability of complete data across all three diagnostic platforms represents a rare clinical scenario, enabling a precise head-to-head validation against cerebral amyloid pathology. Within this multimodal validation cohort, 14 patients had a time interval of less than two years between plasma p-tau217 sampling and eZIS imaging, while seven had an interval exceeding two years, a relaxation permitted to maximize the inclusion of these high-value data. With amyloid PET serving as the absolute reference standard, plasma p-tau217 demonstrated superior diagnostic performance compared to eZIS. Diagnostic performance metrics were listed in Table 4.
Although plasma p-tau217 showed stronger agreement with amyloid PET positivity, all diagnostic estimates should be interpreted cautiously because of the limited number of amyloid-negative participants. Notably, several amyloid-positive participants exhibited only mild abnormalities on eZIS, whereas some participants with elevated eZIS indices demonstrated relatively low amyloid burden. These observations support the notion that plasma p-tau217 and cerebral perfusion abnormalities reflect related but biologically distinct processes.
3.2.3. Summary of Main Findings
Three principal findings emerged from this study. First, plasma p-tau217 and eZIS indices demonstrated only modest concordance in a clinically heterogeneous MCI population. Second, optimal eZIS thresholds in this elderly cohort were higher than previously reported reference values, suggesting an influence of vascular pathology, white matter disease, and cerebral atrophy on perfusion-based biomarkers. Third, within the amyloid PET validation cohort, plasma p-tau217 demonstrated closer concordance with cerebral amyloid pathology than any individual eZIS parameter. Collectively, these findings suggest that plasma p-tau217 and eZIS provide complementary rather than interchangeable information regarding biological processes occurring along the Alzheimer disease continuum.
4. Discussion
Based on the three key findings. We proposed the following discussion.
4.1. Plasma p-tau217 and eZIS Reflect Different Biological Processes
A key observation of this study is that plasma p-tau217 and eZIS should not be viewed as competing biomarkers. Rather, they appear to reflect different biological processes occurring along the AD continuum.
According to the contemporary AT(N) framework, biomarkers may be classified according to the pathological processes they represent, including amyloid deposition (A), tau pathology (T), and neurodegeneration (N) [3]. Plasma p-tau217 has consistently demonstrated strong associations with both amyloid and tau pathology and is increasingly regarded as a blood-based surrogate marker of AD pathology. In contrast, cerebral perfusion abnormalities measured by eZIS are likely to reflect downstream functional consequences of neurodegeneration, synaptic dysfunction, and network disconnection.
To interpret these results, we propose a conceptual visualization using two opposing arrows. Plasma p-tau217 acts as an arrow pointing directly to amyloid pathology, representing the upstream core of AD. Conversely, eZIS highlights hypoperfusion, reflecting downstream manifestations. Given these opposing positions in the pathological cascade, we infer that complex co-pathologies exert a more profound influence on the presentation of eZIS.
This biological distinction may explain the relatively modest concordance observed between plasma p-tau217 and eZIS in the present study. Amyloid accumulation may precede substantial reductions in cerebral blood flow by several years, whereas perfusion abnormalities may become more prominent during later stages characterized by neuronal injury and functional impairment. Consequently, discordance between these biomarkers should not necessarily be interpreted as diagnostic disagreement but rather as evidence that they capture different stages of disease progression.
4.2. Why Was eZIS Performance Lower Than Expected?
Previous studies have reported favorable diagnostic performance of eZIS for distinguishing early AD from cognitively normal individuals and for predicting progression from MCI to dementia. In contrast, the present study demonstrated relatively limited discrimination by all three eZIS indices.
Several factors may explain this finding. Primarily, the present cohort was substantially older than the populations evaluated in the original eZIS validation studies. With a mean age exceeding 75 years, these patients presented with highly heterogeneous clinical profiles. Notably, a subset of participants who underwent TRODAT imaging exhibited relatively low binding ratios, suggesting the presence of mixed neurodegenerative pathologies rather than pure AD, see Appendix Table A4. Additionally, cerebral perfusion is inherently influenced by multiple age-related processes beyond AD pathology. Common vascular comorbidities in this older cohort, such as chronic hypertension, small vessel disease, and white matter hyperintensities, can independently contribute to regional reductions in cerebral blood flow. Consequently, these perfusion abnormalities render SPECT less specific for cerebral amyloid deposition compared to molecular biomarkers directly related to AD [48,49]. Finally, structural brain changes further confound eZIS measurements through partial volume effects. Although the system provides objective quantification of regional cerebral blood flow, significant cortical volume loss (cerebral atrophy) prevalent in elderly populations can artificially reduce measured perfusion values. Together, these structural and vascular confounders increase variability and limit the overall diagnostic specificity of perfusion-based biomarkers in real-world clinical settings.
These considerations are supported by our ROC analyses, which suggested optimal eZIS thresholds substantially higher than previously reported reference values. This observation suggests that standard cutoff values derived from younger or less vascularly burdened populations may not be directly applicable to elderly memory-clinic populations.
Furthermore, as contemporary diagnostic frameworks increasingly incorporate concepts of brain resilience and cognitive reserve, it is understood that clinical manifestations of cognitive decline are often delayed in individuals with higher educational and socio-behavioral engagement [50,51,52]. As a result, these patients frequently present at an older age, harboring a significantly higher burden of age-related comorbidities, such as cerebrovascular pathology and brain atrophy. This demographic reality explains the attenuated diagnostic performance of eZIS and underscores the need for age- and comorbidity-adjusted diagnostic approaches in real-world clinical settings.
4.3. Validation Against Amyloid PET
The validation sub-cohort provided an opportunity to compare plasma p-tau217 and eZIS directly against cerebral amyloid pathology.
Within this subgroup, plasma p-tau217 demonstrated stronger concordance with amyloid PET positivity than any individual eZIS parameter. This finding is consistent with a growing body of literature demonstrating close associations between plasma p-tau217 and amyloid PET across the AD continuum.
From a biological perspective, this result is not unexpected. Plasma p-tau217 is closely linked to molecular events occurring during amyloid-associated tau dysregulation, whereas cerebral perfusion abnormalities represent functional consequences that may be influenced by multiple additional factors.
Furthermore, previous large-scale studies have reported that the PPV of plasma p-tau217 for predicting amyloid PET positivity can reach approximately 93% [20,53]. In contrast, our head-to-head comparison revealed that the highest PPV between plasma p-tau217 and eZIS indicators was only 66%. This discrepancy of nearly 30% highlights the significant impact of clinical cofactors. Specifically, complex co-pathologies and varied trajectories of downstream neurodegeneration can independently lead to cerebral hypoperfusion, thereby uncoupling functional imaging results from pure molecular AD pathology.
Importantly, however, several participants demonstrated discordant findings between plasma p-tau217, eZIS, and amyloid PET. Some amyloid-positive individuals exhibited only mild perfusion abnormalities, whereas others demonstrated substantial perfusion reductions despite relatively modest amyloid burden. Such observations further support the concept that perfusion imaging and blood biomarkers provide complementary information rather than redundant measurements.
Accordingly, our findings should not be interpreted as evidence that plasma p-tau217 can replace functional neuroimaging. Instead, plasma biomarkers and perfusion imaging appear to contribute distinct information regarding pathological burden, neurodegeneration, and cerebrovascular status.
4.4. Clinical Implications
The present findings yield several practical implications for clinical practice.
Foremost, plasma p-tau217 appears highly suitable as an initial screening biomarker for identifying individuals who harbor underlying AD pathology. Compared with amyloid PET or cerebrospinal fluid analyses, blood-based testing offers substantial advantages in terms of accessibility, cost-effectiveness, and patient acceptance. Thus, blood-based biomarkers represent a robust, non-invasive, and practical modality for aiding AD diagnosis and prognostic staging, particularly serving as a primary gatekeeper to identify patients suitable for DMTs. Furthermore, recent longitudinal clock models utilizing plasma p-tau217 have demonstrated that older individuals experience a markedly shorter interval between p-tau217 positivity and the onset of clinical symptoms [54]. As these authors emphasized, age-related co-pathologies, such as cerebrovascular disease, not only confound functional imaging results but also actively accelerate the progression of dementia in p-tau217-positive elderly patients.
In addition, despite its weaker association with specific amyloid pathology, eZIS retains significant clinical utility. Perfusion abnormalities reflect the downstream functional impact of the disease on cerebral networks, capturing contributions from both neurodegenerative and vascular mechanisms. Consequently, the diagnostic value of eZIS may be particularly pronounced in early-onset AD (EOAD), where patients typically present with a purer AD pathological profile and a minimal burden of vascular co-pathologies. In these cases of relatively pure AD, eZIS can effectively delineate the characteristic AD-specific hypoperfusion patterns. Conversely, in patients with mixed etiologies, elevated or atypical eZIS indices can serve as a critical warning sign, indicating the presence of overlapping pathologies and the need for further diagnostic workup. Importantly, in the context of DMTs, eZIS holds potential utility for longitudinal follow-up. It can serve as a valuable tool to track downstream functional changes and evaluate whether a suboptimal clinical response to therapy is driven by the progression of mixed co-pathologies.
Ultimately, the integration of blood-based biomarkers and functional imaging provides a more comprehensive assessment than either modality alone. While plasma biomarkers can accurately detect the presence of molecular AD pathology, perfusion imaging characterizes its downstream functional consequences and the compounding effects of coexisting cerebrovascular disease. This multimodal approach will become increasingly vital as DMTs are integrated into routine clinical practice, where the precise biological characterization and staging of individual patients are essential for determining treatment eligibility.
4.5. Limitations
Several limitations should be acknowledged. First, the overall sample size was relatively modest, reflecting the strict temporal inclusion criteria applied to minimize disease progression–related confounding between plasma sampling and SPECT acquisition. Second, the amyloid PET validation cohort was small and highly imbalanced, consisting of 18 amyloid-positive and only 3 amyloid-negative participants. Consequently, estimates of specificity and negative predictive value should be interpreted cautiously. Third, the retrospective single-center design may limit generalizability to other populations. Fourth, the study population consisted primarily of elderly patients with substantial vascular burden and white matter disease. Although this characteristic reflects real-world clinical practice, the findings may differ in younger populations or in patients with more biologically pure AD pathology. Finally, the present study focused on cerebral perfusion SPECT and plasma p-tau217. Future prospective investigations incorporating additional multimodal biomarkers and functional clinical metrics, such as immersive spatial navigation assessments, are warranted to provide a more comprehensive understanding of biomarker interactions and clinical trajectories across the AD continuum.
5. Conclusions
In this cohort of elderly patients with MCI, plasma p-tau217 demonstrated closer concordance with cerebral amyloid pathology than eZIS-derived perfusion measures. However, the modest agreement observed between these biomarkers suggests that they capture different biological aspects of disease progression.
Rather than representing competing diagnostic tools, plasma p-tau217 and eZIS appear to provide complementary information regarding amyloid pathology, neurodegeneration, and cerebrovascular burden. Plasma p-tau217 can guide initial treatment eligibility, while eZIS provides essential longitudinal insights into mixed etiologies and functional disease trajectories. Such integration may therefore facilitate a more comprehensive evaluation of heterogeneous MCI populations and improve biological characterization across the Alzheimer's disease continuum.
Author Contributions
Conceptualization, M.-C.P.; methodology, M.-C.P. and I.-L.H.; software, H.M.; validation, M.-C.P. and I.-L.H.; formal analysis, I.-L.H.; investigation, M.-C.P. and I.-L.H.; resources, M.-C.P.; data curation, M.-C.P. and I.-L.H.; writing—original draft preparation, I.-L.H.; writing—review and editing, M.-C.P., H.M. and Y.-T.P. ; visualization, M.-C.P. and I.-L.H.; supervision, M.-C.P.; project administration, M.-C.P.; funding acquisition, M.-C.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Taiwan AI Center of Excellence (National Hub), grant numbers 111-2634-F-038-001-, 112-2634-F-038-001-, 113-2634-F-038-001-.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of National Cheng Kung University Hospital (NCKUH IRB B-ER-113-494, 11 April 2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We are especially grateful to Professor Nan-Tsing Chiu from the Division of Nuclear Medicine, Department of Medical Imaging, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan, for his expert advice on brain imaging and assistance in analyzing the TRODAT imaging data. We gratefully acknowledge the Summer Research Project Grant no. NCKUMCS2025-047 and NCKUMCS2026-041 from College of Medicine at National Cheng Kung University. Support was received from Taiwan AI Center of Excellence (National Hub), grant numbers 111-2634-F-038-001-, 112-2634-F-038-001-, 113-2634-F-038-001-.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AD | Alzheimer’s disease |
| eZIS | Easy Z-Score Imaging System |
| MCI | Mild cognitive impairment |
| p-tau217 | Phosphorylated tau217 |
| PET | Positron emission tomography |
| rCBF | Regional cerebral blood flow |
| SPECT | Single-photon emission computed tomography |
| VOI | Volume of interest |
| DMTs | Disease-modifying therapies |
Appendix A

Table A1.
Distribution of 62 participants according to eZIS severity and plasma p-tau217 results.
| Plasma p-tau217 0.63 pg/mL | Plasma p-tau217 0.63 pg/mL | |
|---|---|---|
| Severity1.19 | 29 | 15 |
| Severity1.19 | 9 | 9 |
Table A2.
Distribution of 62 participants according to eZIS extent and plasma p-tau217 results.
| Plasma p-tau2170.63 pg/mL | Plasma p-tau2170.63 pg/mL | |
|---|---|---|
| Extent14.2 | 24 | 13 |
| Extent14.2 | 14 | 11 |
Table A3.
Distribution of 62 participants according to eZIS ratio and plasma p-tau217 results.
| Plasma p-tau217 0.63 pg/mL | Plasma p-tau21 0.63 pg/mL | |
|---|---|---|
| Ratio2.22 | 21 | 14 |
| Ratio2.22 | 17 | 10 |
Appendix B
Table A4.
Statistical values of TRODAT-1 SPECT imaging parameters in the 12 patients.
| Right striatal TRODAT-1 binding ratio | Left striatal TRODAT-1 binding ratio | Striatal asymmetry index |
|---|---|---|
| 0.4212 [0.3470,0.4558] 0.1561 | 0.4774 [0.3618,0.5613] 0.1843 | 15.20 [4.750,22.43] 11.32 |
Note. Data are presented as (mean, [IQR], SD.).
References
- Berry, D.A.; Dhadda, S.; Kanekiyo, M.; Li, D.; Swanson, C.J.; Irizarry, M.; Kramer, L.D.; Berry, S.M. Lecanemab for Patients With Early Alzheimer Disease: Bayesian Analysis of a Phase 2b Dose-Finding Randomized Clinical Trial. JAMA Netw Open 2023, 6, e237230. [CrossRef]
- Sims, J.R.; Zimmer, J.A.; Evans, C.D.; Lu, M.; Ardayfio, P.; Sparks, J.; Wessels, A.M.; Shcherbinin, S.; Wang, H.; Monkul Nery, E.S.; et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. Jama 2023, 330, 512–527. [CrossRef]
- Jack, C.R., Jr.; Andrews, J.S.; Beach, T.G.; Buracchio, T.; Dunn, B.; Graf, A.; Hansson, O.; Ho, C.; Jagust, W.; McDade, E.; et al. Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup. Alzheimers Dement 2024, 20, 5143–5169. [CrossRef]
- Matsuda, H.; Mizumura, S.; Nagao, T.; Ota, T.; Iizuka, T.; Nemoto, K.; Kimura, M.; Tateno, A.; Ishiwata, A.; Kuji, I.; et al. An easy Z-score imaging system for discrimination between very early Alzheimer's disease and controls using brain perfusion SPECT in a multicentre study. Nucl Med Commun 2007, 28, 199–205. [CrossRef]
- Matsuda, H.; Mizumura, S.; Nagao, T.; Ota, T.; Iizuka, T.; Nemoto, K.; Takemura, N.; Arai, H.; Homma, A. Automated discrimination between very early Alzheimer disease and controls using an easy Z-score imaging system for multicenter brain perfusion single-photon emission tomography. AJNR Am J Neuroradiol 2007, 28, 731–736. [CrossRef]
- Matsuda, H.; Ohnishi, T.; Asada, T.; Li, Z.J.; Kanetaka, H.; Imabayashi, E.; Tanaka, F.; Nakano, S. Correction for partial-volume effects on brain perfusion SPECT in healthy men. J Nucl Med 2003, 44, 1243–1252.
- Takemaru, M.; Kimura, N.; Abe, Y.; Goto, M.; Matsubara, E. The evaluation of brain perfusion SPECT using an easy Z-score imaging system in the mild cognitive impairment subjects with brain amyloid-β deposition. Clin Neurol Neurosurg 2017, 160, 111–115. [CrossRef]
- Hirose, T.; Takayama, T.; Shibata, N.; Murakami, K.; Arai, H. A Pilot Study on Cerebral Blood Flow and Mini-Mental State Examination to Predict Amyloid Deposition in Preclinical Alzheimer's Disease. Psychiatry Clin Psychopharmacol 2023, 33, 1–7. [CrossRef]
- Hayashi, H.; Kobayashi, R.; Kawakatsu, S.; Morioka, D.; Otani, K. Utility of Easy Z-Score Imaging System-Assisted SPECT in Detecting Onset Age-Dependent Decreases in Cerebral Blood Flow in the Posterior Cingulate Cortex, Precuneus, and Parietal Lobe in Alzheimer's Disease with Amyloid Accumulation. Dement Geriatr Cogn Dis Extra 2020, 10, 63–68. [CrossRef]
- Kaneta, T.; Nakatsuka, M.; Nakamura, K.; Seki, T.; Yamaguchi, S.; Tsuboi, M.; Meguro, K. Improved Diagnostic Accuracy of SPECT Through Statistical Analysis and the Detection of Hot Spots at the Primary Sensorimotor Area for the Diagnosis of Alzheimer Disease in a Community-Based Study: "The Osaki-Tajiri Project". Clin Nucl Med 2016, 41, e1–6. [CrossRef]
- Pai, Y.T.; Matsuda, H.; Pai, M.C. Using eZIS to Predict Progression from MCI to Dementia in Three Years. Diagnostics (Basel) 2024, 14. [CrossRef]
- Yamamoto, S.; Yoshida, N.; Sakurai, N.; Okada, Y.; Satoh, M.; Takeshita, K.; Nakai, M.; Abe, K.; Yoshimura, M.; Saito, K. Clinical Utility of eZIS in Cerebral Blood Flow SPECT. Diagnostics (Basel) 2025, 15. [CrossRef]
- Matsuda, H. The role of neuroimaging in mild cognitive impairment. Neuropathology 2007, 27, 570–577. [CrossRef]
- Hayashi, H.; Kobayashi, R.; Kawakatsu, S.; Ohba, M.; Morioka, D.; Otani, K. Comparison of the decreases in regional cerebral blood flow in the posterior cingulate cortex, precuneus, and parietal lobe between suspected non-Alzheimer's disease pathophysiology and Alzheimer's disease. Psychogeriatrics 2021, 21, 716–721. [CrossRef]
- Waragai, M.; Mizumura, S.; Yamada, T.; Matsuda, H. Differentiation of early-stage Alzheimer's disease from other types of dementia using brain perfusion single photon emission computed tomography with easy Z-score imaging system analysis. Dement Geriatr Cogn Disord 2008, 26, 547–555. [CrossRef]
- Grande, G.; Valletta, M.; Rizzuto, D.; Xia, X.; Qiu, C.; Orsini, N.; Dale, M.; Andersson, S.; Fredolini, C.; Winblad, B.; et al. Blood-based biomarkers of Alzheimer’s disease and incident dementia in the community. Nature Medicine 2025, 31, 2027–2035. [CrossRef]
- Hu, S.; Yu, H.; Gao, J. The pTau217/Aβ(1-42) plasma ratio: The first FDA-cleared blood biomarker test for diagnosis of Alzheimer's disease. Drug Discov Ther 2025, 19, 208–209. [CrossRef]
- Thijssen, E.H.; La Joie, R.; Strom, A.; Fonseca, C.; Iaccarino, L.; Wolf, A.; Spina, S.; Allen, I.E.; Cobigo, Y.; Heuer, H.; et al. Plasma phosphorylated tau 217 and phosphorylated tau 181 as biomarkers in Alzheimer's disease and frontotemporal lobar degeneration: A retrospective diagnostic performance study. Lancet Neurol 2021, 20, 739–752. [CrossRef]
- Palmqvist, S.; Janelidze, S.; Quiroz, Y.T.; Zetterberg, H.; Lopera, F.; Stomrud, E.; Su, Y.; Chen, Y.; Serrano, G.E.; Leuzy, A.; et al. Discriminative Accuracy of Plasma Phospho-tau217 for Alzheimer Disease vs Other Neurodegenerative Disorders. Jama 2020, 324, 772–781. [CrossRef]
- Ashton, N.J.; Brum, W.S.; Di Molfetta, G.; Benedet, A.L.; Arslan, B.; Jonaitis, E.; Langhough, R.E.; Cody, K.; Wilson, R.; Carlsson, C.M.; et al. Diagnostic Accuracy of a Plasma Phosphorylated Tau 217 Immunoassay for Alzheimer Disease Pathology. JAMA Neurol 2024, 81, 255–263. [CrossRef]
- Lin, Y.S.; Kwon, H.S.; Lee, W.J.; Hwang, M.; Jeong, J.H.; Koh, S.H.; Choi, S.H.; Fuh, J.L. Cross-cultural validation of plasma p-tau217 and p-tau181 as precision biomarkers for amyloid PET positivity: An East Asian study in Taiwan and Korea. Alzheimers Dement 2025, 21, e14565. [CrossRef]
- Jonaitis, E.M.; Janelidze, S.; Cody, K.A.; Langhough, R.; Du, L.; Chin, N.A.; Mattsson-Carlgren, N.; Hogan, K.J.; Christian, B.T.; Betthauser, T.J.; et al. Plasma phosphorylated tau 217 in preclinical Alzheimer's disease. Brain Commun 2023, 5, fcad057. [CrossRef]
- Mattsson-Carlgren, N.; Janelidze, S.; Palmqvist, S.; Cullen, N.; Svenningsson, A.L.; Strandberg, O.; Mengel, D.; Walsh, D.M.; Stomrud, E.; Dage, J.L.; et al. Longitudinal plasma p-tau217 is increased in early stages of Alzheimer's disease. Brain 2020, 143, 3234–3241. [CrossRef]
- Insel, P.S.; Mattsson-Carlgren, N.; Langford, O.; Caruso, V.M.; Leuzy, A.; Young, C.B.; Boxer, A.; Aisen, P.S.; Sperling, R.A.; Mormino, E.C.; et al. Concurrent Changes in Plasma Phosphorylated Tau 217, Tau PET, and Cognition in Preclinical Alzheimer Disease. JAMA Neurol 2025, 82, 985–993. [CrossRef]
- Bouteloup, V.; Villain, N.; Vidal, J.S.; Gonzalez-Ortiz, F.; Yuksekel, I.; Santos, C.; Schraen-Maschken, S.; Pellegrin, I.; Lehmann, S.; Blennow, K.; et al. Cognitive Phenotyping and Interpretation of Alzheimer Blood Biomarkers. JAMA Neurol 2025, 82, 506–515. [CrossRef]
- Binks, S.N.M.; Graff-Radford, J. Evolving Role of Plasma Phosphorylated Tau 217 in Alzheimer Disease-Time for Tau. JAMA Neurol 2025, 82, 981–982. [CrossRef]
- Zhong, X.; Wang, Q.; Yang, M.; Lin, G.; Yao, K.; Wu, Z.; Xu, D.; Zhou, H.; Chen, B.; Shi, H.; et al. Plasma p-tau217 and p-tau217/Aβ1-42 are effective biomarkers for identifying CSF- and PET imaging-diagnosed Alzheimer's disease: Insights for research and clinical practice. Alzheimers Dement 2025, 21, e14536. [CrossRef]
- Kasuga, K.; Kikuchi, M.; Kikkawa-Saito, E.; Tsukie, T.; Ishiguro, T.; Miyashita, A.; Iwatsubo, T.; Ikeuchi, T. Evaluation of plasma p-tau217 biomarkers in detecting amyloid pathology and predicting cognitive outcomes: Observations from Japanese Alzheimer's disease neuroimaging initiative cohort. J Prev Alzheimers Dis 2026, 13, 100502. [CrossRef]
- Rudolph, M.D.; Sutphen, C.L.; Register, T.C.; Lockhart, S.N.; Rundle, M.M.; Hughes, T.M.; Bateman, J.R.; Solingapuram Sai, K.K.; Whitlow, C.T.; Craft, S.; et al. Evaluation of plasma p-tau217 for detecting amyloid pathology in a diverse and heterogeneous community-based cohort. medRxiv 2025. [CrossRef]
- Malek-Ahmadi, M.; Sharma, S.; Stipho, F.; Denkinger, M.; Singh, A.; Brum, W.S.; Ashton, N.J. Plasma Phosphorylated Tau 217 and Amyloid Burden in Older Adults Without Cognitive Impairment: A Meta-Analysis. JAMA Neurology 2026, 83, 13–19. [CrossRef]
- Khalafi, M.; Dartora, W.J.; McIntire, L.B.J.; Butler, T.A.; Wartchow, K.M.; Hojjati, S.H.; Razlighi, Q.R.; Shirbandi, K.; Zhou, L.; Chen, K.; et al. Diagnostic accuracy of phosphorylated tau217 in detecting Alzheimer's disease pathology among cognitively impaired and unimpaired: A systematic review and meta-analysis. Alzheimers Dement 2025, 21, e14458. [CrossRef]
- Schöll, M.; Verberk, I.M.W.; Del Campo, M.; Delaby, C.; Therriault, J.; Chong, J.R.; Palmqvist, S.; Alcolea, D. Challenges in the practical implementation of blood biomarkers for Alzheimer's disease. Lancet Healthy Longev 2024, 5, 100630. [CrossRef]
- van der Thiel, M.; Rodriguez, C.; Van De Ville, D.; Giannakopoulos, P.; Haller, S. Regional Cerebral Perfusion and Cerebrovascular Reactivity in Elderly Controls With Subtle Cognitive Deficits. Front Aging Neurosci 2019, 11, 19. [CrossRef]
- Dai, W.; Lopez, O.L.; Carmichael, O.T.; Becker, J.T.; Kuller, L.H.; Gach, H.M. Mild cognitive impairment and alzheimer disease: Patterns of altered cerebral blood flow at MR imaging. Radiology 2009, 250, 856–866. [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR). Neurology 1993, 43, 2412–2412–a. [CrossRef]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch Neurol 2001, 58, 1985–1992. [CrossRef]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The Cognitive Abilities Screening Instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int Psychogeriatr 1994, 6, 45–58; discussion 62. [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975, 12, 189–198. [CrossRef]
- Lai, R.; Li, B.; Bishnoi, R. P-tau217 as a Reliable Blood-Based Marker of Alzheimer's Disease. Biomedicines 2024, 12. [CrossRef]
- Orduña Dolado, A.; Stomrud, E.; Ashton, N.J.; Nilsson, J.; Quijano-Rubio, C.; Jethwa, A.; Brum, W.S.; Brinkmalm Westman, A.; Zetterberg, H.; Blennow, K.; et al. Effects of time of the day at sampling on CSF and plasma levels of Alzheimer' disease biomarkers. Alzheimers Res Ther 2024, 16, 132. [CrossRef]
- Jiang, Y.; Zheng, W.; Xia, Z.; Wong, W.W.; Cheng, L.K.W.; Ip, F.C.; Choi, S.M.; Chan, A.L.T.; Lam, C.Y.; Ho, K.S.; et al. Head-to-head comparison of brain-derived pTau217 and total pTau217 for brain amyloid and tau pathology classification. Proc Natl Acad Sci U S A 2026, 123, e2536792123. [CrossRef]
- Chatterjee, P.; Ivanic, S.; Southon, A.; McCarthy, C.; Patel, S.K.; Christensen, M.; Darby, D.; Bush, A.I.; Ayton, S.; Werden, E.; et al. Real world diagnostic performance of plasma p-tau217 for early-onset Alzheimer's disease in a cognitive disorders tertiary care setting. J Alzheimers Dis 2025, 108, 387–396. [CrossRef]
- Nguyen Ho, P.T.; Hoepel, S.J.W.; Rodriguez-Ayllon, M.; Luik, A.I.; Vernooij, M.W.; Neitzel, J. Sleep, 24-Hour Activity Rhythms, and Subsequent Amyloid-β Pathology. JAMA Neurol 2024, 81, 824–834. [CrossRef]
- Quintas-Neves, M.; Almeida, F.C.; Gauthreaux, K.; Teylan, M.A.; Mock, C.N.; Kukull, W.A.; Crary, J.F.; Oliveira, T.G. Fazekas scale magnetic resonance imaging assessment in Alzheimer’s disease and primary age-related tauopathy. Neuroradiology 2024, 66, 2185–2193. [CrossRef]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. AJR Am J Roentgenol 1987, 149, 351–356. [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O'Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol 2013, 12, 822–838. [CrossRef]
- Šimundić, A.M. Measures of Diagnostic Accuracy: Basic Definitions. Ejifcc 2009, 19, 203–211.
- Zhang, D.; Zhang, J.; Zhang, B.; Zhang, J.; He, M. Association of Blood Pressure, White Matter Lesions, and Regional Cerebral Blood Flow. Med Sci Monit 2021, 27, e929958. [CrossRef]
- Ong, J.J.H.; Leow, Y.J.; Qiu, B.; Tanato, P.; Zailan, F.Z.; Sandhu, G.K.; Kandiah, N. Association of Enlarged Perivascular Spaces With Early Serum and Neuroimaging Biomarkers of Alzheimer Disease Pathology. Neurology 2025, 105, e213836. [CrossRef]
- Rajah, M.N.; Dixon, R.A.; Einstein, G.; Stern, Y.; Badhwar, A.; Buckley, R.; Campbell, K.; Christophe, K.; Deska, J.; Duarte, A.; et al. A roadmap for conducting more inclusive research on brain resilience in ageing and dementia. Nature Reviews Neuroscience 2026. [CrossRef]
- Pappalettera, C.; Carrarini, C.; Miraglia, F.; Vecchio, F.; Rossini, P.M. Cognitive resilience/reserve: Myth or reality? A review of definitions and measurement methods. Alzheimers Dement 2024, 20, 3567–3586. [CrossRef]
- Lavretsky, H.; Khalsa, S.; Oughli, H.A.; Ibanez, A.; Cruzat, J.; Edwards, E.; Newhouse, P.; Bassetti, C.L.A.; Begue, I.; Winkler, A.S.; et al. The role of brain health and resilience in reshaping trajectories of late-life neuropsychiatric disorders. Neuropsychopharmacology 2026. [CrossRef]
- Benina, N.; Buitrago, L.; De Simone, F.I.; Radwan, R.R.; Miller, M.C.; Martin, K.; Dickson, D.; Ho, S.; Moghekar, A.; Albert, M.; et al. Plasma pTau 217/β-amyloid 1-42 ratio for enhanced accuracy and reduced uncertainty in detecting amyloid pathology. Brain 2026, 149, 1168–1181. [CrossRef]
- Petersen, K.K.; Milà-Alomà, M.; Li, Y.; Du, L.; Xiong, C.; Tosun, D.; Saef, B.; Saad, Z.S.; Du-Cuny, L.; Coomaraswamy, J.; et al. Predicting onset of symptomatic Alzheimer's disease with plasma p-tau217 clocks. Nat Med 2026. [CrossRef]
Figure 1.
Schematic representation of the study design and research focus.(Created in https://BioRender.com).
Figure 1.
Schematic representation of the study design and research focus.(Created in https://BioRender.com).

Figure 2.
The participant selection and flowchart of this study.

Figure 3.
The ROC curve of severity.

Figure 4.
The ROC curve of extent.

Figure 5.
The ROC curve of ratio.

Table 1.
Demographic and clinical characteristics.
| Low plasma p-tau217 (n=24) | High plasma p-tau217 (n=38) | p-value | |
|---|---|---|---|
| Demographic data | |||
| Age when p-tau217 performed (mean, [IQR], SD) |
75.29 [70.25,82.75] 7.147 | 75.55 [72.00,80.25] 6.616 | 0.7491 |
| Education, years (mean, [IQR], SD) | 8.583 [6,12] 4.323 | 9.684 [6,14] 5.353 | 0.4300 |
| Gender (male) (n, percentage) | 9 (37.5%) | 10 (26.32%) | 0.4030 |
| Comorbidities | |||
| Hypertension | 10 (41.7%) | 18 (47.4%) | 0.7945 |
| Dyslipidemia | 7 (29.2%) | 7(18.4%) | 0.3626 |
| Diabetes mellitus | 11 (45.8%) | 8 (21.1%) | 0.0509 |
| Hearing impairment | 6 (25.0%) | 8 (21.1%) | 0.7617 |
| Coronary artery disease | 5 (20.8%) | 6(15.8%) | 0.7362 |
| Insomnia | 9 (37.5%) | 9 (23.7%) | 0.2652 |
| Microbleed | 2 (8.33%) | 3 (7.89%) | 1.000 |
| Cognitive assessments | |||
| CDR-SB (mean, [IQR], SD) | 1.583 [0.625,2.375] 0.9286 | 1.961 [1.500,2.500] 0.8958 | 0.1348 |
| MMSE (mean, [IQR], SD) | 22.67 [20.00,25.75] 3.306 | 21.37 [18.75,23.25] 3.071 | 0.1549 |
| CASI | |||
| Total score (mean, [IQR], SD) | 75.04 [68.25,84.50] 9.989 | 70.00 [66.00,76.25] 9.623 | 0.0757 |
| Remote memory (mean, [IQR], SD) | 9.708 [10.00,10,00] 0.9079 | 9.737 [10.00,10,00] 0.6851 | 0.9186 |
| Recent memory**** (mean, [IQR], SD) | 6.708 [4.250,8.750] 2.596 | 3.737 [2.000,5.000] 2.127 | <0.0001 |
| Attention (mean, [IQR], SD) | 7.000 [6.000,8.000] 1.142 | 6.895 [6.000,8.000] 1.226 | 0.7970 |
| Mental manipulation (mean, [IQR], SD) | 7.083 [6.000,10.00] 2.636 | 7.921 [7.000,10.00] 2.148 | 0.1976 |
| Orientation* (mean, [IQR], SD) | 14.54 [13.00,17.75] 3.401 | 12.26 [9.000,17.00] 3.950 | 0.0113 |
| Abstract thinking (mean, [IQR], SD) | 6.667 [6.000,8.000] 1.308 | 7.053 [6.000,8.000] 1.064 | 0.3076 |
| Language (mean, [IQR], SD) | 9.417 [9.000,10.00] 0.6539 | 9.132 [9.000,10.00] 1.044 | 0.4534 |
| Drawing (mean, [IQR], SD) | 8.708 [8.000,10.00] 1.989 | 8.342 [8.000,10.00] 2.831 | 0.7552 |
| Verbal fluency (mean, [IQR], SD) | 5.042 [4.000,6.000] 1.459 | 4.921 [4.000,6.000] 1.634 | 0.7678 |
| The eZIS indicators | |||
| Severity (mean, [IQR], SD) | 1.367 [1.030,1.698] 0.3952 | 1.515 [1.183,1.838] 0.6338 | 0.4358 |
| Extent (mean, [IQR], SD) | 18.52 [8.825,26.15] 13.92 | 23.82 [8.963,36.88] 19.49 | 0.4317 |
| Ratio (mean, [IQR], SD) | 2.319 [1.120,3.288] 1.456 | 3.089 [1.510,4.425] 2.162 | 0.2633 |
| Severity1.19 (n, percentage) | 15 (62.5%) | 29 (76.3%) | 0.2652 |
| Extent14.2 (n, percentage) | 13 (54.2%) | 24 (63.2%) | 0.5989 |
| Ratio2.22 (n, percentage) | 14 (58.3%) | 21 (55.3%) | 1.000 |
| Zero abnormal indicator (n, percentage) | 9 (37.5%) | 9 (23.7%) | 0.2652 |
| One abnormal indicator (n, percentage) | 0 (0.00%) | 3 (7.90%) | 0.2766 |
| Two abnormal indicators (n, percentage) | 3 (12.5%) | 7 (18.4%) | 0.7272 |
| Three abnormal indicators (n, percentage) | 12 (50.0%) | 19 (50.0%) | 1.000 |
| More than two abnormal indicators (n, percentage) |
15 (62.5%) | 26 (68.4%) | 0.7837 |
| Fazekas scale (PWMH, DWMH) (n, percentage) | |||
| (0-1,0-1) | 12 (50.0%) | 17 (44.7%) | >0.9999 |
| (0-1,2-3) | 3 (12.5%) | 5 (13.1%) | |
| (2-3,0-1) | 1 (4.17%) | 2 (5.26%) | |
| (2-3,2-3) | 5 (20.8%) | 6 (15.8%) | |
| No MRI data | 3 (12.5%) | 8 (21.1%) | |
| Biomarker | |||
| Plasma p-tau217 value**** (mean, [IQR], SD) | 0.3631 [0.2270,0.4973] 0.1590 | 1.236 [0.8393,1.612] 0.5331 | <0.0001 |
Note. IQR: interquartile range; CASI: Cognitive Abilities Screening Instrument; MMSE: Mini-mental State Examination; CDR: Clinical Dementia Rating; SB: sum of boxes; eZIS: easy Z-score imaging system; Plasma p-tau217: plasma phosphorylated tau217; PWMH: periventricular white matter hyperintensity DWMH: deep white matter hyperintensity ****p 0.0001 **p 0.01 *p 0.05.
Table 2.
Demographic and clinical characteristics of the 21 participants who underwent all three diagnostic evaluations (eZIS, plasma p-tau217, and amyloid PET).
Table 2.
Demographic and clinical characteristics of the 21 participants who underwent all three diagnostic evaluations (eZIS, plasma p-tau217, and amyloid PET).
| Non-AD MCI (n=3) | AD MCI (n=18) | p-value | |
|---|---|---|---|
| Demographic data | |||
| Age when p-tau217 performed (mean, [IQR], SD) | 76.33 [70.00,81.00] 5.686 | 72.39 [69.00,75,50] 4.925 | 0.2856 |
| Education, years* (mean, [IQR], SD) | 17.33 [14.00,22.00] 4.163 | 10.89 [6.00,14.50] 4.364 | 0.0489 |
| Gender (male) (n, percentage) | 2 (66.7%) | 5 (27.8%) | 0.2474 |
| Comorbidities | |||
| Hypertension | 2 (66.7%) | 10 (55.6%) | 1.0000 |
| Dyslipidemia* | 2 (66.7%) | 1 (5.56%) | 0.0414 |
| Diabetes mellitus* | 2 (66.7%) | 0 (0.00%) | 0.0143 |
| Hearing impairment | 0 (0.00%) | 3 (16.7%) | 1.0000 |
| Coronary artery disease | 0 (0.00%) | 3 (16.7%) | 1.0000 |
| Insomnia | 0 (0.00%) | 6 (33.3%) | 0.5263 |
| Microbleed | 0 (0.00%) | 1 (5.56%) | 1.0000 |
| Cognitive assessments | |||
| CDR-SB (mean, [IQR], SD) | 2.000 [0.500,4.000] 1.803 | 1.972 [1.375,2.625] 0.8484 | 0.7992 |
| MMSE* (mean, [IQR], SD) | 26.00 [24.00,29.00] 2.646 | 22.78 [21.75,24.25] 1.833 | 0.0451 |
| CASI | |||
| Total score* (mean, [IQR], SD) | 83.33 [76.00,91.00] 7.506 | 74.22 [71.25,76.50] 4.930 | 0.0383 |
| Remote memory (mean, [IQR], SD) | 10.00 [10.00, 10.00] 10.00 | 9.944 [10.00, 10.00] 0.2357 | >0.9999 |
| Recent memory* (mean, [IQR], SD) | 8.677 [7.000,11.00] 2.082 | 4.222 [3.000,5.250] 2.157 | 0.0180 |
| Attention (mean, [IQR], SD) | 8.000 [8.000,8.000] 0.000 | 7.278 [6.750,8.000] 1.074 | 0.4263 |
| Mental manipulation (mean, [IQR], SD) | 8.667 [6.000,10.00] 2.309 | 8.722 [8.000.10.00] 1.565 | 0.9173 |
| Orientation (mean, [IQR], SD) | 16.00 [13.00,18.00] 2.646 | 12.00 [9.750,13.00] 3.308 | 0.0714 |
| Abstract thinking (mean, [IQR], SD) | 7.333 [7.000,8.000] 0.5774 | 7.111 [6.750,8.000] 1.023 | 0.7060 |
| Language (mean, [IQR], SD) | 9.333 [9.000,10.00] 0.5774 | 9.611 [9.000,10.00] 0.7775 | 0.5211 |
| Drawing (mean, [IQR], SD) | 9.333 [9.000,10.00] 0.5774 | 9.667 [10.00,10.00] 1.188 | 0.0797 |
| Verbal fluency (mean, [IQR], SD) | 6.000 [5.000,7.000] 1.000 | 5.889 [4.750,7.000] 1.530 | >0.9999 |
| The eZIS indicators | |||
| Severity (mean, [IQR], SD) | 1.510 [1.200,1.950] 0.3915 | 1.364 [1.123,1.488] 0.4095 | 0.7248 |
| Extent (mean, [IQR], SD) | 16.95 [9.090,22.59] 7.020 | 19.51 [8.160,22.22] 15.34 | 0.8977 |
| Ratio (mean, [IQR], SD) | 2.413 [1.280,4.420] 1.743 | 2.931 [1.613,4.018] 2.037 | 0.5338 |
| Severity1.19 (n, percentage) | 3(100%) | 13(72.2%) | 0.5489 |
| Extent14.2 (n, percentage) | 2(66.7%) | 12(66.7%) | 1.000 |
| Ratio2.22 (n, percentage) | 1(33.3%) | 10(55.6%) | 0.5865 |
| Zero abnormal indicator (n, percentage) | 0(0.00%) | 5(27.8%) | 0.5489 |
| One abnormal indicator (n, percentage) | 1(33.3%) | 0(0.00%) | 0.1429 |
| Two abnormal indicators (n, percentage) | 1(33.3%) | 4(22.2%) | 1.0000 |
| Three abnormal indicators (n, percentage) | 1(33.3%) | 9(50.0%) | 1.0000 |
| More than two abnormal indicators (n, percentage) |
2(66.7%) | 13(72.2%) | 1.0000 |
| Fazekas scale (PWMH, DWMH) (n, percentage) | |||
| (0-1,0-1) | 0 (0.00%) | 11 (61.1%) | 0.0833 |
| (0-1,2-3) | 0 (0.00%) | 0 (0.00%) | |
| (2-3,0-1) | 1 (33.3%) | 1 (5.56%) | |
| (2-3,2-3) | 2 (66.7%) | 5 (27.8%) | |
| No MRI data | 0 (0.00%) | 1 (5.56%) | |
| Biomarker | |||
| Plasma p-tau217 value (mean, [IQR], SD) | 0.9327 [0.6450,1.280] 0.3217 | 1.272 [0.8375,1.822] 0.6146 | 0.4707 |
| Centiloid scale | |||
| Centiloid scale value** (mean, [IQR], SD) | 0.8333 [-7.900,7.600] 7.935 | 88.12 [54.35,104.6] 42.30 | 0.0015 |
Note. AD-MCI: mild cognitive impairment due to Alzheimer’s disease; non-AD MCI: mild cognitive impairment due to non-Alzheimer’s disease; IQR: interquartile range; CASI: Cognitive Abilities Screening Instrument; MMSE: Mini-mental State Examination; CDR: Clinical Dementia Rating; SB: sum of boxes; eZIS: easy Z-score imaging system; Plasma p-tau217: plasma phosphorylated tau217; PWMH: periventricular white matter hyperintensity DWMH: deep white matter hyperintensity ****p 0.0001 **p 0.01 *p 0.05.
Table 3.
Diagnostic performance of the three eZIS indicators.
| Severity | Extent | Ratio | |
|---|---|---|---|
| Sensitivity | 76.3% | 63.2% | 55.3% |
| Specificity | 37.5% | 41.7% | 45.8% |
| PPV | 66.0% | 64.9% | 60.0% |
| NPV | 50.0% | 44.0% | 37.0% |
| Diagnostic accuracy | 61.3% | 56.5% | 50.0% |
Table 4.
Diagnostic performance of plasma p-tau217 and three eZIS indicators.
| Plasma p-tau217 | Severity | Extent | Ratio | |
|---|---|---|---|---|
| Sensitivity | 94.4% | 72.2% | 66.7% | 55.6% |
| Specificity | - | - | 33.3% | 66.7% |
| PPV | 85.0% | 81.25% | 85.7% | 90.9% |
| NPV | - | - | 14.3% | 20.0% |
| Diagnostic accuracy | 81.0% | 61.9% | 61.9% | 57.1% |
Note. space means that no patient meets the condition in our study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



