Submitted:
20 May 2026
Posted:
21 May 2026
You are already at the latest version
Abstract
Background/Objectives: Oral candidiasis is an infection of the oral cavity caused by Candida albicans. Mucoadhesive buccal films could adhere to the buccal mucosa for prolonged periods, improving the therapeutic outcomes of patients with oral candidiasis. This study aimed to develop and evaluate the properties of fluconazole containing sodium alginate/methylcellulose-based buccal films for potential treatment of oral candidiasis. Methods: Drug-polymer compatibility was investigated using FT-IR spectrophotometry. Three optimised fluconazole films (F1 to F3) containing 1-1.6% sodium alginate and methylcellulose (1.6%) were formulated using the solvent casting method. Their physicomechanical properties were characterised using standard protocols. Drug content and in vitro drug release profiles were evaluated using UV-visible spectroscopy; in vitro / ex vivo mucoadhesion studies were conducted using the shaking water bath technique, and their antifungal activity against Candida albicans was evaluated using the agar ditch method. Results: FT-IR data analysis revealed that sodium alginate, methyl cellulose and fluconazole were compatible in the films. The films were off-white, smooth, peelable, thin, with satisfactory pH values, folding endurance, drug content, excellent zones of inhibition against Candida albicans (40 mm), controlled drug release profile (3.6-4.1 mg/cm2 after 6 h), and they displayed Korsmeyer-Peppas drug release kinetics. Film F3 containing 1.6% sodium alginate and 1.6% of methylcellulose exhibited superior swelling index (70±1%), tensile strength (0.68±0.04 MPa) and in vitro/ex vivo mucoadhesion time (5.5±0.3 h; 2.3±0.3 h) relative to other studied films. Conclusions: The sodium alginate content of the films influenced their tensile and muco-adhesive properties. Film F3 was the most promising formulations, for potential treatment of oral candidiasis.
Keywords:
sodium alginate
; methylcellulose
; fluconazole
; buccal films
; oral candidiasis
; physicomechanical
; mucoadhesion
; antifungal
; drug content
; drug release
1. Introduction
Candidiasis, also known as oral thrush, is a fungal infection primarily caused by Candida albicans, the most common species found in the human oral cavity [1]. Patients with oral candidiasis present with loss of taste or an unpleasant taste in the mouth; inflamed mouth and throat; cracks at the corners of the mouth, and painful, burning sensation in the mouth [2].
Predisposing factors to developing oral candidiasis include poor oral hygiene, excessive use of mouthwash, smoking, diabetes mellitus, cancer, and immunocompromised conditions such as HIV infection [1,3]. Approximately 95% of HIV-positive individuals experience oral candidiasis during their illness, and it is often a prognostic indicator of AIDS [4]. Globally, it is estimated that 9.5 million HIV-positive individuals suffer from oral candidiasis [5]. Given the high incidence and associated morbidity of oral candidiasis, effective treatment of the disease is crucial, particularly in populations with weakened immune systems.
Fluconazole (2,4-difluoro-α,α 1 -bis (1H-1,2,4-triazol-1-ylmethyl) benzyl alcohol), a synthetic triazole antifungal agent, is one of the approved drugs for treating moderate to severe cases of oral candidiasis [6]. Fluconazole exerts its antifungal effects by inhibiting the enzyme, lanosterol 14-α-demethylase, resulting in improved permeability of the fungal cell membrane to fluconazole, and resulting in fungal cell death [7].
The clinical effectiveness of conventional fluconazole formulations such as tablets, suspensions, and infusions is limited by the extensive systemic distribution of fluconazole, resulting in an increased risk of systemic toxicity. In addition, oral formulations are degraded by stomach acid and liver enzymes, leading to subtherapeutic concentrations of fluconazole within the oral tissues [8]. Though, moderate to severe cases of oral candidiasis have been effectively treated by administering 100-200 mg of fluconazole orally once daily for 7 to 14 days, long duration of treatment may result in poor patient compliance [6]. Moreover, systemic therapies are associated with poor patient acceptance due to its invasiveness. Therefore, there is strong need to develop buccal drug delivery systems that can facilitate localized drug delivery, minimize systemic exposure, reduce the potential for adverse effects, and promote effective treatment of oral candidiasis.
Buccal films comprise of film-forming agents, mucoadhesive polymers, plasticisers, and polymers that can facilitate controlled drug release [9]. Glycerol and propylene glycol are the most widely used plasticising agent that improve the flexibility of film formulations [9]. Examples of mucoadhesive polymers that have been used to formulate buccal films include chitosan, sodium alginate and hydroxypropylmethylcellulose [10,11,12]. Mucoadhesive films adhere to the oral mucosa, facilitating controlled release of the loaded drug for prolonged periods, enhancing treatment efficacy and patient compliance due to reduced frequency of dosing.
Over the last two decades, mucoadhesive buccal films have been well-researched due to flexibility, convenience of application, their capability to avoid gastric acidic and hepatic enzymatic drug degradation as well as their ability to deliver therapeutic agents for local or systemic therapeutic effects [13]. In addition, buccal film can be customised to accommodate required amount of the therapeutic agents, enabling personalised medicines [9].
Different buccal products were investigated for local and systemic drug delivery. For instance, fluticasone, felodipine and haloperidol containing buccal films were used systemically to control asthma, blood pressure, and schizophrenia, respectively [14,15,16] while cetylpyridinium chloride and doxycycline hyclate containing buccal films have been investigated for localised drug delivery to treat bacterial infections and periodontitis, respectively [10,17].
Various buccal products that exert systemic therapeutic effect such as buprenorphine (Belbuca) and fentanyl (Onsolis) have been commercialised [18,19]. However, there are no marketed drug containing buccal films to treat localized buccal diseases, including oral candidiasis [20]. This gap highlights the need for further research into buccal film formulations that can deliver antifungal agents such as fluconazole, in a controlled manner, for the effective treatment of oral candidiasis.
Fluconazole is an ideal candidate for buccal drug delivery because it can effectively permeate the oral mucosa due to its satisfactory physicochemical properties (molecular weight: 306.3 Da; log P: 0.4) [21]. The development of mucoadhesive fluconazole containing buccal film could facilitate a reduction in the therapeutic dose of fluconazole from 200 mg to 5 mg and minimize side effects associated with disease treatment via the oral and systemic route of administration due to its localised drug delivery capability.
Sodium alginate is a natural, hydrophilic, anionic polymer obtained from marine brown seaweed, with a linear structure primarily composed of (1,4)-linked b-D-mannuronic acid units and a-L-guluronic acid units [22]. It has intrinsic mucoadhesive property due to its carboxylic groups that interact with the hydroxyl groups of mucin glycoproteins [23]. Methylcellulose is a semi-synthetic, hydrophilic, non-ionic polymer that has mucus-penetrating potential, and it can facilitate controlled drug release [24]. In addition, both sodium alginate and methylcellulose have film-forming properties [25]. Moreover, these polymers are generally recognised as safe (GRAS) according to the Food and Drug Administration, USA [26]. Therefore, they have been selected in the current study to formulate mucoadhesive fluconazole containing buccal films, for potential treatment of oral candidiasis.
Patel and coworkers reported that optimised sodium alginate (SA)/polyvinylalcohol (PVA)-based fluconazole films containing 1% SA and 1% PVA exhibited satisfactory physicomechanical properties, ex vivo rat skin residence time of 8 h, and controlled drug release profile over 8 h [27]. However, the anti-fungal activity of the optimised fluconazole containing buccal film was not investigated. Therefore, the possibility of translating the film formulation from the research laboratory to the clinics and market cannot be ascertained.
Dinte et al., (2023) revealed that doxycycline hyclate containing hydroxypropyl methylcellulose (HPMC) E3/HPMC K4/Carbopol 940 (1: 0.05: 0.35) was the most promising film for potential treatment of periodontitis in terms of its physicomechanical, mucoadhesive, controlled drug release profile, non-irritancy to the buccal tissues and efficacy against experimentally induced periodontitis in rat models [12]. Nevertheless, their newly developed buccal films are not intended to treat oral candidiasis.
Posaconazole is typically used to treat oral candidiasis when the disease is resistant to itraconazole and fluconazole therapy. Recently, Szekalska et al., (2023) reported that optimised posaconazole containing calcium carbonate-crosslinked alginate/pectin-based buccal films prepared using 1% of sodium alginate and 1% pectin exhibited improved mechanical properties and facilitated controlled drug release compared to the non-crosslinked films. However, the calcium carbonate crosslinking process compromised the film formulation’s mucoadhesiveness and antifungal activity against Candida albicans [11]. Therefore, the novel posaconazole containing buccal film may result in therapeutic failure in the clinics due to the limited interaction between the posaconazole containing films and the diseased buccal mucosal tissues. Moreover, the film formulation was not suited for the first line treatment of oral candidiasis.
To our knowledge, buccal films have never been commercialised for the treatment of oral candidiasis. The combination of sodium alginate, methylcellulose and appropriate plasticiser could generate an aesthetically appealing, quality and efficacious buccally delivered dosage form. Also, the influence of increasing amounts of sodium alginate with a constant concentration of methylcellulose, on the properties of fluconazole films, will be investigated. This study aimed to formulate fluconazole containing sodium alginate/methylcellulose-based buccal films and evaluate their physicomechanical, mucoadhesive, drug release, stability, and antifungal properties, for potential treatment of oral candidiasis.
2. Materials and Methods
2.1. Materials
Sodium Alginate (Sigma, UK), methylcellulose, low substitution (FengChen, Ltd, China); propylene glycol (Dongying Runze New Materials Ltd, China), fluconazole (Macklin, China), phosphate buffer (pH 6.8), dialysis membrane (MWCO12–14 kDa) (Medicell Membranes Ltd, UK); and cellulose membrane (0.45 μm; Merck, UK), Sabouraud dextrose agar, and nutrient agar. Deionised water was used for all experiment. All other chemicals were of analytical grade and used without further purification.
2.2. Ethical Approval of Studies Involving Porcine Buccal Mucosal Tissues
Ethical approval was obtained to evaluate the ex vivo porcine buccal mucoadhesiveness of the novel fluconazole films (CMUL/ACUREC/08/24/1696), dated November 17, 2024. The porcine buccal mucosal tissues were excised from freshly slaughtered pigs intended for food and transported over ice-cold water to the laboratory and used within 24 h of procurement. The location of the abattoir is Lagos, Nigeria. The work complied with the regulations of the College of Medicine, University of Lagos Animal Care and Use Research Ethics Committee, Lagos, Nigeria.
2.3. Methods
2.3.1. Drug/Polymers Compatibility Studies– Attenuated Transmittance Reflectance-Fourier Transform Infrared (ATR-FTIR) Spectroscopy
Solid samples of fluconazole, sodium alginate and methyl cellulose alone and in combination with other ingredients used to formulate fluconazole film, were scanned using the ATR-FTIR spectrometer (Agilent CARY 630) from 4000 to 650 cm-1, at a resolution of 8 cm-1, and 32 scans was conducted for each tested sample to generate the FT-IR data. This procedure was also conducted on optimised film formulations to confirm that fluconazole remained compatible with the polymers after buccal film development.
2.3.2. Preparation of Fluconazole Containing Buccal Films
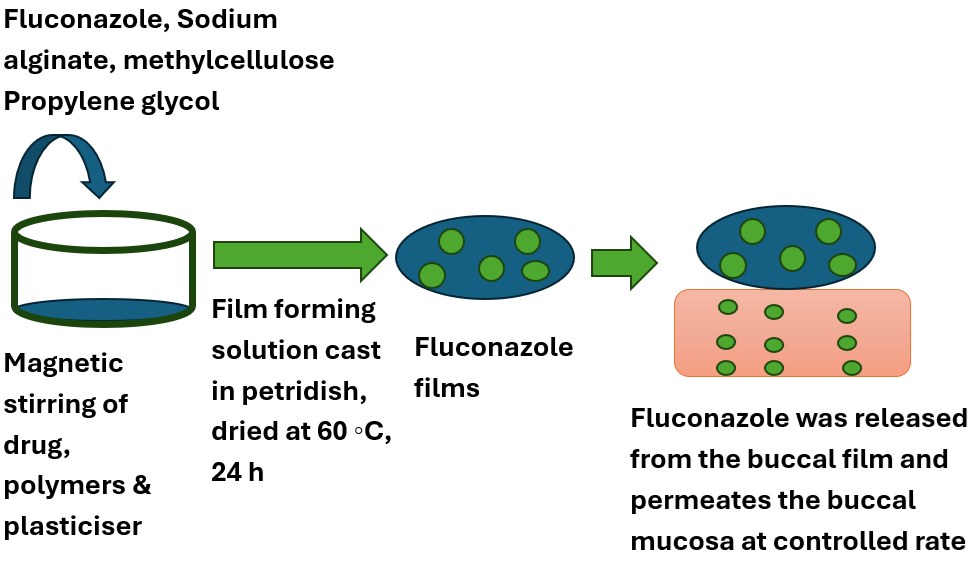
Sodium alginate/Methyl cellulose-based fluconazole containing buccal films were prepared using solvent casting technique [24]. The compositions of the film formulations are presented in Table 1. First, sodium alginate and methylcellulose were dispersed in predetermined volume of water and stirred for 1 hour using a magnetic stirrer. Then, the calculated amount of fluconazole and plasticiser (glycerol or propylene glycol) were added to the film forming solution, and the mixture was stirred for an additional 1 h. Afterward, 45 mL of each drug-containing solution was transferred into 90 mm glass petri dishes and dried in a desktop oven (Morex Medical, UK) at 600 C for 20-24 h. The dried fluconazole films were secured in baking paper/aluminium foils and stored in a desiccator at room temperature.
2.4. Physicomechanical Evaluation
2.4.1. Organoleptic Studies
The appearance, odour, peelability, texture and homogeneity of the fluconazole containing buccal films were assessed by sensory examination.
2.4.2. Weight Uniformity Evaluation
The extent of weight uniformity of the films was evaluated by weighing five films (1 cm x 1 cm) using an electronic balance (Dawood, China) and the average weight of each film was calculated and expressed as mean ± SD.
2.4.3. Film thickness Evaluation
The thickness values of the optimised films (1 cm x 1 cm) were measured using a micrometer screw gauge (Japan Scientific, Japan), and the mean film thickness values were recorded [24].
2.4.4. Surface pH
The surface pH values of the optimised fluconazole films (2 cm x 2 cm) were evaluated using a previously reported method, with simulant salivary fluid used for experimentation [24]. The fluconazole containing buccal films were placed in various petridishes containing 2 mL of simulant salivary fluid (pH 6.8), and the films are allowed to swell for 15 min. Then, the surface pH values of the hydrated film were determined using a digital pH meter (PH-3012B, Shenzhen Tomtop Technology Co Ltd., China).
2.4.5. Folding Endurance
The Folding endurance values of the optimised buccal films were determined by repeatedly folding the films (1 x 2 cm2) at the same axis; and counting the number of folds the film tolerated before tearing [24].
2.4.6. Tensile Test
The tensile properties of the optimized fluconazole containing buccal films were evaluated using a previously reported method [24]. The polymeric films were cut into 1 cm × 3 cm rectangular sections, and the film samples were investigated using the Universal Testing Machine (Instron-series 3369, USA), fitted with a 50 kN load cell. The film sections were mounted between two clamps and stretched at a rate of 50 mm/min with an applied load range of about 50 N and a gauge length of 5 cm. The experiment was carried out at 20 °C and relative humidity of 60%.
The tensile strength of the film is the maximum amount of tensile stress that the film can withstand before tearing while the percent elongation at break (EOB) or breaking strain value of the film is shown in Equation (1).
2.5. Swelling Index - Percent Hydration
2.5.1. Preparation of Simulant Salivary Fluid
Phosphate buffer solution (pH 6.8, 0.2 M), which served as the simulant saliva, was prepared by dissolving 13.872 g of potassium dihydrogen phosphate and 35.084 g of disodium hydrogen phosphate in deionized water (200 mL) and stirred for 1 h. The pH of the buffer solution was adjusted to pH 6.8 before making up the buffer solution to the required volume (250 mL).
2.5.2. Evaluation of Swelling Index
The swelling indexes of the optimised films was evaluated as percentage simulant salivary fluid hydration. Briefly, each film (1 cm × 1 cm) was weighed (W1) and dipped in simulated saliva (PBS pH 6.8; 10 mL) maintained at 37 ± 1 ◦C. Then, the film was removed from the simulant saliva at various time intervals (5, 10, 15, 20, 25, 30, and 35 min), and the film was wiped and reweighed (W2) [24].
The percentage film hydration was calculated using the Equation (2).
2.6. In Vitro Mucoadhesion Studies
The in vitro mucoadhesion time values of the fluconazole films were evaluated using a published method [24]. The prehydrated cellulose membrane (2x3 cm2) was glued to the surface of a glass slide (2.5 x 7.5 cm). Buccal film (1 x 1 cm2) was cut, and its surface was wetted using phosphate buffered saline (PBS; pH 6.8). The test film was brought in contact with the surface of the cellulose membrane (simulant buccal membrane) by applying suitable force for 10 s. Then, PBS (100 mL) was poured into the beaker and the glass slide securing the membrane and film was placed into the beaker at an angle of 45 ° such that the membrane and film are completely immersed in the simulant saliva. Afterward, the beaker was placed in a shaker water bath (SHA-C; Etrack Scientific Instruments, England) maintained at 37 ͦ C and agitated at 75 rpm to simulate buccal physiological conditions. The time required for complete erosion or detachment of the fluconazole film from the simulant buccal membrane was recorded as the mucoadhesion time.
2.7. Ex Vivo Porcine Buccal Mucoadhesion Studies
The ex vivo porcine buccal mucoadhesion values of the fluconazole films were determined using the method described in section 2.6, with the simulant buccal (cellulose) membrane replaced with porcine buccal mucosal tissues. Briefly, buccal mucosal tissues were obtained from freshly slaughtered pigs collected from the local abattoir, and the animal tissues were transported over ice-cold water (pH 7.0±0.2) to the laboratory. Excess connective tissues were trimmed using a scalpel blade and the buccal mucosal surfaces were protected from damage during tissue preparation. Then, the buccal mucosal tissues (2 cm x 3 cm) were rinsed using phosphate buffer (pH 6.8) prior to experimentation and attached to a glass slide (2.5 x 7.5 cm) using an adhesive. The fluconazole film (1 cm x 1 cm) was brought in contact with the glass slide securing the buccal tissues (2 cm x 2 cm) for 10 s. Then the glass slide was placed in a beaker containing phosphate buffer (100 mL; pH 6.8) at 45 ͦ, and the beaker was maintained in a water bath agitated at 75 rpm to mimic buccal environment. The ex vivo buccal mucoadhesion time, which is the time taken for the studied films to detach from the buccal mucosal tissues, was recorded.
2.8. Drug Content Evaluation
Buccal film (1 x 1 cm2) that should contain 5 mg of fluconazole, was dispersed in methanol (80 mL), and stirred magnetically for 30 min. Then, the drug solution was filtered and made up to 100 mL drug solution in a volumetric flask. Afterward, the drug solution was agitated in an ultrasonic bath. In addition, pure fluconazole (5 mg) was dissolved in methanol; filtered and made up to 100 mL in a volumetric flask using methanol. The samples were analyzed using a UV–visible spectrophotometer (UV-6300PC, VWR Instruments, Canada) at wavelength of maximum fluconazole absorption (208 nm).
The percent drug content (Equation 3) was determined as follows:
2.9. In Vitro Drug Release Studies
Simulant salivary fluid was prepared (described in section 2.5) and mixed with methanol (1:1) and the pH of the drug release medium was adjusted to pH 6.8 using 0.1 M hydrochloric acid solution. The drug release studies of the optimised fluconazole films were carried out using the Franz diffusion cells. A pre-hydrated cellulose membrane (Millipore, 0.45 μm) was mounted between the donor and receptor medium. The receptor compartment was filled with simulated salivary fluid/methanol (1:1; 20 mL, pH 6.8). The Franz cell was placed on a magnetic stirrer, constantly stirred throughout the experiment; maintained at 37 °C and equilibrated for 30 min before the hydrated film (1 × 1 cm) containing 5 mg of fluconazole was placed in the donor compartment. Aliquots (2 mL) were withdrawn from the receptor compartment at predetermined time intervals (0.5 h, 1, 2, 4, and 6 h) and immediately replaced with an equal amount of fresh prewarmed simulated salivary fluid to maintain sink conditions. Withdrawn samples were assayed for drug content at the wavelength of maximum drug absorption (261 nm) using a UV–visible spectrophotometer (UV-6300 PC; VWR Instruments, Canada) and applying a validated UV method (Table S1). Standard solutions of fluconazole in simulated salivary fluid/methanol mixture, pH 6.8 (1:1) (5 μg/mL to 100 μg/mL), were used to construct a standard calibration curve for fluconazole quantification.
The generated fluconazole release data was fitted into different drug release kinetic models (zero-order, first-order, Higuchi and Korsemeyer–Peppas model equation) to predict the drug release kinetics of the fluconazole films [24].
2.10. Antifungal Assay Against C. albicans
The antifungal activities of fluconazole containing buccal films against Candida albicans were studied using a Sabouraud agar ditch technique [24]. Briefly, the fluconazole film (1 x 1 cm2) was placed into a ditch cut in the agar plate and freshly prepared calibrated Candida culture loops was streaked across the agar in the petridish at a right angle from the ditch to the edge of the plate. The plate was incubated for 72 h at 25 °C. The positive control plates contained fluconazole solution. Afterward, zones of fungal inhibition were recorded for the optimised fluconazole containing buccal films.
2.11. Real-Time Stability Studies
The real-time stability profiles of the optimized fluconazole containing buccal film formulations were evaluated according to the ICH guidelines for intermediate stability studies [28]. The optimized films were wrapped in baking paper/aluminium foil and maintained at 30 ± 2 °C/65 ± 5% RH for six months. The fluconazole films were observed monthly for changes in their organoleptic properties and folding endurances and observations were noted.
2.12. Statistical Analysis
All experiments were carried out in triplicates and data were presented as mean ± standard deviation. One-Way ANOVA / Bonferroni post-hoc test was used for statistical analysis, with p < 0.05 indicating significant statistical differences between datasets.
3. Results
3.1. Drug-Polymer Compatibility Profile
The FTIR spectra of fluconazole, methylcellulose and sodium alginate, and the optimised fluconazole films are shown in Figure 1. The functional groups present in sodium alginate and methylcellulose were similar: Absorption bands at 1017-1021 cm-1 depicting C-O-C glycosidic bonds and those at 1401-1408 cm-1 indicated symmetric stretching of COO groups in sodium alginate. Fluconazole, sodium alginate and methylcellulose had peaks appearing at 1584-1587 cm-1, suggesting C-C stretch in ring and asymmetric stretching of COO groups, while absorption bands at 2843-3660 cm-1 represented their C-H and O-H stretch. In addition, fluconazole had a distinctive C-N stretch at 1140-1274 cm-1.
3.2. Organoleptic Properties
Fluconazole containing sodium alginate/methylcellulose-based buccal films were successfully formulated using propylene glycol as the plasticiser. Figure 2 showed the three optimised fluconazole-containing films with varying concentrations of sodium alginate while maintaining a constant concentration of methylcellulose (1.6% w/w) and plasticiser (10%) across all samples. The films were off-white, odourless, peelable, homogenous, with smooth texture.
3.3. Physicomechanical Properties of Fluconazole Films
The mean weights of the fluconazole films (1 cm x 1 cm) ranged from 0.1 g to 0.12 g (Table 2).
Also, the thickness, surface pH, folding endurance values as well as swelling indexes and disintegration time values of the optimised fluconazole films (F1, F2, and F3) are presented in Table 2.
3.4. Tensile Properties of Buccal Films
The tensile strength and breaking strain values of the optimised films are provided in Figure 3a and b.
3.5. In Vitro and Ex Vivo Mucoadhesion Time Profiles
The mean time needed to detach the studied fluconazole buccal films from the simulant (cellulose membrane) or ex vivo buccal mucosa are the in vitro and ex vivo mucoadhesion time, respectively. The in vitro mucoadhesion time increased in this order: film F1: 3.0±0.6 h < F2: 3.8±0.4 h < F3: 5.5±0.3 h (Figure 4). The ease of detachment of the optimised fluconazole films from ex vivo buccal mucosal tissues exhibited a similar trend: Film F1: 1.2±0.3 h < 1.6±0.1 h < 2.3±0.3 h.
3.6. Uniformity of Drug Contents
The drug content values of the optimised fluconazole films are detailed in Table 3.
3.7. In Vitro Drug Release Profiles
3.7.1. Standard Calibration Curve of fluconazole in simulant salivary fluid/methanol (1:1; pH 6.8)
The fluconazole in simulant salivary fluid/methanol mixture (1:1) calibration curve is presented in Figure S1; with r2 value of 0.9988 and the equation of the graph was y = 0.0132x.
3.7.2. Fluconazole Flux Across Simulant Buccal Mucosa
The various fluconazole flux values from fluconazole films F1 to F3 through the simulant buccal membranes, are presented in Figure 5.
The result of fitting the fluconazole films’ drug release data to different drug release kinetic models (Zero-order, First order, Higuchi and Korsmeyer-Peppas models) are presented in Table 4.
3.8. Antifungal Profiles of Fluconazole Films Against Candida albicans
3.9. Real-Time Stability Profiles
The fluconazole buccal films were stable at 30 ± 2 °C and a relative humidity of 65 ± 5% after a study period of 6 months.
4. Discussion
Oral candidiasis is one of the most common oral diseases affecting immunocompromised patients such as HIV-positive individuals, cancer patients; people on prolonged intravenous steroid and antibiotic use; geriatrics and some paediatrics [6]. Fluconazole is one of the recommended therapeutic agents used to treat oral candidiasis [29]. Oral hygiene and topical fluconazole formulations are effective for the treatment of mild cases of the disease while systemic fluconazole therapy is required for patients that are non-responsive to topical therapy or prone to developing systemic infections [6].
Conventional fluconazole formulations such as oral capsules and tablets induce systemic side effects due to the large volume of fluconazole distribution (0.55-0.65 kg/L) in systemic circulation [27]. Topical creams, lotions and spray exhibit poor drug residence time, inaccurate drug dosing and variation in therapeutic performance. In addition, intravenous fluconazole therapies are invasive, which may limit patients’ compliance to dosage regimen, resulting in therapeutic failure [27].
The buccal route has been increasingly explored in the last decade for local and systemic drug delivery due to its non-invasiveness, avoidance of gastric acidic and hepatic enzymatic drug degradation and facilitation of sustained drug release. Typically, mucoadhesive buccal films adhere to the buccal mucosa for prolonged periods to facilitate film swelling, disintegration, dissolution, drug release and permeation into underlying buccal tissues to facilitate effective disease treatment [27]. This study aimed to formulate mucoadhesive, thin, aesthethically appealing, and cost-effective buccal films using biocompatible, film-forming and mucoadhesive sodium alginate and methylcellulose. The optimised fluconazole films could improve the therapeutic outcomes of patients with oral candidiasis. Also, they could serve as an alternative dosage form to marketed oral fluconazole tablets and topical fluconazole creams, currently used in the clinics.
The FT-IR peaks recorded for fluconazole, sodium alginate and methyl cellulose were evident in the three optimised fluconazole film formulations (Figure 1), and no new peaks were recorded. Nevertheless, there were shifts in the position at which the peaks appeared as well as varied peak intensities. This FT-IR result suggested that there was no remarkable chemical interaction between fluconazole and the polymers used to formulate the optimised buccal films. These findings are in good agreement with the FT-IR spectra of sodium alginate films reported by Moura-Alves et al., (2023), which revealed absorption peaks at 3251, 2933, 1598, 1407 and 1025 cm-1 [30]. The position of these peaks are comparable with that of SA/MC-based films studied in this work.
Preformulation studies revealed that methylcellulose (1.8%) generated highly viscous polymeric dispersion that was difficult to incorporate with sodium alginate and fluconazole. On the other hand, formulation of fluconazole films using glycerol as the plasticiser yielded a sticky, non-peelable film product. This finding may be due to the hydrophilic nature of sodium alginate and methyl cellulose requiring a hydrophobic plasticiser such as propylene glycol to generate a satisfactory film formulation. Therefore, the optimised fluconazole films were formulated using a constant amount of methylcellulose (1.6%) and varying amount of sodium alginate (mucoadhesive polymer). There was a progressive improvement in the homogeneity of the films as the concentration of sodium alginate in the fluconazole films increased from 1% to 1.6%. This could be due to the presence of more sodium alginate molecules facilitating hydrogen bonding with methyl cellulose and promoting homogeneity of the film formulation.
The weight of pharmaceutical films should be light to facilitate patient’s comfort and acceptability. The low standard deviation values recorded during film weight measurement revealed that the film manufacturing process was reproducible, which is desirable to upscale film production. There were significant statistical differences in the weights of the films as their sodium alginate content increased from 1% to 1.6% (p < 0.05). The studied sodium alginate/methylcellulose-based fluconazole films were lighter than the cetylpyridinium chloride loaded chitosan/polyvinylalcohol-based buccal films reported by Abouhussein and coworkers [10] (0.1-0.12 g versus 0.38-0.40 g). Therefore, the novel fluconazole film will be appealing to the patients due to their natural feel after buccal application, improving patient compliance to dosage regimen and therapeutic success.
Interestingly, all the optimised fluconazole films exhibited comparable thickness values (0.08-0.09 mm; p > 0.05). This finding revealed that an increase in the sodium alginate content of the films from 1% to 1. 6% did not have a remarkable impact on the film thickness. Cetylpyridinium chloride containing buccal films displayed comparable thickness with the novel fluconazole films (0.11-0.12 mm versus 0.08-0.09 mm) [10]. On the other hand, the film thickness values of the new fluconazole films were greater than that of the myrtle extract loaded gelatin/pectin/polyvinylpyrrolidone/methylcellulose-based oral films reported by Hashemi and coworkers (0.08 -0.09 mm versus 0.03-0.04 mm) [31]. The thin myrtle extract-loaded oral films may be prone to puncture during handling, transportation and buccal administration, resulting in premature drug loss and short-lived therapeutic effect.
Previously reported hydroxypropyl cellulose/methylcellulose/ethylcellulose-based felodipine containing buccal films, Eudragit RS 100/HPMC-based fluconazole oral strips, HPMCE3/HPMCK4/Carbopol 934-based doxycycline hyclate-based buccal films and Proloc/HPMC/Eudragit RS 100-based rizatriptan benzoate buccal films were thicker than the currently studied fluconazole films (0.12-0.17 mm versus 0.22-0.24 mm versus 0.35-0.45 mm versus 1.02-1.32 mm versus 0.08-0.09 mm)[12,13,15,32]. These findings revealed that the thickness values of buccal films are dependent on the type, number and concentration of polymeric excipients used to prepare the film formulations. Nevertheless, the newly developed fluconazole containing buccal films (0.08-0.09 mm) would be appealing to the patient after buccal application due to their thin dimension. Also, their reduced thickness values could facilitate faster drug dissolution and permeation into underlying buccal mucosal tissues, resulting in the effective treatment of oral candidiasis.
The evaluation of the surface pH of buccal film is an indirect method of evaluating their buccal mucosal irritant potential. There is a strong need to develop buccal films which have surface pH comparable to the buccal pH (6.4) to avoid buccal mucosal irritation [33]. The acceptable pH for buccally delivered formulations could range from 5.5 to 7 to facilitate biocompatibility with the buccal mucosal membranes [17]. Interestingly, there was a statistically significant increase in the acidity of the films as the concentration of sodium alginate used to formulate the films increased from 1% to 1.3% (SA1%: pH 7.61 versus SA1.3%: pH 7.18) (p < 0.05). However, the pH values of films F2 and F3 containing 1.3% and 1.6% of sodium alginate, respectively, are statistically similar (pH 7.18 versus 7.13) (p >0.05).
The novel fluconazole films F2 and F3 containing 1.3% to 1.6% sodium alginate displayed acceptable pH values for buccal drug administration (pH 7.1-7.2). The buccal irritant potential of the studied fluconazole films F1 to F3 (pH 7.13-7.61) may be minimal compared with that of cetylpyridinium chloride containing chitosan/polyvinylalcohol-based buccal films with unsatisfactory surface pH of 4.89-5.35 [10], suggesting that the newly developed films will not pose any irritation to the buccal mucosal tissues.
Folding endurance values of buccal films dictate their ability to maintain their integrity during handling, transportation, and after buccal application. Satisfactory drug containing films display folding endurance values of ≥ 250 as they can withstand repeated folding without breaking [24]. All the studied fluconazole films displayed excellent folding endurance of over 500. The folding endurance values of the optimised sodium alginate/methylcellulose-based fluconazole films were greater than that recorded for hydroxypropyl cellulose/methylcellulose/ethyl cellulose-based felodipine buccal films [15] and HPMC E3/HPMC K4/Carbopol 940-based doxycycline hyclate containing buccal films (> 500 versus 212-232 versus > 350) [12]. These findings suggested that the folding endurance of buccal films was dependent on their polymeric constituents and nature of the loaded drug. Moreover, the interaction between sodium alginate and methylcellulose may be greater than those present between cellulose derivatives.
The tensile strength of buccal films quantifies their stretchable nature whereas the resistance of the buccal film formulation to puncture during handling, transportation and buccal application indicates their “elongation at break” (breaking strain) profile. These tensile parameters were assessed to confirm the mechanical profiles of the optimised buccal films. The composition of the buccal films influenced their tensile strength and breaking strain values (Figure 3 a & b). For instance, the tensile strength of the fluconazole films increased with an increase in their sodium alginate content (Figure 3a). Film F3 containing 1.6% sodium alginate displayed the greatest tensile strength (0.68±0.04 MPa). However, film F3 displayed the least breaking strain (12.28±4.51%). Nevertheless, the breaking strain value of F3 was satisfactory. There was no significant statistical difference between the breaking strain of film F2 and film F3 (Figure 3 b) containing 1.3% and 1.6% of sodium alginate, respectively (13.62±3.88% versus 12.28±4.51%; p >0.05).
Even though film F1 had the best breaking strain (28.81±1.38%) (Figure 3b), it may be unsatisfactory for buccal application due to its poor tensile strength (0.07±0.01 MPa) (Figure 3a), which will compromise its stretchability, resulting in film puncture and poor patient acceptability. Overall, film F3 exhibited the most promising tensile properties required for the buccal delivery of fluconazole. This finding is in good agreement with those reported for the most promising Eudragit L-100/chitosan-based tenofovir containing and boronated 4-arm PEG/PVP/MC-based fluconazole containing vaginal films that exhibited the best tensile strength and least breaking strain [24,34]. In addition, the most promising fluconazole buccal film F3 exhibited improved tensile strength compared to HPMCE3/HPMCK4/Carbopol 934-based doxycycline hyclate containing buccal films reported by Dinte and coworkers (0.68±0.04 MPa versus 0.39 MPa) [12], suggesting that the type of polymeric constituents of film formulation influenced their mechanical properties.
Interestingly, the most promising previously reported boronated 4-arm PEG/MC/PVP-based fluconazole containing vaginal films [24] exhibited greater breaking strain value (54%) than the best SA/MC-based fluconazole buccal films in the current study (12%). Nevertheless, both films exhibited comparable satisfactory tensile strength (0.6 MPa versus 0.7 MPa), revealing that the most promising fluconazole containing buccal films will be suitable for buccal application. This finding may be due to the two film-forming polymeric constituents (methylcellulose and polyvinylpyrrolidone) of the previously reported vaginal film [24] while one film-former (methylcellulose) was employed in the current research to formulate buccal films.
The extent of polymeric film hydration is dependent on the type and physicochemical properties of the constituent polymers [35]. The swelling index data (Table 2) revealed that the sodium alginate content of the film influenced their swelling capabilities. For instance, film F1 containing 1% of sodium alginate exhibited a lesser swelling index than film F3 with sodium alginate content of 1.6% (57±7% versus 70±7%; p < 0.05), suggesting that the concentration of sodium alginate in the films influenced their extent of simulant saliva hydration. However, there was no significant statistical difference between the swelling index of film F2 and F3 containing 1.3% and 1.6% of sodium alginate, respectively (68±2% versus 70±1%; p > 0.05).
Interestingly, the films disintegrated after swelling. This finding could be due to the hydrophilicity of methylcellulose and sodium alginate inducing water uptake into the polymeric films; facilitating relaxation of stretched, twisted or entangled bioadhesive polymer (sodium alginate), leading to the disentanglement of individual polymer chains; generation of macromolecular network; increased porosity and disintegration of the films [36]. Moreover, this disintegration pattern is desirable for the loaded drug to become available at the buccal mucosa surfaces and permeate into the underlying buccal tissues at a controlled rate. Film F3 exhibited the highest disintegration time of 35 min. This finding may be due to the greatest sodium alginate content preventing the dissociation of the film matrix.
The studied SA/MC-based fluconazole films exhibited comparable swelling profile with HPMC/HPC/EC/MC-based felodipine films (57-70% versus 57-80%) [15]. On the other hand, they displayed greater swelling index than Proloc/HPMC/Eudragit RS 100-based rizatriptan benzoate films [13], HPMCE3/HPMCK4/C940-based doxycycline hyclate films [12], chitosan/HPMC or MC or HEC or PVA-based cetylpyridinium chloride films [10] (57-70% versus 20-30% versus 12-43% versus 5-20%). These findings revealed that the nature of the polymeric constituents of the film formulation was a more critical determinant of its swelling potential than the number of polymers present in the films.
Mucoadhesion is a critical parameter that dictates successful buccal drug delivery because insufficient mucoadhesion could displace the buccal film from the site of application, reducing contact time between the drug and the diseased buccal tissues, resulting in therapeutic failure. Cellulose derivatives such as methylcellulose and natural polysaccharides such as sodium alginate possess hydrogel-forming properties [37,38], which are necessary for mucoadhesion. In addition, sodium alginate could interact with buccal mucosal surfaces via non-covalent bonding between the carboxyl groups of alginate and hydroxyl groups of mucin glycoproteins [38]. Moreover, polymer swelling in simulant saliva ensures that the polymer chains uncoil and promote hydrogen bonding and/or electrostatic interaction between polymer and mucosal surfaces [36].
The sodium alginate content of the fluconazole films influenced their in vitro and ex vivo mucoadhesiveness. For instance, the in vitro and ex vivo mucoadhesion time values of formulation F3 containing 1.6% sodium alginate was greater than that of sample F2 and F1 containing 1.3% and 1.6% of sodium alginate, respectively (5.5±0.3 h; 2.3±0.3 h versus 3.8±0.4 h; 1.6 ±0.1 h versus 3.0±0.6 h; 1.2 ±0.3 h). Significant statistical differences between in vitro and ex vivo mucoadhesion time values of the studied fluconazole films became evident when the concentration of sodium alginate in the film increased from 1.3% to 1.6% (p < 0.05).
This finding is in good agreement with previous studies on boronated 4-arm PEG/PVP/MC-based fluconazole vaginal films, with increased content of the mucoadhesive polymer (boronated 4-arm PEG) in the films resulting in an improved in vitro mucoadhesion time profile of the vaginal films [24]. There was good correlation between the swelling index of fluconazole films and their mucoadhesive profile. For instance, film F3 with the highest in vitro and ex vivo mucoadhesion time values (5.5±0.3 h; 2.3±0.3 h) displayed the best swelling index (70±1%). The most promising alginate/pectin based posaconazole containing buccal films exhibited greater ex vivo porcine buccal mucoadhesion time (3.4 h) than the most promising fluconazole containing sodium alginate/methylcellulose-based buccal film (2.3 h), which may be due to differences in the equipment used for experimentation. For instance, posaconazole films were evaluated using a modified USP disintegration tester while the fluconazole films were assessed using a shaking water bath technique [11]. Nevertheless, the currently studied fluconazole films exhibited satisfactory ex vivo mucoadhesion time sufficient to facilitate controlled drug release and permeation into the diseased buccal mucosal tissues.
“Uniformity of drug content evaluation” is an important pharmaceutical quality control test for buccal films. USP recommends that drug content of finished drug products should contain 85-115% of active pharmaceutical ingredient [39]. The studied fluconazole films (Table 3) contained satisfactory level of the drug (98.7-113.8%), which suggested that the solvent casting method of preparing the drug containing films was efficient and the inclusion of appropriate plasticiser (propylene glycol) facilitated uniform drug distribution within the film formulation.
Interestingly, there was a good correlation between the concentration of the mucoadhesive constituent (sodium alginate) of the fluconazole films and their drug content. For instance, the drug content of the fluconazole film F1 containing 1% sodium alginate was lesser than that of film F2 and F3, containing 1.3% and 1.6% of sodium alginate, respectively (98.7±0.2% versus 99.7±0.2% versus 113.8±0.2%). This could be due to greater concentration of sodium alginate facilitating retention of greater amount of the drug within the film formulation. This finding is in good agreement with findings obtained for fluconazole containing vaginal films containing 0.075% of mucoadhesive boronated 4-arm polyethylene glycol (B4PEG) exhibiting greater drug content than similar film formulation containing 0.05% of B4PEG (107% versus 110%) [24].
The amounts of fluconazole released from films F1, F2 and F3 containing 1%, 1.3% and 1.6% of sodium alginate after 6 h were 4046±109 μg/cm2, 4075±359 μg/cm2, and 3645±161 μg/cm2, respectively. Interestingly, there was no significant statistical differences between the amount of fluconazole released from the studied fluconazole films after 6 h (p >0.05) in simulant salivary fluid (pH 6.8), which might be due to their similar methylcellulose content. This finding is in good agreement with previous studies where two different fluconazole films containing 1.6% methylcellulose and differing boronated 4-arm polyethylene glycol content exhibited similar drug flux (4740-4776 μg/cm2) in simulant vaginal fluid (pH 4.2) [24], confirming that the drug release controlling polymer, methylcellulose, was a stronger determinant for fluconazole release profile of the films than the pH of the release medium.
All the studied fluconazole containing buccal films fitted best with the Higuchi and Korsmeyer-Peppas drug release kinetic model (Table 4). Also, their Korsmeyer-Peppas model-associated diffusional exponent (n) values ranged from 3.27 to 3.63, suggesting that fluconazole was released from the film formulation via simulant salivary fluid diffusion into the fluconazole film and relaxation of the sodium alginate/methylcellulose-based polymeric films [40]. This finding is in good agreement with earlier studies on sodium alginate/polyvinyl alcohol and boronated 4-arm polyethylene glycol/polyvinylpyrrolidone/methylcellulose-based fluconazole films that fitted best with the Higuchi model [24,27], suggesting that the type of polymer and drug used to formulate films influenced their drug release kinetics.
Fluconazole solution exhibited superior antifungal activity relative to the studied films F1 to F3 (ZOI: 42.3 mm versus 39.7-40.2 mm). This finding may be due to the lack of polymers in the fluconazole solution which facilitated rapid drug release and antifungal activity, which could result in short-lived therapeutic action in vivo. However, there was no significant statistical differences between the antifungal activity of the fluconazole films F1 to F3 (p > 0.05), suggesting that the polymeric constituents of the fluconazole films did not influence their antifungal activity, and anticandidal effect of the fluconazole films was dependent on the concentration of fluconazole in the film formulations.
The anti-Candida activity of SA/MC-based fluconazole films was less than that of previously studied Eudragit RS 100/HPMC-based fluconazole oral strips [32] and boronated polyethylene glycol/PVP/MC-based fluconazole vaginal films [24] (ZOI: 39.7-40.2 mm versus 47.0 to 49.7 mm versus 49.2-50.8 mm). These findings may be due to differences in the strain of Candida tested as well as the body site where the fungal strains were obtained. Nevertheless, the anti-Candida activity for the newly developed fluconazole films were excellent because effective antifungal products exhibit zone of Candida inhibition of ≥ 20 mm [41].
There were no remarkable differences in the organoleptic and mechanical properties of the optimised fluconazole films after storage at 30 ± 2 °C and a relative humidity of 65 ± 5% for 6 months, indicating that the fluconazole buccal films were stable. The sustained stability of the fluconazole films may be due to the favourable interaction between the polymeric constituents and drugs.
5. Conclusions and Future Directions
For the first time, mucoadhesive sodium alginate/methylcellulose-based fluconazole buccal films were successfully formulated and characterised, for potential treatment of oral candidiasis. FTIR analysis confirmed no significant chemical interactions between fluconazole and the chosen polymers, ensuring drug stability and compatibility with polymeric excipients used to formulate the buccal films. The films exhibited satisfactory organoleptic, physicomechanical, swelling, mucoadhesive properties, drug release profiles, stability, and antifungal activity, indicating their potential for effective treatment of oral candidiasis. Interestingly, all the optimised fluconazole films displayed excellent antifungal activity against Candida albicans (zone of Candida inhibition: 40 mm). The fluconazole films containing 1.6% SA and 1.6% MC (F3), was the most promising formulation based on its surface pH, tensile strength, swelling index and mucoadhesiveness. It could be used as an alternative dosage to the marketed fluconazole gel, for the potential treatment of oral candidiasis. The new SA/MC-based buccal films could result in drug dosage reduction from 150 mg to 5 mg as well as avoidance of side effects associated with oral and systemic drug delivery and improved patient compliance.
Future research could explore a combination of boronated polymer and sodium alginate as the mucoadhesive polymer and the influence of the type and concentration of polymers on the mucoadhesive and antifungal properties of the novel film formulation will be investigated.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/doi/s1, Table S1: Chromatographic (UV) Analytical Method Validation parameters for fluconazole quantification in simulant salivary fluid/methanol mixture (1:1; pH 6.8), with accuracy and precision of the UV method determined from three graded fluconazole concentrations (low, medium and high), i.e. 5 μg/mL, 25 μg/mL and 75 μg/mL; n = 3; Figure S1: Fluconazole Calibration Curve prepared using standard solutions of fluconazole in phosphate buffer/methanol (1:1), pH 6.8; n = 3; Figure S2: Images revealing zones of C. albicans inhibition exhibited by fluconazole solution and fluconazole films F1 to F3.
Author Contributions
Conceptualization, O.K.; Methodology/Investigation, A.O., A.A; O.K.; Writing – Original Draft Preparation, A. O., A. A.; Writing – Reviewing & Editing – C. A., O. K.; Data Curation/Visualisation, A.O., O.K., Software/Validation/Formal Analysis, O.K., Resources/Funding Acquisition, O.K., A.O., Project Administration/Supervision, C. A., O. K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Dataset available on request from the authors.
Acknowledgments
The authors are grateful to Mr. Abdul-Rahman Usman, Department of Pharmaceutical Microbiology and Biotechnology, University of Lagos, Nigeria for his help with microbiological assay. We also appreciate Dr. Emmanuel Ajoge, Obafemi Awolowo University, Ile-Ife, Nigeria for his assistance with the tensile evaluation of the buccal films.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Singh, A.; Verma, R.; Murari, A.; Aqrawal, A. Oral candidiasis: An overview. J. Oral. Maxillofac. Pathol. 2014, 18, 81–85. [Google Scholar] [CrossRef]
- Ashman, R.B.; Farah, C.S. Oral candidiasis: Clinical manifestations and cellular adaptive host responses. In Fungal Immunology: From an Organ Perspective; Fidel, P.L., Huffnagle, G.B., Eds.; Springer: Boston, Massachusetts, 2005; pp. 59–83. [Google Scholar] [CrossRef]
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6(1), 15–42. [Google Scholar] [CrossRef]
- Mushi, M.F.; Bader, O.; Taverne-Ghadwal, L.; Bii, C.; Groß, U.; Mshana, S.E. Oral candidiasis among African human immunodeficiency virus-infected individuals: 10 years of systematic review and meta-analysis from sub-Saharan Africa. J. Oral. Microbiol. 2017, 9(1), 1317579. [Google Scholar] [CrossRef]
- Ambe, N.F.; Longdoh, N.A.; Tebid, P.; Bobga, T.P.; Nkfusai, C.N.; Ngwa, S.B.; et al. The prevalence, risk factors and antifungal sensitivity pattern of oral candidiasis in HIV/AIDS patients in Kumba District Hospital, Southwest Region, Cameroon. Pan Afr. Med. J. 2020, 36, 23. [Google Scholar] [CrossRef]
- Taylor, M.; Brizuela, M.; Raja, A. Oral Candidiasis Bookshelf ID: NBK545282. StatPearls Publishing LLC, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK545282/ (accessed on 23rd October 2024).
- Pasko, M.T.; Piscitelli, S.C.; Van Slooten, A.D. Fluconazole: a new triazole antifungal agent. DICP 1990, 24(9), 860–867. [Google Scholar] [CrossRef]
- Ashok, A.; Mangalore, R.P.; Morrissey, C.O. Azole therapeutic drug monitoring and its use in the management of invasive fungal disease. Curr. Fungal Infect. Rep. 2022, 16, 55–69. [Google Scholar] [CrossRef]
- Shipp, L.; Liu, F.; Kerai-Varsani, L.; Okwuosa, T.C. Buccal films: A review of therapeutic opportunities, formulations & relevant evaluation approaches. J. Control Rel 2022, 352, 1071–1092. [Google Scholar] [CrossRef]
- Abouhussein, D.; el Nabarawi, M.A.; Shalaby, S.H.; El-Bary, A.A. Cetylpyridinium chloride chitosan blended mucoadhesive buccal films for treatment of pediatric oral diseases. J. Drug Deliv. Sci. Technol. 2020, 57, Article 101676. [Google Scholar] [CrossRef]
- Szekalska, M.; Czajkowska-Kosnik, A.; Maciejewska, B.; Misztalewska-Turkowicz, I.; Wilczewska, A.Z.; Bernatoniene, J.; et al. Mucoadhesive Alginate/pectin films crosslinked by calcium carbonate as carriers of a model antifungal drug – Posaconazole. Pharmaceutics 2023, 15, 2415. [Google Scholar] [CrossRef]
- Dinte, E.; Muntean, D.M.; Andrei, V.; Bosca, B.A.; Dudescu, C.M.; Barbu-Tudoran, L.; et al. In Vitro and In Vivo Characterisation of a Mucoadhesive Buccal Film Loaded with Doxycycline Hyclate for Topical Application in Periodontitis. Pharmaceutics 2023, 15(2), 580. [Google Scholar] [CrossRef]
- Nair, A.B.; Shah, J.; Jacob, S.; Al-Dhubiab, B.E.; Patel, V.; Sreeharsha, N.; et al. Development of mucoadhesive buccal film for rizatriptan: in vitro and in vivo evaluation. Pharmaceutics 2021, 13(5), 728–743. [Google Scholar] [CrossRef]
- Ammar, H.O.; Ghorab, M.M.; Mahmoud, A.A.; Shahin, H.I. Design and in vitro/in vivo evaluation of ultra-thin mucoadhesive buccal film containing fluticasone propionate. AAPS PharmSciTech 2017, 18(1), 93–103. [Google Scholar] [CrossRef]
- Haritha, K.; Devi, N.; Durga, A.; Himaja, V.; Mounika, P.; Vyshnavi, V. Buccal Films Containing Felodipine: In vitro and In vivo Evaluation. Int. J. Pharm. Sci. Rev. Res. 2018, 53(2), 33–39. [Google Scholar]
- Soradech, S.; Williams, A.; Khutoryanskiy, V. Synthesis of poly (2-hydroxyethyl ethyleneimine) and its mucoadhesive film formulations when blended with chitosan for buccal delivery of haloperidol. Macromol. Biosci. 2025, 2400642, 1–12. [Google Scholar] [CrossRef]
- Abdella, S.; Afinjuomo, F.; Song, Y.; Upton, R.; Garg, S. Mucoadhesive Buccal Film of Estradiol for Hormonal Replacement Therapy: Development and In-Vivo Performance Prediction. Pharmaceutics 2022, 14, 542. [Google Scholar] [CrossRef] [PubMed]
- Bastos, F.; Pinto, A.C.; Nunes, A.; Simoes, S. Oromucosal products–Market landscape and innovative technologies: A review. J. Control Rel 2022, 348, 305–320. [Google Scholar] [CrossRef]
- Srivastava, N.; Aslam, S. Recent advancements and patents on buccal drug delivery systems: A comprehensive review. Recent Pat. Nanotechnol. 2022, 16, 308–325. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Nair, A.B.; Boddu, S.H.; Gorain, B.; Sreeharsha, N.; Shah, J. An updated overview of the emerging role of patch and film-based buccal delivery systems. Pharmaceutics 2021, 13(8), 1206. [Google Scholar] [CrossRef]
- Drug Bank. Fluconazole. 2023. Available online: https://go.drugbank.com/drugs/DB00196 (accessed on 23rd October 2024).
- Costa, M.J.; Marques, A.M.; Pastrana, L.M.; Teixeira, J.A.; Sillankorva, S.M.; Cerqueira, M.A. Physicochemical properties of alginate-based films: Effect of ionic crosslinking and mannuronic and guluronic acid ratio. Food Hydrocoll. 2018, 81, 442–448. [Google Scholar] [CrossRef]
- Khan, S.; Boateng, J.S.; Mitchell, J.; Trivedi, V. Formulation, characterisation and stabilisation of buccal films for paediatric drug delivery of omeprazole. AAPS PharmSciTech 2015, 16(4), 800–810. [Google Scholar] [CrossRef]
- Kolawole, O.M.; Okeke, P.K. Formulation and Evaluation of boronated 4-arm polyethylene glycol/polyvinyl pyrrolidone/methylcellulose-based fluconazole films for the potential treatment of vaginal candidiasis. JDDST 2025, 107, 106838. [Google Scholar] [CrossRef]
- Pamlenyi, K.; Kristo, K.; Jojart-Lacz, K.; Regdon, G., Jr. Formulation and optimization of sodium alginate polymer film as a Buccal Mucoadhesive Drug Delivery System Containing Cetirizine Dihydrochloride. Pharmaceutics 2021, 13(5), 619. [Google Scholar] [CrossRef]
- U.S. Food; Drug Administration. Code for Federal Regulations Title 21 Part 184—Direct Food Substances Affirmed as Generally Recognized as Safe. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1724 (accessed on 23rd October 2024).
- Patel, S.K.; Shah, D.R.; Tiwari, S. Bioadhesive films containing fluconazole for mucocutaneous candidiasis. Indian J. Pharm. Sci. 2015, 55–61. [Google Scholar] [CrossRef]
- ICH. ICH harmonized tripartite guideline – stability testing of new drug substances and products [Q1A (R2). 2003. Available online: https://database.ich.org/sites/default/files/Q1A%28R2%29%20Guideline.pdf (accessed on 28 May 2024).
- Govindarajan, A.; Bistas, K.G.; Ingold, C.J.; Patel, P.; Aboeed, A. StatPearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537158/ (accessed on 12th April 2025).
- Moura-Alves, M.; Lauriano Souza, V. G.; Silva, J.A.; Esteves, A.; Pastrana, L.M.; Saraiva, C.; et al. Characterisation of Sodium Alginate-Based Films Blended with Olive Leaf and Laurel Leaf Extracts Obtained by Ultrasound-Assisted Technology. Food 2023, 12(22), 4076. [Google Scholar] [CrossRef]
- Hashemi, M.; Ramezani, V.; Seyedabadi, M.; Ranjbar, A.M.; Jafari, H.; Honarvar, M.; et al. Formulation and Optimization of oral mucoadhesive patches of Myrtus Communis by Box Behnken Design. Adv. Pharm. Bull. 2017, 7(3), 441–450. Available online: http://apb.tbzmed.ac.ir. [CrossRef]
- Renꞔber, S.; Karavana, S.Y.; Yilmaz, F.F.; Eraꞔ, B.; Nenni, M.; Gurer-Orhan, H.; et al. Formulation and evaluation of fluconazole loaded oral strips for local treatment of oral candidiasis. JDDST 2019, 49, 615–621. [Google Scholar] [CrossRef]
- Sandri, G.; Rossi, S.; Ferrari, F.; Bonferoni, M.C.; Muzzarelli, C.; Caramella, C. Assessment of chitosan derivatives as buccal and vaginal penetration enhancers. Eur. J. Pharm. Sci. 2004, 21(2-3), 351–359. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Cazorla-Luna, R.; F. Notario-Pérez, F.; Rubio, J.; Ruiz-Caro, R.; A. Tamayo, A.; Veiga, M.D. Eudragit® L100/chitosan composite thin bilayer films for intravaginal pH-responsive release of Tenofovir. Int. J. Pharm. 2022, 616, 121554. [Google Scholar] [CrossRef]
- Avachat, A.M.; Gujar, K.N.; Wagh, K.V. Development and evaluation of tamarind seed xyloglucan-based mucoadhesive buccal films of rizatriptan benzoate. Carbohydr. Polym. 2013, 91, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Boateng, J.; Okeke, O. Evaluation of Clay-Functionalized Wafers and Films for Nicotine Replacement Therapy via Buccal Mucosa. Pharmaceutics 2019, 11, 104. [Google Scholar] [CrossRef]
- Conti, S.; Maggi, L.; Segale, L.; Machiste, E.O.; Conte, U.; Grenier, P.; et al. Matrices containing NaCMC and HPMC: 2. Swelling and release mechanism study. Int. J. Pharm. 2007, 333(1-2), 143–151. [Google Scholar] [CrossRef] [PubMed]
- Szekalska, M.; Puciłowska, A.; Szymańska, E.; Ciosek, P.; Winnicka, K. Alginate: Current Use and Future Perspectives in Pharmaceutical and Biomedical Applications. Int. J. Polym. Sci. 2016, Article ID 7697031, 1–17. [Google Scholar] [CrossRef]
- USP/NF. Uniformity of dosage units. United states pharmacopeia and national formulary. USP 43-NF 38: General Chapter <905> Uniformity of Dosage Units, United States Pharmacopeia Convention (2020).
- Baggi, R.B.; Kilaru, N.B. Calculation of predominant drug release mechanism using Peppas-Sahlin model, Part-1 (Substitution method): A linear regression approach. Asian J. Pharm. Technol. 2016, 6(4), 223–230. Available online: https://ajptonline.com/AbstractView.aspx?PID=2016-6-4-5. [CrossRef]
- Nurcahyanti, A.D.R.; Liliana, M.; Surja, S.S. Inhibitory activity of Lagerstreomia speciosa extract against Candida albicans, Aspergillus fumigatus, and Aspergillus flavus. J. Appl. Pharm. Sci. 2024, 14(2), 281–285. [Google Scholar] [CrossRef]
Figure 1.
Overlapped spectra of fluconazole, sodium alginate, methyl cellulose, and fluconazole films F1 to F3; F1=SA1%/MC1.6%; F2= SA1.3%/MC1.6%, F3 = SA1.6%/MC1.6%.
Figure 1.
Overlapped spectra of fluconazole, sodium alginate, methyl cellulose, and fluconazole films F1 to F3; F1=SA1%/MC1.6%; F2= SA1.3%/MC1.6%, F3 = SA1.6%/MC1.6%.

Figure 2.
Image of fluconazole films with differing sodium alginate content; F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.
Figure 2.
Image of fluconazole films with differing sodium alginate content; F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.

Figure 3.
(a) Tensile strength and (b) Elongation at Break profiles of fluconazole buccal films; data presented as mean±SD; n = 3; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.
Figure 3.
(a) Tensile strength and (b) Elongation at Break profiles of fluconazole buccal films; data presented as mean±SD; n = 3; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.

Figure 4.
In vitro and ex vivo porcine buccal mucoadhesion time profiles of fluconazole films at 37 ͦC; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC (in vitro mucoadhesion time values); F1, F2 and F3ex: data from ex vivo mucoadhesion studies.
Figure 4.
In vitro and ex vivo porcine buccal mucoadhesion time profiles of fluconazole films at 37 ͦC; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC (in vitro mucoadhesion time values); F1, F2 and F3ex: data from ex vivo mucoadhesion studies.

Figure 5.
Fluconazole flux through simulant buccal mucosa over 6 h; release medium: pH 6.8; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.
Figure 5.
Fluconazole flux through simulant buccal mucosa over 6 h; release medium: pH 6.8; Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.


Table 1.
Composition of fluconazole containing buccal films.
| Films | SA (%) | MC (%) | GLY (%) | PG (%) | FLU (mg/cm2) |
|---|---|---|---|---|---|
| AF1 | 1 | 1.8 | 10 | - | 5 |
| BF1 | 1 | 1.6 | 10 | - | 5 |
| F1 | 1 | 1.6 | - | 10 | 5 |
| AF2 | 1.3 | 1.8 | 10 | - | 5 |
| BF2 | 1.3 | 1.6 | 10 | - | 5 |
| F2 | 1.3 | 1.6 | - | 10 | 5 |
| AF3 | 1.6 | 1.8 | 10 | - | 5 |
| BF3 | 1.6 | 1.6 | 10 | - | 5 |
| F3 | 1.6 | 1.6 | - | 10 | 5 |
Key: SA : sodium alginate ; MC : methylcellulose ; GLY : glycerol ; PG : propylene glycol ; FLU : fluconazole ; AF1, AF2, AF3 (Viscous film forming solutions), BF1, BF2, BF3 (sticky, unstable films) ; F1=SA1%/MC1.6%; F2= SA1.3%/MC1.6%, F3 = SA1.6%/MC1.6% (optimised films).
Table 2.
Physicomechanical properties of fluconazole films.
| Samples | Weight (g) | Thickness (mm) | Folding Endurance |
Surface pH | Disintegration time in SSF (min) | Swelling index (%) |
|---|---|---|---|---|---|---|
| F1 | 0.10±0.01 | 0.09±0.01 | > 500 | 7.61±0.03 | 5 | 57±7 |
| F2 | 0.11±0.01 | 0.08±0.01 | > 500 | 7.18±0.03 | 10 | 68±2 |
| F3 | 0.12±0.01 | 0.09±0.01 | > 500 | 7.13±0.05 | 35 | 70±1 |
Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC; SSF: simulant salivary fluid.
Table 3.
Percent Drug Content of fluconazole films; data presented as mean±SD; n = 3.
| Formulations | Drug Content (%) |
|---|---|
| F1 | 98.7±0.2 |
| F2 | 99.7±0.2 |
| F3 | 113.8±0.2 |
Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.
Table 4.
Drug release data for fluconazole films fitted to various drug kinetic models – Zero-order, First order, Higuchi and Korsmeyer-Peppas models.
Table 4.
Drug release data for fluconazole films fitted to various drug kinetic models – Zero-order, First order, Higuchi and Korsmeyer-Peppas models.
| Kinetic models | Zero | first | Higuchi | Korsmeyer-Peppas | |||||
|---|---|---|---|---|---|---|---|---|---|
| Sample | r2 | k1 | r2 | k2 | r2 | k3 | r2 | k4 | n-value |
| F1 | 0.928 | 9.8193 | 0.6674 | 1.0597 | 0.9796 | -28.295 | 0.9722 | 1.4492 | 3.3368 |
| F2 | 0.8986 | 20.211 | 0.7167 | 1.333 | 0.9689 | -10.707 | 0.981 | 1.5762 | 3.6292 |
| F3 | 0.8897 | 12.026 | 0.668 | 1.095 | 0.9639 | -14.211 | 0.9633 | 1.4216 | 3.2732 |
Table 5.
Zones of Inhibition (mm) against C. albicans for fluconazole solution and films; data presented as mean±SD; n = 3.
Table 5.
Zones of Inhibition (mm) against C. albicans for fluconazole solution and films; data presented as mean±SD; n = 3.
| Sample | Mean ± SD |
|---|---|
| Fluconazole solution | 42.3 ±0.5 |
| F1 | 39.7 ±0.5 |
| F2 | 40.2 ±0.2 |
| F3 | 39.7 ± 0.5 |
Key: F1: Fluconazole/1% SA/1.6% MC; F2: Fluconazole/1.3% SA/1.6% MC; F3: Fluconazole/1.6% SA/1.6% MC.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



