Submitted:
08 April 2026
Posted:
09 April 2026
You are already at the latest version
Abstract
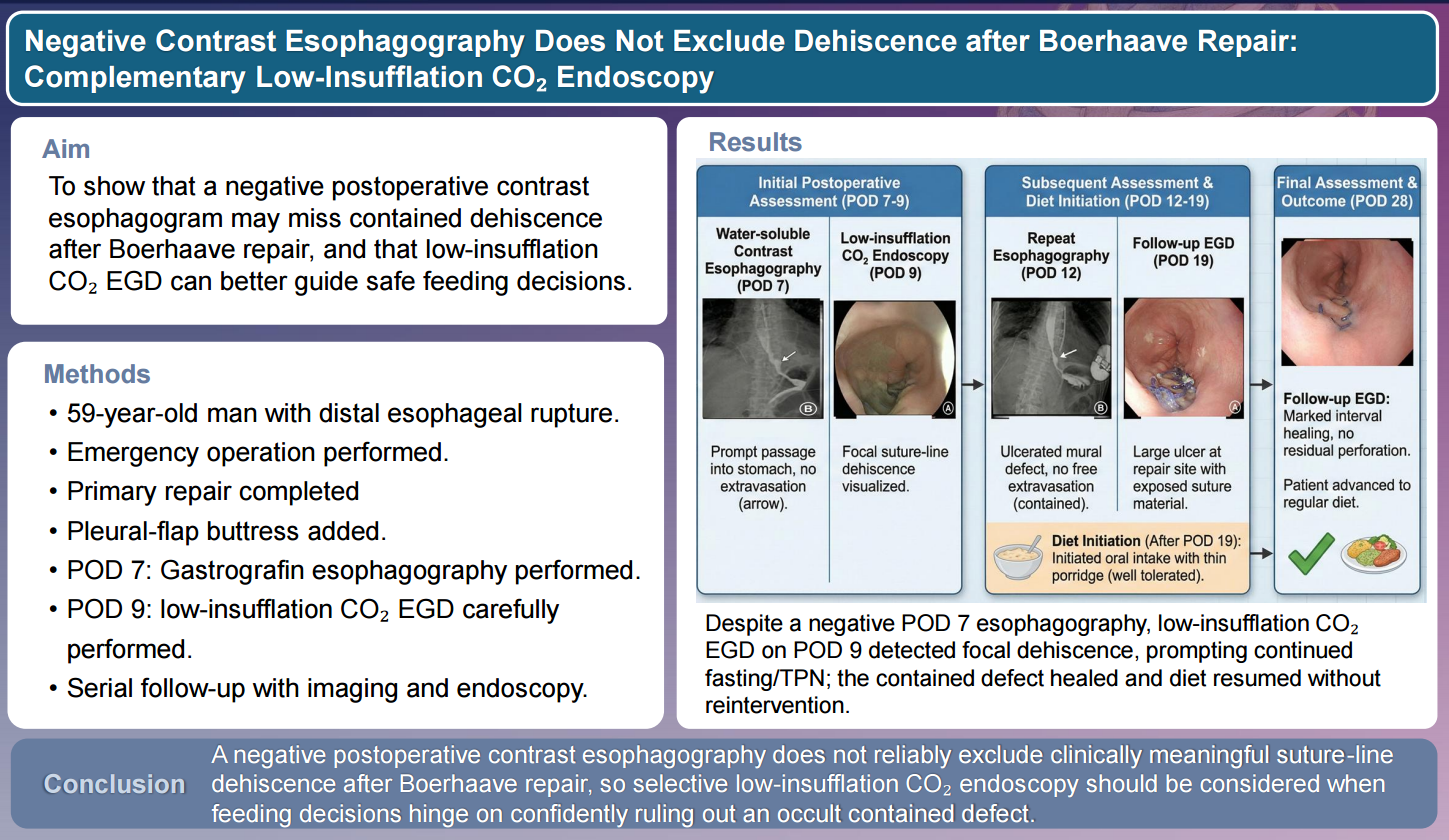
After repair of Boerhaave syndrome, assessment of repair integrity is important because occult dehiscence may progress to mediastinitis or pleural sepsis. Water-soluble contrast esophagography is commonly used before resuming oral intake, but absence of contrast extravasation does not necessarily exclude a small or contained defect. We report a 59-year-old man with post-emetic distal esophageal rupture who underwent emergency primary repair with pleural-flap buttress and drainage. Although he remained clinically stable, water-soluble contrast esophagography on postoperative day (POD) 7 showed no extravasation. Because feeding decisions required greater structural confidence, low-insufflation carbon dioxide (CO2) esophagogastroduodenoscopy (EGD) was performed on POD 9 and revealed focal suture-line dehiscence. Oral intake was deferred, and conservative management with fasting and total parenteral nutrition was continued. Serial reassessment suggested a contained defect, and oral intake was reintroduced cautiously. A regular diet was started only after POD 28 endoscopy showed marked interval healing, and follow-up endoscopy at 3 months confirmed complete mucosal healing. This case highlights that negative postoperative contrast esophagography does not exclude persistent dehiscence and that low-insufflation CO2 endoscopy may provide useful complementary structural information in selected patients.
Keywords:
Boerhaave syndrome
; esophageal perforation
; contrast esophagography
; endoscopy
; carbon dioxide
; dehiscence
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



