
Submitted:
02 March 2026
Posted:
03 March 2026
You are already at the latest version
Abstract
Background: Childhood obesity has become a major global health concern and is increasingly recognized as a factor influencing skeletal development. Emerging evidence suggests that excess adiposity may alter craniofacial growth patterns, potentially affecting orthodontic diagnosis, treatment planning, and airway function. However, the extent to which obesity influences craniofacial morphology in growing individuals remains incompletely understood. Objective: To evaluate the relationship between body mass index (BMI) and craniofacial morphology in children and adolescents using selected sagittal and linear craniofacial parameters, and to determine the independent effects of age and sex on these associations. Methods: This cross-sectional orthodontic study included 130 healthy subjects aged 19 or younger. Anthropometric measurements were recorded, and BMI was calculated to classify participants into normal weight, overweight, and obese groups. Standardized lateral cephalometric radiographs were obtained, and twenty-one skeletal and soft-tissue parameters were analyzed. Statistical evaluation included tests of normality, one-way ANOVA, and post-hoc comparisons to assess differences according to BMI, sex, and age groups. Results: Obesity was significantly associated with increased sagittal skeletal dimensions. Mandibular body length, mandibular unit length, SNB angle, and maxillary unit length demonstrated progressive increases across BMI categories (p < 0.05). In contrast, vertical growth parameters showed no significant differences. Soft-tissue analysis revealed reduced facial convexity and lower facial height ratios in obese subjects. Age was strongly associated with increases in linear jaw dimensions, whereas sex differences were limited primarily to skeletal size rather than morphological relationships. Conclusions: Childhood obesity is associated with enhanced sagittal craniofacial growth, particularly involving mandibular structures, while vertical skeletal patterns remain largely unaffected. These findings highlight the importance of incorporating BMI assessment into orthodontic evaluation and suggest that obesity may influence growth timing, facial morphology, and airway-related risk factors.
Keywords:
orthodontics
; childhood obesity
; body mass index
; cephalometry
; craniofacial growth
; mandibular development
; skeletal maturation
Introduction
Childhood obesity has become one of the most significant global public health challenges, with its prevalence increasing substantially over the past several decades [1]. Data from the National Health and Nutrition Examination Survey (NHANES) indicate that prevalence rose from approximately 5% in the 1960s to 10–12% during 1988–1994, reaching nearly 16% by the early 2000s [2]. This upward trend is accompanied by pronounced ethnic and socioeconomic disparities. For example, a large survey among primary school children in New York City reported that approximately 41% were overweight and 22% obese, with higher rates observed among Hispanic and African-American populations compared to Caucasian and Asian groups [3].
The etiology of childhood obesity is complex and multifactorial. Genetic predisposition, particularly variations affecting leptin metabolism and appetite regulation, plays an important role [4,5]. However, environmental and behavioral factors remain major contributors [6]. Sedentary lifestyles, especially prolonged screen exposure, reduce physical activity while simultaneously increasing exposure to advertising for energy-dense foods, thereby promoting excessive caloric intake [2]. Dietary patterns have also shifted toward increased consumption of refined carbohydrates, sugar-sweetened beverages, and high-glycemic foods, contributing to metabolic imbalance and fat accumulation. Psychosocial determinants such as chronic stress, family instability, depression, and low socioeconomic status further increase obesity risk, while parental obesity strongly predicts childhood obesity [2,3].
Childhood obesity is associated with numerous systemic and psychosocial complications. Cardiometabolic consequences include hypertension, dyslipidemia, insulin resistance, and type II diabetes, with approximately 80–85% of pediatric diabetes cases occurring in overweight or obese children [4,5]. Other associated conditions include polycystic ovarian syndrome, fatty liver disease, gallstones, orthopedic abnormalities such as Blount’s disease, asthma, and obstructive sleep apnea related to airway narrowing and craniofacial anatomical factors [6,7]. Beyond physical morbidity, obese children frequently experience reduced self-esteem, social stigmatization, and long-term socioeconomic disadvantages [8].
In recent years, increasing attention has been directed toward the potential relationship between obesity and craniofacial development. Orthodontic research suggests that obesity is associated with measurable differences in craniofacial morphology that may influence airway dimensions and susceptibility to obstructive sleep apnea [9]. Cephalometric studies report that obese individuals often exhibit longer cranial bases, reduced ANB angles, and more anterior mandibular positioning compared with normal-weight peers, indicating a tendency toward altered sagittal skeletal relationships [9,10]. Three-dimensional soft-tissue analyses further demonstrate increased facial widths, larger mandibular dimensions, and deeper facial profiles in obese adolescents, with similar tendencies observed even in mildly overweight individuals [10].
Additional evidence indicates that obesity may be associated with craniofacial development through endocrine pathways, including alterations in growth hormone activity. Cephalometric investigations have reported increased linear measurements of the mandible, maxilla, and anterior cranial base in obese subjects, with the most pronounced differences involving mandibular length [9,10,11]. These findings support the concept that obese children may exhibit differences in skeletal growth timing and maturation patterns during development [9,10,11].
Beyond systemic health implications, childhood obesity has important relevance for orthodontic diagnosis and treatment planning [9,10,11,12]. Because orthodontic patients are typically evaluated during active growth periods, variations in skeletal maturation can substantially influence diagnostic interpretation, treatment timing, and therapeutic outcomes [13]. Obesity-related differences in craniofacial growth may affect sagittal jaw relationships, facial profile harmony, and airway morphology, thereby increasing susceptibility to sleep-disordered breathing [6,7,14].
Despite growing interest in this field, the association between excess body weight and craniofacial morphology remains incompletely understood. Existing studies are often limited by small sample sizes, methodological heterogeneity, and inconsistent evaluation of both skeletal and soft-tissue structures [9]. These limitations highlight the need for integrated investigations combining anthropometric assessment with cephalometric analysis to clarify the extent to which obesity is associated with craniofacial growth patterns [15].
2. Materials and Methods
2.1. Study Design and Ethical Approval
This cross-sectional observational study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of the participating university hospital (Approval No. 2709/27.12.2023). Written informed consent was obtained from all participants and their parents or legal guardians before inclusion.
2.2. Study Population and Sample Selection
The study sample consisted of 130 consecutively recruited subjects aged between 4 and 19 years who presented for orthodontic evaluation at a university orthodontic department over six months.
Inclusion criteria were:
- -
- Age ≤ 19 years at the time of examination
- -
- Absence of craniofacial syndromes or congenital anomalies
- -
- No history of previous orthodontic treatment
- -
- Availability of high-quality standardized lateral cephalometric radiographs
Exclusion criteria included:
- -
- Systemic conditions known to affect growth or bone metabolism
- -
- History of craniofacial trauma or surgery
- -
- Radiographs with positioning errors or insufficient diagnostic quality
Because participants were recruited from an orthodontic population, the sample represents individuals seeking orthodontic care rather than the general pediatric population.
2.3. Anthropometric Assessment and BMI Classification
Body weight was measured to the nearest 0.1 kg using a calibrated digital scale, and height was measured to the nearest 0.1 cm using a stadiometer under standardized conditions. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2).
Participants were categorized according to World Health Organization (WHO) BMI-for-age percentile standards:
- -
- Normal weight: BMI between the 5th and 85th percentile
- -
- Overweight: BMI between the 85th and 95th percentile
- -
- Obesity: BMI ≥ 95th percentile
BMI percentiles were calculated using WHO AnthroPlus software based on the WHO 2007 growth reference [16].
2.4. Cephalometric Imaging and Analysis
Standardized lateral cephalometric radiographs were obtained using the same digital cephalometric unit under identical exposure parameters. All images were acquired with subjects positioned in natural head posture, teeth in centric occlusion, and lips at rest.
Cephalometric tracing and measurements were performed using Dolphin Imaging software (Version 11.95, Dolphin Imaging & Management Solutions, Chatsworth, CA, USA) by a single calibrated examiner under standardized conditions.
The following skeletal and soft-tissue variables were analyzed:
Sagittal skeletal parameters
- -
- SNA angle (°)
- -
- SNB angle (°)
- -
- ANB angle (°)
Linear skeletal measurements
- -
- Maxillary unit length (mm)
- -
- Mandibular unit length (mm)
- -
- Mandibular body length (mm)
Soft-tissue parameters
- -
- Facial convexity angle (°)
- -
- Lower-to-total facial height ratio (%)
2.5. Measurement Reliability
To assess intra-observer reliability, 20 randomly selected radiographs were retraced after a two-week interval. Intraclass correlation coefficients (ICCs) ranged from 0.92 to 0.97, indicating excellent measurement reproducibility.
2.6. Age Stratification and Growth Phase Classification
Participants were stratified into four age groups representing biologically relevant developmental stages:
- -
- 4.0–10.9 years: prepubertal growth phase
- -
- 11.0–12.9 years: pubertal onset phase
- -
- 13.0–14.9 years: peak pubertal growth phase
- -
- 15.0–19.9 years: post-pubertal maturation phase
This classification was based on established associations between chronological age ranges and cervical vertebral maturation (CVM) stages described in orthodontic growth studies [17,18].
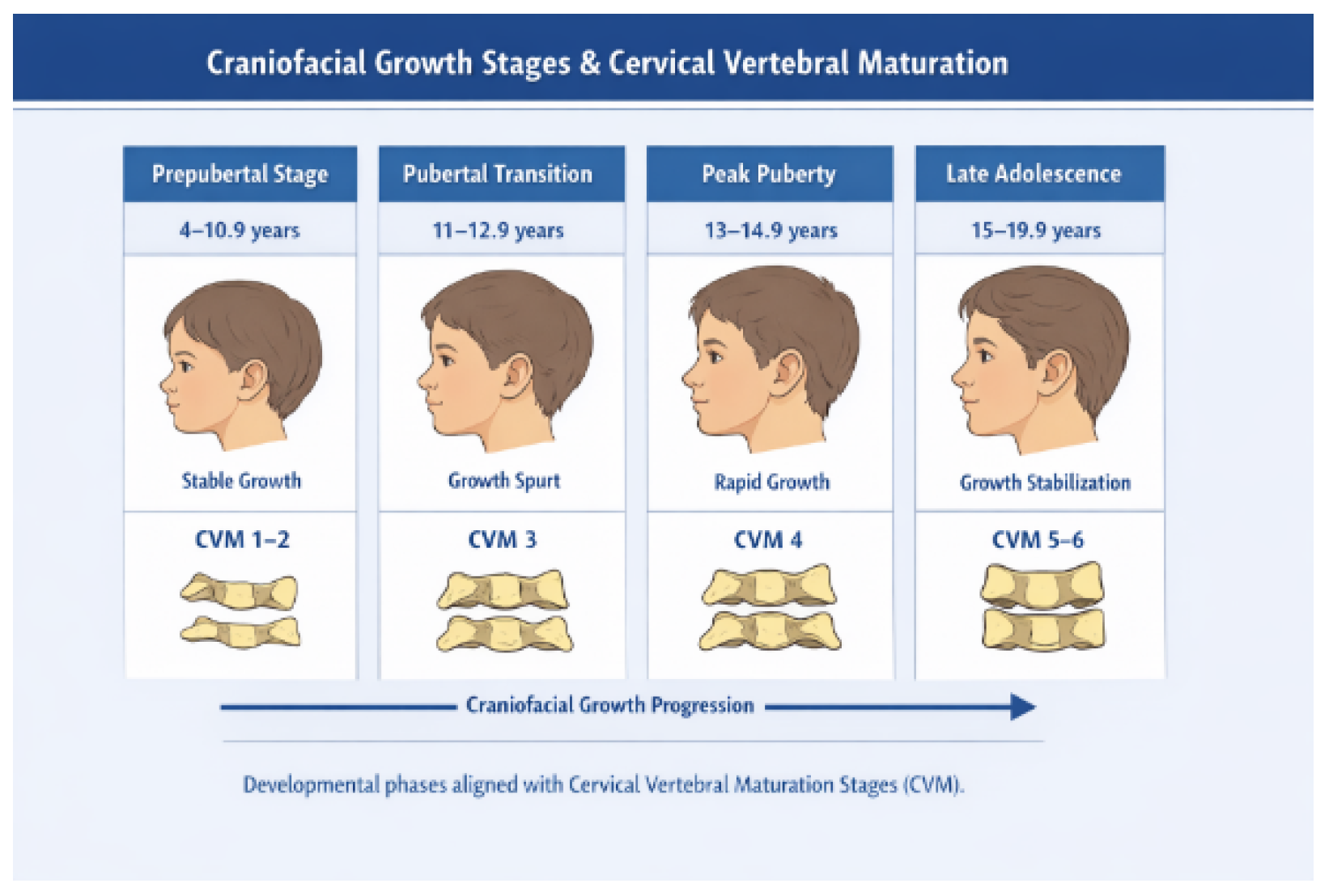
Age stratification was designed to reflect biologically relevant skeletal maturation stages based on established cervical vertebral maturation (CVM) protocols. Chronological age ranges were selected to approximate the developmental phases corresponding to CVM stages described by Baccetti, Franchi, and McNamara [17,18], thereby enabling biologically meaningful evaluation of obesity-related craniofacial growth differences. The youngest group (4.0–10.9 years) predominantly represented prepubertal development (CVM stages 1–2), characterized by relatively stable craniofacial growth rates. The 11.0–12.9-year group corresponded to the onset of the pubertal growth spurt (CVM stage 3), during which acceleration of mandibular growth typically begins. Participants aged 13.0–14.9 years reflected the peak pubertal growth phase (CVM stage 4), associated with maximum mandibular elongation and pronounced sagittal skeletal changes. The oldest group (15.0–19.9 years) represented post-pubertal maturation stages (CVM stages 5–6), during which craniofacial growth progressively stabilizes as skeletal development approaches completion [17,18].
This classification allowed the present study to evaluate obesity-related craniofacial differences in relation to biologically meaningful growth phases rather than relying solely on chronological age, thereby improving the interpretability and orthodontic relevance of the findings.
Figure 1.
Developmental phases aligned with Cervical Vertebrae Maturation CVM.
2.7. Statistical Analysis
Statistical analysis was performed using SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA).
The analytical workflow included:
- Normality assessment using the Shapiro–Wilk test
- Descriptive statistics reported as mean ± standard deviation
- One-way ANOVA to evaluate differences among BMI groups
- Tukey post-hoc testing for pairwise comparisons
- Independent t-tests to assess sex differences
- Two-way ANOVA to examine independent effects of age and BMI
- Multivariate linear regression analysis to determine independent predictors of craniofacial parameters after adjustment for age and sex. Ninety-five percent confidence intervals were calculated for all regression coefficients.
Effect sizes were evaluated using partial eta squared (η2) for ANOVA models.
Statistical significance was set at: p < 0.05
2.8. Sample Size Considerations
Based on post-hoc power analysis, the sample size provided >80% statistical power to detect moderate effect sizes at α = 0.05.
3. Results
3.1. Sample Characteristics
The study included 130 participants, of whom 73% were classified as normal weight, 14% overweight, and 13% obese. Females represented a slightly larger proportion of the sample. The largest age group corresponded to early-to-mid adolescence (Table 1).
Most participants were of normal weight (73%), with a slightly higher female representation. The largest proportion belonged to early-to-mid adolescence.
3.2. Data Distribution
All cephalometric variables demonstrated normal distribution according to the Shapiro–Wilk test, allowing the use of parametric statistical methods (Table 2).
All primary variables demonstrated normal distribution, allowing parametric statistical testing.
3.3. Craniofacial Differences According to BMI
Significant associations were observed between BMI and sagittal craniofacial dimensions (Table 3). Mandibular unit length, mandibular body length, SNB angle, and maxillary unit length progressively increased across BMI categories (p < 0.05).
In contrast, vertical skeletal parameters did not differ significantly among BMI groups.
Soft-tissue analysis demonstrated reduced facial convexity and lower facial height ratios in obese subjects, indicating a tendency toward a less convex facial profile.
3.4. Sex-Related Differences
Male participants exhibited significantly larger linear skeletal dimensions, including anterior cranial base length, maxillary unit length, and mandibular unit length (p < 0.01). However, no significant sex differences were observed in angular skeletal relationships or soft-tissue parameters.
3.5. Age-Related Craniofacial Changes
Age was strongly associated with increases in maxillary and mandibular linear dimensions. The most pronounced growth occurred between the prepubertal and early pubertal groups, corresponding to the onset of accelerated skeletal development.
Smaller increments were observed during later adolescence, indicating stabilization of craniofacial growth as skeletal maturity approached.
Table 3 shows clearly: progressive mandibular dominance with BMI, reduced ANB in obesity, thus sagittal prognathic tendency, increased skeletal linear dimensions, decreased facial convexity, and reduced vertical proportional balance
The results demonstrate that BMI is primarily correlated with sagittal craniofacial development, especially mandibular growth and positioning, while vertical skeletal relationships remain largely unaffected. Age mainly impacts linear skeletal growth, and sexual dimorphism is predominantly related to skeletal size rather than morphology.
3.6. Age–BMI Interaction Results
Two-way ANOVA analysis demonstrated significant independent effects of both age and BMI on craniofacial morphology (Table 4). Age exerted a strong influence on linear skeletal parameters, with progressive increases observed in maxillary and mandibular dimensions across developmental stages. The most pronounced growth occurred between the prepubertal and early pubertal groups, followed by smaller increments and near stabilization in late adolescence.
BMI showed a significant independent association primarily with sagittal skeletal relationships. Higher BMI values were correlated with increased SNB angle, greater mandibular body and unit lengths, and reduced facial convexity, indicating a tendency toward enhanced mandibular prognathism in overweight and obese subjects. Vertical proportional relationships remained relatively stable, although facial height ratio demonstrated modest reductions in older and higher-BMI groups.
No significant interaction effect between age and BMI was identified, suggesting that obesity primarily amplifies normal growth patterns rather than altering their developmental timing.
A significant difference was observed among BMI groups for mandibular length (F = 8.45, p < 0.001, η2 = 0.12), indicating a moderate effect size.
3.7. Multivariate Regression Analysis
Multivariate regression analysis confirmed that BMI independently predicted several craniofacial parameters after adjustment for age and sex.
Higher BMI was significantly associated with increased mandibular prognathism, reflected by greater SNB angle and mandibular unit length, as well as reduced ANB angle and facial convexity.
Age remained the strongest determinant of linear skeletal growth, while sex showed a moderate influence primarily related to skeletal size.

Table 5.
Multivariate Linear Regression Analysis of Factors Influencing Craniofacial Parameters.
| Dependent Variable | Predictor | β Coefficient | Standard Error | p Value |
|---|---|---|---|---|
| SNB (°) | BMI | 0.18 | 0.05 | <0.001 |
| Age | 0.22 | 0.04 | <0.001 | |
| Sex (Male) | 0.09 | 0.03 | 0.014 | |
| Mandibular unit length (mm) | BMI | 0.36 | 0.07 | <0.001 |
| Age | 0.48 | 0.06 | <0.001 | |
| Sex (Male) | 0.21 | 0.05 | 0.002 | |
| ANB (°) | BMI | −0.14 | 0.04 | 0.001 |
| Age | −0.09 | 0.03 | 0.019 | |
| Sex (Male) | −0.05 | 0.02 | 0.087 | |
| Facial convexity angle (°) | BMI | −0.31 | 0.06 | <0.001 |
| Age | −0.28 | 0.05 | <0.001 | |
| Sex (Male) | −0.07 | 0.03 | 0.041 |
All regression models demonstrated good explanatory power, with adjusted R2 values ranging from 0.41 to 0.63. Regression coefficients are presented with 95% confidence intervals.
Discussion
The present study provides evidence that childhood obesity is associated with measurable differences in craniofacial morphology, primarily involving sagittal skeletal dimensions [9,12]. The findings demonstrate a consistent pattern of increased mandibular and maxillary linear measurements in overweight and obese subjects, accompanied by progressive increases in SNB angle and reductions in soft-tissue convexity [10]. These results collectively suggest a tendency toward greater mandibular prominence and altered sagittal facial relationships in children with elevated body mass index [10,12,19]. Importantly, vertical skeletal parameters remained largely unchanged, indicating that obesity appears to be selectively associated with anteroposterior craniofacial growth rather than vertical facial development. These observations differ from some previous reports suggesting proportionally increased anteroposterior and vertical craniofacial dimensions in overweight children and adolescents [20].
Obesity-related craniofacial differences were most evident during the pubertal growth phase, suggesting a possible interaction between metabolic status and periods of accelerated skeletal maturation [9,21].
The enlargement of mandibular dimensions represented the most pronounced morphological change identified in this investigation. Mandibular unit length showed the strongest association with BMI, displaying a progressive increase across weight categories. This pattern supports the hypothesis that increased adiposity may be associated with enhanced skeletal growth activity during critical developmental periods [22]. The mandibular condyle, as a major site of endochondral growth, is known to be responsive to systemic metabolic and hormonal influences, and increased growth activity in obese individuals may reflect altered endocrine regulation [23]. Previous studies suggest that hyperinsulinemia and elevated insulin-like growth factor-1 levels, commonly observed in obese children, have been proposed to stimulate chondrocyte proliferation and matrix deposition within condylar cartilage, thereby contributing to increased mandibular growth [24,25]. In addition, leptin and other adipokines secreted by adipose tissue may further modulate bone metabolism and growth plate activity, potentially influencing skeletal enlargement in this population [26,27].
The observed increase in maxillary length in obese subjects, although less pronounced than mandibular changes, indicates that obesity may be associated with broader craniofacial skeletal development rather than isolated mandibular growth alone [9,28]. However, the predominance of mandibular differences suggests a differential sensitivity of craniofacial structures to metabolic and hormonal influences, with the mandible appearing particularly responsive to obesity-related growth variations [29]. This observation is consistent with previous cephalometric and three-dimensional imaging studies reporting larger mandibular dimensions and more prognathic skeletal profiles in overweight adolescents [9,10].
In contrast to sagittal findings, vertical craniofacial parameters did not demonstrate significant differences across BMI groups. This suggests that obesity may not substantially modify vertical growth patterns or facial divergence, reinforcing the concept that the primary craniofacial associations of increased adiposity relate to forward skeletal growth rather than vertical rotational changes [9,30]. The relative stability of vertical measurements across BMI categories also supports the view that intrinsic growth direction is largely genetically determined and less susceptible to metabolic influences [31,32].
Soft-tissue analysis revealed a reduction in facial convexity and lower facial height ratios among obese subjects. These changes likely reflect both underlying skeletal differences and increased soft-tissue thickness associated with adipose deposition [33,34]. The reduction in convexity has clinical relevance, as it may mask or exaggerate underlying skeletal discrepancies, potentially complicating orthodontic diagnosis [35]. Furthermore, altered soft-tissue profiles in obese individuals may contribute to reduced upper airway dimensions and increased susceptibility to obstructive sleep apnea [36]. The interaction between craniofacial morphology and airway patency represents an important interdisciplinary consideration in pediatric orthodontic assessment [36,37].
Age stratification according to biologically defined growth phases represents a methodological strength of this study. By grouping participants according to prepubertal, pubertal transition, peak growth, and late maturation stages, the analysis accounts for known variations in craniofacial growth velocity, particularly mandibular development, thereby reducing age-related confounding and improving the interpretability of BMI-related skeletal associations [38,39].
Sex-related differences observed in this study were limited to linear skeletal dimensions, with males demonstrating larger cranial base and jaw lengths compared to females. These findings are consistent with established patterns of sexual dimorphism in craniofacial growth and reflect overall differences in skeletal size rather than morphological pattern [40]. The absence of significant differences in angular and soft-tissue parameters suggests that obesity-related craniofacial variations occur similarly in both sexes [9,40].
Age-related analysis revealed expected progressive increases in maxillary and mandibular lengths throughout childhood and adolescence, with the most pronounced growth occurring during early developmental stages [17,18]. The attenuation of differences in late adolescence suggests that skeletal maturation eventually reduces variability in craniofacial dimensions, supporting previous observations that obesity may be associated with earlier attainment of peak growth velocity without necessarily altering final adult morphology [10,29].
From a clinical perspective, these findings underscore the importance of incorporating anthropometric assessment into orthodontic diagnostic protocols [41]. Failure to consider BMI may lead to misinterpretation of skeletal relationships, particularly in cases presenting with apparent mandibular prognathism [19,23,25,28]. Moreover, differences in growth patterns among obese patients may influence the timing and effectiveness of orthopedic treatment interventions, highlighting the need for individualized treatment planning.
Despite its strengths, including standardized radiographic methodology, selected craniofacial parameters, and high measurement reliability, this study has several limitations. The cross-sectional design precludes evaluation of longitudinal growth trajectories and does not allow causal inference. Additionally, BMI does not reflect fat distribution patterns or metabolic status, which may differentially influence skeletal growth [27,32]. Future longitudinal investigations incorporating hormonal assessments and advanced three-dimensional imaging are needed to further clarify the biological mechanisms underlying obesity-related craniofacial differences. Unmeasured confounders such as pubertal status, endocrine variations, and breathing patterns may have influenced craniofacial morphology, and the orthodontic sample limits generalizability to the broader pediatric population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Sorana Maria Bucur; Methodology, Sorana Maria Bucur; Software, Dorin Ioan Cocoș; Validation, Cristian Olteanu and Eugen Bud; Formal analysis, Mioara Decusară; Investigation, Dorin Ioan Cocoș, Cristian Olteanu and Mariana Păcurar; Resources, Cristian Olteanu and Mariana Păcurar; Data curation, Dorin Ioan Cocoș; Writing—original draft, Sorana Maria Bucur; Writing—review & editing, Sorana Maria Bucur; Visualization, Mioara Decusară and Eugen Bud; Supervision, Eugen Bud. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This cross-sectional observational study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of the participating university hospital (Approval No. 2709/27.12.2023).
Informed Consent Statement
Written informed consent was obtained from all participants and their parents or legal guardians before inclusion.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author(s).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: Public-health crisis, common-sense cure. Lancet 2002, 360, 473–479. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Secular trends in regional differences in nutritional biomarkers and self-reported dietary intakes among American adults: National Health and Nutrition Examination Survey (NHANES) 1988–1994 to 2009–2010. Public Health Nutr. 2018, 21, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, L.E.; List, D.G.; Marx, T.; May, L.; Helgerson, S.D.; Frieden, T.R. Childhood obesity in New York City elementary school students. Am. J. Public Health 2004, 94, 1496–1500. [Google Scholar] [CrossRef] [PubMed]
- Vourdoumpa, A.; Paltoglou, G.; Charmandari, E. The genetic basis of childhood obesity: A systematic review. Nutrients 2023, 15, 1416. [Google Scholar] [CrossRef]
- Verma, M.; Kapoor, N.; Senapati, S.; Singh, O.; Bhadoria, A.S.; Khetarpal, P.; Kumar, S.; Bansal, K.; Ranjan, R.; Kakkar, R.; et al. Comprehending the epidemiology and aetiology of childhood obesity: Integrating life course approaches for prevention and intervention. Diabetes Ther. 2025, 16, 1177–1206. [Google Scholar] [CrossRef]
- Narang, I.; Mathew, J.L. Childhood obesity and obstructive sleep apnea. J. Nutr. Metab. 2012, 2012, 134202. [Google Scholar] [CrossRef] [PubMed]
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in children and adolescents: Epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Harrist, A.W.; Swindle, T.M.; Hubbs-Tait, L.; Topham, G.L.; Shriver, L.H.; Page, M.C. The social and emotional lives of overweight, obese, and severely obese children. Child Dev. 2016, 87, 1564–1580. [Google Scholar] [CrossRef]
- Verdecchia, A.; Suárez-Fernández, C.; Menéndez Diaz, I.; Sanz, V.G.; Spinas, E.; Cobo, T. Obesity and overweight conditions in children and adolescents (6–18 years) and their impact on craniofacial morphology: A systematic review. Children 2025, 12, 377. [Google Scholar] [CrossRef]
- Hancock, S.; Carmack, A.; Kocher, M.; Rezende Silva, E.; Sulkowski, T.; Nanney, E.; Graves, C.; Mitchell, K.; Jacox, L.A. Influence of BMI percentile on craniofacial morphology and development in adolescents. Part II: Elevated BMI is associated with larger final facial dimensions. Eur. J. Orthod. 2024, 46, cjad043. [Google Scholar] [CrossRef]
- Lee, R.W.; Vasudavan, S.; Hui, D.S.; Prvan, T.; Petocz, P.; Darendeliler, M.A.; Cistulli, P.A. Differences in craniofacial structures and obesity in Caucasian and Chinese patients with obstructive sleep apnea. Sleep 2010, 33, 1075–1080. [Google Scholar] [CrossRef]
- Gibas-Stanek, M.; Bilińska, M.; Kaminkova, P.; Direr, P.; Fudalej, P.S. Influence of body mass index on facial soft tissue morphology in growing non-obese children. Eur. J. Orthod. 2025, 47, cjaf069. [Google Scholar] [CrossRef]
- Tentaş, S.; Özden, S. Deep learning-based evaluation of skeletal maturation: A comparative analysis of five hand-wrist methods. Orthod. Craniofac. Res. 2025, 28, 943–954. [Google Scholar] [CrossRef]
- Nokes, B.; Schueler, A.; Darquenne, C.; Schmickl, C.N.; Wojeck, B.S.; Moore, S.; Deyoung, P.; McGinnis, L.; Theilmann, R.J.; Gruenberg, E.; et al. The impact of obesity on upper airway anatomy as assessed by magnetic resonance imaging and obstructive sleep apnea endotypic traits. Front. Physiol. 2025, 16, 1648767. [Google Scholar] [CrossRef]
- Al-Jewair, T.; Marwah, S.; Preston, C.B.; Wu, Y.; Yu, G. Correlation between craniofacial structures, anthropometric measurements, and nasopharyngeal dimensions in black adolescents. Int. Orthod. 2021, 19, 96–106. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baccetti, T.; Franchi, L.; McNamara, J.A. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin. Orthod. 2005, 11, 119–129. [Google Scholar] [CrossRef]
- McNamara, J.A., Jr.; Franchi, L. The cervical vertebral maturation method: A user’s guide. Angle Orthod. 2018, 88, 133–143. [Google Scholar] [CrossRef]
- Alfaro, J.M.; Manrique, R.; Santamaría, A.; Álvarez, E.; Manes, C.; Jiménez, M. Effects of endocrine disorders on maxillary and mandibular growth in Colombian children and adolescents: A cross-sectional study. Eur. Arch. Paediatr. Dent. 2024, 25, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Danze, A.; Jacox, L.A.; Bocklage, C.; Whitley, J.; Moss, K.; Hardigan, P.; Garcia-Godoy, C.E.; Jackson, T.H. Influence of BMI percentile on craniofacial morphology and development in children and adolescents. Eur. J. Orthod. 2021, 43, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, A.; Torre, I.C.; Diaz, I.M.; Sanz, V.G.; Mesa, Y.G.; Cobo, T.; Gallardo, V.P. Analysis of the relationship between body mass index (BMI) and dento-skeletal maturation: A cross-sectional case-control study. Dent. J. 2025, 13, 8. [Google Scholar] [CrossRef]
- Ke, D.; Lu, D.; Cai, G.; Zhang, J.; Wang, X.; Suzuki, K. Accelerated skeletal maturation is associated with overweight and obesity as early as preschool age: A cross-sectional study. BMC Pediatr. 2020, 20, 452. [Google Scholar] [CrossRef]
- Tsutsumi-Arai, C.; Tran, A.; Arai, Y.; Ono, W.; Ono, N. Mandibular condylar cartilage in development and diseases: A PTHrP-centric view. Orthod. Craniofac. Res. 2025, 28, S70–S80. [Google Scholar] [CrossRef]
- Chen, Y.; Ke, J.; Long, X.; Meng, Q.; Deng, M.; Fang, W.; Li, J.; Cai, H.; Chen, S. Insulin-like growth factor-1 boosts the developing process of condylar hyperplasia by stimulating chondrocyte proliferation. Osteoarthr. Cartil. 2012, 20, 279–287. [Google Scholar] [CrossRef]
- Joshi, A.S.; Hatch, N.E.; Hayami, T.; Jheon, A.; Kapila, S. IGF-1 TMJ injections enhance mandibular growth and bone quality in juvenile rats. Orthod. Craniofac. Res. 2022, 25, 183–191. [Google Scholar] [CrossRef]
- Francisco, V.; Pino, J.; Gonzalez-Gay, M.A.; Mera, A.; Lago, F.; Gómez, R.; Mobasheri, A.; Gualillo, O. Adipokines and inflammation: Is it a question of weight? Br. J. Pharmacol. 2018, 175, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.X.; Yang, T. Roles of leptin in bone metabolism and bone diseases. J. Bone Miner. Metab. 2015, 33, 474–485. [Google Scholar] [CrossRef]
- Alfaro, J.M.; Manrique, R.; Santamaría, A.; Álvarez, E.; Manes, C.; Jiménez, M. Effects of endocrine disorders on maxillary and mandibular growth in Colombian children and adolescents: A cross-sectional study. Eur. Arch. Paediatr. Dent. 2024, 25, 17–25. [Google Scholar] [CrossRef]
- Gordon, L.A.; Miller, S.F.; Caplin, J.; Galang-Boquiren, M.T.; Alrayyes, S.; Nicholas, C.L. Childhood obesity may accelerate timing of human facial growth. Arch. Oral Biol. 2021, 121, 104964. [Google Scholar] [CrossRef] [PubMed]
- Vora, S.R.; Tam, S.; Katsube, M.; Pliska, B.; Heda, K. Craniofacial form differences between obese and nonobese children. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 744–752.e3. [Google Scholar] [CrossRef] [PubMed]
- Boulan, L.; Milán, M.; Léopold, P. The Systemic Control of Growth. Cold Spring Harb. Perspect. Biol. 2015, 7, a019117. [Google Scholar] [CrossRef]
- Arnott, S.A.; Chiba, S.; Conover, D.O. Evolution of intrinsic growth rate: Metabolic costs drive trade-offs between growth and swimming performance in Menidia menidia. Evolution 2006, 60, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Jiang, W.; Yao, K.; Sun, H.; Lu, X.; Yu, W. Craniofacial, Dental, and Upper Airway Morphologic features of Severely Obese Adults with Obstructive Sleep Apnea. Int. Dent. J. 2025, 75, 1736–1744. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Camastra, S.; Vitali, A.; Anselmino, M.; Gastaldelli, A.; Bellini, R.; Berta, R.; Severi, I.; Baldi, S.; Astiarraga, B.; Barbatelli, G.; et al. Muscle and adipose tissue morphology, insulin sensitivity and beta-cell function in diabetic and nondiabetic obese patients: Effects of bariatric surgery. Sci. Rep. 2017, 7, 9007. [Google Scholar] [CrossRef]
- Saloom, H.F.; Boustan, R.; Seehra, J.; Papageorgiou, S.N.; Carpenter, G.H.; Cobourne, M.T. The impact of obesity on orthodontic treatment outcome in adolescents: A prospective clinical cohort study. Eur. J. Orthod. 2021, 43, 165–172. [Google Scholar] [CrossRef]
- Voltan, C.; Concer, F.; Pecoraro, L.; Pietrobelli, A.; Piacentini, G.; Zaffanello, M. Exploring the Complex Interplay of Obesity, Allergic Diseases, and Sleep-Disordered Breathing in Children. Children 2024, 11, 595. [Google Scholar] [CrossRef]
- Huynh, N.; Zhang, J.; Pliska, B.; Amin, R.; Narang, I.; Chadha, N.; Cholette, M.C.; Kirk, V.; Montpetit, A.; Vezina, K.; et al. Prevalence of Altered Craniofacial Morphology in Children With OSA. J. Sleep Res. 2025, 34, e70060. [Google Scholar] [CrossRef]
- Nahhas, R.W.; Valiathan, M.; Sherwood, R.J. Variation in timing, duration, intensity, and direction of adolescent growth in the mandible, maxilla, and cranial base: The Fels longitudinal study. Anat. Rec. 2014, 297, 1195–1207. [Google Scholar] [CrossRef]
- Kim, N.-H.; Lee, J.-H.; Lee, S.; Choi, Y.J.; Chung, C.J.; Lee, K.-J.; Kim, K.-H. Growth Velocity and the Pubertal Growth Spurt Across Skeletal Maturity Stages in Class II Malocclusion: A Longitudinal Analysis. Children 2025, 12, 1612. [Google Scholar] [CrossRef] [PubMed]
- Gu, T.; Zhang, S.; Xiao, C.; Hu, S.; Xiong, X. Sex differences in craniofacial parameters of children and adolescents: A comparative study with the maturation of cervical vertebrae using a cephalometric method. J. Clin. Pediatr. Dent. 2024, 48, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Dudnik, O.V.; Mamedov, A.A.; Dybov, A.M.; Kharke, V.V.; Timoshenko, T.V.; Skakodub, A.A.; Maclennan, A.B.; Bille, D.S. Application of additional anthropometric and functional methods in children undergoing orthodontic treatment using braces. Saudi Dent. J. 2021, 33, 222–228. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Distribution of participants.
| Variable | Category | n |
|---|---|---|
| BMI | Normal Weight | 95 |
| Overweight | 18 | |
| Obese | 17 | |
| Sex | Male | 53 |
| Female | 77 | |
| Age group | 4–10.9 yrs | 26 |
| 11–12.9 yrs | 39 | |
| 13–14.9 yrs | 42 | |
| 15–19.9 yrs | 23 |
Table 2.
Shapiro–Wilk normality testing for key cephalometric variables.
| Parameter | W value | p Value | Distribution |
|---|---|---|---|
| SNA | 0.972 | 0.118 | Normal |
| SNB | 0.968 | 0.094 | Normal |
| ANB | 0.955 | 0.061 | Normal |
| Maxillary unit length | 0.979 | 0.164 | Normal |
| Mandibular unit length | 0.966 | 0.083 | Normal |
| Mandibular body length | 0.971 | 0.107 | Normal |
| Facial convexity angle | 0.963 | 0.072 | Normal |
| Facial height ratio | 0.976 | 0.149 | Normal |
Table 3.
Cephalometric parameters by BMI category.
| Parameter | Normal Weight | Overweight | Obese | p Value |
|---|---|---|---|---|
| SNA (°) | 82.4 ± 3.0 | 85.0 ± 3.3 | 84.1 ± 3.1 | 0.010 |
| SNB (°) | 79.2 ± 2.9 | 81.5 ± 3.0 | 82.4 ± 3.2 | 0.003 |
| ANB (°) | 3.2 ± 1.8 | 3.5 ± 1.7 | 1.7 ± 1.6 | 0.012 |
| Maxillary unit length (mm) | 97.0 ± 4.1 | 98.6 ± 4.4 | 100.1 ± 4.3 | 0.017 |
| Mandibular unit length (mm) | 123.0 ± 6.6 | 126.4 ± 7.0 | 129.6 ± 6.7 | 0.002 |
| Mandibular body length (mm) | 74.0 ± 5.1 | 76.5 ± 5.0 | 78.2 ± 5.3 | 0.013 |
| Facial convexity angle (°) | 15.3 ± 4.1 | 12.8 ± 3.8 | 10.1 ± 3.4 | 0.005 |
| Facial height ratio (%) | 95.4 ± 3.6 | 91.1 ± 4.0 | 87.2 ± 4.3 | 0.007 |
Table 4.
Influence of age and BMI on key craniofacial parameters.
| Parameter | 4–10.9 yrs | 11–12.9 yrs | 13–14.9 yrs | 15–19.9 yrs | Age Effect (p) | BMI Effect (p) |
|---|---|---|---|---|---|---|
| SNA (°) | 81.2 ± 2.9 | 82.5 ± 3.1 | 83.2 ± 3.3 | 83.6 ± 3.5 | 0.039 | 0.010 |
| SNB (°) | 77.8 ± 3.1 | 79.6 ± 3.2 | 80.9 ± 3.4 | 81.3 ± 3.6 | <0.001 | <0.001 |
| ANB (°) | 3.4 ± 1.9 | 2.9 ± 1.8 | 2.3 ± 1.7 | 2.1 ± 1.6 | 0.021 | 0.012 |
| Maxillary unit length (mm) | 93.5 ± 4.6 | 96.1 ± 4.4 | 98.0 ± 4.8 | 99.0 ± 5.1 | <0.001 | 0.017 |
| Mandibular unit length (mm) | 118.3 ± 6.2 | 123.5 ± 6.6 | 127.3 ± 7.1 | 129.0 ± 7.4 | <0.001 | <0.001 |
| Mandibular body length (mm) | 70.0 ± 4.2 | 73.5 ± 4.6 | 76.1 ± 5.0 | 76.9 ± 5.2 | <0.001 | 0.013 |
| Facial convexity angle (°) | 16.4 ± 4.6 | 14.2 ± 4.4 | 11.9 ± 4.2 | 11.0 ± 4.3 | <0.001 | 0.005 |
| Facial height ratio (%) | 96.6 ± 5.2 | 92.1 ± 4.9 | 89.3 ± 4.7 | 87.7 ± 4.5 | <0.001 | 0.007 |
Values expressed as mean ± SD. Two-way ANOVA tested the independent effects of age and BMI.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



