Submitted:
26 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
The security crisis in Burkina Faso has displaced over two million people, disproportionately affecting women and children, who are exposed to multiple forms of violence. This study assesses the resilience capacity of internally displaced women in the Boucle du Mouhoun region. A mixed-methods approach was employed with 1,056 participants, combining questionnaires administered via KoboToolbox and semi-structured interviews, in compliance with ethical standards. Findings reveal statistically significant correlations between year of displacement and both physical (r = 0.150, p = 0.017) and psychological violence (r = 0.072, p = 0.022). Nearly 46.74% of respondents lost relatives in atrocious circumstances (summary executions, throat-slitting, immolation), generating post-traumatic disorders including chronic insomnia, flashbacks, and psychosis. Despite psychosocial support from NGOs, prayer (39.74%) and silence (23.36%) remain the predominant coping strategies. These findings underscore the imperative for psychosocial interventions grounded in the victims’ cultural habitus to enhance their effectiveness.
Keywords:
internally displaced women
; trauma
; psychological care
; spiritual resilience
; Burkina Faso
1. Introduction
For the past decade, Burkina Faso has faced extreme violence from terrorist armed groups affiliated with Al-Qaeda (Jama’at Nasr al-Islam wal Muslimin, JNIM) and the Islamic State (Islamic State in the Greater Sahara, ISGS). The escalation of violence and the expansion of this crisis across 13 regions has generated approximately 2,062,533 internally displaced persons (IDPs), composed primarily of women and children. From 2020 to 2021, more than 1,425 violent events were recorded in 11 regions of Burkina Faso, with 51% of these attacks targeting the civilian population. In 2023, authorities counted approximately 133,994 IDPs (84,649 women and 49,345 men), representing 63.17% women in the Boucle du Mouhoun region ([1]).
The magnitude of violence against the civilian population does not affect men and women to the same degree. Women are prime targets during crises because they are perceived as the future of society ([2]) or as social regulators through their positions as mothers, spouses, homemakers, and producers ([3,4]). Moreover, they are used as weapons or methods of psychological warfare against adversaries to leave an indelible mark ([5]). In Haiti, for example, [6] describes the rape of opposition women by armed forces as a strategy of deterrence and family exclusion from political activities. From this perspective, [7] analyze sexual violence during conflicts as a political construction whose primary objective is to symbolically humiliate men by desecrating the bodies of their women. [8] characterizes this approach of systematic rape of women as a “conscious crime of intimidation” designed to render docile and terrorize men who cooperate with or join the regular army. However, [9] distinguishes between strategic violence and opportunistic violence. Strategic violence generally refers to execution of command hierarchy orders as a tactic of collective terror. Opportunistic violence, meanwhile, is not ordered by the hierarchy but represents personal initiatives by combatants.
Cohen and Nordås [10]) work on data from 1989 to 2009 from the Sexual Violence in Armed Conflict platform found that 32% of 117 armed actors systematically resort to sexual violence. For these authors, this widespread sexual violence is explained by the weakness and fragmentation of armed groups’ command chains, forced recruitment of combatants, absence of internal justice mechanisms in these armed groups, and total impunity for perpetrators of sexual violence. This violence and absence of justice mechanisms should not be analyzed as a loss of control by the command hierarchy over combatants but rather as payment in kind and a pledge of cohesion between the hierarchy and combatants.
In the Nigerian context, school-age girls are the primary targets ([11]) of the Boko Haram terrorist armed group. Indeed, the [12] highlights in its work the kidnapping of 200 girls from Chibok secondary school in 2014 and 100 other schoolgirls in 2018 in the village of Dapchi. These girls are sometimes used as human shields during regular army assaults, as kamikazes ([13,14]), or as “human bombs” ([15]). These kidnappings are sometimes analyzed as retaliatory measures against the detention of family members of Boko Haram armed group combatants by the Nigerian state. However, research shows that these hostage women are sometimes used as intelligence and surveillance agents for new hostages to brainwash them ([14]) or as cooks and weapons carriers ([15]). These women are integrated into their apparatus to capitalize on the element of surprise against regular forces. Beyond this, the sexual slavery to which they are subjected under the banner of forced marriage fits within the perverse logic of creating a new generation of combatants who would benefit from socialization anchored in the group’s Islamist ideology ([14]).
When they escape from armed groups, they are stigmatized by the community because children born from these non-consensual relations are labeled as “bad blood” ([15]). This social disqualification renders these women, already traumatized by years of captivity, even more vulnerable, thereby facilitating their return to these armed groups. Indeed, according to [16] study, more than 1.69 million women in the Democratic Republic of Congo (DRC) were rape victims. These Congolese women suffered genital mutilations, public humiliations, and carried rape pregnancies ([17]). Unlike Congo, in Iraq, Daesh subjected women to sexual slavery, sold them, or gave them as gifts to combatants. These figures appear to underestimate reality according to work by [18,19] because the subject remains sensitive and touches victims’ intimacy. Consequently, very few women report for fear of being rejected or stigmatized.
Burkina Faso, Mali, and Niger face the same reality experienced by women in Nigeria, DRC, and Iraq. Indeed, according to the [20] report, women are victims of sexual violence and psychosocial distress. While the literature is abundant on sexual violence during conflicts, this article aims to determine the different forms of violence, their consequences on internally displaced women’s (IDW) mental health, their psychological care, and resilience strategies developed by IDW.
2. Materials and Methods
2.1. Study Coverage Area
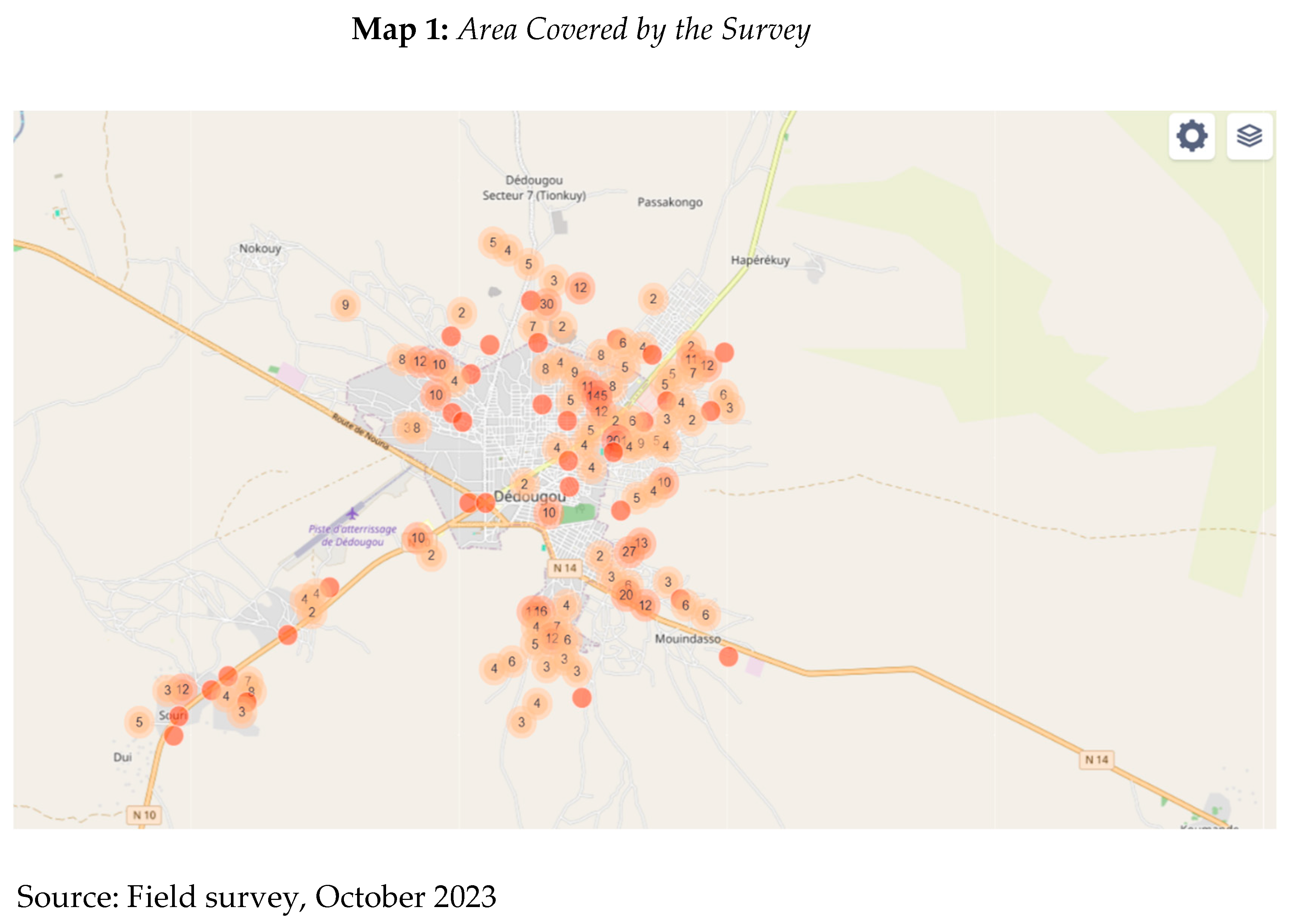
The city of Dédougou is a department and an urban commune located in the Mouhoun province of Burkina Faso. According to the [21], its population is estimated at 123,934 inhabitants. The commune of Dédougou shares borders with the following communes: to the east with the commune of Douroula, to the west with Sanaba and Bourasso, to the north with the communes of Sono and Gassan, and to the southeast with the commune of Safané. Administratively, Dédougou is subdivided into seven sectors and 37 villages. It brings together several ethnic groups (Bwaba, Marka, Fulani, Mossi, Samo, etc.), with the main languages spoken being Bwamu and Jula. Its economic activity is based primarily on agriculture and livestock farming. Map 1 indicates the area covered during data collection.
1.2. Study Population
The surveyed population consisted primarily of all internally displaced women (IDW) located on official and unofficial sites. Women victims of terrorism constitute the target population of our study in the city of Dédougou. Additionally, spouses, adult children, and close relatives constituted the control population. The survey was also extended to resource persons including non-governmental organizations (NGOs) operating in the area and state structures (Social Action).
1.3. Methods
The study of psychological and social care for women victims of terrorism is a complex object. According to [22], understanding and explaining complex social phenomena requires an integrative approach. Therefore, to grasp the scope and complexity of this theme, we opted for a convergent mixed design ([23]). This involved independent and simultaneous collection of quantitative and qualitative data. The quantitative data aimed to capture the scope and nature of the violence suffered as well as its traumatic manifestations. The qualitative approach aimed to capture the lived history of violence and the therapeutic pathway of violence victims.
1.4. Data Collection Tools and Techniques
To work on a subject as sensitive as violence against IDW, we constructed two categories of tools. The questionnaire was developed using KoboToolbox, a digital tool adapted to field surveys, facilitating data entry, centralization, and quality control of collected information. The questionnaire was structured into three main parts: information about the respondent (village of origin, year of departure, number of children, marital status, and profession before departure), types of violence suffered and types of trauma felt, and preferred therapeutic pathway.
Semi-structured interviews conducted with women victims of terrorism were carried out using an interview guide. This technique aimed to collect information on the causes of displacement, identify multiple forms of violence suffered (physical, psychological, verbal, economic, and sexual) before and during flight, the lived experience, and therapeutic pathway for this violence.
1.6. Sampling and Sample
In this quantitative study, we used two sampling techniques due to the geographic dispersion (see Map 1) of the majority of internally displaced persons: a combination of simple random sampling and snowball sampling. The absence of a sampling frame or exhaustive list of internally displaced persons led to privileging this mixed approach to constitute the quantitative sample. Indeed, the simple random sampling technique on official sites ensured statistical representativeness. The snowball sampling technique borrowed from the qualitative method identified those who had resettled in informal habitats or were housed with guardians. This strategy aimed to guarantee complete and representative coverage of IDPs in the Dédougou commune given their geographic dispersion. As for qualitative sampling, purposive sampling was privileged with inclusion criteria based on categories concerned by the interviews. The main inclusion criterion was internally displaced status for women, for NGOs working in the humanitarian field, for state agents being from the Ministry of Social Action, and for mental health professionals work ing in the humanitarian sector. Triangulation and information saturation led to ending our interviews after observing constancy. Table 1 summarizes the quantitative and qualitative sample.
1.7. Analysis Methods and Informed Consent
The qualitative data gathered from our empirical investigations were transcribed and analyzed using the artificial intelligence tool NotebookLM while ensuring fidelity to respondents’ statements. We conducted thematic content analysis of verbatim responses following the method of [24]. The use of respondents’ statements for analytical purposes adhered to ethical principles and professional standards in the social and human sciences in the absence of an institutional ethics committee. We took care not to use participants’ real identities. Additionally, before beginning each interview, participants’ free and informed consent was obtained. Furthermore, the sensitive nature of the subject required isolation of participants to access their intimate experiences and guarantee their physical and moral safety. The quantitative data collected via the KoboToolbox platform were exported to IBM SPSS Statistics 20 software for variable cross-tabulations and Pearson correlation calculations. Microsoft Excel 2020 was used to generate statistical tables.
Moreover, this study draws on [25] resilience theory and [26] intersectionality theory as an analytical framework for gender inequalities in adaptive capacity and the differentiated impact of trauma related to violence perpetrated by terrorist armed groups. IDW, not possessing the same social capital, develop differentiated adaptive strategies to context ([27]) to heal their emotional and physical wounds. For [25], the role of social and affective bonds and the individual’s inner liberating strength play a crucial role in individual reconstruction.
3. Results
This section presents the profiles of women victims of violence, the correlations between displacement and violence intensity, the lived experience of violence by IDW, and finally their resilience capacity facing the trauma suffered.
3.1. Profile of Internally Displaced Women (IDW)
The analysis of individual variables such as marital status, profession, and number of dependent children aims primarily to capture their vulnerability to violence. Indeed, we start from the postulate that widows, youth, the unemployed, and those with numerous dependent children are vulnerable social categories. Indeed, Table 2 below indicates that the vast majority of IDW were farmers (51.4%), 22.4% homemakers, 20% traders. A minority had occupations such as sewing, gardening, hairdressing, craftwork (weaving, pottery, etc.), community health aide, etc. A small proportion of women were involved in livestock raising, only 0.3%. However, after forced displacement, the vast majority of displaced persons struggle to exercise their former profession in the new refuge zone. Sociocultural constraints, land scarcity, and monetization of land transactions in the Dédougou commune impede their access to agricultural land portions to practice subsistence agriculture. Consequently, these IDW reconvert for the most part to collecting gravel, sand, dead wood, plastic bags, and begging to meet family members’ needs.

Table 2.
Professional Status of IDW.
| Professional Status | Frequency | Percentage |
| Farmer | 522 | 51.4 |
| Homemaker | 227 | 22.4 |
| Trader | 203 | 20.0 |
| Student | 22 | 2.2 |
| Seamstress | 12 | 1.2 |
| Gardener | 7 | 0.7 |
| Hairdresser | 6 | 0.6 |
| Artisan | 5 | 0.5 |
| Community health aide | 4 | 0.4 |
| University student | 4 | 0.4 |
| Total | 1,015 | 100.0 |
Source: Field survey, October 2023.
Table 3.
Number of dependent children by marital status of IDW.
| Number of dependent children | None | 1-3 | 4-6 | 7-9 | 10-12 | 13-19 | Total | Freq | P% |
| Single | 43 | 18 | 1 | 2 | 0 | 0 | 64 | 64 | 6.3 |
| Cohabiting | 2 | 15 | 7 | 2 | 1 | 1 | 28 | 28 | 2.8 |
| Divorced | 0 | 3 | 4 | 2 | 1 | 0 | 10 | 10 | 1.0 |
| Married | 32 | 224 | 355 | 122 | 23 | 3 | 759 | 759 | 74.8 |
| Widow | 3 | 23 | 79 | 40 | 9 | 0 | 154 | 154 | 15.2 |
| Total | 80 | 283 | 446 | 168 | 34 | 4 | 1,015 | 1,015 | 100 |
Source: Field survey, October 2023.
This table indicates that women with married and widow status constitute the most important category. They have 90% of the children under their care. Married women represent 74.8% of the sample and widows 15.2%. The other categories have 10% of children under their care. However, 43.9% of IDW have between 4 to 6 children under their care, 27.9% between 1 and 3 children, 16.6% have between 7 to 9 children. Those with more than 10 children under their care represent 3.7% of the sample. Moreover, it emerges that 1.95% of widows have no children under their care. This category of widows is more vulnerable emotionally as they have no attachment at the family unit level. They are more exposed to trauma effects if they do not receive adequate care. A significant number of these women became widows following attacks.
3.2. Escalation and Temporal Intensification of Violence
The IDW surveyed on official sites and in unarranged peripheral neighborhoods originate from about one hundred villages in the Sourou and Bankuy regions. However, the vast majority come from Djédougou or Guédougou, Gassan, Sanaba, and Douroula and underwent forced displacement from 2017 to 2023. The peak of forced displacement occurred in 2022 followed by a decline in 2023. All IDW, 100%, justify their displacement by violence and ultimatums from terrorist armed groups. Communities received short deadlines of 24 hours or 3 days to evacuate the village at risk of execution for disobedience.
Table 4, represented in Figure 1, determines the Pearson relationship between certain temporal variables and types of violence. Here, correlation is significant with two variable types (physical and psychological). The sample size (N) for the year of displacement variable is 1,015 IDW. It emerges from Figure 1 that the correlation is statistically significant between physical and psychological violence. Indeed, there is a significant positive correlation (r = 0.0738, p = 0.0186) between year of displacement and physical violence. These data reveal that the more recent the displacement, the greater the probability and intensity of physical violence increases, or inversely. This correlation is significant between year of displacement of IDW and psychological violence (r = 0.072, p = 0.0219). However, there is a significant negative correlation (r = -0.0498, p = 0.1126) between year of displacement and social violence (exclusion, rejection). This significance suggests that the more recent the year of displacement, the less they feel rejected or socially excluded, or inversely. These data allow us to affirm that over the years, IDW are perceived positively by the host population.
In addition to these types of violence, Table 4 allows us to affirm that correlations between year of displacement and sexual violence (r = -0.0172, p = 0.5834), verbal (r = 0.0198, p = 0.5285), and economic (r = 0.0103, p = 0.7432) are not statistically significant because p-values are greater than 0.05.
Table 5 above reveals that there is a moderate significant positive correlation between physical violence and psychological violence (r = 0.5006). Those who are victims of physical violence tend to suffer verbal violence (r = 0.4297). Persons suffering from physical violence are also victims of social exclusion.
Sophisticated terror strategy: The lived experience of violence by women
These studies examine violence experienced by IDW before, during, and after displacement. Violence suffered by most IDW before forced displacement included deprivation of liberty and imposition of strict laws to govern behaviours according to Islamic precepts. Under the control of terrorist armed groups in their villages of origin, inhabitants were under threat of execution, beatings, prohibitions against playing music, consuming millet beer, playing soccer, etc. Physical violence included imposition of the hijab or black robes to cover their entire bodies. Those who did not respect these dress codes were beaten, humiliated, raped before their spouses.
However, most atrocities were committed during attacks and forced displacement. Table 6 indicates that 46.3% of IDW lost at least one family member (spouse, children, brothers, sisters, brother-in-law, father-in-law) or community member during attacks. Men were shot in the head, others had throats slit, others were thrown into wells or burned alive. Sometimes, men were gathered in a single location to be executed in masse before women and children, as was the case with residents of the village of Guédougou. In this context of extreme violence, some families were decimated. Women’s narratives were marked by silence, tears, bitter laughter, interjections. Men, regardless of age, were systematically targeted for killing. This “scorched earth” policy strategy aimed to deter any collaboration or enlistment of men in the Volunteers for the Defense of the Homeland (VDP) auxiliary force. Moreover, forcing women and children to witness the murder of their loved ones fit within an electro-shock and deterrence policy. This is the case of Respondent 17 who finds herself the sole survivor of her family in the city of Dédougou:
Me, in any case, I no longer know if I am human. I live today just to live. If you kill yourself, they will accuse you of having committed a crime. Otherwise, I prefer to be dead than alive to have peace. When our village was attacked, I lost twelve (12) members of my family the same day. I lost my husband, my children, and my husband’s brother. The terrorists’ targets were boys. They came one morning and killed most of the boys. When they attacked the village, my husband had already left with our son to go fishing in the river. They were killed. I did not even see their bodies. Currently, I live alone here.
In addition to this victim, Respondent 21 was instead forced with her children to witness her husband’s execution. Indeed, she recounts the lived experience of this day of atrocity in these terms:
I am from Koumbara. We were stopped and stripped by the terrorists during our flight from our village. Then, they slit my husband’s throat before my eyes and my children. They forced us to walk to reach where we wished to take refuge. At one point, they wanted to burn us alive. I was lost, desperate. I took the road on foot with my three children to Dédougou here.
Respondent 4 experienced similar violence. Indeed, she was instead forced to witness the slitting of her only son’s throat. Through her narrative, it emerges that victims also suffer moral torture and insults. Verbal constraint is exercised on them not to manifest their mourning and express their pain. It emerges from her words, the atrocity of violence in these terms:
I come from the village of Bao. My eldest son had his throat slit before my eyes because he refused to join them. He was killed on a Wednesday. I went mad, I cannot overcome this cruelty. I cried so loud that “those people” (referring to terrorists) came back to tell me to shut my mouth or they would burn me alive. I responded that they could kill me. They came back the following Friday, giving us an ultimatum to leave the village in the afternoon. They formally forbade us from going to Tougan which was the nearest village otherwise we all risked dying. I had lost reason with the loss of my only son who took care of me and his six sisters since their father’s death.
Unlike these violence victims, Respondent 4 from the village of Bouna was forced with her husband into infanticide and cannibalism. The extreme trauma of this day of violence is recounted by the victim in these words:
I come from Bouna. During our displacement here, we did not suffer violence. It was rather before we displaced... About three years ago, one afternoon, armed individuals came to our village. They told inhabitants to leave immediately. I was almost at term. My husband told me we could not keep pace with the others... We stayed and at 7 p.m. we started walking, a few steps from the house I started losing water. We returned to the house to give birth. We rested a bit and the next morning very early, when we were preparing to leave, they landed at our house, they asked us why we did not leave, that we did not receive the order to leave the village, no? My husband responded that we received it, but that we could not leave because I was at term and I just gave birth. They said nothing, but they went out to confer for a good while and one of them came back ordering my husband to take the baby, slit its throat, cut it into pieces, and cook it. Hmm, we were so shocked, devastated, it is inhuman. We begged them in vain. Oh Lord! I cried, my husband even was overwhelmed by the situation. He lost the power of speech, he could not even speak. The worst is that after cooking, they wanted to force us to eat the meat and soup of our baby (cries). It was like a bad dream yet it was real. In fear of being next, we started serving the soup (our baby’s flesh), the Defense and Security Forces arrived in time to prevent them from committing this ignominy. There were exchanges of gunfire, thank God our FDS prevailed and we got out unharmed (cries).
An analysis of this verbatim reveals trauma among women exposed to violence experienced during assassinations of their husbands and children. The execution of spouses, children, and acquaintances left deep mental scars in certain IDW. This trauma manifests through mental disorders, loss of speech, insomnia, repetitive nightmares, anxiety, flashbacks, and tears. Some end up feeling “crazy” or desperate to the point of considering suicide as an alternative to eradicating mental suffering.
Establishing family relationships with IDW highlights that certain categories are more affected than others. Indeed, Table 7 indicates that the category of spouses (17.45%) and children (19.96%) constitutes 37.41% of human losses. This category represents an essential part of the family structure and the one with which IDW have a direct link. Brothers/Sisters constitute 25.90%, a quarter of human losses recorded during attacks and kidnappings. The parent’s category represents 21.94% and 14.75% of neighbours and acquaintances.
Spiritual resilience and post-traumatic psychological care.
Facing violence, IDW adopt several attitudes or self-protection mechanisms. These protection mechanisms vary from one actor to another. Figure 2 indicates that 39.74% of women take refuge in prayer sessions as a therapeutic strategy. They depend largely on this type of spiritual support mechanism to manage stress and trauma related to extreme violence experienced. Faith and prayer function as a refuge and allow many victims to find inner peace and give meaning to tragic events. Women console themselves by placing their fate in God’s hands. Non-religious strategies such as silence (23.36%) and support from loved ones (17.48%) appear as protection mechanisms against violence. Silence indicates internalization of trauma, difficulty externalizing suffering, or the conviction that opening up to expose one’s resentments appears dangerous. Unlike this silence, those who confide in loved ones indicate the importance of immediate social capital in the healing process of inner wounds.
A small percentage of women resort to authorities, only 15.2%. This situation is due to unfamiliarity with institutions empowered to emotionally support victims of psychological violence. Only 4.22% resort to strategies such as throwing themselves into work and recourse to traditional remedies. Indeed, collecting gravel and dead wood in forests appears as therapy for women. The occupation allows drowning negative thoughts (suicidal thoughts) and overcoming the pain of tragic events experienced. Another strategy used by women victims of violence is the use of decoctions (herbal teas, bark, etc.) to rid themselves of lost souls of their loved ones who haunt them. Facing mental trauma and illnesses, these strategies appear as an alternative to modern medicine which requires more financial means.
Indeed, from semi-structured interviews, it emerges that IDW rarely resort to psychologists for accompaniment in healing psychological wounds. However, certain IDW installed on official sites benefit from accompaniment and follow-up by psychologists. Awareness sessions are organized by social action agents, nurses, and NGOs (Red Cross, Médecins Sans Frontières, or INTERSOS). Care consists of conducting home visits to victims by performing psychological exercises, educational awareness sessions, discussions, spiritual and emotional support. This appears in the words of Respondent 7 (Psychologist at an NGO) in these terms:
Persons who are victims of terrorism need awareness, psycho-education, individual interviews, relaxation therapy. With these different aids, the individual manages to overcome their disorders and also adapt to a new way of life.
This also emerges from the words of Respondent 32: “Once, NGO agents came to talk with us to encourage us. This helps us forget our fears and our traumas.” Respondents recognize free care for psychological health problems. However, a vast majority of IDW affirm not resorting to or consulting psychologists made available to them in housing camps. Contrary to this information, NGOs like Médecins Sans Frontières affirm receiving around 30 to 40 persons per week with post-traumatic disorders for complete care. This free care is mentioned by Respondent 3 (agent of a humanitarian NGO) in these words:
Care for persons who are victims of terrorism is free. After receiving them, we make a diagnosis to know the state and intensity of the harm they suffer. We also make a follow-up program for the person and a care plan for the sick person.
A comparative analysis of verbatim from humanitarian workers and women victims of trauma reveals that IDW are unaware of the existence of free psychological care. Indeed, they announce financial difficulties as a barrier to consulting a psychologist. For other categories, their priority is ensuring children have food so as not to die of hunger. The latter are convinced that these psychological consultations will not bring back loved ones lost in attacks.
4. Discussion
Our empirical investigations reveal a reality observable in all conflict-infested zones, whether symmetric or asymmetric: women become a terrain of political and media confrontation. In certain conflicts like Vietnam, the slogan was “Occupy women’s wombs” ([28]). Indeed, in conflict zones, they are more exposed to risks of pregnancy, sexually transmitted diseases, and social disqualification as highlighted in work by [6,7,15]. Very few IDW admit having suffered different forms of sexual violence because it is a risk of being ineligible for marriage or being socially excluded ([18,19,28,29,30]). The sociocultural context and negative perception of rape explain this negative correlation (r = -0.0172; p-value = 0.5834). Most often, they wall themselves in silence and choose to die with the secret of rape so as not to appear as beings soiled by the enemy ([29]) or be rejected by family and community. Moreover, this study indicates a significant positive correlation between physical, psychological (r = 0.5006), and verbal (r = 0.4297) violence. This indicates that victims suffered physical, verbal, and psychological violence. Indeed, during attacks, women were forced to wear the hijab, were beaten, insulted, and humiliated in public.
The absence of significant correlation regarding social violence (p = 0.1126) corroborates results obtained by [31] within the framework of the PARJEF-PDI project in the North and Boucle du Mouhoun regions. This report also indicates that the majority of households appreciate their relationship with the host population. Indeed, 56% estimate that there is cohesion between host households and IDPs. However, for [32], host population vulnerability and other factors constitute major risks that can lead to conflicts and deterioration of social cohesion with displaced persons. Consequently, it proposes addressing grievances, inequalities, marginalization, violence, and existing interethnic tensions before resettling forcibly displaced persons.
Trauma symptoms due to exposure to extreme violence in Burkina Faso are similar to observation data from [33] among Yazidi women in Iraq. In both contexts, women witnessed execution of their spouses and male children. Consequently, they become insomniacs, develop suicidal feelings, lose power of speech, and develop feelings of madness ([34]). Moreover, we also note neurovegetative hyperactivation (hypervigilance and chronic insomnia), traumatic re-experiencing (“the slitting of my son’s throat haunts me,” “I see my son burned alive again”).
In terms of therapeutic pathway, our results reveal that women resorted to prayer (39.74%) and silence (23.6%) as post-traumatic disorder management strategies. These results are similar to findings by [35] on the therapeutic pathway of persons with mental disorders in the North region of Burkina Faso. From this perspective, [36] suggest integrating a culturally anchored resilience approach to care. Integrating prayer into psychological disorder care would strongly contribute to improving victims’ mental health status. However, systematic disqualification of this prayer-based approach in favor of standardized interventions does not provide a culturally anchored response. Taking this reality into account by NGOs and the Ministry of Social Action in their diagnostic and care approach would contribute to significantly improving women’s condition. Moreover, our study reveals that despite free psychological care, very few women resort to it. Free care and psychologist availability in displaced persons’ camps does not guarantee professional care attendance rates. This low recourse is explained primarily by four interacting factors: geographic dispersion of IDW, ignorance of psychological services’ existence, perception of these services as the “madhouse,” and inversion in need hierarchy compared to Maslow’s classification. They place their food needs before their psychological well-being. For others, consulting a psychologist is not culturally anchored in habitus and most often, users of these services are labelled “white” or fragile.
In the same vein, [37] explains that systematic imposition of the DSM approach in societies with another conception of person and suffering appears ineffective in terms of expected responses. The author emphasizes that in these non-Western societies with different nosology’s from Western society, psychological distress is sometimes perceived as spiritual possession or a response to transgression of ancestral prohibitions, etc. Moreover, this is the conviction of some of our respondents who affirm having used decoctions for purification baths to rid themselves of haunting by suffering souls of loved ones killed in atrocious conditions. Modern medicine cannot provide a response to “red deaths,” an IDW told us. These beliefs escape biomedical Western reading grids. Studies by [38,39] in Sierra Leone and [40] in Zimbabwe demonstrate that child soldiers’ participation in deliverance prayers and community therapy groups have a positive effect on children’s anxio-depressive symptoms. However, our results show limits in “spiritual resilience” adopted by IDW confronted with cannibalism, infanticide, or extermination of all family members. The expression “I live just to live” reveals their dehumanization, their loss of taste for life. This category of victim having no more emotional attachment, if not assisted and followed, is most inclined to suicide ([41,42]) or “fatalistic suicide” ([43]). Our results join conclusions of work by [34] on dehumanization and loss of existential meaning characteristic of Post-Traumatic Stress Disorder (PTSD).
However, adoption of silence by certain IDW as an individual defense mechanism to attenuate trauma appears risky in the long term. Indeed, in our context, 23.6% of IDW resort to this strategy. However, for [44], this therapy approach allows short-term response to traumatic situation survival but constitutes a danger for the person long-term. For this author, it is a solution potentially carrying chronic long-term disorders. These persons present a risk of depression evaluated at 2.5 times compared to persons confiding in a PTSD professional ([19]). Follow-up of this vulnerable IDW category appears urgent as they are predisposed to relapse.
An intersectional analysis of sociodemographic profile reveals that IDW are not a homogeneous group. Their vulnerability varies according to marital status, professional status, and family burden. Indeed, widows representing 15.2% of the sample, 43.9% have 4 to 6 children under their care, and 51.4% were farmers. However, those who held small agricultural exploitations in their village of origin to meet some of their food, economic, clothing, and health needs struggle to access a land portion in the reception zone. Indeed, [45]) study reveals that land scarcity, land transactions, sociocultural constraints, and perception of IDPs as privileged (food donations, cash transfers, free care in health facilities, etc.) complicate their right to access an agricultural land portion with the host population. In the trauma context, work appears as a refuge to escape depression. This inability to exercise former occupations in the reception zone renders their economic, social, and psychological reconstruction even more vulnerable. They are victims of double trauma: the mental burden of meeting children’s food and health needs but also the loss of spouses, children, and loved ones in inhuman conditions. Those who lost an immediate family unit member represent 37.41% of human losses. This reality reflects the collapse of family support structures in grief situations but also their socioeconomic reference point ([46]). Indeed, our results indicate that 46.3% of IDW lost a loved one, which constitutes an alarming indicator of human cost. In the Democratic Republic of Congo, [16] also found that women lost approximately 40% of their immediate loved ones in violence. An intersectional analysis reveals differential vulnerability between widowhood status and motherhood. Indeed, according to [18], widows present 3.2 times greater risk of sinking into psychological distress than married women in the same situation. The 1.95% of widows who lost husband and child in the crisis are most often invisible as they have no family, economic, and emotional support network. This widow category is more vulnerable and runs greater risk of slipping into chronic depression. Facing this reintegration reality, IDW reconvert for the most part to collecting gravel, sand, dead wood, plastic bags, and begging to meet their family members’ needs.
5. Conclusions
The study on resilience of women victims of terrorism in Burkina Faso highlights the multiform and systematic extreme violence to which they were exposed before and during forced displacement. They were victims of physical violence (mutilation, beatings), psychological violence (cannibalism, infanticide, exposure to execution of loved ones, public humiliation, etc.), and sexual violence (touching, rape). This deliberate brutality maintained by terrorist armed groups against the civilian population fits within a logic of spatial marking through mediatisation of violence. Extreme violence serves to deter men, women, and youth from enlisting or collaborating with defence and security forces. Implementation of the “scorched earth” policy consisted of systematically executing men and male youth. This human tragedy has consequences on the social, economic, and vulnerability levels of IDW. Indeed, these victim women present signs of post-traumatic disorders. Most have chronic insomnia, flashbacks, nightmares, madness, loss of speech, isolation, tears, etc. Moreover, this research highlights vulnerability according to marital status and family burden. Indeed, childless widows, women with 4 to 6 years under their care, whether widows or not, present differentiated vulnerability risks. However, if they are cared for by psychologists from humanitarian NGOs and Social Action in internally displaced persons’ camps, many escape their coverage due to their geographic dispersion, ignorance, and negative perception of psychologists. The vast majority turn to prayer and silence to face trauma. These results therefore suggest contextual intervention anchored in cultural nosology’s of post-traumatic disorders with priority targeting of isolated widows and women with numerous children under their care. Moreover, accompanying IDW in exercising income-generating activities appears as a solution to reduce vulnerability risks and accentuation of post-traumatic disorders.
Funding
This research received no external funding and was conducted using the author’s own resources.
Institutional Review Board Statement
Due to the absence of an institutional ethics committee at our university, this study was conducted in strict adherence to ethical standards governing humanities and social sciences research. All participant’s rights were fully respected throughout the research process.
Informed Consent Statement
Free and informed consent was secured at the commencement of each interview. Verbal informed consent was obtained from all study participants. Given that the overwhelming majority of participants were non-literate, requesting written consent would have posed a significant barrier to participation, as potential participants expressed concern about signing documents they could not read or fully understand. All participants were nonetheless informed that data would be used exclusively for academic purposes. Anonymity was guaranteed to all participants to ensure their willingness to participate.
Data Availability Statement
Pursuant to new regulations enacted in August 2025 that prohibit the collection and dissemination of raw data pertaining to internally displaced persons in Burkina Faso, the datasets generated during this study cannot be made publicly avaible due to legal, confidentiality, and ethical constraints.
Acknowledgments
We are grateful to all third year undergraduate students in sociology and anthropology who assisted with data collection. Our profound appreciation and encouragement are extended to the participants who courageously overcame their trauma to share they intimate experiences with us. During de preparation of this manuscript, the authors used NotebookLM for the processing of qualitative data, Genspark for generating Pearson correlation visualisations, and Claude for English translation. The authors have thoroughly reviewed and edited all outputs and assume full responsibility for the content of this publications.
Conflicts of Interest
The authors declare no conflicts of interest. As this research received no external funding, the study design, data collection and interpretation, manuscript writing, and the decision to publish the findings were undertaken entirely as personal scholarly initiative.
Abbreviations
The following abbreviations are used in this manuscript:
| IDW | Internally Displaced Women |
| IDPs | Internally Displaced Persons |
| PTSD | Post-Traumatic Stress Disorder |
References
- MAHSN. Gender and women dashboard 2023. Direction Générale des Études et des Statistiques Sectorielles, 2025. Available online: http://cns.bf/IMG/pdf/dgess-mahsn_tableau_de_bord_2023_f_g.pdf.
- Santoire, E. Women and violent extremism in West Africa. Institute for Security Studies. 2020. [Google Scholar]
- DCAF; OSCE/ODIHR; UN Women. Gender, preventing violent extremism and countering terrorism (Policy Brief No. 3). DCAF. 2019. Available online: https://www.dcaf.ch/sites/default/files/publications/documents/GSPolicyBrief_PVE%20CVE%20CT_FR%20FINAL_0.pdf.
- Foutem, F. M. Women and violent extremism in the Lake Chad Basin; Institute for Security Studies, 2021. [Google Scholar]
- Guignard, C. Sexual violence in wartime: Weapon, method, strategy or practice? In stitut du Genre en Géopolitique; 2020. [Google Scholar]
- Longtin, D. Violence against women in Haiti: Between the (inter)national assistance network and the representation of Haitian feminist organizations (1991–2008). Master’s thesis, Université du Québec à Montréal, 2010. [Google Scholar]
- Taxil, B.; Massias, J.-P. Sexual violence in armed conflicts: What responses from international law and transitional justice? IFJD 2024. [Google Scholar]
- Brownmiller, S. Against our will: Men, women and rape; Simon & Schuster, 1975. [Google Scholar]
- Wood, E. J. Conflict-related sexual violence and the policy implications of recent research. International Review of the Red Cross 2015, 96(894), 35–60. [Google Scholar] [CrossRef]
- Cohen, D. K.; Nordås, R. Sexual violence in armed conflict: Introducing the SVAC dataset (1989–2009). Journal of Peace Research 2014, 51(3), 418–428. [Google Scholar] [CrossRef]
- Zenn, J. The terrorist calculus in kidnapping girls in Nigeria: Cases from Chibok and Dapchi. CTC Sentinel 2018, 11(3), 1–8. Available online: https://ctc.westpoint.edu/the-terrorist-calculus-in-kidnapping-girls-in-nigeria-cases-from-chibok-and-dapchi.
- Federal Ministry of Education (Nigeria). Education Today Journal. Federal Ministry of Education. 2021. Available online: https://education.gov.ng/wp-content/uploads/2022/01/FME-Journal-2021.pdf.
- Barna, J. Insecurity in context: The rise of Boko Haram in Nigeria. In European Parliament; Directorate-General for External Policies, Policy Department, 2014. [Google Scholar]
- Bloom, M.; Matfess, H. Women as symbols and swords in Boko Haram’s terror. Prism 2016, 6(1), 104–121. [Google Scholar]
- UNODC. Handbook on children recruited and exploited by terrorist and violent extremist groups: The role of the justice system; United Nations Office on Drugs and Crime, 2017. [Google Scholar]
- Peterman, A.; Palermo, T.; Bredenkamp, C. Estimates and determinants of sexual violence against women in the Democratic Republic of Congo. American Journal of Public Health 2011, 101(6), 1060–1062. [Google Scholar] [CrossRef] [PubMed]
- Eriksson Baaz, M.; Stern, M. Sexual violence as a weapon of war? Perceptions, prescriptions and problems in the Congo and beyond; Zed Books, 2013. [Google Scholar]
- Hynes, M.; Robertson, K.; Ward, J.; Crouse, C. A determination of the prevalence of gender-based violence among conflict-affected populations in East Timor. Disasters 2004, 28(3), 294–321. [Google Scholar] [CrossRef]
- De Oliveira Araujo, J. O.; Reichenheim, M. E.; Moraes, C. L. Prevalence of sexual violence among refugees: A systematic review. Revista de Saúde Pública 2019, 53, 78. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6752644/. [CrossRef] [PubMed]
- CONASUR. Rapport sur la situation des personnes déplacées internes; CONASUR, 2023. [Google Scholar]
- RGPH. Cinquième recensement général de la population et de l’habitation du Burkina Faso. In Institut National de la Statistique et de la Démographie; 2019. [Google Scholar]
- Creswell, J.W.; Plano Clark, V.L. Designing and conducting mixed methods research, 3rd ed.; Sage Publications, 2017. [Google Scholar]
- Fetters, M. D.; Curry, L. A.; Creswell, J. W. Achieving integration in mixed methods designs: Principles and practices. Health Services Research 2013, 48(6pt2), 2134–2156. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006, 3(2), 77–101. [Google Scholar] [CrossRef]
- Cyrulnik, B. Les vilains petits canards. In Odile Jacob; 2001. [Google Scholar]
- Collins, P. H. Intersectionality as critical social theory; Duke University Press, 2019. [Google Scholar]
- Rutter, M. Psychological resilience and prospective mechanisms. American Journal of Orthopsychiatry 1987, 57(3), 316–331. [Google Scholar] [CrossRef]
- Maquestiau, A.; In’t Zandt, N. Sexual violence in conflict: Moving beyond militarized responses. In International Alert; 2017. [Google Scholar]
- Bouvier, P. Sexual violence, health and humanitarian ethics: Toward a global, person-centered approach. International Review of the Red Cross 2014, 96(894), 125–146. [Google Scholar] [CrossRef]
- Tengueri, Y. Breaking the code of silence: Sexual violence and campus culture at Daniel Ouezzin Coulibaly University, Burkina Faso. Frontiers in Sociology 2026, 10, 1652314. [Google Scholar] [CrossRef]
- OCADES. Rapport du projet PARJEF-PDI. In OCADES Caritas Burkina; 2022. [Google Scholar]
- FAO. REFERENCE MANQUANTE – citée dans le texte mais absente de la liste de références / MISSING REFERENCE – cited in text but absent from reference list. Please provide full bibliographic details. 2021.
- Cetorelli, V.; Sasson, I.; Shabila, N.; Burnham, G. Mortality and kidnapping estimates for the Yazidi population in the area of Mount Sinjar, Iraq, in August 2014: A retrospective household survey. PLOS Medicine 2017, 14(5), e1002297. [Google Scholar] [CrossRef]
- Elbert, T.; Hinkel, H.; Maedl, A.; Hermenau, K.; Hecker, T.; Schauer, M.; Lancaster, P. Sexual and gender-based violence in the Kivu provinces of the Democratic Republic of Congo: Insights from former combatants. In World Bank Working Paper; 2013. [Google Scholar]
- Ouedraogo, S. Management of mental disorders in northern Burkina Faso: About 35 cases followed by the association Sauvons Le Reste. Master’s thesis, Université Senghor, 2019. Available online: https://hdl.handle.net/20.500.12177/5337.
- Panter-Brick, C.; Leckman, J. F. Editorial commentary: Resilience in child development-Interconnected pathways to wellbeing. Journal of Child Psychology and Psychiatry 2013, 54(4), 333–336. [Google Scholar] [CrossRef]
- Summerfield, D. The invention of post-traumatic stress disorder and the social usefulness of a psychiatric category. British Medical Journal 2001, 322(7278), 95–98. [Google Scholar] [CrossRef]
- Betancourt, T. S.; McBain, R.; Newnham, E. A.; Akinsulure-Smith, A. M.; Brennan, R. T.; Weisz, J.; Beardslee, W. R. The intergenerational impact of war: Longitudinal relationships between caregiver and child mental health in postconflict Sierra Leone. Journal of Child Psychology and Psychiatry 2015, 56(12), 1335–1343. [Google Scholar] [CrossRef]
- Betancourt, T. S.; Brennan, R. T.; Rubin-Smith, J.; Fitzmaurice, G. M.; Gilman, S. E. Sierra Leone’s former child soldiers: A longitudinal study of risk, protective factors, and mental health. Journal of the American Academy of Child & Adolescent Psychiatry 2010, 49(6), 606–615. [Google Scholar] [CrossRef]
- Patel, V.; Saxena, S.; Lund, C.; Thornicroft, G.; Baingana, F.; Bolton, P.; Unützer, J. The Lancet Commission on global mental health and sustainable development. The Lancet 2018, 392(10157), 1553–1598. [Google Scholar] [CrossRef] [PubMed]
- De Jong, J. T. V. M.; Komproe, I. H.; Van Ommeren, M.; El Masri, M.; Araya, M.; Khaled, N.; van de Put, W.; Somasundaram, D. Lifetime events and posttraumatic stress disorder in 4 postconflict settings. JAMA 2001, 286(5), 555–562. [Google Scholar] [CrossRef]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R. A.; van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA 2009, 302(5), 537–549. [Google Scholar] [CrossRef] [PubMed]
- Durkheim, É. Le suicide: Étude de sociologie; Routledge, 2005. [Google Scholar]
- Tol, W. A.; Stavrou, V.; Greene, M.; Mergenthaler, C.; van Ommeren, M.; de Jong, J. T. V. M. Sexual and gender-based violence in areas of armed conflict: A systematic review of mental health and psychosocial support interventions. Conflict and Health 2013, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Tengueri, Y. Land situation of internally displaced women in the commune of Dédougou, Burkina Faso. Revue Hybrides 2023, 1(1), 200–215. [Google Scholar]
- Human Rights Watch. "We found their bodies later that day": Atrocities by armed Islamists and security forces in Burkina Faso’s Sahel region. Human Rights Watch. 2019. Available online: https://www.hrw.org/sites/default/files/report_pdf/burkinafaso0319_web.pdf.
Figure 1.
Pearson Correlation. Source: Data 2022 and 2023.
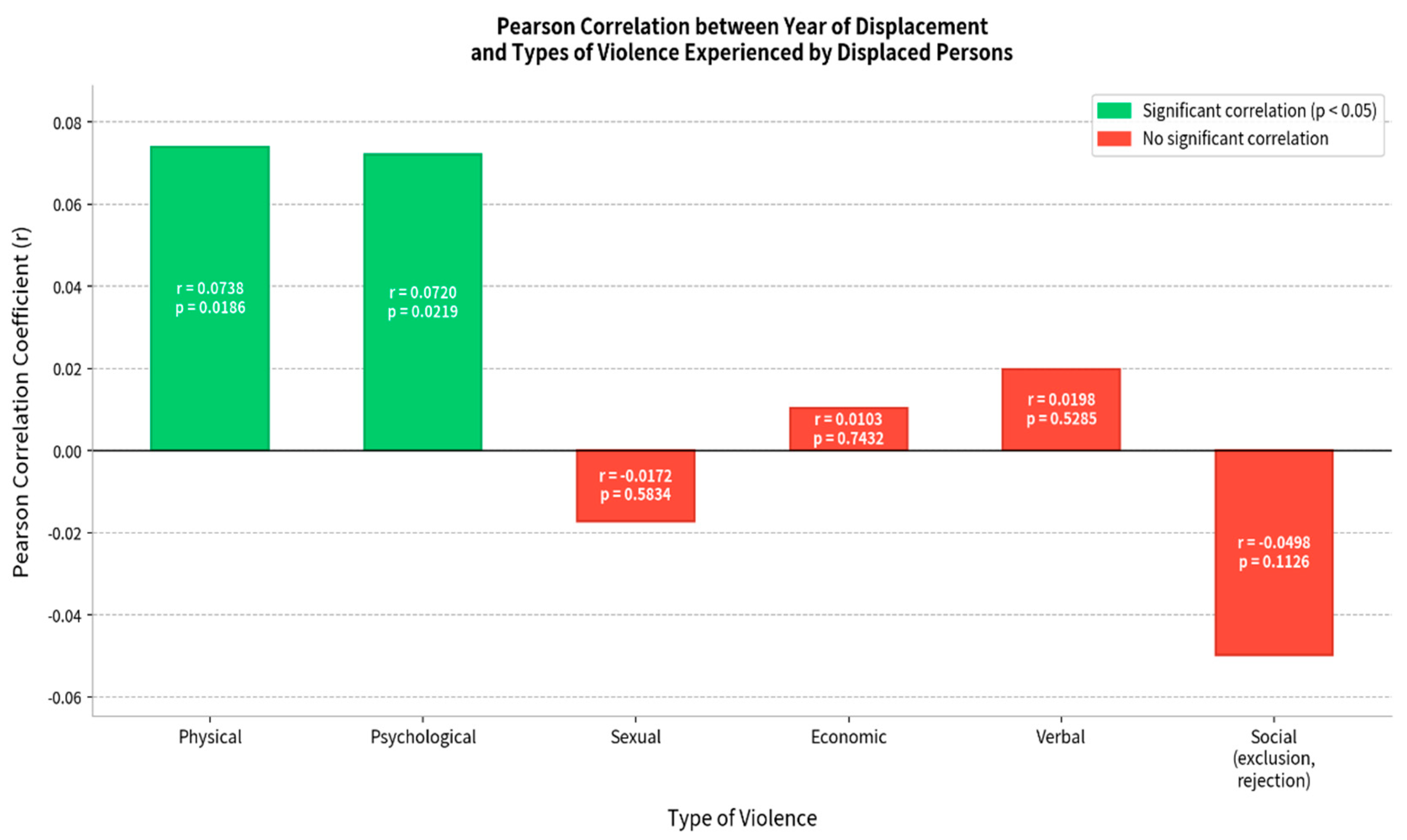
Figure 2.
Recourse facing violence. Source: Field survey, October 2023.
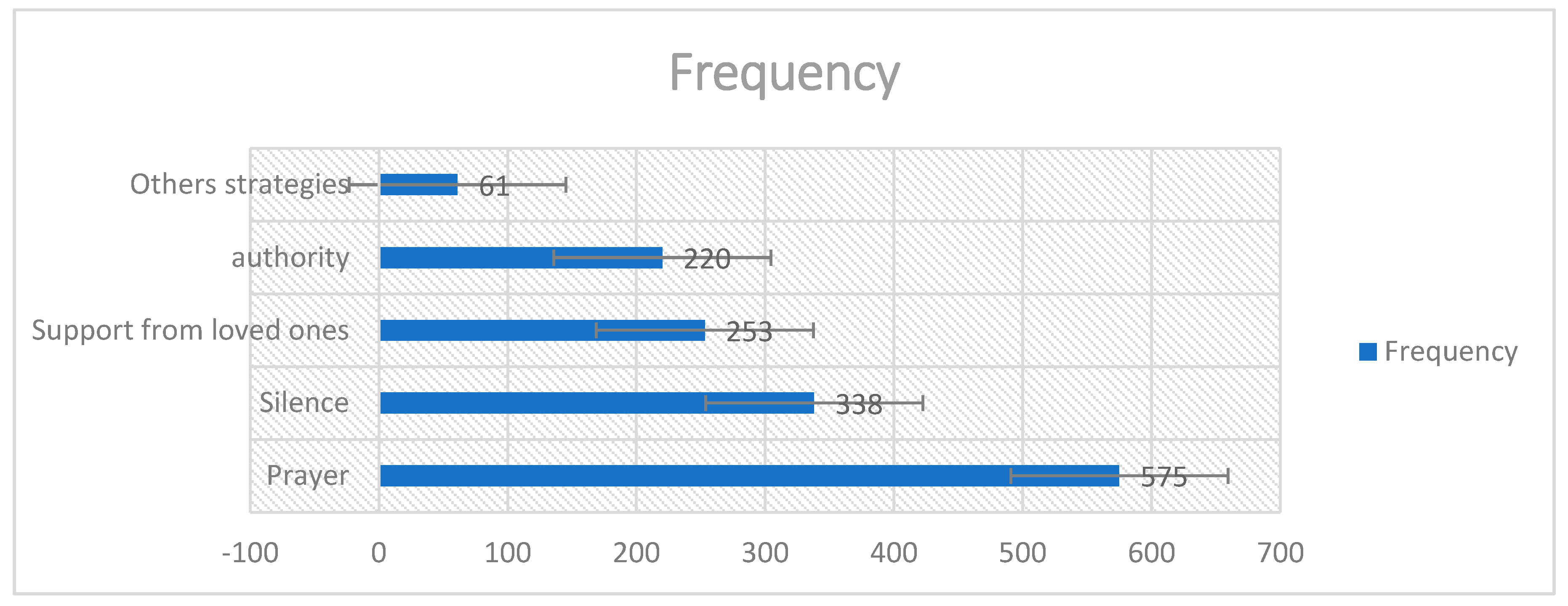
Table 1.
Quantitative and Qualitative Sample. Source: Field survey, October 2023.
| Survey Type | Sampling Type | Survey Population | Sample |
| Quantitative survey | Simple random | IDW | 1015 |
| Qualitative survey |
Purposive |
Spouses | 25 |
| Women victims of violence | 11 | ||
| NGOs (ASMADE, INTERSOS, OCADES, Médecins Sans Frontières) | 04 | ||
| Social Action | 01 | ||
| TOTAL | 1056 |
Table 4.
Pearson correlations between year of displacement and types of violence.
| Type of Violence | Correlation Coefficient (r) | p-value | Interpretation |
|---|---|---|---|
| Physical | 0.0738 | 0.0186 | Significant correlation (p < 0.05) |
| Psychological | 0.072 | 0.0219 | Significant correlation (p < 0.05) |
| Sexual | -0.0172 | 0.5834 | No significant correlation |
| Economic | 0.0103 | 0.7432 | No significant correlation |
| Verbal | 0.0198 | 0.5285 | No significant correlation |
| Social (exclusion, rejection) | -0.0498 | 0.1126 | No significant correlation |
Source: Field survey, October 2023; IBM SPSS 20.
Table 5.
Pearson correlations among types of violence.
| Type of Violence | Physical | Psychological | Sexual | Economic | Verbal | Social |
| Physical | 1 | 0.5006 | 0.1915 | 0.2331 | 0.4297 | 0.2113 |
| Psychological | 0.5006 | 1 | -0.0075 | 0.1968 | 0.286 | 0.2818 |
| Sexual | 0.1915 | -0.0075 | 1 | -0.03 | 0.1724 | -0.0238 |
| Economic | 0.2331 | 0.1968 | -0.03 | 1 | 0.1098 | 0.2188 |
| Verbal | 0.4297 | 0.286 | 0.1724 | 0.1098 | 1 | -0.0118 |
| Social | 0.2113 | 0.2818 | -0.0238 | 0.2188 | -0.0118 | 1 |
Source: Field survey, 2023.
Table 6.
Human losses before and during forced displacement.
| Did you lose a family member during the attack | Frequency | Percentage |
| No | 545 | 53.7 |
| Yes | 470 | 46.3 |
| Total | 1,015 | 100.0 |
Source: Field survey, October 2023.
Table 7.
Type of relationship with victims.
| Relationship with Victim | Frequency | Percentage |
| Spouse | 97 | 17.45 |
| Child | 111 | 19.96 |
| Parent | 122 | 21.94 |
| Brother/sister | 144 | 25.90 |
| Others | 82 | 14.75 |
| Total | 556 | 100.00 |
Source: Field survey, October 2023.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



