
Submitted:
16 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Background: Conversational artificial intelligence (AI), including chatbots and large language models (LLM), based agents, is increasingly explored as a digital health intervention in physical rehabilitation. These systems offer potential benefits in patient education, treatment adherence, self-management support, and clinical workflow augmentation. Despite rapid technological advances, a comprehensive synthesis of their applications in physiotherapy, particularly within specific national contexts such as Greece, is lacking. Objective: This scoping review aims to map the existing literature on conversational AI agents in physical rehabilitation, examine their system design and clinical applications, and identify research gaps and future directions relevant to Greek physiotherapy practice.Methods: Following PRISMA-ScR guidelines, peer-reviewed studies, preprints, technical reports, and regulatory documents published between 2010 and 2026 were identified through searches of biomedical, rehabilitation, and computer science databases. Eligible studies involved conversational AI systems applied to physiotherapy or musculoskeletal rehabilitation. Data were extracted on system architecture, interaction modality, clinical use case, reported outcomes, and implementation considerations. Results: The literature shows growing interest in conversational AI for exercise coaching, adherence monitoring, patient education, and triage. Recent studies increasingly employ LLM-based architecture and retrieval-augmented generation to improve response accuracy. However, clinical evidence remains heterogeneous, with limited randomized trials and inconsistent outcome measures. Few studies address linguistic adaptation, cultural appropriateness, or regulatory alignment in Greek healthcare settings. Conclusions: Conversational AI agents represent a promising adjunct to physiotherapy services but remain at an early stage of clinical maturity. Responsible integration into Greek rehabilitation practice will require rigorous evaluation, localization, and regulatory alignment.
Keywords:
conversational artificial intelligence
; physiotherapy
; rehabilitation
; large language models
; digital health
; Greece
; scoping review
1. Introduction
1.1. Digital Transformation in Physiotherapy
Digital health technologies have become increasingly integrated into physiotherapy and rehabilitation practice, driven by rising chronic disease prevalence, workforce constraints, and growing demand for patient-centered care. Tele-rehabilitation platforms, wearable sensors, and mobile health applications have expanded access to rehabilitation services while supporting self-management and continuity of care. Within this evolving landscape, artificial intelligence (AI) has emerged as a key enabler of personalized, scalable, and data-driven rehabilitation interventions [1].
Physiotherapy is particularly well suited to digital augmentation due to its emphasis on education, exercise prescription, behavioral adherence, and long-term engagement. However, many existing digital tools rely on static content or limited interactivity, which may constrain patient motivation and responsiveness [2]. Conversational AI agents, systems capable of engaging users through natural language dialogue, offer a novel approach to addressing these limitations by providing interactive, adaptive, and context-aware support.
1.2. Conversational AI and Large Language Models
Conversational AI encompasses a range of technologies, including rule-based chatbots, natural language understanding systems, and, more recently, large language models (LLMs). Early healthcare chatbots relied on predefined decision trees and scripted responses, limiting flexibility and scalability. Advances in deep learning and transformer-based architecture have enabled LLMs capable of generating coherent, context-sensitive responses across diverse domains [3].
In healthcare, LLM-based conversational agents have been explored for clinical documentation, patient education, triage, and decision support. In rehabilitation contexts, their potential applications include exercise instruction, symptom monitoring, motivational coaching, and clarification of treatment plans. Voice-enabled interfaces further enhance accessibility, particularly for older adults or individuals with motor or visual impairments.
Despite this promise, concerns remain regarding response accuracy, hallucinations, data privacy, and ethical use. These risks are particularly salient in rehabilitation, where incorrect guidance may lead to injury or delayed recovery. Consequently, careful evaluation and governance are essential prior to widespread clinical deployment [4,5].
1.3. Rationale for a Greek-Focused Perspective
Greece presents a distinctive context for the adoption of conversational AI in physiotherapy. The Greek healthcare system combines public and private provision, with physiotherapists playing a central role in musculoskeletal and neurological rehabilitation. Linguistic specificity, cultural expectations regarding clinician–patient interaction, and regulatory obligations under European Union law influence the feasibility and acceptability of AI-based interventions [5,6].
To date, most conversational AI research has been conducted in English-speaking or Northern European settings. Limited attention has been paid to localization, Greek-language performance, or alignment with national rehabilitation pathways. A focused synthesis is therefore warranted to inform future research and implementation strategies tailored to Greek physiotherapy [7].
1.4. Objectives
The objectives of this scoping review are to:
- Map the existing literature on conversational AI agents used in physical rehabilitation and physiotherapy.
- Examine system design characteristics and clinical application domains.
- Identify gaps, ethical considerations, and future research priorities relevant to Greek physiotherapy practice.
2. Methods
2.1. Study Design
This review followed a scoping review methodology, selected to comprehensively map the breadth and nature of evidence in an emerging research field. The review was conducted in accordance with the PRISMA Extension for Scoping Reviews (PRISMA-ScR) [8]. The complete PRISMA-ScR checklist is provided in Appendix A (Table A1).
2.2. Eligibility Criteria
Studies were included if they:
- Involved conversational AI systems (chatbots, voice assistants, or LLM-based agents).
- Were applied to physical rehabilitation, physiotherapy, or musculoskeletal care.
- Reported design characteristics, clinical applications, or evaluation outcomes.
Exclusion criteria included non-interactive AI systems (e.g., imaging-only algorithms), studies unrelated to rehabilitation, and opinion pieces without substantive technical or clinical content.
2.3. Information Sources and Search Strategy
Search was conducted across biomedical, rehabilitation, and computer science databases, supplemented by grey literature from regulatory bodies and professional organizations. The search timeframe spanned 2010–2026 to capture both early chatbot systems and recent LLM-based developments.
Search Results Summary
- SciSpace Basic Search: 100 papers
- SciSpace Full Text Search: 100 papers
- SciSpace Library Search: 0 papers
- Google Scholar: 19 papers
- PubMed: 20 papers
- ArXiv: 20 papers
- Total papers found: 259 papers across all databases
- After deduplication and AI-powered reranking: 114 unique papers, ranked by relevance
- Selected: 9 high relevant
2.4. Study Selection and Data Charting
Titles and abstracts were screened for relevance, followed by full-text review. Data were charted using a standardized extraction form capturing publication characteristics, system architecture, interaction modality, clinical use case, outcomes, and implementation considerations. The study selection process is summarized in Figure 1.
A total of 259 records were identified through database searches. After removal of duplicates, 114 records were screened, and 9 studies met the inclusion criteria.
3. Results
3.1. Study Selection and Characteristics
The literature search yielded a diverse body of confirmation spanning rehabilitation science, digital health, artificial intelligence, and human–computer interaction. Most included studies were published after 2018, reflecting the rapid emergence of conversational AI and large language models in healthcare contexts. Study designs included feasibility studies, pilot randomized controlled trials, observational analyses, technical system descriptions, and narrative or scoping reviews [9,10].
Most studies originated from North America, Western Europe, and East Asia, with limited representation from Southern Europe and minimal direct proof from Greek clinical settings. Target populations primarily included individuals with musculoskeletal disorders, particularly knee osteoarthritis, as well as broader rehabilitation cohorts [11].
3.2. Design Characteristics of Conversational AI Agents
Conversational AI systems varied substantially in architectural design. Earlier systems relied on rule-based dialogue trees and scripted responses, whereas more recent approaches employed large language models, often augmented with retrieval-based mechanisms to constrain output and reduce hallucination risk. Interaction modalities included text-based chatbots, voice-enabled assistants, and hybrid systems integrating mobile sensors or wearable inputs.
Voice-based agents were increasingly explored for rehabilitation contexts due to their accessibility and potential to support hands-free interaction during exercise execution. However, multilingual capability and dialect adaptation remained inconsistently addressed, with Greek language support largely absent from evaluated systems.
Types of Agents
This section classifies the conversational and text AI agents reported in rehabilitation research and links each class to representative studies. The table below compares common agent forms, their interaction modes, typical uses, and concrete research examples. The main categories of conversational agents identified in the literature are summarized in Table 1.
3.3. Clinical Applications in Physical Rehabilitation
The reviewed literature identified several dominant application domains in physical rehabilitation. Exercise prescription and coaching emerged as the most prevalent use case, with conversational agents delivering structured guidance, reminders, and motivational feedback to support home-based programs. Adherence monitoring and behavioural reinforcement were frequently embedded within these systems, reflecting a broader emphasis on sustaining long-term engagement.
Beyond exercise delivery, conversational agents were implemented across multiple stages of the rehabilitation pathway, including prehabilitation, postoperative recovery, discharge planning, and long-term follow-up. Across studies, applications clustered around six primary functional domains:
- Postoperative follow up and reassurance. SMS/chat agents handle routine recovery questions and can reduce unnecessary clinic contacts by reassuring patients or escalating when needed [13].
- Initial assessment and recommendations LLM based advisors are prototyped to offer symptom interpretation, exercise suggestions, and referenced guidance to support self-management or clinician decision making [17].
- Therapist supports and monitoring. Robot integrated, and sensor connected systems pair automated monitoring with conversational interaction to provide feedback and support personalized sessions [18].
Collectively, these use cases demonstrate that conversational agents are primarily positioned as supportive tools that extend rehabilitation beyond the clinic, rather than as autonomous clinical decision-makers. The cited studies describe varied deployment contexts, target populations, and technological maturity levels, reflecting a field that remains innovative but heterogeneous [12,13,14,15,16,17,18,19].
3.4. Evidence of Effectiveness and Safety
Evidence supporting clinical effectiveness remains mixed and methodologically heterogeneous. Many studies remain small-scale feasibility evaluations, and robust long-term randomized data across conditions is lacking. Few investigations employed adequately powered randomized controlled designs, and outcome measures varied substantially across studies.
Empirical findings can be grouped into several thematic categories.
- Quality of life and engagement A multistage study of a full featured virtual coach for older patients reported engagement above UX thresholds and QoL improvements of >10% between experimental and control groups [12].
- Technical performance and user satisfaction A Portuguese Parkinson’s conversational agent (PANDORA) achieved 100% domain coverage and coherence in technical evaluation and scored 4.2–4.9/5 on user satisfaction in a small user study, suggesting potential for increased engagement though impact on long term exercise adherence remains unproven [19].
- Postoperative feasibility and satisfaction An SMS chatbot for hip arthroscopy patients yielded 80% of users rating helpfulness as good/excellent and handled 79% of independent patient questions appropriately in a 6 week prospective cohort [13].
- Implementation and feasibility A chatbot supervising home rehabilitation after total knee replacement was implemented and found feasible in the postoperative period, supporting adherence monitoring and automated interactions though larger efficacy trials are pending [14].
- Cognitive therapy applications Mobile conversational systems for stroke rehabilitation were designed to adapt exercises to user needs and accessibility constraints, with prototypes demonstrating feasibility for elderly and disabled users [15].
Safety considerations were inconsistently examined. Although risks related to inaccurate guidance, over-reliance on automated advice, and data privacy were acknowledged, systematic mitigation strategies were rarely evaluated empirically.
Overall, current indication suggests promising feasibility and engagement outcomes; however, the literature remains largely pilot-scale, condition-specific, and usability-focused rather than grounded in large, high-quality randomized clinical trials [12,13,14,15,16,17,18,19]. The field therefore appears developmentally active but not yet clinically mature.
3.5. Implications for Greek Physiotherapy Practice
From a Greek healthcare perspective, the findings highlight both opportunity and challenge. Conversational AI agents may support service continuity amid workforce constraints and geographic disparities, particularly in extending rehabilitation follow-up beyond urban clinical centers. However, meaningful implementation would require alignment with linguistic norms, professional practice standards, and European regulatory frameworks, including GDPR and the AI Act.
Importantly, the technological architectures underlying these systems vary in complexity and clinical risk profile, which has direct implications for their safe integration into Greek physiotherapy practice. Across the reviewed literature, rehabilitation-oriented conversational agents combine traditional dialogue management structures with emerging AI-driven reasoning, behavioural modelling, and sensing technologies.
Several dominant technological approaches can be identified:
- Motivational and behavioural models Conversation content is often driven by behaviour change frameworks; PANDORA was explicitly designed around Self Determination Theory to target autonomy, competence, and relatedness [19].
- LLMs with grounding and retrieval LLM based advisors are being prototyped with external knowledge conditioning and citation mechanisms to mitigate hallucinations while recommending exercises and OTC symptom relief [17].
- Sensor integration and robotics Systems combine conversational interfaces with motion sensors or robotic devices to monitor exercise performance and provide adaptive feedback in real time [18].
- Reinforcement learning and adaptive policies Research proposes reinforcement learning approaches to personalize coaching strategies and dialogue policies, aiming to optimize adherence outcomes over time [20].
Examples in the literature illustrate hybrid configurations, such as multimodal virtual coaches integrating behavioural dialogue models [12], motivational SDT-driven chatbots for Parkinson’s exercises [19], and LLM-based advisors conditioned on verifiable external sources [17].
Taken together, these technological choices suggest that implementation in Greece would likely require a phased and supervised integration model, where lower-risk, rule-based systems are adopted first, followed by more adaptive AI-driven approaches once appropriate oversight, validation, and regulatory safeguards are established.
3.6. Summary of Evidence
Conversational and text AI agents are used in physical rehabilitation, ranging from embodied virtual coaches and mobile chatbots to LLM-based advisors and robot-integrated systems. Studies report improved engagement, measurable quality of life gains in some trials, and high user satisfaction, but clinical validation and safety remain evolving.
4. Discussion
4.1. Principal Findings and Health System Context
This scoping review has identified a growing body of research on conversational AI agents in physical rehabilitation, particularly in applications such as exercise coaching, adherence support, patient education, and preliminary triage. While the evidence base is expanding, robust clinical evaluation and long-term outcome data remain limited. Importantly, the Greek healthcare context presents both opportunities and challenges for the adoption of these technologies.
The Greek healthcare system operates under a centralized structure, with the National Organization for the Provision of Health Services (EOPYY) acting as the principal statutory health insurance fund. EOPYY reimburses a range of healthcare services, including physiotherapy delivered by both public and contracted private practitioners. Under the Unified Health Benefits Regulation, insured individuals have access to services such as physiotherapy, occupational therapy, speech therapy, and psychotherapy, often with co-payments depending on provider contracts with EOPYY [5]. Despite recent primary care reforms, fee-for-service reimbursement persists for physiotherapy and other allied health services, although incentives for preventive and health promotion activities are being explored [10].
Physiotherapy remuneration and job satisfaction in Greece have been subject to longstanding structural challenges. A survey of self-employed physiotherapists indicated that many perceive current reimbursement models as insufficient relative to productivity, potentially affecting workforce retention and practice innovation [11]. Alongside reimbursement concerns, physiotherapists in Greece have demonstrated a willingness to adopt digital health modalities such as telerehabilitation, a trend accelerated by the COVID-19 pandemic. Nevertheless, many practitioners report the need for additional training and formal guidelines to support effective and safe remote practice [21].
4.2. Implications for Regulatory, Professional, and Educational Frameworks
The implementation of conversational AI in physiotherapy must be considered within national policy frameworks and professional practice standards. Greece is making progress in digital healthcare infrastructure, with initiatives such as the National eHealth Interoperability Framework aiming to support secure digital data exchange and the development of national electronic health records. These developments could provide a foundation for the integration of AI technologies into routine care pathways. However, Greece has not yet established mechanisms for prescribing digital therapeutics or reimbursing digital health applications, a domain that remains less developed compared with international models such as Germany’s DiGA initiative.
The integration of AI systems also raises regulatory considerations under the EU AI Act and the General Data Protection Regulation (GDPR). AI applications that influence clinical decision making or prescribe exercise regimens may be classified as high-risk, necessitating stringent requirements related to safety, transparency, and bias mitigation. Embedding these standards within Greek physiotherapy workflows will require collaborative governance involving professional associations, regulatory authorities, and health system planners.
4.3. Equity, Accessibility, and Workforce Capacity
Conversational AI has the potential to enhance access to physiotherapy services across Greece, particularly for populations in remote or underserved regions where workforce shortages are pronounced. Evidence from home healthcare initiatives indicates that physiotherapists constitute a substantial proportion of rehabilitative care delivered in community settings, highlighting the importance of distributed models of care. AI-enabled platforms, when designed inclusively and implemented with appropriate clinical oversight, could extend the reach of qualified clinicians while reducing travel and scheduling barriers for patients.
However, broader healthcare system pressures, such as high out-of-pocket expenditures and ongoing resource constraints, may attenuate both patient and provider uptake of novel digital tools. Greek patients contribute a significant proportion of total healthcare costs directly, while funding shortfalls at EOPYY can influence service availability and provider participation in public reimbursement schemes. Addressing these economic factors will be essential to ensuring equitable access to AI-supported rehabilitation services [11].
4.4. Research Gaps and Strategic Priorities
Although the existing literature on conversational AI in rehabilitation has established important foundations, substantial gaps remain. Future research should prioritize:
- Evaluate clinical effectiveness through robust controlled trials with standardized outcome measures.
- Assess safety, reliability, and algorithmic bias specifically for localized language contexts including Greek.
- Explore reimbursement models and policy incentives that support sustainable integration.
- Develop training curricula and professional standards for digital competency among physiotherapists.
- Engage patients and providers in co-design frameworks to ensure usability and ethical alignment.
Cross-disciplinary collaboration among rehabilitation scientists, AI engineers, health economists, and policymakers will be essential to realize the full potential of conversational AI within physiotherapy, both globally and in the Greek healthcare context [21].
5. Conclusions
Conversational AI agents represent a promising yet clinically immature technology in physical rehabilitation. Although feasibility, engagement, and usability findings are encouraging, robust evidence regarding long-term clinical effectiveness, safety validation, and standardized outcome measurement remains limited.
Future progress will depend on large-scale controlled trials, structured safety and escalation frameworks, improved trustworthiness of LLM-based systems, and adaptive personalization strategies that balance innovation with reliability. Equally important is the integration of these technologies into clearly defined care pathways with appropriate therapist oversight and regulatory compliance.
Within the Greek healthcare context, responsible adoption will require linguistic localization, professional governance, and alignment with European regulatory standards. With rigorous evaluation and phased implementation, conversational AI may evolve from experimental support tools to clinically embedded adjuncts in physiotherapy practice.
Appendix A
Appendix A1. PRISMA-ScR Checklist

Table A1.
PRISMA Extension for Scoping Reviews (PRISMA-ScR) Checklist.
| Section | Item | Description | Manuscript Location |
| Title | 1 | Identify the report as a scoping review | Title |
| Abstract | 2 | Structured summary | Abstract |
| Introduction | 3 | Rationale | Section 1 |
| Introduction | 4 | Objectives | Section 1 |
| Methods | 5 | Protocol and registration | Section 2 |
| Methods | 6 | Eligibility criteria | Section 2.1 |
| Methods | 7 | Information sources | Section 2.2 |
| Methods | 8 | Search strategy | Section 2.2 |
| Methods | 9 | Selection of sources | Section 2.3 |
| Methods | 10 | Data charting process | Section 2.4 |
| Methods | 11 | Data items | Section 2.4 |
| Results | 12 | Synthesis of results | Section 3 |
| Discussion | 13 | Summary of evidence | Section 4 |
| Discussion | 14 | Limitations | Section 4.4 |
| Discussion | 15 | Conclusions | Section 5 |
References
- Alowais, S. A.; Alghamdi, S. S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A. I.; Almohareb, S. N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.; Yami, M. S.; Albekairy, A. M. A pilot study of mobile artificial intelligence voice assistants in early knee osteoarthritis detection; TMR Publishing Group, 2023. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006, 3(2), 77–101. [Google Scholar] [CrossRef]
- Clusmann, J.; et al. Current applications and challenges in large language models for health care. Communications Medicine 2025, 5(1), Article 17. [Google Scholar] [CrossRef]
- Cross, M.; Smith, E.; Hoy, D.; Carmona, L.; Wolfe, F.; Vos, T.; Williams, G.; Gabriel, S.; March, L. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Annals of the Rheumatic Diseases 2014, 73(7), 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Regulation (EU) 2024/1689 laying down harmonised rules on artificial intelligence. Official Journal of the European Union 2024. [Google Scholar]
- Hong, Q. N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; Rousseau, M.-C.; Vedel, I. Mixed Methods Appraisal Tool (MMAT), version 2018; Canadian Intellectual Property Office, 2018. [Google Scholar]
- Ji, Z.; Lee, N.; Frieske, R.; Yu, T.; Su, D.; Xu, Y.; Ishii, E.; Bang, Y. J.; Madotto, A.; Fung, P. Survey of hallucination in natural language generation. ACM Computing Surveys 2023, 55(12), 1–38. [Google Scholar] [CrossRef]
- Lee, P.; Bubeck, S.; Petro, J. The application of large language models in medicine: A scoping review. iScience 2024, 27(5), 109935. [Google Scholar] [CrossRef]
- Meskó, B.; Topol, E. J. The imperative for regulatory oversight of large language models in healthcare. npj Digital Medicine 2025, 8(1), Article 15. [Google Scholar] [CrossRef]
- Thirunavukarasu, A. J.; et al. Large language models in medicine. Nature Medicine 2024, 30(6), 1526–1538. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Straus, S. E. & PRISMA Extension for Scoping Reviews (PRISMA-ScR) Checklist Group PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine 2018, 169(7), 467–473. [Google Scholar] [CrossRef] [PubMed]
- [1] H. Schlieter et al., Virtual Coaching for Home Rehabilitation - Evidence of an Empirical Study. Studies in health technology and informatics 2024, vol. 316, 147–151. [CrossRef]
- Dwyer, T. Use of an Artificial Intelligence Conversational Agent (Chatbot) for Hip Arthroscopy Patients Following Surgery. Arthroscopy, sports medicine, and rehabilitation 2023, vol. 5 2(no. 2), e495–e505. [Google Scholar] [CrossRef]
- Blasco, J.-M.; Roig-Casasús, S.; Igual-Camacho, C.; Díaz-Díaz, B.; Pérez-Maletzki, J. Conversational chatbot to promote adherence to rehabilitation after total knee replacement: implementation and feasibility. Archives of Physical Medicine and Rehabilitation 2022. [Google Scholar] [CrossRef]
- Griol, D.; Callejas, Z. Mobile Conversational Agents for Stroke Rehabilitation Therapy; June 2019; pp. 513–518. [Google Scholar] [CrossRef]
- Hocking, J.; Maeder, A. Motivational Embodied Conversational Agent for Brain Injury Rehabilitation; Apr 2021. [Google Scholar] [CrossRef]
- Almeida, R.; Sousa, H.; Cunha, L. F.; Guimarães, N.; Campos, R.; Jorge, A. Physio: An LLM-Based Physiotherapy Advisor. arXiv.org abs/2401.01825. 2024. [Google Scholar] [CrossRef]
- Lee, M. H.; Siewiorek, D. P.; Smailagic, A.; Bernardino, A.; Badia, S. B. i. Enabling AI and Robotic Coaches for Physical Rehabilitation Therapy: Iterative Design and Evaluation with Therapists and Post-Stroke Survivors; 15 June 2021. [Google Scholar] [CrossRef]
- Macedo, P.; Madeira, R. N.; Santos, P. A.; Mota, P. R.; Alves, B. R.; Pereira, C. A Conversational Agent for Empowering People with Parkinson’s Disease in Exercising Through Motivation and Support. Applied Sciences 2024, vol. 15(no. 1), 223–223. [Google Scholar] [CrossRef]
- Sivakumar, R. “CONVERSATIONAL AI AND REINFORCEMENT LEARNING FOR VIRTUAL COACHING IN PHYSIOTHERAPY”. Available online: https://cuestionesdefisioterapia.com/index.php/es/article/view/2920.
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A. N.; Kaiser, Ł.; Polosukhin, I. Attention is all you need. Advances in Neural Information Processing Systems 2017, 30, 5998–6008. [Google Scholar]
Figure 1.
PRISMA-ScR flow diagram illustrating identification, screening, eligibility, and inclusion of studies.
Figure 1.
PRISMA-ScR flow diagram illustrating identification, screening, eligibility, and inclusion of studies.
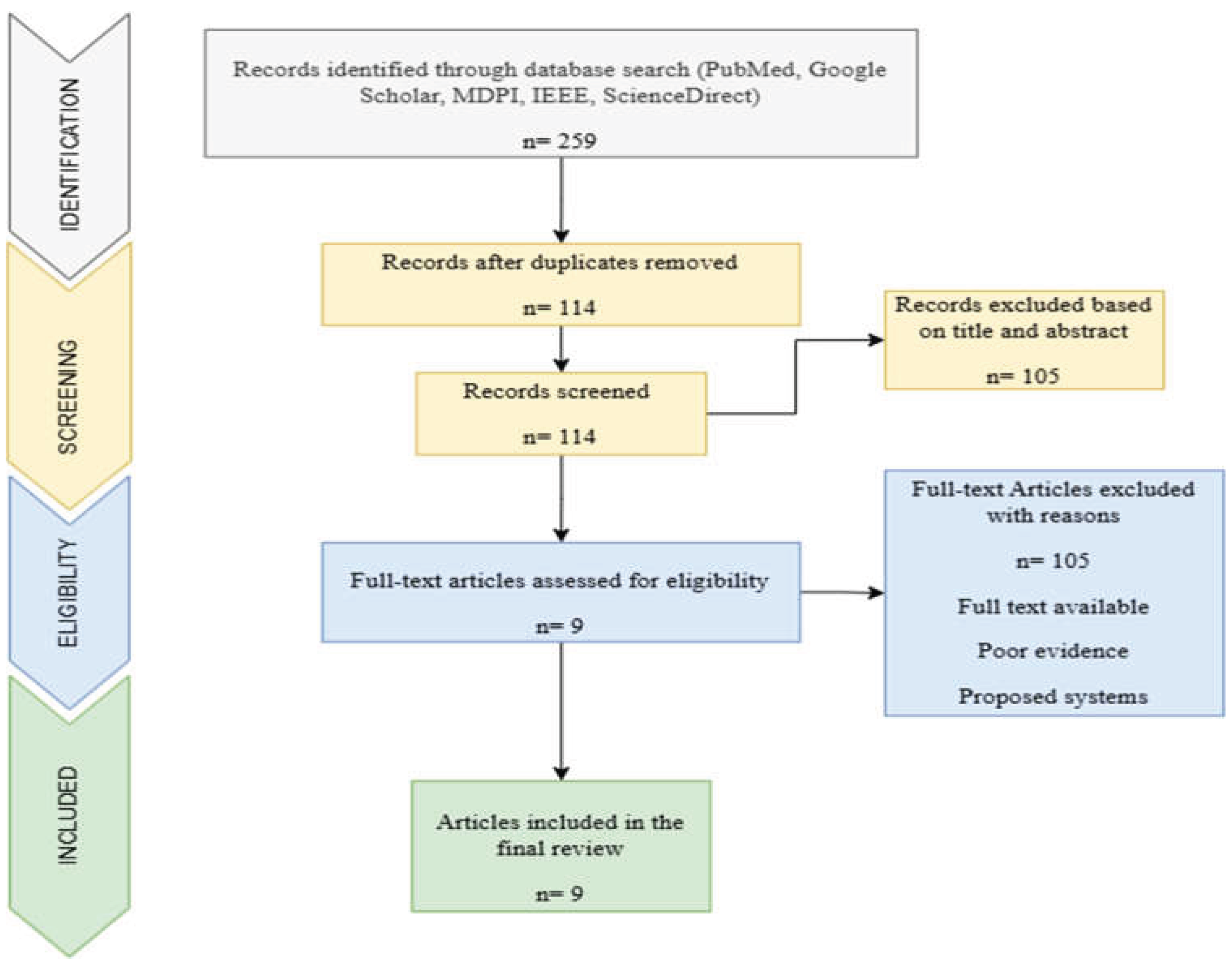
Table 1.
Types of Conversational AI Agents in Rehabilitation.
| AGENT CLASS | FORM AND INTERACTION MODE | TYPICAL USE CASES | EXAMPLE STUDY |
| EMBODIED VIRTUAL COACH | Avatar or animated agent with voice and/or text, multimodal interaction | Home exercise guidance, motivation, long-term adherence | Virtual coaching for older adults with QoL gains [12] |
| TEXT CHATBOTS AND SMS AGENTS | Rule-based or ML chat flows delivered by SMS, mobile app, or web chat | Postoperative follow-up, appointment triage, adherence prompts | Hip arthroscopy SMS agent "Felix" [13] ; knee replacement chatbot feasibility [14] |
| MOBILE CONVERSATIONAL THERAPY APPS | Multimodal app with conversational UI for cognitive and motor exercises | Stroke cognitive exercises, tailored therapy routines | Mobile stroke rehabilitation conversational app [15] |
| EMBODIED CONVERSATIONAL AGENTS FOR COGNITIVE REHAB | Dialogue systems tailored to cognitive impairments with personalization | Brain injury cognitive and motivational support | Motivational ECA for brain injury rehabilitation [16] |
| LLM-BASED PHYSIOTHERAPY ADVISORS | Large language models with knowledge grounding and retrieval | Initial triage, exercise recommendations, citing sources | Physio LLM-based advisor prototype [17] |
| ROBOT-INTEGRATED AI COACHES | Conversational front end combined with sensors/robotics and automated monitoring | Real-time exercise guidance and performance feedback | Design and stakeholder evaluation of AI/robotic coaches [18] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



