Submitted:
26 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Background: Right anterior thoracotomy aortic valve replacement (RAT-AVR) is an established minimally invasive alternative to conventional sternotomy; however, published series predominantly reflect late-experience data from specialised centres. Real-world outcomes during early adoption remain underreported. Methods: We describe a contemporary operative technique for RAT-AVR and report early outcomes from a consecutive single-surgeon cohort undergoing isolated surgical aortic valve replacement between 2015 and 2025. Pre-operative imaging protocols, cannulation strategies, myocardial protection techniques, and valve implantation methods are detailed. Peri-operative characteristics and early clinical outcomes were analysed using prospectively collected registry data. Results: A total of 156 consecutive patients underwent RAT-AVR. Median age was 70 years, and 72% were male. Peripheral femoral cannulation was used in 96% of cases. Median cardiopulmonary bypass and cross-clamp times were 109 and 79 minutes, respectively. Conversion to sternotomy occurred in two patients (1%). Thirty-day mortality was 1.3%. Rates of stroke (0%), acute kidney injury (3%), and reoperation for bleeding (4%) were low. A broad range of valve sizes (19–27 mm) and prosthesis types were implanted without limitation imposed by the approach. Conclusions: In this consecutive single-surgeon series, including the learning phase of adoption, RAT-AVR was integrated safely into routine practice with favourable early outcomes. This approach represents a reproducible and pragmatic minimally invasive option for isolated surgical aortic valve replacement.
Keywords:
right anterior thoracotomy
; minimally invasive cardiac surgery
; aortic valve replacement
; learning curve
; femoral cannulation
; surgical technique
; registry data
; cardiopulmonary bypass
1. Introduction
Median sternotomy has traditionally been the standard surgical approach for cardiac surgical operations, offering reliable exposure and reproducibility across a broad range of cardiac procedures. However, as early as the 1990s, advances in cardiopulmonary bypass technology, imaging, instrumentation, and peri-operative care stimulated increasing interest in minimally invasive cardiac surgery. In isolated aortic valve replacement (AVR) procedures, where surgical access is limited to the aortic valve and root, minimally invasive approaches offer the potential to reduce surgical trauma while maintaining procedural safety and durability [1].
Several minimally invasive strategies for surgical AVR have since been described, including upper hemi-sternotomy, right anterior thoracotomy, and more recently, multi-port endoscopic or robotic-assisted techniques [1,2]. Concurrently, the widespread adoption of transcatheter aortic valve implantation (TAVI) has reshaped patient expectations and referral patterns, with increasing emphasis on reduced access trauma, faster recovery, and early quality-of-life benefits. As a result, there is growing interest in surgical AVR techniques that minimise invasiveness while preserving the long-term advantages of a surgical prosthesis, particularly in younger or low-risk patients and in those with anatomical features unsuitable for transcatheter intervention [3,4].
Right anterior thoracotomy AVR (RAT-AVR) is one such minimally invasive surgical approach that avoids median sternotomy while providing direct access to the aortic valve. Reported series have demonstrated favourable early and mid-term outcomes, including low mortality and acceptable cardiopulmonary bypass and cross-clamp times [5,6,7]. Despite these results, uptake of RAT-AVR has been variable, with ongoing concerns regarding patient selection, learning curve, and integration into established surgical practice [8,9]. Furthermore, many published series originate from highly specialised centres, limiting insight into real-world adoption during the early phases of implementation [5,7].
In this study, we describe our contemporary RAT-AVR technique, refined over a ten-year period, and report early outcomes from a consecutive single-surgeon cohort of 156 patients. This series includes the initial adoption and learning phase of the technique within a mature cardiothoracic surgical practice. The objectives of this study are to present a reproducible operative strategy using predominantly standard cardiac surgical instrumentation, to evaluate peri-operative and early clinical outcomes, and to assess the feasibility and safety of integrating RAT-AVR into routine surgical practice.
2. Materials and Methods
Operative Technique
Pre-operative Assessment and Patient Selection
All patients undergo comprehensive pre-operative evaluation in accordance with standard cardiac surgical practice. Trans-thoracic echocardiography, coronary artery assessment, and routine laboratory investigations are performed to confirm the indication for isolated aortic valve replacement and to exclude concomitant pathology requiring alternative surgical access. Patients considered for RAT-AVR undergo routine contrast-enhanced computed tomography (CT) aortography extending from the thoracic inlet to the femoral vessels. This imaging is critical for procedural planning. Particular attention is paid to the spatial relationship of the ascending aorta relative to the midline, as this directly influences exposure. Optimal access is generally achieved when at least 50% of the ascending aorta lies to the right of the midline at the level of the pulmonary artery bifurcation. Additional factors, including anterior–posterior depth of the ascending aorta and chest wall morphology, are incorporated into surgical planning. The same CT study is used to assess femoral and distal aortic anatomy to determine suitability for peripheral arterial cannulation.
Anaesthesia and Positioning
General anaesthesia is administered with standard monitoring, including radial arterial pressure monitoring, large-bore internal jugular venous catheterisation, urinary catheterisation, and external defibrillation pads. A single-lumen endotracheal tube is routinely used, as single-lung ventilation is not required. Patients are positioned supine with a slight leftward tilt, typically achieved using a rolled towel beneath the right scapula. This manoeuvre rotates the ascending aorta anteriorly and optimises exposure through the limited thoracotomy incision.
Cannulation Strategy
Cardiopulmonary bypass is most commonly established using peripheral femoral arterial and venous cannulation. Prior to thoracic entry, the common femoral artery and vein are surgically exposed through a 2-4 cm oblique incision. Purse-string sutures are placed in both vessels to facilitate cannulation. After systemic heparinisation, femoral cannulation is performed using the Seldinger technique under transoesophageal echocardiographic guidance to confirm correct guidewire and cannula positioning. Central arterial or venous cannulation may be employed selectively when clinically indicated, such as when the common femoral artery is heavily diseased.
Thoracic Exposure
A 4 to 8 cm skin incision is made over the superior border of the right third rib, extending laterally from the sternal edge (Figure 1). The right internal mammary artery and vein are identified, controlled with clips, and divided. To mobilise the right 3rd rib and optimise exposure, the edge of the sternal body is divided adjacent to the 3rd right sterno-costal junction using an oscillating saw. A V-shaped osteotomy is created to allow stable re-approximation at closure. The pleural cavity is entered, and soft tissue and rib retractors are positioned. The right lung is gently retracted laterally using a moist pack to expose the mediastinum. Mediastinal fat overlying the pericardium is excised, and the pericardium is opened longitudinally over the ascending aorta.
Following initiation of cardiopulmonary bypass and cooling to 34 °C, pericardial retraction sutures are placed and exteriorised through the thoracotomy incision. These sutures elevate and stabilise the ascending aorta while drawing it toward the operative field, substantially improving exposure for cross-clamping and aortotomy.
Myocardial Protection and Cross-Clamping
A left ventricular vent is inserted via the right superior pulmonary vein. An antegrade cardioplegia cannula is placed in the ascending aorta. A suitable plane for cross-clamping is developed using blunt dissection. A flexible cross-clamp is preferred in our practice, as it can be shaped to accommodate the restricted access and introduced without obstructing the operative field (Figure 2). Alternative low-profile clamps, including Chitwood-type clamps, may be used depending on surgeon preference and patient anatomy. Following cross-clamp application, myocardial arrest is achieved with antegrade long-acting cardioplegia, typically modified Del-Nido solution. In patients with more than mild aortic regurgitation, direct ostial cardioplegia is administered to ensure adequate myocardial protection, particularly in the setting of left ventricular hypertrophy or anticipated long aortic clamp times.
Aortic Valve Exposure and Implantation
A transverse or oblique aortotomy is performed. Aortic retraction sutures are placed to provide a direct, coaxial (“down-the-barrel”) view of the aortic valve (Figure 3). This orientation facilitates conventional valve excision and annular debridement. Several technical considerations are specific to this approach. Meticulous attention is paid to minimising calcific debris spillage, as assistant access for suction is limited. Annular sutures adjacent to the right coronary sinus can be technically more challenging and are therefore placed early in the sequence rather than deferred.
Valve implantation is performed using the surgeon’s standard technique. The thoracotomy approach does not impose restrictions on prosthesis type or size.
Closure
Following valve implantation, the aortotomy is closed with 5/0 polypropylene suture in a single continuous layer and rewarming is initiated. A right ventricular pacing wire and pericardial drain are positioned prior to cross-clamp removal, as exposure becomes more limited once cardiac activity resumes. These are exteriorised through a separate stab incision. After adequate reperfusion, patients are weaned from cardiopulmonary bypass and decannulated, with meticulous attention to haemostasis at both central and peripheral access sites. The pericardium is closed.
The third rib is re-approximated to the sternum using a figure-of-eight heavy polyglactin braided suture to restore chest wall stability. The internal mammary vessels are re-inspected to confirm haemostasis. All incisions are closed in layers with absorbable sutures. A single-shot intercostal nerve block with a long-acting local anaesthetic (e.g., ropivacaine) is administered prior to skin closure to facilitate postoperative analgesia and early extubation.
Research Methods
We conducted a retrospective observational cohort study to evaluate the safety, feasibility and short-term results of right anterior thoracotomy aortic valve replacement (RAT-AVR). All consecutive patients who underwent isolated surgical AVR via a right anterior thoracotomy performed by a single surgeon (C.H.Y) at University Hospital Geelong or St John of God Geelong Hospital, Victoria, Australia, between January 2015 and November 2025 were included. Patients undergoing concomitant cardiac procedures or requiring alternative access were excluded.
This study retrospectively analysed de-identified data of the single surgeon’s patient records within from the Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) Cardiac Surgery Database, a binational clinical quality registry that has prospectively collected operative and outcome data for over two decades as part of a structured quality assurance program [10]. The ANZSCTS Database Program has been described previously and operates under standing Human Research Ethics Committee approval for data collection and governance. The present analysis involved only pre-existing, non-identifiable registry data and did not involve direct patient contact or intervention. Use of these data for secondary research purposes was conducted under the governance framework of the ANZSCTS registry and existing institutional oversight. Continuous variables are presented as median with interquartile range (IQR), and categorical variables as frequency and percentage. Given the descriptive nature of this consecutive cohort study, no comparative hypothesis testing was performed. Statistical analyses were conducted using R software (version 4.3.0, R Core Team, Vienna, Austria).
3. Results
A total of 156 patients underwent isolated aortic valve replacement via right anterior thoracotomy during the study period. Baseline demographic and clinical characteristics are summarised in Table 1. The cohort had a median age of 70 years, with a predominance of male patients (72%). The median body mass index was 28.9 kg/m², with most patients classified as overweight or obese. A significant proportion of patients had a history of smoking (44%). Co-morbidities were otherwise typical of a contemporary surgical AVR population, including diabetes mellitus (19%), chronic lung disease requiring inhalers (13%), and prior cerebrovascular events (6%). Five patients (3%) had a pre-existing permanent pacemaker.
Pre-operative echocardiographic characteristics are detailed in Table 2. Severe aortic stenosis was the most common primary indication for surgery, present in 81% of patients, while 19% had predominant severe aortic regurgitation. In patients with significant aortic regurgitation, ostial cardioplegia was delivered without difficulty, and no issues related to myocardial protection were observed. Valve pathology was most frequently idiopathic calcific degeneration (69%), followed by bicuspid aortic valve disease (28%). Isolated cases included failed transcatheter aortic valve implantation, active infective endocarditis, and rheumatic valve disease.
Intra-operative details are summarised in Table 3. Cardiopulmonary bypass was established using peripheral cannulation in the vast majority of cases, while central arterial and/or venous cannulation was employed selectively when required, demonstrating the feasibility of both strategies within this approach. Median cardiopulmonary bypass time was 109 minutes, and median aortic cross-clamp time was 79 minutes. There was a trend toward reduction in cross-clamp and CPB time after the first 50 cases (data not shown). A wide range of prosthetic valve sizes, from 19 mm to 27 mm, and multiple valve types were successfully implanted through the right anterior thoracotomy exposure (Figure 4), indicating that valve selection was not constrained by the surgical approach.
Early outcomes following right anterior thoracotomy AVR were favourable, with low rates of peri-operative morbidity. Detailed recovery metrics and peri-operative complications are outlined in Table 4. Conversion to sternotomy occurred in two patients (1%). Causes were bleeding from the left atrial appendage related to left ventricular vent placement and iatrogenic Type A aortic dissection caused by femoral cannulation of a diseased femoral vessel. Six patients (4%) required return to theatre during the index admission, most commonly for evacuation of retained haemothorax.
Post-operative recovery was characterised by early ventilator weaning and relatively short intensive care and hospital stays. Median ventilation time was 7.9 hours, with most patients extubated on the day of surgery. Median ICU length of stay was 47.8 hours, and median hospital length of stay was 6 days. Chest drain output in the first four hours was low, with a median blood loss of 130 mL. Blood product transfusion was required in only 17% of patients. Minor post-operative complications were infrequent, with low rates of new renal dysfunction (3%) or transient neurological events (1%). Complications related to peripheral cannulation were uncommon, with a low incidence of access-site seroma or infection.
There were two deaths within 30 days of surgery (1.3%). One occurred in a high-risk octogenarian female patient who had been declined trans-catheter intervention for anatomical reasons and subsequently developed refractory diastolic heart failure in the immediate post-operative period. The second death occurred suddenly after hospital discharge; coronial post-mortem examination did not identify a procedural cause, and the event was presumed to be arrhythmic.
4. Discussion
The present series demonstrates that RAT-AVR can be introduced safely into routine surgical practice, with low morbidity and mortality and without the need for highly restrictive patient selection beyond standard anatomical suitability for minimally invasive access. Importantly, these outcomes were achieved in a consecutive single-surgeon cohort that includes the early learning phase of adoption, providing insight into real-world implementation rather than results derived from late-experience or highly selected populations.
Patient selection, particularly with respect to aortic anatomy, is frequently cited as a potential limitation of RAT-AVR. While a rightward position of the ascending aorta facilitates exposure, our experience suggests that this criterion should be viewed as a guiding consideration rather than an absolute exclusion. With systematic pre-operative CT assessment and the routine use of intra-operative adjuncts such as strategic pericardial retraction sutures, satisfactory exposure was achievable in the majority of patients referred for isolated AVR, in keeping with prior reports [5,8]. Notably, elevated body mass index and a high prevalence of smoking history did not preclude successful completion of the procedure in this cohort.
Peripheral femoral cannulation was used in most cases, with central cannulation employed selectively when clinically indicated. Access-site complications were uncommon, an observation of particular relevance given ongoing concerns regarding groin morbidity associated with peripheral bypass strategies. These findings are consistent with existing data demonstrating that femoral cannulation can be performed safely when supported by careful imaging, appropriate patient selection, and meticulous surgical technique [11,12].
A further strength of RAT-AVR lies in its technical versatility. The approach permits a direct, coaxial view of the aortic valve and allows valve excision and implantation to be performed using standard surgical instruments and familiar techniques. In this series, a broad range of valve sizes (19–27 mm) and prosthesis types were implanted without apparent limitation imposed by the access strategy. This flexibility is particularly relevant in contemporary surgical AVR practice, where prosthesis selection remains central to long-term outcomes [4].
Although cardiopulmonary bypass and cross-clamp times were modestly longer than those typically reported for conventional sternotomy AVR, this finding is consistent with minimally invasive series and reflects inclusion of the early learning phase [1,5,6]. Prior analyses have suggested a learning curve of approximately 30–50 cases for minimally invasive AVR [7,9]. In our experience, operative efficiency improved progressively after the initial cases, supporting the feasibility of structured adoption within an established surgical practice.
Early outcomes in this cohort compare favourably with contemporary benchmarks for isolated surgical AVR performed via conventional sternotomy and other minimally invasive approaches [2,3,13]. Mortality was low, conversion to sternotomy was uncommon, and rates of major complications—including stroke, renal dysfunction, bleeding, and re-intervention—were consistent with those reported in established RAT-AVR series [1,5,6].Together, these findings support the procedural safety of the approach when performed in appropriately selected patients, even during the initial phases of adoption.
Recent ANZSCTS reports of isolated surgical aortic valve replacement performed predominantly via conventional sternotomy demonstrate early mortality rates typically ranging between 1-2%, with stroke rates of approximately 1–2%, acute kidney injury rates of 3–5%, transfusion rates of 30-45%, and re-operation for bleeding between 4–6% [13]. In the present RAT-AVR cohort, 30-day mortality was 1.3%, with no permanent stroke events, acute kidney injury in 3%, transfusion rate of 17% and return to theatre in 4%. While direct statistical comparison is not possible in the absence of risk adjustment or matched controls, these findings suggest that early outcomes during adoption of the RAT-AVR approach fall within reported national benchmark ranges.
Several limitations should be acknowledged. This study is retrospective and lacks a contemporaneous sternotomy comparator group. Outcomes were not risk-adjusted, and follow-up was limited to early post-operative outcomes. Longer-term durability, functional recovery, and patient-reported outcomes were not assessed. While the single-surgeon nature of the series enhances internal consistency, it may limit generalisability across different institutional settings.
5. Conclusions
In summary, right anterior thoracotomy AVR represents a safe, versatile, and reproducible minimally invasive approach to isolated surgical aortic valve replacement. In this consecutive single-surgeon experience, favourable early outcomes were achieved across a broad patient population, including during the learning phase of adoption. These findings support RAT-AVR as a pragmatic minimally invasive strategy that can be integrated into contemporary cardiothoracic surgical practice without reliance on specialised technology or excessively restrictive patient selection.
Author Contributions
Conceptualization, D.S. and C.H.Y.; methodology, D.S. and C.H.Y.; software, D.S.; formal analysis, D.S.; data curation, D.S., A.M., P.J. and C.H.Y.; writing—original draft preparation, D.S.; writing—review and editing, D.S., A.M., P.J. and C.H.Y; supervision, C.H.Y.; project administration, C.H.Y. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
This study analysed de-identified data from the ANZSCTS Cardiac Surgery Database, which operates under standing HREC approval for data collection and governance. In accordance with the Australian National Statement on Ethical Conduct in Human Research, secondary analysis of non-identifiable registry data does not require additional ethics approval.
Informed Consent Statement
Patient consent was waived as the study involved analysis of de-identified registry data only.
Data Availability Statement
No new data were created as part of this study.
Conflicts of Interest
C.H.Y. serves as a surgical proctor for Medtronic and Artivion and as an Intuitive Surgical proctor for robotic thoracic surgery. The other authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AVR | Aortic valve replacement |
| RAT-AVR | Right anterior thoracotomy aortic valve replacement |
| CT | Computed tomography |
References
- Shehada, S.-E.; Elhmidi, Y.; Mourad, F.; Wendt, D.; El Gabry, M.; Benedik, J.; Thielmann, M.; Jakob, H. Minimal access versus conventional aortic valve replacement: a meta-analysis of propensity-matched studies. Interact Cardiovasc Thorac Surg 2017, 25, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Li, D.; Cheng, N.; Li, L.; Dong, S.; Shen, H.; Zhang, L.; Jiang, S. Comparative efficacy of totally thoracoscopic, mini-thoracotomy, and mini-sternotomy approaches in aortic valve replacement. Sci Rep 2024, 14, 17625. [Google Scholar] [CrossRef] [PubMed]
- Jahangiri, M.; Bilkhu, R.; Embleton-Thirsk, A.; Dehbi, H.-M.; Mani, K.; Anderson, J.; Avlonitis, V.; Baghai, M.; Birdi, I.; Booth, K.; et al. Surgical aortic valve replacement in the era of transcatheter aortic valve implantation: a review of the UK national database. BMJ Open 2021, 11, e046491. [Google Scholar] [CrossRef] [PubMed]
- Praz, F.; Borger, M.A.; Lanz, J.; Marin-Cuartas, M.; Abreu, A.; Adamo, M.; Ajmone Marsan, N.; Barili, F.; Bonaros, N.; Cosyns, B.; et al. 2025 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2025, 46, 4635–4736. [Google Scholar] [CrossRef] [PubMed]
- Glauber, M.; Gilmanov, D.; Farneti, P.A.; Kallushi, E.; Miceli, A.; Chiaramonti, F.; Murzi, M.; Solinas, M. Right anterior minithoracotomy for aortic valve replacement: 10-year experience of a single center. J Thorac Cardiovasc Surg 2015, 150, 548–556.e2. [Google Scholar] [CrossRef] [PubMed]
- Gilmanov, D.; Miceli, A.; Ferrarini, M.; Farneti, P.; Murzi, M.; Solinas, M.; Glauber, M. Aortic valve replacement through right anterior minithoracotomy: can sutureless technology improve clinical outcomes? Ann Thorac Surg 2014, 98, 1585–1592. [Google Scholar] [CrossRef] [PubMed]
- Fatehi Hassanabad, A.; King, M.A.; Karolak, W.; Dokollari, A.; Castejon, A.; de Waard, D.; Smith, H.N.; Holloway, D.D.; Adams, C.; Kent, W.D.T. Right anterior mini thoracotomy approach for aortic valve replacement. Innovations (Phila) 2024, 19, 494–508. [Google Scholar] [CrossRef] [PubMed]
- Martella, A.; Kernis, S.; Curiale, S.; Ndubizu, U.; Cichelli, J. Right thoracotomy minimally invasive AVR: use of preoperative CT scan to plan incision. J Cardiothorac Surg 2015, 10, A28. [Google Scholar] [CrossRef]
- Masuda, T.; Nakamura, Y.; Ito, Y.; Kuroda, M.; Nishijima, S.; Okuzono, Y.; Hirano, T.; Hori, T. The learning curve of minimally invasive aortic valve replacement for aortic valve stenosis. Gen Thorac Cardiovasc Surg 2020, 68, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.; Williams-Spence, J.; Shardey, G.C.; Smith, J.A.; Reid, C.M. The Australian and New Zealand Society of Cardiac and Thoracic Surgeons Database Program – two decades of quality assurance data. Heart Lung Circ 2019, 28, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Ramchandani, M.; Al Jabbari, O.; Abu Saleh, W.K.; Ramlawi, B. Cannulation strategies and pitfalls in minimally invasive cardiac surgery. Methodist Debakey Cardiovasc J 2016, 12, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Lamelas, J.; Williams, R.F.; Mawad, M.; LaPietra, A. Complications associated with femoral cannulation during minimally invasive cardiac surgery. Ann Thorac Surg 2017, 103, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Mundy, J; Williams-Spence, J; Tran, L; Solman, N; McLaren, J; Marrow, N; Ong, J; Reid, C. The Australian and New Zealand Society of Cardiac and Thoracic Surgeons’ Cardiac Surgery Database Program Annual Report 2023. Report No. 17. September 2024. [Google Scholar]
Figure 1.
Standard skin markings, with superior border of 3rd rib marked.
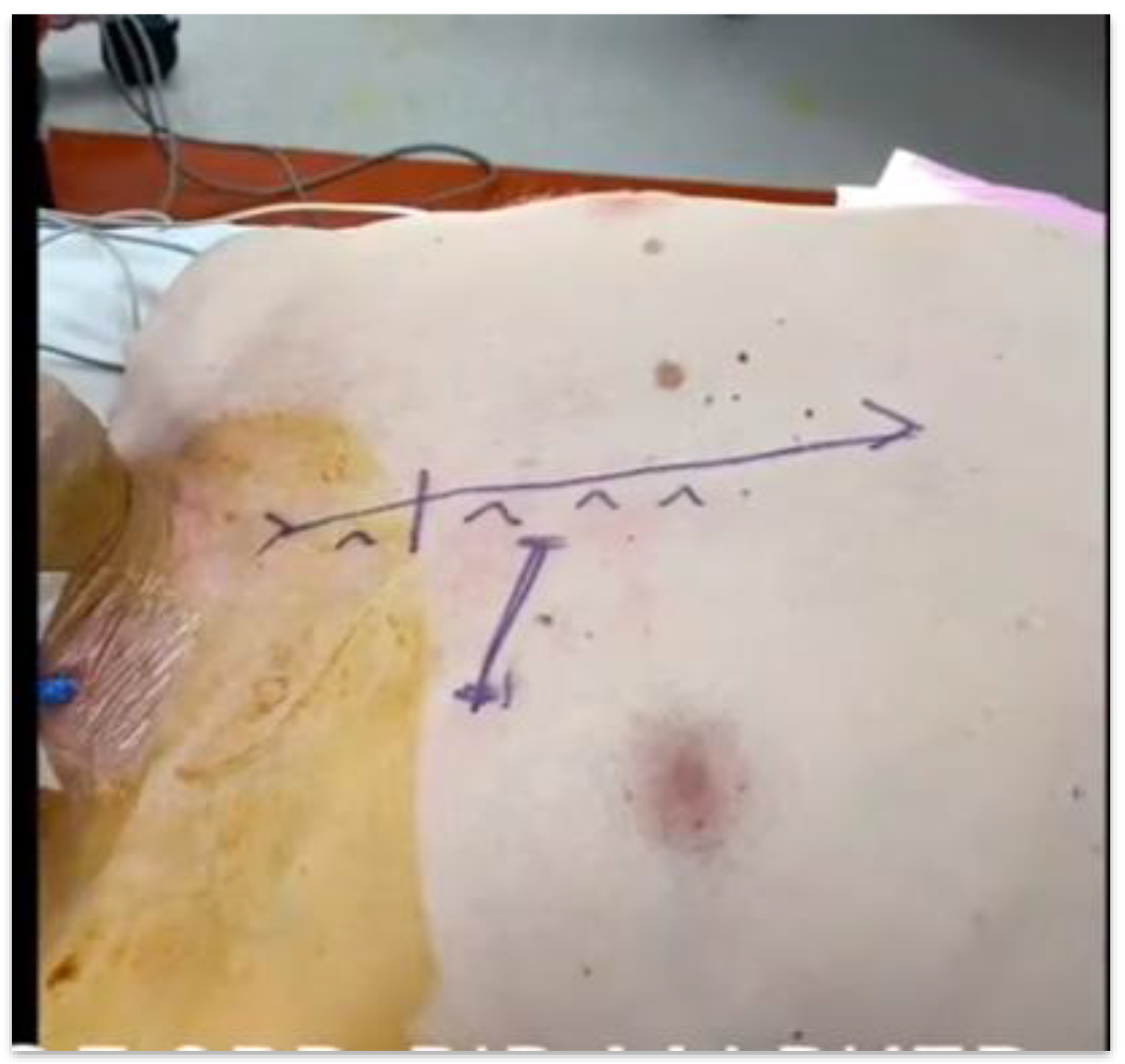
Figure 2.
Surgical field at the time of cross-clamp, demonstrating position of cross-clamp, aortic root vent, and right superior pulmonary vein vent.
Figure 2.
Surgical field at the time of cross-clamp, demonstrating position of cross-clamp, aortic root vent, and right superior pulmonary vein vent.
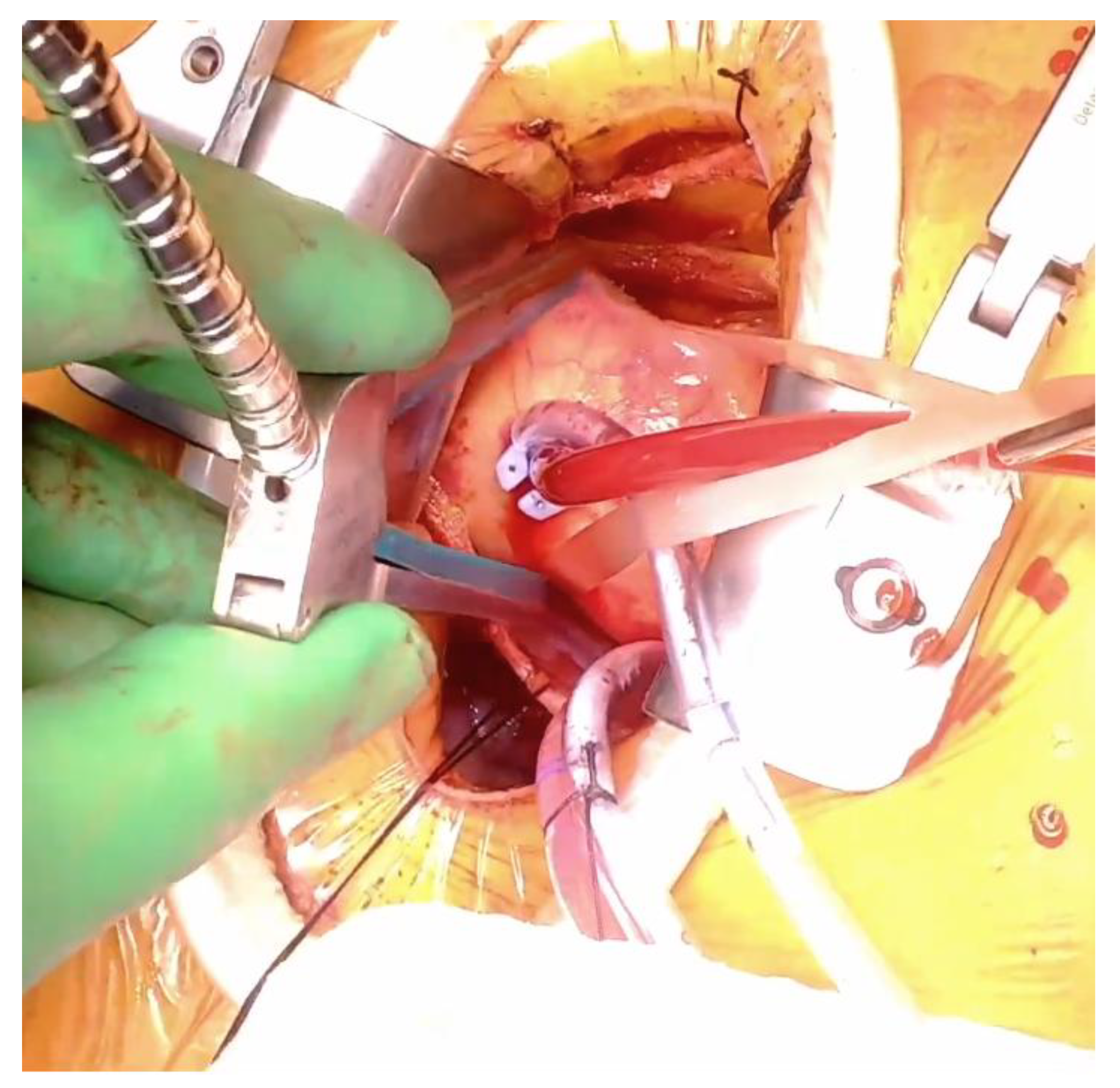
Figure 3.
View of the aortic valve after aortic retraction sutures are placed.
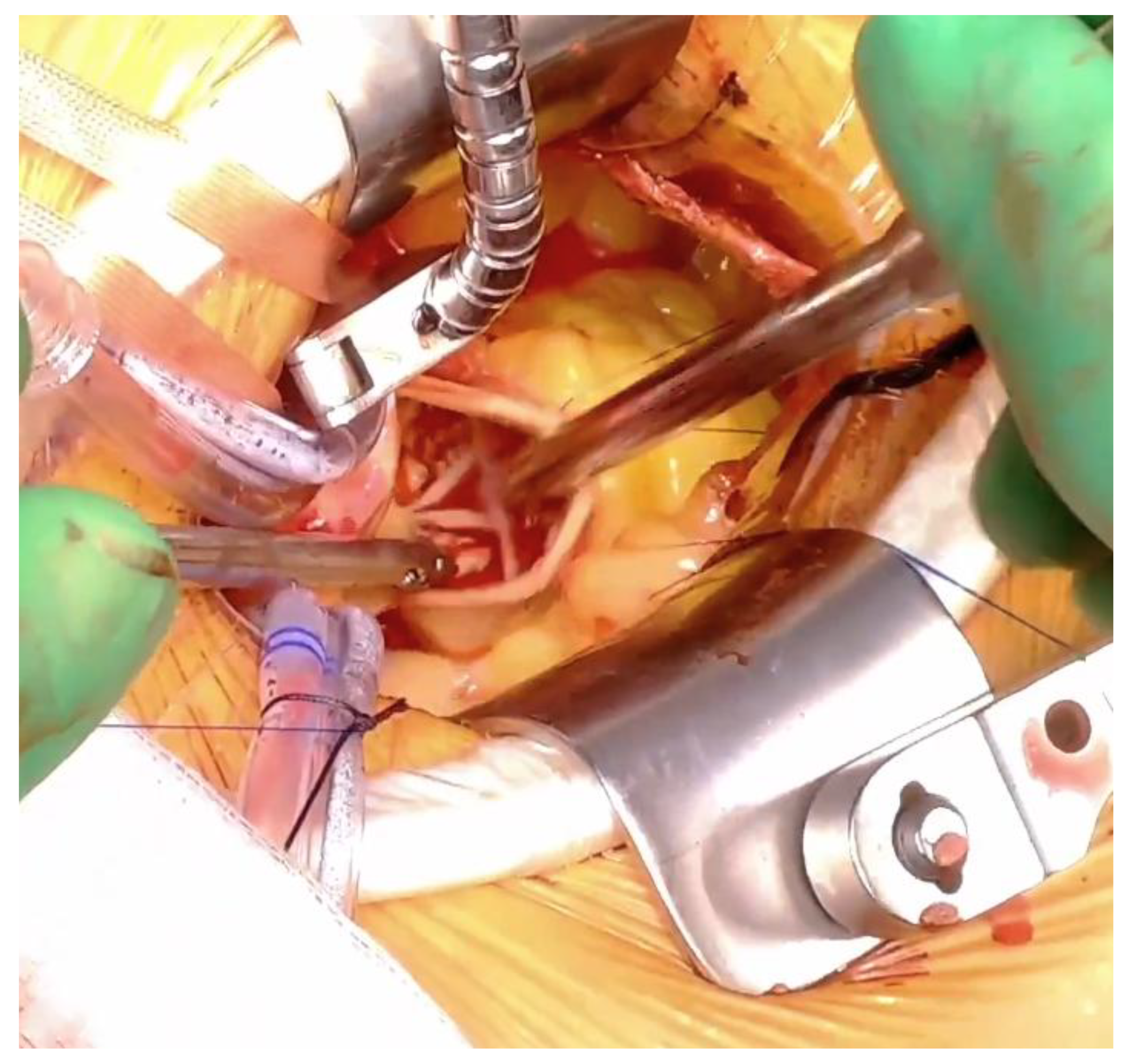
Figure 4.
Summary of valve sizes and valve types used throughout the stud.
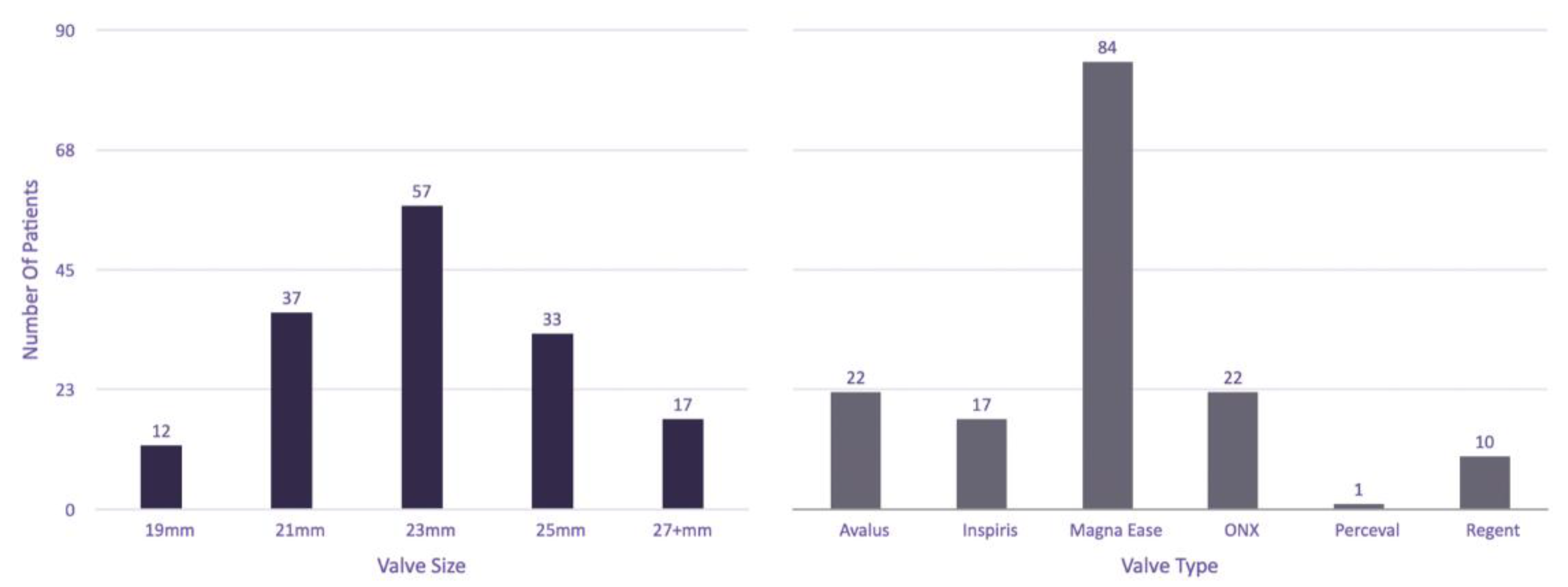

Table 1.
Patient characteristics of all 156 patients.
| Demographics | |
|---|---|
| Age | 70.0 [62.0 - 75.0] |
| Male Gender | 112/156 (72%) |
| BMI | 28.9 [25.4 - 31.8] |
| Smoking History | 68/156 (44%) |
| Significant Comorbidities | |
| Lung Disease (Asthma or COPD) | 21/156 (13%) |
| Diabetes | 30/156 (19%) |
| Previous Stroke or TIA | 10/156 (6%) |
| Peripheral Vascular Disease | 5/156 (3%) |
| Current Infective Endocarditis | 1/156 (1%) |
| Immunosuppressive therapy | 6/156 (4%) |
| Permanent Pacemaker | 5/156 (3%) |
Table 2.
Preoperative echocardiography findings.
| Haemodynamics | N = 156 |
|---|---|
| Aortic Valve Primary Pathology | |
| Severe AS | 127/156 (81%) |
| Severe AR | 29/156 (19%) |
| Pathogenesis | |
| Idiopathic Calcific | 108/156 (69%) |
| Bicuspid | 45/156 (28%) |
| Failed TAVR | 1/156 (1%) |
| Active IE | 1/156 (1%) |
| Rheumatic | 1/156 (1%) |
| Pre-operative Ejection Fraction | |
| Normal | 118/156 (76%) |
| Mild Reduction | 28/156 (18%) |
| Moderate Reduction | 7/156 (4%) |
| Severe Reduction | 3/156 (2%) |
Table 3.
Cardiopulmonary bypass details.
| Intra-operative Characteristic | N = 156 |
|---|---|
| Cross-Clamp Time | 79.0 [69.0 – 91.5] |
| CPB Time | 109 [98.0 – 129.5] |
| Arterial Cannulation Site | |
| Central | 7/156 (4%) |
| Femoral | 149/156 (96%) |
| Venous Cannulation Site | |
| Central | 2/156 (1%) |
| Femoral | 154/156 (99%) |
Table 4.
Post-operative recovery and complications.
| Characteristic | N = 156 |
|---|---|
| Major Outcomes | |
| 30-day mortality | 2/156 (1%) |
| Return to Theatre | 6/156 (4%) |
| Conversion to Sternotomy | 2/156 (1%) |
| Length of Stay | |
| Ventilation Time (Hours) | 7.9 [5.4 - 16.5] |
| ICU Length of Stay (Hours) | 47.8 [28.4 - 72.2] |
| Hospital Length of Stay (Days) | 6.0 [5.0 - 8.0] |
| Bleeding and Transfusion | |
| ICC output first 4 hours (ml) | 130.0 [90.0 - 190.0] |
| Any Blood Transfusion | 27/156 (17%) |
| Complications | |
| New AKI | 4/156 (3%) |
| TIA | 2/156 (1%) |
| Stroke (Permanent) | 0/156 |
| New AF | 38/156 (24%) |
| PPM Insertion | 10/156 (6%) |
| Groin Seroma or Infection | 3/156 (2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



