
Submitted:
19 February 2026
Posted:
27 February 2026
You are already at the latest version
Abstract
Background/Objectives: Kidney injury is a frequent complication of multiple myeloma (MM) and monoclonal gammopathies. Podocyte stress markers, such as urinary nephrin and podocin, have been studied in other renal diseases but their utility in paraprotein-related kidney disease remains unclear. This pilot study investigated the association of urinary nephrin and podocin levels with albuminuria and biopsy-proven podocytopathy in patients paraprotein-related diseases. Methods: We retrospectively analyzed 75 patients with plasma cell dyscrasias including MM and MGRS and 11 healthy controls. Urinary podocin and nephrin mRNA levels were measured using qPCR, and urinary podocin protein levels were quantified via ELISA. Associations were assessed between these biomarkers and urinary pro-tein-to-creatinine ratio (uPCR), albumin-to-creatinine ratio (uACR), and histologically confirmed podocytopathia. Diagnostic performance was evaluated using Receiver Op-erating Characteristic (ROC) analysis. Results: Higher urinary podocin protein levels were significantly associated with lower uACR (p=0.007) and uPCR (p=0.026). Neither podocin nor nephrin mRNA showed sig-nificant associations with proteinuria metrics. ROC analysis indicated that podocin ELISA (AUC=0.350) and podocin mRNA (AUC=0.510) lacked diagnostic accuracy for predicting renal involvement. The presence of urinary tract infection (UTI) was a sig-nificant confounder, leading to increased levels of podocin and nephrin mRNA. Conclusions: Urinary podocin shows a trend toward elevation in MM/MGRS patients with histological podocyte injury. The study revealed an unexpected inverse association between urinary podocin and albuminuria, suggesting complex release kinetics or stage mismatches in this population. Given the confounding effect of UTIs and the pilot na-ture of this study, further research is required to validate these podocyte proteins as prognostic biomarkers in paraprotein-related kidney disease.
Keywords:
multiple myeloma
; paraproteinemias
; podocytes
; intracellular signaling peptides and proteins
; biomarkers
1. Introduction
Kidney injury is a well-recognized complication of monoclonal gammopathies and multiple myeloma (MM) [1,2]. While tubular injury from free light chains and cast nephropathy is often the focus, glomerular lesions—especially podocyte injury, or podocytopathy—contribute to proteinuria and renal dysfunction in this context [3,4,5,6]. Distinguishing glomerular damage with podocyte injury from purely tubular injury has diagnostic and prognostic implications and might allow for non-invasive longitudinal evaluation of renal response to treatment.
Podocyte-derived biomarkers detectable in urine, such as nephrin and podocin, offer a potential noninvasive window into glomerular injury [7,8,9]. Nephrin, a transmembrane protein of the slit diaphragm, plays a central role in filtration barrier integrity and intracellular signaling, and perturbations in nephrin expression or phosphorylation are linked to podocyte dysfunction [10,11,12]. Podocin, an integral membrane protein interacting with nephrin and cytoskeletal linkers, is critical for anchoring slit diaphragm complexes and has been studied in podocyte injury models and glomerular disease [13,14,15,16]. In non-myeloma glomerular diseases, detectable nephrinuria and podocinuria have been correlated with disease activity as well as chronic histological damage [17,18]. For example, urinary nephrin has been proposed as an early indicator of glomerular injury, sometimes preceding overt proteinuria [19]. A recent clinical study also measured urinary nephrin and podocalyxin in various glomerular diseases, finding correlations with disease severity, albeit with low sample size [17]. However, to date, there is very limited direct evidence whether urinary nephrin or podocin levels are associated with podocytopathy in the context of MM or monoclonal gammopathy.
Given the mechanistic plausibility and the unmet need for noninvasive glomerular biomarkers in paraprotein-related kidney disease, we here investigate urinary nephrin and podocin concentrations associated with albuminuria, proteinuria and the presence of biopsy-proven podocytopathy in patients with MM or monoclonal gammopathy of renal significance (MGRS). We test this hypothesis by comparing urinary podocin and nephrin levels in patients with and without histologically confirmed podocyte injury and exploring their relationships with proteinuria metrics such as albumin-to-creatinine ratios (uACR).
2. Materials and Methods
Patient Cohort
We retrospectively identified 75 patients with plasma cell dyscrasias, predominantly multiple myeloma and MGRS, and 11 healthy controls. Frozen urine samples were available from our biobank; for a subset of patients, samples were obtained on the day of diagnostic kidney biopsy. As this work represents a pilot study focusing on processes and methods rather than hypothesis testing or effect estimation, no detailed sample size calculation was planned. We included subjects of at least 18 years of age, who had provided informed consent for sample collection and subsequent storage in our biobank. Exclusion criteria were active participation in an interventional clinical trial within four weeks prior to sample collection. All subjects reported normal urine production and normal hydration levels at the time of sample collection.
Urine Samples
A total of 8 mL of morning urine was centrifuged at 3000 rpm for 10 min. The supernatant was immediately frozen at −80 °C. The urinary sediment was lysed in 1000 µL Trizol reagent.
RNA Isolation
The RNAzol lysate was mixed with 250 µL chloroform, briefly mixed by frequent inverting, and phase separation was performed by centrifugation at 12,000 g for 15 min. The aqueous phase was transferred to a separate tube and RNA was precipitated by adding 500 µL isopropanol followed by centrifugation at 12,000 g for 20 min. After a brief wash with 70% ethanol, the RNA pellet was air-dried and resuspended in RNase-free water. The RNA was either used directly for reverse transcription or frozen at −80 °C.
Reverse Transcription and Real-Time Quantitative PCR
For qPCR of podocin (Hs00387817_m1) and nephrin (Hs00190446_m1), a TaqMan assay from Applied Biosystems was used. As housekeeping control, a VIC-labeled GAPDH probe set (Applied Biosystems, Foster City, CA) was added to each reaction, with the water volume reduced accordingly. Gene expression levels were analyzed using the ΔΔCT method with normal kidney tissue as reference.
Podocin ELISA
A podocin-specific ELISA was obtained from Abcam (Human Podocin ELISA Kit, ab245708). Urine analysis for podocin concentration was performed according to the manufacturer’s instructions.
Statistical Analysis
Categorical data were reported as absolute numbers and relative frequencies, and continuous data as mean ± standard deviation or median and interquartile range, as appropriate. The main continuous predictors nephrin and podocin were modeled on their original scales.
Pearson correlations with Sidak-corrected p-values were used to assess relationships of the three predictors (nephrin mRNA, podocin mRNA, podocin ELISA) with urinary protein-to-creatinine (uPCR) and albumin-to-creatinine ratios (uACR). uPCR and uACR were log-transformed for normalization.
To test the null hypothesis of no difference between predictors in categorized outcome groups, we applied bootstrapped ANOVA or t-test, as appropriate. To quantify associations between predictors and continuous outcomes, nonparametric Epanechnikov regression with bootstrap confidence intervals was used, as assumptions for ordinary least squares regression were not met.
Receiver operating characteristic (ROC) analyses were performed to assess the diagnostic and discriminatory performance of the assessed podocyte markers in subjects affected with a form of plasma cell dyscrasia and albuminuria. Comparisons between AUCs of the different biomarkers were performed using paired DeLong test.
Data management and analysis were conducted using R version 4.5.1 (R foundation, Vienna, Austria) and Stata 17 (Stata Corp., College Station, TX). A two-sided p-value < 0.05 was generally considered statistically significant. Results are provided as mean ± standard deviation unless specified otherwise.
Ethics Approval
Approval was obtained from the local ethics committee of the Medical University of Vienna (approval number: 2435/2020)
3. Results
A summary of the patient cohort included in this study is presented in Table 1.
Higher levels of podocin as assessed by ELISA were significantly associated with lower amounts of urinary protein- and albumin excretion (uPCR: β= −0.158, 95%CI −0,311 to 0.059, p = 0.026; uACR: β = −0,265, 95%CI −0,487 to 0,094, p = 0.007). Both podocin-mRNA and nephrin-mRNA did not show significant association with uPCR or uACR (Table 2).
ROC analysis, performed to evaluate the diagnostic performance of the podocyte markers in patients with plasma cell dyscrasia and albuminuria, demonstrated limited diagnostic accuracy for podocin RNA (AUC 0.510, 95% CI 0.354–0.666), podocin ELISA (AUC 0.350, 95% CI 0.202–0.498), and nephrin mRNA (AUC 0.350, 95% CI 0.202–0.498). No significant difference in predictive performance was observed between models (p = 0.352) (Figure 1).
Importantly, both podocin and nephrin mRNA were significantly increased when urinary tract infection (UTI) was present, while no significant differences in protein levels were shown for podocin ELISA (p = 0.007, p = 0.080 and p = 0.293, respectively) (Table 3).
Protein levels of podocin and mRNA levels of both podocin and nephrin did not differ significantly between different forms of MGRS, MM or healthy controls (Table 4).
mRNA and protein levels did not differ significantly between other clinical conditions (Supplementary Table S1).
Regression analysis did not show significant association of the assessed parameters with histology confirmed podocytopathy, however, a trend towards significance was detected for podocin ELISA (β = 0.200, 95%CI 0.017 to 0.414, p = 0.097) (Table 5).
4. Discussion
In the present work we investigated whether urinary nephrin and podocin in terms of mRNA transcripts or protein are reflective of glomerular injury, as assessed by uACR levels and—where available—biopsy-proven podocytopathy in patients with MM or monoclonal gammopathy. Our results revealed a non-significant trend toward higher urinary podocin protein levels in subjects with histologic podocyte injury. Interestingly and counter-intuitively, we also found elevated podocin to be significantly associated with lower ACR.
Although the association did not reach statistical significance, likely due to lack of statistical power as a reflection of the highly experimental nature of our study, the direction of the effect is biologically credible as podocin release into urine might reflect podocyte stress, detachment, or slit diaphragm disruption prior to or concurrent with visible glomerular injury [20]. This is in line with previous reports, demonstrating podocyturia as an early marker of glomerular damage in various kidney diseases and is in agreement with previous findings by Jiminez et al. regarding the prognostic role of urinary podocin and nephrin in diabetic kidney disease [18]. Immunoglobulin- or light chain depositions along glomerular structures can trigger complement activation and may thus preferentially affect podocytes in certain instances [21,22,23,24]. The inverse correlation between urinary podocin and ACR is counterintuitive, since albuminuria is often taken as a proxy for glomerular barrier injury [25]. Possible explanations include a temporal mismatch in disease stage, whereby podocin shedding and podocyte fragment release may precede overt glomerular albumin leakage, as well as differences in biomarker kinetics, with podocin being released early in disease progression and subsequently declining in advanced stages [26]. Thus, urinary podocin may represent a different phase of podocyte injury than ACR. Additionally, we found significantly increased levels of urinary podocin and nephrin mRNA where UTI was present despite the absence of convincing evidence for ascending UTI or pyelonephritis. While it is possible that these markers of podocyte stress were elevated as a consequence of systemic inflammation in this context, to the best of our knowledge these findings are novel and warrant further investigation and external confirmation [27]. Importantly, these associations with current UTI, together with low sample size, may explain our expected findings of ROC analysis, where podocin protein levels and nephrin mRNA levels showed worse-than-random predictive performance for renal involvement.
Urinary nephrin did not show robust associations in our analysis. This may reflect differences in release kinetics as experimental models suggest that nephrin shedding earlier in slit diaphragm disruption, while podocin release requires more advanced or severe podocyte detachment [28]. In conditions outside myeloma, nephrinuria correlates with severity of glomerular disease and proteinuria. [17,19]
Strengths of our study include the pairing of urinary podocyte stress marker measurements with histologic confirmation of podocytopathy in a subset of subjects, which is rare in this disease domain. Limitations include modest sample size, heterogeneity of underlying renal manifestations of monoclonal gammopathy or myeloma, cross-sectional design and non-availability of nephrin protein levels. Additionally, we kidney biopsies were performed only in a subset of patients as they were not deemed indicated in the remaining individuals due to clinical lack of evidence of kidney disease.
While our results do not provide definitive answers regarding the clinical usefulness of these biomarkers, our experimental data may inform future trials evaluating the feasibility of podocyte stress markers as prognostic biomarkers in MM and MGRS.
In summary, our study provides preliminary experimental evidence that urinary podocin may trend higher in subjects with biopsy-proven podocytopathy in MM and MGRS and shows an unexpected inverse association with albuminuria, while nephrin mRNA failed to show a clear relationship in this dataset. These results support further exploration of urinary podocyte proteins as noninvasive biomarkers of glomerular injury in paraprotein-related kidney disease in larger collectives or as components of diagnostic biomarker panels. However, our findings warrant caution when assessing podocyte markers in the presence of UTI. Alternatively, nephrin and podocin should be investigated as markers of UTI in specific investigations [29]. Future research should evaluate nephrin and podocin in larger cohorts, integrate multiple biomarkers, and assess longitudinal dynamics.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: p-value table for between-group comparisons of levels of urinary podocyte biomarkers between sexes and/or conditions.
Author Contributions
Conceptualization, O.H., L.W. and W.W.; methodology, O.H. and W.W.; formal analysis, O.H. and L.W.; investigation, T.R., H.A. and L.W.; resources, T.R. and L.W.; data curation, L.W. and W.W.; writing—original draft preparation, O.H.; writing—review and editing, D.G. and T.R.; supervision, W.W.; funding acquisition, G.S. and W.W. All authors have read and agreed to the published version of the manuscript.”
Funding
Funding for this research was provided by the Medical Scientific Fund of the Mayor of the City of Vienna, grant number 22100.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Medical University of Vienna (approval number 2435/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Primary data is available upon reasonable request addressed to the corresponding author (oliver.helk@meduniwien.ac.at).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LC | Light Chain |
| uACR | Urinary Albumin-to-Creatinine Ratio |
| MM | Multiple Myeloma |
| MGUS | Monoclonal Gammopathy of Unknown Significance |
| MGRS | Monoclonal Gammopathy of Renal Significance |
References
- Leung, N.; Bridoux, F.; Hutchison, C.A.; Nasr, S.H.; Cockwell, P.; Fermand, J.-P.; Dispenzieri, A.; Song, K.W.; Kyle, R.A. Monoclonal gammopathy of renal significance: When MGUS is no longer undetermined or insignificant. Blood 2012, 120, 4292–4295. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Merlini, G.; Bridoux, F.; Leung, N.; Mikhael, J.; Harrison, S.J.; Kastritis, E.; Garderet, L.; Gozzetti, A.; van de Donk, N.; et al. Management of multiple myeloma-related renal impairment: Recommendations from the International Myeloma Working Group. Lancet Oncol. 2023, 24, e293–e311. [Google Scholar] [CrossRef] [PubMed]
- Leung, N.; Bridoux, F.; Batuman, V. The evaluation of monoclonal gammopathy of renal significance. Nat. Rev. Nephrol. 2019, 15, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Nasr, S.H.; Said, S.M. Renal Pathology Society/IKMG consensus on pathologic definitions and terminology of monoclonal gammopathy–associated kidney lesions. Kidney Int. 2025, 108, 184–193. [Google Scholar] [CrossRef]
- Finkel, K.W.; Cohen, E.P.; Shirali, A.; Abudayyeh, A. Paraprotein-Related Kidney Disease: Evaluation and Treatment of Myeloma Cast Nephropathy. Clin. J. Am. Soc. Nephrol. 2016, 11, 2273–2279. [Google Scholar] [CrossRef] [PubMed]
- Reiter, T.; Pajenda, S.; O’Connell, D.; Lynch, C.; Kapps, S.; Agis, H.; Schmidt, A.; Wagner, L.; Leung, N.; Winnicki, W. Renal Expression of Light Chain Binding Proteins. Front. Med. 2020, 7, 609582. [Google Scholar] [CrossRef]
- Jimenez, A.S.; et al. Urinary nephrin and podocin as biomarkers of podocyte injury in glomerular disease. Kidney Int. Rep. 2021, 6, 452–462. [Google Scholar] [CrossRef]
- Zeng, L.; Ng, J.K.-C.; Fung, W.W.-S.; Chan, G.C.-K.; Chow, K.-M.; Szeto, C.-C. Urinary podocyte stress marker as a prognostic indicator for diabetic kidney disease. BMC Nephrol. 2024, 25, 32. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, A.; Sato, Y.; Iwakiri, T.; Komatsu, H.; Kikuchi, M.; Kitamura, K.; Wiggins, R.C.; Fujimoto, S. Urine podocyte mRNAs mark disease activity in IgA nephropathy. Nephrol. Dial. Transplant. 2015, 30, 1140–1150. [Google Scholar] [CrossRef]
- Kandasamy, Y.; Smith, R.; Lumbers, E.R.; Rudd, D. Nephrin—A biomarker of early glomerular injury. Biomark. Res. 2014, 2, 21. [Google Scholar] [CrossRef]
- Ristola, M.; et al. Nephrinuria as an early marker of podocyte injury and disease activity. Nephrol. Dial. Transplant. 2020, 35, 2141–2149. [Google Scholar] [CrossRef]
- Trimarchi, H. Mechanisms of Podocyte Detachment, Podocyturia, and Risk of Progression of Glomerulopathies. Kidney Dis. 2020, 6, 324–329. [Google Scholar] [CrossRef]
- Nagata, M. Podocyte injury and its consequences. Kidney Int. 2016, 89, 1221–1230. [Google Scholar] [CrossRef]
- Tabatabaeifar, M.; Wlodkowski, T.; Simic, I.; Denc, H.; Mollet, G.; Weber, S.; Moyers, J.J.; Brühl, B.; Randles, M.J.; Lennon, R.; et al. An inducible mouse model of podocin-mutation-related nephrotic syndrome. PLoS ONE 2017, 12, e0186574. [Google Scholar] [CrossRef]
- Kestilä, M.; Lenkkeri, U.; Männikkö, M.; Lamerdin, J.; McCready, P.; Putaala, H.; Ruotsalainen, V.; Morita, T.; Nissinen, M.; Herva, R.; et al. Positionally cloned gene for a novel glomerular protein--nephrin--is mutated in congenital nephrotic syndrome. Mol. Cell 1998, 1, 575–582. [Google Scholar] [CrossRef]
- Garg, P. A Review of Podocyte Biology. Am. J. Nephrol. 2018, 47, 3–13. [Google Scholar] [CrossRef]
- Giannou, P.; Gakiopoulou, H.; Stambolliu, E.; Petras, D.; Chalkia, A.; Kapota, A.; Palamaris, K.; Hadziyannis, E.; Thomas, K.; Alexakou, Z.; et al. Urine Nephrin and Podocalyxin Reflecting Podocyte Damage and Severity of Kidney Disease in Various Glomerular Diseases—A Cross-Sectional Study. J. Clin. Med. 2024, 13, 3432. [Google Scholar] [CrossRef]
- Jimenez, A.S.; et al. Urinary podocin mRNA and protein as prognostic biomarkers of renal injury. Am. J. Physiol. Renal Physiol. 2021, 320, F876–F885. [Google Scholar] [CrossRef]
- Mesfine, B.B.; Vojisavljevic, D.; Kapoor, R.; Watson, D.; Kandasamy, Y.; Rudd, D. Urinary nephrin-a potential marker of early glomerular injury: A systematic review and meta-analysis. J. Nephrol. 2024, 37, 39–51. [Google Scholar] [CrossRef]
- Schwarz, K.; Simons, M.; Reiser, J.; Saleem, M.A.; Faul, C.; Kriz, W.; Shaw, A.S.; Holzman, L.B.; Mundel, P. Podocin, a raft-associated component of the glomerular slit diaphragm, interacts with CD2AP and nephrin. J. Clin. Investig. 2001, 108, 1621–1629. [Google Scholar] [CrossRef]
- Cassano Cassano, R.; Bonadio, A.G.; Del Giudice, M.L.; Giannese, D.; Galimberti, S.; Buda, G. Light chain deposition disease: Pathogenesis, clinical characteristics and treatment strategies. Ann. Hematol. 2025, 104, 2083–2093. [Google Scholar] [CrossRef]
- Yu, X.-J.; Zhou, X.-J.; Wang, S.-X.; Zhou, F.-D.; Zhao, M.-H. Monoclonal light chain crystalline podocytopathy and tubulopathy associated with monoclonal gammopathy of renal significance: A case report and literature review. BMC Nephrol. 2018, 19, 322. [Google Scholar] [CrossRef]
- Khalighi, M.A.; Revelo, M.P.; Abraham, J.D.; Shihab, F.; Ahmed, F. Light Chain Podocytopathy Mimicking Recurrent Focal Segmental Glomerulosclerosis. Am. J. Transplant. 2017, 17, 824–829. [Google Scholar] [CrossRef]
- Sethi, S.; Rajkumar, S.V. Monoclonal gammopathy-associated proliferative glomerulonephritis. Mayo Clin. Proc. 2013, 88, 1284–1293. [Google Scholar] [CrossRef]
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, S117–S314. [CrossRef]
- Lioudaki, E.; Stylianou, K.G.; Petrakis, I.; Kokologiannakis, G.; Passam, A.; Mikhailidis, D.P.; Daphnis, E.K.; Ganotakis, E.S. Increased Urinary Excretion of Podocyte Markers in Normoalbuminuric Patients with Diabetes. Nephron 2015, 131, 34–42. [Google Scholar] [CrossRef]
- Ilatovskaya, D.V.; Behr, A.; Staruschenko, A.; Hall, G.; Palygin, O. Mechanistic Insights Into Redox Damage of the Podocyte in Hypertension. Hypertension 2025, 82, 14–25. [Google Scholar] [CrossRef]
- Nakatsue, T.; Koike, H.; Han, G.D.; Suzuki, K.; Miyauchi, N.; Yuan, H.; Salant, D.J.; Gejyo, F.; Shimizu, F.; Kawachi, H. Nephrin and podocin dissociate at the onset of proteinuria in experimental membranous nephropathy. Kidney Int. 2005, 67, 2239–2253. [Google Scholar] [CrossRef]
- Sun, J.; Cheng, K.; Xie, Y. Urinary Tract Infections Detection with Molecular Biomarkers. Biomolecules 2024, 14, 1540. [Google Scholar] [CrossRef]
Figure 1.
Diagnostic performance of urinary podocyte biomarkers for predicting kidney involvement in Multiple Myeloma.
Figure 1.
Diagnostic performance of urinary podocyte biomarkers for predicting kidney involvement in Multiple Myeloma.
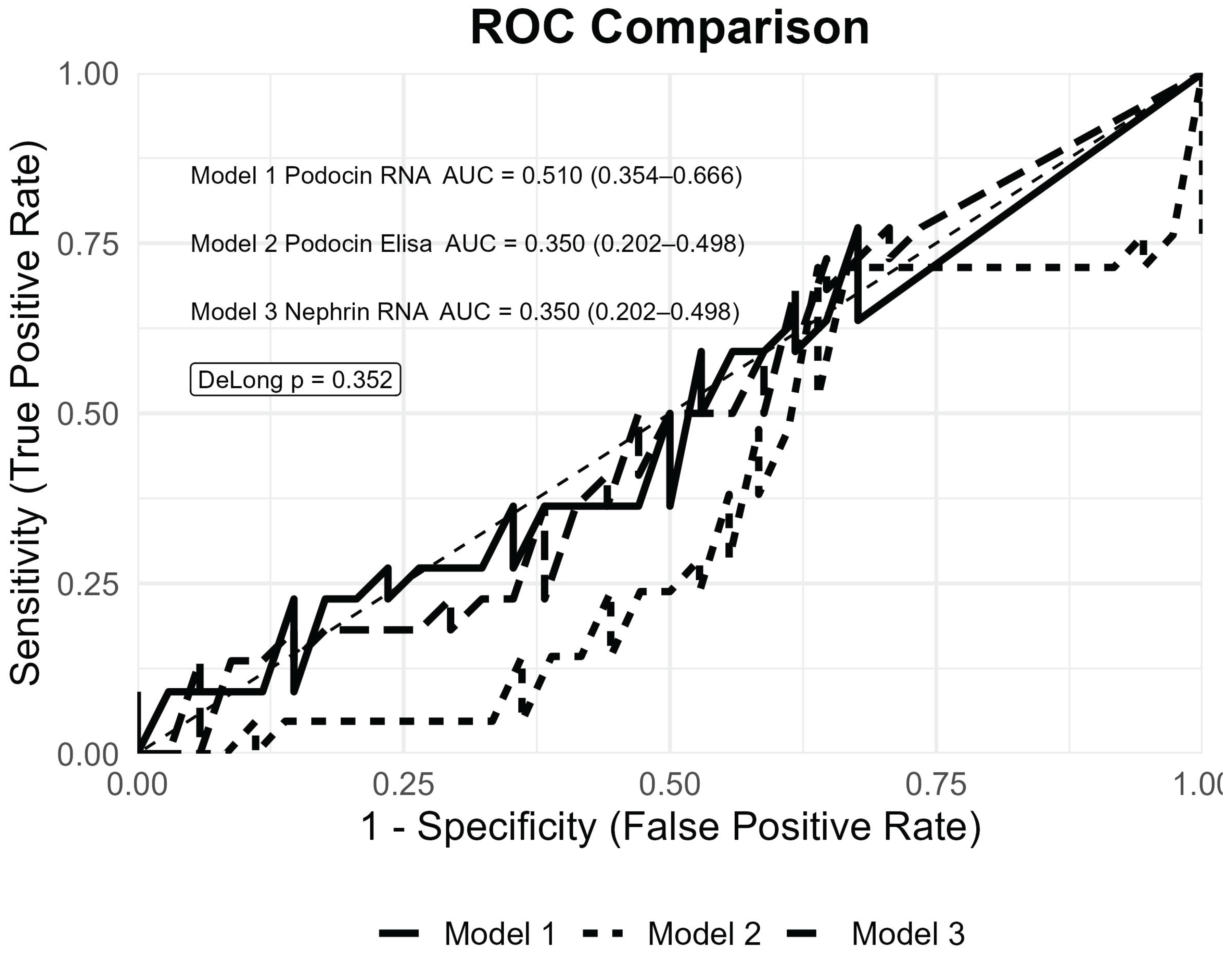

Table 1.
Baseline characteristics of the study cohort.
| Characteristics | Total Cohort (n = 86) |
|---|---|
|
Age (years) sex—n (%) - male |
67,2 ± 12,0 49 (57%) |
| - female | 37 (43%) |
| BMI | 26,4 ± 4,9 |
|
Hematological condition—n (%) - MM - MGRS - LC Amyloidosis - MGUS - healthy controls |
56 (65,1%) 3 (3,5%) 8 (9,3%) 8 (9,3%) 11 (12,8%) |
|
Laboratory parameters: - uPCR (mg/g) - uACR (mg/g) - eGFR (mL/min/1.73m2) - Serum total protein (g/L) - Serum Albumin (g/L) - HbA1c (%) - Presence of microhematuria (%) |
1016,5 ± 2551,3 570,5 ± 2180,3 63,6 ± 31,3 65,4 ± 8,8 40,2 ± 5,8 5,5 ± 0,5 15 (17,9%) |
|
Comorbidities—n (%) - arterial hypertension - type II diabetes mellitus - coronary heart disease - heart disease - glomerulonephritis - kidney transplantation Histomorphology—n (%) - number of biopsies subjects - evidence of podocytopathia in >20 of glomeruli |
38 (44,1%) 10 (11,8%) 9 (10,6%) 3 (3,5%) 3 (3,5%) 6 (7,0%) 23 (26,4%) 11 (47,8%) |
Table 2.
Association between urinary podocyte biomarkers with urinary protein-creatinine-ratio and urinary albumin-creatinine-ratio.
Table 2.
Association between urinary podocyte biomarkers with urinary protein-creatinine-ratio and urinary albumin-creatinine-ratio.
| Variable | β (95% CI) Podocin-ELISA | p | β (95% CI) Podocin-mRNA |
p | β (95% CI) Nephrin-mRNA |
p |
|---|---|---|---|---|---|---|
| uPCR (mg/g) | −0,158 (−0,311; 0.059) | 0,026 | 0,043 (−0,175; 0,103) | 0,591 | −0,045 (−0,233; 0,120) | 0,643 |
| uACR (mg/g) | −0,265 (−0,487; 0,094) | 0,007 | 0,021 (−0,354; 0,125) | 0,942 | −0,026 (−0,398; 0,266) | 0,878 |
Table 3.
Impact of concurrent urinary tract infection (UTI) on urinary podocyte biomarker controls.
| UTI Excluded | UTI Present | p-Value | |
|---|---|---|---|
| n | 65 | 19 | |
| Marker | |||
| Podocin ELISA | 8,85 ± 2,33 | 9,00 ± 4,38 | 0,293 |
| Podocin mRNA | 6,56 ± 4,72 | 9,83 ± 4,51 | 0,007 |
| Nephrin mRNA | 7,05 ± 4,30 | 9,82 ± 3,13 | 0,080 |
Table 4.
Comparison of urinary podocyte biomarkers across the spectrum of plasma cell dyscrasias and association between urinary podocyte biomarkers and biopsy-proven podocytopathy.
Table 4.
Comparison of urinary podocyte biomarkers across the spectrum of plasma cell dyscrasias and association between urinary podocyte biomarkers and biopsy-proven podocytopathy.
| MM | MGRS | LC Amyloidosis | MGUS | Control | p-Value | |
|---|---|---|---|---|---|---|
| n | 56 | 3 | 8 | 8 | 11 | |
| Marker | ||||||
| Podocin ELISA [pg/mL] | 9,22 ± 2,62 | 8,27± 1,54 | 6,36 ± 4,53 | 9,82 ± 1,63 | 3,92 ± 3,92 | 0,183 |
| Podocin mRNA * | 7,27 ± 4,72 | 10,38 ± 1,81 | 8,67 ± 4,76 | 4,13 ± 5,19 | 7,67 ± 4,63 | 0,203 |
| Nephrin mRNA * | 6,90 ± 4,63 | 10,70 ± 0,65 | 9,91 ± 1,89 | 6,78 ± 4,53 | 9,32 ± 1,54 | 0,141 |
Table 5.
Association between urinary podocyte biomarkers and biopsy-proven podocytopathy.
| Variable | β (95% CI) Podocin-ELISA | p-Value | β (95% CI) Podocin-mRNA |
p-value | β (95% CI) Nephrin-mRNA |
p-Value |
|---|---|---|---|---|---|---|
| Podocytopathia | 0,200 (0,017 to 0,414) | 0,097 | −0,106 (−0,396 to 0,097) | 0,433 | −0.334 (−1.164 to 0.430) | 0,458 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



