Submitted:
23 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
Toxoplasmosis is a cosmopolitan zoonosis that particularly threatens pregnant women and immunocompromised individuals. Among people living with HIV, Toxoplasma gondii may invade the central nervous system, producing neuropathological effects associated with mental and psychiatric disorders. We assessed the seroprevalence of anti–T. gondii IgG in HIV-infected and HIV-uninfected residents of Iquitos, Peru, and evaluated an in-house ELISA based on total lysed antigen (TLA) against a commercial kit. In this observational cross-sectional study, 151 participants were enrolled: 92 HIV-positive and 59 HIV-negative. Overall IgG seroprevalence was 88.08% (133/151), reaching 91.30% (84/92) in the HIV-positive group and 83.05% (49/59) in the HIV-negative group. Seroprevalence was highest among adults aged 36–60 years (89.33%; 67/75) and among males (89.77%; 79/88) versus females (85.71%; 54/63). Mean optical density values were greater in HIV-positive participants (1.37±0.393; 95% CI 1.28–1.45) than in HIV-negative participants (0.565±0.200; 95% CI 0.510–0.620), and were higher in men overall (1.18±0.502; 95% CI 1.07–1.30). These findings indicate very high exposure to T. gondii in Iquitos, with higher IgG prevalence and antibody levels in HIV-positive individuals. The marked OD difference suggests stronger IgG responses among HIV-positive participants, highlighting potential risk for toxoplasmic encephalitis. Serological screening and preventive counseling may be warranted in high-burden Amazonian communities.
Keywords:
Toxoplasma gondii
; seroprevalence
; HIV
1. Introduction
Toxoplasmosis is a cosmopolitan zoonosis that affects most warm-blooded animals, including humans. It comprises an acute phase and a chronic phase. People acquire the infection by consuming raw or undercooked meat, water, vegetables, or fruits contaminated with oocysts, through accidental inoculation, transfusion/transplantation, or congenitally [1,2]. The etiological agent is Toxoplasma gondii (T. gondii), an intracellular protozoan that has two adaptable stages in humans for its survival and propagation. Tachyzoites are the rapidly multiplying form that disseminates, and bradyzoites are the form that encysts in human tissues [2,3].
Toxoplasmosis is an infection that almost always goes unnoticed in immunocompetent people, but it poses a risk to pregnant women and immunocompromised individuals due to the risk of primary infection or reactivation [4]. In individuals infected with the Human Immunodeficiency Virus (HIV), tachyzoites can spread through the bloodstream to various organs, such as the brain, eyes, and muscles, causing fatal complications [5,6].
The most common and most severe manifestation of the disease is toxoplasmic encephalitis, and latent toxoplasmosis is also responsible for neuropathological effects that cause mental and psychiatric disorders due to the active proliferation of the parasite within the brain, such as anxiety, schizophrenia spectrum disorders, depression, and suicidal behavior [7]. In patients with HIV, the risk of toxoplasmosis reactivation depends on access to antiretroviral therapy and the patient's immune status. Reactivation can occur when the CD4 count is generally less than 200 cells/mm³ and it occurs in up to 30% of patients, causing serious complications [7,8].
Approximately 30% of the world’s population is infected with T. gondii [9]. In South America, the seroprevalence of toxoplasmosis can range from 7% to 38% [9,10]. These variations can mainly be explained by geographic region, dietary habits, sanitation, and host susceptibility [4]. Surveillance for toxoplasmosis is limited in Peru. The latest national report, from 2022, shows a seroprevalence of 45.2% (498/1101) [11]. However, it is not possible to identify or differentiate the percentage of at-risk populations, such as people with HIV.
In the last 3 years (2023 – 2025), studies have focused on the Peruvian Amazon as the main hotspot for cases with high seroprevalence, especially in people with HIV, and have reported a seroprevalence between 71% and 97% [12,13,14]. The elevated seroprevalence values reflect the importance of conducting surveillance in at-risk populations, especially in the Peruvian Amazon. In this regard, the main objective of this study was to determine the seroprevalence of IgG against T. gondii in an HIV-positive group and an HIV-negative group in the city of Iquitos, Peru.
2. Materials and Methods
2.1. Ethical Statment
This study was approved by the Ethics Committee of the Peruvian University Cayetano Heredia, registered with code numbers 62495 and 201148. Samples were collected only after obtaining informed consent from the participants or a health care proxy.
2.2. Study Design and study sites
An observational, cross-sectional study was conducted to detect IgG antibodies against T. gondii in sera from HIV-infected and non-infected individuals using an in-house ELISA test with total lysate antigen (TLA) from the T. gondii RH strain. Participants were recruited in Iquitos, the capital of the Loreto department in the Peruvian Amazon, located in the northeast of Peru. Geographically, it is a riverine plain with a tropical and humid climate, experiencing constant rainfall throughout the year and temperatures ranging from 21 °C to 33 °C [15].
2.3. Participants recruitment and collection of information
We enrolled hospitalized individuals from the general population in Iquitos. HIV
positive individuals were enrolled in Hospital Regional de Loreto, as part of an ongoing study of people with HIV and possible neurological infections. HIV negative participants were recruited as part of a study on tick-borne disease in households with dogs. Briefly, 286 houses in Iquitos were randomly selected and visited. Only patients who were older than 18 years old and signed the informed consent, or had it signed by a representative, were included in the study.
We collected a total of 151 serum samples. Of these, 92 were from HIV-positive individuals and 59 from HIV-negative individuals. Samples were categorized by sex and into three age groups: young adults (18 - 35 years), adults (36 - 60 years), and older adults (61 - 78 years).
2.4. Laboratory tests for HIV
Hospitalized patients were tested for HIV by the "Programa de Control de Enfermedades de Transmisión Sexual y SIDA (PROCETSS)". According to this program, a commercially available ELISA (AccuBioTech, Beijing, China) was used as a screening test, and Western Blot was employed as a confirmatory test. Non-hospitalized individuals were tested for HIV using the INSTI HIV Self-Test (bioLytical Laboratories Inc, BC, Canada), which has a sensitivity of 100% and a specificity of 99.5%.
2.5. In-house ELISA TLA Test
Seroprevalence was determined using an in-house ELISA. Total lysate antigens (TLA) of T. gondii were obtained via cell culture following the protocols of Flores et al., 2025. Tachyzoites of the RH strain of T. gondii were cultured in LLC-MK2 cell lines. The ELISA using TLA (ELISA-TLA) for IgG detection against T. gondii was validated against a commercial ELISA (Vircell Microbiologist, code G1027), which uses native antigens from the RH strain of T. gondii. Positive and negative concordance rates were 98.3% and 100%, respectively [12].
Polystyrene plates were sensitized with TLA at a concentration of 1 µg/mL in 0.05 M bicarbonate-carbonate buffer. Free binding sites were blocked with skim milk in Phosphate Buffer Saline (PBS) 1X + 0.05% Tween 20. The primary antibody was used at 1:500 dilution and the secondary antibody at 1:10,000. Readings were taken at 450 nm using an ELISA reader. Each sample was run in duplicate, and each plate included a pool of four negative controls, three positive controls, and a blank. The cut-off value was calculated as the mean of the negative controls plus three standard deviations.
2.6. Data analysis
The study population (n = 151) was described by summarizing categorical variables (HIV infection status, sex, and age groups) as absolute frequencies and percentages. Optical density (OD450) values were summarized as means, standard deviations, and 95% confidence intervals. To compare mean OD450 values between HIV-infected and non-infected groups (92 and 59 sera, respectively), as well as across different age groups and between sexes, an independent samples two-tailed Student’s t-test was used, with a significance level of p < 0.05. The comparison between age groups was performed non-parametrically using the Kruskal-Wallis test.
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
Of the 151 serum samples collected, 60.93% (92/151) were from individuals infected with HIV, while 39.07% (59/151) were from HIV-negative individuals. 58.28% (88/151) of participants were male and 41.72% (63/151) were female, 49.67% (75/151) of participants were between 36 and 60 years of age, 46.36% (70/151) were in the 18-35 years group, and only 3.97% (6/151) of participants were aged 61-78 years (Table 1).
3.2. Seroprevalence of Toxoplasmosis in the Study Population
Using the ELISA-TLA assay, the overall seroprevalence of anti-T. gondii IgG in the study population was 88.08% (133/151). Overall, 60.93% (92/151) of participants were HIV-positive, and IgG seroprevalence was significative higher (p<0.0001) in the HIV-positive group (91.30% [84/92]) than in the HIV-negative group (83.05% [49/59]). In HIV-positive participants, mean OD450 values were 1.37 ± 0.393 (95% CI: 1.28–1.45) among seropositive individuals and 0.169 ± 0.0668 (95% CI: 0.113–0.224) among seronegative individuals, whereas in HIV-negative participants the corresponding mean OD450 values were 0.565 ± 0.200 (95% CI: 0.510–0.620) and 0.0734 ± 0.0232 (95% CI: 0.167–0.272), respectively (Figure 1). HIV infection was present in 63.16% (84/133) of IgG-Anti-T. gondii seropositive participants and in 44.44% (8/18) of IgG- Anti-T. gondii seronegative participants.
Analysis of T. gondii IgG seroprevalence by age showed that adults aged 36 - 60 years had the highest proportion of positive results, with 89.33% (67/75) and a mean OD450 of 0.979 ± 0.521 (95% CI: 0.859 - 1.10), followed by young adults aged 18 - 35 years, with 87.14% (61/70) and a mean OD450 of 0.976 ± 0.610 (95% CI: 0.831 - 1.12). Older adults aged 61 - 78 years had with a seroprevalence of 83.33 % (5/6) and a mean OD450 of 0.747 ± 0.430 (95% CI: 0.296 -1.20) (Figure 2A). Regarding sex distribution, 89.77% (79/88) of men in the general population were seropositive, with a mean OD450 of 1.18 ± 0.502 (95% CI: 1.07 - 1.3), while 85.74% (54/63) of women were seropositive, with a mean OD450 of 0.909 ± 0.489 (95% CI: 0.776 - 1.04). Anti-T. gondii IgG seronegativity was observed in 10.23% (9/88) of men and 14.29% (9/63) of women. According to our cut-off value (OD450: 0.360), the mean optical density was 0.209 ± 0.081 (95% CI: 0.147–0.271) and 0.185 ± 0.067 (95% CI: 0.133–0.237), respectively (Figure 2B).
4. Discussion
The seroprevalence of IgG antibodies against T. gondii in the present study was 88.08% (133/151), which is higher than the global average reported in the meta-analysis by Molan et al. (2019), which found a seroprevalence of 25.7% across various populations, including children, adults, and pregnant women [9]. Similarly, the study by Sengupta and cols., covering data from 1959 to 2020, reported a global seroprevalence of 36% [16]. Both studies indicate higher prevalence rates in Africa and South America. The high seroprevalence in some regions of South America is associated with living in rural, tropical or subtropical areas, poor sanitary conditions or a deficient immune system [17,18,10].
Iquitos has a tropical climate and is characterized by a lower-middle socioeconomic level, with 8.63% of the population living in poverty [19]. Its geographical isolation from Lima, the capital, exacerbates challenges related to governance, economic development, and access to healthcare [19]. Furthermore, environmental changes due to global warming have affected parasite ecology, with T. gondii demonstrating increased oocyst sporulation under environmental stressors [20]. Seasonal rainfall and increased river flow have been shown to facilitate the release of oocysts from soil into water, further exacerbating the spread of the parasite [21].
A higher seroprevalence of T. gondii was observed in HIV-infected individuals, at 91.30% (84/92), compared with 83.05% (49/59) among HIV-negative individuals. These findings align with global studies indicating a higher prevalence of latent toxoplasmosis among people with HIV [22,23,24].
The higher optical density values observed in HIV-positive individuals reflect a greater concentration of anti-T gondii IgG antibodies compared with HIV-negative individuals. This finding supports previous reports indicating a high burden of latent toxoplasmosis in people living with HIV, particularly in settings with limited access to early diagnosis and treatment. In immunocompromised hosts, the reduced capacity to control parasite replication facilitates persistence and reactivation of T. gondii, which exhibits a marked neurotropism and can cause severe organ damage, especially in the central nervous system [4,7,8].
This issue is particularly relevant for individuals with CD4⁺ T-cell counts < 200 cells/mm³. In Latin America, although HIV-related mortality has declined in recent years, the incidence of new infections has increased by approximately 13%. Moreover, an estimated 14% of people living with HIV remain unaware of their infection, and nearly one-third are diagnosed at advanced stages [25]. In regions such as Loreto, one of the Peruvian departments with the highest burden of HIV infection in recent years and a high prevalence of toxoplasmosis, these conditions further increase the risk of opportunistic infections. Epidemiological monitoring of this population using serological screening methods, such as ELISA, is therefore essential, as parasite reactivation in susceptible individuals can lead to severe organ involvement, particularly affecting the central nervous system, with potentially irreversible consequences [6,8].
Although no statistically significant differences were observed across age groups, higher seroprevalence among adults is consistent with previous studies showing an age-related increase in T. gondii IgG positivity, which is generally interpreted as a marker of cumulative exposure rather than age-specific susceptibility [16,26]. Sex-related differences in T. gondii seroprevalence remain inconsistent across studies, with some reports indicating higher prevalence in men, while others describe higher rates in women, particularly in the context of pregnancy due to increased screening and heightened clinical awareness [27,28]. In the present study, seroprevalence was higher among male participants compared with females. Higher optical density values observed in males may reflect differences in exposure intensity or cumulative risk rather than sex-specific susceptibility, potentially influenced by behavioral or occupational factors. Overall, sex alone is unlikely to represent an independent risk factor for T. gondii infection and should be interpreted within the context of environmental exposure and host-related factors.
This study has certain limitations that should be acknowledged. IgG antibodies against T. gondii were detected using an in-house indirect ELISA based on TLA, which, although previously validated, may present cross-reactivity with other apicomplexan parasites circulating in endemic regions such as the Peruvian Amazon [29]. In addition, the use of TLA does not allow for discrimination between different stages of infection. Future studies incorporating more specific antigens, such as recombinant or stage-specific proteins, may improve diagnostic specificity and enable a more refined assessment of infection dynamics [30,31]. Despite these limitations, the high seroprevalence observed highlights the substantial burden of T. gondii infection in this setting and supports the relevance of the findings.
5. Conclusions
This study demonstrates a high seroprevalence of IgG antibodies against Toxoplasma gondii in both HIV-infected and HIV-uninfected individuals in Iquitos, Peru, with a greater burden observed among people living with HIV. These findings highlight the endemic nature of toxoplasmosis in the Peruvian Amazon and underscore the vulnerability of immunocompromised populations in this setting.
Author Contributions
Margot Faustino: Conceptualization, Investigation, Methodology, Writing-original draft and Writing-review & editing. Carlos A. Flores: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing-original draft and Writing-review & editing. Edith S. Málaga-Machaca: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing-original draft and Writing-review & editing. Juan Jiménez-Chunga: Conceptualization, Investigation, Supervision, Validation, Writing-review & editing. Maritza Calderon: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing-review & editing.
Funding
This research was funded by the Consejo Nacional de Ciencia, Tecnología e Innovación Tecnológica (CONCYTEC) within the framework of the competition “E041-2023-02 Proyectos de Investigación Aplicada”, grant number PE501083007-2023-02.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia (UPCH) (protocol codes 62495 and 201148, dates of approval: April 25, 2023 and March 13, 2020, respectively.).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Samples were only collected if the participant, or a health care proxy, signed the informed consent.
Data Availability Statement
Data will be made available on request.
Acknowledgments
We thank Dr. Robert H. Gilman, Dr. Natalie Bowman, Dr. Cusi Ferradas, M.Sc. Andrea Diestra, Dr. Michael Sciaudone, Dra. Viviana Pinedo and Lic. Lilia Cabrera for their technical assistance and for providing laboratory facilities during the development of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HIV | Human Immunodeficiency Virus |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| IgG | Immunoglobulin G |
| TLA | Total Lysate Antigen |
| CI | Confidence Interval |
| OD450 | Optical Density at 450 nm |
| CD4 | Cluster of Differentiation 4 |
References
- Tenter, AM; Heckeroth, AR; Weiss, LM. Toxoplasma gondii: from animals to humans. Int J Parasitol. 2000, 30(12-13), 1217–58. [Google Scholar] [CrossRef] [PubMed]
- Hill, DE; Chirukandoth, S; Dubey, JP. Biology and epidemiology of Toxoplasma gondii in man and animals. Anim Health Res Rev. 2005, 6(1), 41–61. [Google Scholar] [CrossRef] [PubMed]
- Robert-Gangneux, F; Dardé, ML. Epidemiology of and diagnostic strategies for toxoplasmosis. Clin Microbiol Rev. 2012, 25(2), 264–96. [Google Scholar] [CrossRef] [PubMed]
- Dubey, JP. History of the discovery of the life cycle of Toxoplasma gondii. Int J Parasitol. 2009, 39(8), 877–82. [Google Scholar] [CrossRef]
- Dardé, ML; Peyron, F. Toxoplasma y toxoplasmosis. EMC - Pediatría 2013, 48(1), 1–12. [Google Scholar] [CrossRef]
- Basavaraju, A. Toxoplasmosis in HIV infection: an overview. Trop Parasitol 2016, 6(2), 129–35. [Google Scholar] [CrossRef]
- Botero-Rodríguez, F; Zárate-Velasco, AM; Cote Martínez, D; Gómez-Restrepo, C; Duarte Osorio, A. Infección por Toxoplasma gondii como factor de riesgo para desarrollar esquizofrenia: revisión de la literatura. Univ Med. 2023, 64(2). [Google Scholar] [CrossRef]
- Dian, S; Ganiem, AR; Ekawardhani, S. Cerebral toxoplasmosis in HIV-infected patients: a review. Pathog Glob Health 2023, 117(1), 14–23. [Google Scholar] [CrossRef]
- Molan, A; Nosaka, K; Hunter, M; Wang, W. Global status of Toxoplasma gondii infection: systematic review and prevalence snapshots. Trop Biomed. 2019, 36(4), 898–925. [Google Scholar]
- Zavala-Hoppe, A; Piguave-Cacao, R; Ponce-Macias, N. Epidemiología y factores de riesgo de la toxoplasmosis en los países de Latinoamérica. MQRInvestigar 2025, 9(1), e234. [Google Scholar] [CrossRef]
- Instituto Nacional de Salud (INS). Anuario estadístico 2023 [Internet]. INS: Lima, 2023; Available online: https://www.gob.pe/institucion/ins/informes-publicaciones/3833116-anuario-estadistico.
- Flores, BCA; Ferradas, C; Málaga-Machaca, ES; Diestra, A; Steinberg, HE; Calla, J; et al. Seroprevalence and factors associated with infection with Toxoplasma gondii in Iquitos and Lima, Peru. Am J Trop Med Hyg. 2025, 113(3), 600–6. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, HE; Bowman, NM; Diestra, A; Ferradas, C; Russo, P; Clark, DE; et al. Detection of toxoplasmic encephalitis in HIV positive patients in urine with hydrogel nanoparticles. PLoS Negl Trop Dis. 2021, 15(3), e0009199. [Google Scholar] [CrossRef]
- Steinberg, HE; Ramachandran, PS; Diestra, A; Pinchi, L; Ferradas, C; Kirwan, DE; et al. Clinical and metagenomic characterization of neurological infections of people with human immunodeficiency virus in the Peruvian Amazon. Open Forum Infect Dis. 2023, 10(11), ofad515. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Prieto, AJY; Quispe Roldan, JF; Sanchez Rosales, KIB; Casasola Lescano, X; Sanjinez Viera, YM; Giraldo Malca, UF. Climate variation in the Amazonian peneplain due to deforestation and urban expansion in Iquitos - Peru, between 1984 and 2023. In Proceedings of the 22nd LACCEI International Multi-Conference for Engineering, Education, and Technology: Sustainable Engineering for a Diverse, Equitable, and Inclusive Future at the Service of Education, Research, and Industry for a Society 5.0, San Jose, Costa Rica, 2024 Jul 17-19; LACCEI. [Google Scholar] [CrossRef]
- Sengupta, PP; Jacob, SS; Suresh, KP; Rajamani, S; Maharana, SM. Exploring global trends in human toxoplasmosis seroprevalence by meta-analysis. Exp Parasitol. 2025, 275, 108971. [Google Scholar] [CrossRef] [PubMed]
- Pari, J; Yauyo, R; Aquino, A; Adauto, M; Ochoa, S; Rojas, A; et al. Toxoplasma gondii infection in risk population groups from Andes Peruvian. Open J Med Microbiol. 2020, 10, 26–32. [Google Scholar] [CrossRef]
- Gontijo da Silva, M; Clare Vinaud, M; de Castro, AM. Prevalence of toxoplasmosis in pregnant women and vertical transmission of Toxoplasma gondii in patients from basic units of health from Gurupi, Tocantins, Brazil, from 2012 to 2014. PLoS One 2015, 10(11), e0141700. [Google Scholar] [CrossRef]
- Ministerio de Desarrollo e Inclusión Social (MIDIS). REDinforma report [Internet]. 8 Jan 2026. Available online: https://app.midis.gob.pe/RedInforma/Reporte/ReportePDF?vCodTema=1.
- Patz, JA; Graczyk, TK; Geller, N; Vittor, AY. Effects of environmental change on emerging parasitic diseases. Int J Parasitol. 2000, 30(12-13), 1395–405. [Google Scholar] [CrossRef]
- Yan, C; Liang, LJ; Zheng, KY; Zhu, XQ. Impact of environmental factors on the emergence, transmission and distribution of Toxoplasma gondii. Parasit Vectors 2016, 9, 137. [Google Scholar] [CrossRef]
- Liu, L; Liu, LN; Wang, P; Lv, TT; Fan, YG; Pan, HF. Elevated seroprevalence of Toxoplasma gondii in AIDS/HIV patients: a meta-analysis. Acta Trop. 2017, 176, 162–7. [Google Scholar] [CrossRef]
- Voyiatzaki, C; Zare Chormizi, AD; Tsoumani, ME; Efstathiou, A; Konstantinidis, K; Chaniotis, D; et al. Seroprevalence of Toxoplasma gondii among HIV positive patients under surveillance in Greek infectious disease units: a screening study with comparative evaluation of serological methods. Pathogens 2024, 13(5), 375. [Google Scholar] [CrossRef]
- Safarpour, H; Cevik, M; Zarean, M; Barac, A; Hatam-Nahavandi, K; Rahimi, MT; et al. Global status of Toxoplasma gondii infection and associated risk factors in people living with HIV. AIDS 2020, 34(3), 469–74. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization. HIV/AIDS in the Americas: regional epidemiological update 2025 [Internet]. 2025. Available online: https://www.paho.org/en/topics/hivaids.
- Jimenez-Chunga, J; Gomez-Puerta, LA; Vargas-Calla, A; Castro-Hidalgo, J; Sánchez-Chicana, C; Calderón-Sánchez, M. Seroprevalence of Toxoplasma gondii, risk factors and knowledge about toxoplasmosis in undergraduate students from Lima, Peru. Acta Trop. 2024, 255, 107233. [Google Scholar] [CrossRef] [PubMed]
- Yu, CP; Chen, BC; Chou, YC; Hsieh, CJ; Lin, FH. The epidemiology of patients with toxoplasmosis and its associated risk factors in Taiwan during the 2007-2020 period. PLoS One 2023, 18(8), e0290769. [Google Scholar] [CrossRef] [PubMed]
- Shoukat, T; Awan, UA; Mahmood, T; Afzal, MS; Wasif, S; Ahmed, H; et al. Epidemiology of toxoplasmosis among the Pakistani population: a systematic review and meta-analysis. Pathogens 2022, 11(6), 675. [Google Scholar] [CrossRef]
- Gondim, LFP; Mineo, JR; Schares, G. Importance of serological cross-reactivity among Toxoplasma gondii, Hammondia spp., Neospora spp., Sarcocystis spp. and Besnoitia besnoiti. Parasitology 2017, 144(7), 851–68. [Google Scholar] [CrossRef]
- Ferra, BT; Chyb, M; Sołowińska, K; Holec-Gąsior, L; Skwarecka, M; Baranowicz, K; et al. The development of Toxoplasma gondii recombinant trivalent chimeric proteins as an alternative to Toxoplasma lysate antigen (TLA) in enzyme-linked immunosorbent assay (ELISA) for the detection of immunoglobulin G (IgG) in small ruminants. Int J Mol Sci. 2024, 25(8), 4384. [Google Scholar] [CrossRef]
- Dong, H; Zhang, J; Wang, Q; Shen, Y; Zhou, B; et al. Development of an indirect ELISA for detecting Toxoplasma gondii IgG antibodies based on a recombinant TgIMP1 protein. PLoS Negl Trop Dis. 2024, 18(8), e0012421. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Seroprevalence of IgG antibodies against T. gondii according to HIV infection status. Each circle represents the OD450 result obtained using the in-house ELISA-TLA test. The cut-off indicated by dashed lines, established at 0.360 ± 0.068. Among IgG-positive results, a significant difference was observed between HIV-infected and non-infected groups (p<0.0001).
Figure 2.
Distribution of IgG antibodies against T. gondii according to age and sex in the general population. The cut-off was set at 0.360 ± 0.068. (a). Comparison of OD450 values among age groups (18 - 35, 36-60, and 61 - 78 years); no significant differences were observed. (b). Comparison of OD450 values by sex; among positive results, a significant difference was observed between men and women (p value = 0.0469).
Figure 2.
Distribution of IgG antibodies against T. gondii according to age and sex in the general population. The cut-off was set at 0.360 ± 0.068. (a). Comparison of OD450 values among age groups (18 - 35, 36-60, and 61 - 78 years); no significant differences were observed. (b). Comparison of OD450 values by sex; among positive results, a significant difference was observed between men and women (p value = 0.0469).
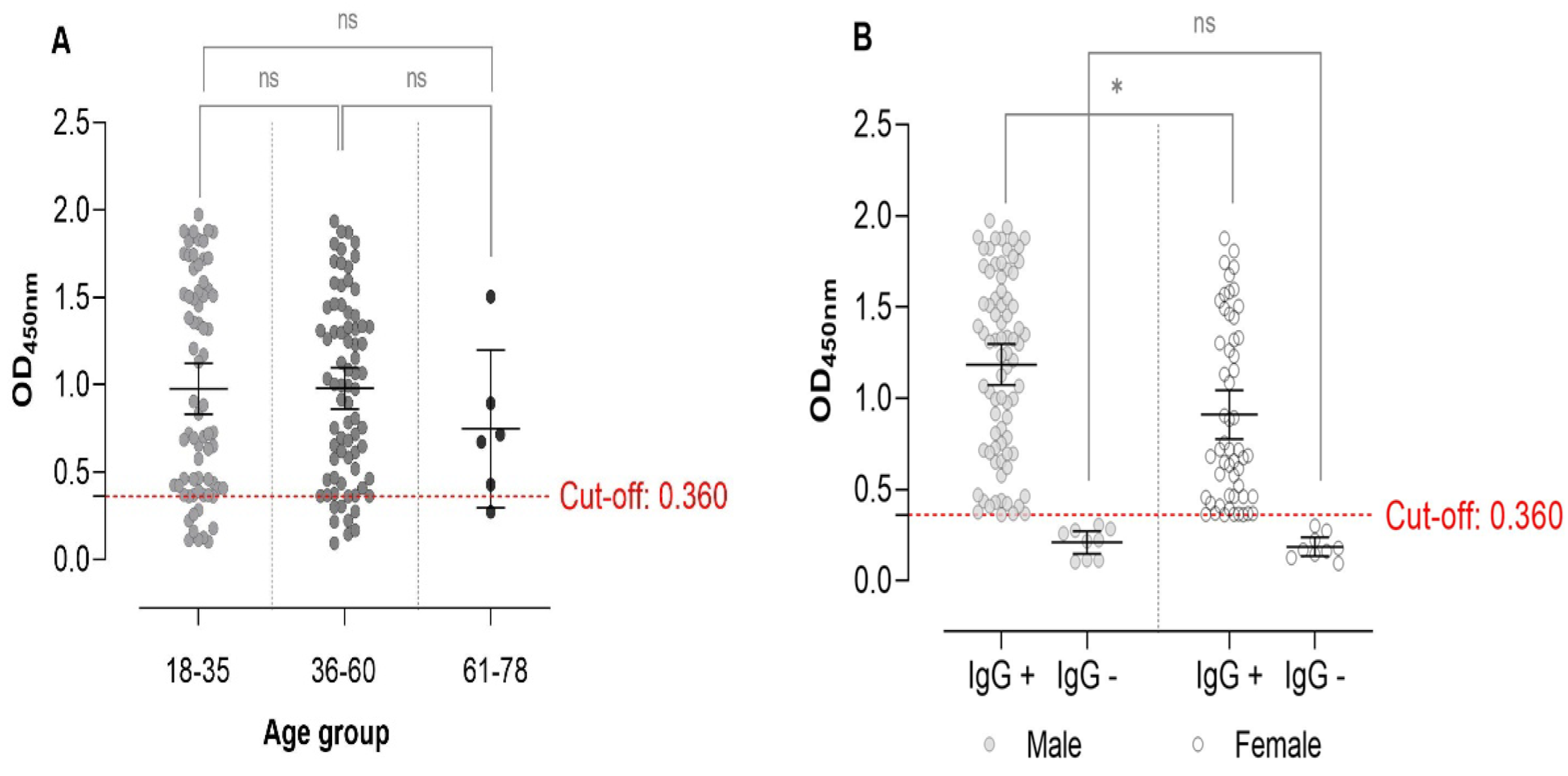

Table 1.
Characteristics of the Study Population (n = 151).
| Characteristics | Total, n (%) |
| Age Group | |
| 18 - 35 years | 70 (46.36) |
| 36 - 60 years | 75 (49.67) |
| 61 - 78 years | 6 (3.97) |
| Sex | |
| Male | 88 (58.28) |
| Female | 63 (41.72) |
| HIV Infection Status | |
| Positive | 92 (60.93) |
| Negative | 59 (39.07) |
| Seroprevalence of T. gondii | |
| Positive | 133 (88.08) |
| Negative | 18 (11.92) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



